Highlights
Amgen and AstraZeneca have launched Tezspire (tezepelumab), a new drug indicated for the add-on maintenance treatment of adult and pediatric patients aged 12 years and older with severe asthma.
Tezspire is approved by the U.S. Food and Drug Administration (FDA).
- Tezspire is not indicated for the relief of acute bronchospasm or status asthmaticus.
Tezspire is under regulatory review in Europe, Japan, and several other countries around the world.
Tezspire has successfully passed a clinical evaluation that confirmed its suitability for treating patients with severe asthma that cannot be controlled with existing medications.
Amgen and AstraZeneca, those behind the development of Tezspire, are excited, as Tezspire could revolutionize the treatment of severe asthma, which does not respond to the current pharmacological armamentarium of inhaled drugs, biologics, and oral corticosteroids.
Tezspire significantly reduced the number of asthma attacks, and did so, remarkably, regardless of eosinophilic disease status, allergic status, and fractional exhaled nitric oxide (FeNO), biomarkers assessed by clinicians in the task of selecting treatment options.
Because Tezspire works effectively without any linkage to the eosinophilic disease profile, it is suitable for a wide patient population. In about half of patients with severe asthma, it is not of the eosinophilic subtype. Tezspire is the first and only biologic for severe asthma that does not have a phenotype (eosinophilic or allergic) or biomarker limitation within its approved label
Tezspire is a drug that works differently from any other anti-asthmatic drugs currently on the market.
Yes, oral corticosteroids, which are cheap and widely available, are the mainstay of treatment for severe asthma but they come with an abundance of serious adverse events.
Industry estimates suggest that annual sales of Tezspire will exceed $750 million by 2026. Other projections are more optimistic believing that Tezspire will reach peak sales of $1.6 billion without much trouble and then grow to $3 billion a year.
In parallel, Tezspire is being investigated in the treatment of chronic obstructive pulmonary disease (COPD), chronic spontaneous urticaria (CSU), and severe chronic rhinosinusitis with nasal polyps (CRSwNP).
Asthma: Unmet Need for Powerful New Medicines
Asthma is a chronic inflammatory respiratory disease affecting approximately 339 million people worldwide. Of these, 10% have severe asthma, with persistent symptoms and exacerbations despite medium- and high-dose inhaled corticosteroid therapy (ICS), long-acting beta-agonists (LABA), and add-on medications.
Patients with severe asthma are at increased risk of exacerbations and are hospitalized twice as often as patients with nonsevere asthma. The severity of uncontrolled asthma results in high health care costs and poor quality of life due to excessive symptoms, life-threatening exacerbations, increased comorbidity, and high requirements for pharmacotherapy.
Current biologic drugs for severe asthma target immunoglobulin E (IgE), interleukin 5 (IL-5), IL-5 receptor alpha (IL-5RA), interleukin 4 (IL-4) receptor alpha (IL-4RA), and interleukin 13 (IL-13). Alas, all of these drugs — Xolair (omalizumab), Nucala (mepolizumab), Cinqair/Cinqaero (reslizumab), Fasenra (benralizumab) and Dupixent (dupilumab) — have limited indications: against asthma with an eosinophilic phenotype; with an allergic phenotype; severe asthma with type 2 inflammation and elevated levels of eosinophils and/or fractional exhaled nitric oxide (FeNO).
Moreover, clinical studies have found that the above anti-asthmatic drugs reduce the frequency of exacerbations by approximately 50% and result in variable improvements in lung function and symptom severity. The lack of complete treatment efficacy may be explained by the fact that the targets of the drugs offered are individual cytokines or cell types, while other components of the asthmatic inflammatory response remain untouched.
Thus, by targeting pharmacotherapy at some inflammatory mediator in the upstream signaling pathways that is triggered earlier in the inflammatory response and activates a greater variety of inflammatory pathways, cytokines, and cells, it might be possible to have a greater beneficial effect on asthma pathophysiology, thereby providing enhanced effective control of its course.
Such therapy would prove particularly relevant in patients with low eosinophil counts (including low inflammatory type 2); in asthma that is caused by multiple inflammatory pathways; and in disease that does not respond adequately to existing biologic drugs.
Tezspire: Tezepelumab and Treatment of Asthma — Mechanism of Action
Tezepelumab (AMG 157, MEDI9929) is a human monoclonal IgG2λ antibody targeted against thymic stromal lymphopoietin (TSLP) whose overexpression is seen in asthma and leads to its exacerbation, symptom complex, and physiological effects such as bronchoconstriction, hyperactivity, and airway remodeling. Tezepelumab specifically binds TSLP thereby blocking its interaction with its heterodimeric receptor. This is reflected by suppressing the production of a number of inflammatory cytokines and cells. Administration of tezepelumab results in decreased blood levels of eosinophils, serum immunoglobulin E (IgE), fractional exhaled nitric oxide (FeNO), interleukin 5 (IL-5), and interleukin 13 (IL-13).

Thymic stromal lymphopoietin is a cytokine produced by epithelial cells in response to pro-inflammatory stimuli and is involved in the initiation and maintenance of airway inflammation and is a key regulator of many inflammatory processes through the downstream signaling cascade. Among the triggers associated with asthma exacerbations are allergens, viruses, and other airborne particles. TSLP expression in the airways is increased in patients with asthma and correlates with disease severity.
Thymic stromal lymphopoietin is also involved in the pathogenesis of several allergic conditions. Elevated levels of TSLP protein are found in skin lesions in atopic dermatitis (eczema). Aberrant TSLP expression is seen in allergic diseases of the gastrointestinal tract, including Crohn’s disease, eosinophilic esophagitis, ulcerative colitis, and even cancer. Increased TSLP expression is seen in chronic obstructive pulmonary disease (COPD).
Tezspire: Tezepelumab in Treatment of Uncontrolled Severe Asthma — Efficacy and Safety
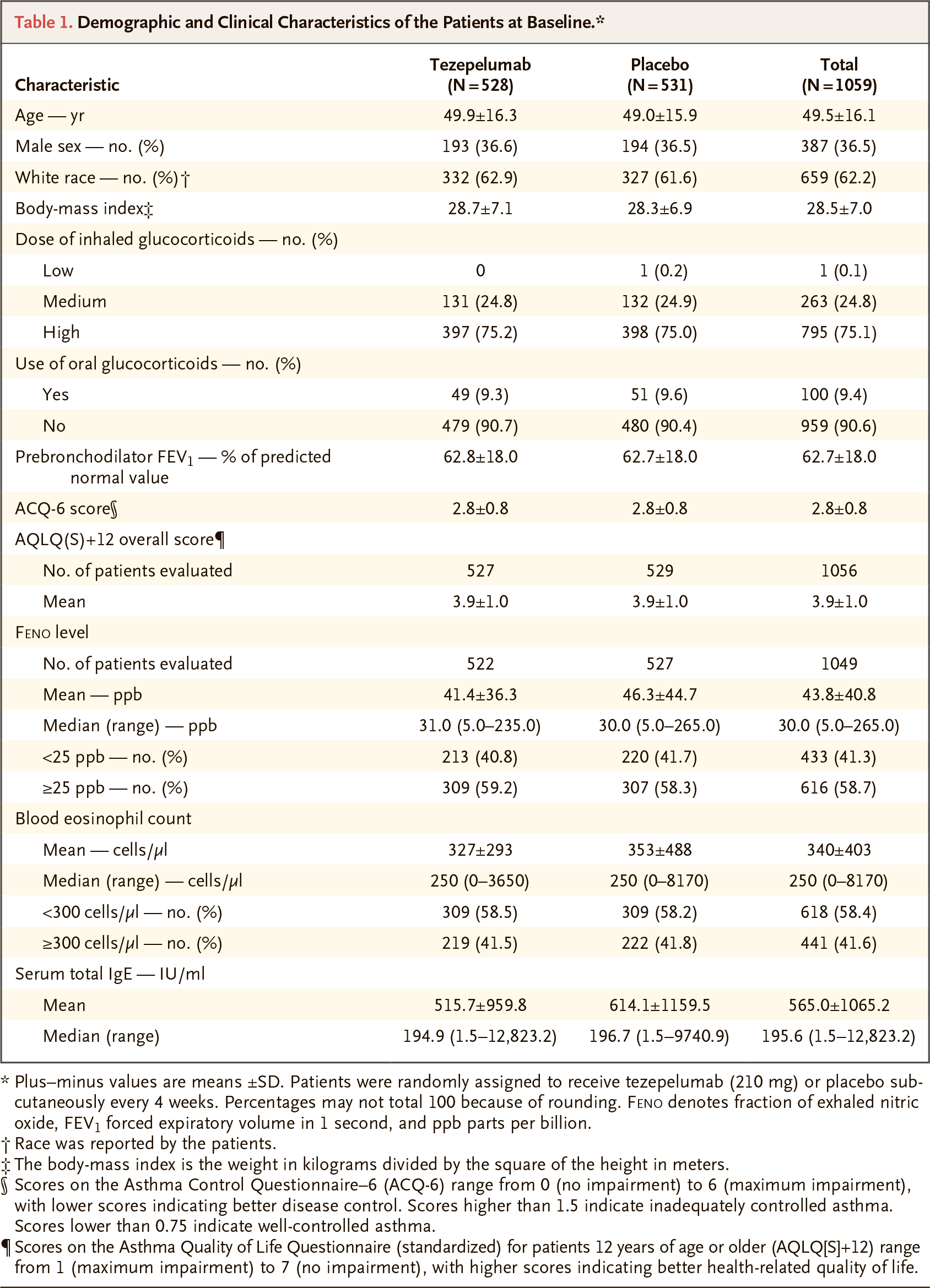
The NAVIGATOR (NCT03347279) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial enrolled patients (n=1060) of adult and adolescent age (12–80 years) with severe uncontrolled asthma, being treated with a single asthma controller medication (combined with or without an oral corticosteroid [OCS]) on medium- or high-dose inhaled corticosteroids (ICS) [equivalent to ≥500 mcg of fluticasone propionate cumulatively per day].
Mandatory participation criteria included: morning (before bronchodilator use [albuterol or salbutamol]) forced expiratory volume in 1 second (FEV1) <80% of predicted normal (<90% for subjects in adolescent age 12–17 years); Asthma Control Questionnaire-6 (ACQ-6) score ≥1.5; at least 2 asthma exacerbations in the past year.
The study recruited approximately equal proportions of patients with high (≥300 cells/μL) and low (<300 cells/μL) blood eosinophils.
The subjects, who continued on standard antiasthmatic therapy, were given placebo or tezepelumab by subcutaneous injection at a dose of 210 mg once a month for 48 weeks.
The primary endpoint was the annualized asthma exacerbation rate (AAER) during the 52-week therapy.
Tezspire group showed a 56% (95% CI: 47–63) decrease in AAER relative to the placebo group (p<0.001).
When outcomes were considered according to baseline eosinophil counts of ≥300, <300, and <150 cells/μL, administration of Tezspire resulted in a 70% (95% CI: 60–78; p<0.001), 41% (95% CI: 25–54; p<0.001), and 39% (95% CI: 12–58) drop in AAER, respectively.
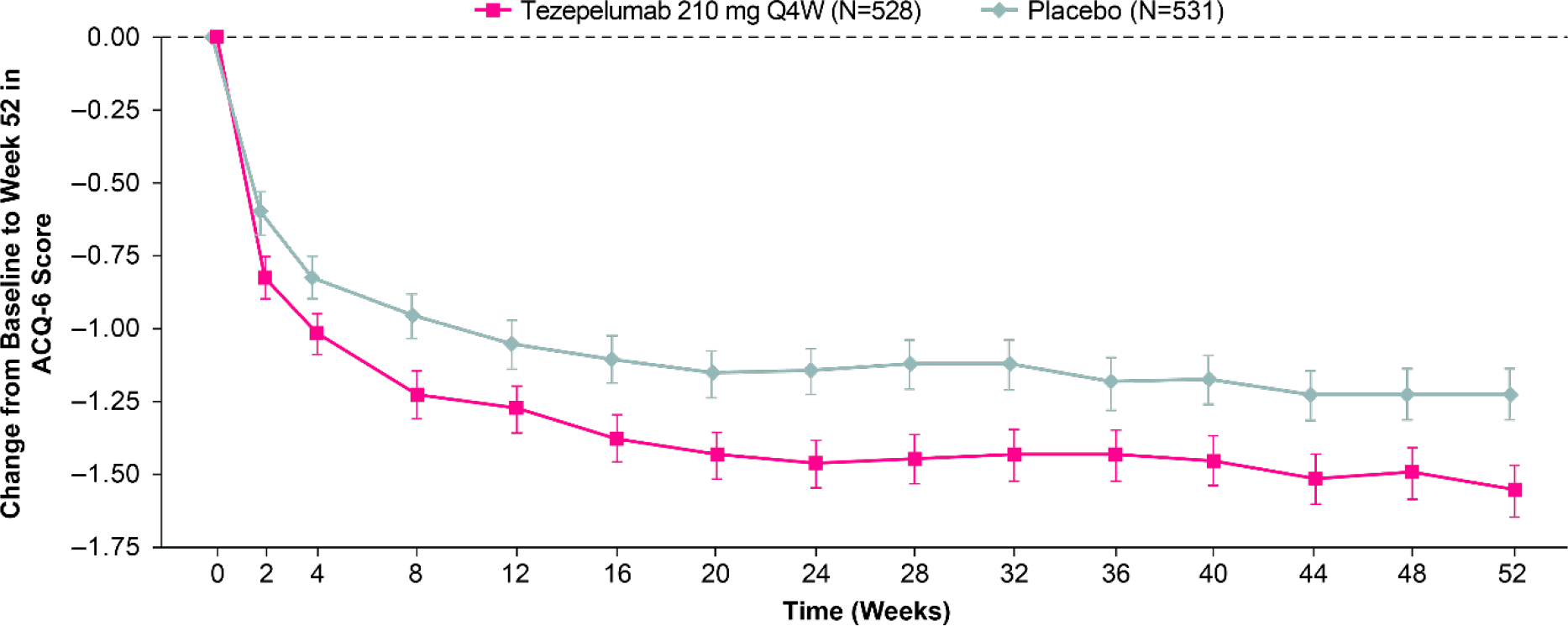
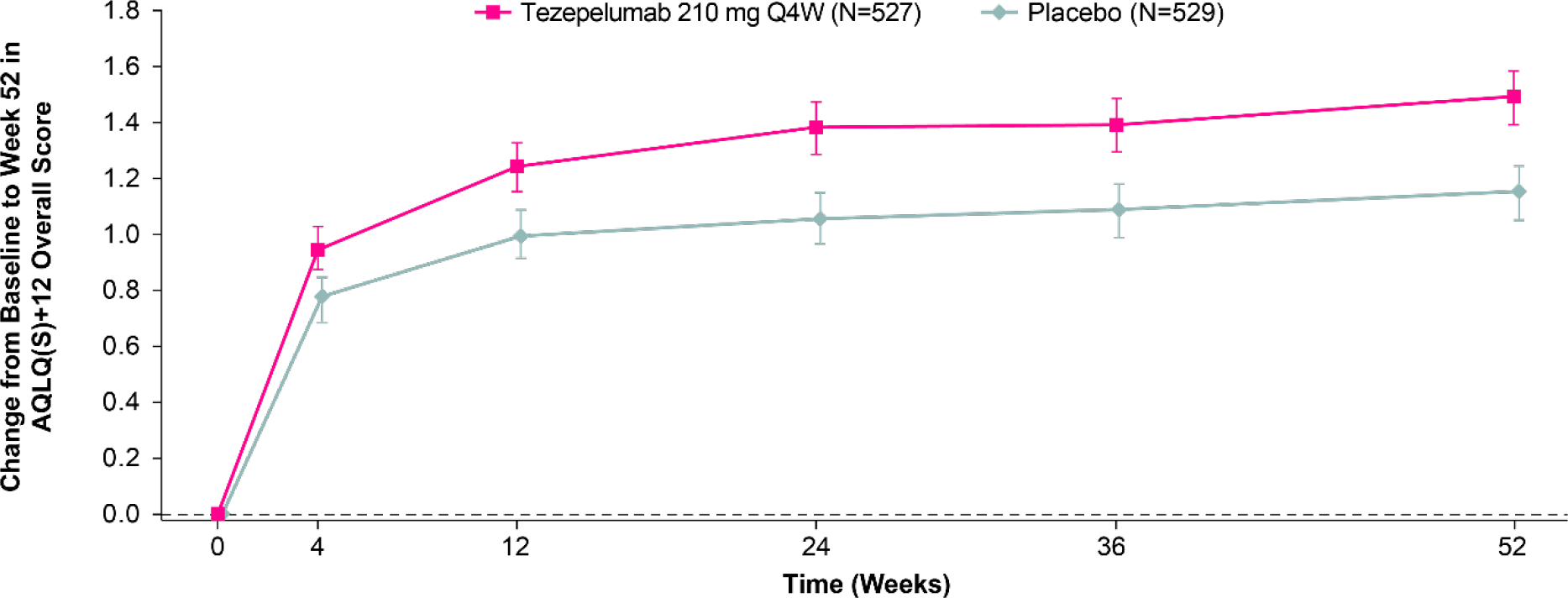
Use of Tezspire was reflected by a significant improvement (p<0.001) relative to placebo in secondary endpoints such as lung functions, asthma control, and health-related quality of life: FEV1, ACQ-6 score, and Standardized Asthma Quality of Life Questionnaire for 12 years and older (AQLQ[S]+12), respectively.
Tezspire reduced by 79% the frequency of such asthma exacerbations that lead to hospitalization or the need to seek emergency medical care.
Adverse events were experienced by 77.1% of patients in Tezspire group and 79.5% in the placebo group. Among the most common adverse reactions were nasopharyngitis, upper respiratory tract infections, and headache. The safety profile of tezepelumab was not associated with anaphylactic reactions, pneumonia, stroke, or Guillain–Barré syndrome; these have previously been reported including in the PATHWAY (NCT02054130) phase 2b clinical trial.
By the way, the PATHWAY confirmed that administration of tezepelumab provided a 61–71% reduction (depending on the dose) in severe uncontrolled asthma exacerbations and without association with patients’ eosinophilic profile or any other type 2 inflammatory biomarker.
Tezspire: Tezepelumab for Asthma — Full Results of Pivotal Clinical Trial
AstraZeneca and Amgen have provided the full results of the 52-week NAVIGATOR clinical trial.
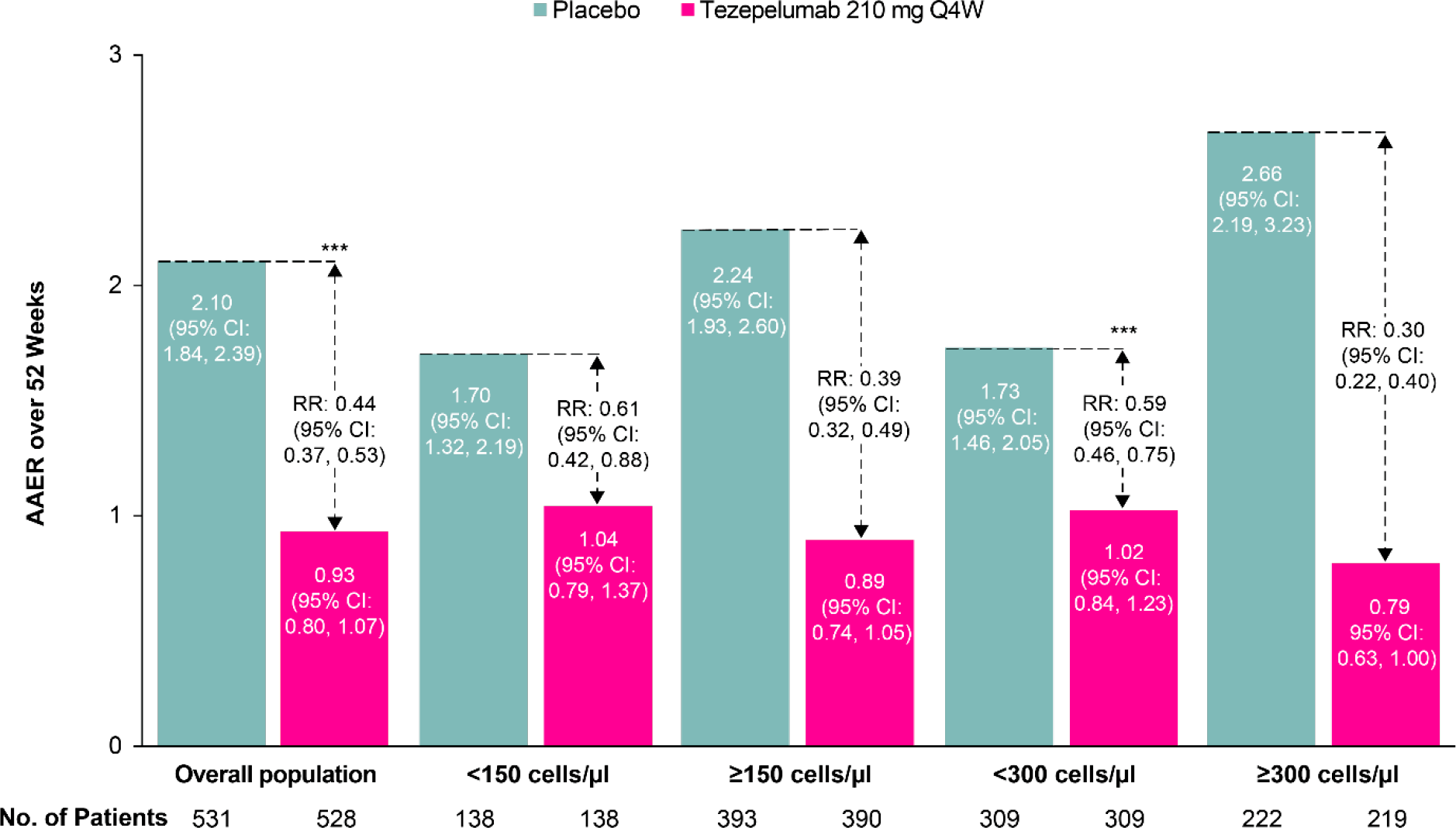
In Tezspire group, the annualized asthma exacerbation rate (AAER) was 0.93 (95% CI: 0.80–1.07) — versus 2.10 (95% CI: 1.84–2.39) in the placebo group: rate ratio (RR) 0.44 (95% CI: 0.37–0.53); p<0.001. In other words, therapy of asthma with tezepelumab resulted in a 56% reduction in the risk of asthma exacerbation. The drug also clearly delayed the time to the first exacerbation.

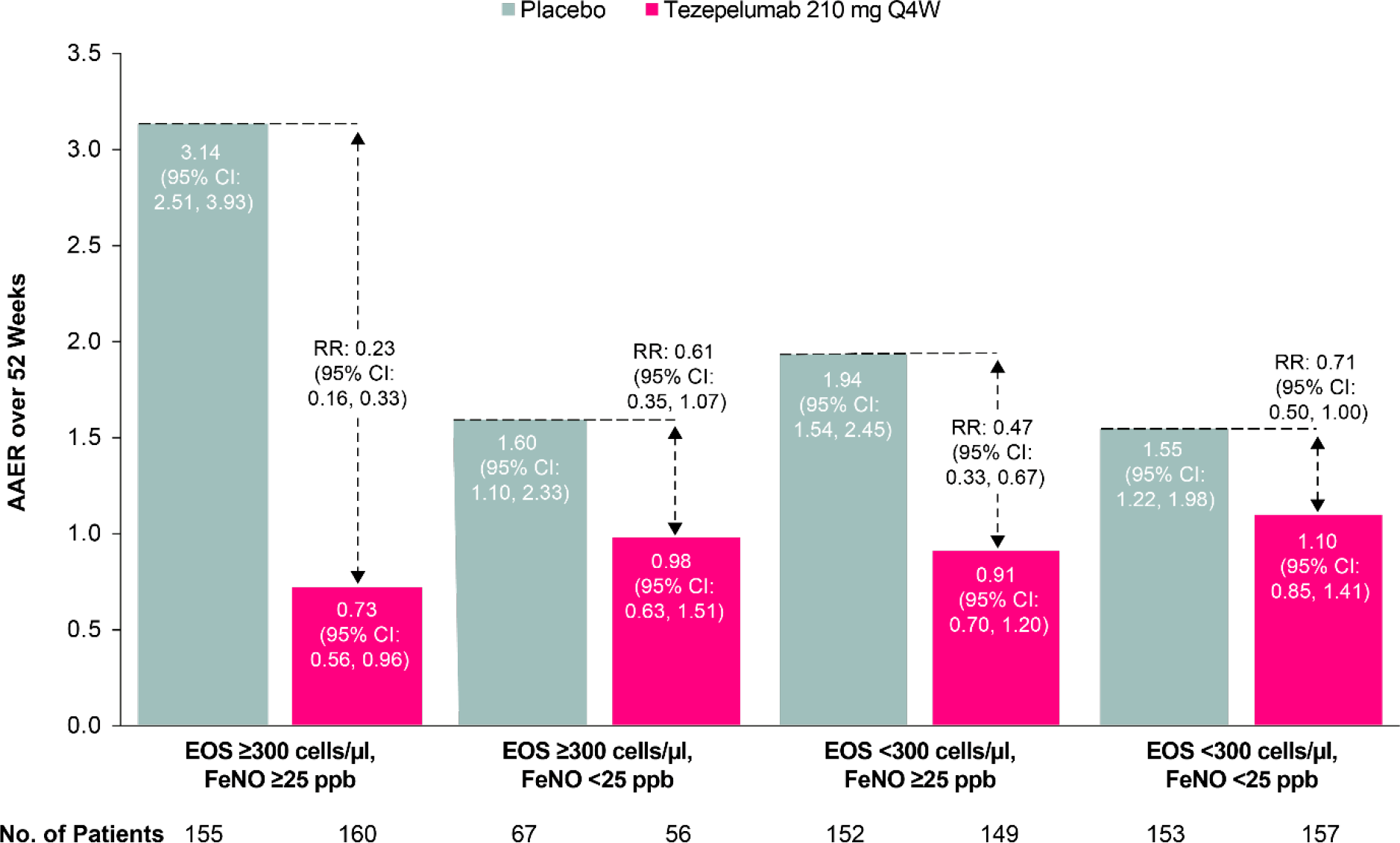
Tezspire therapy was effective regardless of asthma biomarkers — eosinophilic disease status (blood eosinophil count), fractional exhaled nitric oxide (FeNO), or allergic status. Although, however, the efficacy of treatment was still better with severe eosinophilia or high FeNO levels.
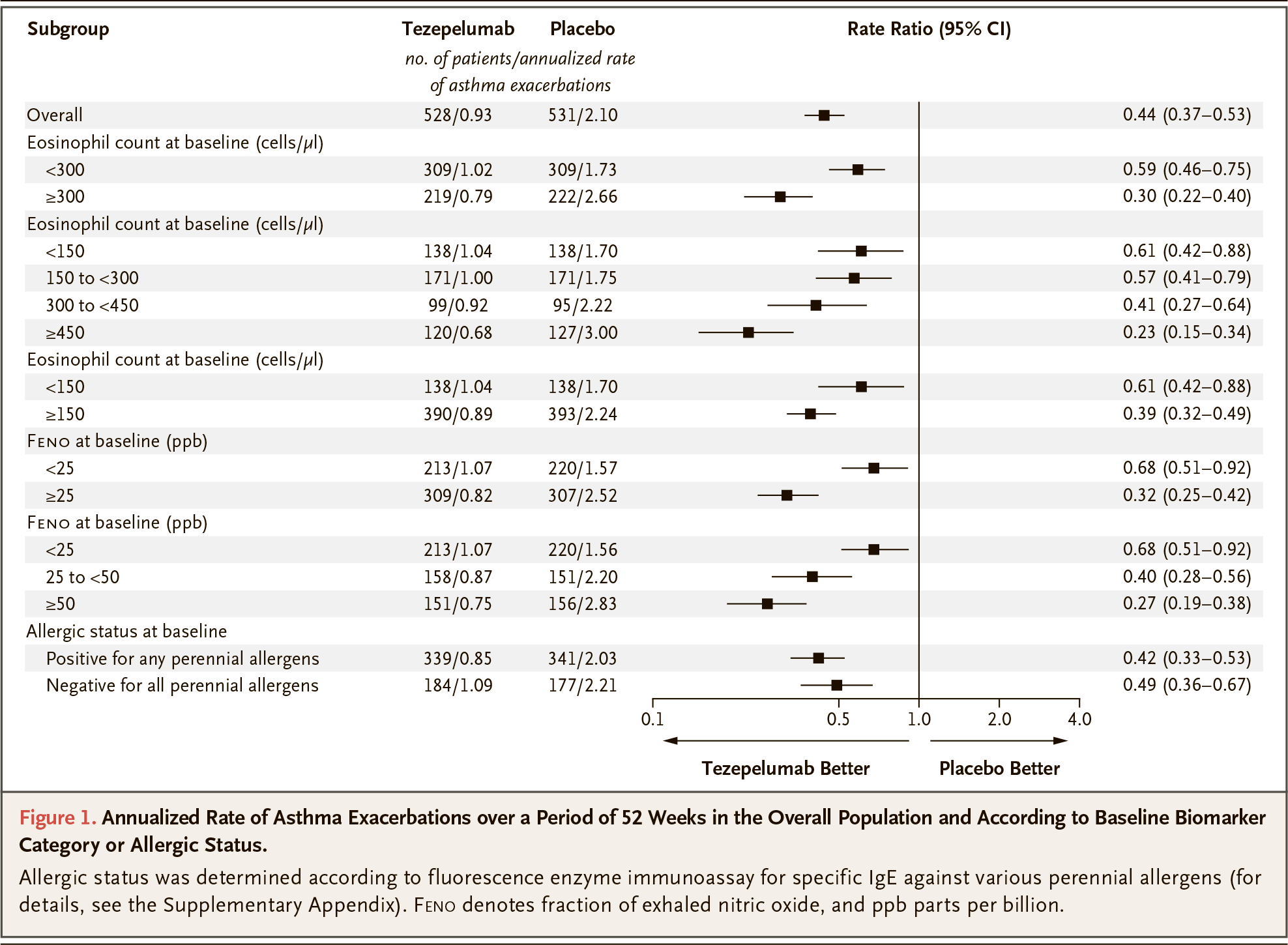
Thus, when the blood eosinophil counts were less than 300 cells/μL, the AAER was 1.02 (95% CI: 0.84–1.23) in the tezelumab group — versus 1.73 (95% CI: 1.46–2.05) in the placebo group: RR 0.59 (95% CI: 0.46–0.75); p<0.001. If eosinophil counts exceeded 300 cells/μL, AAER was 0.79 (95% CI: 0.63–1.00) — vs. 2.66 (95% CI: 2.19–3.23): RR 0.30 (95% CI: 0.22–0.40).
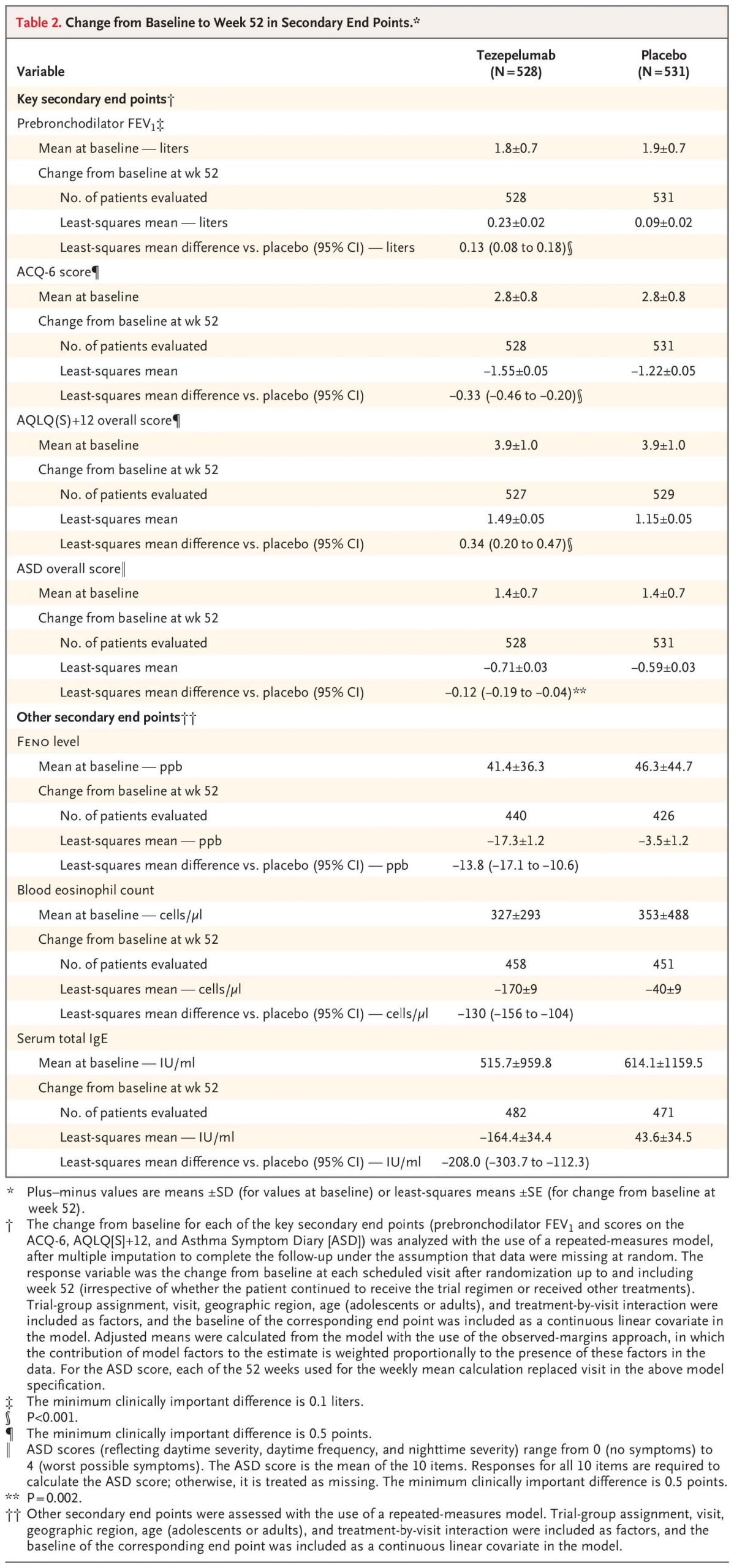
At the end of the clinical trial, prebronchodilator forced expiratory volume in 1 second (FEV1) increased by 0.23 L — versus 0.09 L: difference 0.13 L (95% CI: 0.08–0.18); p<0.001. The therapeutic effect here began to be observed at week 2 of treatment sustaining throughout the study.

Changes in other secondary points were as follows:
- Asthma Control Questionnaire–6 (ACQ-6) score: −1.55 — versus −1.22, difference −0.33 (95% CI: −0.46 — −0.20), p<0.001
- Standardized Asthma Quality of Life Questionnaire for 12 years and older [AQLQ(S)+12] score: +1.49 — vs. +1.15, difference 0.34 (95% CI: 0.20–0.47), p<0.001
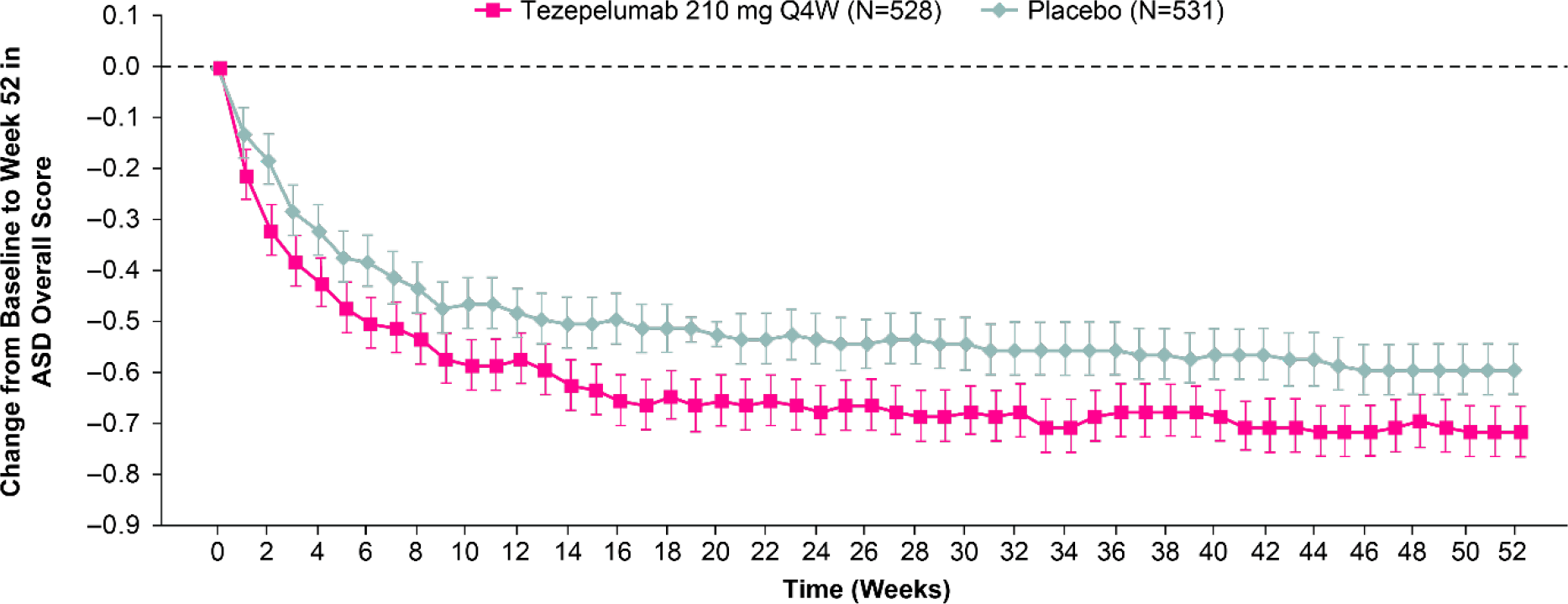
- Asthma Symptom Diary (ASD) score: −0.71 — vs. −0.59, difference −0.12 (95% CI: −0.19 — −0.04), p=0.002.
The incidence of such asthma exacerbations that forced an emergency visit or led to hospitalization was 0.06 (95% CI: 0.04–0.09) among patients who received tezepelumab — versus 0.28 (95% CI: 0.20–0.37) in the control group: RR 0.21 (95% CI: 0.12–0.37).
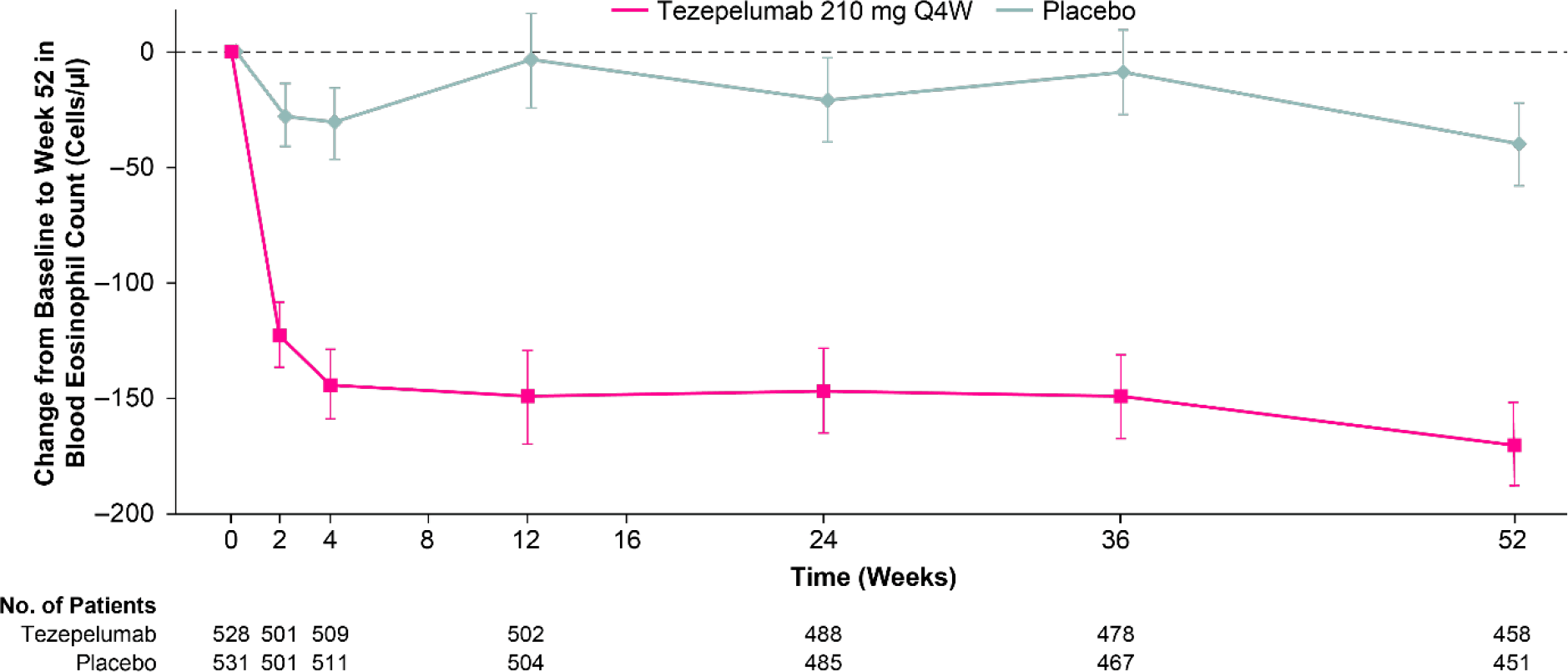
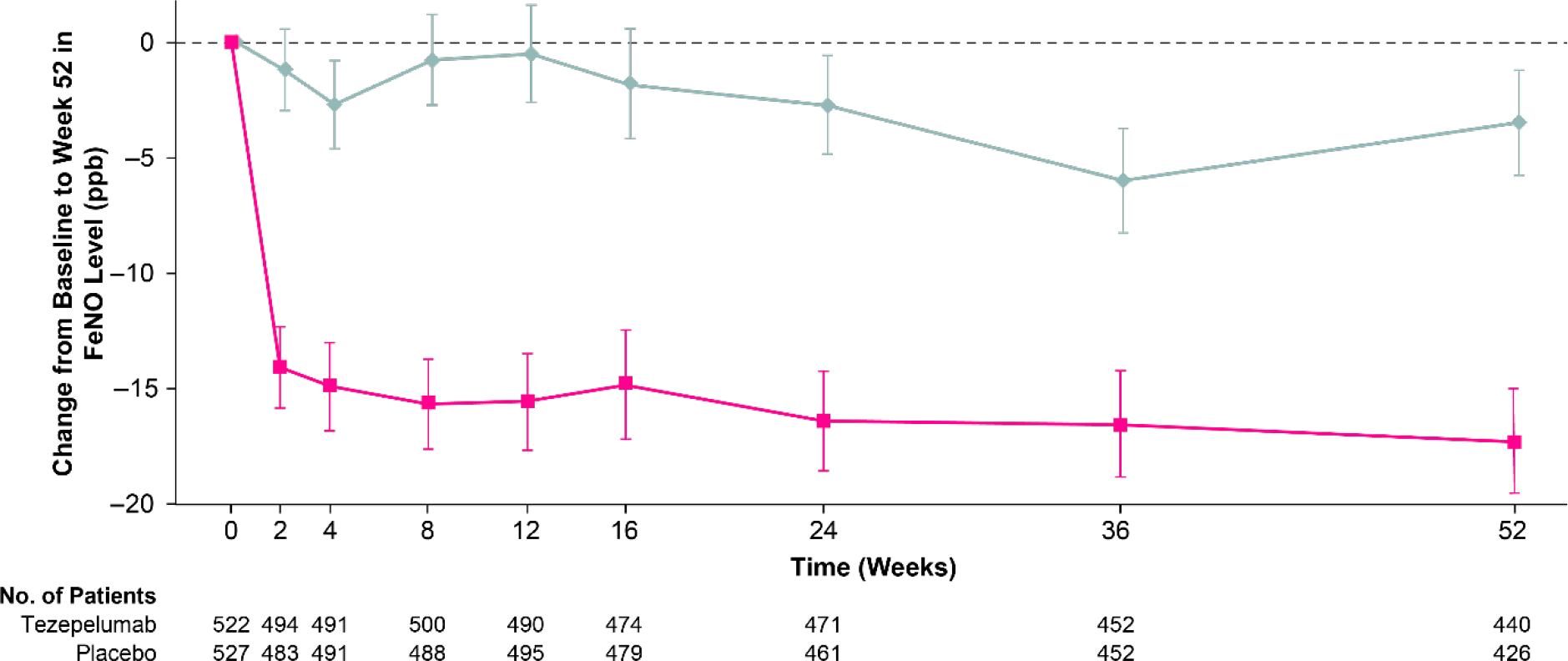
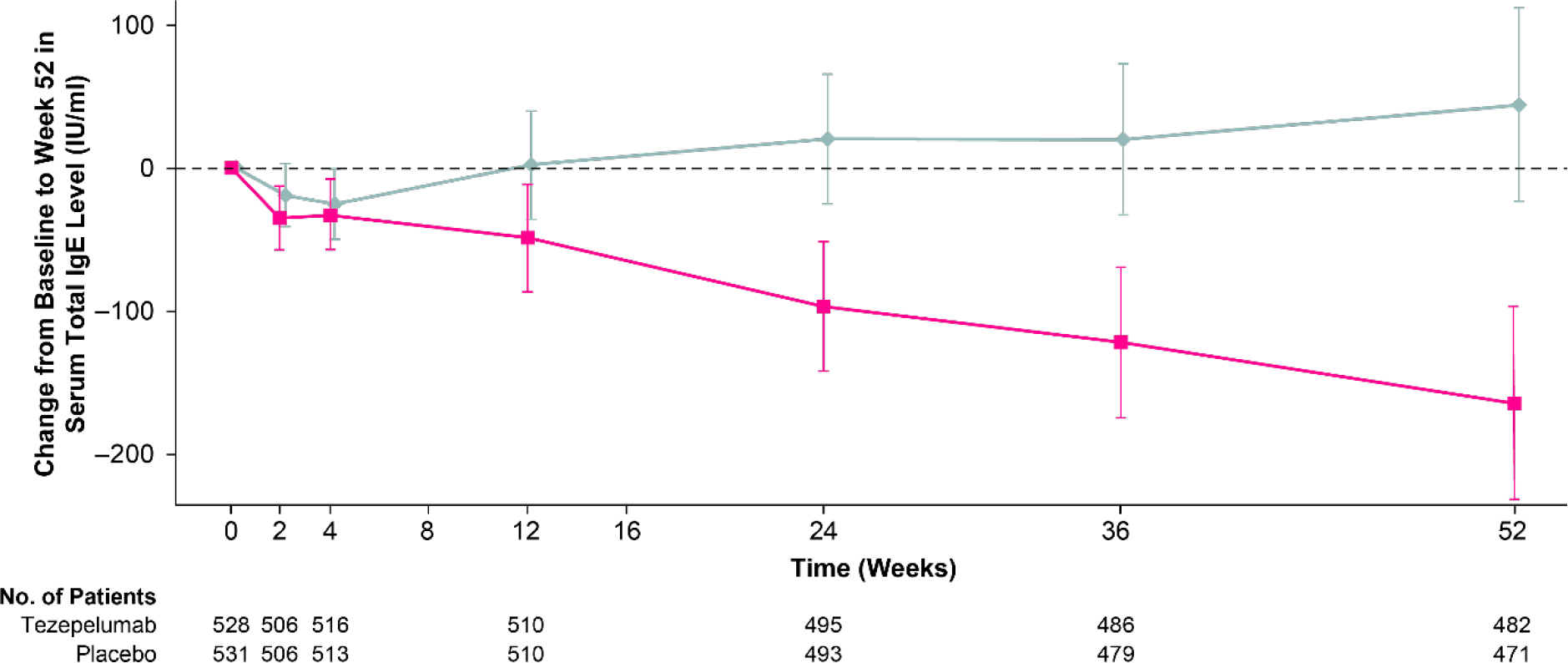
Administration of Tezspire resulted in a decrease in eosinophil counts and FeNO levels starting at week 2 of treatment. Serum total immunoglobulin E (IgE) levels gradually decreased throughout the 52-week therapy period.
Tezspire: Tezepelumab in Asthma — Important Points
The 70% reduction in the frequency of asthma exacerbations per year that tezepelumab has produced in the therapy of eosinophilic asthma (≥300 cells/μL) gives it a strong competitive position in the face of already existing biological drugs.
The fact that Tezspire has also shown beneficial therapeutic effects in patients with asthma without an eosinophilic profile (<150 cells/μL) suggests that the drug, if it passes the regulatory approval step, could be used on a broad patient population.
For example, the best-selling Dupixent (dupilumab), a monoclonal antibody against interleukin 4 (IL-4) and interleukin 13 (IL-13) promoted by Sanofi and Regeneron Pharmaceuticals, failed to outperform placebo in this subgroup of asthmatics.
Apparently, targeting thymic stromal lymphopoietin (TSLP) by tezepelumab is more optimal than targeting individual cytokines downstream of the inflammatory cascades. This is why Tezspire has proven to be suitable for the treatment of asthma without any clinical biomarker at all. It should be understood that current anti-asthmatic biologic drugs bypass non-eosinophilic asthma, although such patients are approximately half of all asthma sufferers.
The only complaint about tezepelumab is that it failed to reduce the dose of daily oral corticosteroids without losing asthma control. The unsuccessful SOURCE (NCT03406078) phase 3 clinical trial may be due to its duration. The dose reduction was carried out over 36 weeks, whereas a similar trial of Fasenra, Dupixent and Nucala lasted shorter, 16–20 weeks.
- It should be understood that Tezspire was still able to favorably affect corticosteroid dependence: in the experimental drug group, a numerically large proportion of patients achieved at least a 90% reduction in their corticosteroid dose — 54.1% of patients versus 46.1% in the placebo group.
Anti-asthmatic Biological Drugs
Xolair
Xolair (omalizumab) by Roche and Novartis targets immunoglobulin E (IgE) and approved for the treatment of moderate-to-severe asthma with an allergic phenotype.
Nucala
Nucala (mepolizumab) by GlaxoSmithKline targets interleukin 5 (IL-5) and approved for the treatment of severe asthma with an eosinophilic phenotype.
Cinqair/Cinqaero
Cinqair/Cinqaero (reslizumab) by Teva Pharmaceutical Industries targets IL-5 and approved for the treatment of severe asthma with an eosinophilic phenotype.
Fasenra
Fasenra (benralizumab) by AstraZeneca targets IL-5 receptor alpha (IL-5RA) and approved for the treatment of severe asthma with an eosinophilic phenotype.
Dupixent
Dupixent (dupilumab) by Sanofi and Regeneron Pharmaceuticals targets interleukin 4 (IL-4) receptor alpha (IL-4RA), shared by IL-4 and interleukin 13 (IL-13), and approved for the treatment of severe asthma with an eosinophilic phenotype or with oral corticosteroid dependence.
Extras
Tezspire (tezepelumab). Prescribing information. US. [PDF]
Tezepelumab: a differentiated, first-in-class investigational therapy for a broad population with severe uncontrolled asthma. Amgen. February 26, 2021. [PDF]
Efficacy and safety of tezepelumab in adults and adolescents with severe, uncontrolled asthma: results from the phase 3 NAVIGATOR study. [PDF]
Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med. 2021 May 13;384(19):1800-1809. [source]
Tezepelumab — use in patients with OCS-dependent asthma. AstraZeneca, Medical Information Department. May 14, 2021. [PDF]
Tezepelumab — mechanism of action in asthma. AstraZeneca, Medical Information Department. May 14, 2021. [PDF]
Tezepelumab — general safety and tolerability in asthma. AstraZeneca, Medical Information Department. May 14, 2021. [PDF]
Tezepelumab — NAVIGATOR asthma exacerbation study. AstraZeneca, Medical Information Department. May 12, 2021. [PDF]
Efficacy and safety of tezepelumab in adults and adolescents with severe, uncontrolled asthma: results from the phase 3 NAVIGATOR study. American Academy of Allergy, Asthma & Immunology (AAAAI) 2021 Virtual Annual Meeting, February 26–March 1, 2021. [PDF]
NAVIGATOR: a phase 3 multicentre, randomized, double-blind, placebo-controlled, parallel-group trial to evaluate the efficacy and safety of tezepelumab in adults and adolescents with severe, uncontrolled asthma. Respir Res. 2020 Oct 13;21(1):266. [source]
SOURCE: a phase 3, multicentre, randomized, double-blind, placebo-controlled, parallel group trial to evaluate the efficacy and safety of tezepelumab in reducing oral corticosteroid use in adults with oral corticosteroid dependent asthma. Respir Res. 2020 Oct 13;21(1):264. [source]
Tezepelumab treatment effect on annualized rate of exacerbations by baseline biomarkers in uncontrolled severe asthma patients: phase 2b PATHWAY study. American Thoracic Society (ATS) Congress, May 17–22, 2019. [PDF]
Tezepelumab in adults with uncontrolled asthma. N Engl J Med. 2017 Sep 7;377(10):936-946. [source]