Challenge of Treating Acne Vulgaris
Acne vulgaris is the most common chronic skin disorder of adolescents and young adults and is characterized by noninflammatory lesions (open and/or closed comedones —blackheads and whiteheads) and inflammatory lesions (papules, pustules, nodules, or cysts) usually located on the face, neck, back, chest, and shoulders.
Acne is the eighth most common disease in the world, affecting more than 640 million people worldwide. The manifestation of acne often occurs against the background of pubertal hormonal changes; the pathology affects approximately 85% of adolescents and young adults between the ages of 12 and 25. Acne may persist or even develop into adulthood, especially among women.
Comedones appear due to blockage of hair follicles, the main causes of which are: excessive sebum secretion due to androgen overproduction, increased deposition of keratin, colonization of follicles by the Cutibacterium acnes (formerly called Propionibacterium acnes), local release of pro-inflammatory factors.
Acne may be a manifestation of certain endocrinological diseases: usually polycystic ovarian syndrome and, less frequently, late-onset congenital adrenal hyperplasia or Cushing syndrome.
The pharmacological armamentarium to combat acne includes both topical and systemic products and is very broad. Drugs can be divided into four groups depending on which pathophysiological factor of acne they target:
- follicular hyperproliferation and abnormal desquamation
- topical isotretinoin
- oral retinoids
- azelaic acid
- salicylic acid
- hormonal therapy.
- increased sebum production
- oral isotretinoin
- hormonal therapy.
- C. acnes proliferation
- benzoyl peroxide
- topical and oral antibiotics
- azelaic acid.
- inflammation
- oral isotretinoin
- oral tetracyclines
- topical retinoids
- azelaic acid
- topical dapsone.
Despite the wide range of medications for acne vulgaris, which are often used in various combinations (particularly if mixed inflammatory and noninflammatory lesions), patients and physicians are still in need of new pharmacological methods to treat this disease.
One of the challenges of treatment is suboptimal adherence to acne medications include early discontinuation due to unwanted side effects, lack of understanding of treatment, and overall dissatisfaction with it. So, treatment can be associated with skin irritation, dryness, burning, pruritus, redness, or allergic contact dermatitis. Relatively slow onset of action for many acne therapies also makes these treatments innately discouraging for patients. Specifically, there is often a latency period of at least 6 to 8 weeks until the appearance of a definite clinical improvement which often progresses slowly.
It should be understood that the algorithm for treating acne, being quite complex and cumbersome, involves an abundance of conditions and assessments of patient characteristics and the specific course of the disease. In any case, the consensus view is that acne vulgaris is a chronic condition that typically requires continued treatment to maintain improvement.
In the course of acne management, other methods of treatment are also being used: physical modalities (e.g., chemical peels, intralesional corticosteroids, laser therapy, photodynamic therapy), complementary/alternative therapies (e.g., tea tree oil, herbal supplements, biofeedback, acupuncture), dietary management (e.g., low-glycemic index diets, low-calcium diets). You should know that some of them have never been proven. For example, photodynamic therapy with photosensitizer 5-aminolevulinic acid (ALA) plus pulsed dye laser appears to provide only transient improvement in inflammatory acne lesions. Acupuncture has limited and inconsistent evidence for its effect on acne. Acne is not associated with poor hygiene and improper cleansing: frequency of face washing does not appear to improve or worsen acne severity, and there is limited evidence to support or refute face washing for acne treatment. Dietary restriction is not shown to be beneficial in acne treatment but a small trial suggests a low-glycemic-load diet may improve acne.
Aklief: Trifarotene Is First Fourth-Generation Retinoid in 20 Years
Swiss Galderma offered Aklief (trifarotene), a new medicine in the form of a cream for the topical treatment of acne vulgaris in patients 9 years and older. Aklief can be used to treat both facial (forehead, cheeks, nose, and chin) and truncal (chest, shoulders, and back) acne.
Aklief was approved by the U.S. Food and Drug Administration (FDA) in October 2019.
In Canada, Aklief was approved in November 2019 but for use by individuals 12 years of age and older.

What Are Retinoids?
Topical retinoids are used in the treatment of both comedonal (noninflammatory) acne and inflammatory acne and are used in the primary treatment of most patients due to their comedolytic, anti-inflammatory and depigmenting properties.
Retinoids, being derivatives (vitamers) of vitamin A, work by binding to two families of nuclear receptors in keratinocytes: retinoic acid receptor (RAR) and retinoid X receptor (RXR). The retinoid-receptor complex is transported to the nuclei where it activates specific regulatory DNA sequences called retinoic acid response elements (RAREs) which stimulate the transcription of target genes. The effect is to normalize follicular keratinization and decrease the cohesive capacity of keratinocytes resulting in less follicular occlusion and formation of microcomedones. In addition to its direct effect on comedogenesis, the retinoid-receptor complex suppresses inflammation through competition for coactivator proteins of the transcription factor AP-1 and suppression of toll-like receptor 2 (TLR2) expression.

Although more than 2,000 retinoid compounds have been developed, only a limited number have found use in clinical practice. Thus, the first generation was formed by nonaromatic retinoids such as retinol, retinal, tretinoin, isotretinoin, and alitretinoin; the second generation was represented by mono-aromatic etretinate and acitretin; the third generation gave rise to the poly-aromatic retinoids bexarotene, tazarotene, and adapalene.

What Is Distinguishing Features of Trifarotene?
Topical trifarotene belongs to the fourth generation of retinoids — heterocyclic compounds. Trifarotene was the first new retinoid approved against acne in more than 20 years. The molecule, being an RAR agonist, is 20 times more selective to its gamma receptor (RAR-γ) than to its alpha receptor (RAR-α) or beta receptor (RAR-β); trifarotene is also inactive towards RXR. Due to this selectivity, trifarotene significantly eliminates the problem of skin irritation often encountered when targeting RAR-β with retinoids. Trifarotene is active and stable in keratinocytes, and since it is metabolized by hepatic microsomes in an accelerated manner, its safety and tolerability profile is quite decent and bypasses the so-called retinoid dermatitis.
Aklief: Efficacy and Safety of Trifarotene Treatment for Acne Vulgaris
Regulatory approval of Aklief came from the results of two phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) pivotal clinical trials PERFECT 1 (NCT02566369) and PERFECT 2 (NCT02556788) covering patients (n=2420) with moderate acne vulgaris.
The eligibility criteria were patient age 9 years and older, moderate facial acne (IGA score of 3, ≥20 inflammatory lesions and ≥25 noninflammatory lesions in the face), moderate truncal acne (PGA score of 3, ≥20 inflammatory lesions and ≥20 to <100 noninflammatory lesions on the areas of the trunk reachable for self-application).
All participants had inflammatory and noninflammatory acne on the face (forehead, cheeks, nose, chin), while 99% of patients also had it on the trunk (chest, shoulders, back).
Aklief cream applied daily for 12 weeks resulted in a statistically significant (p<0.001) improvement of the symptoms and signs of acne compared to placebo according to the Investigator’s Global Assessment (IGA) and the Physician’s Global Assessment (PGA) scales as well as according to the absolute and relative changes in the number of inflammatory and noninflammatory acne lesions. The disappearance of the lesions began to occur after two and four weeks of treatment on the face and trunk, respectively (p<0.05).
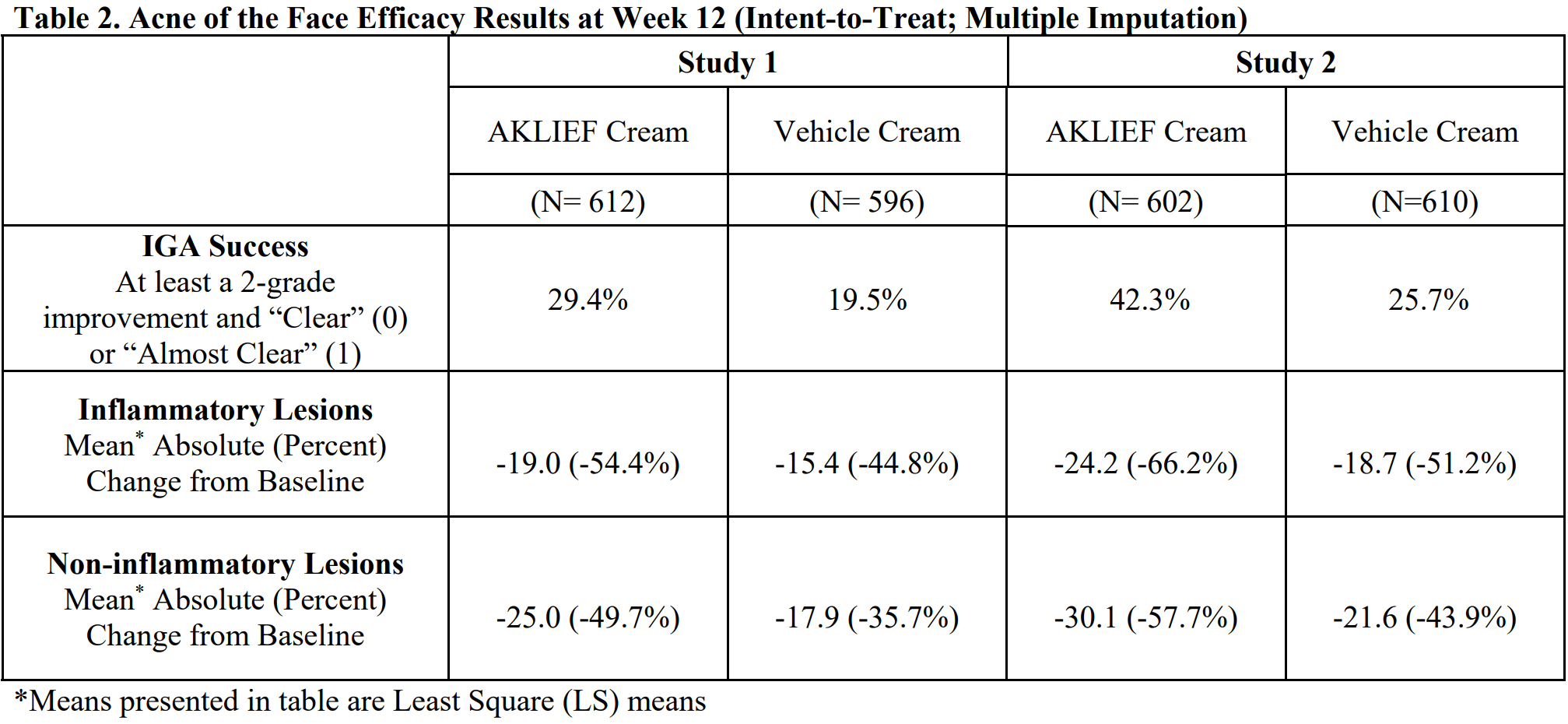
Thus, in the trifarotene groups, 29.4% and 42.3% of patients in PERFECT 1 and PERFECT 2, respectively — versus 19.5% and 25.7% of participants in the placebo groups — reached the primary endpoint defined by getting rid of facial acne according to IGA score 1 (almost clear skin) or 0 (clear skin) and its improvement by at least 2 points.
Those receiving trifarotene showed an absolute decrease in the number of inflammatory lesions by an average of 19.0 and 24.2 — versus 15.4 and 18.7 in the control groups. The number of noninflammatory lesion counts reduced by an average of 25.0 and 30.1 — versus 17.9 and 21.6.

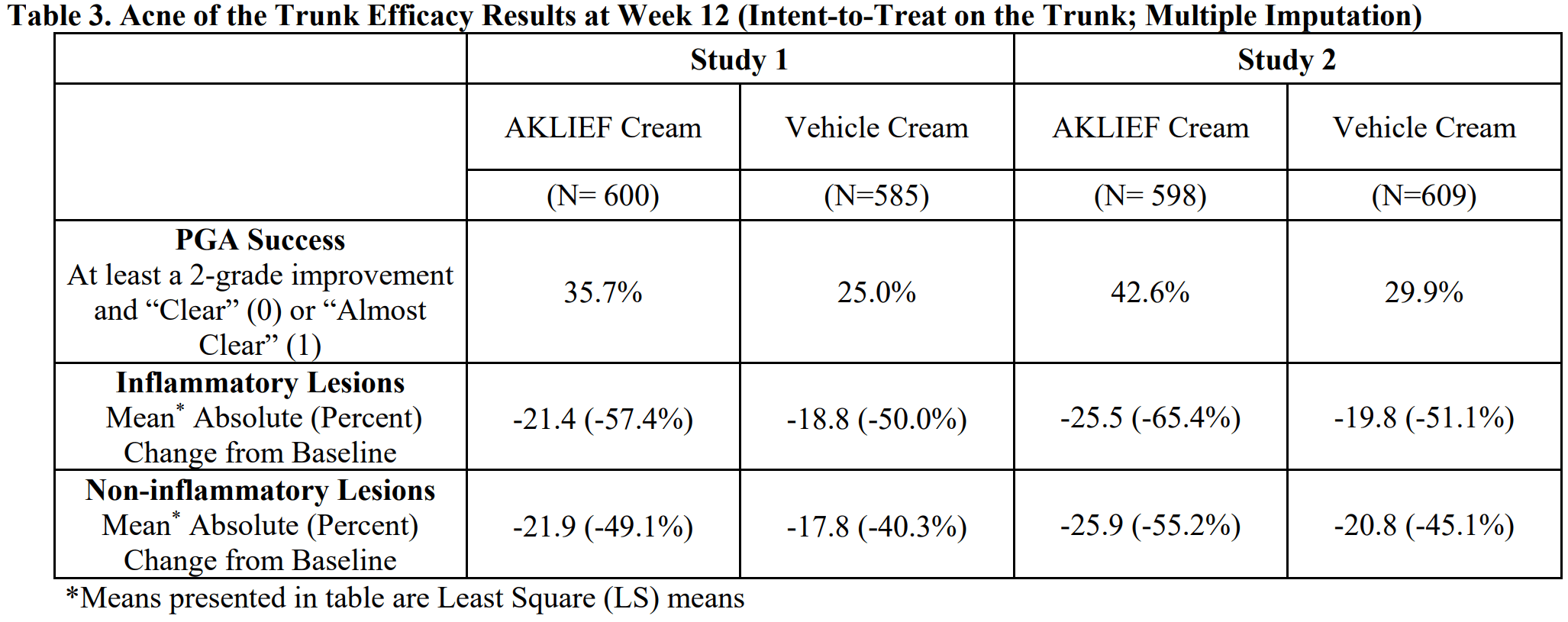
The rates of success with trifarotene according to the truncal PGA (identical to IGA) were 35.7% in PERFECT 1 and 42.6% in PERFECT 2 — versus 25.0% and 29.9%, respectively for placebo.

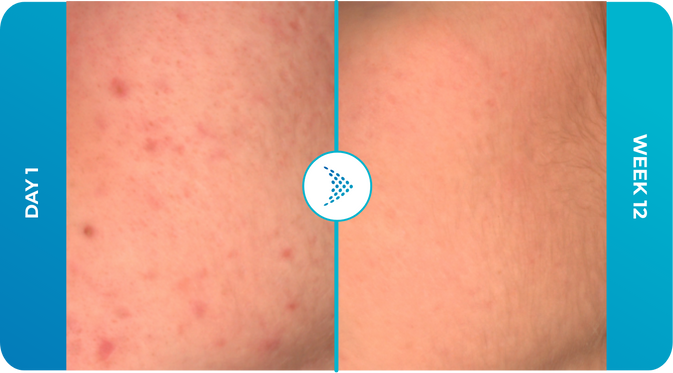
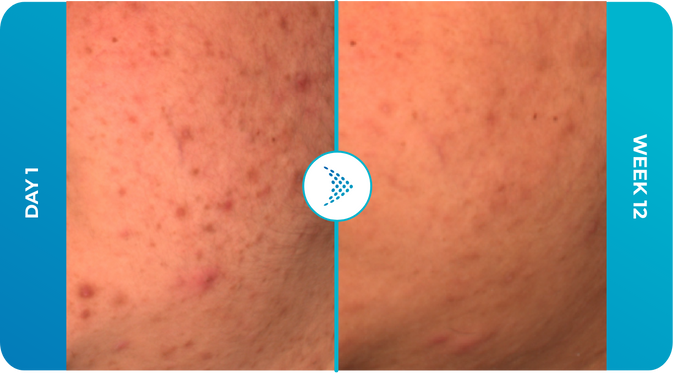
The official Aklief’s website features before and after photos of patients treated for acne vulgaris with this drug. Of course, these photos should not be taken as definitive proof of the efficacy of trifarotene, they are offered for illustrative purposes only.
[twenty20 img1=”641″ img2=”642″ offset=”0.5″][twenty20 img1=”643″ img2=”644″ offset=”0.5″]
[twenty20 img1=”645″ img2=”646″ offset=”0.5″]
Among the most common adverse effects of Aklief treatment were skin irritation (in 7.5% of patients), sunburn (2.6%), and itching (2.4%). Local irritation related to trifarotene cream was transient and consistent with the known pattern of topical retinoid dermatitis; tolerability was better on the trunk than on the face.
The concomitant use of non-acne-inducing and hypoallergenic moisturizers to alleviate skin irritation was recommended, but not in the periods one hour before and one hour after Aklief cream application.
Aklief: Real-World Experience With Trifarotene for Treatment of Acne Vulgaris
If you examine the reviews of people who have used Aklief to treat acne vulgaris and reported their experiences on the Reddit discussion platform, it becomes apparent that the drug helps some people, while others do not. And this is obvious because every acne case is unique. Again, it should be well understood that the beneficial healing effect of Aklief usually manifests itself after many months of continuous use.
For example, one 30-year-old woman who has carried the burden of acne for over 10 years testified to complete skin cleansing after 5 months of using Aklief.

Another woman noted marked improvements in her acne after 2.5 months of applying Aklief.

Another young lady was pleased with how the skin texture on her chin changed for the better after 3 weeks of Aklief acne treatment.

After 9 months of using Aklief (usually every other day), the acne was almost gone, the obvious changes to improvement began to appear after a couple or three months.
[twenty20 img1=”2567″ img2=”2568″ offset=”0.5″] [twenty20 img1=”2569″ img2=”2570″ offset=”0.5″]Aklief was very successful in getting rid of acne in two to three months.




The 6-month use of Aklief has paid off.


Negative experiences with Aklief were also reported: one girl’s skin condition worsened after 1 month of using the cream.

One guy’s 1.5 months of acne treatment with Aklief resulted in significant skin worsening.


And this is what happened after 10 weeks of unsuccessful use of Aklief.
[twenty20 img1=”2582″ img2=”2583″ offset=”0.5″]
Extras
Aklief (trifarotene). Prescribing information. U.S. [PDF]
Aklief (trifarotene). FDA CDER. Multi-disciplinary review and evaluation. [PDF]
Topical trifarotene: a new retinoid. Br J Dermatol. 2018 Aug;179(2):231-232. [source]
Randomized phase 3 evaluation of trifarotene 50 μg/g cream treatment of moderate facial and truncal acne. J Am Acad Dermatol. 2019 Jun;80(6):1691-1699. [source]
Long-term safety and efficacy of trifarotene 50 μg/g cream, a first-in-class RAR-γ selective topical retinoid, in patients with moderate facial and truncal acne. J Eur Acad Dermatol Venereol. 2020 Jan;34(1):166-173. [source]
Amzeeq: World’s First Topical Formulation of Antibiotic Minocycline
Israel’s Foamix Pharmaceuticals has developed Amzeeq (minocycline), a new drug indicated to treat inflammatory lesions of nonnodular moderate to severe acne vulgaris in patients 9 years of age and older.
Amzeeq was approved by the FDA in October 2019.
Amzeeq (FMX-101) is a 4% minocycline in foam form applied topically. Minocycline is a semi-synthetic, second-generation tetracycline with broad-spectrum bacteriostatic and anti-inflammatory activity, and is one of the most commonly prescribed oral antibiotics for acne vulgaris. Unlike tetracycline itself, bacteriostatic effect minocycline realized through reversible inhibition of protein synthesis and microbial replication at the level of 30S subunits of ribosomes, lasts two to four times longer.

Minocycline, with its proven anti-inflammatory activity in acne (because of a specific modulatory effect on epidermal cytokines), shows a very low propensity to develop resistance in C. acnes when compared to erythromycin, clindamycin, tetracycline, or doxycycline.
Prior to Amzeeq, minocycline was only available in oral form and its administration was accompanied by systemic side effects (tinnitus, dizziness, and hyperpigmentation of skin, mucous membranes, and teeth). Foamix is responsible for creating a topical version of minocycline. A serious problem that stood in the way of development was the extreme instability of this molecule (as well as other tetracyclines) which breaks down in the presence of water, alcohol, surfactants, or polymers — traditional components of topical drug formulations. It is also sensitive to light and oxidation.
Foamix has discovered that a suspension of minocycline in a non-aqueous hydrophobic matrix provides the greatest stability for minocycline. Following recent trends in topical drug delivery, Amzeeq uses a foam-based vehicle. The foam formulation of Amzeeq has micronized minocycline hydrochloride crystals suspended and dispersed throughout the product. Particle size plays an important role in effective topical acne treatment because smaller particles can better penetrate the pilosebaceous unit, delivering the active ingredient to the target site without resulting in an increase in the transdermal penetration. In addition to improving the ability of a drug to penetrate into the skin, micronization helps protect the stability of drugs, making them more photostable. Suspension of micronized minocycline in the non-aqueous vehicle limits its interaction with other components of the composition. Micronization of minocycline in Amzeeq also prevents a grainy sensation on the skin, ensures consistency of the product, and facilitates application by preventing clogging of the actuator valve of the pressurized aerosol packaging in canisters.

Amzeeq: Efficacy and Safety of Topical Minocycline Treatment for Acne Vulgaris
The efficacy and safety of Amzeeq were studied in three phase 3 clinical trials NCT02815267, NCT02815280, and NCT03271021 (randomized, double-blind, placebo-controlled, multicenter) involving patients (n=2418) with moderate-to-severe acne vulgaris.
Subjects (age 9 years or older) were to have inflammatory and noninflammatory lesion counts of 20–50 and 25–100, respectively, and an IGA score of 3 (moderate severity) or 4 (severe).
For 12 weeks, participants were topically treated once daily with Amzeeq or placebo, and no other additional topical or systemic medications affecting the course of acne were allowed.
All three clinical trials demonstrated statistically significant superiority of topical minocycline over placebo — according to an IGA score of 0 (clear skin) or 1 (almost clear skin) with an accompanying reduction of at least 2 points — and it worked particularly well in the largest trial NCT03271021 providing therapy success in 30.8% of Amzeeq’s patients versus 19.6% of controls (p<0.0001).

Among the most common adverse events to Amzeeq therapy, if we talk about their mild severity: erythema (14.2% of patients), hyperpigmentation (12.4%) [most often indicating inflammatory and postinflammatory changes due to acne], dry skin (6.8%), itching (5.1%), skin peeling (3.2%).
[twenty20 img1=”663″ img2=”664″ offset=”0.5″][twenty20 img1=”665″ img2=”666″ offset=”0.5″]
Topical Minocycline: Two More Things
In November 2019, Foamix and Menlo Therapeutics announced a merger under the latter brand. The companies seamlessly complemented each other’s expertise: Menlo deals with serlopitant, a highly selective neurokinin 1 receptor (NK1R) antagonist being developed in itch therapy for conditions such as prurigo nodularis and psoriasis as well as for chronic itching of unspecified etiology. However, serlopitant, tested in clinical trials, failed, and therefore its further development was discontinued.
In September 2020, Menlo changed its name to VYNE Therapeutics.
In late May 2020, the FDA approved the topical foam Zilxi (minocycline, 1.5%) for the treatment of inflammatory lesions of rosacea in adults.
FCD105, topical foam of 3% minocycline and 0.3% retinoid adapelene for the treatment of moderate-to-severe acne vulgaris, continues to be developed.
Extras
Amzeeq (minocycline). Prescribing information. U.S. [PDF]
Amzeeq (minocycline). FDA CDER. Multi-disciplinary review and evaluation. [PDF]
Formulation and profile of FMX101 4% minocycline topical foam for the treatment of acne vulgaris. J Clin Aesthet Dermatol. 2020 Apr;13(4):14-21. [source]
A novel topical minocycline foam for the treatment of moderate-to-severe acne vulgaris: results of 2 randomized, double-blind, phase 3 studies. J Am Acad Dermatol. 2019 Jan;80(1):168-177. [source]
Efficacy and safety of a novel topical minocycline foam for the treatment of moderate to severe acne vulgaris: a phase 3 study. J Am Acad Dermatol. 2020 Apr;82(4):832-837. [source]
Open-label extension study evaluating long-term safety and efficacy of FMX101 4% minocycline foam for moderate-to-severe acne vulgaris. J Clin Aesthet Dermatol. 2019 Oct;12(10):16-23. [source]
Winlevi: Clascoterone Is First Acne Drug With Completely New Mechanism of Action in 40 Years
Winlevi (clascoterone) is a new drug indicated for the topical treatment of acne vulgaris in patients 12 years of age and older.
The cream Winlevi, offered by Italia’s Cassiopea, was approved by the FDA in August 2020.
Winlevi is the first acne vulgaris medication in the last four decades to feature a completely new mechanism of action.

Winlevi: Mechanism of Action of Clascoterone for Treatment of Acne Vulgaris
Androgen receptors (ARs) are expressed throughout the skin and are found in the sebaceous glands, sebocytes (secretory cells of the sebaceous gland), and dermal papilla cells. Circulating and locally (skin) synthesized androgens such as testosterone and dihydrotestosterone (DHT) bind to the AR and stimulate sebum production in both males and females.
Androgen inhibition is an effective strategy for the treatment of acne in females; these drugs suppress androgen production, thereby reducing circulating androgens.
Clascoterone (CB-03-01) is a first-in-class topical AR inhibitor. Although the exact mechanism of action of this steroid anti-androgen is unknown, it is believed that the molecule (cortexolone 17α-propionate) competes with androgens, mainly DHT, for binding to AR in the sebaceous glands and hair follicles.
Clascoterone suppresses the local (cutaneous) effects of DHT, manifested as acne, by, it is thought, inhibiting lipid production from sebocytes and reducing pro-inflammatory cytokines — mediators excited by androgens. Unlike oral hormone therapy for acne clascoterone can be used by both women and men.

Clascoterone is rapidly converted to cortexolone, a metabolite with a known and acceptable safety profile. Because of this as well as the apparently exclusively local action of clascoterone, the risk of non-target or systemic side effects is probably minimized.
Winlevi: Efficacy and Safety of Clascoterone Treatment for Acne Vulgaris
Clascoterone has been validated in two design-identical phase 3 clinical trials NCT02608450 and NCT02608476 (randomized, double-blind, placebo-controlled, multicenter, international) involving patients (n=1421) aged 12 years and older with facial acne vulgaris.
Participants’ disease was to be characterized by the presence of inflammatory and noninflammatory acne lesions numbering 30-75 and 30-100, respectively, and an IGA score of 3 (moderate severity) or 4 (severe).
For 12 weeks, subjects were given placebo or clascoterone twice daily.
By the primary endpoint, set by reaching an IGA score of 0 (clear skin) or 1 (almost clear skin), with a simultaneous it’s reduction of at least 2 points, came out 18.8% and 20.9% of patients in the Winlevi groups — versus 8.7% and 6.6% in the placebo groups. The resulting difference of 10.1% (95% CI: 4.1–16.0) and 14.3% (95% CI: 8.9–19.7) was statistically significant (p<0.001).

The number of noninflammatory acne lesions decreased by an absolute 20.4 and 19.5 in the clascoterone groups (by 32.6% and 29.6%), and by 13.0 and 10.8 in the placebo groups (by 21.8% and 15.7%) [p<0.001].
The number of inflammatory acne lesions in the Winlevi groups decreased by an absolute 19.3 and 20.1 (by 44.6% and 47.1%), while in the control groups they decreased by 15.4 and 12.6 (by 36.3% and 29.7%) [p=0.003 and p<0.001].
Administration of clascoterone did not show any significant difference from placebo when it came to local skin reactions, such as edema, erythema/redness, pruritus, scaling/dryness, skin atrophy, stinging/burning, striae rubrea, telangiectasia. If these occurred while prescribing Winlevi it was recommended to discontinue or reduce the frequency of use of the drug.
Clascoterone can lead to suppression of the hypothalamic–pituitary–adrenal (HPA) axis.
An additional long-term safety trial of clascoterone among patients (n=347) who received Winlevi twice daily for up to 9 months found no significant variation in the statistical distribution of adverse reactions, leading to the conclusion that long-term use of the drug is possible.
Clascoterone: What’s Next
Cassiopea, which separated from parent Cosmo Pharmaceuticals in June 2015, continues to conduct clinical trials of clascoterone (in solution form) for the treatment of androgenetic alopecia in men and women. The experimental drug is being marketed under the brand name Breezula.
Androgenetic alopecia, which is the most common cause of hair loss, is caused by dihydrotestosterone (DHT) production. Androgens normally stimulate terminal hair growth in many areas of the body, such as the beard or axilla, but exert the opposite inhibitory effect on the scalp if the hair follicles there are genetically sensitive to DHT. High local concentrations of DHT result in progressive miniaturization of the follicles (thinning of the hair) and shortening of the hair growth cycle, leading to characteristic male pattern baldness.
Extras
Winlevi (clascoterone). Prescribing information. U.S. [PDF]
Winlevi (clascoterone). FDA CDER. Multi-disciplinary review and evaluation. [PDF]
Efficacy and safety of topical clascoterone cream, 1%, for treatment in patients with facial acne: two phase 3 randomized clinical trials. JAMA Dermatol. 2020 Jun; 156(6): 1–10. [source]
Open-label, long-term extension study to evaluate the safety of clascoterone (CB-03-01) cream, 1% twice daily, in patients with acne vulgaris. J Am Acad Dermatol. 2020 Aug;83(2):477-485. [source]
Cassiopea. Annual report of 2020. [PDF]
What Is the Best Acne Treatment?
As mentioned at the beginning of our review, the choice of medications for the treatment of acne vulgaris is not an easy task. Each patient must be approached individually taking into account all the proper factors specific to his or her medical history and the peculiarities of the course of the disease.
And even more so, the efficacy of acne treatment should never be compared based on the results obtained in clinical trials of different drugs. Such cross-trial comparisons are methodologically incorrect due to differences in the mechanisms of action of the drugs, terms of inclusion in the studies, and variations in recruited patient populations.
Nevertheless, for reference purposes, here are the results of the Aklief, Amzeeq, and Winlevi clinical trials summarized in one table.
Aklief, Amzeeq, and Winlevi: treatment efficacy of facial acne vulgaris. Cross-trial comparision
Trial 1 | Trial 2 | Trial 3 |
||||
|---|---|---|---|---|---|---|
| IGA Success | Difference from Vehicle | IGA Success | Difference from Vehicle | IGA Success | Difference from Vehicle | |
| Aklief | 29.4% | 9.9 % | 42.3% | 16.6 % | ||
| Vehicle | 19.5% | 25.7% | ||||
| Amzeeq | 8.1% | 3.3% | 15.8% | 7.4% | 30.8% | 11.2% |
| Vehicle | 4.8% | 8.4% | 19.6% | |||
| Winlevi | 18.8% | 10.1% | 20.9% | 14.3% | ||
| Vehicle | 8.7% | 6.6% | ||||