Highlights
Bristol-Myers Squibb is engaged in large-scale development of the experimental drug deucravacitinib, which is being studied in the treatment of various autoimmune diseases.
- Deucravacitinib pronounced doo-krav-a-sih-ti-nib.
In mid-September 2022, the U.S. Food and Drug Administration (FDA) approved Sotyktu (deucravacitinib) for the treatment of moderate-to-severe plaque psoriasis in adult patients who are candidates for systemic therapy or phototherapy.
Subsequently, Sotyktu will add treatment for other autoimmune diseases, including psoriatic arthritis, ulcerative colitis, Crohn’s disease, systemic lupus erythematosus, discoid lupus erythematosus, and subacute cutaneous lupus erythematosus.
Sotyktu is a powerful drug, and in a convenient oral formulation. The healing power of deucravacitinib — at least in the treatment of psoriasis — has come very close to the effectiveness of biological drugs (monoclonal antibodies), which are difficult to produce, expensive, and not convenient to administer due to their injectable nature.
Importantly, treatment with deucravacitinib is not accompanied by any serious or severe adverse events (AEs). Unlike all other related drugs in the class of inhibitors of Janus kinases (JAKs), the prescribing information for Sotyktu do not include a boxed warning indicating risks of dangerous AEs.
Given both deucravacitinib’s new mechanism of action and its very acceptable safety profile, it has the ability to make billions of dollars for Bristol-Myers Squibb. Well, it will give immeasurably suffering patients an extra chance for healing.
For U.S. patients, the price of Sotyktu is set at $6,146 (excluding discounts and rebates) for a one-month course of treatment. A year’s worth of therapy would cost $74,000. This is one-third more than the cost of treating psoriasis with Otezla (apremilast).
According to industry forecasts, deucravacitinib sales will reach $2.4 billion annually by 2026. Peak demand for deucravacitinib will easily reach $4 billion annually.
- Sotyktu (deucravacitinib). Prescribing information. U.S. [PDF]
- Bristol-Myers Squibb could have given deucravacitinib another brand name, because it has many other trademarks: Cetycvu, Evtyclu, Euklartyk, Tycruva, Tycneek/Tykneek/Tyqneek, Ticybly, Tykdeuvy/Tyqdeuvy, Tykperlo, Tyqamply, Tyqzenic, Xtyklir.

Treating Psoriasis: Pharmacological Innuendo
Despite the remarkable achievements of the pharmaceutical industry in the treatment of psoriasis (and indeed any other autoimmune disease), there is still a high unmet medical need for new, safe, and effective drugs, especially oral drugs.
Biological drugs have brought psoriasis therapy to a new level of effectiveness: it is often possible to achieve complete (or almost) clearance of the skin. Mechanistically we are talking about blocking tumor necrosis factor (TNF); interleukin 12 (IL-12) and simultaneously interleukin 23 (IL-23); either interleukin 17A (IL-17A), or its receptor (IL-17RA), or IL-17A and interleukin 17F (IL-17F); only IL-23. Nevertheless, there are a number of claims to such medications: parenteral route of administration (intravenous or subcutaneous), risk of immunogenicity, a number of adverse events, loss of efficacy during treatment.
The field of oral psoriatic drugs is developing but not everything is smooth with them either. For example, the standard methotrexate, cyclosporine, and acitretin are characterized by adverse events, drug-drug interactions, and long-term toxicity. The seemingly good apremilast does not help much.
JAK–STAT Signaling Pathway: Key to Treating Autoimmune Diseases
The JAK–STAT pathway, which provides intracellular cytokine signaling, is important for both normal and pathological conditions when it comes to immune-mediated inflammatory diseases. Thus, in the case of psoriasis, for which the IL-23/IL-17 axis is currently considered the most important pathogenic pathway, blocking JAK–STAT with small-molecule inhibitors is clinically effective. And there is evidence of this: a number of commercialized JAK inhibitors do well in treating psoriasis. However, the relative non-specificity and low therapeutic index (they are unsafe) have slowed JAK inhibitors integration into the pharmacotherapy armamentarium of psoriasis.
Suppression of the JAK–STAT pathway leads to inhibition of the production of cytokines that are pathogenetically involved in the development and progression of psoriasis. Numerous attempts to inhibit (selectively and not) one or more members of the Janus kinase family have proven that the approach works. But the accompanying side effects have turned out to be quite unpleasant.
Blocking JAK–STAT is too serious and powerful a process, since it affects a number of other related signaling pathways and inhibits the production of too many different cytokines. On the one hand, the inflammatory process is stopped; on the other hand, dysregulation of the immune, cardiovascular, and nervous systems occurs manifesting, for example, in worsened cardiac function in patients with congestive heart failure, impaired lipid profile, or increased risk of thrombosis and infectious diseases.
Again, JAK selectivity is not an easy task. Due to the high homology of the ATP active site throughout the kinome (and it contains over 500 kinases!) and especially in the JAK family, it is very difficult to implement highly selective targeting of a particular JAK member while maintaining selectivity within the kinome. As a result, the JAK inhibitors on the market were either not selective at all or with very moderate selectivity. That would be all right, but too narrow a therapeutic window (due to the inability to increase the dose because of adverse events) does not allow for serious improvement of treatment outcomes without a dramatic increase in side effects.
The pharmaceutical industry is looking for options to suppress the JAK–STAT pathway that differ from current approaches to targeting Janus kinases. And Bristol-Myers Squibb seems to have succeeded.
Sotyktu: Mechanism of Action of Deucravacitinib
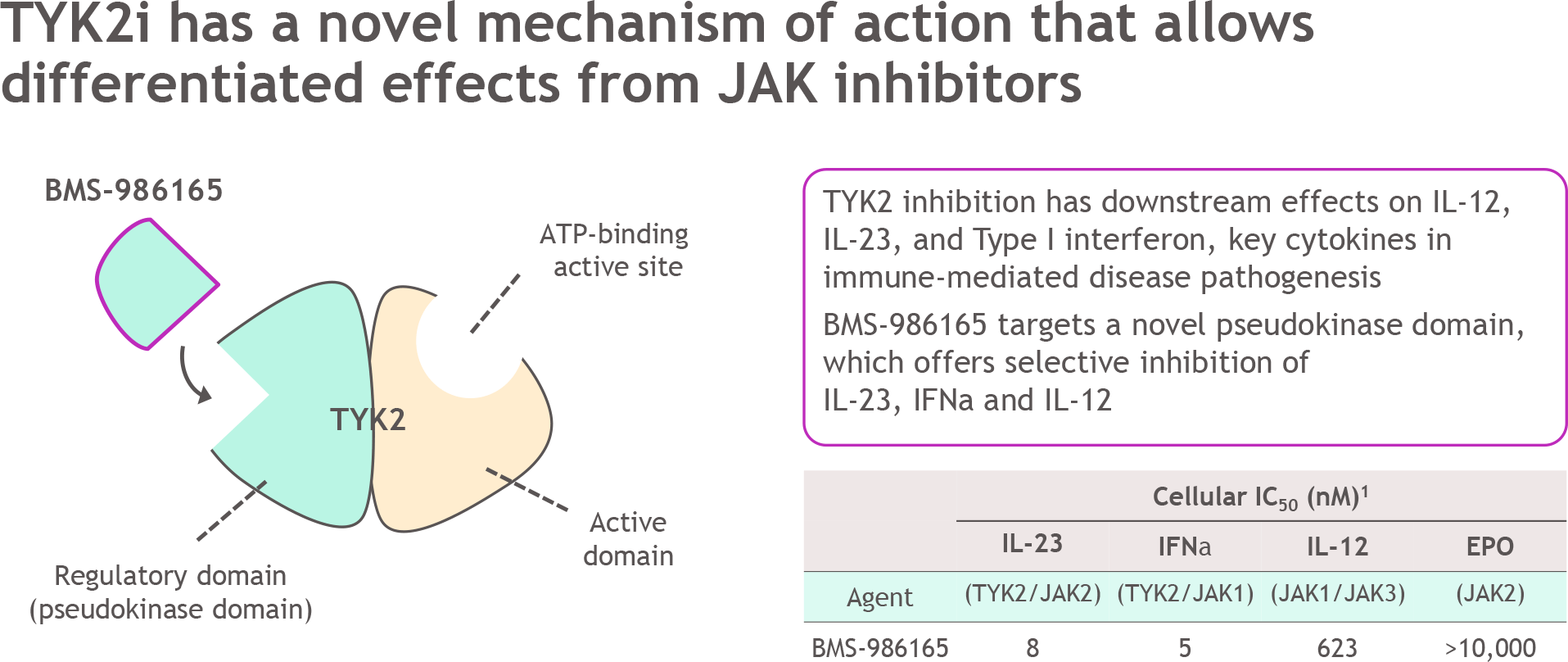
Deucravacitinib (BMS-986165) is a first-in-class oral selective allosteric inhibitor of non-receptor tyrosine-protein kinase 2 (TYK2).
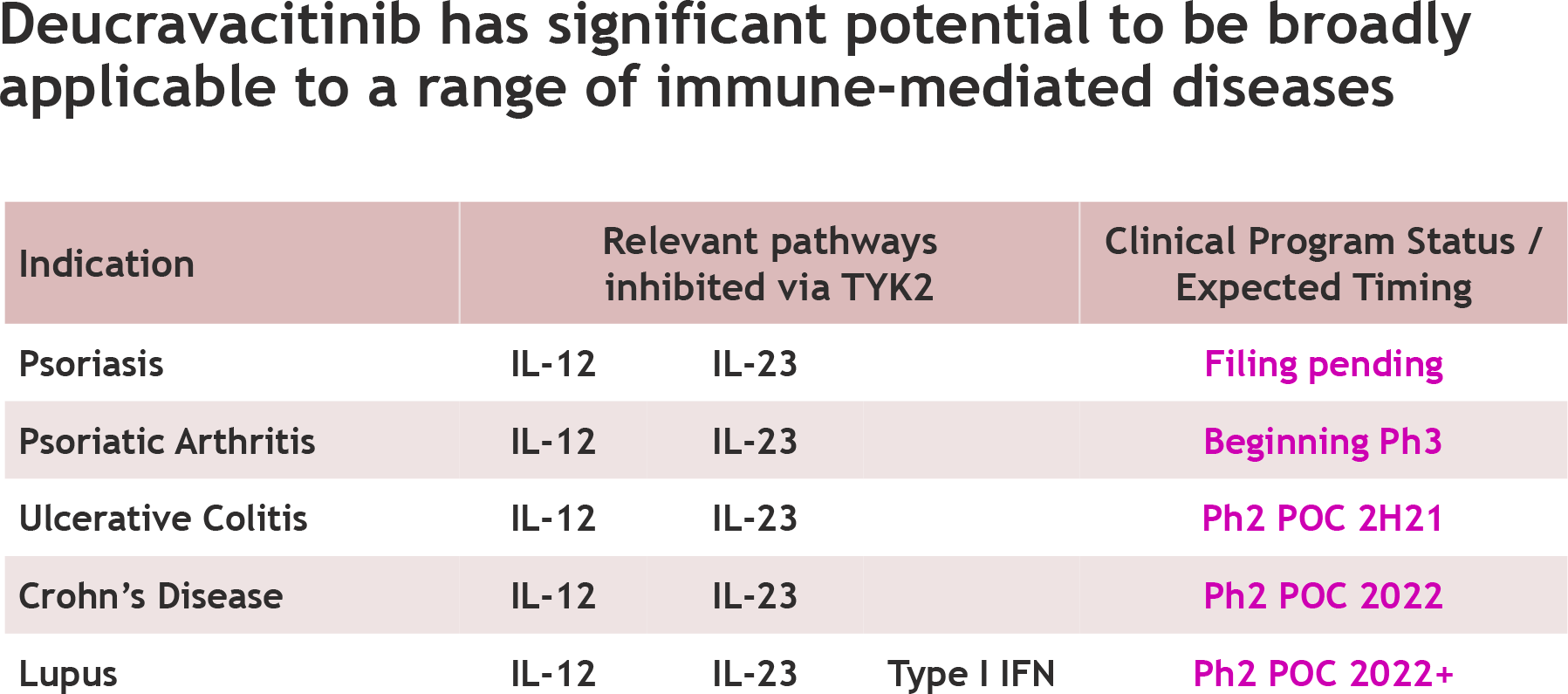
TYK2 enzyme, as an intracellular signaling kinase, mediates the signaling of interleukin 23 (IL-23), interleukin 12 (IL-12), and interferon type I (IFN I), key cytokines in the pathogenesis of psoriasis. Suppression of TYK2 inhibits their expression which is beneficial for therapeutic outcomes. In fact, deucravacitinib affects the pathogenesis of psoriasis through effects on the IL-23/Th17/Th22 axis.
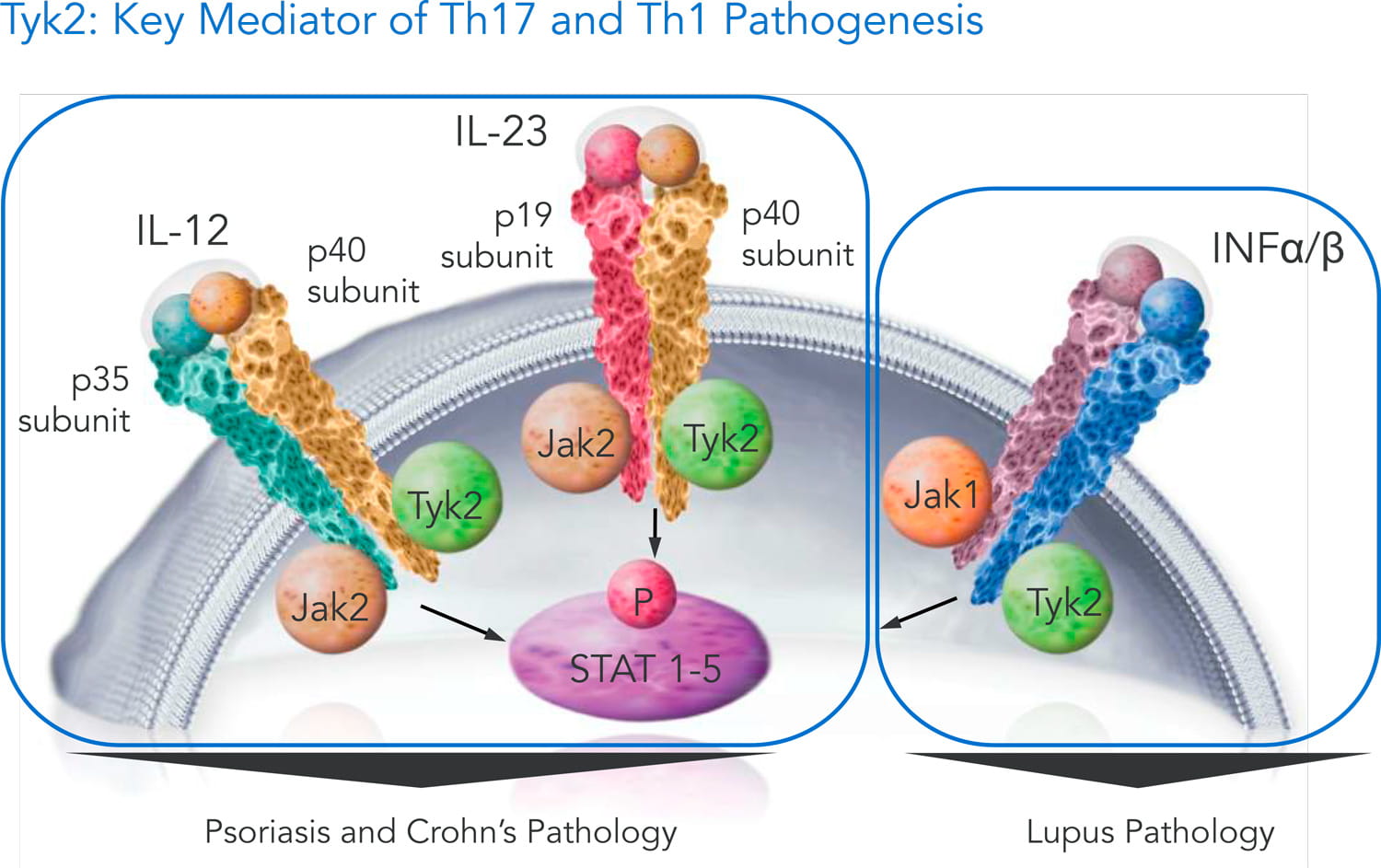
TYK2 belongs to the Janus kinase (JAK) family, which also includes Janus kinases 1, 2, and 3 (JAK1, JAK2, and JAK3). There are quite a few JAK inhibitors circulating on the market that have proven their own suitability in the task of very effective treating autoimmune disorders. Alas, all commercialized JAK inhibitors are accompanied by adverse events, often serious and severe.
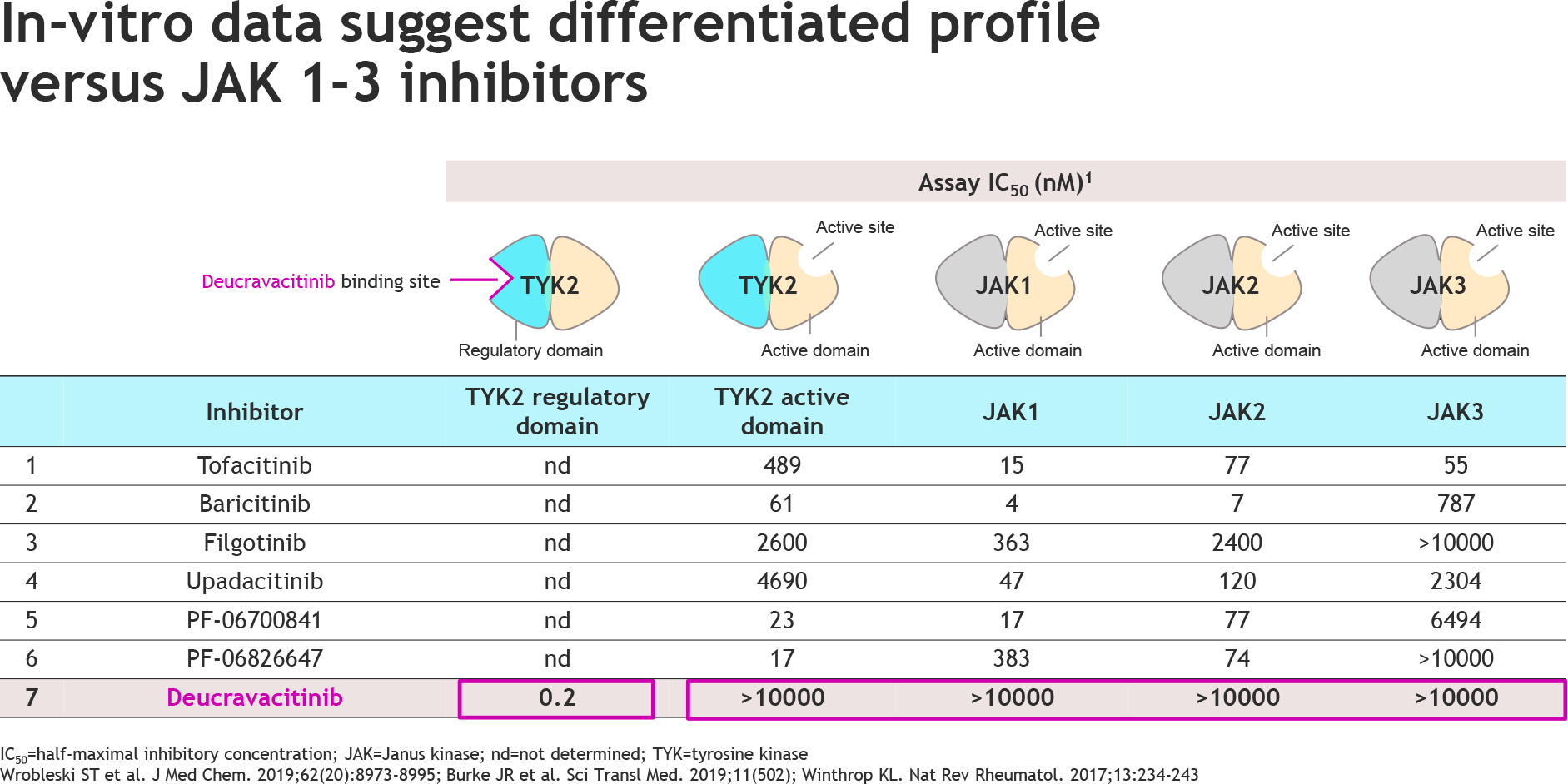
Deucravacitinib is incredibly selective against TYK2; the drug compound does not affect JAK1, JAK2, or JAK3 in any way. Moreover, deucravacitinib binds TYK2 in the regulatory (pseudokinase, JH2) domain rather than in the active (catalytic, JH1) domain. In other words, instead of inhibiting catalytic kinase activity by blocking ATP (with subsequent blocking of phosphorylation and signal transduction), functional inhibition is accomplished through an allosteric mechanism. A strict targeting of the regulatory domain of TYK2 avoided any impact on the other members of the JAK family because their regulatory domains are different but their active domains are very similar.
By strictly targeting only TYK2, deucravacitinib is spared any of the safety problems inherent in all existing JAK inhibitors, whether it is an increased risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction, non-fatal stroke), serious infections (which can lead to hospitalization or death), malignancies, thrombosis, all-cause mortality.
Sotyktu for Psoriasis Treatment: Better Than Otezla
Deucravacitinib did well in the first pivotal phase 3 (randomized, double-blind, placebo-controlled, active comparison group, multicenter, international) clinical trial POETYK PSO-1 (NCT03624127) that tested its safety and effectiveness in the therapy of adult patients (n=666) with moderate-to-severe plaque psoriasis.
In the group of subjects who received a daily 6-mg dose of Sotyktu, a greater proportion of participants than in the placebo group reached the primary endpoints of at least 75% skin clearance, according to the Psoriasis Area and Severity Index (PASI 75), and clear or almost clear skin, according to the static Physician Global Assessment (sPGA 0/1), after 16 weeks of treatment.
The deucravacitinib group also outperformed the group treated with Otezla (apremilast), an oral selective phosphodiesterase 4 (PDE4) inhibitor.
By the way, Otezla, formerly owned by Bristol-Myers Squibb, had to be sold to Amgen for $13.4 billion, as required by the antitrust regulators overseeing the Celgene takeover.
A second pivotal phase 3 clinical trial POETYK PSO-2 (NCT03611751), following the same protocol, demonstrated similar success.
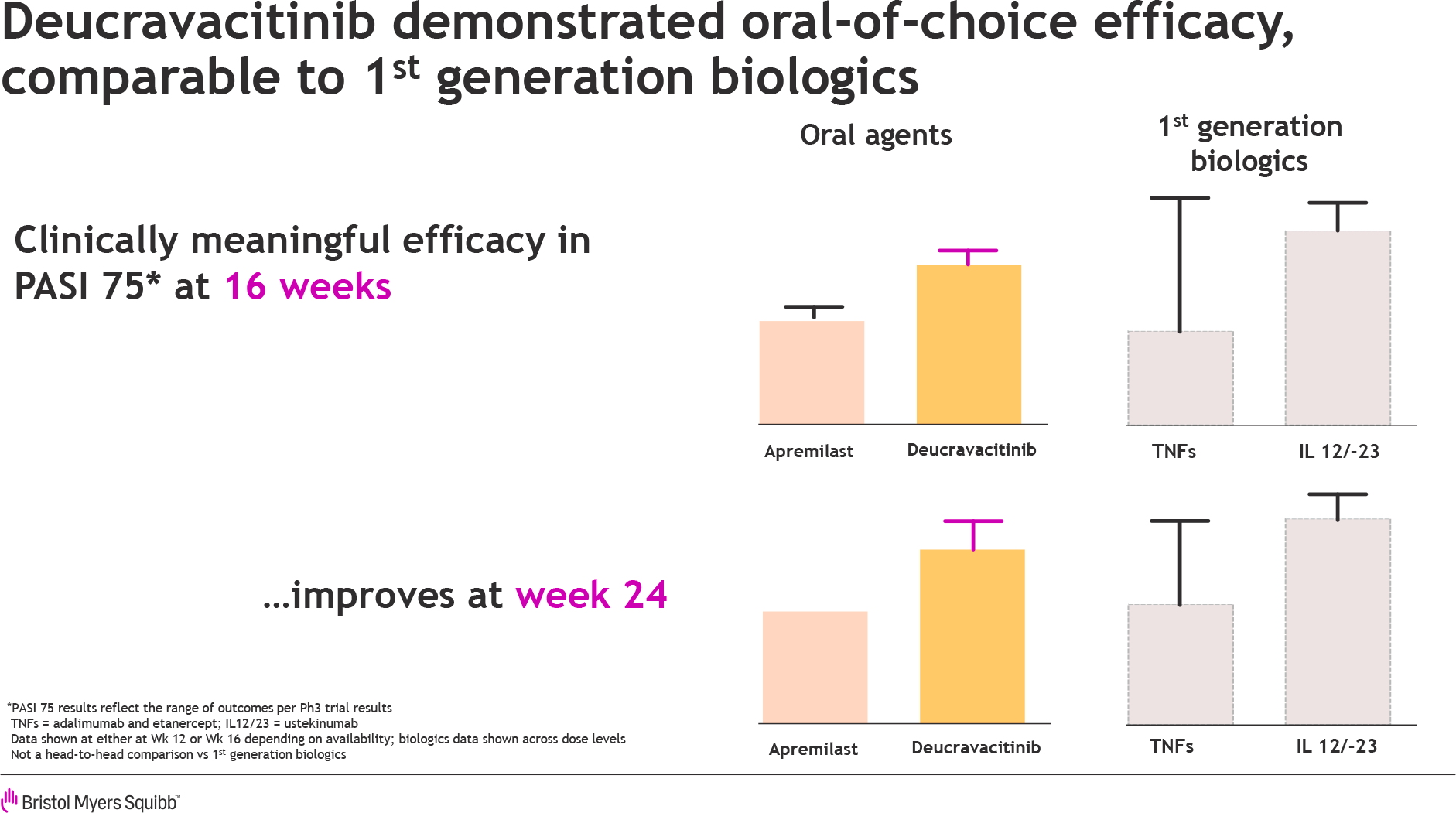
There was considerable hope that the efficacy of Sotyktu will be on par with that shown in the earlier phase 2 clinical trial NCT02931838 when as many as 75% of patients reached PASI 75 in 12 weeks of treatment. By comparison, Otezla gets 33% of psoriasis patients to PASI 75 in 16 weeks.
Thus, the antipsoriatic efficacy of deucravacitinib is thought to be more than twice that of apremilast, given that the former is taken once a day while the latter is taken twice a day.
To meet investors’ high expectations, Bristol-Myers Squibb went for a little “trickery”: POETYK PSO-1 and POETYK PSO-2 have attracted, compared to the recruitment in NCT02931838, a smaller number of patients previously treated with biological drugs for psoriasis — approximately 25% versus 44%. In other words, the response to treatment with deucravacitinib, in theory, should increase.
In addition to its respectable efficacy, which Bristol-Myers Squibb claims is comparable to that of biologics treatment for psoriasis, small-molecule deucravacitinib has a safety profile that distinguishes it from related drugs.
Sotyktu and Psoriasis Treatment: Clinical Trial Full Results
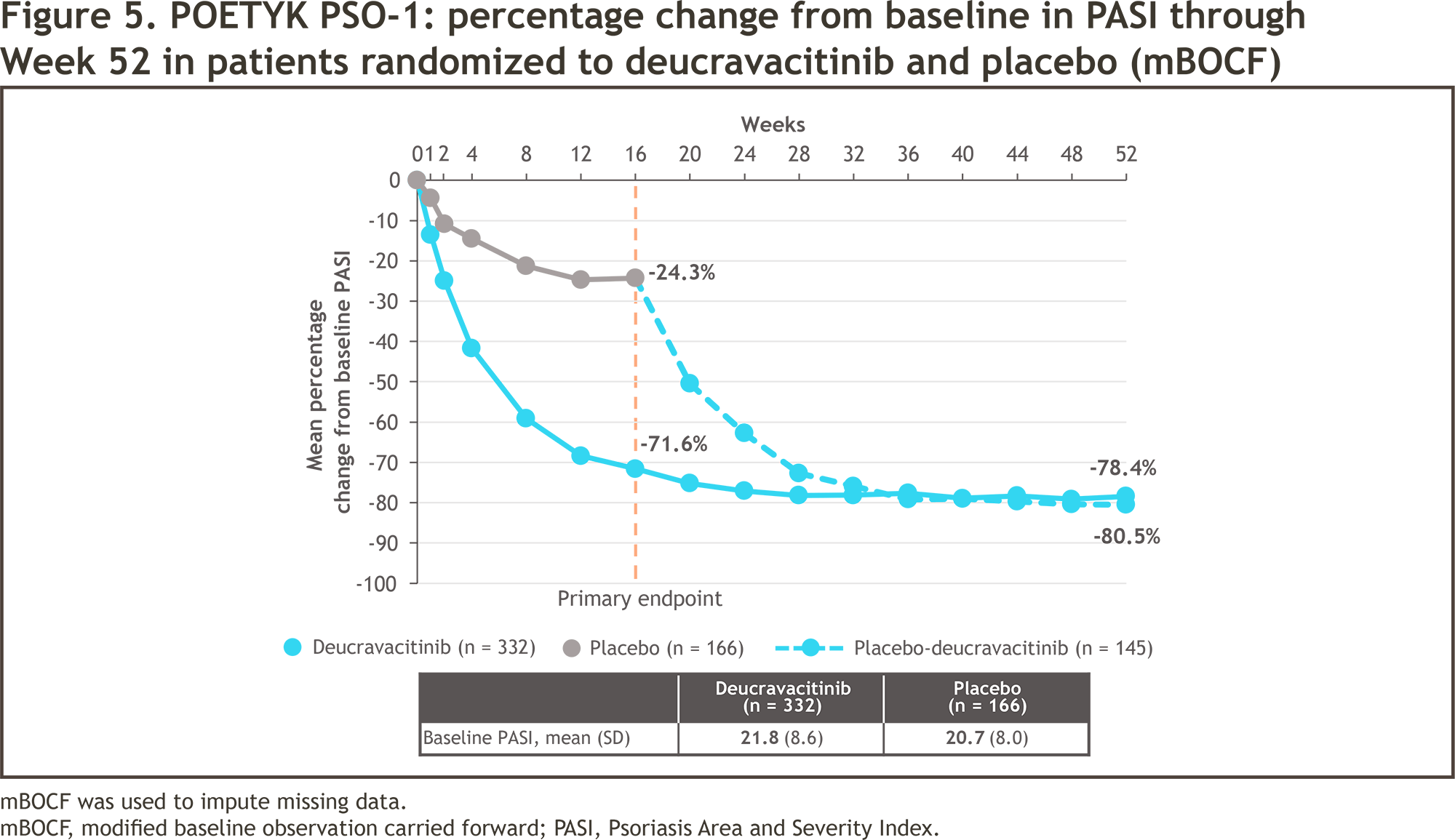
Bristol-Myers Squibb has disclosed the full results of two pivotal phase 3 clinical trials, POETYK PSO-1 (NCT03624127) and POETYK PSO-2 (NCT03611751), which compared the effectiveness of deucravacitinib with placebo or Otezla in treating patients with moderate-to-severe plaque psoriasis. As might be expected, the experimental drug beat the control groups sweepingly.
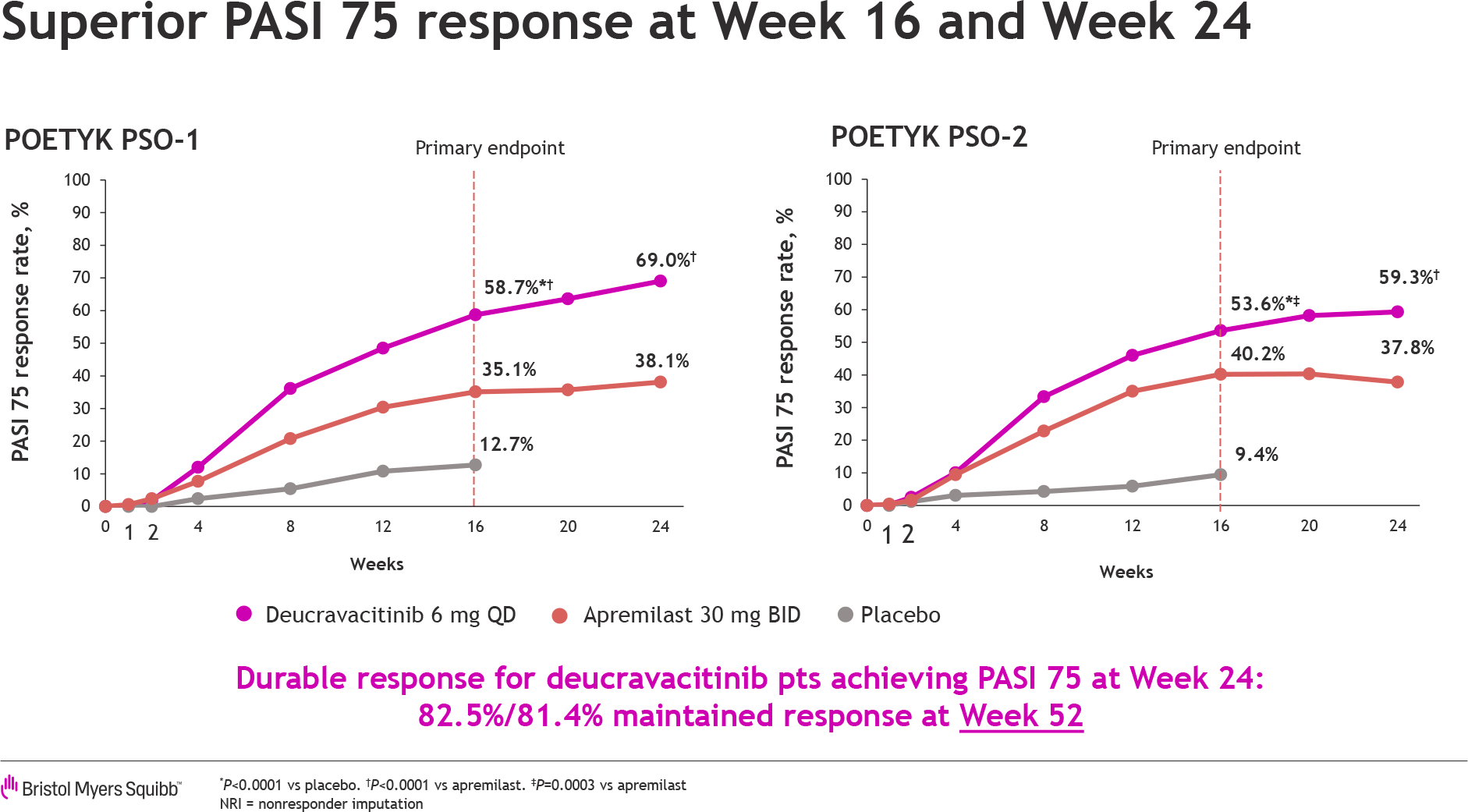
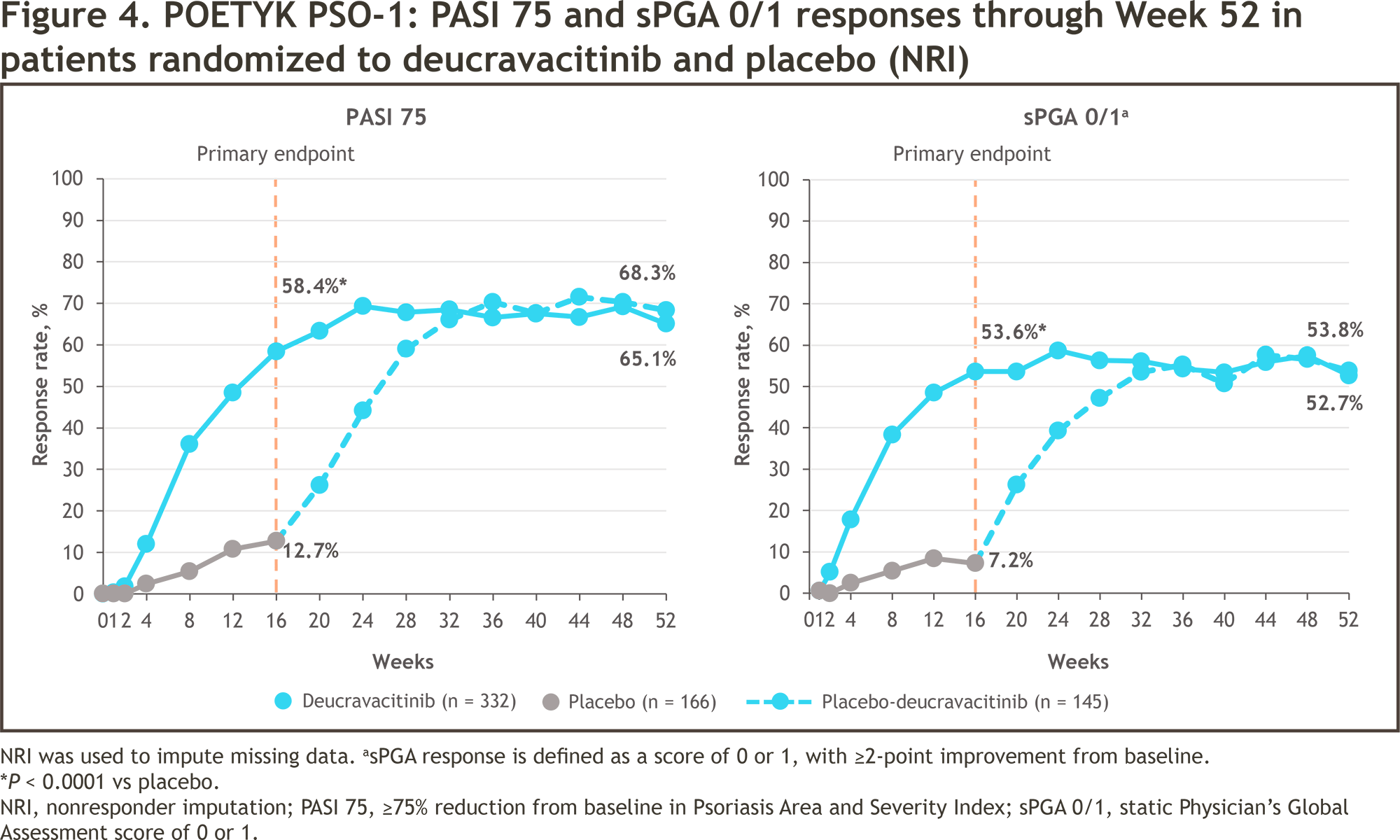
After 16 weeks of treatment, 58% and 53% of patients in the POETYK PSO-1 and POETYK PSO-2 deucravacitinib groups reached PASI 75, respectively — versus 13% and 9% in placebo groups (p<0.0001) and 35% and 40% in apremilast groups (p<0.0001 and p=0.0004).
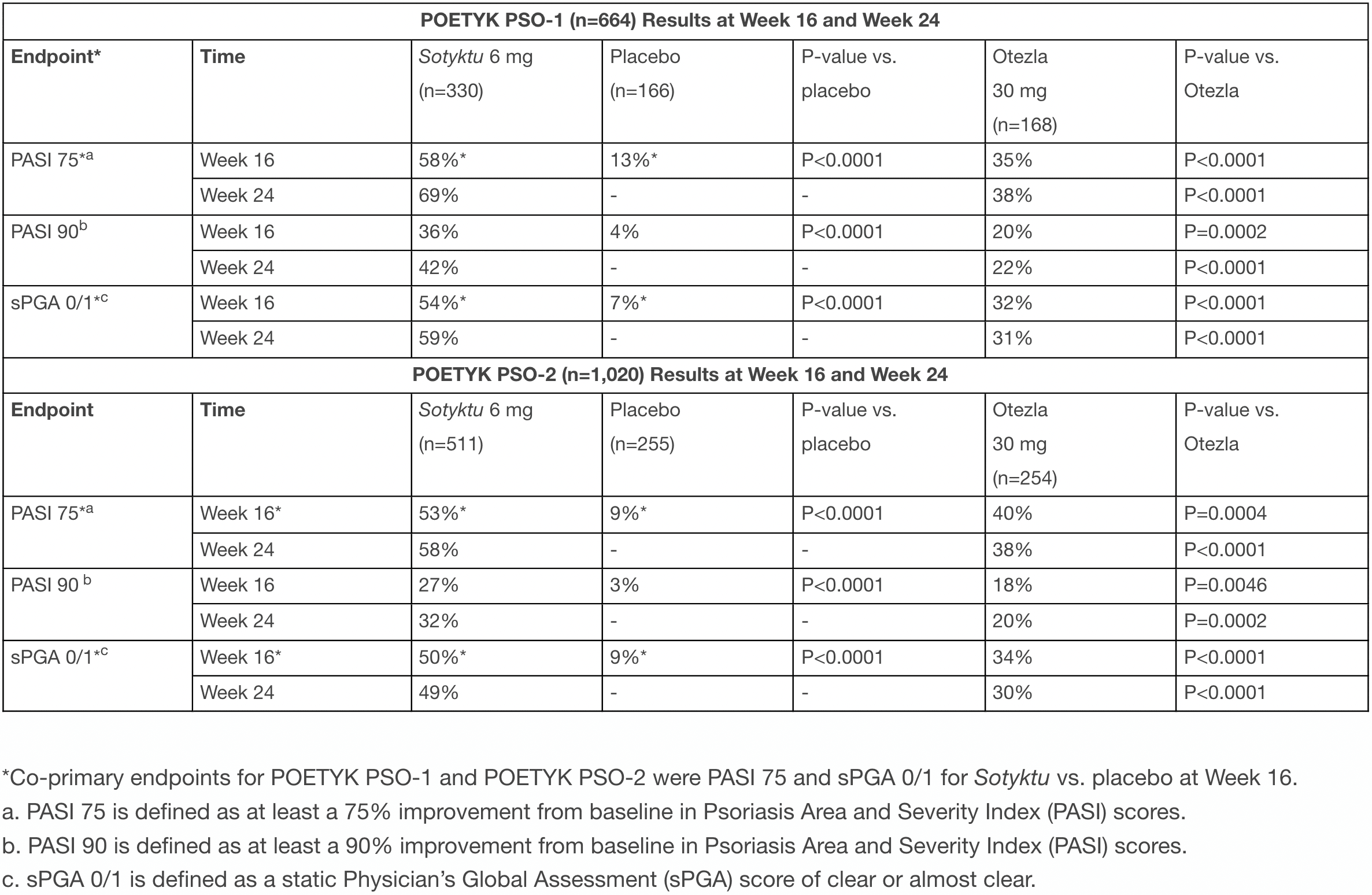
After 24 weeks, response to treatment improved; PASI 75 was evidenced for 69% and 58% of subjects receiving deucravacitinib — vs. 38% and 38% in apremilast groups (p<0.0001).
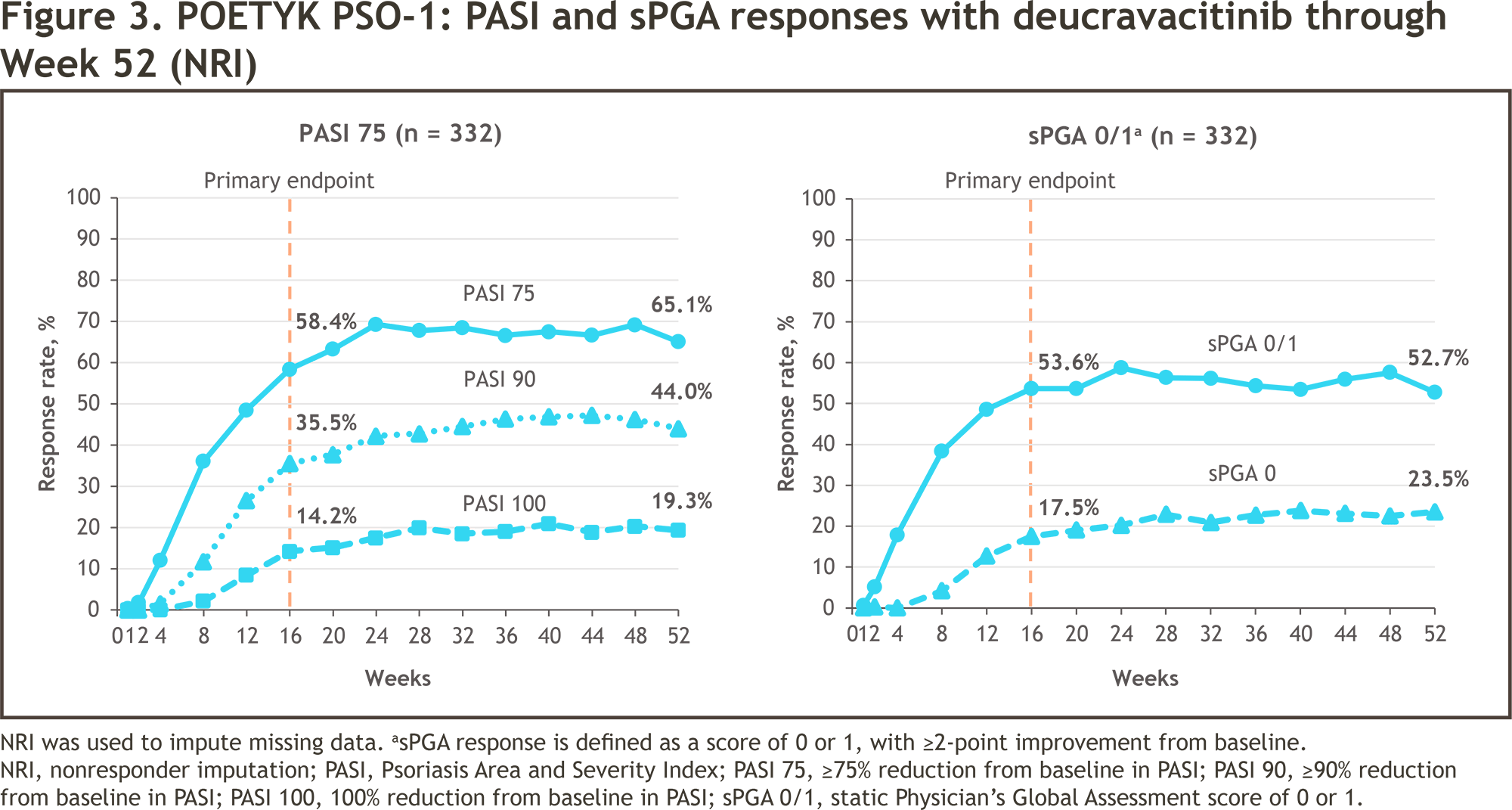
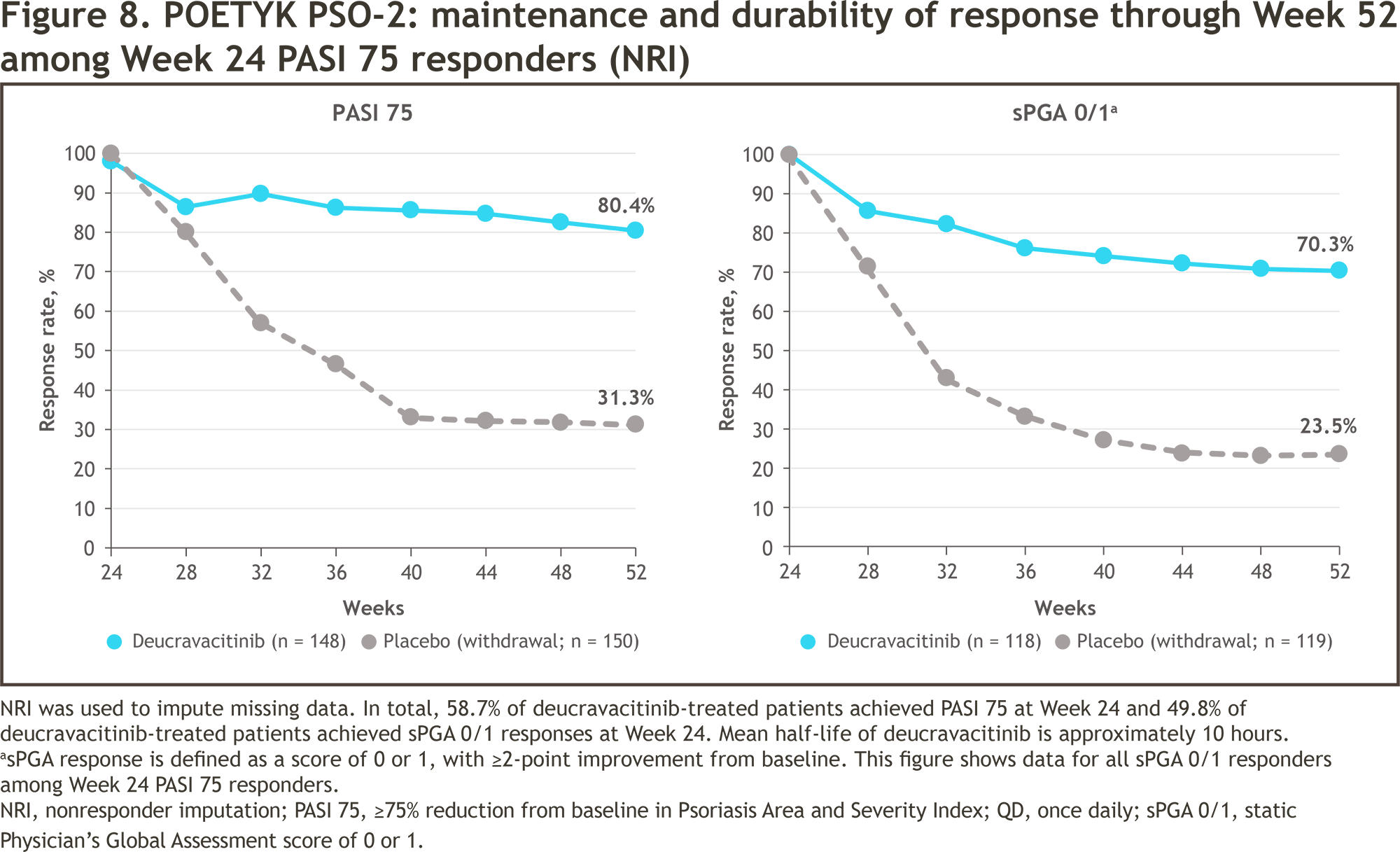
In those patients who received deucravacitinib and reached PASI 75 at week 24 and then continued treatment with it, PASI 75 at week 52 was maintained in 82% and 80%.
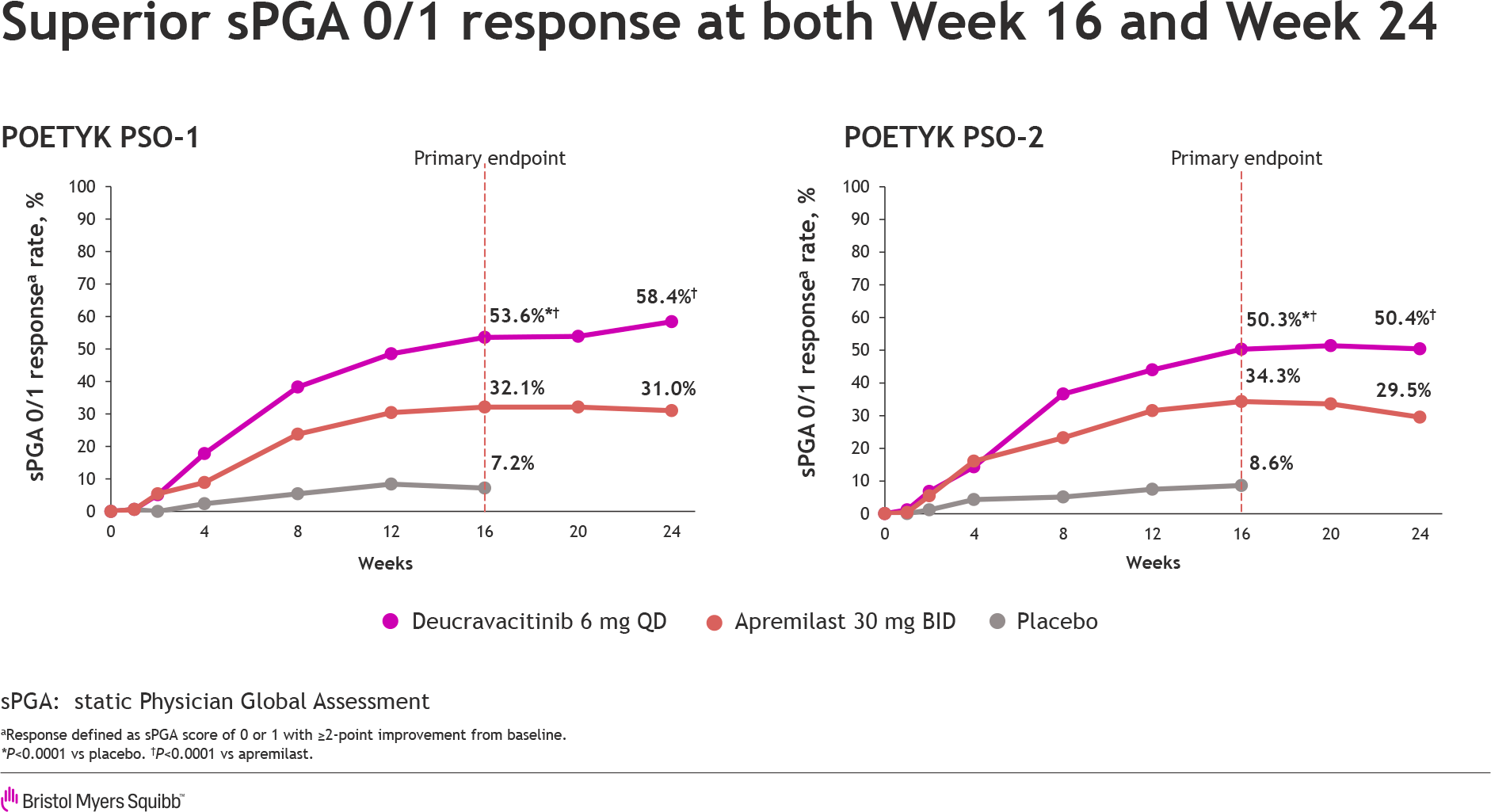
A similar pattern was observed for the psoriasis treatment efficacy index sPGA 0/1 (clear or almost clear skin, with a concomitant improvement of at least 2 points). After 16 weeks of therapy, 54% and 50% of patients treated with deucravacitinib came to it — versus 7% and 9% in the placebo groups (p<0.0001) and 32% and 34% in Otezla groups (p<0.0001).
After 24 weeks of therapy, sPGA 0/1 status was noted for a slightly higher proportion of patients in the deucravacitinib groups (59% and 49%) and, in contrast, decreased in the apremilast groups (31% and 30%) [p<0.0001].
Among other outcomes of Sotyktu therapy:
- PASI 90 after 16 weeks of treatment: in 36% and 27% of patients in POETYK PSO-1 and POETYK PSO-2, respectively
- PASI 90 after 24 weeks: 42% and 32%
- PASI 100 after 16 weeks: 14% and 10%.
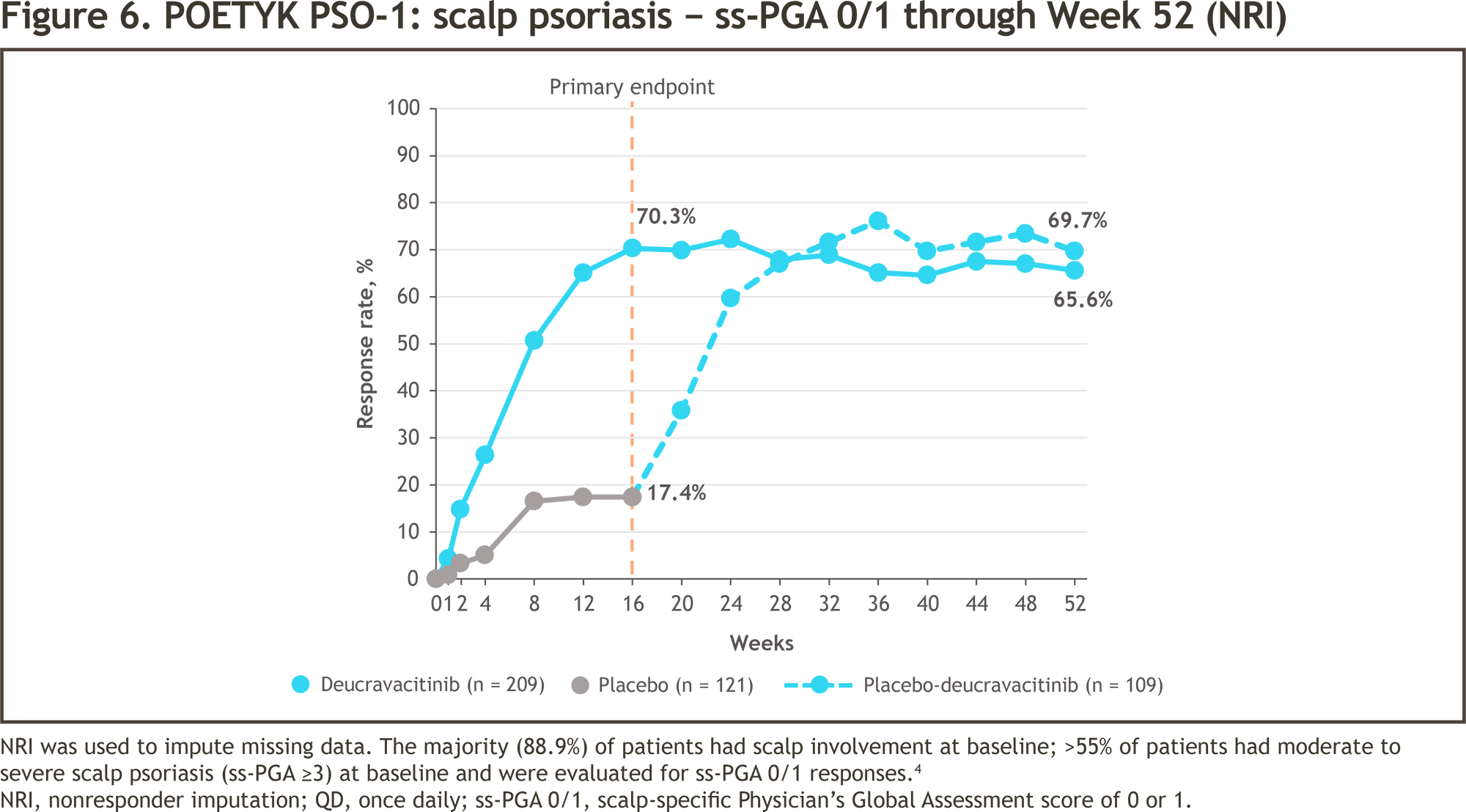
Scalp psoriasis also responded to administration of Sotyktu. After 16 weeks of treatment, sPGA 0/1 status was fair for 70% and 60% of patients — versus 17% in the placebo groups and 39% and 37% in the Otezla groups.
Overall, treatment of psoriasis with oral Sotyktu has demonstrated efficacy comparable to that of first-generation injectable biologic drugs, which are TNF inhibitors such as Humira (adalimumab) or Enbrel (etanercept). Alas, the efficacy of deucravacitinib has not caught up with second-generation biologics such as Stelara (ustekinumab), an interleukin 12 (IL-12) and interleukin 23 (IL-23) inhibitor.
POETYK PSO-1 and POETYK PSO-2 results, collected over 52 weeks of treatment, indicate the maintenance of the therapeutic effect of deucravacitinib from the position of sustaining PASI 75 and/or sPGA 0/1 status. In other words, it makes sense to talk about the rationale for continuous daily use of Sotyktu in order to maintain remission of plaque psoriasis.
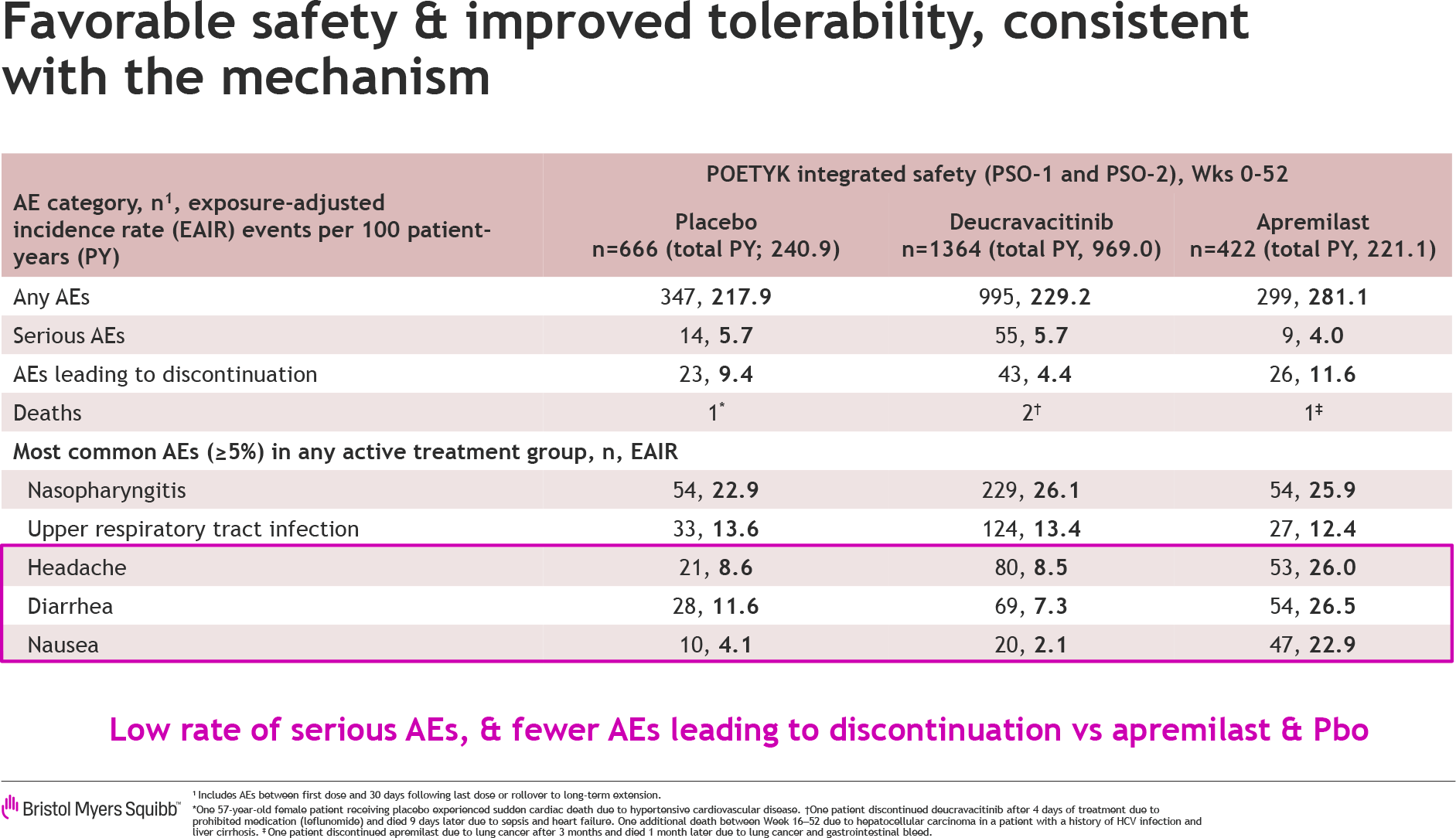
In terms of safety, deucravacitinib was characterized by acceptable tolerability and a similar safety profile to placebo and apremilast. The most common adverse events to deucravacitinib included: nasopharyngitis (in 17% of patients), upper respiratory tract infections (9%), headache (6%), diarrhea (5%), nausea (2%).
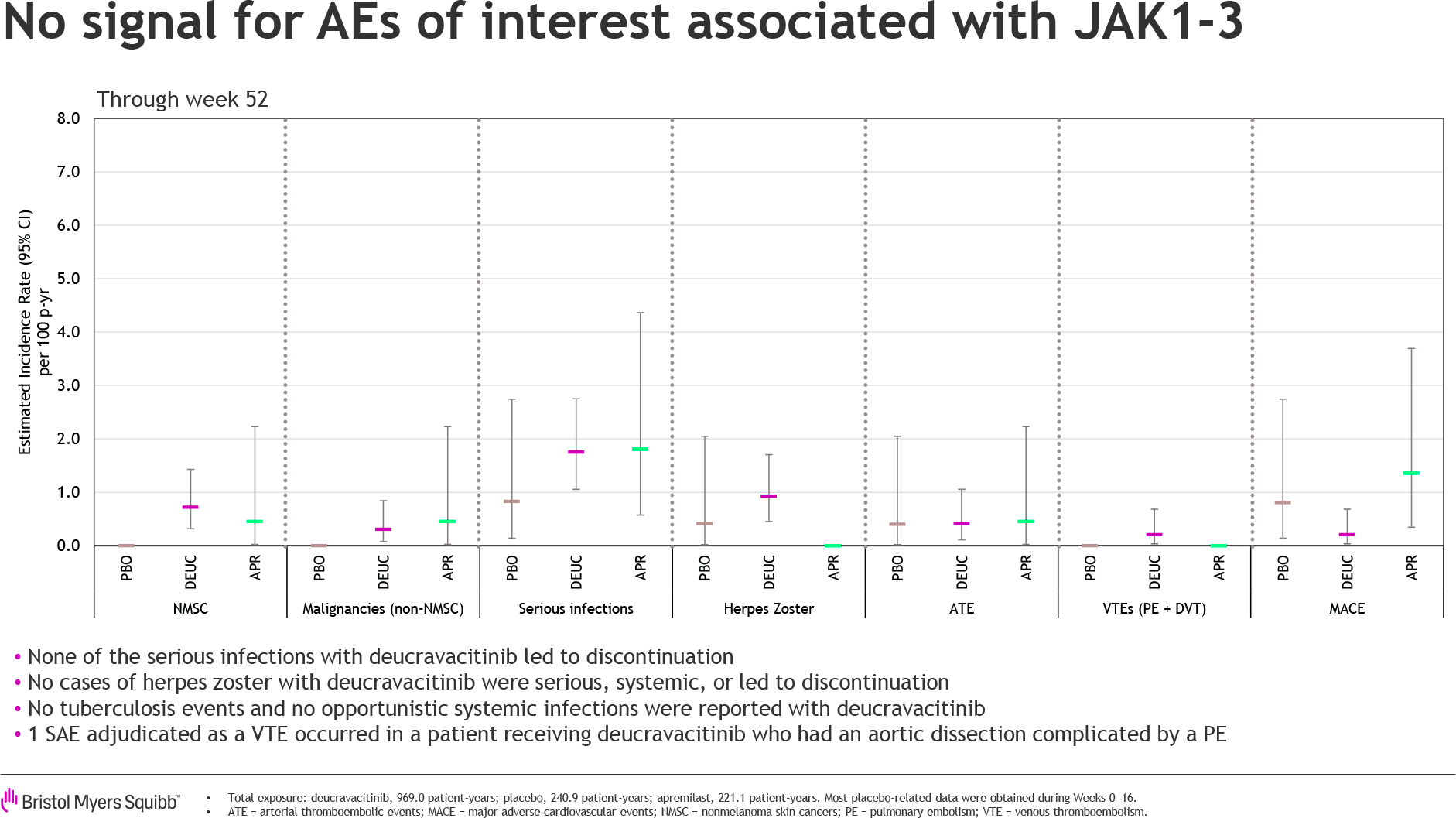
When it comes to adverse events common to all existing JAK inhibitors, there are essentially none for Sotyktu. The frequencies of major adverse cardiovascular events (MACEs), malignancies, venous thromboembolism (VTE), and serious infections were low and evenly distributed between treatment groups.
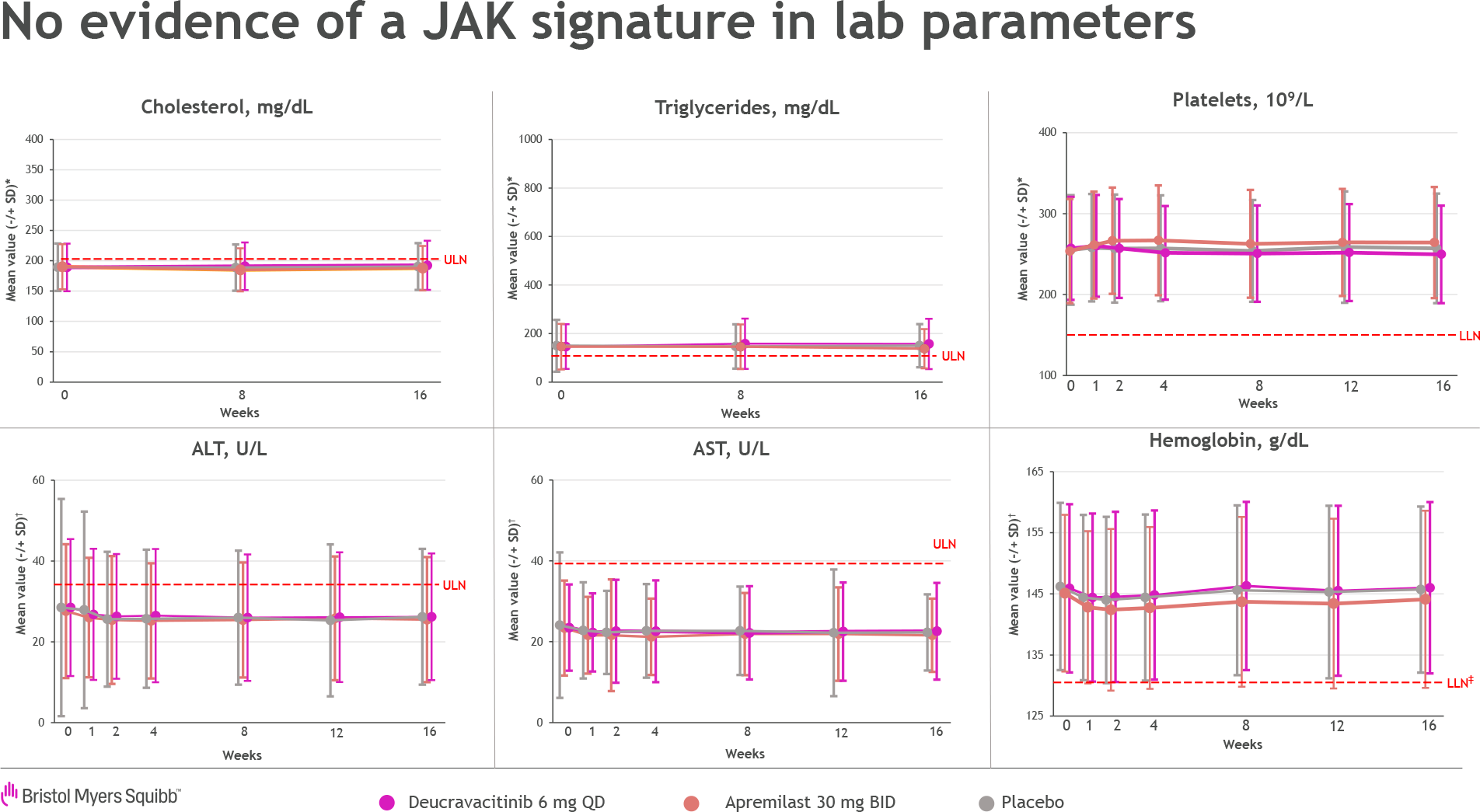
Deucravacitinib had no clinically meaningful effect on changes in metabolic and laboratory parameters, including cholesterol, triglycerides, platelets, hemoglobin, ALT, and AST.
Sotyktu Against Psoriasis: Long-Term Results
The ongoing POETYK PSO-LTE (NCT04036435) phase 3 (nonrandomized, open-label, multicenter, multinational) clinical trial is testing the long-term efficacy and safety of deucravacitinib used for up to 5 years in the treatment of moderate-to-severe psoriasis among patients who have completed the POETYK PSO-1 (NCT03624127) and POETYK PSO-2 (NCT03611751) clinical trials.
After 1 years of therapy, Sotyktu has demonstrated sustained therapeutic efficacy. The response rates to treatment — assessed by a minimum of 75% skin clearance according to the Psoriasis Area and Severity Index (PASI 75) and clear or nearly clear skin according to the static Physician Global Assessment (sPGA 0/1) — were 78% and 59%, respectively.
- Before POETYK PSO-LTE, the PASI 75 and sPGA 0/1 rates were 65% and 51%.
After 2 years of administration of Sotyktu, PASI 75 and sPGA 0/1 rates were fair for 82% and 67% of patients. To PASI 90 came out 55% of the subjects.
No new problems with the safety profile of deucravacitinib were identified. Adverse events, which were predominantly mild-to-moderate in severity, were mainly nasopharyngitis, upper respiratory tract infection, and headache. The incidence of serious adverse events leading to treatment discontinuation remained low over 2 years.
Sotyktu and Treatment of Autoimmune Diseases: New Blockbuster
Bristol-Myers Squibb had unlimited faith in the success of deucravacitinib against psoriasis, and therefore conducted an additional phase 3 clinical trials, POETYK PSO-3 (NCT04167462) and POETYK PSO-4 (NCT03924427). The first study tested Sotyktu in the treatment of moderate-to-severe plaque psoriasis among Chinese, Taiwanese, and South Korean patients, while the second study tested it in Japanese patients with moderate-to-severe plaque psoriasis as well as psoriatic arthritis, erythrodermic psoriasis, and generalized pustular psoriasis.
The 5-year POETYK PSO-LTE (NCT04036435) phase 3 clinical trial evaluating the long-term safety and efficacy of deucravacitinib against plaque psoriasis is ongoing.
Additional phase 3 clinical trials are underway: NCT04772079, testing the applicability of Sotyktu in the treatment of moderate-to-severe plaque psoriasis in adolescents (12–18 years), and PSORIATYK SCALP (NCT05478499), rolling out Sotyktu in the treatment of moderate-to-severe scalp psoriasis.
In parallel, Bristol-Myers Squibb is conducting an extensive clinical program that is examining the usefulness of Sotyktu in other autoimmune diseases including psoriatic arthritis (PsA), systemic lupus erythematosus (SLE), ulcerative colitis (UC), and Crohn’s disease.
According to consensus estimates by EvaluatePharma, by 2024 deucravacitinib will cross the $1 billion sales threshold achieving best-seller status. In 2026, demand could reach $2.4 billion. Bristol-Myers Squibb itself expects at least $4 billion per year by 2029.
In addition to deucravacitinib, Bristol-Myers Squibb has two other TYK2 inhibitors on its pipeline including a shared one with Nimbus Therapeutics.
New drugs like Sotyktu are critical to Bristol-Myers Squibb’s business, which will inevitably face the loss of patent protection for blockbuster drugs like Revlimid (lenalidomide), Eliquis (apixaban), Opdivo (nivolumab), Pomalyst/Imnovid (pomalidomide), Yervoy (ipilimumab). Medicines with expired patents account for approximately 80% of the company’s current revenue.
Sotyktu for Psoriatic Arthritis: Impressive Efficacy
The NCT03881059 phase 2 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial clarified the safety and efficacy of deucravacitinib in the treatment of adult patients (n=203) with psoriatic arthritis (PsA) diagnosed at least 6 months ago.
Participants’ disease must have been in active form: at least 3 swollen and at least 3 tender joints. Other mandatory inclusion criteria: high sensitivity C-reactive protein (hsCRP) ≥ 3 mg/L, at least one psoriatic lesion ≥ 2 cm.
Subjects’ psoriatic arthritis must have been characterized by inadequate response or patient intolerance to at least one nonsteroidal anti-inflammatory drug (NSAID), corticosteroid and/or conventional synthetic disease-modifying antirheumatic drug (csDMARD).
Participants should not have previously been treated for psoriatic arthritis with biologic disease-modifying antirheumatic drugs (bDMARDs) except for a single tumor necrosis factor inhibitor (TNF) to which their disease did not respond appropriately or for which tolerance had developed.
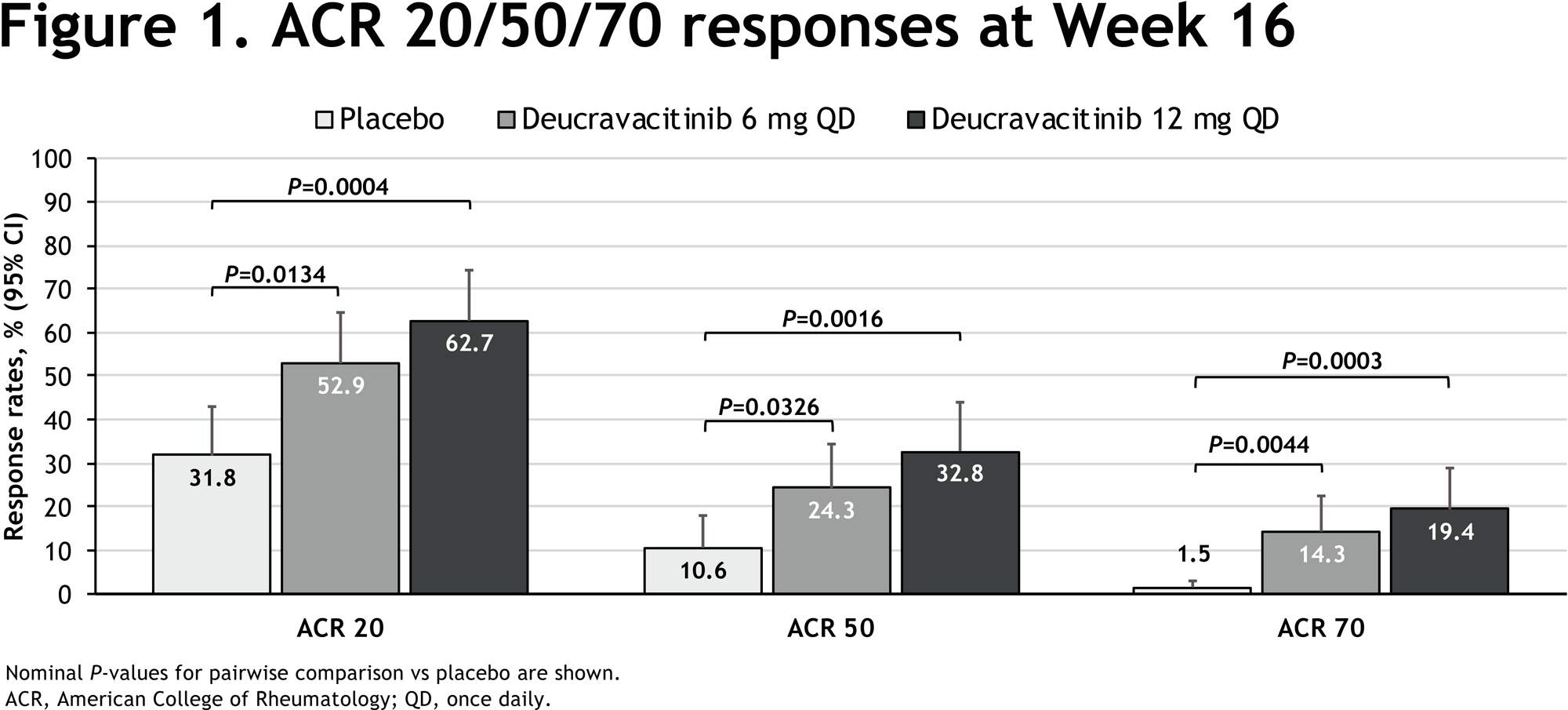
After 16 weeks of treatment, the Sotyktu groups, administered once daily at 6 or 12 mg, reached the primary endpoint of at least 20% improvement in disease signs and symptoms, as estimated by the American College of Rheumatology (ACR 20). This rate was recorded for 53% (n=37/70) and 63% (n=42/67) of patients — versus 32% (n=21/66) in the placebo group (p=0.0134 and p=0.0004).
The administration of Sotyktu provided statistically significant beneficial effects on other clinical outcomes, including important to the patients themselves, such as:
- Improvement in psoriatic arthritis signs and symptoms by at least 50% (ACR 50): among 24% and 33% of patients in the 6- and 12-mg dose deucravacitinib groups — vs. 11% in the placebo group (p=0.0326 and p=0.0016)
- Improvement in psoriatic arthritis signs and symptoms by at least 70% (ACR 70): among 14% and 19% — vs. 1.5% (p=0.0044 and p=0.0003)
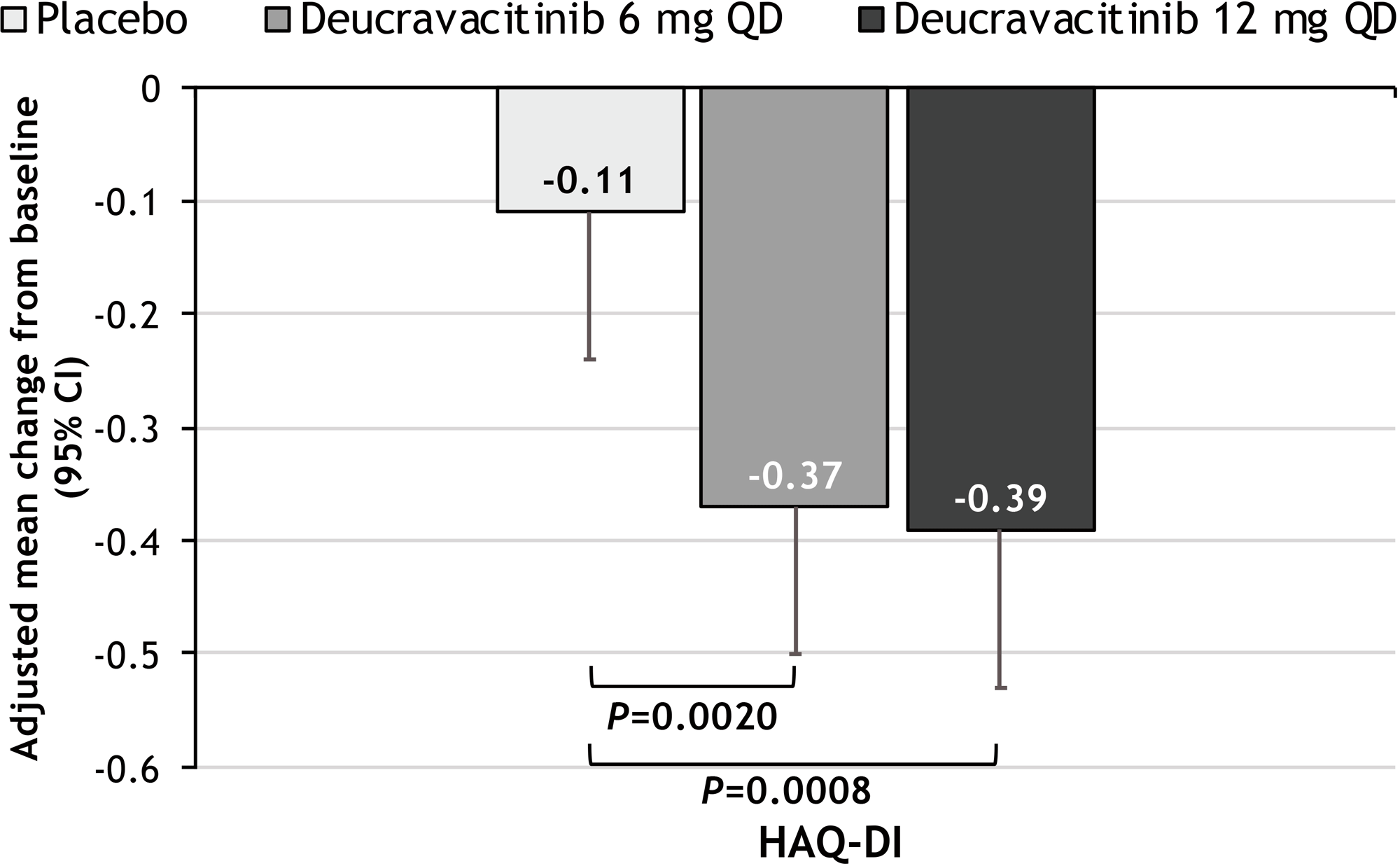
- Improvement in functional status relative to baseline, according to the Health Assessment Questionnaire — Disability Index (HAQ-DI): −0.37 and −0.39 — vs. −0.11 (p=0.0020 and p=0.0008)
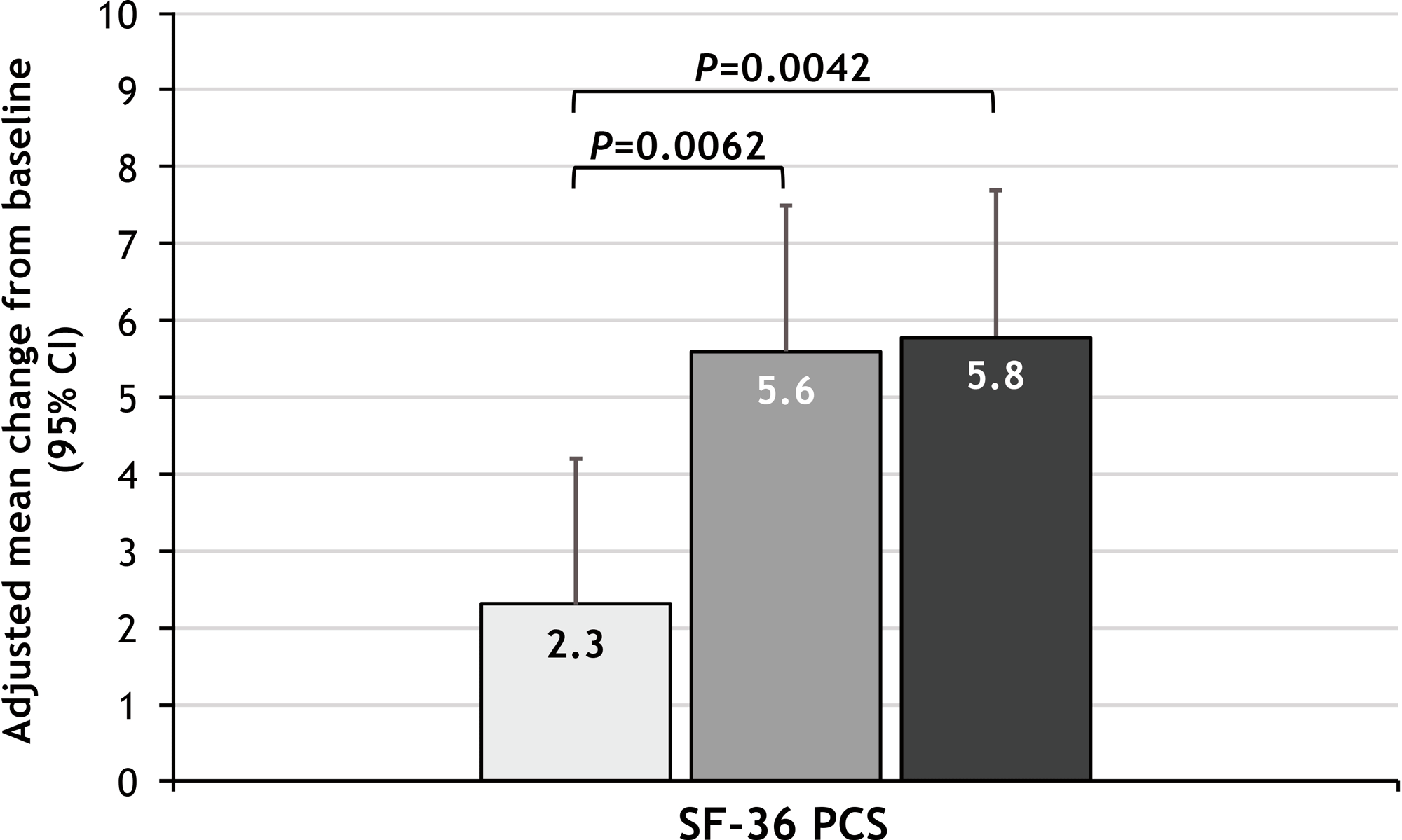
- Improvement in the Physical Component Summary (PCS) score of the Short Form Health Survey — 36 Item (SF-36) Questionnaire: 5.6 and 5.8 — vs. 2.3 (p=0.0062 and p=0.0042).
In addition, treatment of psoriatic arthritis with Sotyktu resulted in several of the following positive changes:
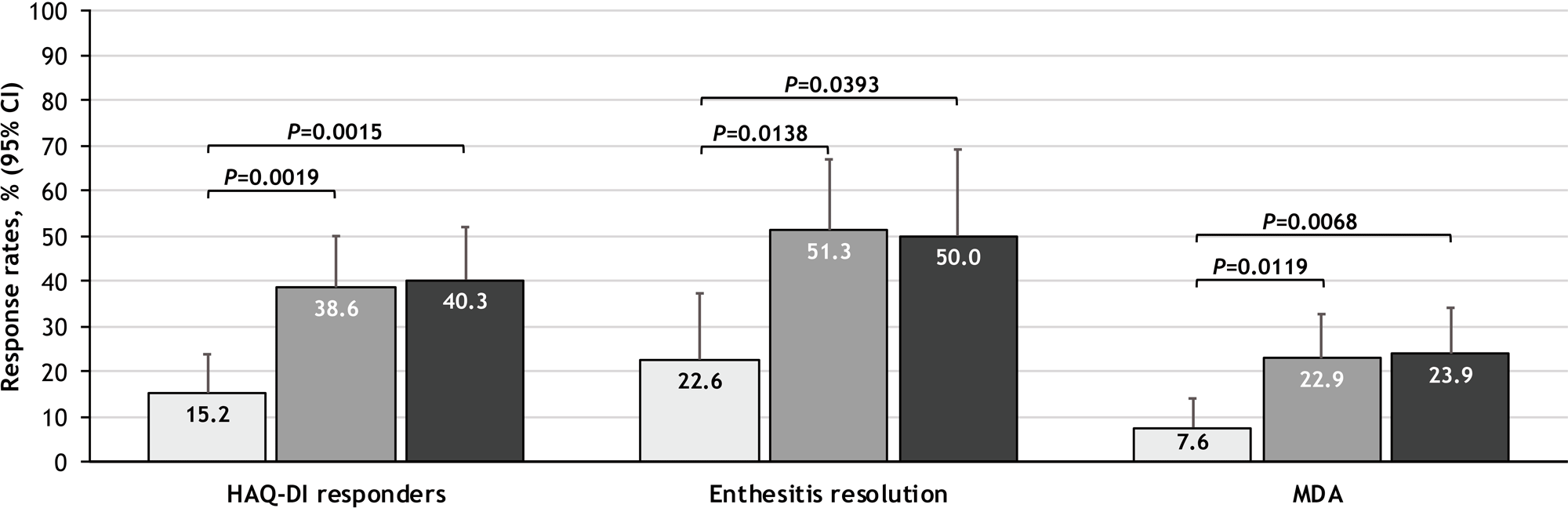
- HAQ-DI response (achieving a minimal clinically significant change in HAQ-DI of 0.35): among 39% and 40% of patients — versus 15% (p=0.0019 and p=0.0015)
- Resolution of enthesitis (connective tissue inflammation between tendons or ligaments and bone) by the Leeds Index: among 51% and 50% — vs. 23% (p=0.0138 and p=0.0393)
- Minimal disease activity (MDA) defined according to the combined assessment of the main criteria of psoriatic arthritis related to joints, skin lesions, pain, global disease activity, and health assessment questionnaire scores: among 23% and 24% — vs. 8% (p=0.0119 and p=0.0068).
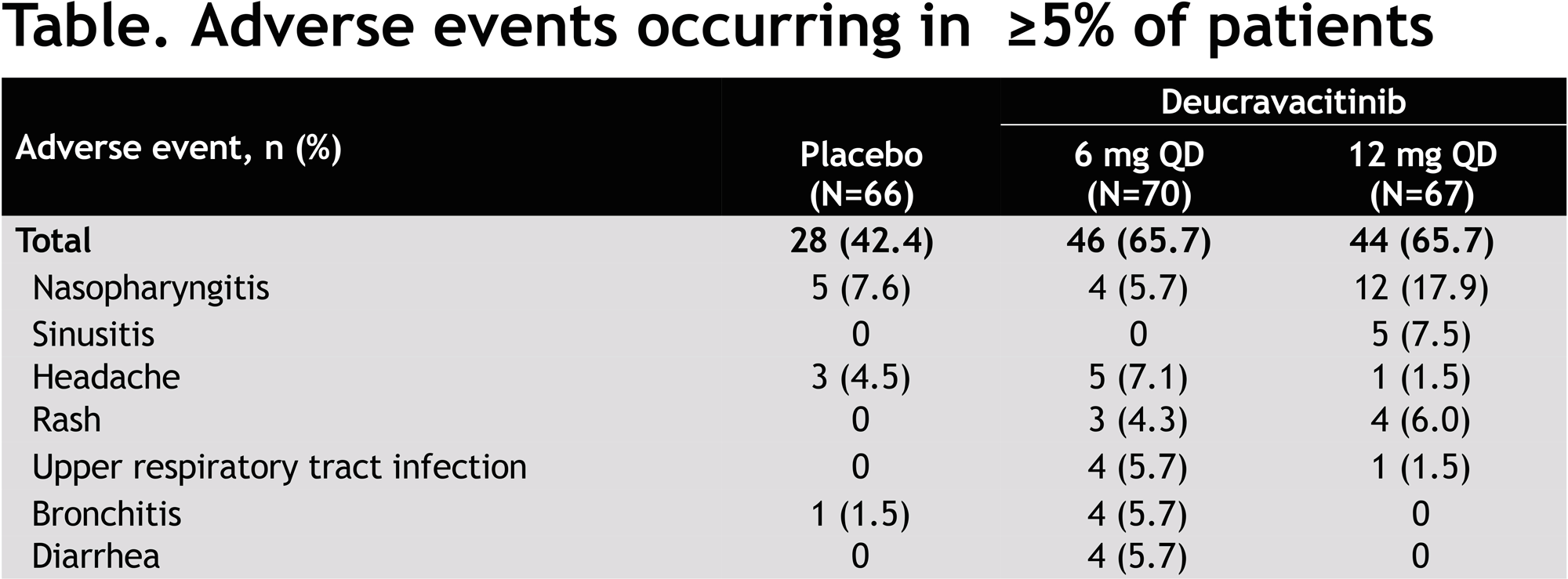
No serious adverse events have been reported with deucravacitinib administration. The most common adverse reactions in the deucravacitinib (6 and 12 mg) and placebo groups included nasopharyngitis (in 6%, 18%, 8% of patients), rash (4%, 6%, 0%), headache (7%, 2%, 5%), upper respiratory infections (6%, 2%, 0%), bronchitis (6%, 0%, 0%), diarrhea (6%, 0%, 0%).
The NCT04908202 phase 3 clinical trial testing Sotyktu in the treatment of active psoriatic arthritis in patients who have not previously received bDMARD is ongoing.
The NCT04908189 phase 3 clinical trial studying Sotyktu in the treatment of active psoriatic arthritis in patients who have not previously received bDMARD or have been treated with TNF inhibitors without success is ongoing.
Sotyktu for Ulcerative Colitis: Not Yet Success
The LATTICE-UC (NCT03934216) phase 2 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial evaluated the effectiveness of deucravacitinib in the treatment of moderate-to-severe ulcerative colitis.
After 12 weeks of therapy, the deucravacitinib group failed to statistically significantly outperform the placebo group in terms of progression to clinical remission.
The administration of deucravacitinib also did not result in a statistically significant difference in secondary endpoints such as clinical response, endoscopic response, and histological improvement.
At this stage, it is unclear why Sotyktu failed in ulcerative colitis. And so Bristol-Myers Squibb will continue to test it in the treatment of this inflammatory bowel disease: to that end, the NCT04613518 phase 2 clinical trial, in which the drug is used at an increased dose, is ongoing. In addition, there is the NCT03599622 phase 2 clinical trial for the treatment of moderate-to-severe Crohn’s disease.
Sotyktu for Systemic Lupus Erythematosus: It All Worked Out
Deucravacitinib has successfully completed the PAISLEY (NCT03252587) phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial among adult patients (n=363) with moderate-to-severe systemic lupus erythematosus (SLE).
Among the study inclusion criteria: diagnosis of systemic lupus erythematosus at least 24 months before screening; either elevated antinuclear antibody levels (ANA; ≥1: 80), or the presence of antibodies to double-stranded DNA (dsDNA), or the presence of antibodies to Smith antigen (anti-Sm); Total Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) score ≥ 6 and clinical SLEDAI-2K score ≥ 4 with joint involvement and/or rash.
For 48 weeks, participants were given deucravacitinib (at a dose of 3 mg twice daily, 6 mg twice daily, or 12 mg once daily) or placebo.
The primary endpoint for therapeutic efficacy was the proportion of patients who demonstrated a reduction in SLEDAI-2K of at least 4 points (SRI-4) after 32 weeks of treatment.
Patients in the 3-mg deucravacitinib (58%; p=0.0006) and 6-mg deucravacitinib (50%; p=0.0210) groups reached the indicated endpoint — versus 34% in the placebo group. Although the group receiving 12 mg deucravacitinib showed a numerical superiority over the control group (45%), the difference was not statistically significant (p=0.078).
Administration of a 3-mg dose of Sotyktu also provided statistically significant improvements, according to a number of secondary endpoints after 48 weeks of treatment, such as SRI-4, British Isles Lupus Assessment Group–based Composite Lupus Assessment (BICLA), Lupus Low Disease Activity State (LLDAS), decrease of ≥ 50% from baseline Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI-50), and change in active (tender and swollen) joint count.
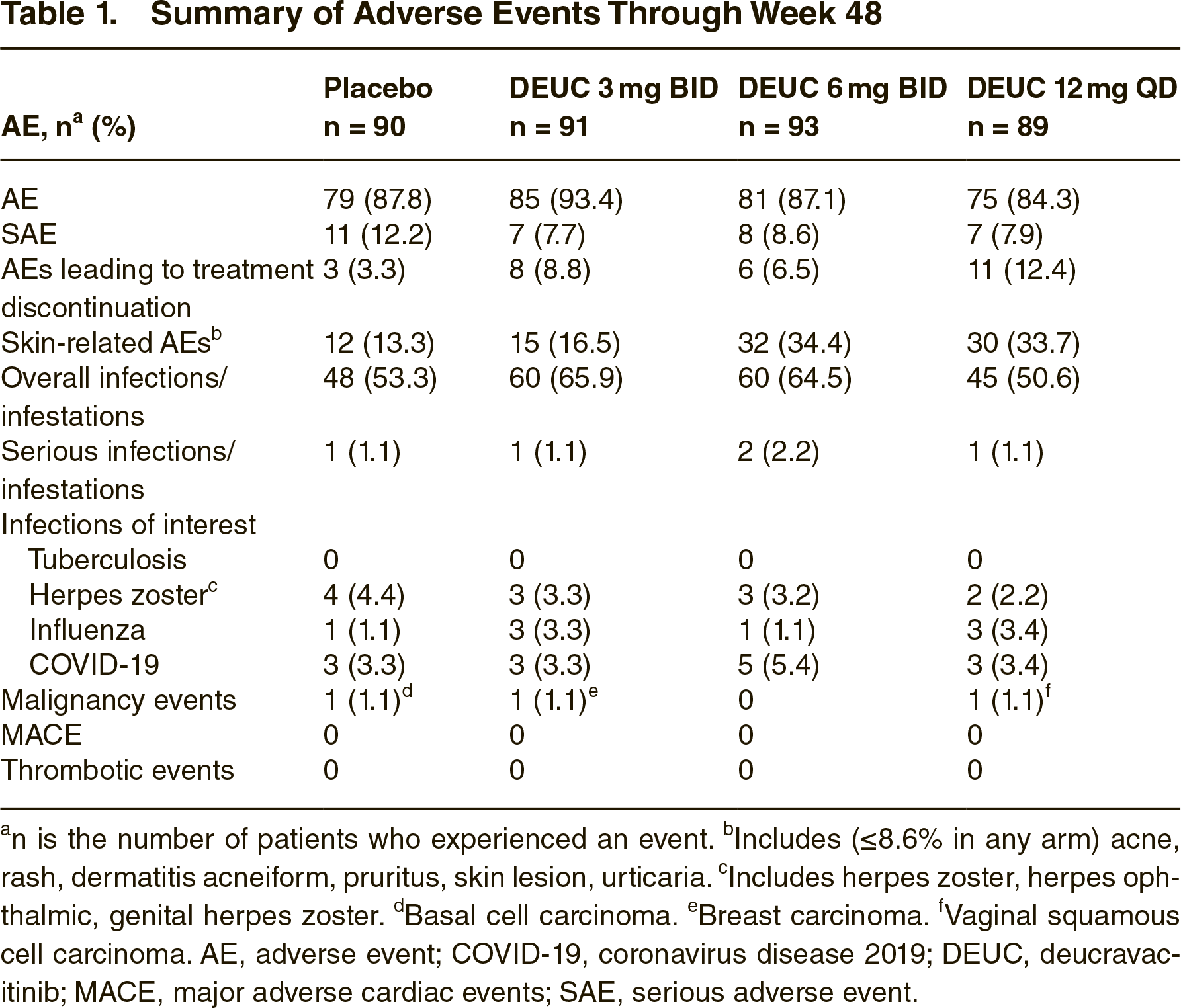
No new safety signals for deucravacitinib were identified: in particular, no fatalities, major adverse cardiovascular events (MACE), thrombosis, systemic opportunistic infections, or active tuberculosis were reported. The frequencies of adverse events were similar in the drug and placebo groups. Among the most common ones observed with deucravacitinib were respiratory tract infections, nasopharyngitis, headache, and urinary tract infections.
PAISLEY participants are invited to continue follow-up in the long-term 3.5-year NCT03920267 phase 2 clinical trial.
The NCT04857034 phase 2 clinical trial, which is evaluating deucravacitinib in the treatment of moderate-to-severe active discoid lupus erythematosus (DLE) and/or subacute cutaneous lupus erythematosus (SCLE) — with or without systemic lupus erythematosus — has been initiated.
In a wave of success, Bristol-Myers Squibb intends to launch a phase 3 clinical trial that will test the therapeutic efficacy of deucravacitinib in the treatment of systemic lupus erythematosus.
Sotyktu: Competing TYK2 Inhibitors
The field of TYK2 inhibitors is handled by Pfizer which has two different molecules. However, they cannot be called targeted exclusively at TYK2; they still affect other Janus kinases.
Ropsacitinib (PF-06826647), TYK2 and JAK2 inhibitor, is being clinically evaluated in the treatment of plague psoriasis and hidradenitis suppurativa (HS). A clinical trial of ropsacitinib in the treatment of ulcerative colitis was discontinued in the fall of 2020.
Brepocitinib (PF-06700841), TYK2 and JAK1 inhibitor, is being validated in the treatment of a wide range of autoimmune inflammatory diseases. Thus, a topical version of brepocitinib is being studied in the treatment of psoriasis and atopic dermatitis (eczema). An oral formulation of brepocitinib is being tried in the treatment of psoriatic arthritis, ulcerative colitis, Crohn’s disease, systemic lupus erythematosus, hidradenitis suppurativa, vitiligo, and alopecia areata.
- In November 2021, it became known that Pfizer had stopped developing ropsacitinib and brepocitinib on its own, giving them to an unnamed startup in which it owns a 25 percent stake.
- In late June 2022, Pfizer announced that brepocitinib and ropsacitinib will be developed by Priovant Therapeutics as part of Roivant Sciences. The oral formulation of brepocitinib is in the following clinical trials: VALOR (NCT05437263) phase 3 treatment of dermatomyositis (DM), NCT03845517 phase 2b treatment of systemic lupus erythematosus, NEPTUNE (NCT05523765) phase 2 treatment of active non-infectious non-anterior uveitis.
Johnson & Johnson and Theravance Biopharma bet on izencitinib (TD-1473) which inhibits all Janus kinases but does so exclusively locally — directly at the site of inflammation in the intestinal wall. An oral izencitinib, characterized by minimal systemic action, being tested in the treatment of ulcerative colitis and Crohn’s disease.
- In August 2021, izencitinib flopped in the RHEA (NCT03758443) phase 2b clinical trial, failing induction treatment of moderate-to-severe active ulcerative colitis. However, the safety profile of izencitinib was favorable: unlike existing JAK inhibitors, there was no typical increase in the risk of infections and thromboembolic events, and there were no clinically significant changes in laboratory findings.
- In January 2022, the DIONE (NCT03635112) phase 2 clinical trial testing isencitinib in the induction treatment of moderate-to-severe active Crohn’s disease was stopped.
In addition, Theravance is investigating TD-8236 and nezulcitinib (TD-0903), inhaled pan-Janus kinase inhibitors, against asthma and COVID-19–related acute respiratory distress syndrome (ARDS), respectively.
- In June 2021, Theravance disclosed the results of the NCT04402866 phase 2 clinical trial testing nezulcitinib in patients hospitalized with COVID-19 in order to reduce the number of days requiring respiratory support. The use of nezulcitinib did not justify itself.
Spain’s Oncostellae is checking OST-122, an inhibitor of TYK2, JAK3, and AMP-activated protein kinase 5 (ARK5, NUAK1) whose action is limited locally, in the therapy of inflammatory bowel disease including ulcerative colitis and Crohn’s disease (including with fibrosis).
In the hands of Belgium’s Galapagos is GLPG3667, TYK2 and JAK1 inhibitor, against psoriasis.
China’s InnoCare Pharma is studying ICP-332 and ICP-488, two TYK2 inhibitors. The first one binds TYK2 in the active domain (JH1) and the second in the regulatory domain (JH2).
Selective allosteric TYK2 inhibitors NDI-034858 and ESK-001 are being studied by Nimbus Therapeutics and Alumis.
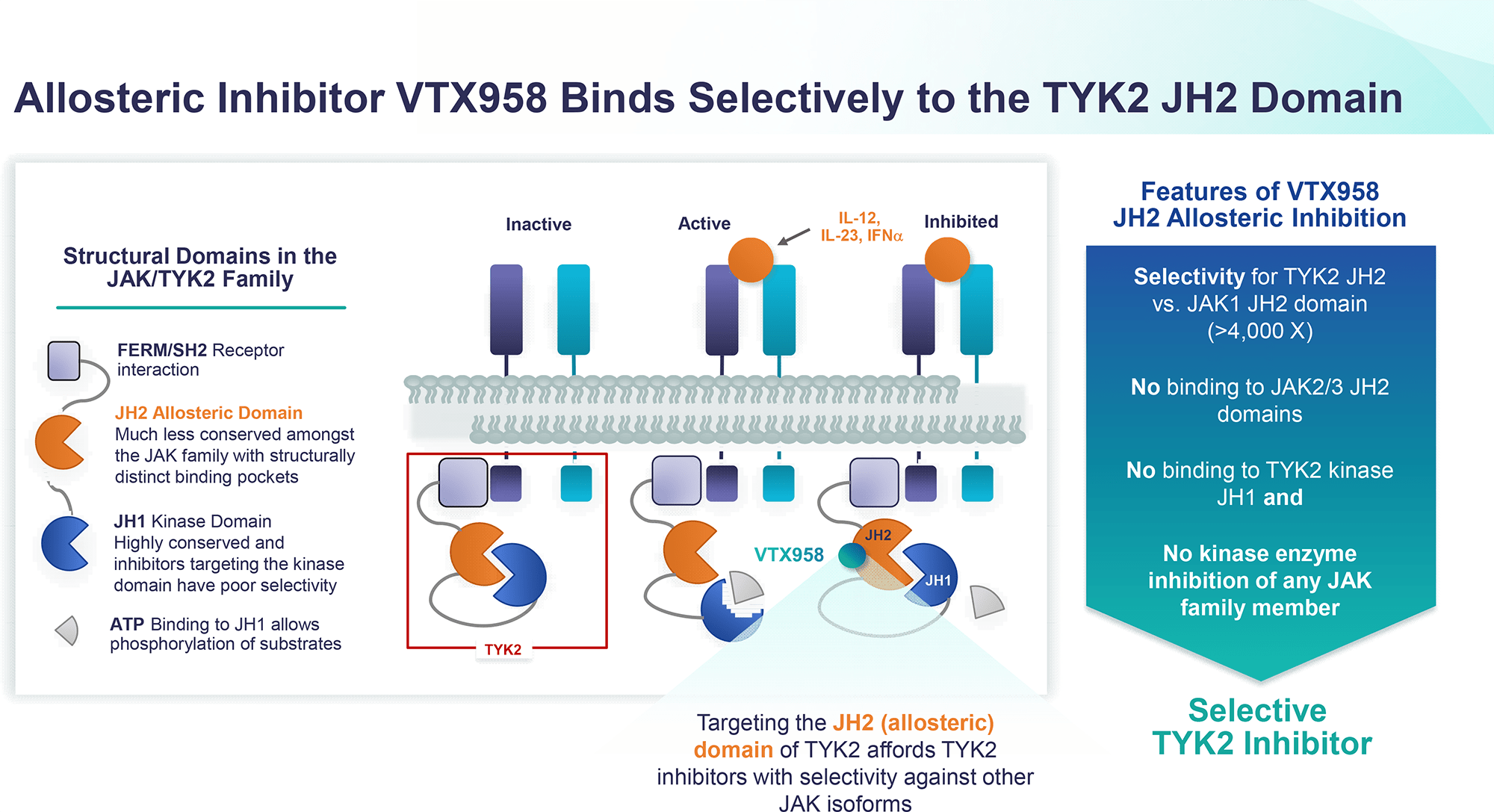
Finally, VTX958, a “pure” selective allosteric TYK2 inhibitor, was started by Ventyx Biosciences.
- In the second half of 2022, VTX958 is scheduled for launch in clinical trials in the treatment of moderate-to-severe psoriasis, psoriatic arthritis, Crohn’s disease, and other autoimmune diseases.
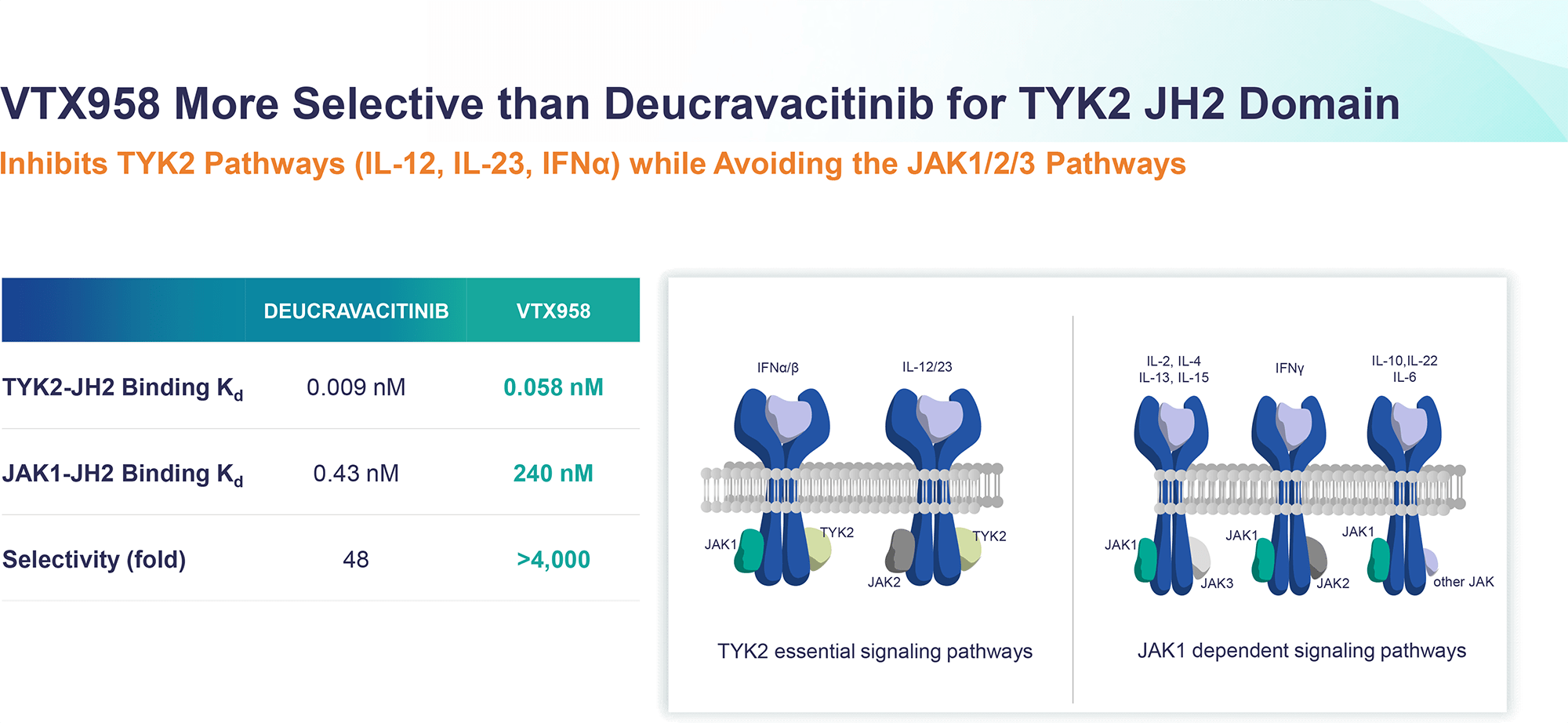
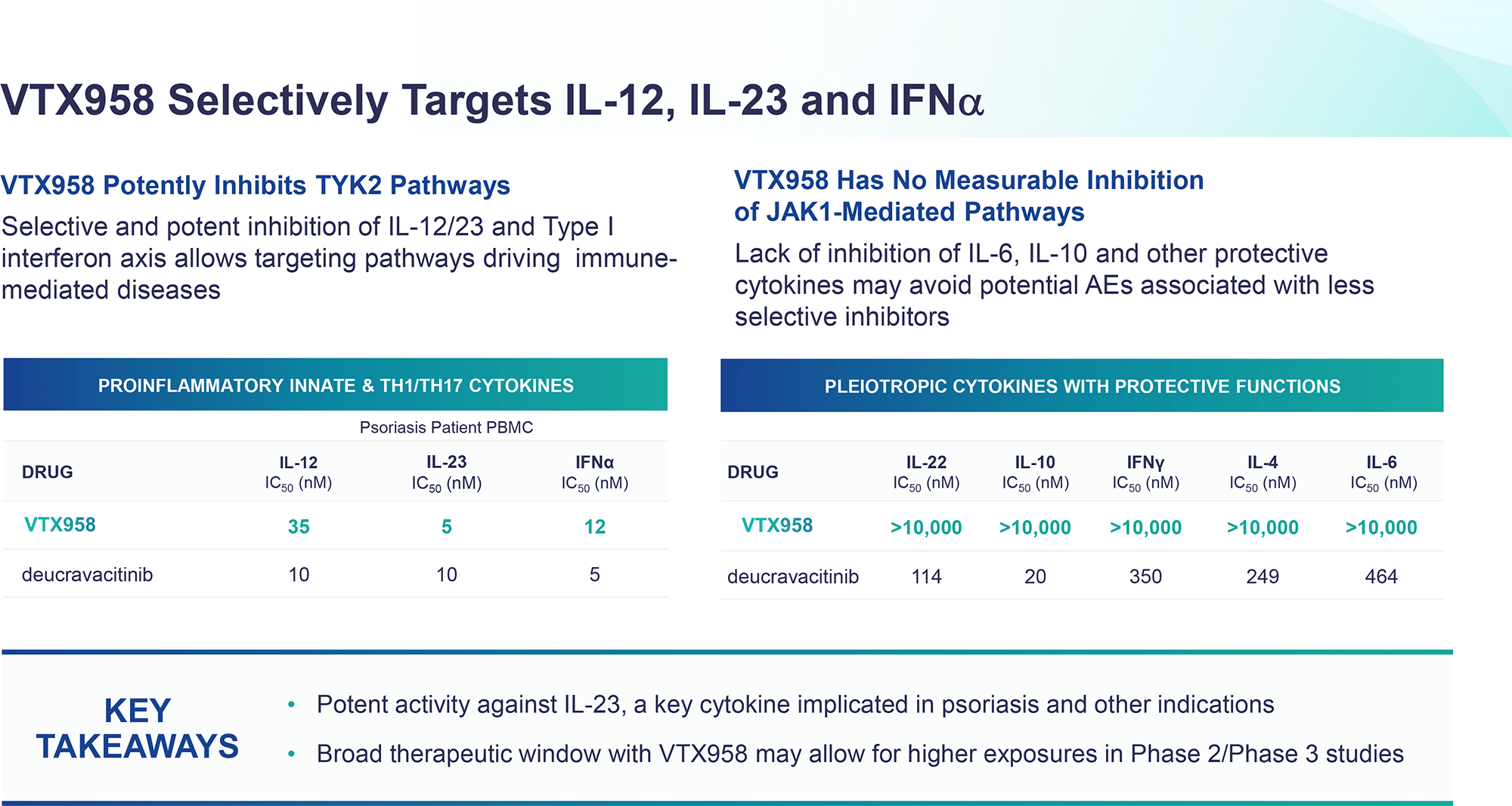
- Oral VTX958, similar to deucravacitinib, binds TYK2 in the regulatory domain (pseudokinase, JH2) rather than the active domain (catalytic, JH1), thereby not affecting the JAK1, JAK2, or JAK3 signaling pathways. At the same time, the selectivity of JH2 binding is more than 4000 times greater than that of JH1 binding, whereas for deucravacitinib this ratio is significantly lower and is 48 times greater. In other words, VTX958 is more targeted to TYK2 than deucravacitinib, resulting in a more pronounced targeted inhibition of interleukin 12 (IL-2), interleukin 23 (IL-23), and interferon type I (IFN I) signaling pathways, which are the drivers of immune-mediated diseases, without affecting other cytokines, which means that risks of unwanted side effects are mitigated. As a result, the therapeutic dose can be substantially increased, resulting in enhanced treatment efficacy without adverse events.
- Ventyx Biosciences. Corporate presentation. May 2022. [PDF]
For Further Reading
Deucravacitinib
Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: Efficacy and safety results from the 52-week, randomized, double-blinded, placebo-controlled phase 3 POETYK PSO-1 trial. J Am Acad Dermatol. 2022 Jul 9;S0190-9622(22)02256-3. [source]
Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a phase II trial in psoriatic arthritis. Ann Rheum Dis. 2022 Jun;81(6):815-822. [source]
Deucravacitinib for the treatment of psoriatic disease. Am J Clin Dermatol. 2022 Aug 12;1-10. [source]
Deucravacitinib in moderate to severe psoriasis: Clinical and quality-of-life outcomes in a phase 2 trial. Dermatol Ther (Heidelb). 2022 Feb;12(2):495-510. [source]
Lack of electrocardiographic effects of deucravacitinib in healthy subjects. Clin Pharmacol Drug Dev. 2022 Apr;11(4):442-453. [source]
Molecular and clinical effects of selective tyrosine kinase 2 inhibition with deucravacitinib in psoriasis. J Allergy Clin Immunol. 2022 Jun;149(6):2010-2020.e8. [source]
Selectivity profile of the tyrosine kinase 2 inhibitor deucravacitinib compared with Janus kinase 1/2/3 inhibitors. Dermatol Ther (Heidelb). 2021 Oct;11(5):1763-1776. [source]
The efficacy and safety of tofacitinib, peficitinib, solcitinib, baricitinib, abrocitinib and deucravacitinib in plaque psoriasis — A network meta-analysis. J Eur Acad Dermatol Venereol. 2022 May 24. [source]
TYK2
TYK2 inhibition: Changing the treatment landscape for psoriasis? Expert Rev Clin Immunol. 2022 Mar;18(3):185-187. [source]
TYK2 as a therapeutic target in the treatment of autoimmune and inflammatory diseases. Immunotherapy. 2021 Sep;13(13):1135-1150. [source]
Tyrosine kinase 2 and Janus kinase‒signal transducer and activator of transcription signaling and inhibition in plaque psoriasis. J Am Acad Dermatol. 2022 Jan;86(1):148-157. [source]
TYK 2 inhibitors for the treatment of dermatologic conditions: The evolution of JAK inhibitors. Int J Dermatol. 2022 Feb;61(2):139-147. [source]
Selective tyrosine kinase 2 inhibition for treatment of inflammatory bowel disease: New hope on the rise. Inflamm Bowel Dis. 2021 Nov 15;27(12):2023-2030. [source]
Tyrosine kinase 2 (TYK2) allosteric inhibitors to treat autoimmune diseases. J Med Chem. 2019 Oct 24;62(20):8951-8952. [source]
JAK inhibitors for treatment of psoriasis: Focus on selective TYK2 inhibitors. Drugs. 2020 Mar;80(4):341-352. [source]
Highly selective inhibition of tyrosine kinase 2 (TYK2) for the treatment of autoimmune diseases: Discovery of the allosteric inhibitor BMS-986165. J Med Chem. 2019 Oct 24;62(20):8973-8995. [source]
Highly selective inhibition of tyrosine kinase 2 (TYK2) for the treatment of autoimmune diseases: discovery of the allosteric inhibitor BMS-986165. J Med Chem. 2019 Oct 24;62(20):8973-8995. [source]
Discovery of tyrosine kinase 2 (TYK2) inhibitor (PF-06826647) for the treatment of autoimmune diseases. J Med Chem. 2020 Aug 25. [source]
Bristol-Myers Squibb
Bristol Myers Squibb. Q2 2022 Results. July 27, 2022. [PDF]
Bristol-Myers Squibb. Q4 2021 Results. February 4, 2022. [PDF]
Bristol-Myers Squibb. JP Morgan Presentation. January 10, 2022. [PDF]
Bristol-Myers Squibb. Investor Event. November 16, 2021. [PDF]
Bristol-Myers Squibb. American Academy of Dermatology (AAD). Investor presentation. April 23, 2021. [PDF]
Bristol-Myers Squibb. Investor series. Immunology & cardiovascular. June 26, 2020 [PDF]
JAK Inhibitors: Big Safety Trouble
The trend now is that the FDA has begun to look very closely at the safety profile of JAK inhibitors. And this reflects badly on the business of the pharmaceutical companies behind their development.
In early September 2021, the FDA issued a final statement indicating that all JAK inhibitors have an increased risk of serious cardiac events (cardiovascular death, nonfatal heart attack, nonfatal stroke), malignancies, thrombosis, and fatal outcomes. As a result, the regulator has only required the prescription of JAK inhibitors if patients do not respond appropriately or cannot tolerate one or more TNF blockers. The FDA was expected to find the mechanism of action of deucravacitinib to be associated with similar risks. However, this was not the case.
↓
In early April 2021, the FDA extended the review of the New Drug Application (NDA) for abrocitinib, a selective JAK1 inhibitor that Pfizer had oriented to treat moderate-to-severe atopic dermatitis. The FDA is also stalling on adding a new indication, ankylosing spondylitis, to arthritis and ulcerative colitis medicine Xeljanz (tofacitinib), a JAK1/JAK2/JAK3 inhibitor. And if expanding the range of indications of Xeljanz is important insofar as it is, in the case of abrocitinib toxicity issues play a critical role, since atopic dermatitis is considered a significantly less severe disease than ankylosing spondylitis and therefore the regulator has higher requirements for the safety profile of this new drug.
↓
In early April 2021, the FDA is not rushing to approve Olumiant (baricitinib), a JAK1/JAK2 inhibitor by Eli Lilly and Incyte, for the treatment of moderate-to-severe atopic dermatitis, although it is already cleared for this indication by the European Medicines Agency (EMA). At one time, the FDA was slowing the decision-making process for the debut of Olumiant. It took the regulator two and a half years to approve the drug, even though the therapeutic dose was halved in the end. In other words, the therapeutic efficacy was reduced in favor of a more acceptable safety profile.
↓
In mid-March 2021, the FDA delayed the verdict on Rinvoq (upadacitinib), a JAK1 inhibitor developed by AbbVie, which is used in the treatment of active moderate-to-severe rheumatoid arthritis and which wants to connect patients with active psoriatic arthritis. On the wave of news, AbbVie lost 5% of its market value, or $10 billion. Rinvoq, positioned as the savior of AbbVie’s business, largely dependent on Humira (adalimumab), which will face the arrival of biosimilars in 2023, raises concerns about its cloudless future. Upadacitinib wants to treat not only psoriatic arthritis but also atopic dermatitis and to do so with a 30-mg dose. This dose, twice as large as the one used in rheumatoid arthritis therapy, smashed Dupixent (dupilumab) by Sanofi and Regeneron Pharmaceuticals, the market leader in atopic dermatitis. However, its prescription comes with toxicity issues. At the same time, Rinvoq is considered one of the safest members of the JAK inhibitor class.
↓
In early February 2021, the FDA issued a warning about the increased risk of major adverse cardiovascular events (MACE) and malignancies with Xeljanz. The safety of Xeljanz continues to be studied and its prescribing may be associated with other risks including pulmonary embolism and mortality.
↓
In mid-December 2020, Gilead Sciences and Galapagos (Belgium) abandoned their efforts to approve Jyseleca (filgotinib) in the United States for the treatment of moderate-to-severe active rheumatoid arthritis after the FDA rejected a New Drug Application (NDA) in August 2020 due to safety concerns. Meanwhile, in late September 2020, Europe and Japan granted marketing authorization to Jyseleca for the specified indication.
JAK Inhibitors on Market
Jakafi/Jakavi (ruxolitinib)
Drug class: JAK1/JAK2 inhibitor.
Developed by Incyte and Novartis.
First approval: November 2011 (U.S.), July 2012 (Europe), July 2014 (Japan).
Jakafi/Jakavi (ruxolitinib) mechanism of action:
Therapeutic indications for ruxolitinib are as follows:
- myelofibrosis (intermediate or high risk [FDA]) including primary myelofibrosis (chronic idiopathic myelofibrosis) and secondary myelofibrosis (developed due to polycythemia vera or essential thrombocythemia)
- polycythemia vera (PV) resistant or intolerant to hydroxyurea
- graft-versus-host disease (GvHD) refractory to steroids
- chronic graft-versus-host disease (cGVHD) after failure of one or two lines of systemic therapy (FDA only).
Adverse events of ruxolitinib are as follows:
- thrombocythemia, anemia, neutropenia
- increased risk of infections
- increased risk of non-melanoma skin cancer
- laboratory abnormalities: lipid elevations.
Xeljanz (tofacitinib)
Drug class: JAK1/JAK2/JAK3 inhibitor.
Developed by Pfizer.
First approval: November 2012 (U.S.), March 2013 (Japan), March 2017 (Europe).
Xeljanz (tofacitinib) mechanism of action:
Therapeutic indications for tofacitinib are as follows:
- moderate-to-severe active rheumatoid arthritis (RA) with inadequate response or intolerance to tumor necrosis factor (TNF) blockers (FDA) or to disease-modifying antirheumatic drugs (DMARDs) [EMA]
- active psoriatic arthritis (PsA) with inadequate response or intolerance to TNF blockers (FDA) or to DMARDs (EMA)
- active ankylosing spondylitis (AS) with inadequate response or intolerance to TNF blockers (FDA) or with inadequate response to conventional therapy (EMA)
- moderate-to-severe active ulcerative colitis (UC) with inadequate response or intolerance to TNF blockers (FDA) or to either conventional therapy or a biologic agent (EMA)
- active polyarticular course juvenile idiopathic arthritis (pcJIA) with inadequate response or intolerance to TNF blockers (FDA) or to DMARDs (EMA)
- juvenile psoriatic arthritis (JPsA) with inadequate response or intolerance to DMARDs (EMA only).
Adverse events of tofacitinib are as follows:
- increased risk of serious infections (which may result in hospitalization or death) caused by bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens such as pneumonia, cellulitis, herpes zoster, urinary tract infection, diverticulitis, appendicitis, tuberculosis, cryptococcosis, histoplasmosis, esophageal candidiasis, pneumocystosis, multidermatomal herpes zoster, cytomegalovirus, BK virus (polyomavirus), listeriosis
- increased risk of lymphoma and other malignancies
- increased risk of thrombosis (sometimes fatal) including pulmonary embolism, deep venous thrombosis, and arterial thrombosis
- increased risk of death (including sudden death) in patients 50 years of age or older with rheumatoid arthritis and at least one cardiovascular risk factor
- gastrointestinal perforation
- laboratory abnormalities: leukocytosis followed by leukopenia, neutropenia, anemia, liver enzyme elevations, lipid elevations.
Olumiant (baricitinib)
Drug class: JAK1/JAK2 inhibitor.
Developed by Eli Lilly and Incyte.
First approval: February 2017 (Europe), July 2017 (Japan), May 2018 (U.S.).
Therapeutic indications for baricitinib are as follows:
- moderate-to-severe active rheumatoid arthritis (RA) with inadequate response to tumor necrosis factor (TNF) blockers (FDA) or with inadequate response or intolerance to disease-modifying antirheumatic drugs (DMARDs) [EMA]
- moderate-to-severe atopic dermatitis (EMA only)
- COVID-19 in hospitalized adults requiring supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation (ECMO)
- severe alopecia areata
Adverse events of baricitinib are as follows:
- increased risk of serious infections (which may result in hospitalization or death) caused by bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens such as pneumonia, herpes zoster, urinary tract infection, tuberculosis, multidermatomal herpes zoster, esophageal candidiasis, pneumocystosis, acute histoplasmosis, cryptococcosis, cytomegalovirus, BK virus (polyomavirus)
- increased risk of lymphoma and other malignancies
- increased risk of thrombosis (sometimes fatal) including pulmonary embolism, deep venous thrombosis, and arterial thrombosis
- gastrointestinal perforation
- laboratory abnormalities: neutropenia, lymphopenia, anemia, liver enzyme elevations, lipid elevations.
Smyraf (peficitinib)
Drug class: JAK1/JAK3 inhibitor.
Developed by Astellas Pharma (Japan).
First approval: March 2019 (Japan), January 2020 (Korea).
Therapeutic indications for peficitinib are as follows:
- rheumatoid arthritis (RA) with inadequate response to conventional therapy (Japan) or to disease-modifying antirheumatic drugs (DMARDs) [Korea].
Adverse events of peficitinib are as follows:
- increased risk of serious infections (which may result in hospitalization or death) caused by bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens such as pneumonia, nasopharyngitis, tuberculosis, herpes zoster
- increased risk of lymphoma and other malignancies
- gastrointestinal perforation
- laboratory abnormalities: neutropenia, lipid elevations.
Rinvoq (upadacitinib)
Drug class: JAK1 inhibitor.
Developed by AbbVie.
First approval: August 2019 (U.S.), November 2019 (Japan), December 2019 (Europe).
Rinvoq (upadacitinib) mechanism of action:
Therapeutic indications for upadacitinib are as follows:
- moderate-to-severe active rheumatoid arthritis (RA) with inadequate response or intolerance to tumor necrosis factor (TNF) blockers (FDA) or to disease-modifying antirheumatic drugs (DMARDs) [EMA]
- active psoriatic arthritis (PsA) with inadequate response or intolerance to TNF blockers (FDA) or to DMARDs (EMA)
- refractory moderate-to-severe atopic dermatitis with inadequate response to systemic drugs including biologics or when use of those therapies are inadvisable (FDA), moderate-to-severe atopic dermatitis (EMA)
- moderate-to-severe active ulcerative colitis (UC) with inadequate response or intolerance to TNF blockers (FDA) or to either conventional therapy or a biologic agent (EMA)
- active ankylosing spondylitis (AS, radiographic axial spondyloarthritis) with inadequate response or intolerance to TNF blockers (FDA) or with inadequate response to conventional therapy (EMA)
- active non-radiographic axial spondyloarthritis (nr-axSpA) with inadequate response to nonsteroidal antiinflammatory drugs (NSAIDs) [EMA only].
Adverse events of upadacitinib are as follows:
- increased risk of serious infections (which may result in hospitalization or death) caused by bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens such as pneumonia, cellulitis, tuberculosis, multidermatomal herpes zoster, oral/esophageal candidiasis, cryptococcosis, pneumocystosis
- increased risk of lymphoma and other malignancies
- increased risk of thrombosis (sometimes fatal) including pulmonary embolism, deep venous thrombosis, and arterial thrombosis
- gastrointestinal perforation
- laboratory abnormalities: neutropenia, lymphopenia, anemia, liver enzyme elevations, lipid elevations
- embryo-fetal toxicity.
Inrebic (fedratinib)
Drug class: JAK2 inhibitor.
Developed by Impact Biomedicines, which was bought by Celgene, which is now part of Bristol-Myers Squibb.
First approval: August 2019 (U.S.), February 2021 (Europe).
Therapeutic indications for fedratinib are as follows:
- myelofibrosis (intermediate-2 or high risk [FDA]) including primary myelofibrosis (chronic idiopathic myelofibrosis) and secondary myelofibrosis (developed due to polycythemia vera or essential thrombocythemia) [EMA — in patients who are Janus kinase (JAK) inhibitor naïve or have been treated with ruxolitinib].
Adverse events of fedratinib are as follows:
- severe and fatal encephalopathy including Wernicke’s encephalopathy due to acute thiamine (vitamin B1) deficiency
- gastrointestinal toxicity: diarrhea, nausea, vomiting
- laboratory abnormalities: anemia, thrombocytopenia, liver enzyme elevations, amylase and lipase elevations.
Jyseleca (filgotinib)
Drug class: JAK1 inhibitor.
Developed by Galapagos and Gilead Sciences.
First approval: September 2020 (Europe), September 2020 (Japan).
Jyseleca (filgotinib) mechanism of action:
Therapeutic indications for filgotinib are as follows:
- moderate-to-severe active rheumatoid arthritis (RA) with inadequate response or intolerance to disease-modifying antirheumatic drugs (DMARDs) [EMA] or to conventional therapy (Japan)
- moderate-to-severe active ulcerative colitis (UC) with inadequate response, lost response, or intolerance to either conventional therapy or a biologic agent (EMA) or with inadequate response to conventional therapy (Japan)
Adverse events of filgotinib are as follows:
- increased risk of serious infections (which may result in hospitalization or death) caused by bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens such as upper respiratory tract infection, pneumonia, urinary tract infection, tuberculosis, herpes zoster, oesophageal candidiasis, cryptococcosis
- increased risk of lymphoma and other malignancies
- increased risk of thrombosis (sometimes fatal) including pulmonary embolism, deep venous thrombosis, and arterial thrombosis
- embryo-fetal toxicity
- increased risk of reduction in male reduced fertility or infertility (possibly irreversible): impaired spermatogenesis and histopathological effects on male reproductive organs
- laboratory abnormalities: creatine phosphokinase elevations, lipid elevations.
Cibinqo (abrocitinib)
Drug class: JAK1 inhibitor.
Developed by Pfizer.
First approval: September 2021 (Japan), December 2021 (Europe), January 2022 (U.S.)
Cibinqo (abrocitinib) mechanism of action:
Therapeutic indications of abrocitinib are as follows:
- refractory moderate-to-severe atopic dermatitis with inadequate response to systemic drugs including biologics or when use of those therapies are inadvisable (FDA only)
- moderate-to-severe atopic dermatitis (EMA), moderate-to-severe atopic dermatitis with inadequate response to existing therapies (Japan).
Adverse events of abrocitinib are as follows:
- increased risk of serious infections (which may result in hospitalization or death) caused by bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens such as herpes simplex, herpes zoster, and pneumonia
- increased risk of malignancies
- increased risk of thrombosis (sometimes fatal) including pulmonary embolism, deep venous thrombosis, and arterial thrombosis
- laboratory abnormalities: creatine phosphokinase elevations, lipid elevations.
Opzelura (ruxolitinib)
Drug class: JAK1/JAK2 inhibitor.
Developed by Incyte.
First approval: September 2021 (U.S.).
Opzelura (ruxolitinib) mechanism of action:
Therapeutic indications for ruxolitinib (in topical formulation) are as follows:
- mild-to-moderate atopic dermatitis with inadequate response to topical prescription therapies or when use of those therapies are inadvisable
- nonsegmental vitiligo
Adverse events of ruxolitinib are as follows:
- increased risk of serious infections (which may result in hospitalization or death) caused by bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens
- increased risk of lymphoma and other malignancies
- increased risk of thrombosis (sometimes fatal) including pulmonary embolism, deep venous thrombosis, and arterial thrombosis
- higher rate of all-cause mortality, including sudden cardiovascular death
- higher rate of major adverse cardiovascular events (MACE) defined as cardiovascular death, non-fatal myocardial infarction, and non-fatal stroke
- laboratory abnormalities: thrombocytopenia, anemia, neutropenia, lipid elevations.
There is also the veterinary drug Apoquel (oclacytinib), a JAK1 inhibitor promoted by Zoetis (formerly Pfizer). The drug is intended for dogs to treat atopic dermatitis and pruritus due to allergic dermatitis.