Highlights
Kimmtrak (tebentafusp) is a new drug indicated for the treatment of unresectable or metastatic uveal melanoma in HLA-A*02:01-positive adult patients.
Kimmtrak, developed by UK-based Immunocore, is approved by the U.S. Food and Drug Administration (FDA).
The introduction of Kimmtrak is a historic milestone and the culmination of pharmacological science that was able to break the one-year life barrier exhibited by patients after uveal melanoma metastasized as the deadliest form of intraocular cancer.
Kimmtrak became the first approved drug to address T-cell receptor technology (TCR).
In the United States, Kimmtrak is priced at $18,760 per dose. Taking into account, first, the need for a weekly dose of the drug and, second, treatment for a median of 5.3 months, the final cost of Kimmtrak therapy for metastatic uveal melanoma is approximately $400,000.

Features of Uveal Melanoma
Uveal melanoma, the most common intraocular cancer in adults, accounts for approximately 3-5% of all melanoma cases. [1] Although uveal melanoma arises from melanocytes, it differs from cutaneous melanoma by having different molecular factors and metastatic patterns, as well as a different tumor-immune microenvironment. [1] [2] [3] [4] These differences are thought to contribute to the lack of clinical response to systemic treatment, including immune checkpoint inhibitors. [5] [6]
Up to half of patients with uveal melanoma experience metastases that develop predominantly in the liver, [7] [8] [9] [10] and the prognosis in such patients is very poor: median overall survival is about 1 year. [6] [11] Remarkably, metastasis can also begin more than 10 years after treatment of the primary tumor, which is why patients should not be considered cured even after a very long follow-up interval. [12]
There is no evidence to suggest improved survival with systemic therapy.
What Is ImmTAC
Immunocore’s know-how is represented by the so-called Immune Mobilizing Monoclonal T-cell receptors Against Cancer (ImmTAC). This is a new class of bispecific fusion proteins that redirect T cells to complexes consisting of a peptide and human leukocyte antigen (HLA). [1] [2]
The architecture of the ImmTAC molecule includes an engineered high-affinity soluble T-cell receptor (TCR) and a single-chain variable fragment (scFv) of anti-CD3 antibody.
Once ImmTAC molecules bind to their specific peptide–HLA (pHLA) complexes on the target cell surface, they recruit and activate polyclonal T cells via CD3 to release inflammatory cytokines and cytolytic mediators directed against target cells.
Since most proteins are processed and presented on the cell surface as a pHLA complex, ImmTAC molecules can in principle be engineered to target almost the entire proteome.
Endowing TCRs with high affinity is necessary in order to multiply the affinity for pHLA complexes since cancer cells can present too few of them.
Kimmtrak: Mechanism of Action of Tebentafusp
Tebentafusp (IMCgp100) consists of a soluble TCR with increased affinity for glycoprotein 100 (gp100), which is HLA-A*02:01-presented on the surface of uveal melanoma tumor cells, and scFv anti-CD3. The gp100 protein is a tumor-associated antigen (TAA) that is highly expressed by melanoma cells, weakly by normal melanocytes, and minimally by other tissues.
To be precise, the highly specific TCR targets not gp100 itself, which is an intracellular peptide, but the nine-amino acid peptide YLEPGPVTA, which is formed as a result of proteasome degradation of gp100 and which is represented on the cell surface by HLA molecules.
After intravenous injection of tebentafusp, its TCR motif targets and binds to gp100 on uveal melanoma tumor cells, and the anti-CD3 motif binds to CD3-expressing T lymphocytes. This leads to selective cross-linking of tumor cells and T cells. Cytotoxic T-lymphocytes (CTL) are recruited to the resulting aggregates (which actually mimic natural immune synapse) mediating the death of malignant cells. [1] [2] [3]
Tebentafusp is suitable for the treatment of approximately half of patients with metastatic uveal melanoma because HLA-A*02:01 (HLA-A serotype 02:01 allele), according to genotyping, is found in 45% of US and European residents.

Aura Biosciences: Anticancer Virus-Like Drug Conjugates
A new class of oncology drugs with a dual mechanism of action.
Kimmtrak: Efficacy and Safety of Tebentafusp in Metastatic Uveal Melanoma Treatment
The IMCgp100-202 (NCT03070392) phase 3 (randomized, open-label, multicenter, international) clinical trial enrolled adult patients (n=378) with previously untreated metastatic uveal melanoma.
Subjects had to have the HLA-A*02:01 genotype.
Exclusion criteria included prior systemic therapy for metastatic or advanced uveal melanoma or localized liver-directed therapy, clinically serious cardiac disease, symptomatic or untreated brain metastases.
Main patient characteristics were as follows: median age 64 years (23–92), 50% female, 36% had elevated lactate dehydrogenase levels, and 94% had liver metastases.
Participants were given Kimmtrak or the investigator’s choice of drug (pembrolizumab, ipilimumab, or dacarbazine) until disease progression or unacceptable toxicity.
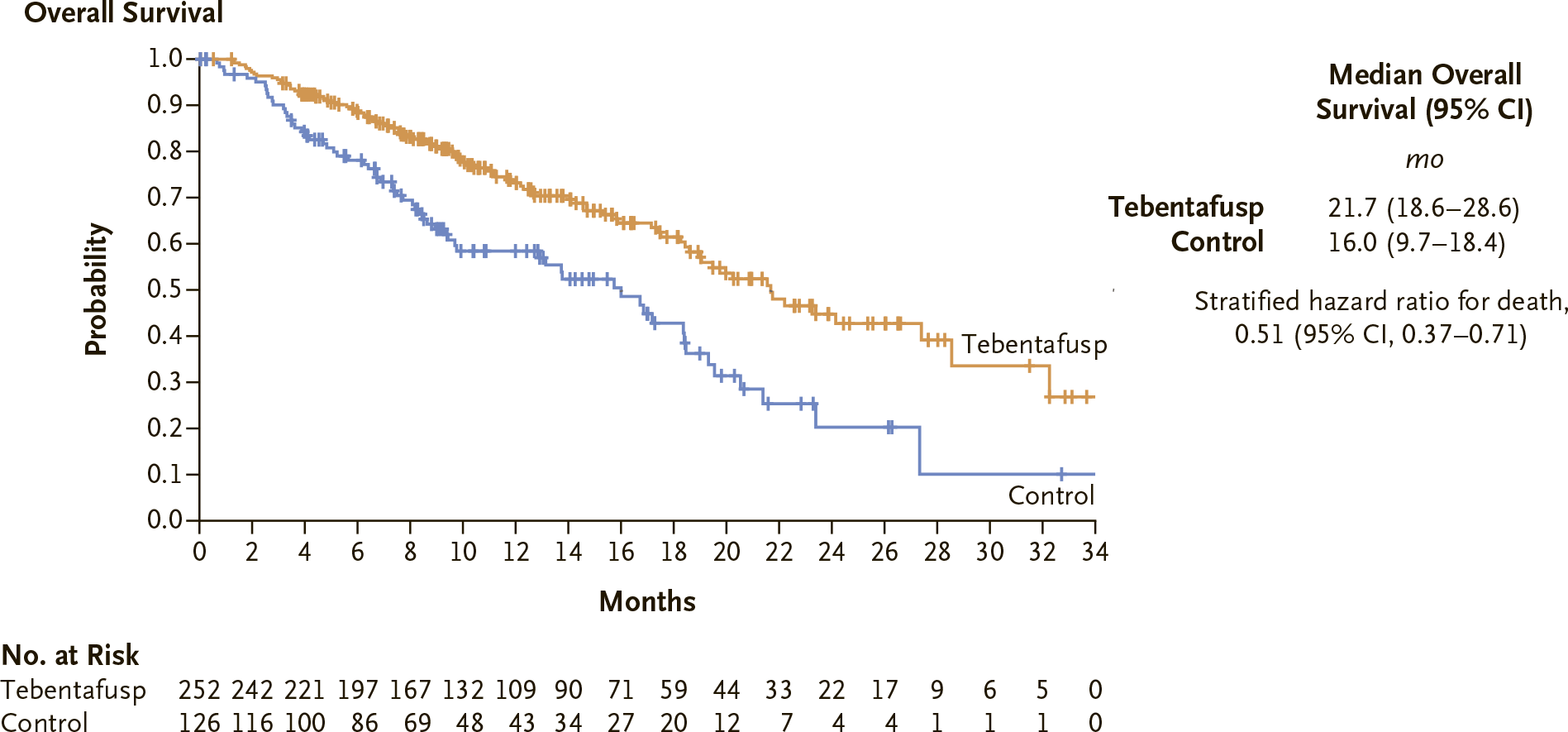
According to the first interim analysis of data collected over a median follow-up period of 14.1 months, the estimated median overall survival (OS) was 21.7 months (95% CI: 18.6–28.6) in the tebentafusp group — versus 16.0 months (95% CI: 9.7–18.4) in the control group. Kimmtrak use against metastatic uveal melanoma reduced the risk of death by 49%: hazard ratio (HR) 0.51 (95% CI: 0.37–0.71; p<0.0001).
The estimated 12-month survival rate came out to 73% (95% CI: 66–79) — vs. 59% (95% CI: 48–67).
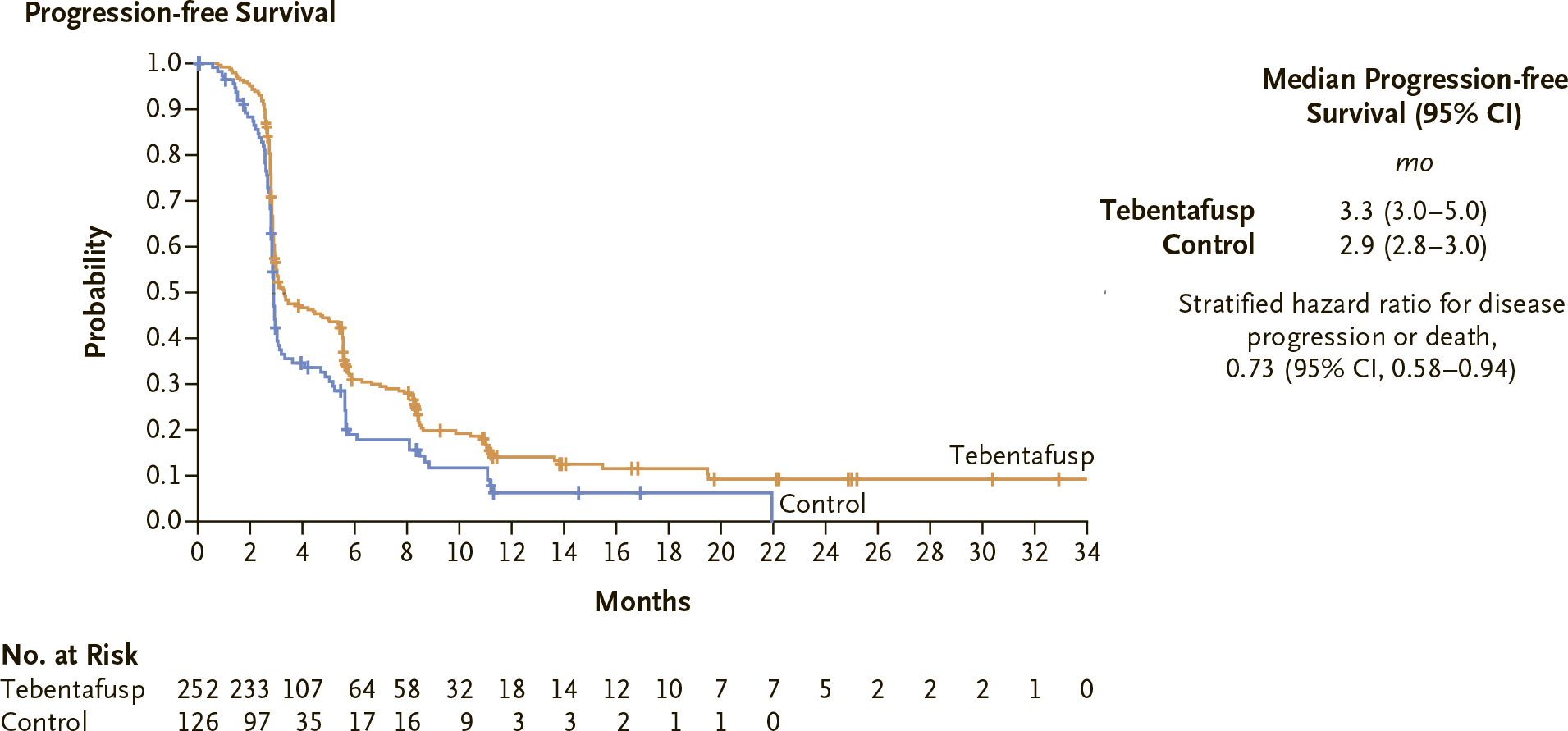
The median progression-free survival (PFS) was 3.3 months (95% CI: 3.0–5.0) — vs. 2.9 months (95% CI: 2.8–3.0). Treatment of metastatic uveal melanoma with Kimmtrak reduced the risk of death or disease progression by 27%: HR 0.73 (95% CI: 0.58–0.94; p=0.0139).
The estimated PFS rate at 6 months in the tebentafusp group was 31% — vs. 19%.
The overall response rate (ORR) was recorded at 9.1% (95% CI: 5.9–13.4) including 0.4% complete response (CR) and 8.7% partial response (PR) — vs. 4.8% (95% CI: 1.8–10.1), including CR 0% and PR 4.8%.
The median duration of response (DoR) was 9.9 months — vs. 9.7 months.
The proportion of patients who had disease control (complete response, partial response, or stable disease for 12 weeks or more) was higher in the tebentafusp group: 46% (95% CI: 39–52) —vs. 27% (95% CI: 20–36).
The prescribing information for Kimmtrak comes with a black-boxed warning about the risks of cytokine release syndrome (CRS), which can be serious or life-threatening. Appropriate monitoring for a minimum of 16 hours after the first three doses of Kimmtrak and then as clinically indicated is recommended.
The most common adverse reactions to tebentafusp administration include: decreased lymphocyte count (91%), increased creatinine (87%), cytokine release syndrome (89%), rash (83%), itching (69%), pyrexia (71%), increased glucose (66%), fatigue (64%), decreased hemoglobin (51%), nausea (49%), chills (48%), edema (45%), abdominal pain (45%).
Extras
Kimmtrak (tebentafusp). Prescribing information. U.S. [PDF]
Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma. N Engl J Med. 2021 Sep 23;385(13):1196-1206. [source]
Gp-100 as a novel therapeutic target in uveal melanoma. Cancers (Basel). 2021 Nov 27;13(23):5968. [source]
Tebentafusp, A TCR/anti-CD3 bispecific fusion protein targeting gp100, potently activated antitumor immune responses in patients with metastatic melanoma. Clin Cancer Res. 2020 Nov 15;26(22):5869-5878. [source]
Tebentafusp: T cell redirection for the treatment of metastatic uveal melanoma. Cancers (Basel). 2019 Jul 11;11(7):971. [source]
Novel TCR-based biologics: mobilising T cells to warm ‘cold’ tumours. Cancer Treat Rev. 2019 Jul;77:35-43. [source]
Polyfunctional response by ImmTAC (IMCgp100) redirected CD8 + and CD4 + T cells. Immunology. 2017 Nov;152(3):425-438. [source]
ImmTAC-redirected tumour cell killing induces and potentiates antigen cross-presentation by dendritic cells. Cancer Immunol Immunother. 2014 May;63(5):437-48. [source]
Monoclonal TCR-redirected tumor cell killing. Nat Med. 2012 Jun;18(6):980-7. [source]