Highlights
Merck & Co. has developed enlicitide chloride (MK-0616), a new drug for lowering low-density lipoprotein (LDL) cholesterol for the treatment and prevention of atherosclerosis.
Enlicitide promises to be a blockbuster. First, it is safe. Second, the drug is made in an easy-to-use oral formulation. Third, enlicitide lowers ‘bad’ cholesterol levels significantly more than all other pills on the market, including bile acid sequestrants, statins, ezetemibe, and bempedoic acid. Fourth, enlicitide is as effective as powerful and expensive injectable LDL cholesterol–lowering drugs such as Praluent (alirocumab), Repatha (evolocumab) and Leqvio (inclisiran).
The demand for enlicitide is expected to be huge due to the fact that the whole world really wants to defeat atherosclerosis as one of the most important causes of cardiovascular diseases, especially coronary artery disease (CAD).
Enlicitide has yet to undergo an extensive clinical trials in hundreds and thousands of patients to be finally convinced of its safety and efficacy.
If everything turns out to be successful, the finished medicine will appear on the market approximately in 2026.
Enlicitide: Mechanism of Action
Low-density lipoprotein (LDL) is one of the five major groups of lipoproteins that transport all fat molecules throughout the body in extracellular water. LDL delivers fat molecules to cells and is involved in the development of atherosclerosis, a process in which fat is oxidized in the artery walls [1].
The low-density lipoprotein receptor (LDLR) is a mosaic protein that mediates endocytosis of cholesterol-enriched LDL. The LDL receptors are the primary receptors for transport of LDL from the systemic bloodstream into cells, each LDLR transports 3,000 to 6,000 fat molecules including cholesterol [2].
Once the LDLR is internalized, it dissociates from its ligand and returns to the cell surface. The LDL receptor makes a similar journey to and from the cell every 10 minutes, totaling several hundred trips over its 20-hour life span. Since each LDL particle contains approximately 1600 cholesterol molecules, this rapid recirculation of LDLR provides an efficient mechanism for cholesterol delivery to cells [3] [4] [5] [6].
In other words, LDL receptors maintain homeostatic levels of LDL in plasma. The liver is responsible for eliminating approximately 70% of circulating LDL. The more extensive the available pool of LDLR, the more efficient the cholesterol transport and the lower its concentration in plasma.
According to the lipid hypothesis (also known as the cholesterol hypothesis), lowering blood cholesterol levels leads to a reduced risk of cardiovascular diseases [7] [8] [9] [10] [11] [12].
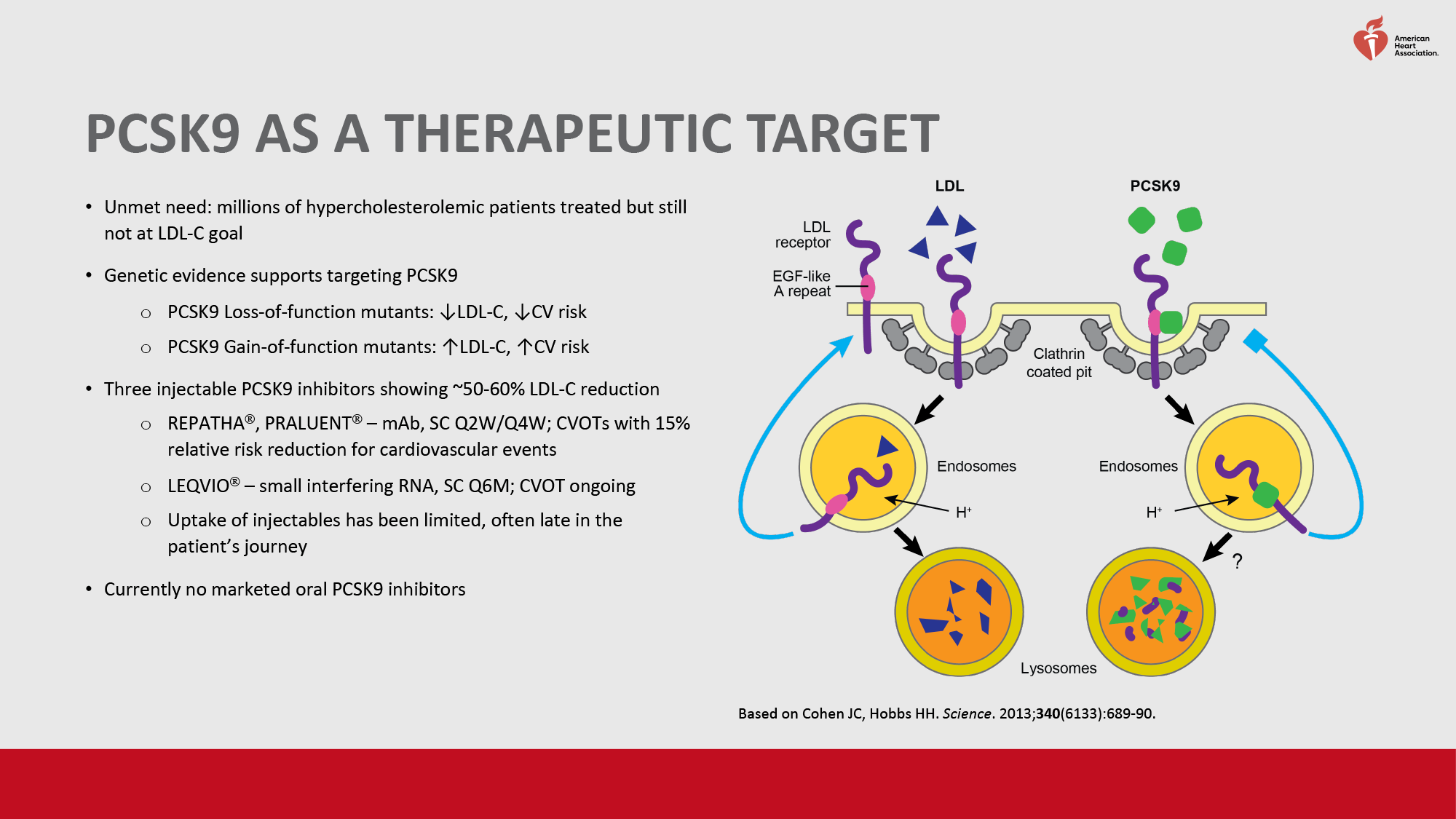
Proprotein convertase subtilisin/kexin type 9 (PCSK9) is one of the most important regulators of LDL cholesterol metabolism. This enzyme binds to LDL receptors located on the surface of hepatocytes. As a result, LDLRs, instead of following their physiologic path of recycling back to the hepatocyte membrane, are redirected to lysomal degradation in the liver. As the pool of free LDL receptors is reduced, plasma LDL cholesterol levels increase [13] [14] [15].
PCSK9 also inhibits intracellular degradation of apolipoprotein B (ApoB), a protein that is a component of LDL and very low density lipoprotein (VLDL) particles [16] [17] [18]. High ApoB levels are associated with high concentrations of LDL particles and are a reliable indicator of cardiovascular disease [19] [20] [21].
Therapeutic blockade of PCSK9 should reduce the plasma concentration of LDL particles transporting cholesterol [22]. Again, according to genetic studies, loss-of-function PCSK9 mutations result in lifelong low cholesterol levels and markedly reduced risk of atherosclerotic cardiovascular disease (ASCVD) [23] [24] [25] [26].
Merck & Co. has set a strategic goal of developing an oral PCSK9 inhibitor that lowers LDL cholesterol at levels equivalent to those provided by the approved monoclonal antibodies Praluent (alirocumab) and Repatha (everocumab).
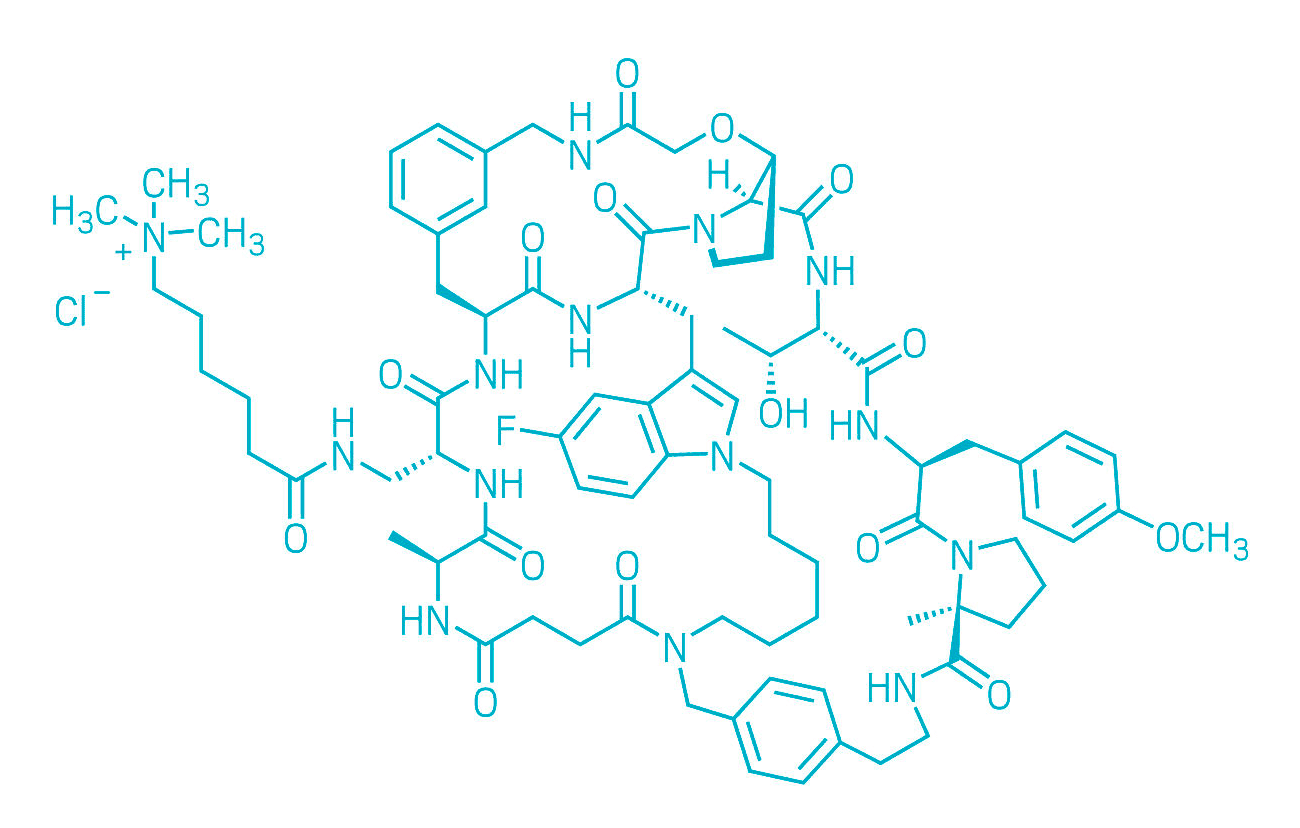
Oral enlicitide chloride (MK-0616) is a synthetic macrocyclic (tricyclic) peptide that performs orthosteric blocking of protein-protein interaction between PCSK9 and LDL receptor. Enlicitide binds to a large flat binding surface on PCSK9, thereby preventing the latter from binding to the LDL receptor. The outcome is an increase in the pool of LDL receptors available for LDL cholesterol clearance [27] [28] [29].
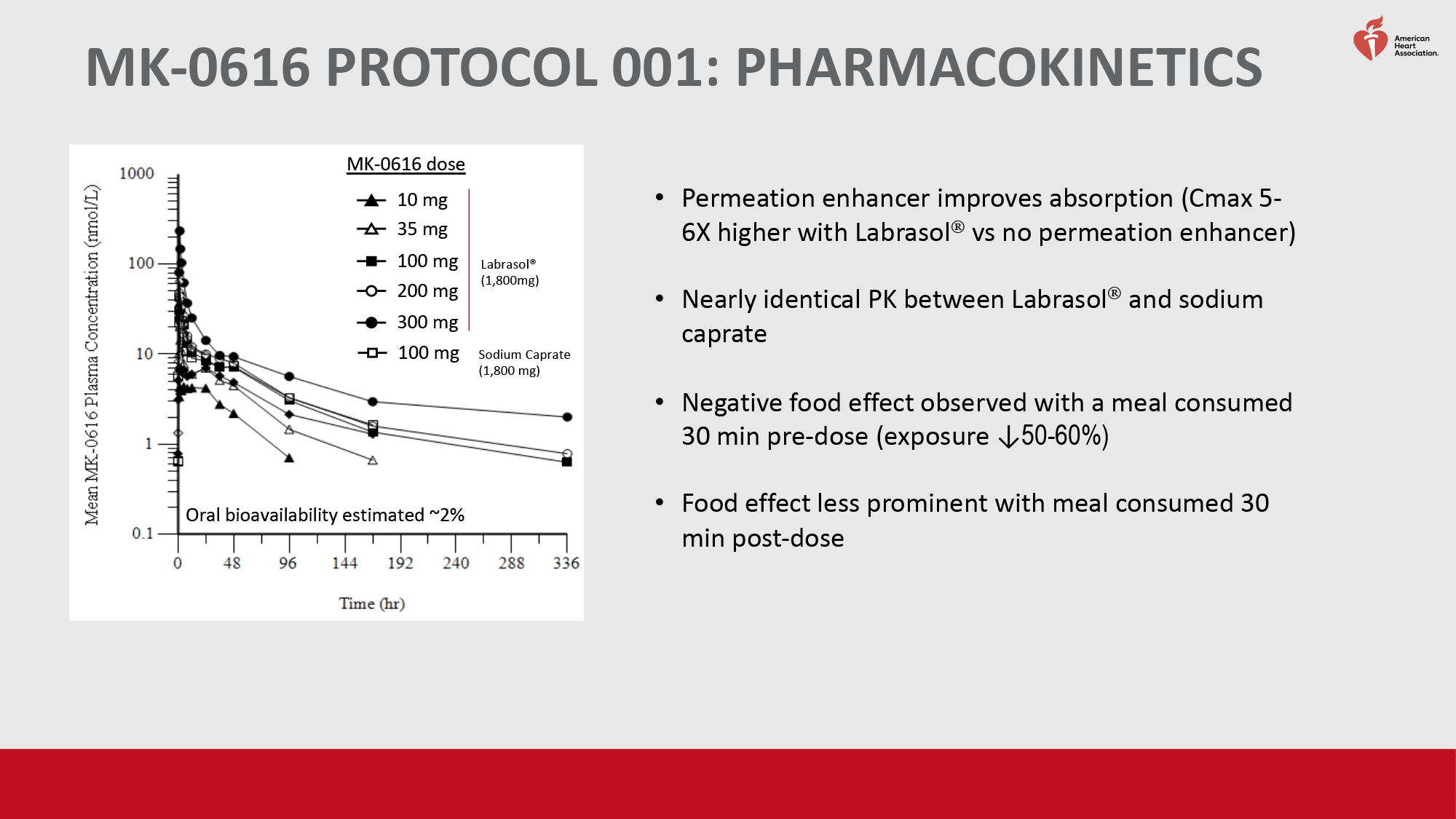
The molecule is characterized by high target binding potency: the affinity is similar to that of monoclonal antibodies against PCSK9. The gastrointestinal absorption of enlicitide is significantly improved by the use of the permeability enhancer sodium caprate.
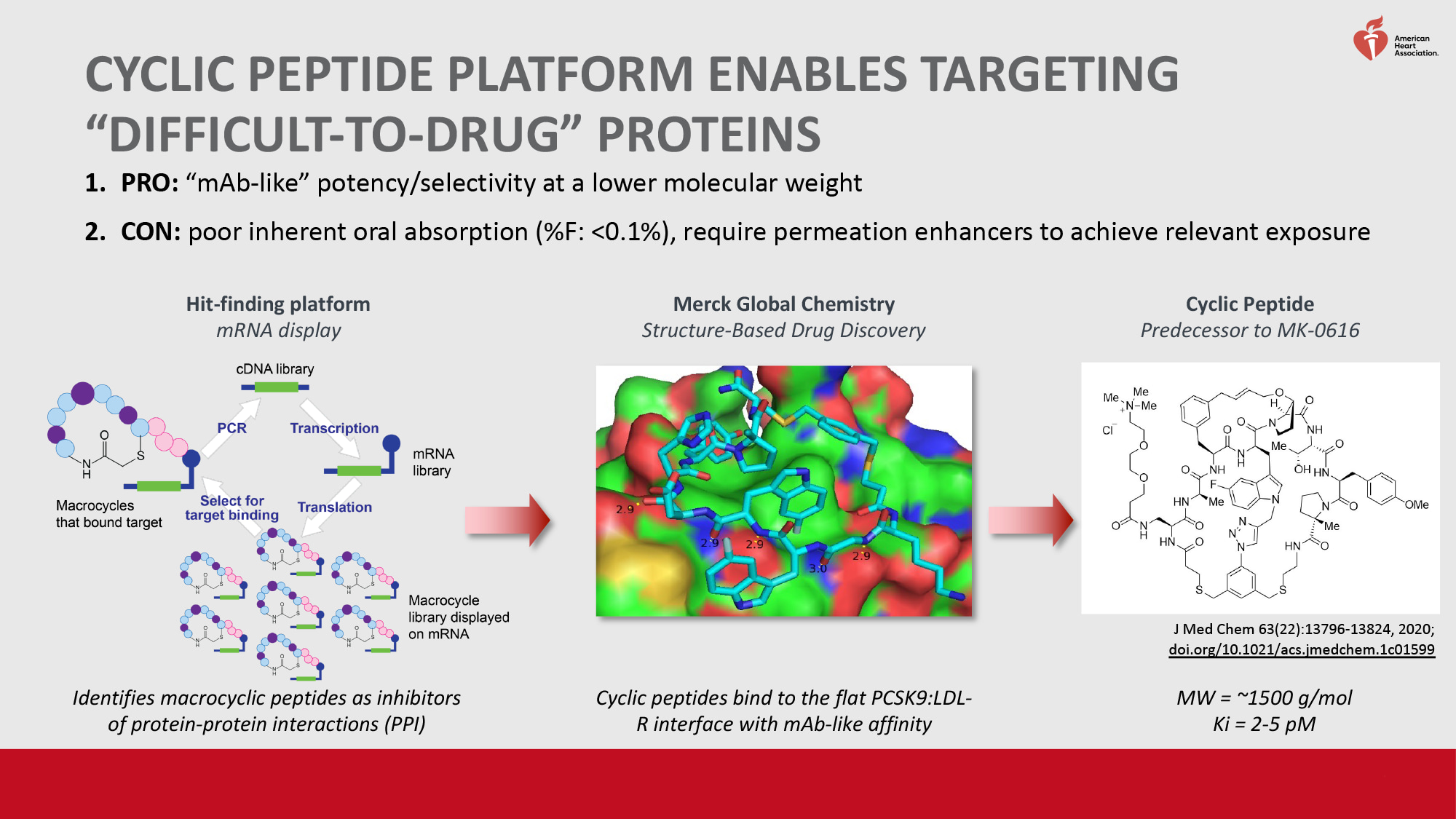
Enlicitide was developed through a partnership formalized in April 2013 between Merck & Co. and Ra Pharmaceuticals, which provided access to the proprietary cyclomimetic platform and which was acquired by Belgium’s UCB in April 2020.
Enlicitide: Details of Clinical Evaluation
Early-Stage Studies
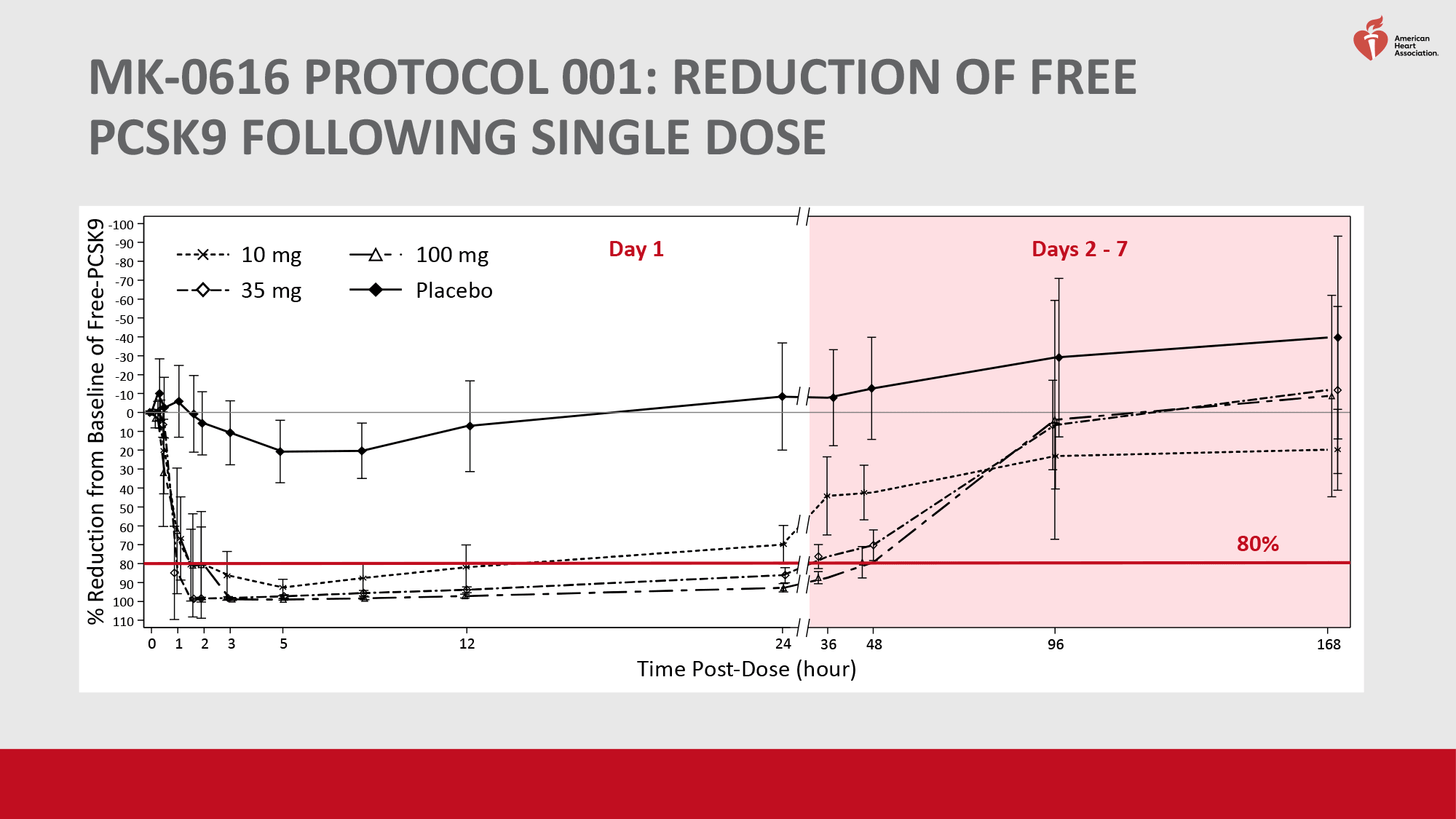
The first clinical trial included healthy men (n=60) randomized to receive enlicitide (MK-0616) daily at a dose of 10 to 300 mg or placebo. Administration of the experimental drug resulted in a reduction in proprotein convertase subtilisin/kexin type 9 (PCSK9) levels by more than 90% from baseline, and regardless of MK-0616 dose.
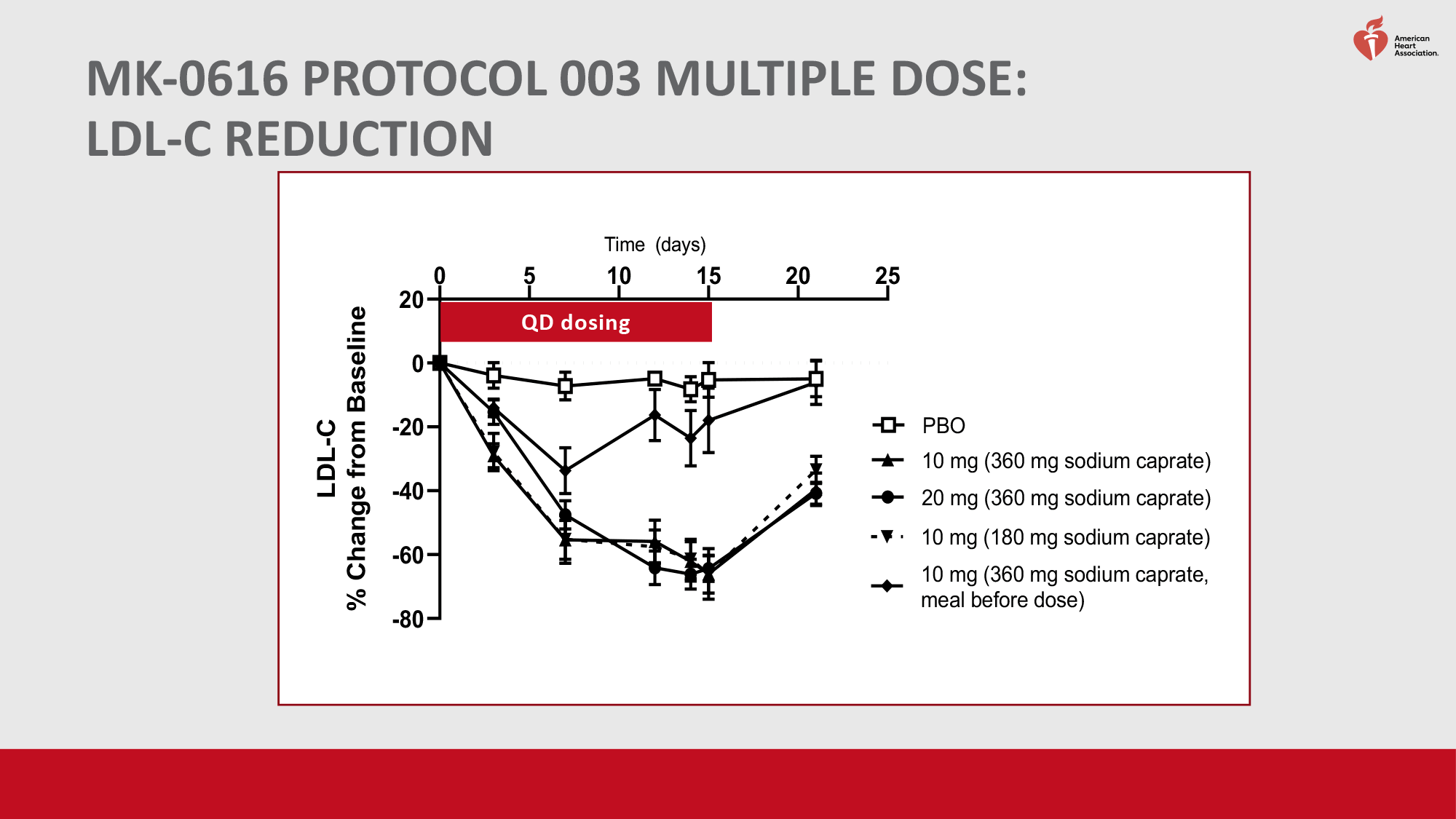
The second clinical trial enrolled men and women (n=40) with high low-density lipoprotein (LDL) cholesterol levels who were already adhering to statin therapy. Participants were administered MK-0616 daily at a dose of 10 or 20 mg or placebo. After 14 days of treatment, enlicitide provided a 65% reduction in LDL cholesterol levels from baseline. In the placebo group, the reduction was less than 5%.
The safety profile of enlicitide was favorable. Daily doses of the drug up to 300 mg did not lead to any serious adverse events.
Mid-Stage Study
The NCT05261126 phase 2b (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial invited adult patients (n=380) with hypercholesterolemia.
Key participant characteristics included: median age 62 years, 49% female; mean low-density lipoprotein (LDL) cholesterol level was 119.5 mg/dL; 39% had atherosclerotic cardiovascular disease (ASCVD) in clinical form, 56% had intermediate or high risk ASCVD, and 5% had borderline risk ASCVD; 39%, 35%, and 26% were not taking statins, were on low- or moderate-intensity statin therapy, and were on high-intensity statin therapy, respectively.
Subjects were administered either enlicitide (MK-0616) at a dose of 6 mg, 12 mg, 18 mg, or 30 mg or placebo daily.
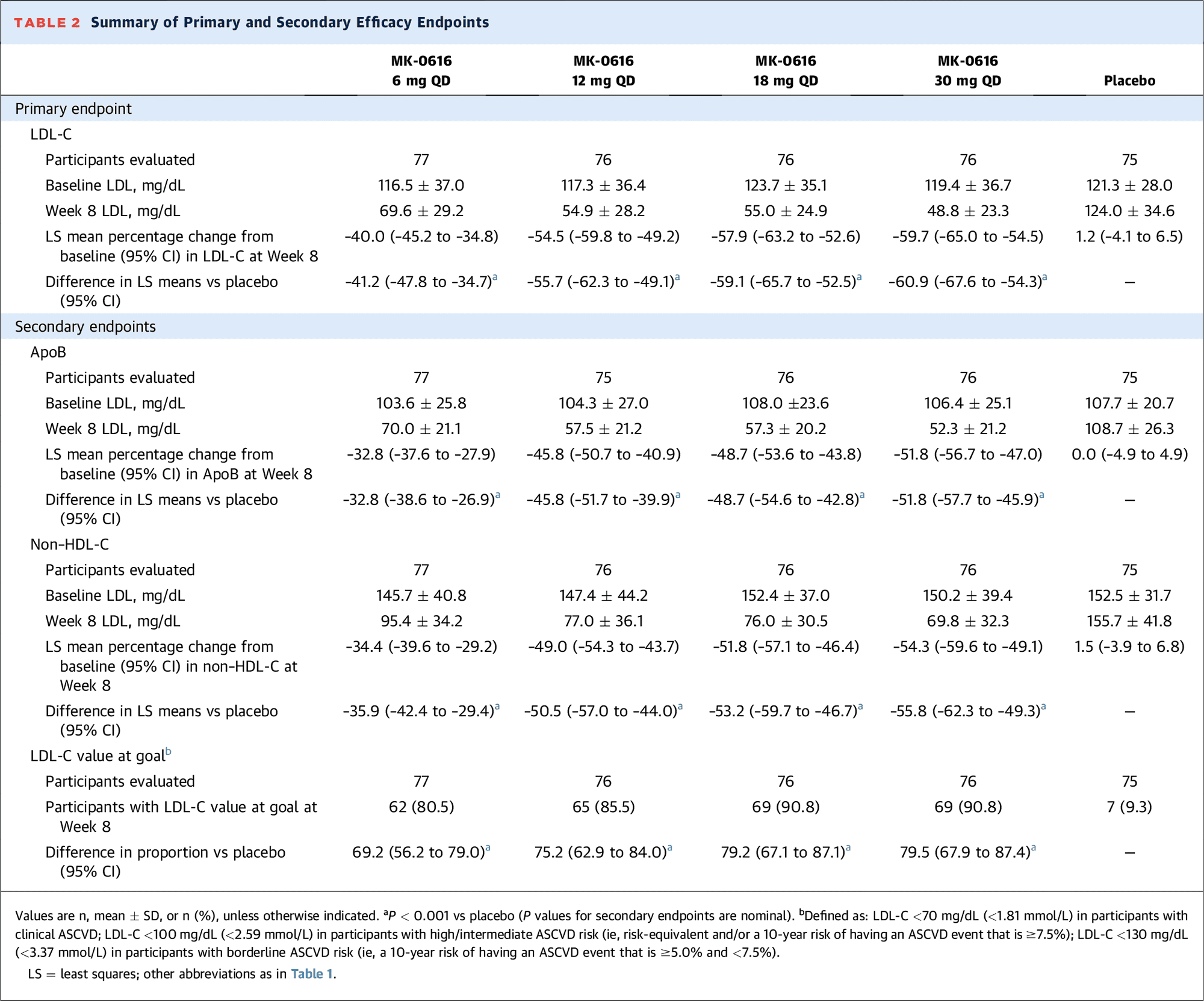
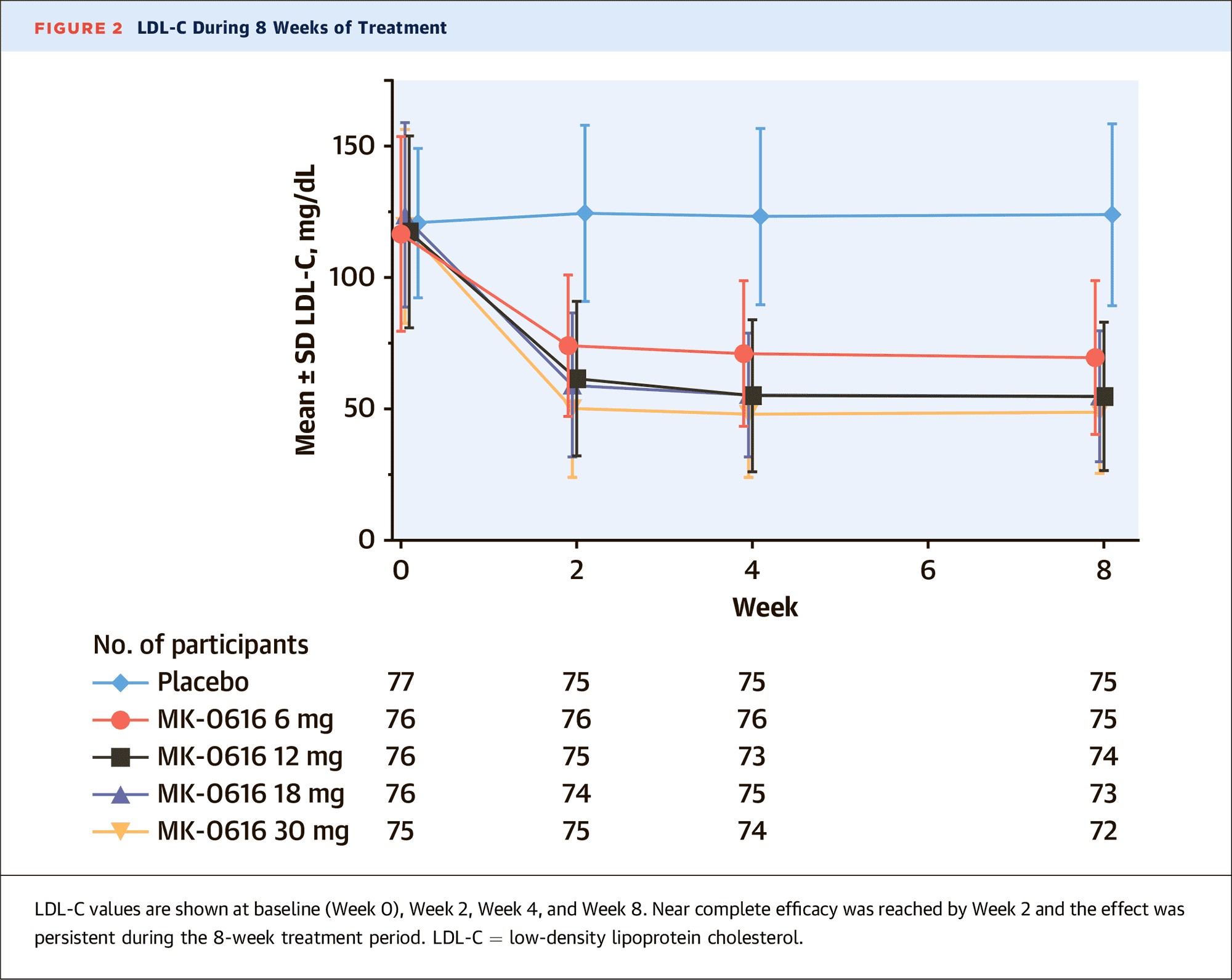
The primary endpoint of treatment efficacy was the percentage change in LDL cholesterol levels.
After 8 weeks, the 6-mg, 12-mg, 18-mg, and 30-mg enlicitide subgroups showed decreases in LDL cholesterol levels of 40%, 55%, 58%, and 60% — versus increases of 1.2% in the placebo group.
The corresponding difference, adjusted for placebo, was statistically significant (p<0.001) and was −41%, −56%, −59%, and −61%.
The target LDL cholesterol levels, calculated according to the risk of ASCVD, were reached by 81%, 86%, 91%, and 91% of patients — vs. 9% in the control group.
Among other beneficial effects of enlicitide in the treatment of hypercholesterolemia, which were mirrored by a significant change, relative to placebo, in the levels of other metabolic parameters that act as important predictors of atherogenic risk:
- apolipoprotein B (ApoB): −33%, −46%, −49%, −52%
- non-high-density lipoprotein (non-HDL) cholesterol: −36%, −51%, −53%, −56%
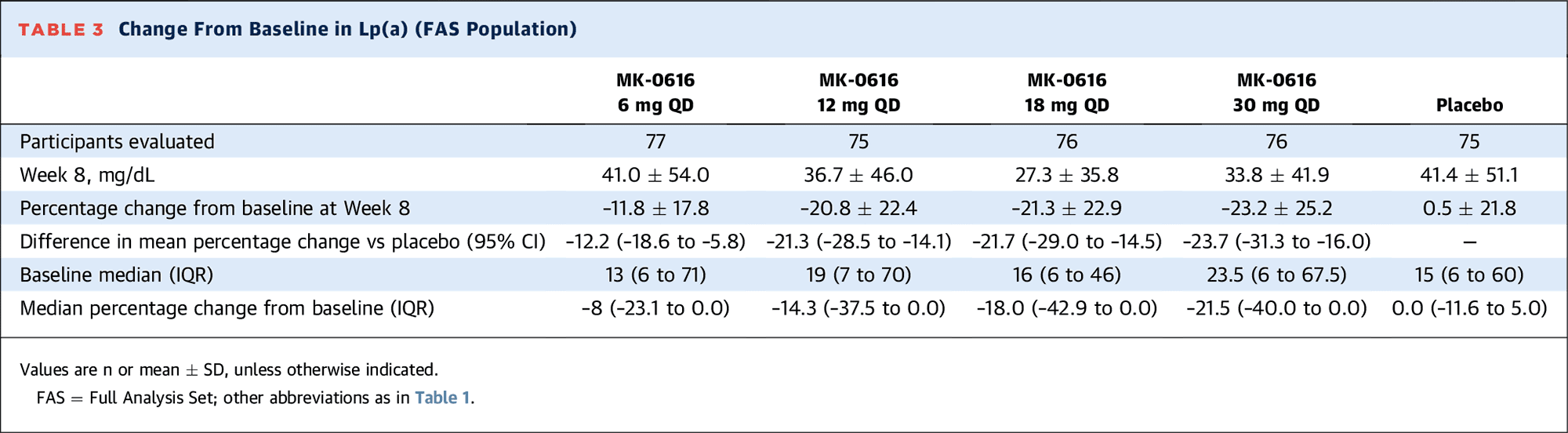
- lipoprotein (a) [Lp(a)]: −12%, −21%, −22%, −24%
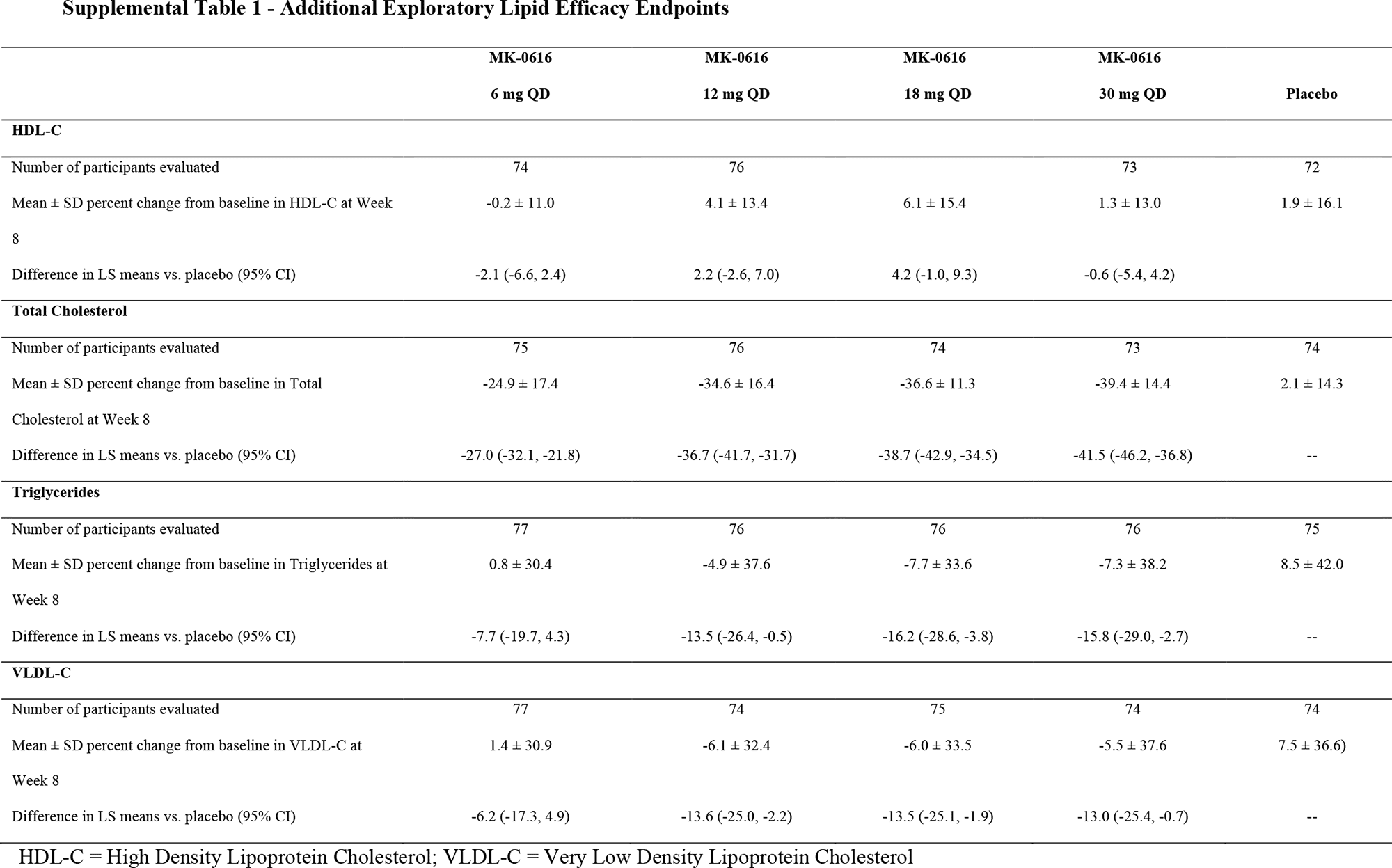
- high-density lipoprotein (HDL) cholesterol: −2%, +2%, +4%, −1%
- total cholesterol: −27%, −37%, −39%, −42%
- triglycerides: −8%, −14%, −16%, −16%
- very-low-density lipoprotein (VLDL) cholesterol: −6%, −14%, −14%, −13%.
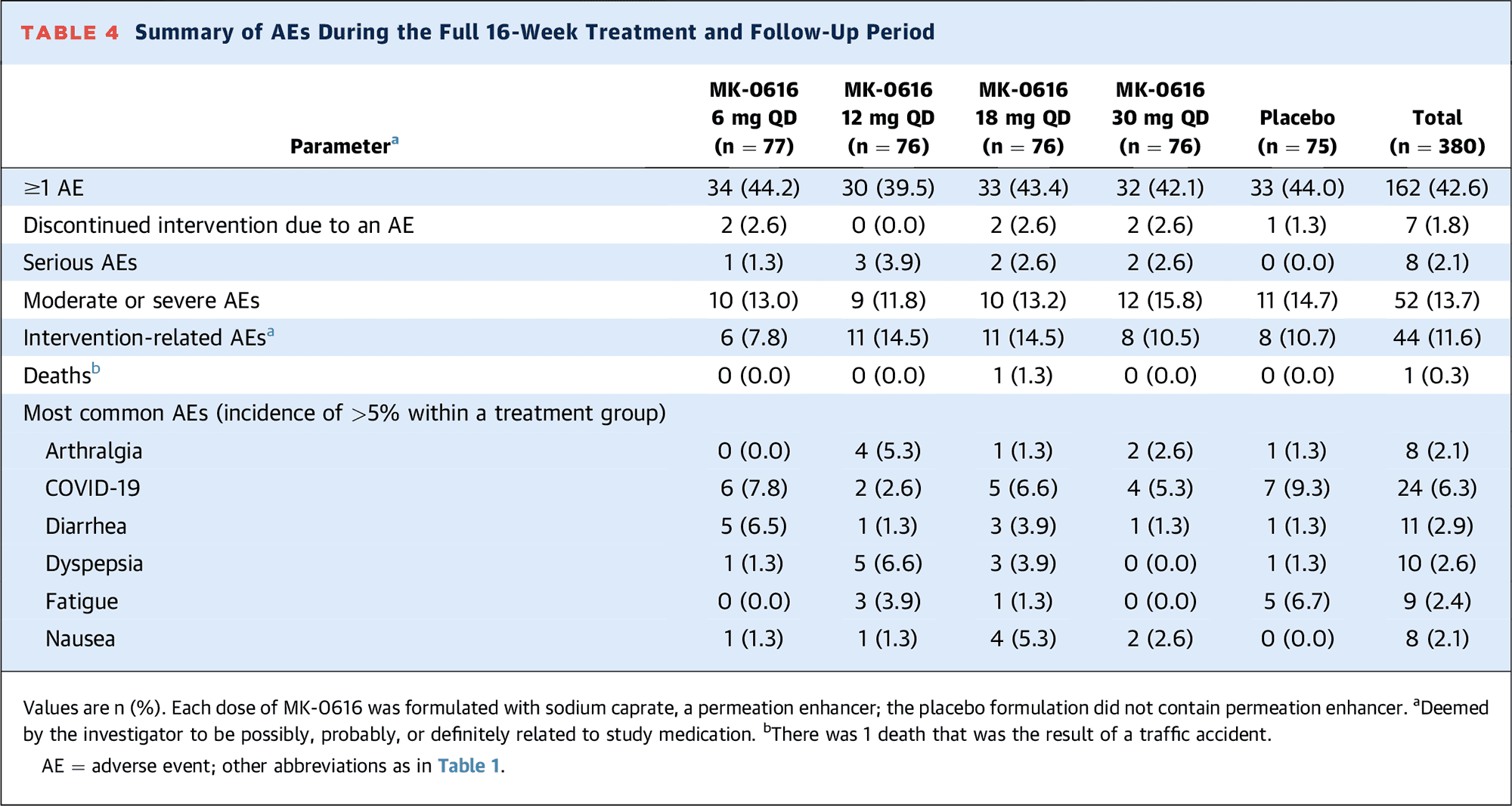
The administration of enlicitide was characterized by acceptable tolerability. The incidences of adverse events (AEs) were identical in the drug subgroups and control group: 40%–44% vs. 44%.
Among the most common AEs that occurred mostly with a mild degree of severity: COVID-19 (in 3%–8% of patients receiving enlicitide — vs. 9% in the placebo group), diarrhea (1%–7% vs. 9%), dyspepsia (0%–7% vs. 1%), fatigue (0%–4% vs. 2%), arthralgia (0%–5% vs. 2%), and nausea (1%–5% vs. 0%).
There were no recorded AEs that manifested in a dose-dependent manner as a result of treatment. Enlicitide was discontinued in 2% of patients due to AEs — vs. 1% in the placebo group.
Late-Stage Studies
In late August 2023, Merck & Co. announced the launch of the CORALreef pivotal clinical program, which will enroll approximately 17,000 people and whose ongoing phase 3 trials will form the basis of the filing for enlicitide (MK-0616), a low-density lipoprotein (LDL) cholesterol–lowering agent:
- CORALreef Lipids (NCT05952856). Adult patients (n=2760) with hypercholesterolemia who either have a history of a serious complication of atherosclerotic cardiovascular disease (ASCVD) and LDL cholesterol (LDL-C) level ≥55 mg/dL, or who have not yet experienced such a complication but are at moderately high risk of developing it and LDL-C ≥70 mg/dL. A serious complication of ASCVD is defined as acute coronary syndrome, myocardial infarction, ischemic stroke, or symptomatic peripheral arterial disease (PAD). The primary endpoint of treatment efficacy is the mean percent change in LDL-C after 24 weeks of therapy.
- CORALreef HeFH (NCT05952869). Adult patients (n=270) with heterozygous familial hypercholesterolemia (HeFH), LDL-C ≥55 mg/dL or ≥70 mg/dL (depending on medical history), adhering to moderate-to-high intensity statin therapy. The primary endpoint of treatment efficacy is the mean percent change in LDL-C after 24 weeks of therapy.
- CORALreef Outcomes (NCT06008756). Adult patients (n=14550) adhering to moderate-to-high intensity statin therapy and with LDL-C ≥70 mg/dL or ≥90 mg/dL (depending on medical history) who either with a history of major complication of ASCVD (myocardial infarction, ischemic stroke, successful peripheral arterial revascularization, or major amputation due to atherosclerosis), or at high risk of developing a first major complication of ASCVD (age ≥50 years and evidence of coronary artery disease (CAD), PAD, or atherosclerotic cerebrovascular disease; age ≥60 years and diabetes mellitus and at least one of the following: microvascular disease, urinary albumin-to-creatinine ratio ≥40 mg/mmol, daily insulin use, or diabetes lasting ≥10 years). The primary endpoint of treatment efficacy is time to first major adverse cardiovascular event (MACE), including fatal CAD, myocardial infarction, fatal and non-fatal ischemic stroke, acute limb ischemia or major amputation, or urgent arterial revascularization (coronary, cerebrovascular, or peripheral).
Results from the CORALreef Lipids and CORALreef HeFH clinical trials will be available by September 2025, while CORALreef Outcomes will not be summarized until the fall of 2029, due to the desire to see long-term six-year outcomes with continued enlicitide administration.
Expert Comments
Therapy with oral statins has long been the gold standard in the treatment of hypercholesterolemia [1] [2]. However, despite guidelines that focus on the use of high-intensity statin therapy, the use of drugs of this class in clinical practice remains challenging, which may be due in part to adverse events and intolerance to statins. In addition, even when successfully introduced, high-dose statins often fail to achieve treatment goals, especially in high-risk patients [3] [4] [5].
Adding nonstatin drugs with alternative mechanisms of action is a recommended strategy, but many patients still remain under-treated [6] [7] [8] [9] [10]. The effectiveness of lowering low-density lipoprotein (LDL) cholesterol (LDL-C) levels with additional oral medications is relatively modest. Thus, bile acid sequestrants add approximately 12%–18% to LDL cholesterol reduction, ezetemibe 20%–25%, bempedoic acid 18% [2] [11] [12].
Experimental enlicitide (MK-0616), an oral proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor under development by Merck & Co. provided, in contrast to the aforementioned oral drugs, a significantly deeper 41%–61% placebo-adjusted reduction in LDL-C levels.
The class of drugs targeting PCSK9 has been around for a long time. Its first members were the Praluent (alirocumab) and Repatha (evolocumab), monoclonal antibodies offered respectively by Sanofi / Regeneron Pharmaceuticals and Amgen in summer 2015.
Alirocumab and evolocumab are able to reduce LDL-C levels by an average of 48%–56% relative to placebo [13] [14]. Despite the rare and patient-friendly dosing, realized by subcutaneous injections once a month or every two weeks, Praluent and Repatha are not in great demand due to their high cost, which is not willing to be covered by health insurance providers.
And it is true: If a course of treatment with statins, which many years ago moved into the category of generic drugs, costs pennies, then for a year’s course of treatment with Praluent or Repatha one had to pay $14,000. However, after a while, when manufacturers realized that the demand is catastrophically low, the price tag was sharply dropped by 60%, down to almost $6,000.
In late December 2020, Novartis launched Leqvio (inclisiran) at a U.S. price of $6,500 per year. The key feature of inclisiran, which is based on RNA interference, is the dosing regimen: In maintenance therapy, it is administered subcutaneously once every six months. The therapeutic efficacy of Leqvio is within the range of 48%–52% reduction in LDL-C levels relative to placebo [15].

Leqvio: Newest Drug Against ‘Very Bad’ Cholesterol
Two injections of inclisiran a year and you can forget about high cholesterol. Novartis doesn’t lie.
The mechanistic difference between the above three drugs is that alirocumab and evolocumab block circulating PCSK9, while inclisiran inhibits PCSK9 synthesis directly.
Given the highly competitive market for PCSK9 inhibitors, there is no doubt that the only way to attract the attention of the patient, physician, and insurance community to enlicitide is through price affordability.
The injectable nature of the three existing anti-PCSK9 medications against ‘bad’ cholesterol, Praluent, Repatha, and Leqvio, even if administered not intravenously, but subcutaneously at home, still does not add to their appeal from the point of view of patients. It is much easier to take an oral statin and believe, even if completely mistakenly, that everything is perfect and in order.
The promising therapeutic efficacy of enlicitide, along with its safety and convenience in tablet form, should be supported by long-term clinical trials. A short 8-week trial is by no means sufficient to provide conclusive evidence, especially in diverse patient populations.
If enlicitide is approved, which could happen closer to 2026, the fight against atherosclerosis, which affects half of the world’s adult population, will reach a qualitatively new level, thanks to the effectiveness and convenience of the forthcoming drug.
The current treatment of cardiovascular diseases is dismal: Up to half of patients stop taking their medications within a year of starting therapy [16] [17] and the same number of people who are indicated for statins do not take them [18], while only 2% of patients who are recommended PCSK9-inhibitors are treated with them [19].
It is safe to say that the cost of enlicitide will not be affordable to everyone, as is the case with cheap statins. It should be expected that the price of enlicitide will not be lower than that of bempedoic acid: In the U.S. the cost of an annual course of Nexletol is $5340 for patients without insurance coverage. Everything depends on Merck & Co., which can easily go along with the greed of its shareholders, asking for a lot of money for enlicitide, thereby essentially putting the business prospects of this drug in the grave. The example of Esperion Therapeutics, which earned modest sums of $75.5 million and $78.4 million for bempedoic acid in 2022 and 2021, is illustrative.
According to industry forecasts, enlicitide has the potential to get to $5 billion at peak sales. And that’s highly optimistic, considering that on the global market the entire class of PCSK9 inhibitors earned $2.3 and $3.1 billion in 2022 and 2023.
Pipeline of PCSK9 Inhibitors
A number of pharma players are working on novel proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors indicated to prevent atherosclerotic cardiovascular complications in dyslipidemia, by lowering low-density lipoprotein (LDL) cholesterol (LDL-C) levels.
Oral Drugs
AstraZeneca is the only one actively developing an oral PCSK9 inhibitor that is a direct competitor to Merck & Co.’s enlicitide (MK-0616).
AZD0780 was purchased from (Dogma Therapeutics) in mid-September 2020. The PURSUIT (NCT06173570) phase 2b clinical trial, in which the experimental drug is administered daily at four different doses to patients with dyslipidemia, will conclude by the end of summer 2024.
AZD0780 is an antisense oligonucleotide (ASO) that binds complementary mRNA of the PCSK9 gene to silence its expression with resultant suppression of protein translation. Oral delivery of ASOs presents several challenges because these compounds are hydrophilic, must pass through the acidic environment of the stomach, and are poorly absorbed in the intestine. By modifying ASO with sodium caprate (to increase intestinal permeability) and an enteric soluble coating (to protect it from the aggressive acidic environment of the stomach), the issues were circumvented: preclinical validation confirmed clinically relevant bioavailability of AZD0780 in the liver [1] [2].
Novo Nordisk was doing roughly the same thing, but in November 2022 the oral PCSK9 inhibitor program NNC0385-0434 (NN6435) was discontinued ‘due to commercial and portfolio considerations.’
NNC0385-0434, being a small-molecule peptide inhibitor of PCSK9, has a chemical structure similar to that of the LDL receptor (LDLR): EGF-like domain A of the latter is used. Therefore, the molecule competitively binds free PCSK9, thereby as if pulling its attention away from binding to the natural LDLR [3].
The issue of dramatically improving the oral bioavailability of NNC0385-0434 was addressed by the addition of sodium caprylate (SNAC), the same absorption enhancer used in the formulation of oral semaglutide, an agonist of glucagon-like peptide-1 receptor (GLP1R) [4].
In the NCT04992065 phase 2 clinical trial among patients with or at risk for atherosclerotic cardiovascular disease (ASCVD), daily administration of NNC0385-0434 at doses of 15 mg, 40 mg, or 100 mg resulted in a 32%, 45%, and 62% reduction in LDL-C levels relative to placebo [3].
Somewhat remarkably, the active comparison group receiving the monoclonal anti-PCSK9 antibody Repatha (evolocumab) by subcutaneous injection every two weeks demonstrated a 59.6% reduction in baseline LDL-C levels, whereas the 100-mg dose of NNC0385-0434 provided a 56.2% reduction, a difference of only 3.4%.
Nothing definite has been heard about the antisense oligonucleotide cepadacursen (CIVI 007), which was discovered by Danish Santaris Pharma, subsequently acquired by Roche, and which CiVi Biopharma plans to transform into an oral drug, CIVI 008. At any rate, a phase 1/2a clinical trial IND filing was scheduled to be submitted to the U.S. Food and Drug Administration (FDA) in the fourth quarter of 2023.
To realize the oral delivery of CIVI 008, a carrier in the form of a salt of N-(5-chlorosalicyloyl)-8-aminocaprylic acid (5-CNAC) is used.
As CiVi suggests, the cost of an annual course of CIVI 008 for U.S. patients will be in the range of $2,000 to $3,000.
The results of the NCT03427710 phase 1 and NCT04164888 phase 2a clinical trials of cepadacursen among patients with hypercholesterolemia have not been published.
China’s CVI Pharmaceuticals has come up with CVI-LM001, an oral small-molecule PCSK9 modulator that increases LDLR expression in the liver and accelerates the removal of LDL-C from the circulation through a dual mechanism of action: The drug inhibits PCSK9 transcription and prevents degradation of LDLR mRNA.
In a phase 1b clinical trial, daily administration of CVI-LM001 to patients with hyperlipidemia provided a 26% reduction in LDL-C levels relative to placebo [5]. However, further development has stalled: the phase 2 clinical trial NCT04438096, started in mid-August 2020, is inactive.
China’s Guangzhou Joyo Pharma is trying its hand with DC371739, an oral small-molecule compound that directly binds the transcription factor HNF1A, thereby inhibiting transcription of PCSK9 and angiopoietin-like 3 (ANGPTL3) genes [6]. The latter, being an inhibitor of lipoprotein lipase (LPL) and endothelial lipase (LIPG), occupies a defining place in lipoprotein metabolism, while it modulates LDL-C in a way that is independent of LDLR and other known mechanisms responsible for the clearance of LDL-C from plasma.
- In early February 2021, Regeneron Pharmaceuticals offered Evkeeza (evinacumab), ANGPTL3 inhibitor for the treatment of homozygous familial hypercholesterolemia (HoFH).
The development of DC371739 was based on the molecular design of tetrahydroprotoberberins extracted from Corydalis ambigua, a plant used in traditional Chinese medicine (TCM).
In a phase 1 clinical trial NCT04927221 among patients with hypercholesterolemia, daily administration of DC371739 reduced LDL-C levels by 19% relative to placebo [6].
Antisense Oligonucleotides
At the end of September 2022, AstraZeneca abandoned the antisense oligonucleotide AZD8233 (ION449) against PCSK9, co-developed with Ionis Pharmaceuticals and administered by monthly subcutaneous injections. The originator, Ionis, is not interested in continuing the expensive development of the drug on its own.
The winding down of the program is due to the competitive environment being fostered. First, there are already monoclonal antibodies, which by analogy are administered subcutaneously once a month and which provide decent efficacy. Second, the emergence of oral enlicitide is imminent.
In the SOLANO (NCT04964557) phase 2b clinical trial among patients with hyperlipidemia, AZD8233 at a dose of 60 mg provided a 62% reduction in LDL-C levels relative to placebo.
In the previous ETESIAN (NCT04641299) phase 2b clinical trial among patients with hypercholesterolemia and high cardiovascular risk, administration of AZD8233 at a dose of 50 mg or 90 mg resulted in a 71% and 77% reduction in LDL-C levels relative to placebo [1].
Monoclonal Antibodies
In mid-August 2023, China’s Innovent Biologics gained local regulatory approval for its PCSK9 inhibitor Sintbilo (tafolecimab). The monoclonal antibody tafolecimab (IBI306), administered subcutaneously every 4 or 6 weeks to patients with primary hypercholesterolemia (including non-familial and heterozygous familial) and mixed dyslipidemia, provided an average 61% reduction in LDL-C levels relative to placebo.
Other Chinese pharma developers are preparing to offer their subcutaneous PCSK9 inhibitors. The monoclonal antibodies ebronucimab (AK102), recaticimab (SHR-1209), and ongericimab (JS002) are developed by Akeso, Jiangsu Hengrui Pharmaceuticals, and Shanghai Junshi Biosciences, respectively.
Of interest is recaticimab, which, when administered every 2 or 3 months, reduced LDL-C levels by 53% and 45% relative to placebo.
Vaccines
The biotech expertise of Vaxxinity, part of United Biomedical, is built around synthetic peptide vaccines that stimulate the production of endogenous antibodies against specified targets.
The optimal combination of proprietary synthetic T helper peptides UBITh linked to target epitopes determines selective activation of the immune system, overcomes immune tolerance to endogenous proteins to induce a targeted humoral B cell response, and minimizes the risks of immune evasion and T cell-mediated cytotoxicity.
Preclinical validation of VXX-401 vaccine in non-human primates demonstrated sustained suppression of PCSK9, reflected by a 30%–50% reduction in LDL-C levels. Immunization was well tolerated and confirmed that immune tolerance had been overcome [1] [2].
A phase 1 clinical study NCT05762276 is ongoing to evaluate the safety, tolerability, immunogenicity, and pharmacodynamics of VXX-401 in healthy volunteers and to elucidate the optimal intramuscular dosing regimen for this vaccine candidate. Results will be available by mid-2024.
Austrian Affiris is engaged in specific active immunotherapy (SAIT), which aims at long-term and sustained suppression of pathogenic target proteins by activating the body’s immune system to make it produce appropriate antibodies. After administration of a therapeutic vaccine, subsequent booster immunizations are administered infrequently: once a year, six months or quarterly.
Affiris’ know-how is built around the AFFITOME biotechnology platform. Amino acid sequences (in the form of short peptides) are created that mimic the epitope regions of the target protein in the body. These are then modified through mutagenesis to be as ‘foreign’ to the immune system as possible (to enhance the immune response). These immunogenic peptide ‘doppelgangers’, called affitopes, are then combined with a protein carrier (to deliver to the body) and adjuvant aluminum hydroxide (to enhance the immune response). After subcutaneous injection, affitopes are recognized by the immune system, which begins to produce antibodies against them, which in parallel attack pathogenic target proteins.
Vaccine candidate AT04 (FB6001), containing 10 amino acid sequences and designed to break immune tolerance to the PCSK9 protein, induces a specific oligoclonal antibody response that cross-reacts with and inhibits the target protein in the face of PCSK9, all without activating autoimmunity.
In the phase 1 clinical trial NCT02508896, healthy volunteers were primed with three doses of the therapeutic AT04 vaccine (at weeks 0, 4, and 8) and then received one booster dose (at week 60, one year later). The reduction in LDL-C levels relative to placebo was 11% and 13% at weeks 20 and 70. Throughout the trial, the average reduction came out to 7% relative to placebo, the maximum recorded was 39% [3].
In late December 2021, China’s Frontier Biotechnologies licensed AT04 for the treatment of hypercholesterolemia.
There is no word on whether anyone is still developing AT04.
Gene Editing
The PCSK9 inhibitors sector is likely to change dramatically in the long term when a therapeutic modality involving a one-time treatment becomes available. Thus, Verve Therapeutics’ VERVE-101 is an in vivo gene editing approach where mRNA instructions delivered to hepatocytes alter, by invoking CRISPR technology, one DNA base pair of the gene encoding PCSK9, thereby disrupting the production of the corresponding protein.
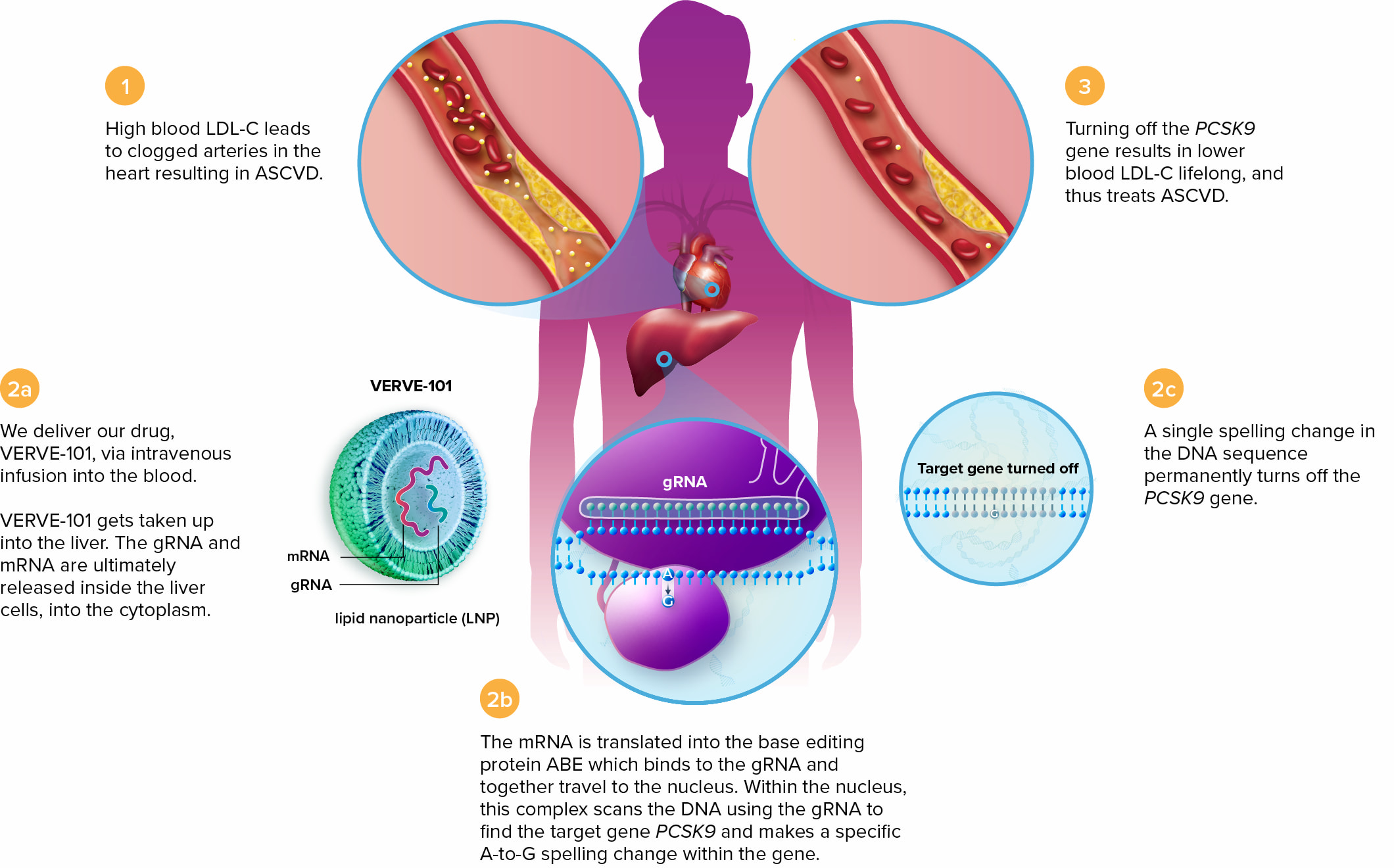
In a preclinical study in non-human primates, a single intravenous infusion of VERVE-101 achieved a shutdown of the PCSK9 gene with 70% efficacy, reflected by an 89% reduction in PCSK9 protein levels in the blood and a 69% reduction in LDL-C levels. Results were maintained throughout the 1.3-year follow-up. Importantly, no prerequisites for transmission of the edited PCSK9 gene to offspring were revealed [1].
The HEART-1 (NCT05398029) phase 1b clinical trial testing PCSK9 gene knockdown among patients with heterozygous familial hypercholesterolemia (HeFH) with advanced atherosclerotic cardiovascular disease (ASCVD) and uncontrolled hypercholesterolemia is ongoing.
According to an interim analysis of data from three patients collected one month after VERVE-101 administration, two subjects in the low-dose group demonstrated reductions in PCSK9 protein levels of 59% and 84%, with concomitant reductions in LDL-C levels of 39% and 48%. One subject in the high-dose group showed corresponding reductions of 47% and 55%, while the achieved drop in LDL-C levels was maintained for 180 days.
In the first half of 2024, Verve plans to launch a phase Ib clinical trial of its design-enhanced gene editing therapy VERVE-102, which is expected to improve the efficacy of disabling the PCSK9 gene.
Verve’s efforts are supported by Eli Lilly.
Precision Biosciences confirmed that the targeted LDL-C–lowering effect realized in non-human primates by in vivo gene intervention in the structure of the PCSK9 gene was maintained over 3 years of follow-up [2].
Precision’s gene editing is implemented through its proprietary ARCUS platform using I-CreI, a naturally occurring genome editing enzyme found in the alga Chlamydomonas reinhardtii and dedicated to highly specific cuts and insertions into cellular DNA. I-CreI belongs to a larger class of enzymes called homing endonucleases or meganucleases.
However, in early January 2023, Precision put the PBGENE-PCSK9 program on pause due to difficulties in obtaining FDA approval for clinical trials.
Others
In the first half of 2024, LIB Therapeutics will submit New Drug Application (NDA) for lerodalcibep (LIB003), a small recombinant fusion protein of PCSK9-binding domain (adnectin) and human serum albumin. Lerodalcibep, stable at room temperature and subcutaneously administered once a month, resulted in a 59% reduction in LDL-C levels relative to placebo [1].