Highlights
Opzelura (ruxolitinib) is a new drug indicated for the treatment of nonsegmental vitiligo in adults and children 12 years and older.
Appropriate regulatory approval was granted by the U.S. Food and Drug Administration (FDA) in mid-July 2022.
Opzelura, implemented in a cream formulation and developed by Incyte, debuted in late September 2021 for the topical short-term and non-continuous chronic treatment of mild to moderate atopic dermatitis in non-immunocompromised adults and pediatric patients aged 12 years and older whose disease is not adequately controlled with topical therapy or when such therapy is not advisable.
Ruxolitinib originally appeared in mid-November 2011 as the systemic oral drug Jakafi/Jakavi for the treatment of myelofibrosis (including primary myelofibrosis and secondary myelofibrosis due to polycythemia vera and essential thrombocythemia). Later it expanded the range of indications to include treatment of polycythemia vera and graft-versus-host disease.

Opzelura: Mechanism of Action of Ruxolitinib in Vitiligo
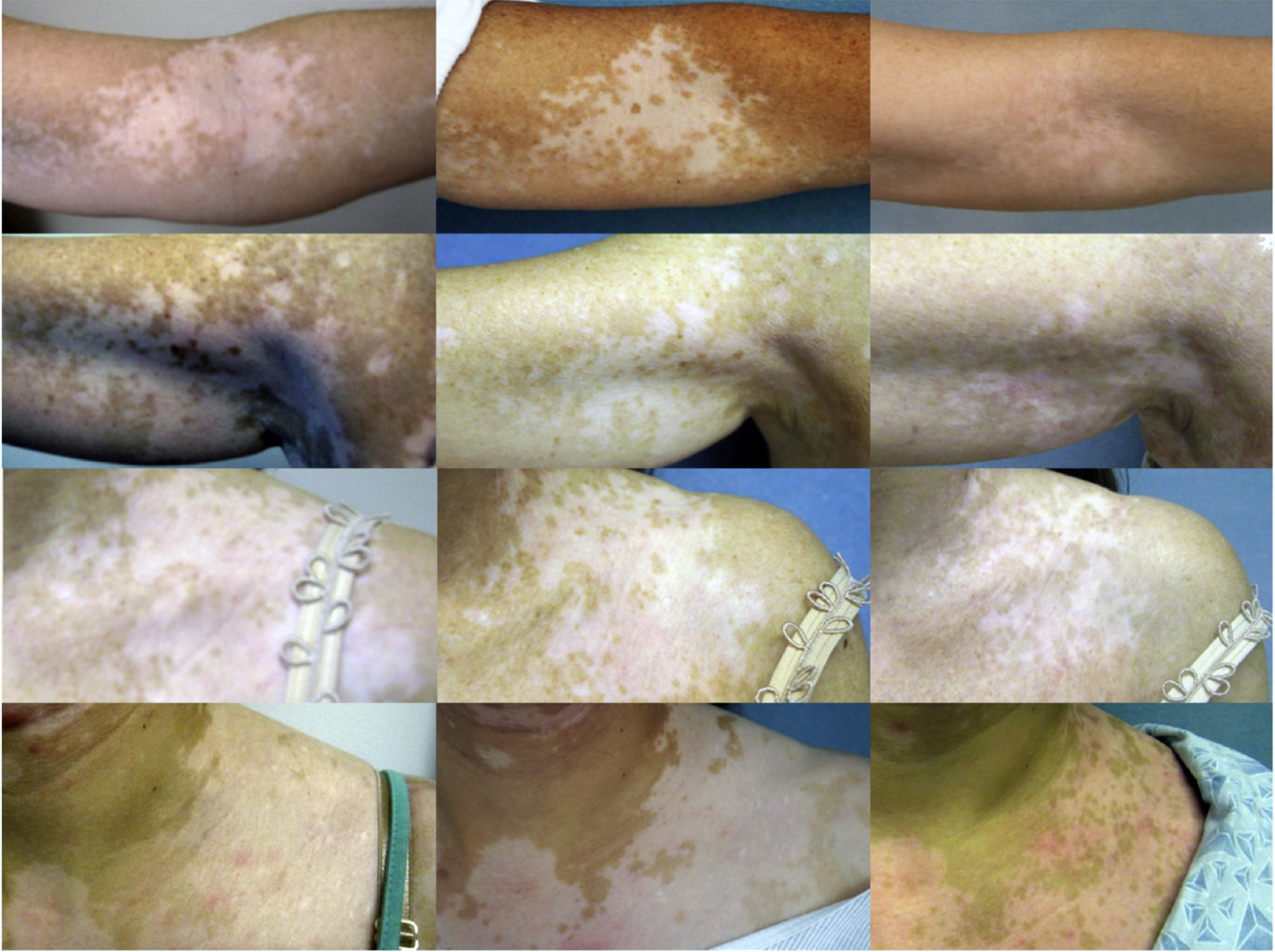
Depigmentation that characterizes vitiligo is caused by the progressive destruction of melanocytes. [1] In vivo and ex vivo studies have provided compelling evidence that melanocyte-specific CD8+ T cells preferentially infiltrate the dermal-epidermal junction adjacent to melanocytes at the border of depigmented lesions and are involved in melanocyte elimination and destruction. [2] [3] [4] [5]
Interferon gamma (IFN-γ), a key cytokine produced by CD8+ T cells, plays a central role in the pathogenesis of vitiligo. [6] Expression of IFN-γ-induced genes, including the T cell chemokine receptor CXCR3 and its multiple ligands (CXCL9, CXCL10, CXCL11), is upregulated in depigmented skin lesions. IFN-γ-induced gene expression is consistent with other findings: an enriched infiltration of CXCR3+ CD8+ T cells, including melanocyte-specific CD8+ T cells, found in vitiligo lesion biopsies, and increased CXCR3 receptor expression on melanocyte-specific T cells in the blood and skin of vitiligo patients. [7] [8] [9] [10] [11]
Based on numerous studies conducted in mouse models of vitiligo, the IFN-γ–chemokine axis and its associated positive feedback loop have been identified as a potential pathway in the initiation and progression of vitiligo. Autoreactive CD8+ T cells produce IFN-γ, which promotes depigmentation. IFN-γ simultaneously stimulates keratinocytes to express CXCR3, which binds to CXCL9 to recruit more melanocyte-reactive T cells. In addition, CXCL10 recruits T cells within the skin via the CXCR3 receptor, which contributes to the prolongation and aggravation of the formed vitiligo lesion. [9] [12] [13] [14]
Ruxolitinib is Janus kinase 1 and 2 (JAK1/JAK2) inhibitor that blocks the JAK/STAT signaling pathway, which is reflected by interruption of IFN-γ signaling pathogenic in vitiligo.
In addition, inhibition of JAK/STAT signaling pathway impairs detachment of melanocytes with low levels of E-cadherin expression in the basal layer of the epidermis, which is a critical step before melanocyte apoptosis. At the same time, the level of matrix metalloproteinase 9 (MMP-9) decreases. This is a powerful factor that is secreted by keratinocytes in response to IFN-γ and tumor necrosis factor (TNF). The level of MMP-9, which stimulates E-cadherin degradation, is elevated in skin and serum of patients with vitiligo. [15] [16]
Blocking the JAK/STAT signaling pathway inhibits interleukin 15 (IL-15) expression. In the pathogenesis of vitiligo relapse, oxidative stress through nuclear factor kappa B (NF-κB) signaling stimulates keratinocytes to express IL-15 and its receptor alpha subunit (IL-15Rα), which activate resident CD8+ memory T cells. [17]
The exact mechanism of action of ruxolitinib in vitiligo is not fully understood (clinical trial NCT04896385 is addressing this), but presumably ruxolitinib also inhibits dendritic cell (DC) differentiation and migration, which leads to a decrease in DC-induced antigen-specific CD4+ and CD8+ T cell responses and suppression of the induction of cytotoxic CD8+ T cell responses, which, as key cellular responses, are involved in the pathogenesis of vitiligo. [18]
The topical formulation of ruxolitinib implemented by Opzelura ensures proper blockade of JAK/STAT in the tissues on which this cream is applied, while the plasma concentration of the drug increases only slightly, which reduces the risk of serious adverse events that may accompany its systemic administration.
Opzelura: Clinical Efficacy and Safety of Ruxolitinib for Vitiligo Treatment
The efficacy and safety of topical ruxolitinib for the treatment of nonsegmental vitiligo were validated in two equally designed TRuE-V1 (NCT04052425) and TRuE-V2 (NCT04057573) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trials, which enrolled patients (n=674) aged 12 years and older whose total area of depigmented lesions in nonsegmental vitiligo on the face and body did not exceed 10% of body surface area. Phototherapy was not allowed during the studies.
Among the main characteristics of the subjects: women 53%, mean time from diagnosis of nonsegmental vitiligo to participation in the study was 14.8 years, Fitzpatrick skin types included I (2% of patients), II (30%), III (40%), IV (19%), V (7%), and VI (2%).
For 24 weeks, patients were administered Opzelura cream twice daily or placebo, and then all participants received Opzelura twice daily for 28 weeks.
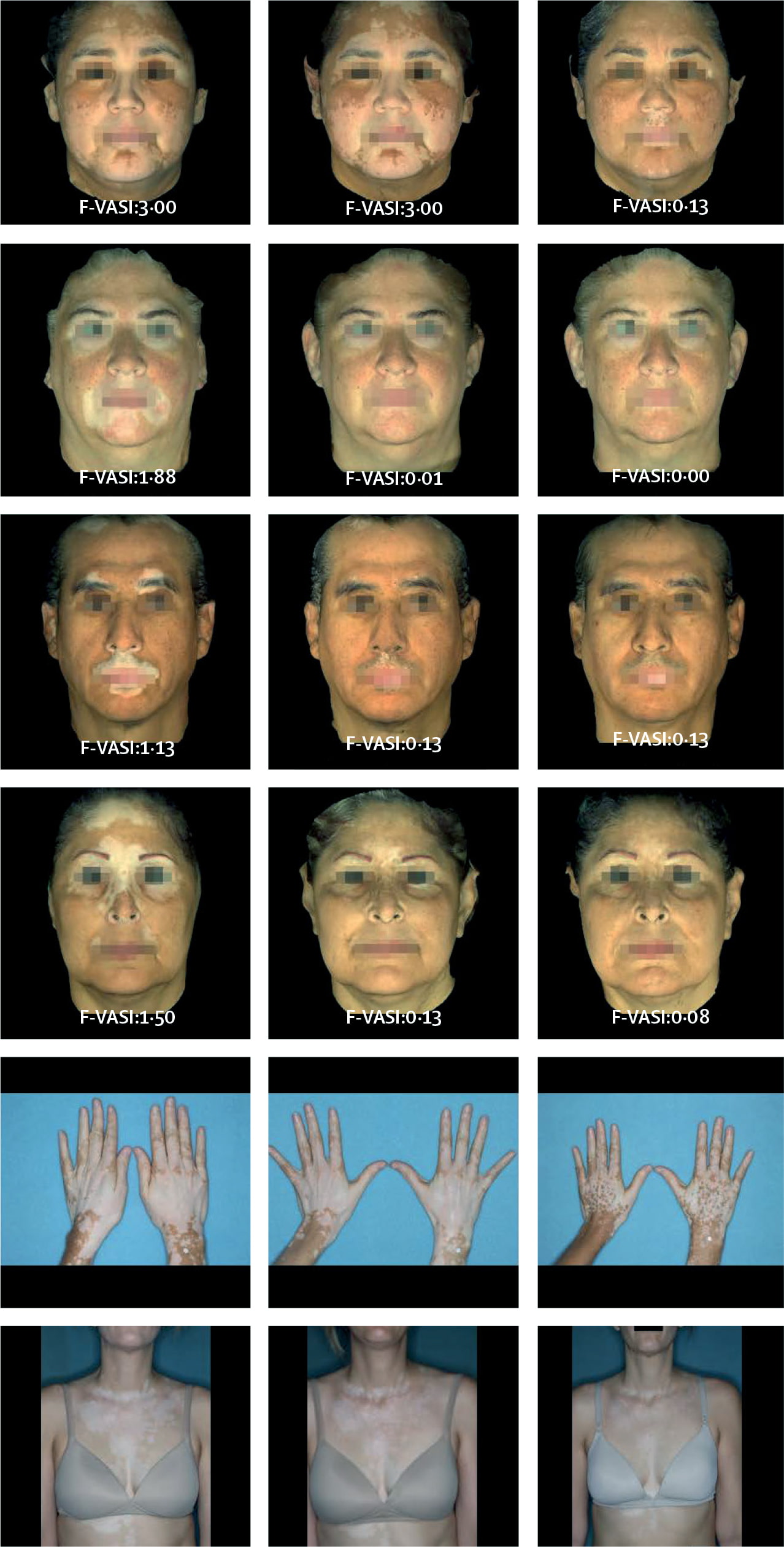
The primary efficacy endpoint for nonsegmental vitiligo treatment was the proportion of patients who, after 24 weeks of treatment, demonstrated at least a 75% improvement in score according to the facial Vitiligo Area Scoring Index (F-VASI75), that is, who showed proper skin repigmentation in areas of vitiligo.
In the TRuE-V1 and TRuE-V2 clinical trials, 30% of patients in the topical ruxolitinib groups reached F-VASI75 — versus 8% and 13% of patients in the placebo groups.
F-VASI90, indicating at least a 90% improvement in facial vitiligo spread, was true for 16% and 15% of subjects — vs. 2% in the control groups.
After an additional 28 weeks of therapy (52 weeks total), the response to Opzelura treatment improved significantly: F-VASI75 was recorded in 53% and 48% of patients and F-VASI90 was recorded in 33% and 28%.
In the NCT03099304 phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial it was shown that the effect of treating vitiligo with topical ruxolitinib twice daily improved according to the duration of treatment. Thus, if after 24 and 52 weeks of therapy 30% and 52% of patients reached F-VASI75, after 104 weeks 74%. After 52 and 104 weeks of treatment, F-VASI90 was observed in 33% and 58% of patients.
It was found that in some patients, repigmentation of vitiligo lesions can persist for a long time even after discontinuation of topical ruxolitinib, which had been treated for two years. Remarkably, no difference was found in changes in serum levels of CXCL9, CXCL10, and IL-15 between patients who retained skin repigmentation and those who experienced vitiligo recurrence after treatment discontinuation. Additional clinical validation is needed to be more reliable.
The addition of narrowband ultraviolet B (NB-UVB) phototherapy to topical ruxolitinib enhances the effect of vitiligo treatment. Thus, upon completion of a 52-week Opzelura administration, F-VASI75 and F-VASI90 were established for 42% and 21% of patients. After NB-UVB applied for at least 12 weeks, the proportions of patients who achieved the above indicators rose to 68% and 58%.
Opzelura was characterized by acceptable tolerability. Among the most common adverse events when prescribing topical ruxolitinib were application site acne (in 6% of patients), application site pruritus (5%), nasopharyngitis (4%), headache (4%), urinary tract infections (2%), application site erythema (2%), pyrexia (1%).
The prescribing information for Opzelura is provided, as in the case of any other JAK inhibitor, with a boxed warning regarding the risks of serious infections (bacterial, fungal, viral) including tuberculosis and opportunistic infections, major adverse cardiovascular events (myocardial infarction, stroke, cardiovascular death), thrombosis, and malignant tumors, including lymphoma. It should be understood that, first, such serious adverse events when prescribing JAK inhibitors are very rare and, second, the topical formulation of ruxolitinib further reduces their risks due to the absence of a significant plasma concentration of the drug.



Expert Comments
The emergence of a highly effective and relatively safe drug for the treatment of vitiligo has opened a new era in the management of this autoimmune disease, which imposes a heavy psychosocial burden on patients due to the fact that the skin depigmentation on the unclothed parts of the body, such as the face and hands, is dramatically evident to others, often unaware of the specificity of the disease, which is not contagious.
Existing topical vitiligo medications, including corticosteroids and calcineurin inhibitors, are essentially used off-label, and there are few controlled trials in large populations. [1] [2]
Results of a meta-analysis of topical corticosteroid therapy for vitiligo with a mean treatment duration of 8 months (2–21) showed that 56% of patients (6 studies) treated with potent corticosteroids (class III) achieved at least 75% repigmentation of vitiligo lesions, with methods for assessing repigmentation varying among studies. [3]
In a meta-analysis of vitiligo treatment with topical calcineurin inhibitors with a mean duration of therapy of 3 months (2–7), a minimum of 75% repigmentation was observed in 18% of patients (19 studies). [4]
Early responses to vitiligo therapy with ruxolitinib in a cream formulation are similar to those with topical calcineurin inhibitors or phototherapy. [4] [5] [6] Long-term administration of ruxolitinib significantly improves response to treatment, with no particular safety concerns, whereas long-term use of topical corticosteroids can lead to skin atrophy and calcineurin inhibitors to local reactions like burning. [3] [4]
Questions remain open regarding both the long-term use of topical ruxolitinib for vitiligo treatment (the safety profile of the drug should be clarified) and the possibility of pausing therapy or complete cancellation (an assessment of the likelihood of vitiligo relapse after achieving the desired efficacy of treatment from a repigmentation perspective is necessary).