Novartis has offered Mayzent (siponimod), a new drug that belongs to disease-modifying therapy (DMT) of multiple sclerosis.
Mayzent, approved by the U.S. Food and Drug Administration (FDA) in March 2019, is intended to treat adult patients with relapsing forms of this demyelinating disease, including clinically isolated syndrome (CIS), relapsing-remitting multiple sclerosis (RRMS), and secondary progressive multiple sclerosis (SPMS) in its active form (that is, still accompanied by relapses).
Mayzent has become the first medication in the United States approved for active secondary progressive multiple sclerosis. This form of the disease is characterized by a gradual deterioration of neurological functions, over time leading to a progressive accumulation of disability (irreversible and mostly independent of relapses), which seriously affects patients’ ability to perform even simple everyday tasks. Patients usually progress to SPMS after the initial phase of RRMS, the most common (85% of initial diagnoses) form of this immune-mediated disease. Half of the patients develop SPMS within ten years of RRMS diagnosis, and 90% develop SPMS within 25 years.
By the way, a few days later, Mavenclad (cladribine) by Merck KGaA, approved for therapy of relapsing forms of multiple sclerosis, including active secondary progressive multiple sclerosis, entered the U.S. market. In August 2019, the medical instructions for the drug Gilenya (fingolimod) appeared to indicate that it can be prescribed for active secondary progressive multiple sclerosis.
Given the vast patient population suitable for Mayzent therapy, its sales will reach $1.3 billion by 2024, according to industry forecasts.
In January 2020, Mayzent received marketing approval in the European Union: siponimod is approved by the European Medicines Agency (EMA) for therapy of adult patients with secondary progressive multiple sclerosis in an active form, the presence of which is confirmed by relapses or inflammatory activity on magnetic resonance imaging (MRI).
In November 2019, Mayzent was approved in Australia. In June 2020, Japan issued a favorable verdict for Mayzent. In December 2020, siponimod came to Russia under the brand name Kiendra. Interestingly, regulators in these countries have approved siponimod for the therapy of secondary progressive multiple sclerosis regardless of the activity of the disease.

Mayzent: Mechanism of Action of Siponimod
Siponimod is an oral selective agonist of sphingosine-1-phosphate (S1P) receptor subtypes 1 (S1PR1) and 5 (S1PR5). The immunomodulatory mechanism of action of siponimod is due to the internalization and degradation of sphingosine-1-phosphate in the ubiquitin-proteasome metabolic pathway, which leads to suppression of migration of a particular subtype of activated lymphocytes (T helpers CD4+ CCR7+ and T killers CD8+ CCR7+) to sites of inflammation while maintaining the integrity of immunological surveillance. Siponimod both sequestered lymphocytes into peripheral lymphoid organs, eliminating them from areas of chronic inflammation, and promoted remyelination and prevention of synaptic defects.
Thus, by binding to S1PR1 on lymphocytes, siponimod prevents their migration to the central nervous system (CNS), providing an anti-inflammatory effect. The molecule, penetrating the CNS, binds to S1PR5 on oligodendrocytes and astrocytes, modulating destructive cellular activity and helping to curb the deterioration of neurological functions associated with SPMS.

Mayzent is appropriately positioned as an improved version of Gilenya (fingolimod), for which Novartis received approval in September 2010 for therapy of relapsing-remitting multiple sclerosis. Gilenya earned $3.15 billion, $3.23 billion, and $3.34 billion in 2016, 2017, and 2018. However, the cash flow has already begun to dry up due to the emergence of less expensive generics of fingolimod. Therefore, the Swiss pharma giant was very concerned about the rapid introduction of a promising replacement.
Fingolimod, being a non-specific S1P modulator, binds to its receptors 1, 3, 4, and 5 (S1PR1, S1PR3, S1PR4, and S1PR5), which is why prescribing Gilenya is associated with the risk of bradycardia and atrioventricular blockade.
Siponimod, due to its selectivity, should be characterized by less prominent safety problems, but this is not the case at all.
Moreover, prescribing Mayzent does require mandatory pre-testing for cytochrome P450 2C9 (CYP2C9) genotype, whose gene, being extremely polymorphic, can lead to serious changes in this enzyme activity, which is reflected by a restriction of any drug or adjustment of its dose.
Siponimod’s direct competitor is ozanimod, a selective agonist of exactly the same 1 and 5 sphingosine-1-phosphate receptor subtypes, which Celgene was developing. Ozanimod was supposed to hit the market in late 2018 but Celgene was inexcusably negligent and careless by sending an incomplete new drug application (NDA) to the regulator. And so additional work had to be done to prepare an updated NDA which was not sent to regulators until late March 2019.

Zeposia: New Drug to Treat Relapsing Multiple Sclerosis
Bristol-Myers Squibb has come up with ozanimod, a direct competitor to Novartis’ fingolimod and siponimod, for the treatment of multiple sclerosis.
Mayzent: Efficacy of Treatment of Multiple Sclerosis With Siponimod
The efficacy of Mayzent was demonstrated in the EXPAND (NCT01665144) phase 3 clinical trial (randomized, double-blind, placebo-controlled, parallel-group, multicenter, international), which enrolled adult patients (n=1651) with secondary progressive multiple sclerosis and 3.0–6.5 points on the Extended Disability Status Scale (EDSS). On average, participants had 16.8 years of disease and 3.8 years from the time the pathology evolved into SPMS, with two years of disability progression before participation in the study.
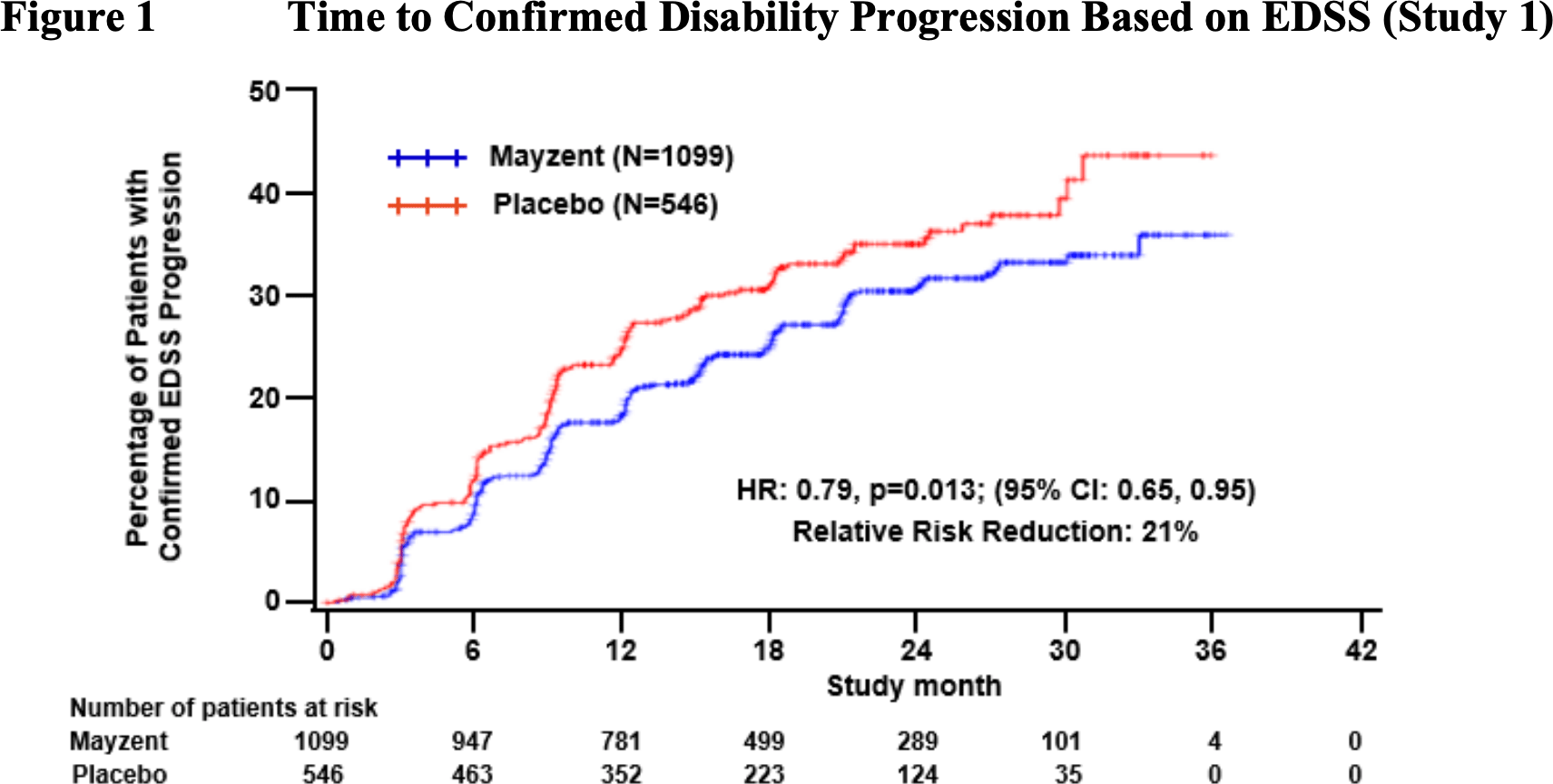
Patients received oral siponimod or placebo daily for a maximum of three years or until a predetermined number of Confirmed Disability Progression (CDP) events occurred. The primary endpoint was the time to CDP onset, whose status was fair for three months. The CDP score was defined by a 1 or 0.5 point deterioration in EDSS — with a baseline EDSS of 3.0–5.0 or 5.5–6.5, respectively.
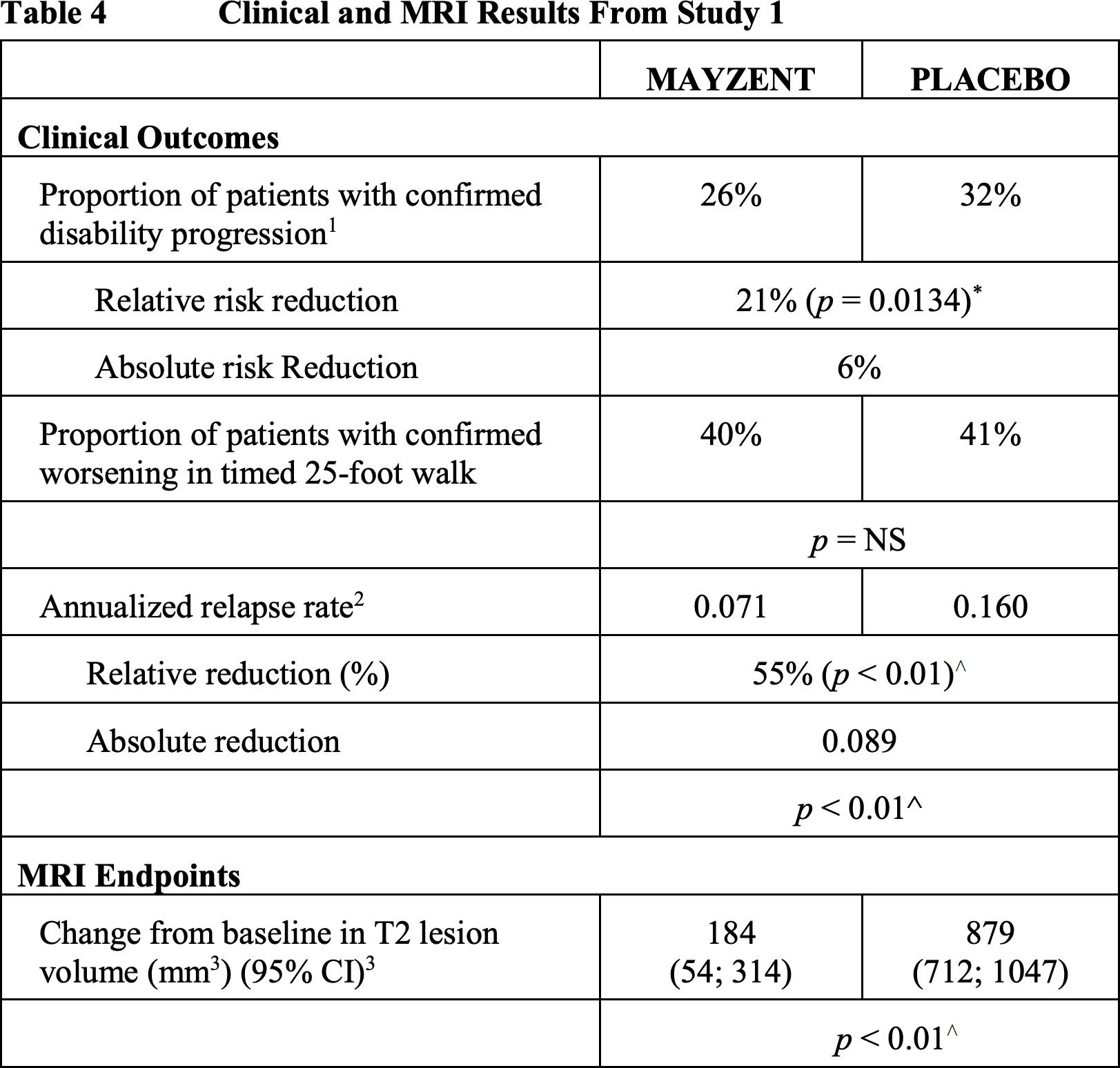
The main results of the siponimod trial are as follows:
- the reduction in risk of 3-months CDP was at 21% (hazard ratio [HR] 0.79; p=0.013)
- reduction in the risk of 6-month CDP came out to 26% (HR 0.74; p=0.0058)
- demonstrated a 55% reduction in annualized recurrence rate (ARR): 0.07 vs. 0.016 (HR 0.45; p<0.0001)
- there was a 46% reduction in the risk of experiencing a first relapse (HR 0.54; p<0.0001)
- documented a relative 23% slowing of the rate of brain volume shrinkage (p=0.0002)
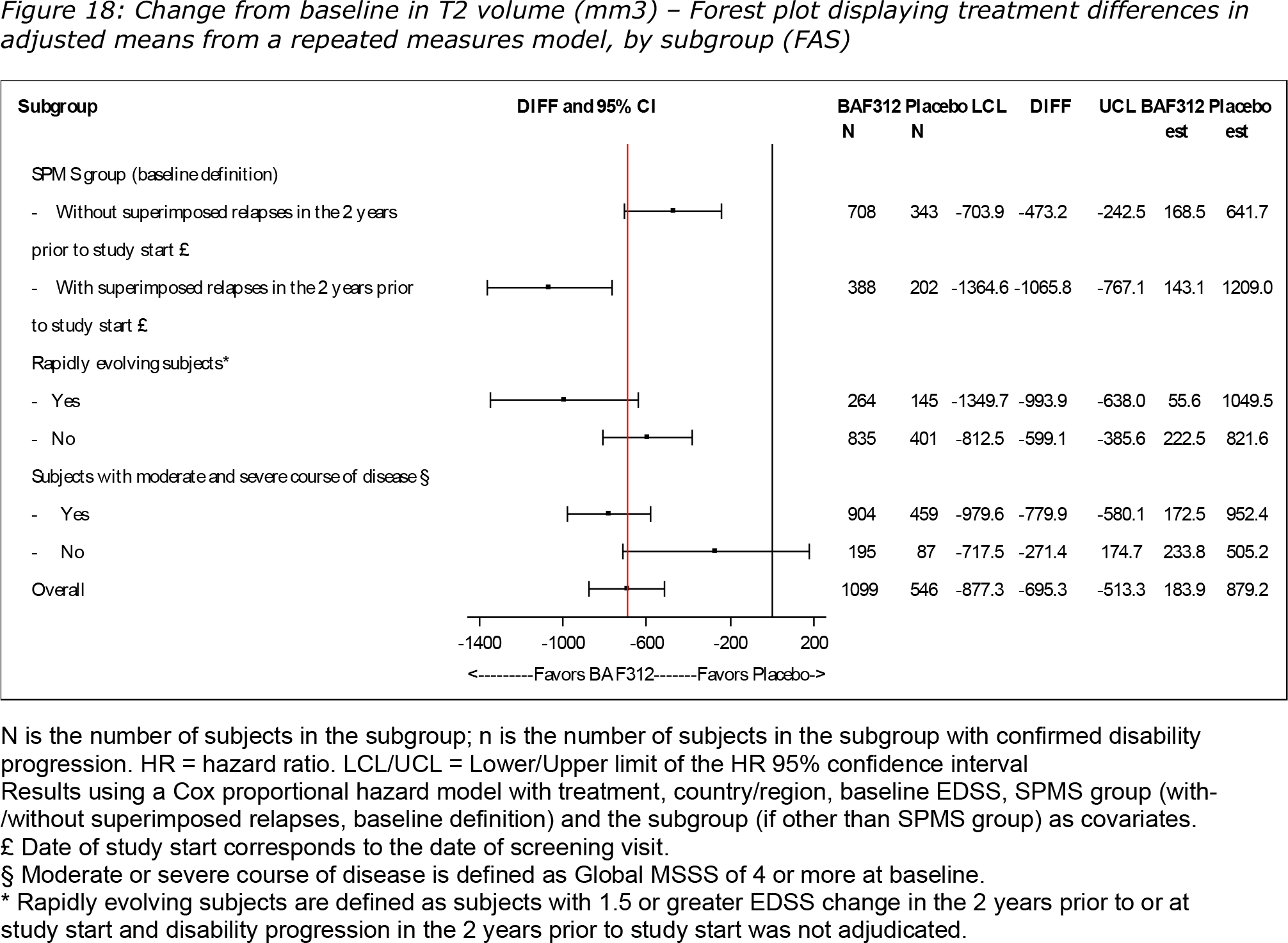
- showed 81% limitation of brain lesion volume growth on T2-weighted MRI images (p<0.0001)
- no statistically significant difference was found with placebo in the Timed 25-Foot Walk (T25FW) test and according to the subjective mobility questionnaire 12-item Multiple Sclerosis Walking Scale (MSWS-12).

Mayzent: Safety of Treating Multiple Sclerosis With Siponimod
Siponimod appears to have a modest and manageable safety profile. Although one might think that a more selective S1P modulator like siponimod (especially one that does not bind S1P3) would mitigate some of the safety concerns with fingolimod, the data does not support this, so a 6-day titration is necessary to reduce the risk of bradyarrhythmia when starting siponimod.
Because S1P3 is also involved with endothelial permeability, one might assume that the risk of macular edema would be reduced with siponimod compared with fingolimod, but the safety data confirm a similar risk of macular edema with siponimod.
Secondary Progressive Multiple Sclerosis: Siponimod Against Wheelchair Dependence
Secondary progressive multiple sclerosis is associated with inexorably evolving walking problems, eventually leading to wheelchair dependence.
Novartis shared the results of additional analysis of data collected at EXPAND showing that prescribing siponimod provided an impressive delay in the time to need for wheelchair use.
In the group of subjects receiving Mayzent, a lower proportion of patients progressed from a baseline EDSS score of 6.5 to a score of 7.0 or higher: 19.2% of patients versus 26.1% in the placebo group. Siponimod reduced the indicated risk by 37.3% (HR 0.63 [95% CI: 0.40–0.97]; p=0.038).

- For the sake of clarity, an EDSS disability score of 6.5 refers to the ability to walk 20 meters without rest but with constant bilateral use of assistive devices like canes, crutches, or walkers, while an EDSS disability score of 7.0 refers to the inability to walk more than five meters even with assistive devices — essentially, the individual is confined to a wheelchair, which he or she can, however, control independently.

In an analytic multistate model, siponimod was shown to result in a 21% reduction in the risk of progression of disability from an initial EDSS score of ≤5 to 5.5–6.0 and a 28% reduction from an EDSS score of 6.5 to sustained ≥7: HR 0.79 [95% CI: 0.63–1.00] and HR 0.72 [95% CI: 0.48–1.06], respectively. However, siponimod did not succeed in reducing the indicated risk for the subgroup of patients whose EDSS score worsened from 5.5–6 to 6.5.

Overall, when the baseline EDSS score was not taken into account, Mayzent therapy reduced the risk of being confined to a wheelchair by 31% (HR 0.69 [95% CI: 0.47–1.01]; p=0.0585).

Under a modeling assumption that the beneficial effect of siponimod would persist, Mayzent was able to extend the time to the need for constant wheelchair use by a median of 4.3 years, meaning that during this time, the drug fixed the EDSS score below 7: the median life expectancy with independent mobility was 16.3 years — versus 12.0 years in the control group.

Mayzent: Long-term Efficacy of Treatment of Multiple Sclerosis With Siponimod
Novartis has disclosed the results of the long-term treatment of secondary progressive multiple sclerosis with siponimod prescribed for up to 5 consecutive years. For this purpose, they analyzed data of patients from the pivotal clinical trial EXPAND, who agreed to continue monitoring them (open study period). At the same time, the group previously receiving placebo for a maximum of 3 years was switched to siponimod prescription.

Among those subjects with secondary progressive multiple sclerosis in the active form who were initially treated with Mayzent, the risk of facing a 6-month CDP event was found to be reduced by 29%, and the time to onset of a 6-month CDP event was extended by 70% when compared with the placebo group that switched to siponimod later.
Among patients with inactive secondary progressive multiple sclerosis, these relative rates were worse: 12.5% and 30%, respectively.

In terms of the annualized relapse rate (ARR) for secondary progressive multiple sclerosis, the group of patients who were continuously adherent to siponimod therapy recorded a 0.07 — versus 0.11 ARR among those who switched to siponimod later (difference was 39.7%; p=0.0023).

Cognitive impairment affects 50–70% of patients with multiple sclerosis, and it is more severe in its progressive, rather than relapsing, form. Cognitive processing speed (CPS) is most often affected. The Symbol Digit Modalities Test (SDMT) is used to check the degree of the impairment. Meaningful worsening of CPS is defined as ≥4-point decrease in the SDMT score.
According to data collected in the open-label period of the EXPAND clinical trial, in active secondary progressive multiple sclerosis, siponimod therapy reduced the risk of 6-month confirmed cognitive worsening (6mCCW) by 33% and delayed the time to 6mCCW event by 70% when compared to the placebo group that switched to Mayzent later.
In the case of inactive secondary progressive multiple sclerosis, these outcomes were not as dramatic: 12.3% and 24%, respectively.

Again, data from the randomized EXPAND period, treatment with siponimod for active secondary progressive multiple sclerosis had a statistically significant effect in terms of sustained worsening or improvement in CPS and, in contrast, did not do so in inactive secondary progressive multiple sclerosis.

Mayzent for Multiple Sclerosis: Inadequate Pricing of Siponimod
Experts from the Institute for Clinical and Economic Review (ICER), to the verdicts of which the pharmaceutical industry players listen with all their attention, conducted a thorough assessment of the adequacy of pricing Mayzent, for a year course of which the Swiss pharmaceutical giant is asking for more than 90 thousand dollars from American patients without insurance coverage.
According to ICER, although the extent to which siponimod restrains the progression of multiple sclerosis regardless of the drug’s effect on recurrent disease activity remains uncertain, the evidence suggests with appropriate conviction that siponimod confers a very slight advantage on patients with active secondary progressive multiple sclerosis over those patients who receive the best symptomatic treatment. And so the current cost of siponimod treatment is greatly overestimated.
ICER believes that the fair cost of a year’s course of Mayzent, calculated using the quality-adjusted life years (QALY) methodology, should fall within the range of $22,000 to $32,000. If the regulator were to approve siponimod also for patients with inactive secondary progressive multiple sclerosis, the fair price would be even lower: between $8,000 and $12,000 — because Mayzent is generally useless for this patient population.
The evidence and clinical efficacy of siponimod does not allow it to be positioned as a drug providing any unique therapeutic benefit for multiple sclerosis, and this is true for any of its phenotypes, including active secondary progressive multiple sclerosis. Siponimod should be categorized as a well-established group of highly effective DMTs against relapsing-remitting forms of multiple sclerosis, which includes such drugs as Gilenya (fingolimod), Lemtrada (alemtuzumab), Tysabri (natalizumab), and Ocrevus (ocrelizumab).
Given the apparent similarity of siponimod to fingolimod, it makes sense for insurance providers to prioritize the latter because of the availability of inexpensive generic copies.
Among the problematic and unresolved questions for Mayzent:
- Diagnosis. It is difficult to draw an exact clinical line between RRMS and SPMS for the reason that disability may worsen with the former and relapses may occur with the latter. It is possible that some patients included in clinical trials of siponimod had a diagnosis of RRMS instead of SPMS.
- Progression without association with relapse activity. It is unclear exactly whether siponimod delays the progression of disability by preventing recurrence. There is also insufficient evidence in favor of siponimod for patients with inactive SPMS.
- Patient-reported outcomes and patient-centered outcomes. Clinical trials of siponimod have not analyzed some patient-relevant outcomes: e.g., improvement in multiple sclerosis symptoms, burden of care, mental health, quality of life.
- Long-term effects. There is insufficient evidence regarding the safety and long-term efficacy of siponimod.
- Comparisons with other DMTs. Reliable data are needed to determine the status of siponimod relative to other DMTs.
The official position of Novartis, reflecting the view of the ICER report, boils down to claims about the methodology. They say that the assessment of the cost-effectiveness of Mayzent is based on a comparison with the absence of any pharmacotherapy for multiple sclerosis, while in practice most patients with secondary progressive multiple sclerosis always received DMTs, although without clinical evidence for their effectiveness in this form of the disease.
By the way, not only are ICER’s QALY methodology unhappy with pharmaceutical manufacturers and industry lobbyists, but patient communities complain about it because if any new drugs fall under the price critique of this nonprofit organization, there is a high probability that insurers will not include them in their formularies. The result is an environment that discriminates against the chronically ill, the elderly, and the disabled people.
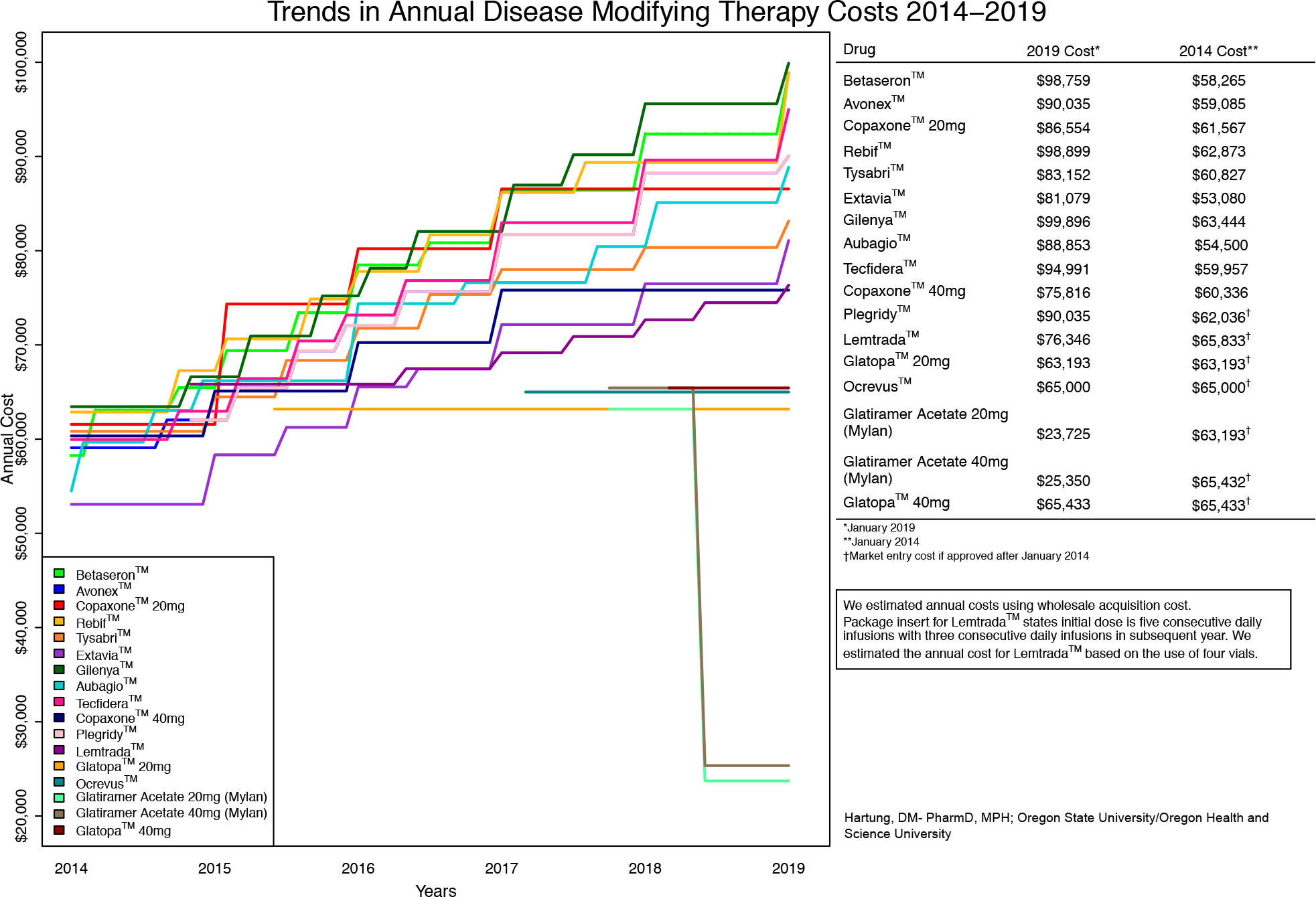
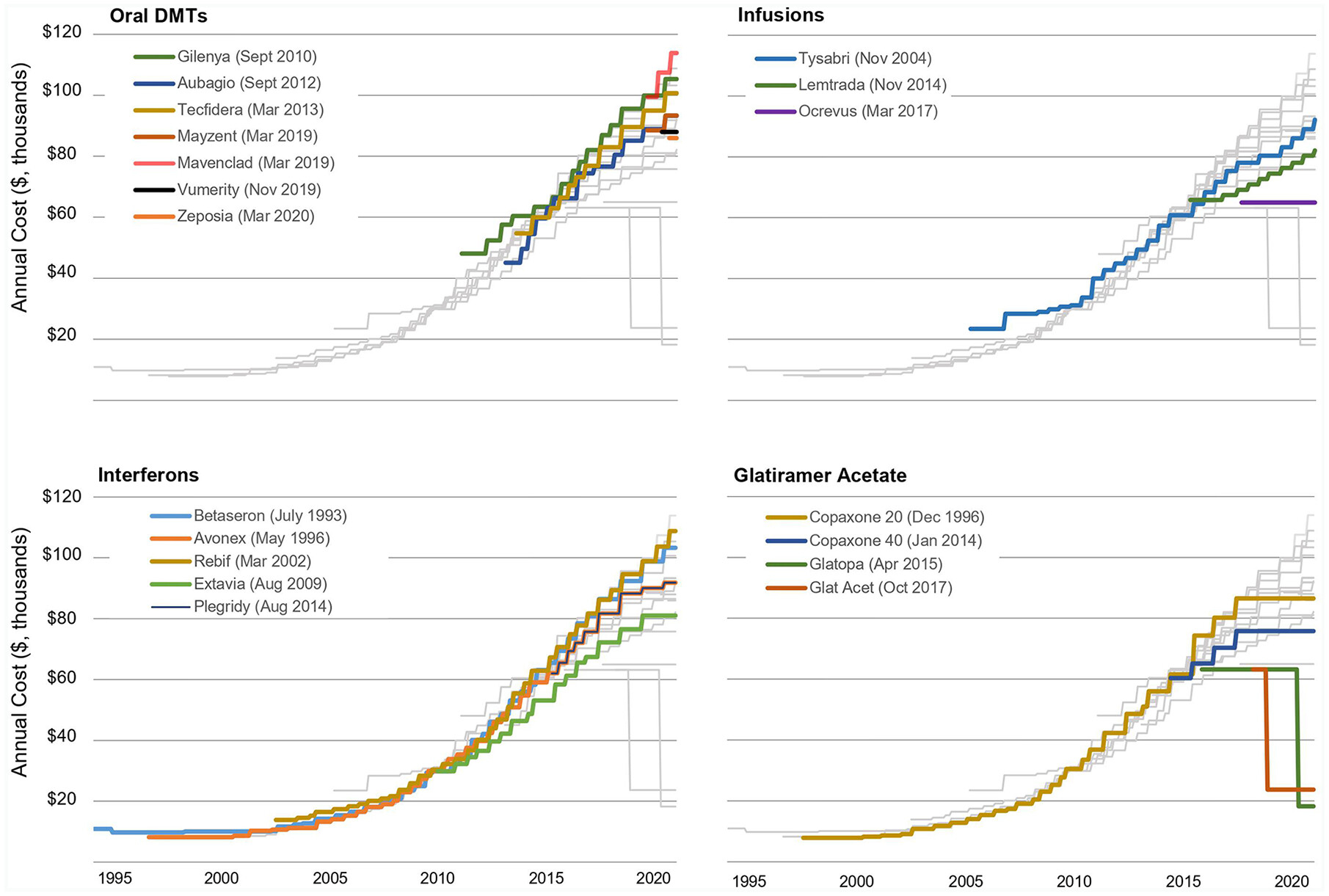
Meanwhile, the cost of multiple sclerosis therapy continues to grow every year: pharmaceutical manufacturers do not stop increasing the prices of older DMTs, even in the face of the emergence of more modern drugs. For example, while in 2004 insured American patients with multiple sclerosis were shelling out an average of $15 a month out of their own pockets, in 2016 the out-of-pocket cost was $309; a 20-fold increase in 12 years.

No one is holding back the cost of multiple sclerosis disease-modifying therapies (DMTs). Oregon Health and Science University. Annual price changes for multiple sclerosis disease-modifying therapies (DMTs). Ther Adv Neurol Disord. 2021 Feb 17;14:1756286420987031.
Mayzent for Treatment of Multiple Sclerosis: Expert Comments
Since 26% of patients in the siponimod group experienced a confirmed disability progression (CDP) after three months, and 32% in the placebo group, the difference of 6%, even though it turned out to be statistically significant, is in fact quite small. Moreover, the drug failed to improve the mobility of the subjects, although this indicator is very important from a clinical point of view.
The effect of Mayzent in inhibiting the loss of healthy brain tissue while preserving brain volume is evident, but it is merely a reflection of the anti-inflammatory properties of this drug. The therapeutic effect of siponimod is most likely due to the fact that in secondary progressive multiple sclerosis the processes of inflammation are more pronounced than in less advanced forms of the disease. This is also confirmed by the fact that in inactive secondary progressive multiple sclerosis siponimod has not demonstrated statistically significant results.
According to industry experts, to be fully confident in the positive effect of Mayzent, it would be nice to conduct another clinical trial. In the meantime, it cannot be stated categorically that this DMT is really effective in secondary progressive multiple sclerosis.
According to the FDA’s Advisory Committee experts, it is very concerning that EXPAND clinical study failed to meet secondary endpoint, time to 3-month confirmed 20% worsening on the T25FW, since the median EDSS of the population was 6.0, a value at which ambulatory dysfunction is the primary determinant of the EDSS.
In addition, there are also concerns about the conduct of the study because attestations that subjects had SPMS were not collected, adjudication of subjects not having clinical documentation of EDSS progression in the prior two years did not consistently occur before randomization, and a “dual database access issue” may have resulted in the unblinding of 101 subjects and affected the outcome of the trial.
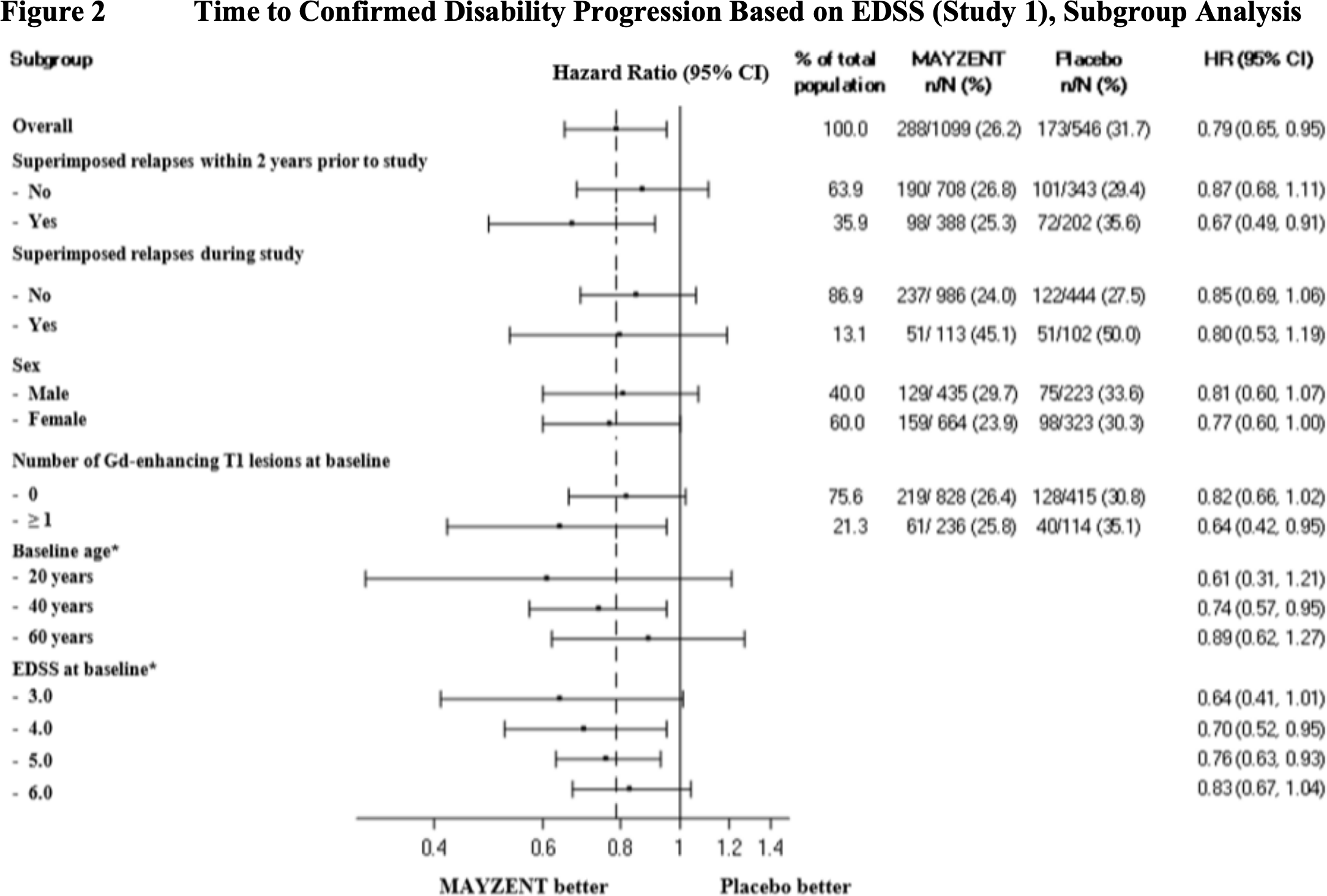
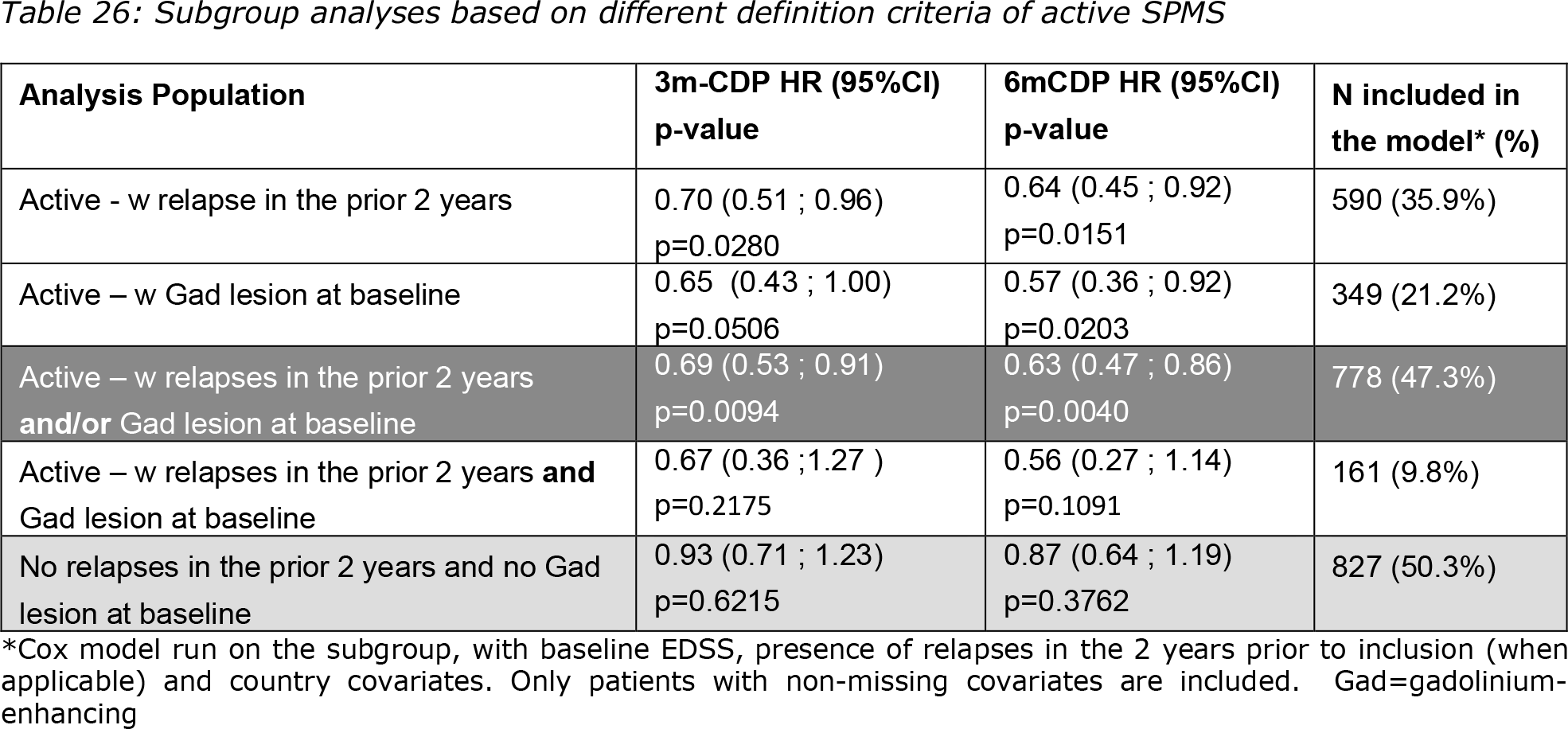
Further analysis suggests that siponimod’s treatment effect on 3-month CDP is driven by the subsets of subjects who experienced relapses in the 2 years prior to randomization, demonstrated gadolinium-enhancing lesions on a baseline MRI, or had an overall disease duration of fewer than 10 years. This suggests that siponimod has a greater treatment effect on the “inflammatory” aspects of the disease, i.e., relapses and MRI activity in subjects with relapsing forms of multiple sclerosis, than it does on the “progressive” aspect of the disease, for which the pathophysiology is poorly defined and raises the question of whether there is sufficient evidence to support the approval of siponimod with an indication for relapsing forms of multiple sclerosis.
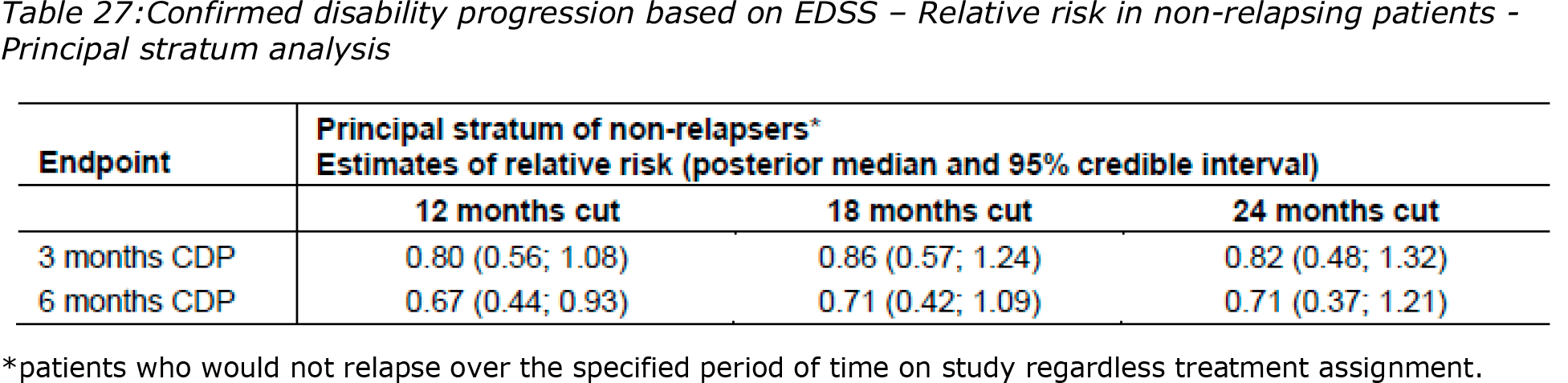
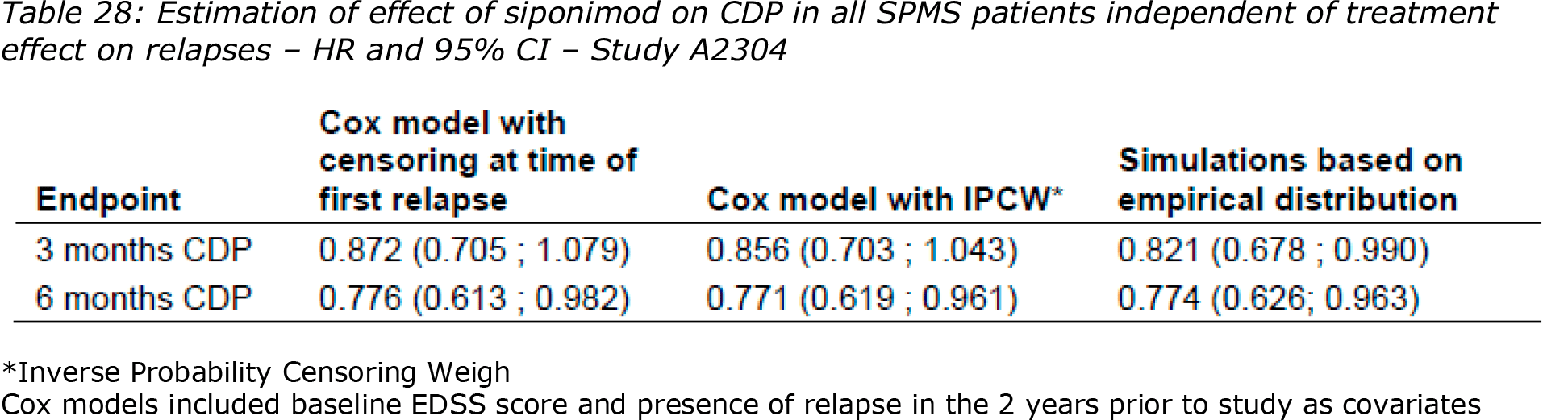
According to EMA’s Committee for Medicinal Products for Human Use (CHMP) experts, although Novartis provided several pre-planned and post hoc analyses, the efficacy of siponimod independent of relapses could not be convincingly shown. In fact, the effect of siponimod on disability progression appeared small in patients without relapses and without focal MRI activity. And that’s why the CHMP is of the opinion that efficacy of siponimod has been demonstrated in patients with SPMS with active disease evidenced by relapses or imaging feature of inflammatory activity.
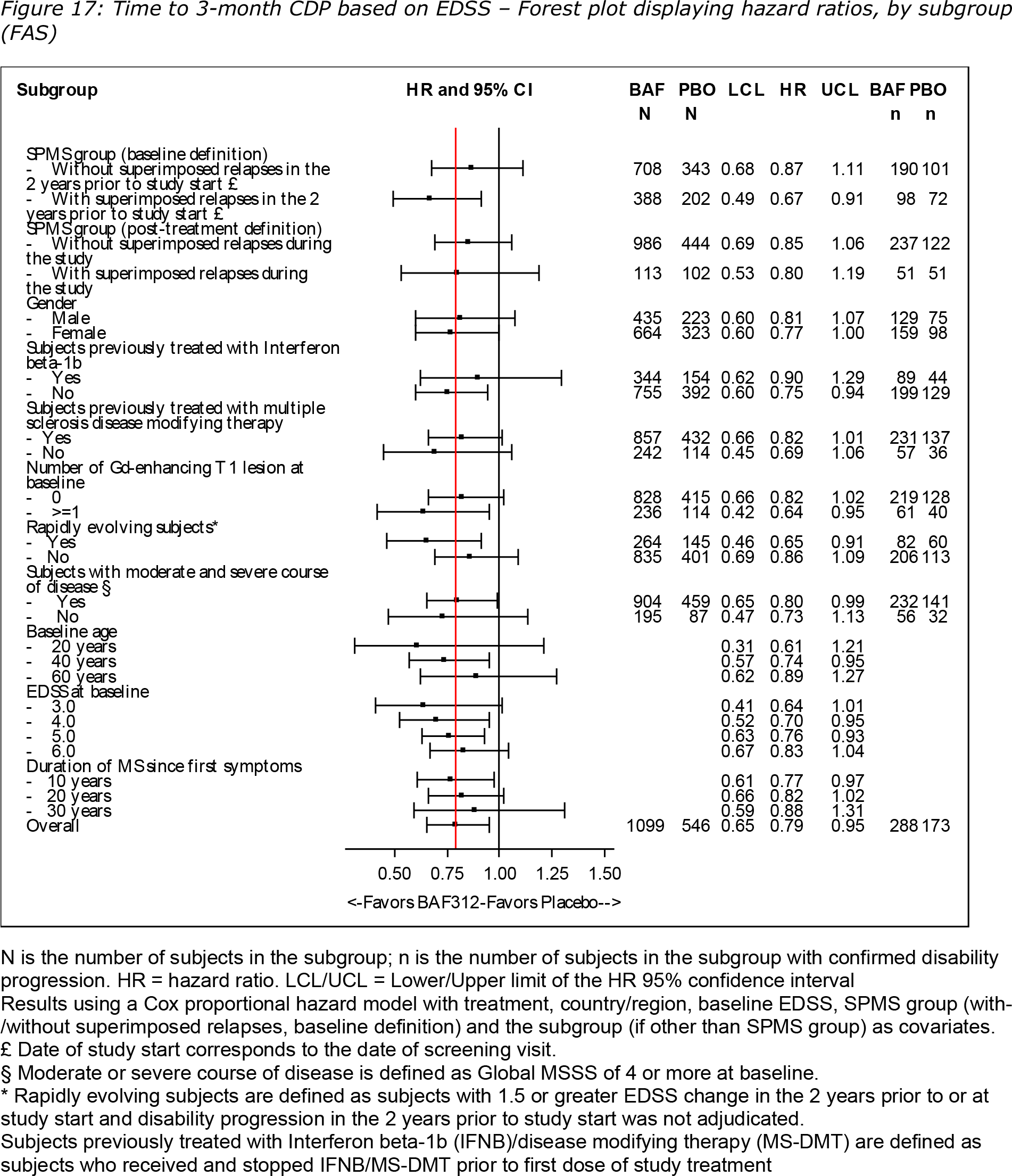
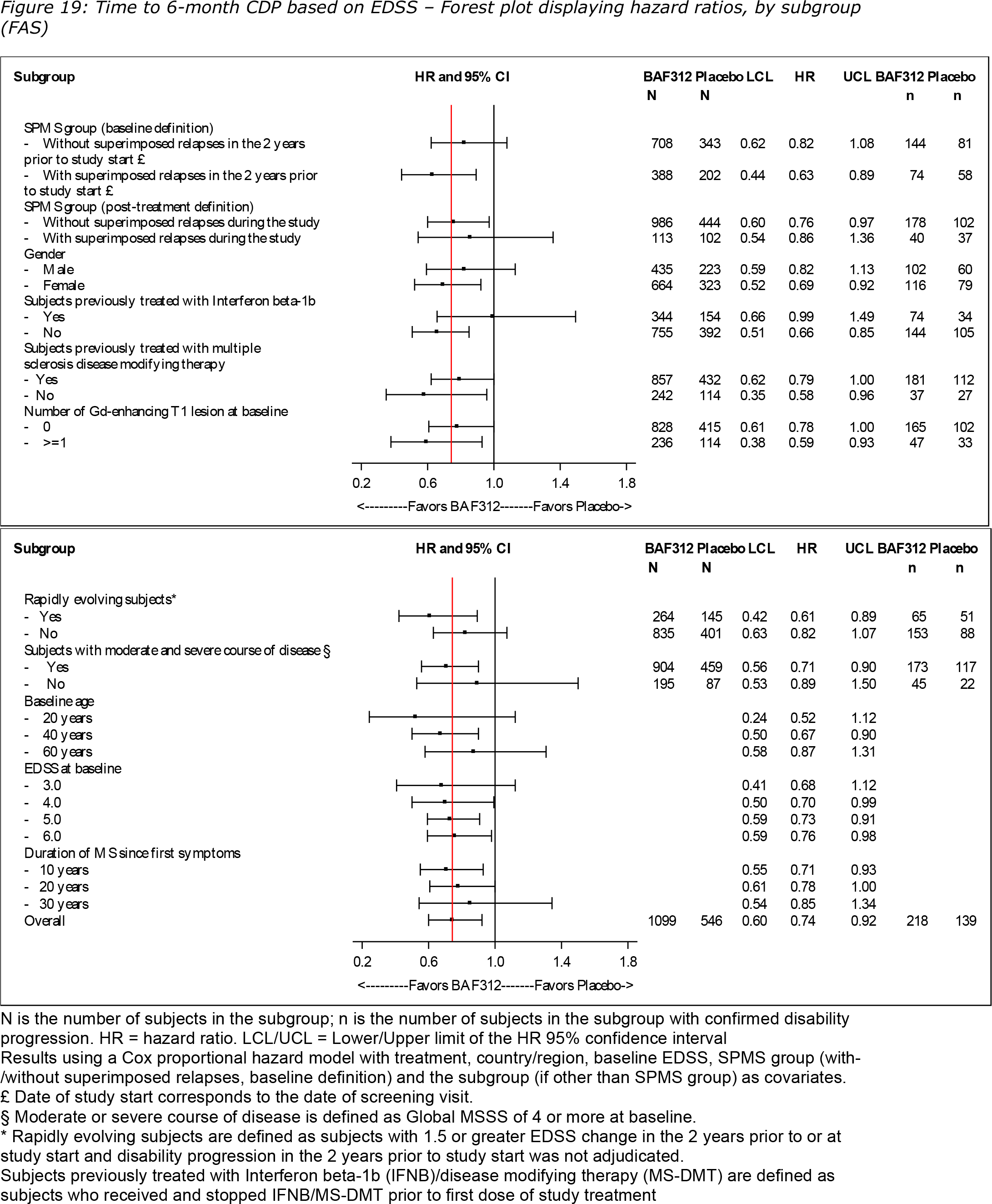
According to experts of Advisory Committee on Medicines (ACM) of Australian Therapeutic Goods Administration (TGA), the EXPAND clinical trial’s primary efficacy outcomes were supported by sensitivity analyses and were consistent in key subgroups. Relapses were reported less commonly in siponimod patients compared with placebo and, clinical outcomes were comparable in SPMS patients with or without superimposed relapses. The benefit in 3-month CDP was higher in relapsing patients (HR 0.85) than in non-relapsing patients (HR 0.87). The benefit in 6-month CDP was also higher in relapsing patients (HR 0.76) than in non-relapsing patients (HR 0.82).
These positive outcomes were supported by a treatment benefit in favor of siponimod compared with placebo for MRI secondary and exploratory endpoints and for cognitive function. There was only a 6.2% benefit in favor of siponimod compared with placebo for the T25W test. However, this negative outcome does not necessarily invalidate the overall positive efficacy outcome of siponimod over placebo, in SPMS management over 48 months.
Extras
Mayzent (siponimod). Prescribing information. U.S. [PDF]
Mayzent (siponimod). FDA CDER. Clinical review. [PDF]
Mayzent (siponimod). Prescribing information. Europe. [PDF]
Mayzent (siponimod). EMA. European Public Assessment Report (EPAR). [PDF]
Mayzent (siponimod). Prescribing information. Australia. [PDF]
Mayzent (siponimod). TGA. Australian Public Assessment Report (AusPAR). [PDF]
Kiendra (siponimod). Prescribing information. Russia. [PDF]
Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study. Lancet. 2018 Mar 31;391(10127):1263-1273. [source]
Siponimod for the treatment of secondary progressive multiple sclerosis: effectiveness and value. ICER. Final evidence report. June 20, 2019. [PDF]
Looming challenges for ICER in assessing the value of rare disease therapies. [PDF]
Dual mode of action of siponimod in secondary progressive multiple sclerosis: a hypothesis based on the relevance of pharmacological properties. ACTRIMS-ECTRIMS Meeting, MSVirtual 2020, September 11‒13, 2020. [PDF]
Sustained reduction of disability and cognitive decline with long-term siponimod treatment in patients with active SPMS: EXPAND data up to 5 years. [PDF]
Impact of siponimod on myelination as assessed by MTR across SPMS subgroups: post hoc analysis from the EXPAND MRI substudy. [PDF]
Effect of siponimod on cognitive processing speed in SPMS patients with active and non-active disease. [PDF]
Safety and tolerability of conversion to siponimod in patients with relapsing multiple sclerosis: interim results of the EXCHANGE study. [PDF]
A first look at the characteristics of patients with multiple sclerosis initiating siponimod therapy in the United States. [PDF]
Baseline characteristics of AMASIA: first real world data of siponimod treated patients with secondary progressive multiple sclerosis. [PDF]