SUMMARY
- High blood pressure affects 1.3 billion people globally.
- Current antihypertensive medications may not be effective in the long term.
- Completely new approach involves blocking angiotensinogen production in liver.
- New drugs can be administered monthly, quarterly, or even semi-annually.
- Zilebesiran and tonlamarsen — fast, reliable, expensive!
WHAT HAPPENED
Alnylam Pharmaceuticals and Ionis Pharmaceuticals have developed innovative drugs to treat hypertension.
These advanced treatments promise to help even when blood pressure cannot be reduced by the existing armamentarium of antihypertensive medications.
Two investigational drugs — zilebesiran and tonlamarsen — address a completely new mechanism of action that has not been used in the treatment of hypertension before. This involves the suppression of angiotensinogen production in the liver.
It is anticipated that the forthcoming drugs will demonstrate efficacy when administered with a very infrequent dosing regimen, with subcutaneous injection once every three or even six months.
In the future, these drugs may evolve into even more convenient oral tablets or capsules taken, for example, once a week or month.
WHY IT MATTERS
Hypertension, or high blood pressure, is a complex multifactorial disease manifested by elevated blood pressure.
The clinical diagnosis of hypertension, according to the majority of consensus guidelines, is made when systolic blood pressure (SBP) exceeds 140 mmHg and diastolic blood pressure (DBP) exceeds 90 mmHg [1] [2] [3]. However, the American Heart Association (AHA) and the American College of Cardiology (ACC) recommend a diagnosis of hypertension when the respective values are above 130 and 80 mmHg, respectively [4].
High blood pressure affects one in four men and one in five women globally, a total of over 1.28 billion people aged 30–79 years [5].
High blood pressure is one of the leading causes of premature death.
High blood pressure that is not adequately treated or left untreated increases the risk of developing or worsening cardiovascular and cerebrovascular diseases, including coronary heart disease (CHD) and stroke. It also contributes to the progression of chronic kidney disease (CKD) [6] [7] [8] [9].
Despite the availability of effective drugs to reduce blood pressure, pharmacotherapy of hypertension leaves much to be desired. Half of patients on chronic antihypertensive medications fail to reach blood pressure targets [10].
This is partly a consequence of the failure of the treating physician to initiate or intensify drug therapy and, second, of poor patient adherence to daily oral antihypertensives [11] [12] [13].
The situation is further complicated by the fact that even when blood pressure appears to be well controlled based on periodic measurements, hypertension control may remain suboptimal due to the marked variability of blood pressure during the diurnal cycle and over time [14] [15] [16].
SOLUTION
Chronic overactivity of the renin–angiotensin–aldosterone system (RAAS) is considered a significant contributing factor in the pathogenesis of cardiovascular diseases, including hypertension, heart failure, cardiac hypertrophy, and atherosclerosis [1] [2].
Inhibition of the RAAS pathway by angiotensin-converting enzyme (ACE) inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs) represents one of the most effective treatments for hypertension and heart failure with reduced ejection fraction (HFrEF) [3] [4] [5] [6] [7].
However, a significant challenge to the full realization of this approach is the potential for on-target toxicity, which manifests primarily as hyperkalemia and renal dysfunction. Consequently, clinical doses must be reduced, limiting the potential for optimal RAAS inhibition and the associated benefits in terms of blood pressure reduction [8].
Pharmacological inhibition of the downstream cascade of the RAAS pathway also leads to the formation of compensatory pathways in the upstream cascade, which further reduces the therapeutic efficacy of antihypertensive drugs [9] [10] [11].
Targeting the upstream cascade of the RAAS pathway by silencing (suppressing the expression of) angiotensinogen (AGT) produced by the liver represents a fundamentally new approach to restraining RAAS activity [12].
Since angiotensinogen is the sole precursor of all angiotensin peptides, its silencing is distinguished by a number of potential advantages over the majority of existing methods of RAAS inhibition [13] [14] [15] [16] [17] [18].
Thus, tissue-specific suppression of angiotensinogen production in the liver, without affecting RAAS inhibition in the kidneys, offers the potential for an enhanced safety profile, as renal homeostasis and the tubuloglomerular feedback are preserved. Consequently, the risks of increased potassium levels and renal dysfunction are reduced.
The risk of compensatory mechanisms that occur in response to ACEIs or ARBs administration and that paradoxically attempt to restore renin, aldosterone, and angiotensin II levels is minimized.
Furthermore, more complete inhibition of localized angiotensin II production in vascular or cardiac tissues would benefit patients with resistant hypertension or heart failure.
ALNYLAM PHARMACEUTICALS AND INNOVATIVE HYPERTENSION TREATMENT
Alnylam Pharmaceuticals is developing an investigational drug, zilebesiran, based on the therapeutic modality of RNA interference (RNAi), which has repeatedly demonstrated its medical validity.
The early-stage clinical trial of zilebesiran was highly successful, and therefore this drug candidate attracted the attention of Roche, which signed a partnership agreement with Alnylam at the end of July 2024 [1].
The agreement stipulates that the Swiss pharmaceutical conglomerate will provide Alnylam with an upfront payment of $310 million, with additional payments to be made as the drug is developed, approved by regulators, and sold. The total amount payable to Alnylam under this agreement may reach a maximum of $2.8 billion. The two companies will jointly market zilebesiran in the United States on an equal profit-sharing basis, with Roche assuming responsibility for sales in all other countries and paying a royalty to Alnylam.
ZILEBESIRAN: HOW IT WORKS
The renin–angiotensin–aldosterone system (RAAS) is a signaling cascade that has been reliably proven to play a crucial role in blood pressure regulation. Its suppression is accompanied by well-known antihypertensive effects [1] [2] [3] [4] [5] [6] [7].
The question of whether or not to block the RAAS has long been irrelevant in clinical scenarios of heart failure, diabetic nephropathy, and chronic kidney disease. The pharmaceutical industry is currently focused on optimizing this blockade.
Zilebesiran (ALN-AGT) is a targeted inhibitor of angiotensinogen (AGT), the earliest precursor of angiotensin I (proangiotensin), which subsequently gives rise to angiotensin II, an oligopeptide hormone that is part of the RAAS and that causes vasoconstriction and increased blood pressure [8].
Zilebesiran is based on RNA interference (RNAi), a natural mechanism of gene silencing (suppression of gene expression) at the stage of transcription, translation, deadenylation, or degradation of messenger RNA (mRNA) by small interfering RNA (siRNA). The discovery of RNAi was awarded the Nobel Prize in 2006 [9].
Zilebesiran interferes with mRNA of the AGT gene, which is reflected by its silencing. Inhibition of angiotensinogen synthesis in the liver leads to a sustained decrease in angiotensin I and eventually angiotensin II levels. As a consequence, blood pressure decreases, because angiotensin II both independently has a vasoconstrictor effect and does it through stimulation of vasopressin synthesis.
Structurally, zilebesiran is composed of two distinct parts: a chemically modified siRNA against AGT and an N-acetylgalactosamine (GalNAc) ligand that binds asialoglycoprotein receptor 1 (ASGR1) on hepatocytes, thereby enabling targeted delivery of the drug to the liver, where endosomal accumulation, slow leakage, and recycling of siRNAs fuel AGT knockdown for a long time.
Zilebesiran employs the proprietary GalNAc-conjugate technology Enhanced Stabilization Chemistry Plus (ESC+), which allows for very infrequent subcutaneous administration of the drug, coupled with endowing it with high selectivity and a broad therapeutic index.
ZILEBESIRAN: IT WILL WORK OUT ALL RIGHT
The fact that Alnylam Pharmaceuticals’ technological approach will work for the treatment of hypertension is evidenced by the RNA interference drugs it has commercialized for rare diseases:
- Onpattro (patisiran) and Amvuttra (vutrisiran): treatments for hereditary transthyretin-mediated (hATTR) amyloidosis with polyneuropathy (hATTR-PN), formerly known as familial amyloid polyneuropathy (FAP) [1] [2].
- Givlaari (givosiran): treatment of acute hepatic porphyria (AHP) [3].
- Oxlumo (lumasiran): treatment of primary hyperoxaluria type 1 (PH1) [4] [5].
All of these drugs are used in an infrequent dosing regimen. Thus, Onpattro requires intravenous infusions once every three weeks, Givlaari should be administered by subcutaneous injection once a month, and Oxlumo and Amvuttra are administered subcutaneously once a quarter.
Furthermore, Novartis has launched Leqvio (inclisiran), an RNA interference drug indicated for the potent reduction of low-density lipoprotein (LDL) cholesterol by subcutaneous injection once every six months. The concept behind Leqvio originated with Alnylam.

Leqvio: Newest Drug Against ‘Very Bad’ Cholesterol
Two injections of inclisiran a year and you can forget about high cholesterol.
ZILEBESIRAN: EFFICACY AND SAFETY
NCT03934307
The NCT03934307 phase 1 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled adult patients with elevated systolic blood pressure (mild to moderate hypertension with 130–165 mmHg) who were not taking any antihypertensive medications (either previously untreated for hypertension or who had refused such medications).
Participants received a single subcutaneous dose of zilebesiran at various doses or placebo.
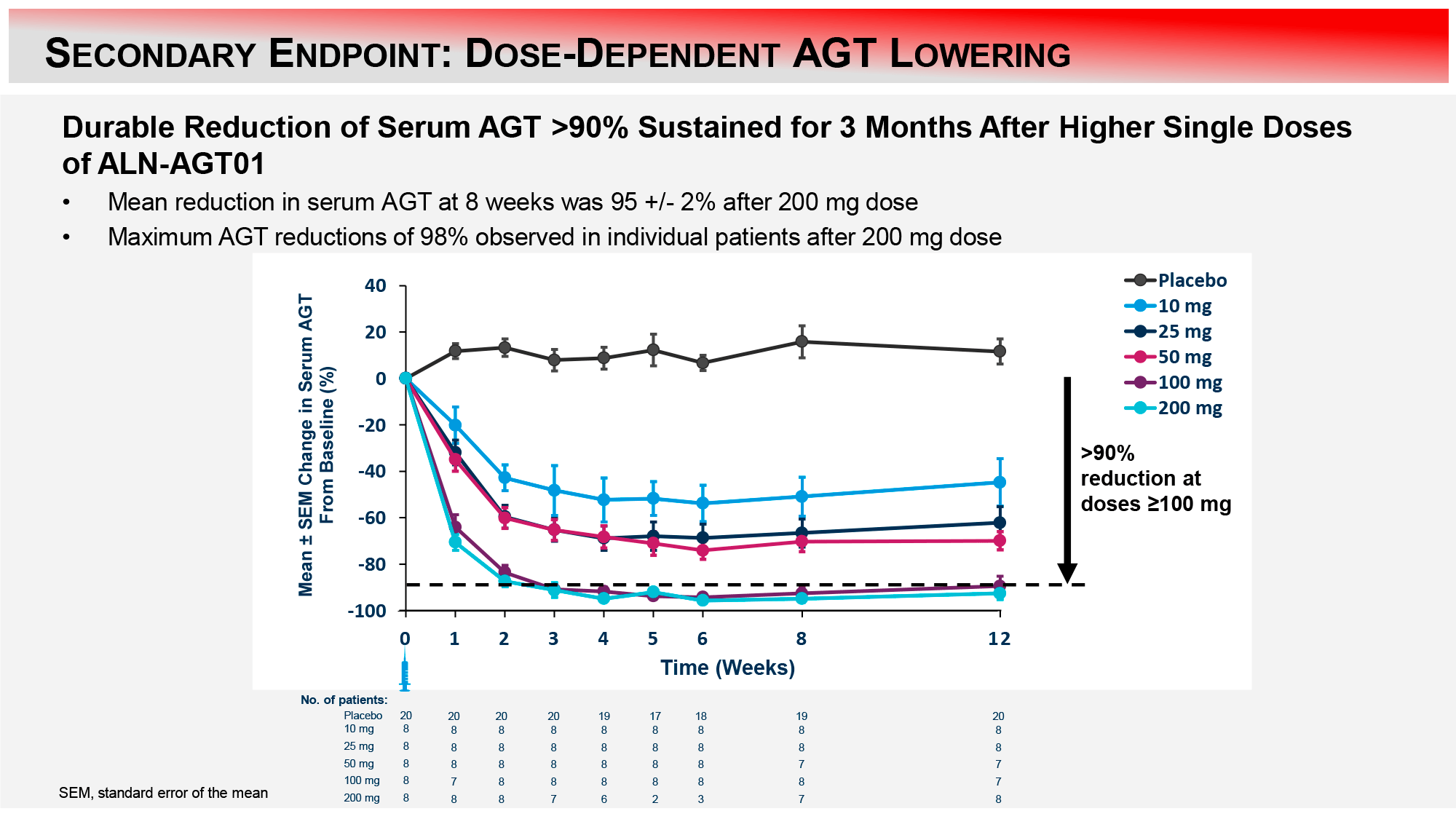
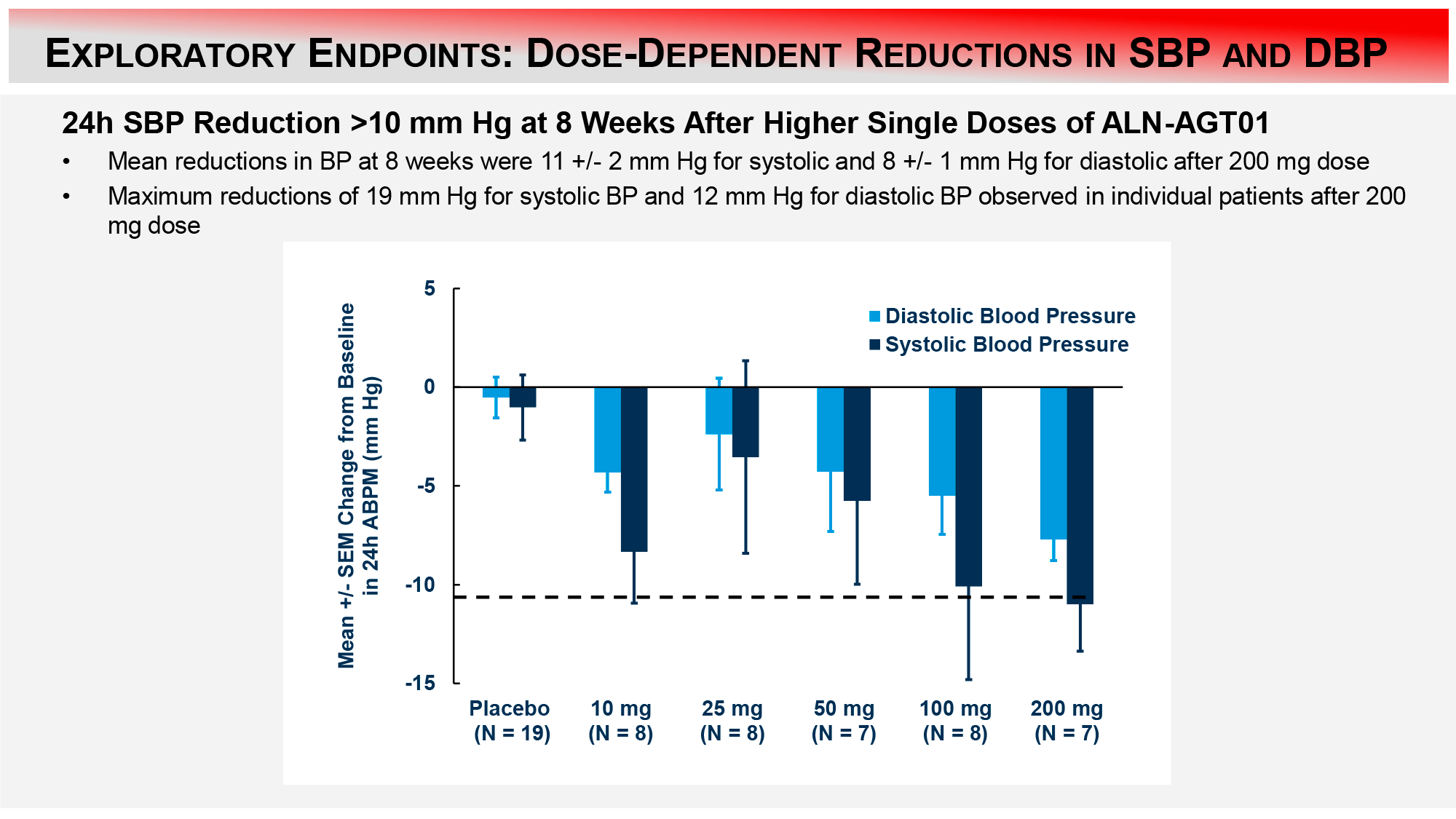
The results of the 200-mg zilebesiran subgroup after 8 weeks are as follows [1]:
- A reduction in serum angiotensinogen (AGT) levels of greater than 90% was maintained at 3 months.
- The mean reductions in systolic blood pressure (SBP) and diastolic blood pressure (DBP) were 11±2 and 8±1 mmHg, respectively, with a maximum reduction of 19 and 12 mmHg observed in some subjects.
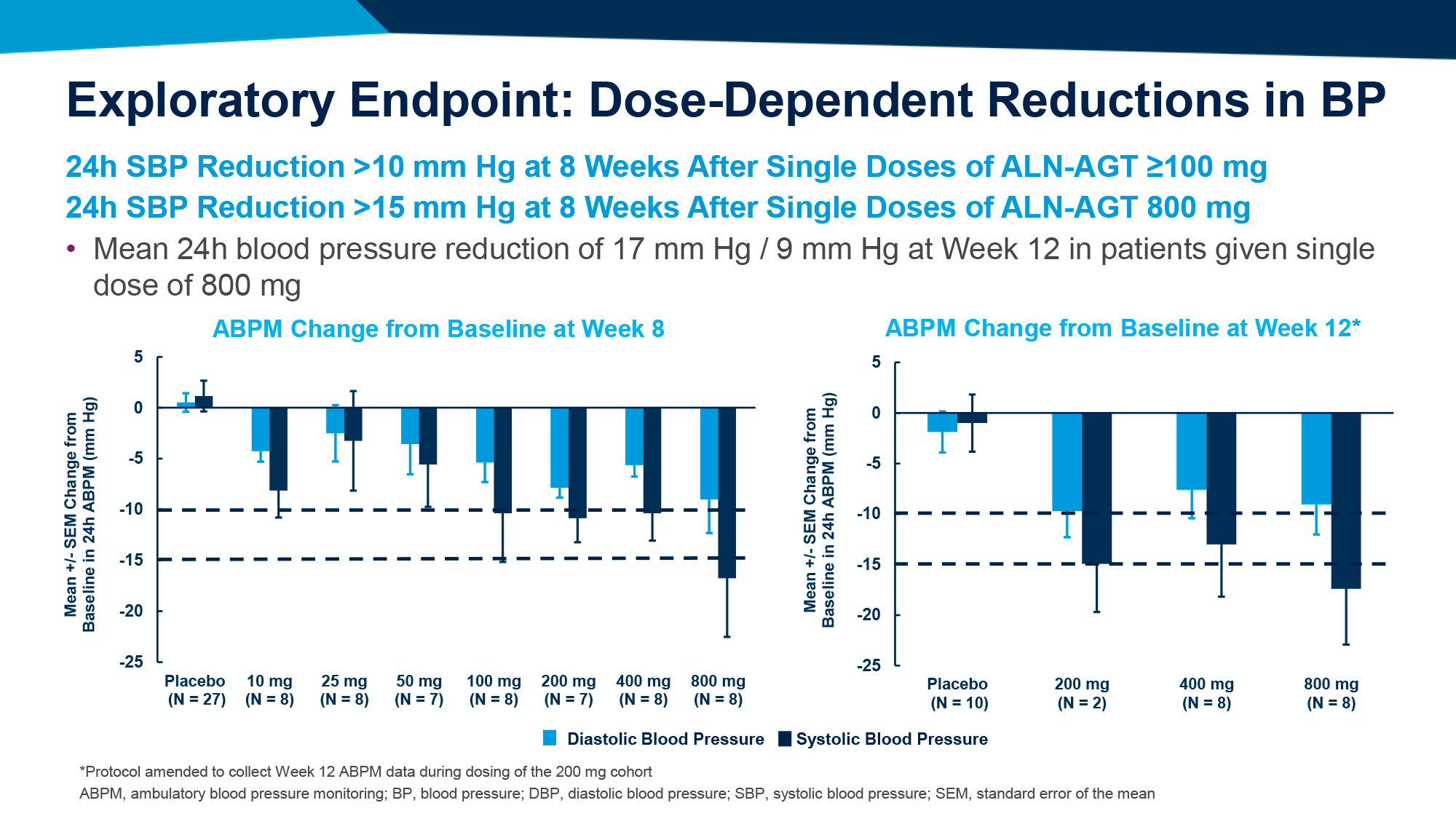
The results after 12 weeks are as follows [2]:
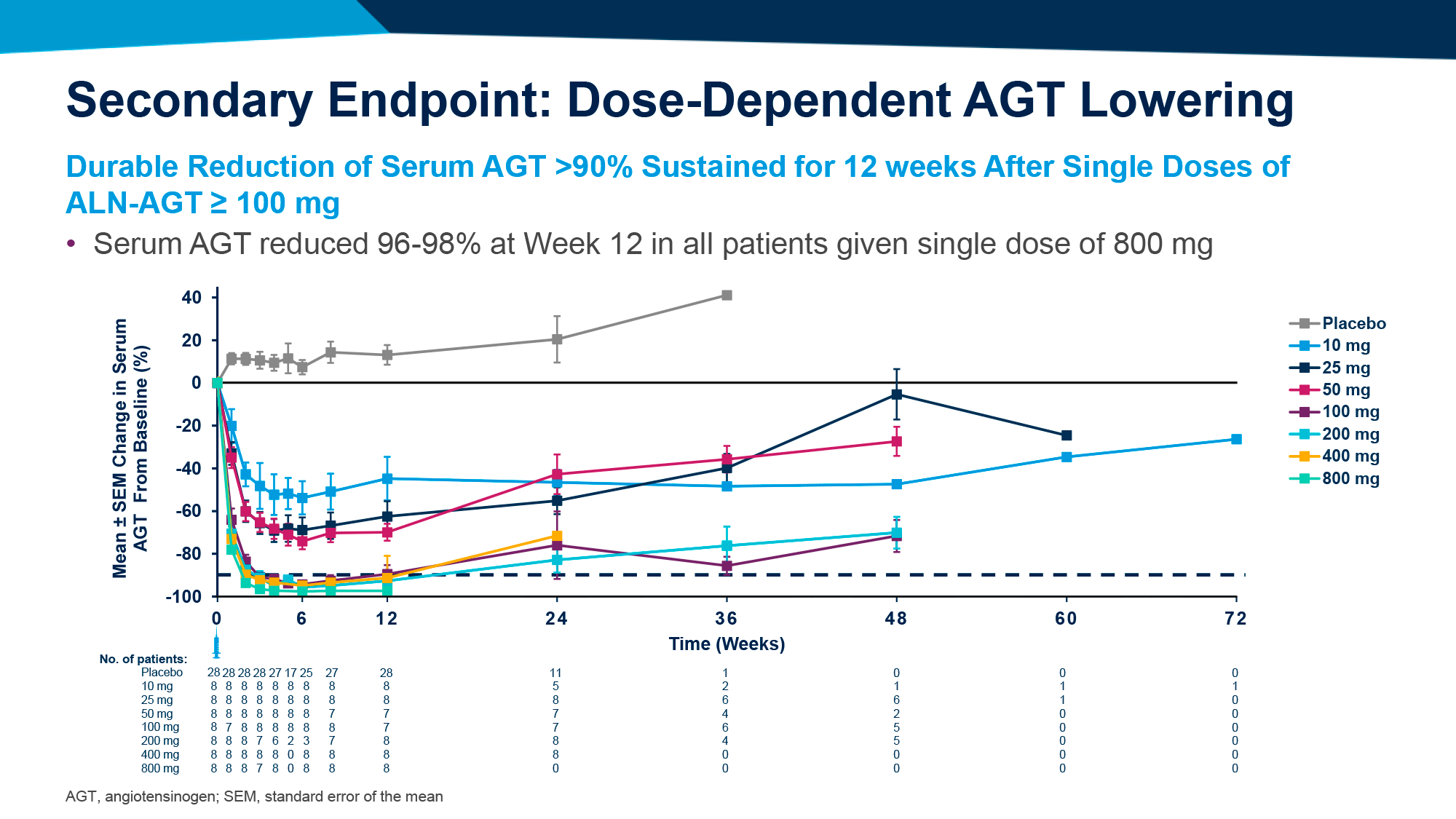
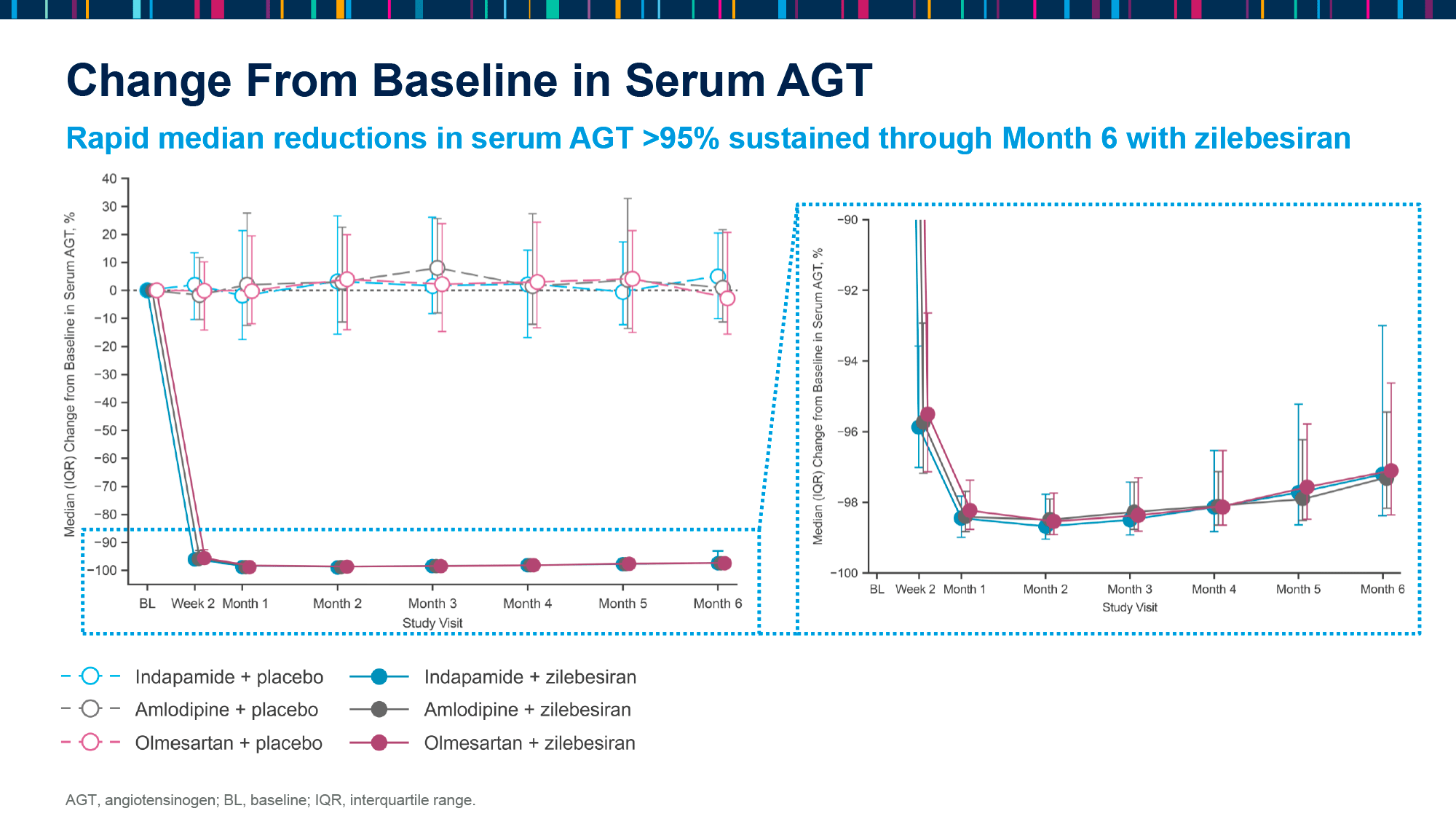
- Subgroups of zilebesiran at a dose of 100 mg and above demonstrated a sustained reduction in serum AGT levels of greater than 90%, with the indicated reduction in the 800-mg subgroup being 96%–98%.
- The administration of zilebesiran at a dose of 100 mg or higher resulted in a reduction in SBP of at least 10 mmHg, with the 800-mg subgroup demonstrating a SBP reduction of greater than 15 mmHg.
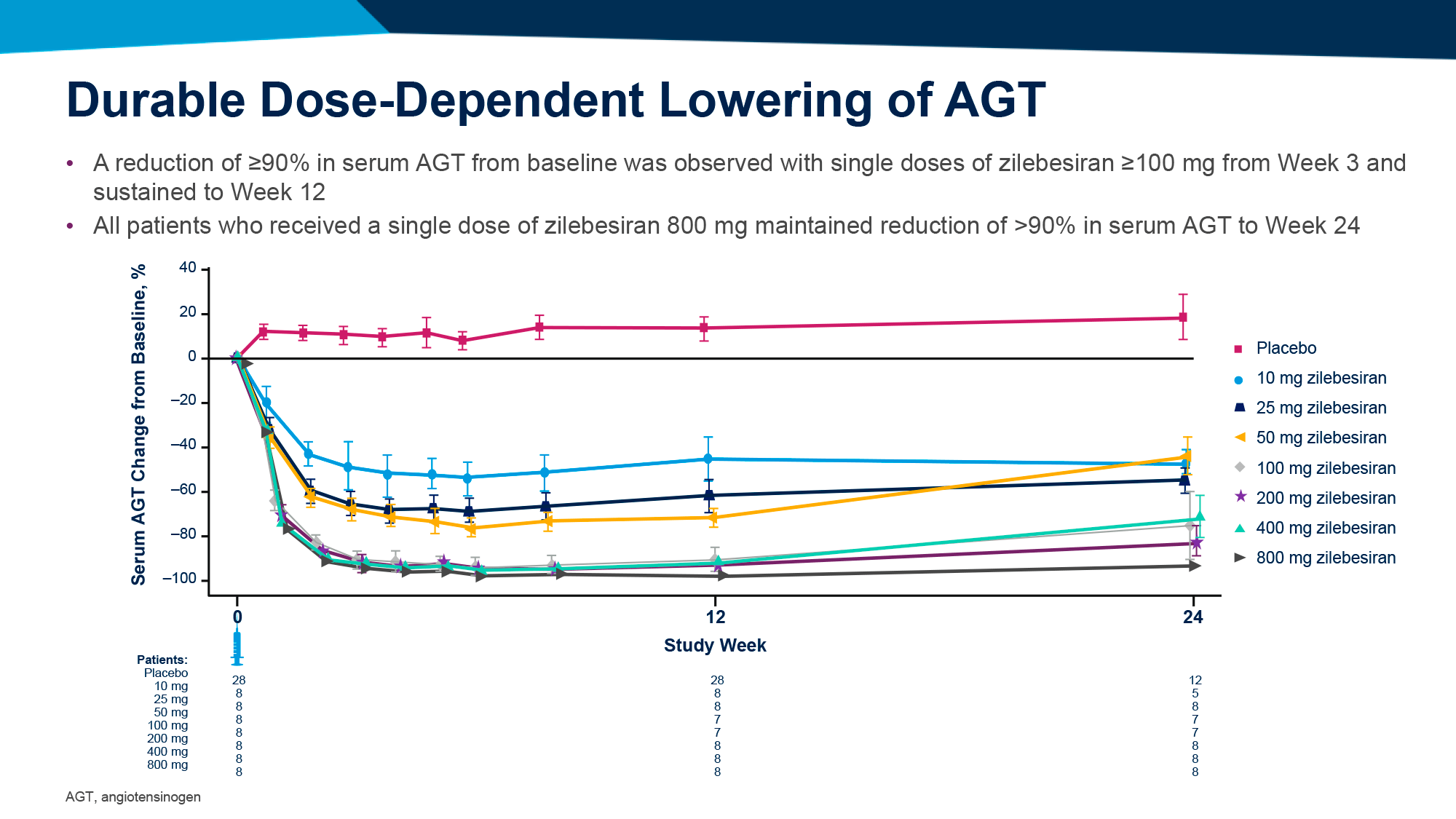
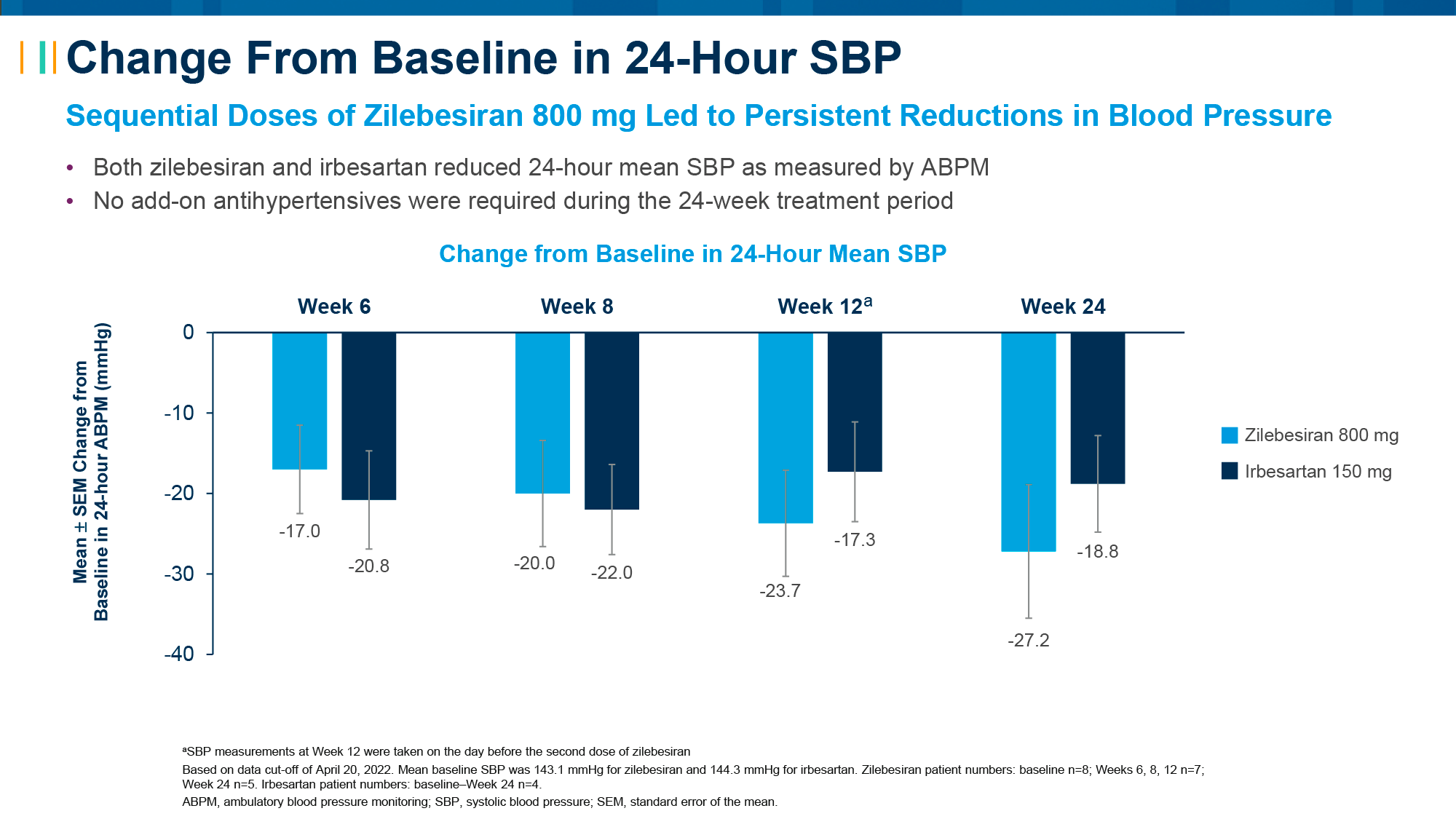
After 24 weeks, the following outcomes were demonstrated [3]:
- At week 3 of follow-up, administration of zilebesiran at a dose of 100 mg or higher resulted in a reduction in serum AGT levels of greater than 90%, which was sustained for 12 weeks. This reduction was also sustained for 24 weeks in the 800-mg subgroup.
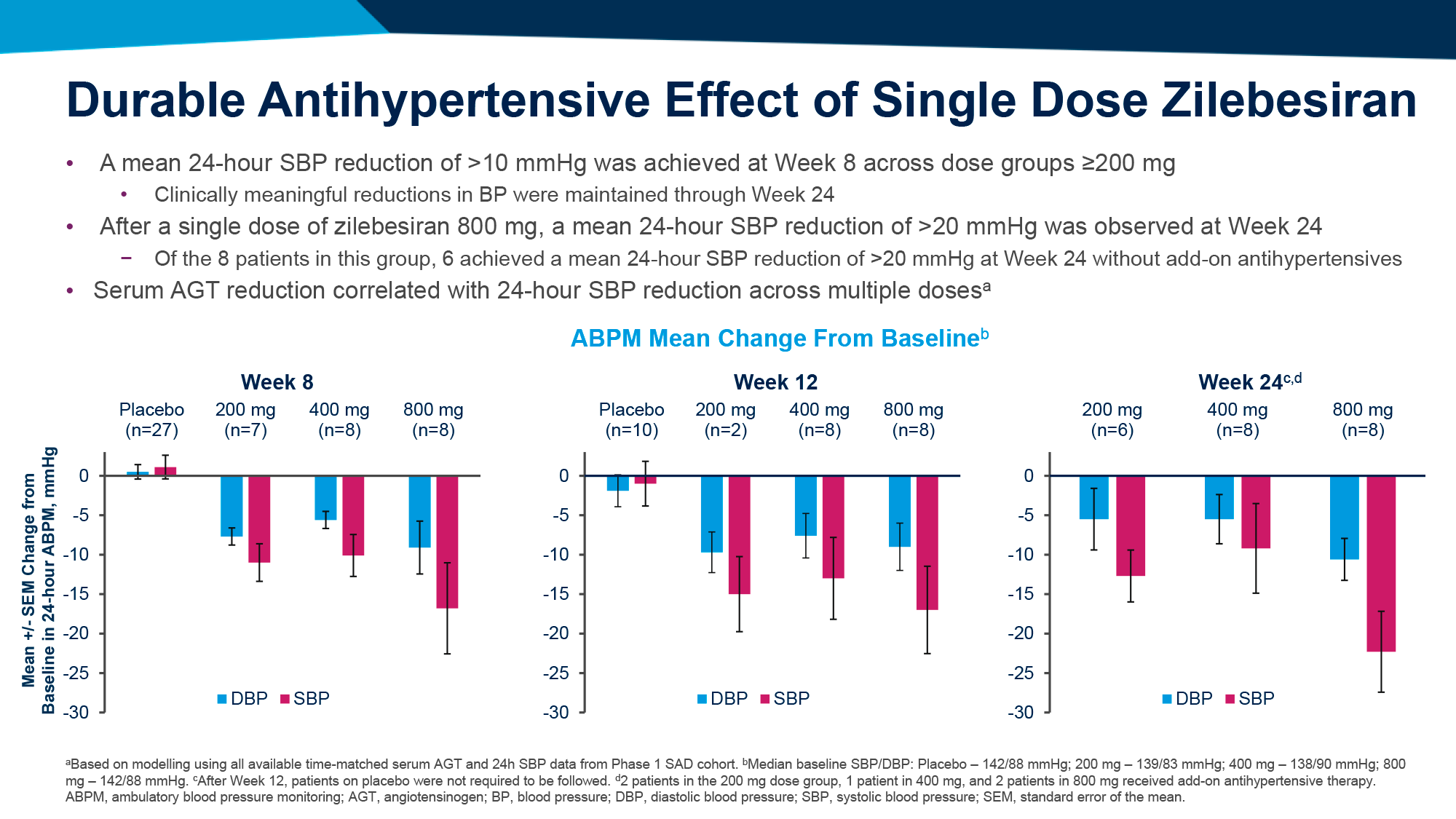
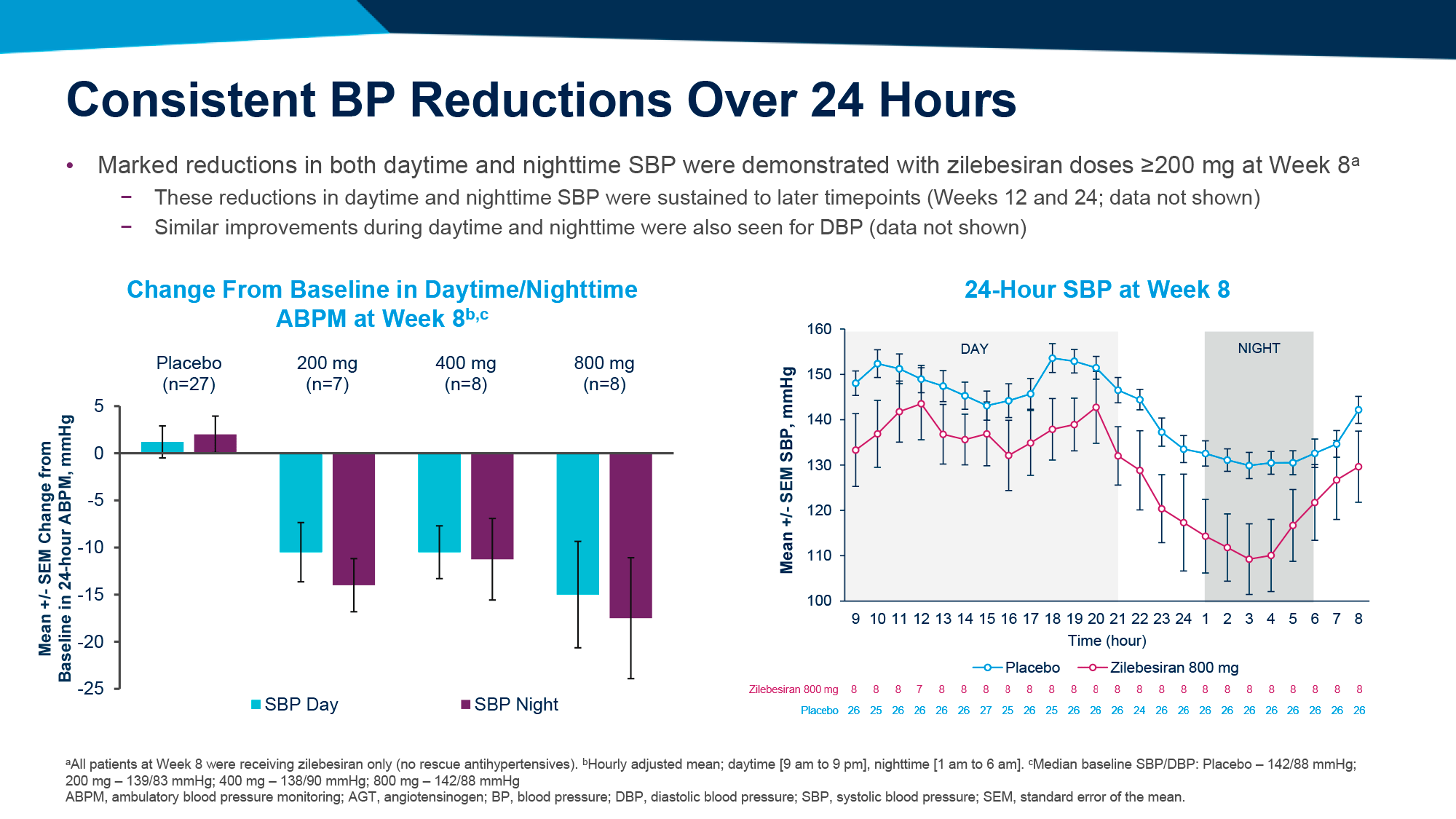
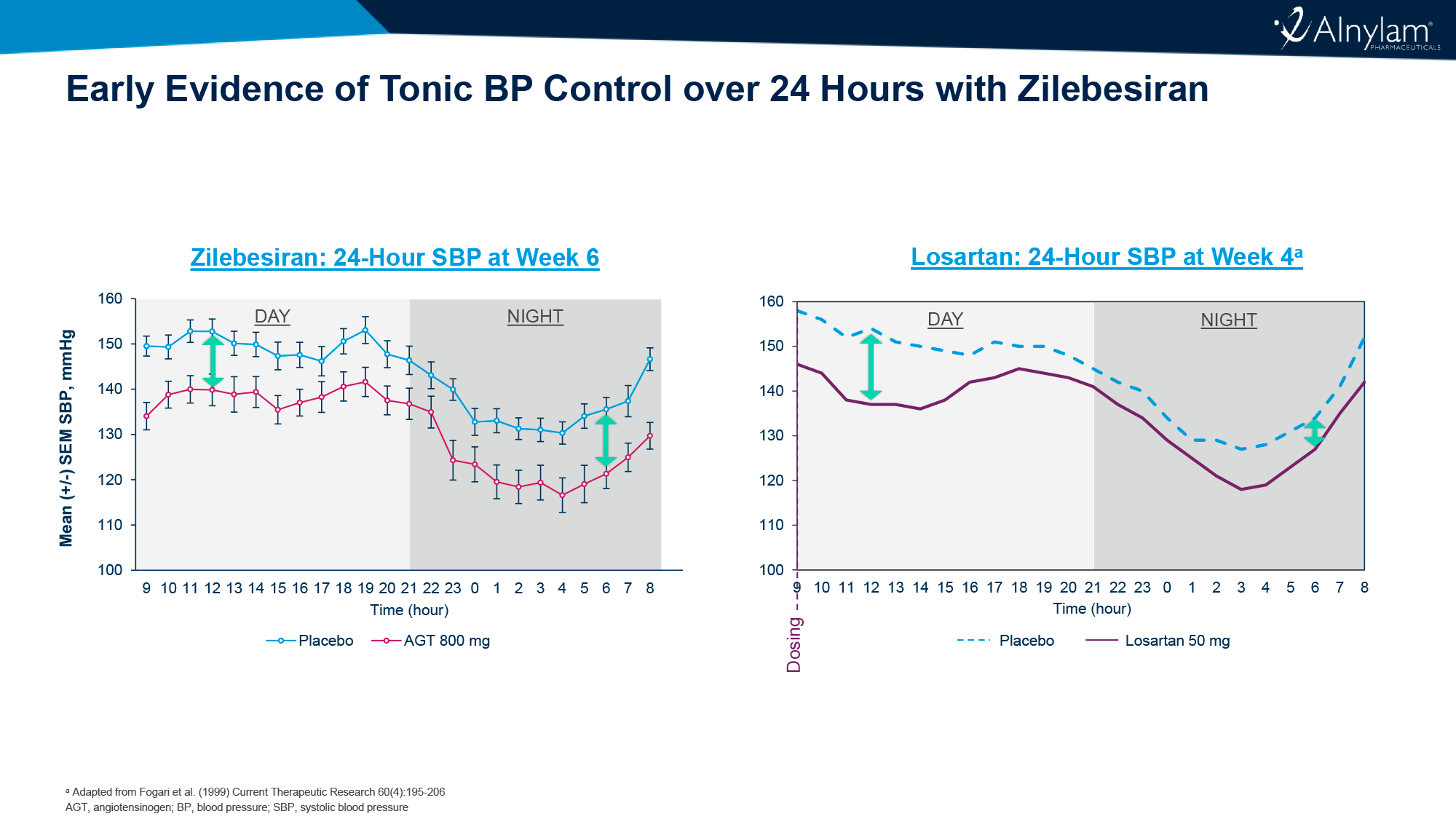
- At week 8 of follow-up, administration of zilebesiran at a dose of 200 mg or higher resulted in a reduction in SBP of at least 10 mmHg, which was maintained throughout the 24-week observation period.
- At week 24 of follow-up in the 800-mg zilebesiran subgroup, the reduction in SBP exceeded 20 mmHg, and this was achieved in 6 of 8 patients without the need for additional antihypertensive medication.
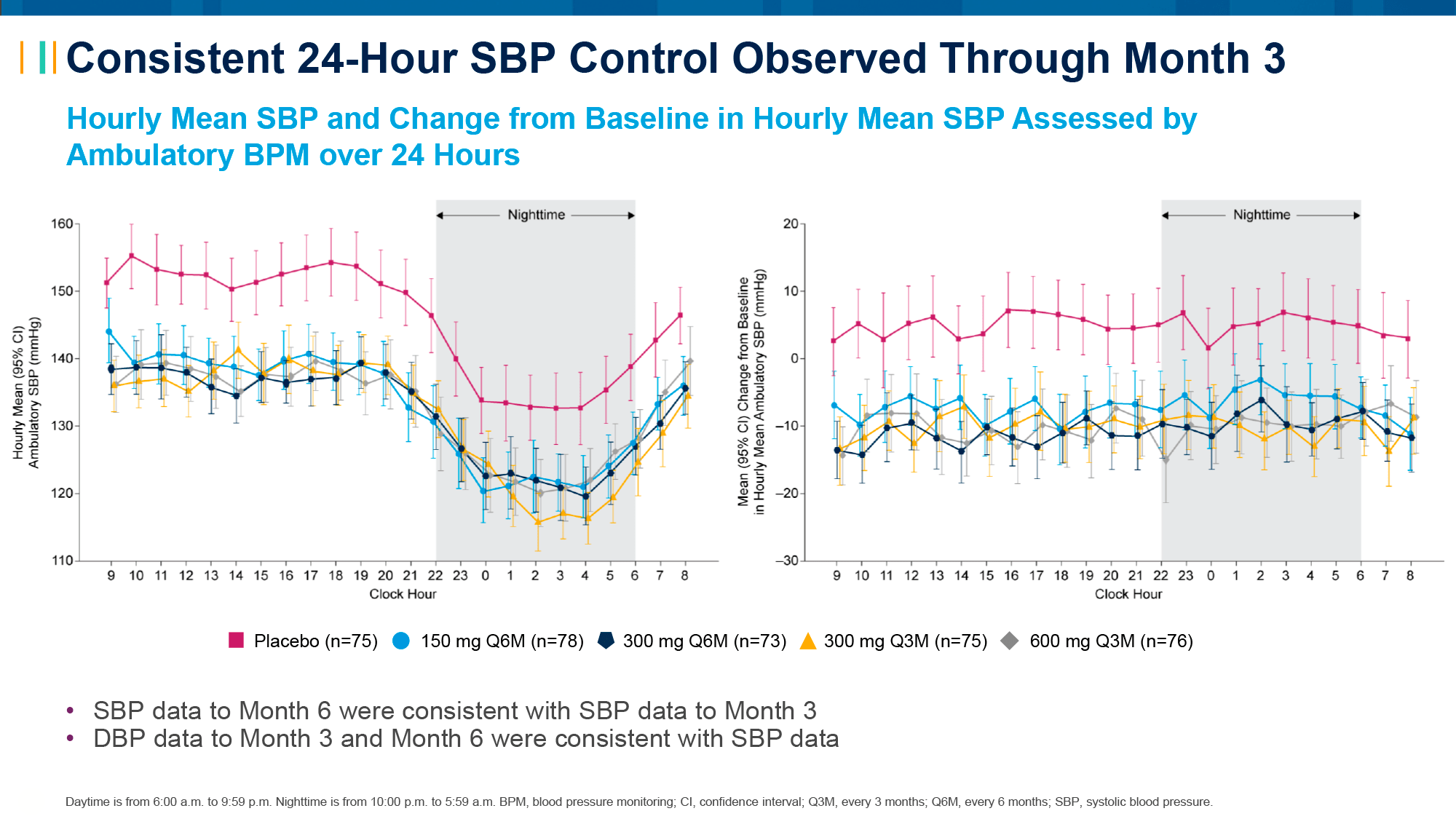
- The administration of zilebesiran at doses of 200 mg and above resulted in a stable and consistent reduction of both SBP и DBP throughout the day and night. This suggests the potential for achieving sustained blood pressure control over an extended period.
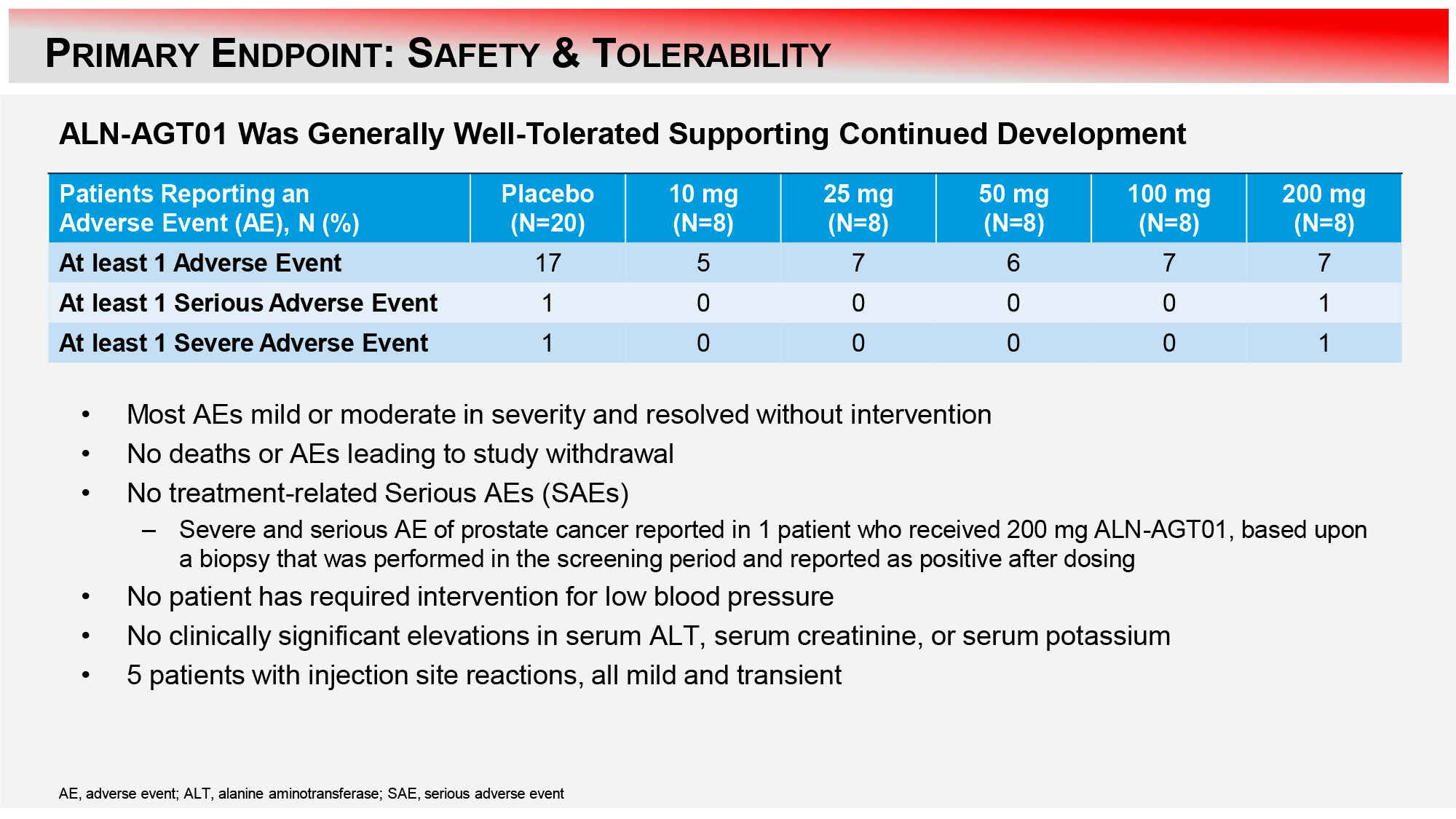
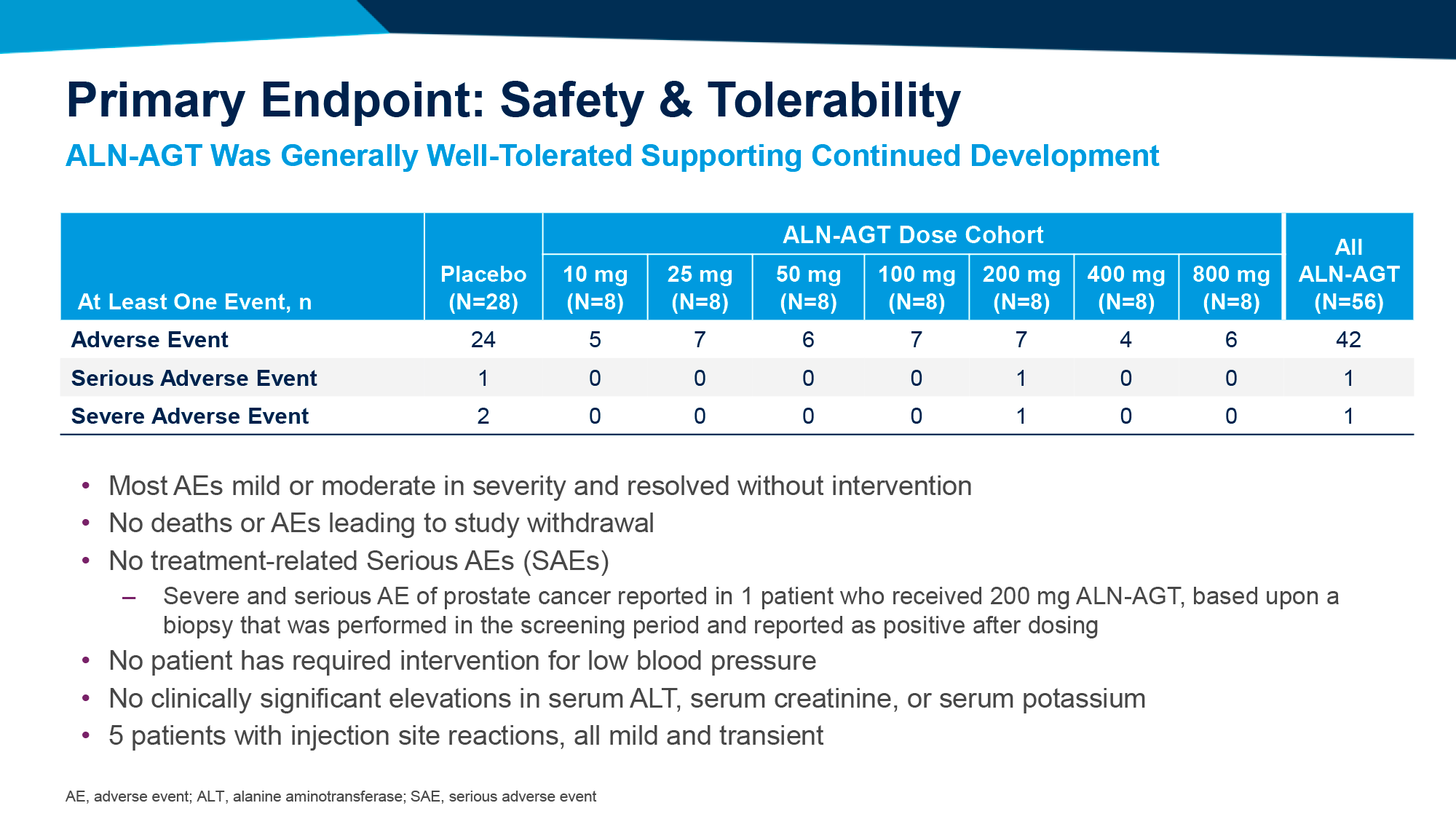
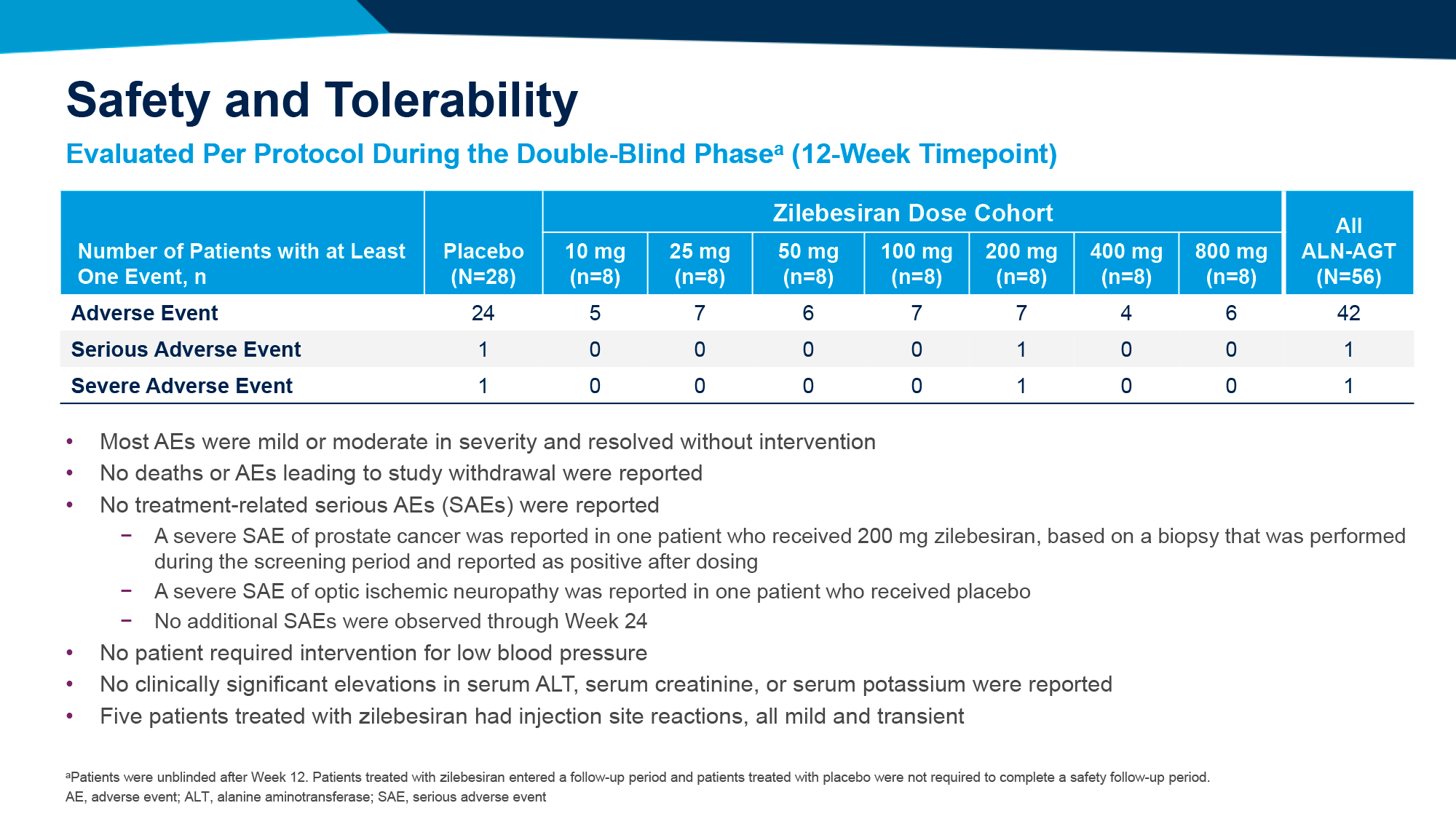
The tolerability of zilebesiran was found to be acceptable, with no serious adverse events (AEs) reported in response to its administration.
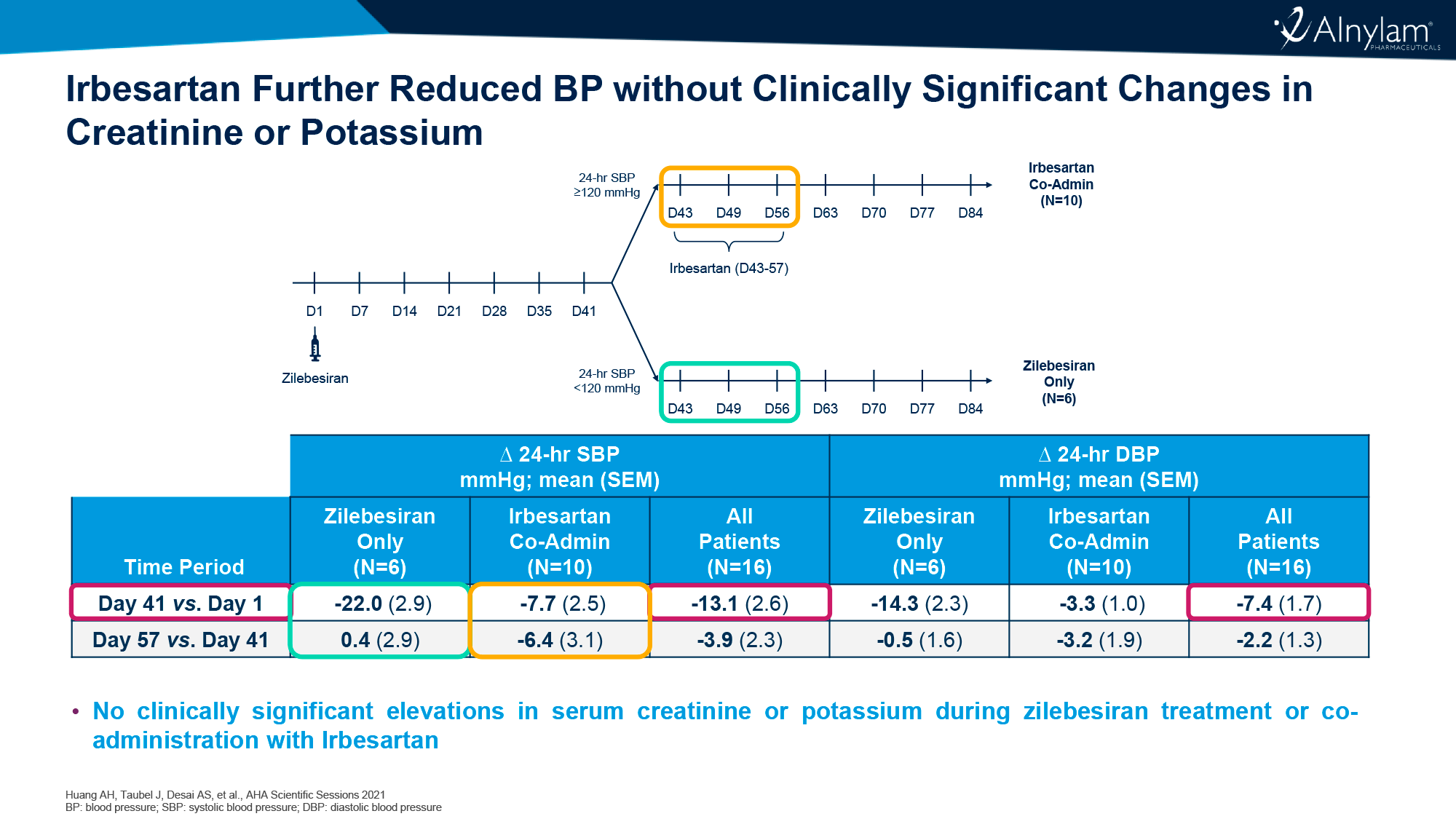
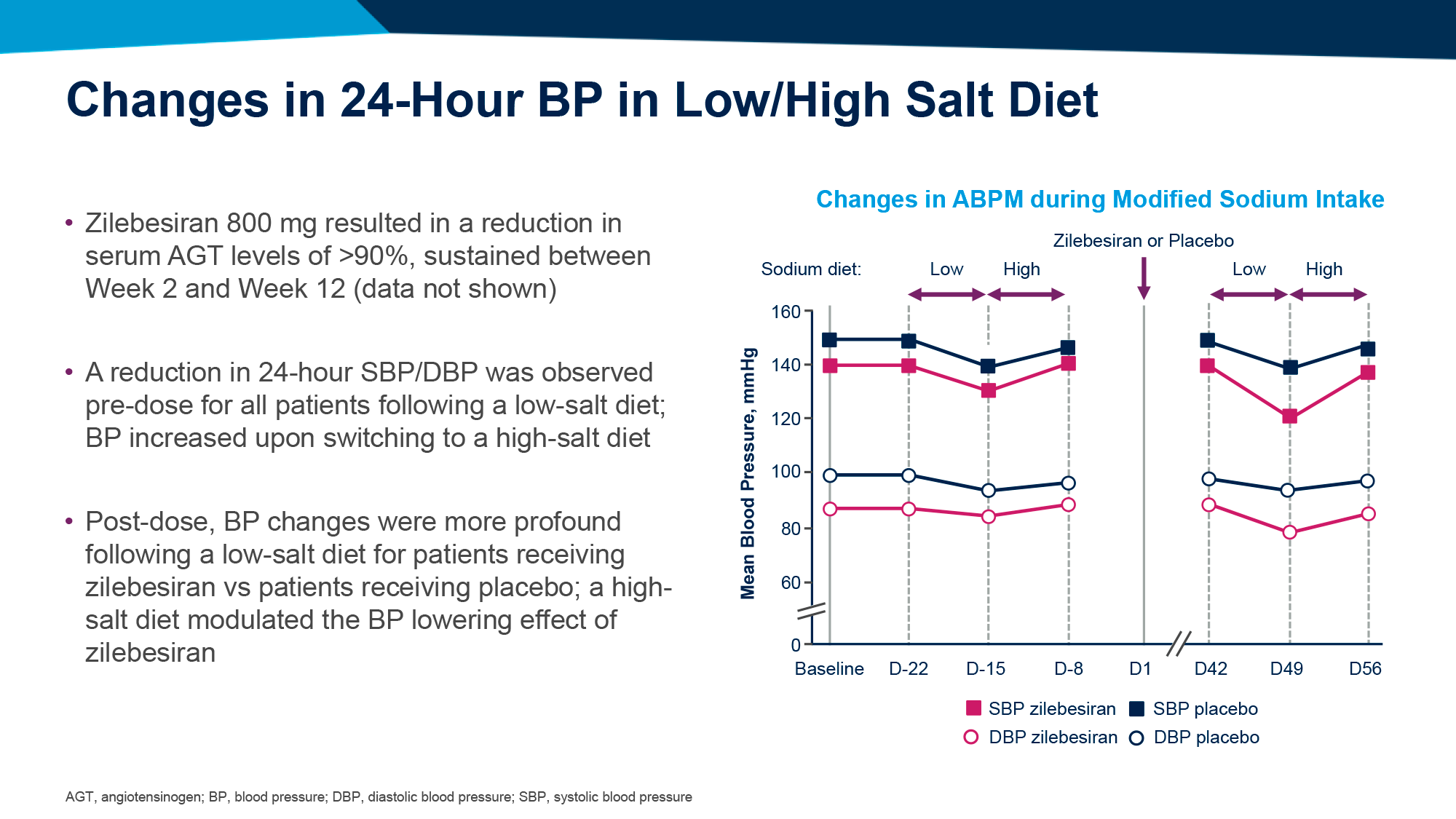
In addition, Alnylam Pharmaceuticals studied an 800-mg zilebesiran on a low-salt diet or concomitant daily administration of 300-mg irbesartan, an angiotensin II receptor blocker (ARB).
An evaluation of zilebesiran on the low-salt diet recommended for hypertensive patients was necessary to ascertain treatment tolerability due to the depletion of body fluid volume caused by sodium loss, which can lead to hypotensive events.
The addition of irbesartan resulted in additional reductions of 6.4 and 3.2 mmHg in SBP and DBP, with no clinically significant changes in serum creatinine and potassium levels.
The findings indicate that a low-salt diet exerts an additional effect, resulting in a more pronounced reduction in blood pressure. This may potentially lead to a reduction in blood pressure that is too low, prompting the consideration of a high-salt diet as a means of preventing hypotensive events.
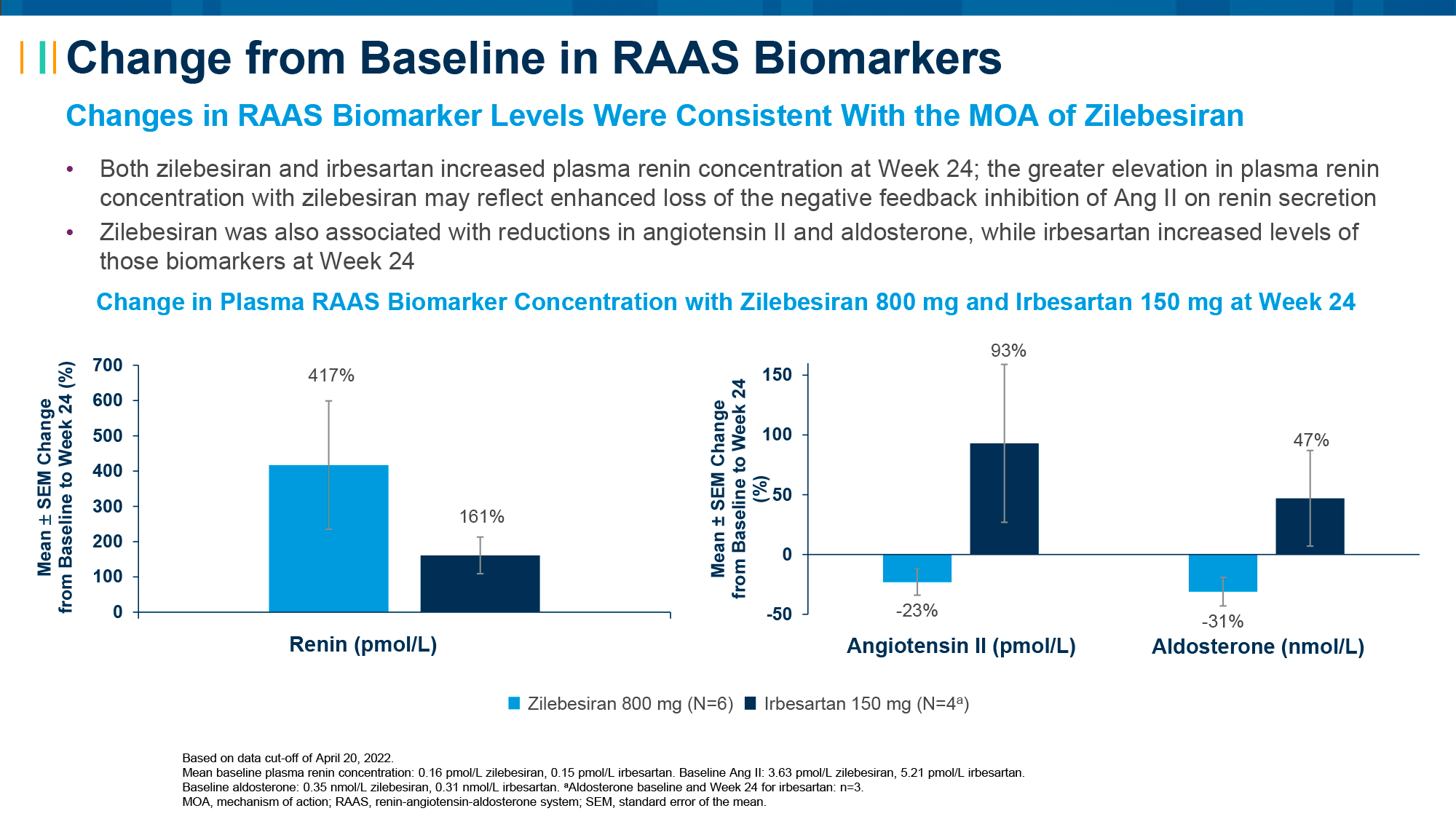
Alnylam also tested zilebesiran among patients with hypertension and class II or III obesity (body mass index [BMI] > 35 kg/m2) but without diabetes mellitus. A marked and sustained reduction in SBP was confirmed, with an increase in renin levels and a decrease in angiotensin II and aldosterone levels reflecting the mechanism of action.
KARDIA-1
The KARDIA-1 (NCT04936035) phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial tested the monotherapy of zilebesiran among adult patients (n=394) with mild to moderate hypertension (daytime mean systolic blood pressure [SBP] between 135 and 160 mmHg) who had not previously been treated for hypertension or who were following a stable course of antihypertensive medications (in either case, subjects were not taking them during the study) [1].
During the 6-month double-blind period, participants were randomly assigned to receive either zilebesiran at a dose of 150, 300, or 600 mg every 6 months or 300 mg 3 three months, or placebo every 3 months. In the subsequent 6-month open-label period, patients in the placebo group were switched to zilebesiran.
Two methods were employed to assess changes in blood pressure (in mmHg) relative to placebo: 24-hour ambulatory blood pressure monitoring (ABPM) and a single blood pressure measurement with a sphygmomanometer (in-office).
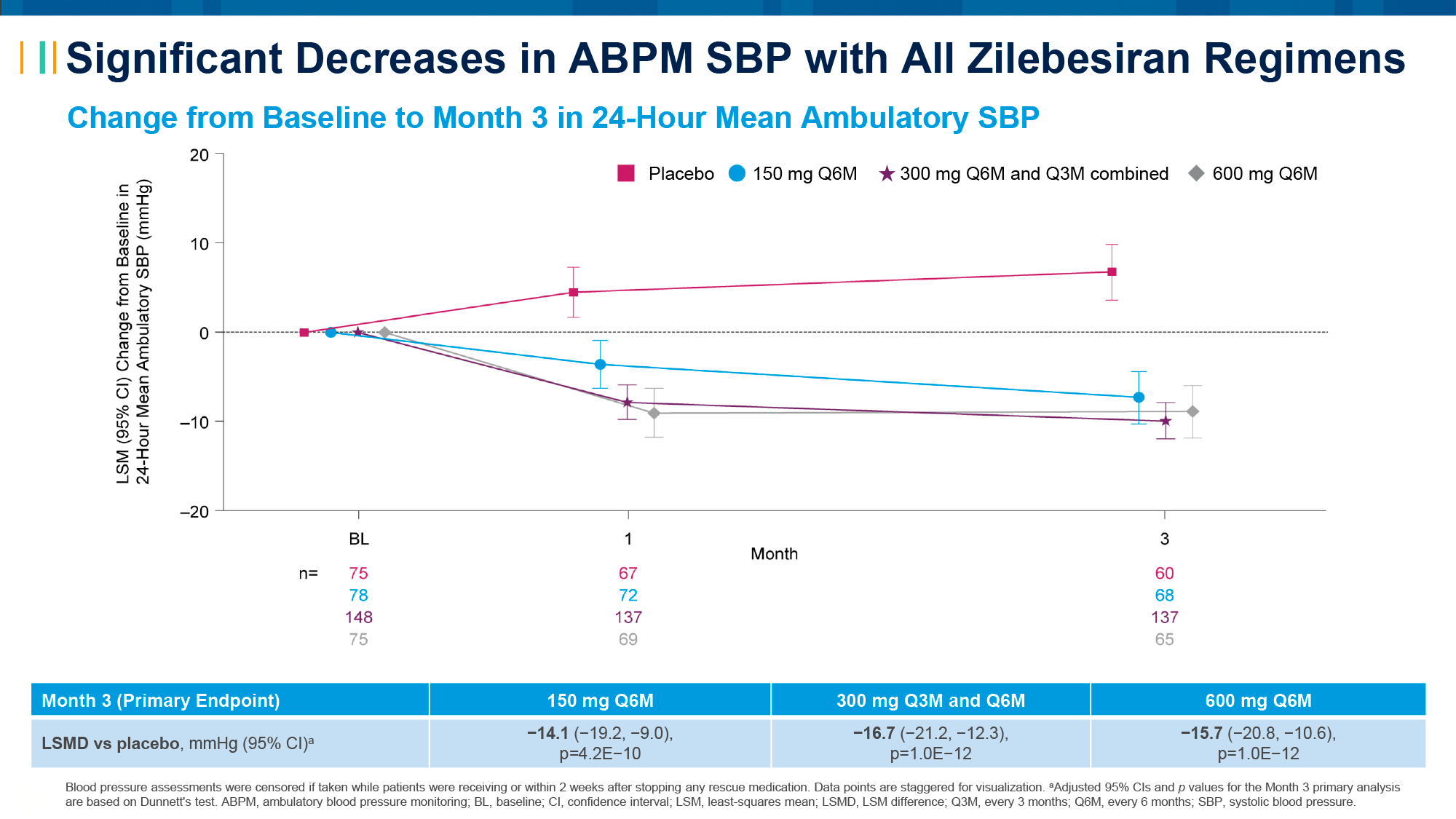
The results were as follows [2] [3] [4].
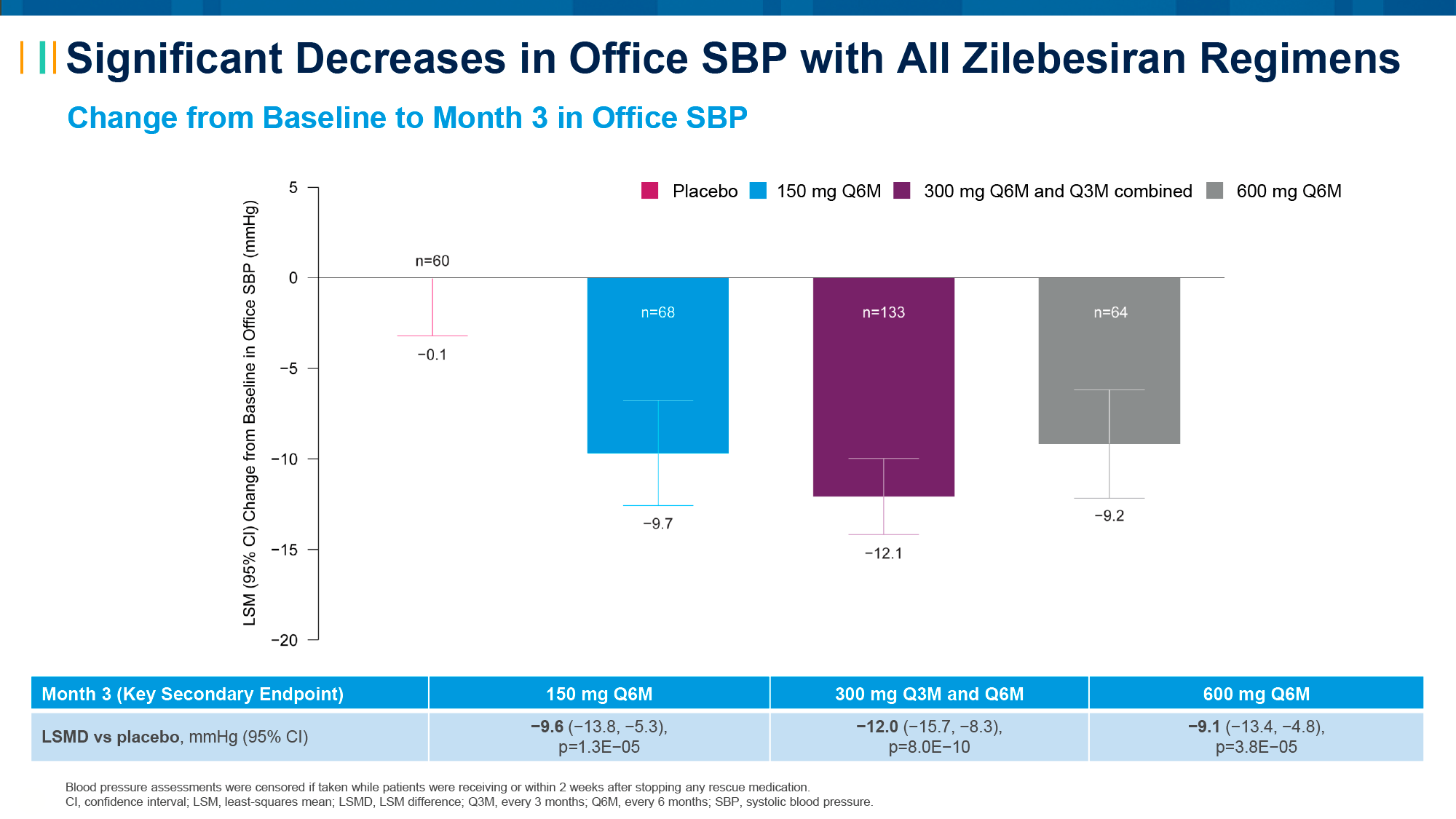
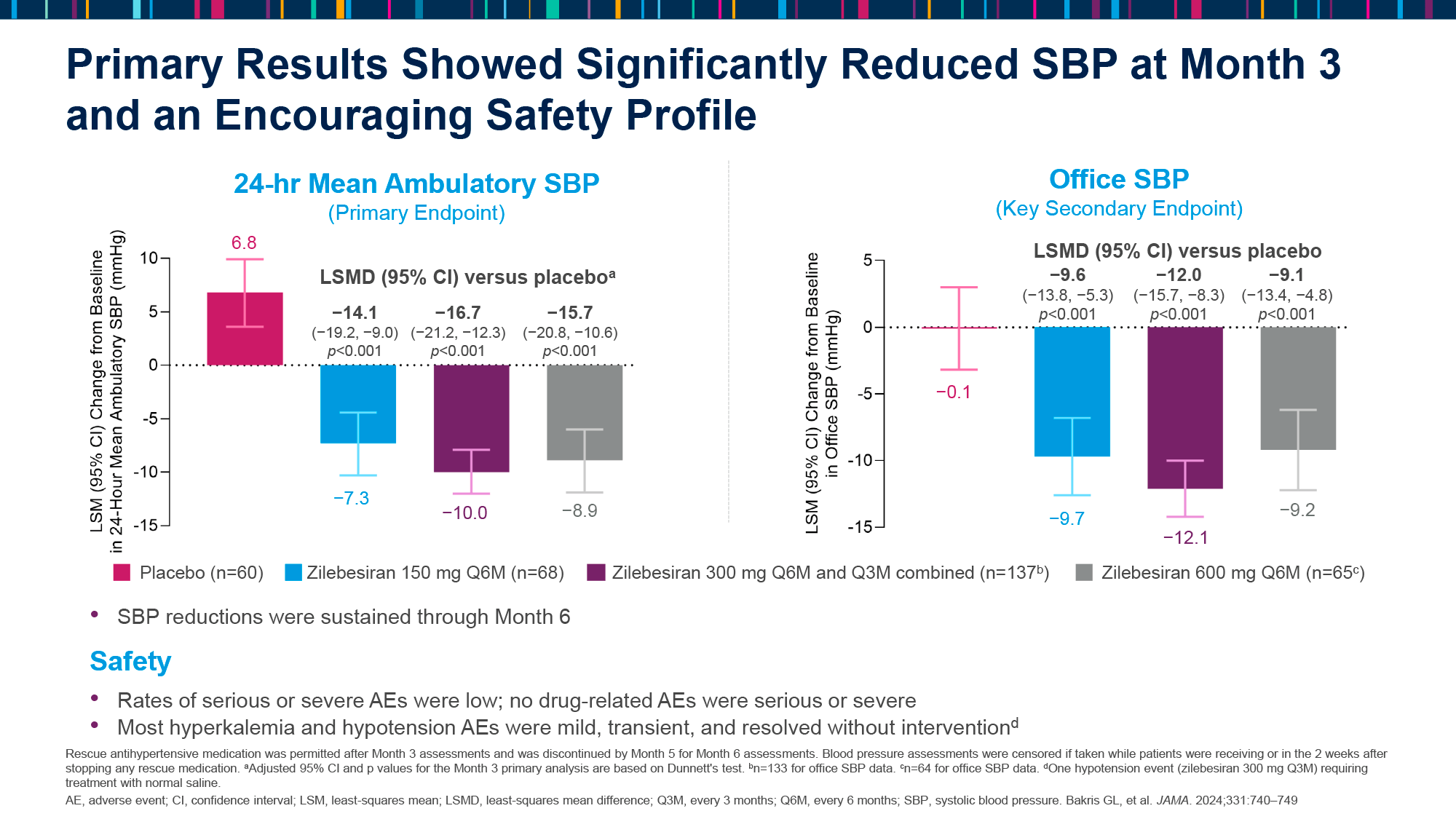
After 3 months, the change in SBP by ABPM was −14.1 (95% CI [hereinafter]: −19.2, −9.0), −16.7 (−21.2, −12.3), and −15.7 (−20.8, −10.6) in subjects who received zilebesiran at doses of 150 mg (every 6 months), 300 mg (every 3 or 6 months), and 600 mg (every 6 months) [p<0.0001].
- The change in SBP by in-office was −9.6 (−13.8, −5.3), −12.0 (−15.7, −8.3), and −9.1 (−13.4, −4.8) [p<0.0001].
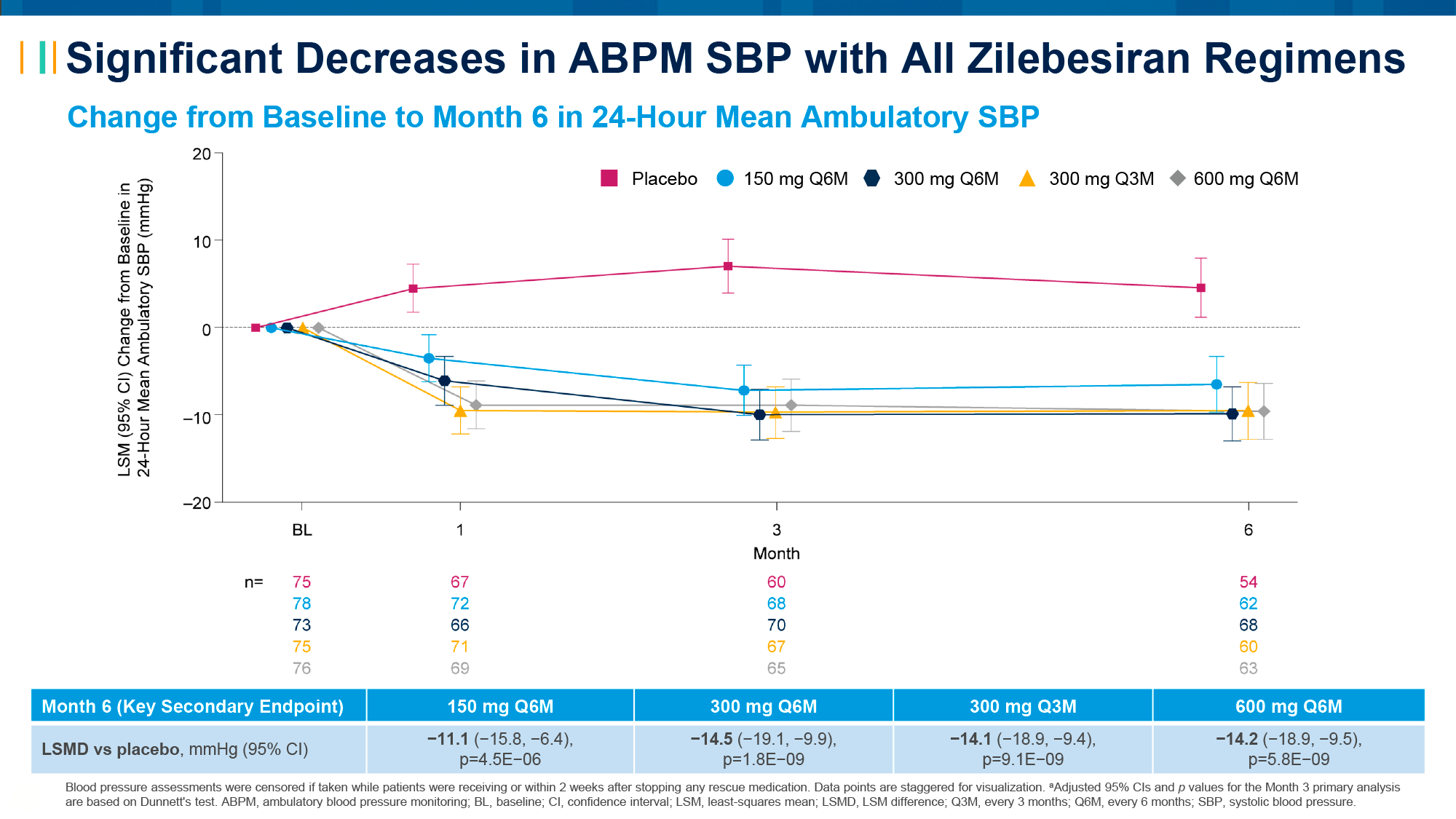
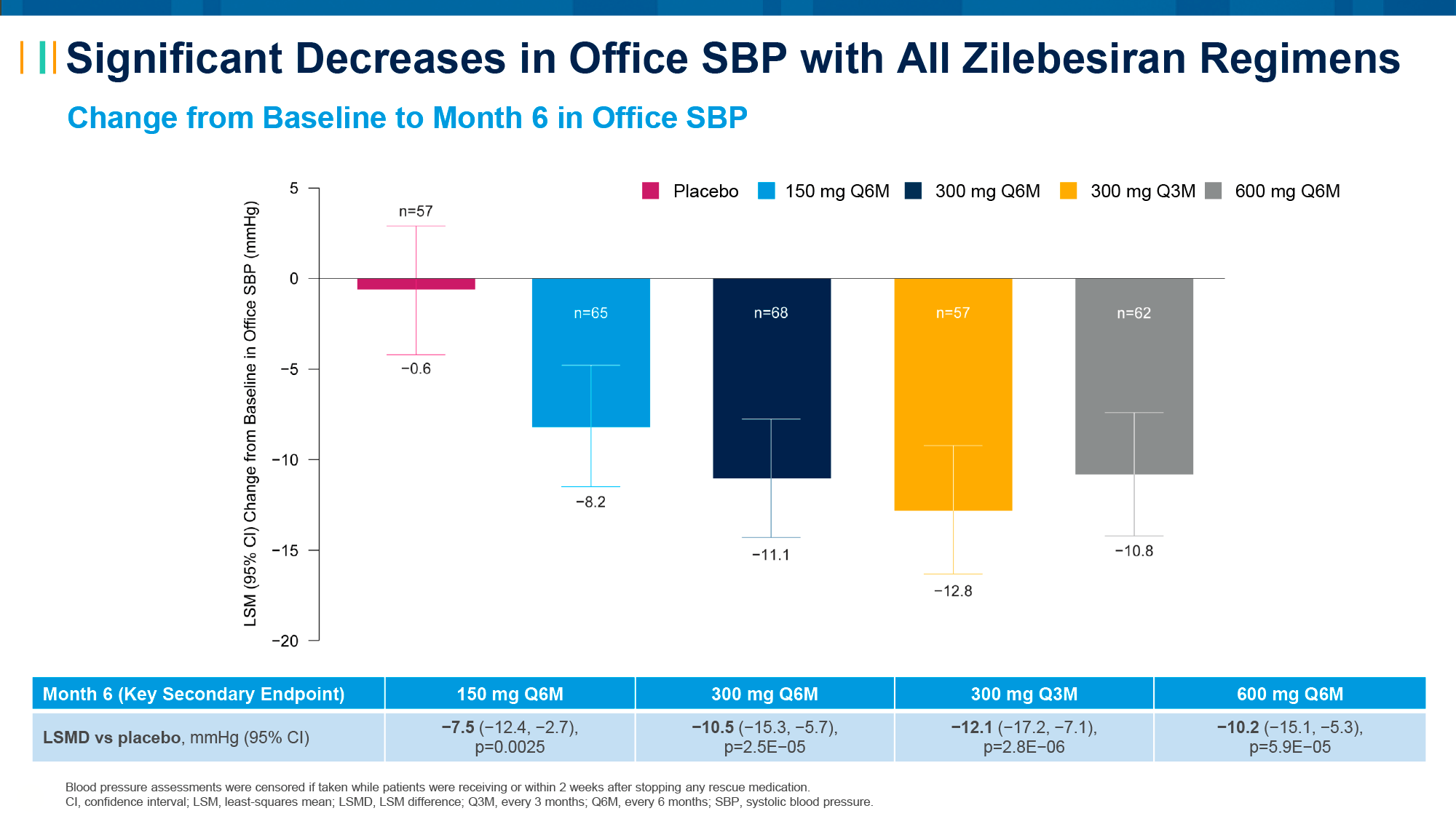
After 6 months, the change in SBP by ABPM was −11.1 (−15.8, −6.4), −14.5 (−19.1, −9.9), −14.1 (−18.9, −9.4), and −14.2 (−18.9, −9.5) in subjects who received zilebesiran at doses of 150 mg (every 6 months), 300 mg (every 6 months), 300 mg (every 3 months), and 600 mg (every 6 months) [p<0.0001].
- The change in SBP by in-office was −7.5 (−12.4, −2.7), −10.5 (−15.3, −5.7), −12.1 (−17.2, −7.1), and −10.2 (−15.1, −5.3) [p=0.0025, p<0.0001].
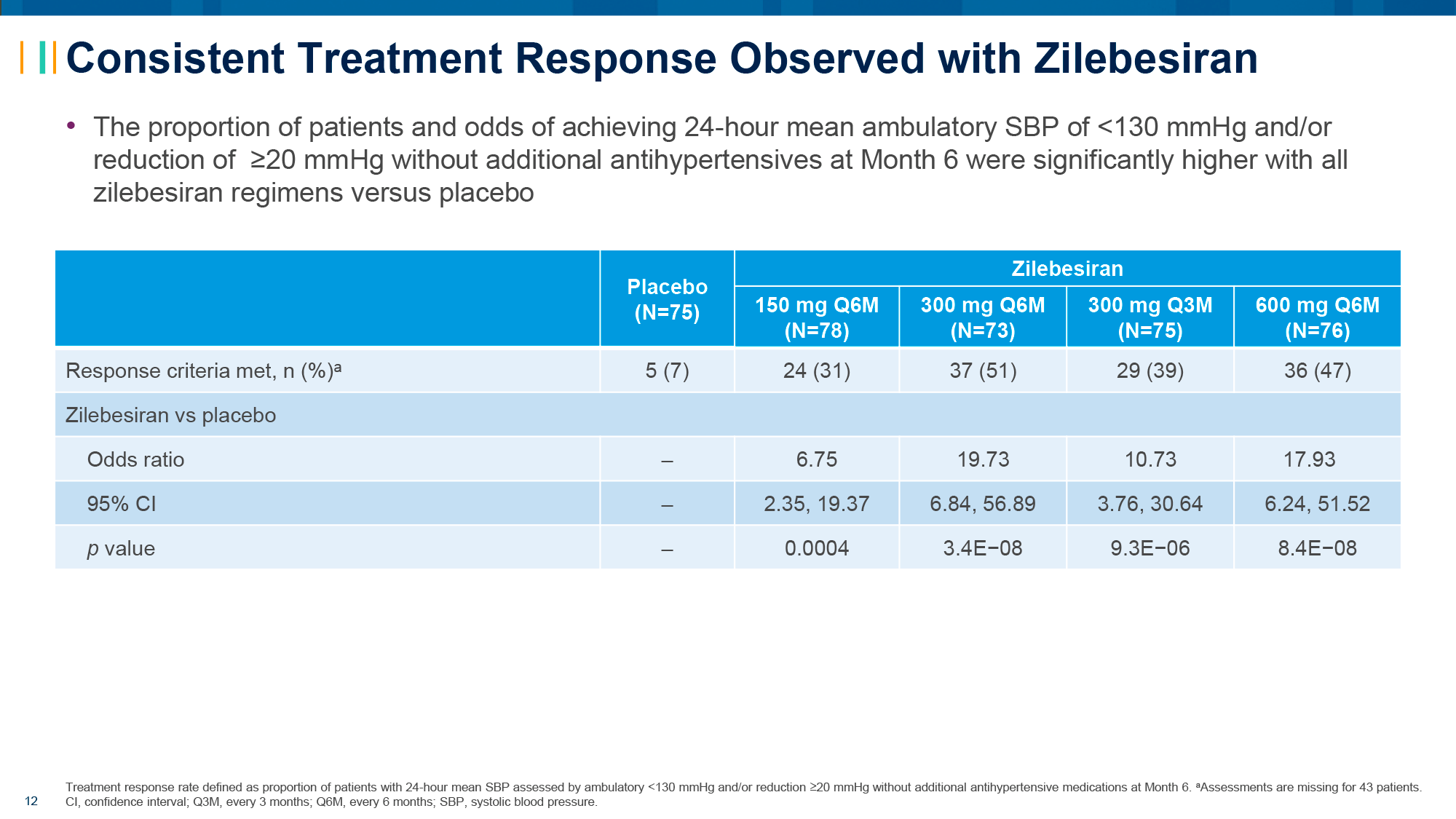
The proportions of patients who responded to treatment, defined as achieving SBP < 130 mmHg and/or SBP reduction of ≥ 20 mmHg without additional antihypertensive medication, at 6 months were 7%, 31%, 51%, 39%, and 47% for participants receiving placebo and zilebesiran at doses of 150 mg (every 6 months), 300 mg (every 6 months), 300 mg (every 3 months), and 600 mg (every 6 months), respectively. The corresponding odds ratios (OR) for achieving a response for the zilebesiran subgroups were 6.8 (2.4–19.4), 19.7 (6.8–56.9), 10.7 (3.8–30.6), and 17.9 (6.2–51.5) [p<0.0001].
Zilebesiran produced consistent and sustained blood pressure reductions throughout the diurnal cycle, including overnight.
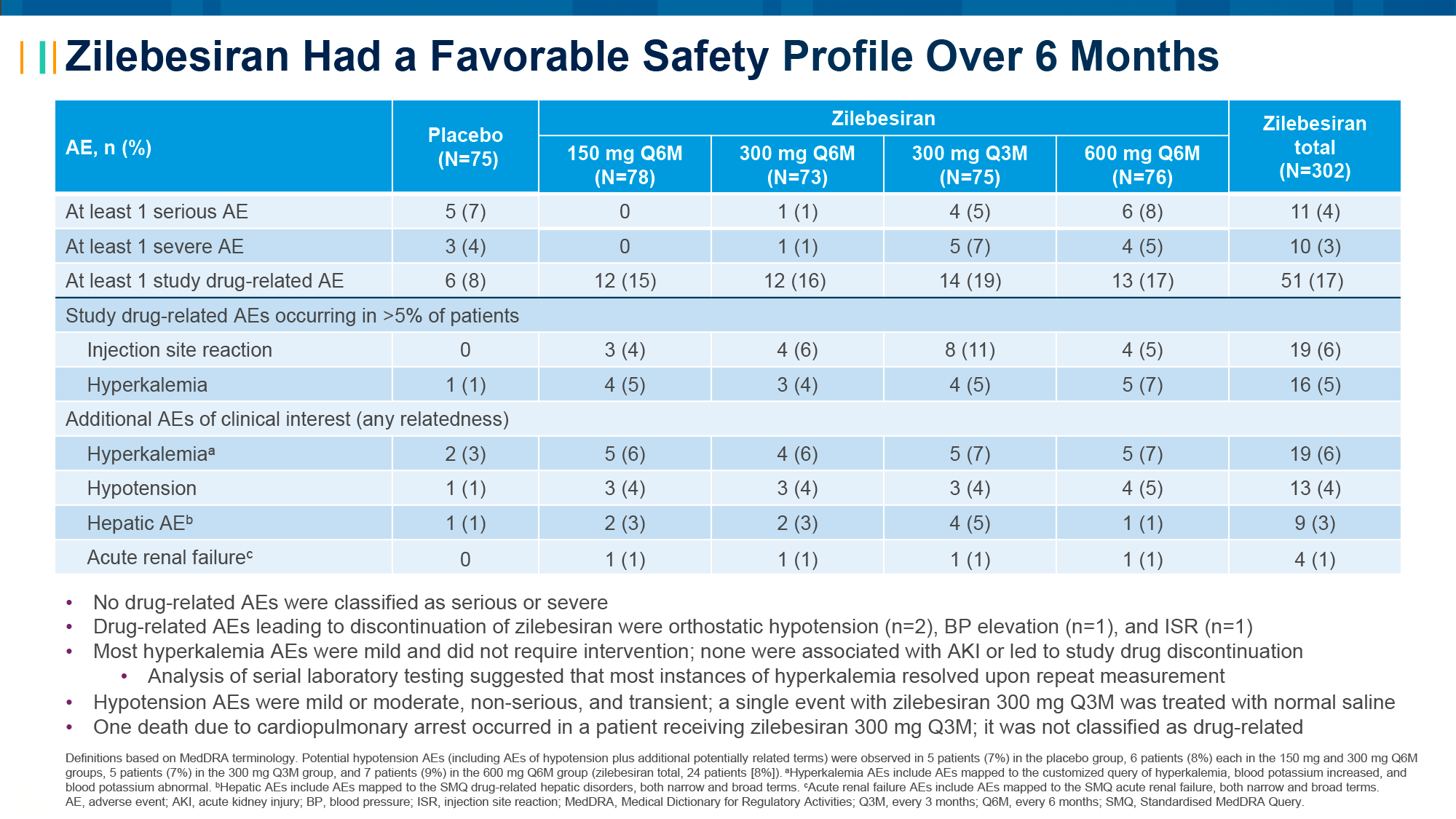
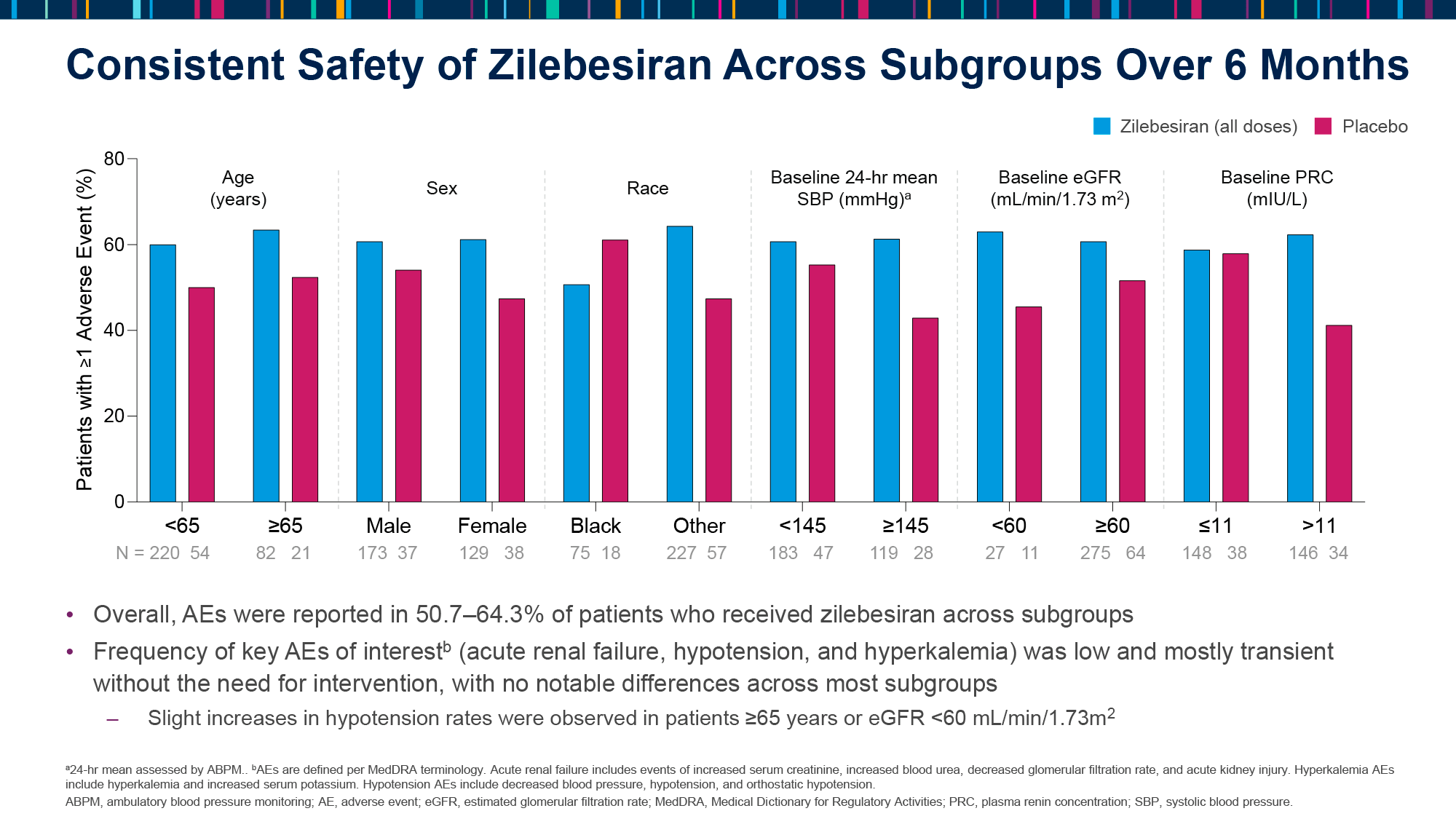
Zilebesiran was well tolerated. Adverse events (AEs) related to hyperkalemia (in 5% of patients receiving zilebesiran — versus 1% in the placebo group) were mild, transient, and resolved without intervention. The number of cases of hypotension was low (4% vs. 1%). No clinically significant changes in renal or hepatic function were observed. Rare cases of serious AEs (4% vs. 7%) and severe AEs (3% vs. 4%) were reported.
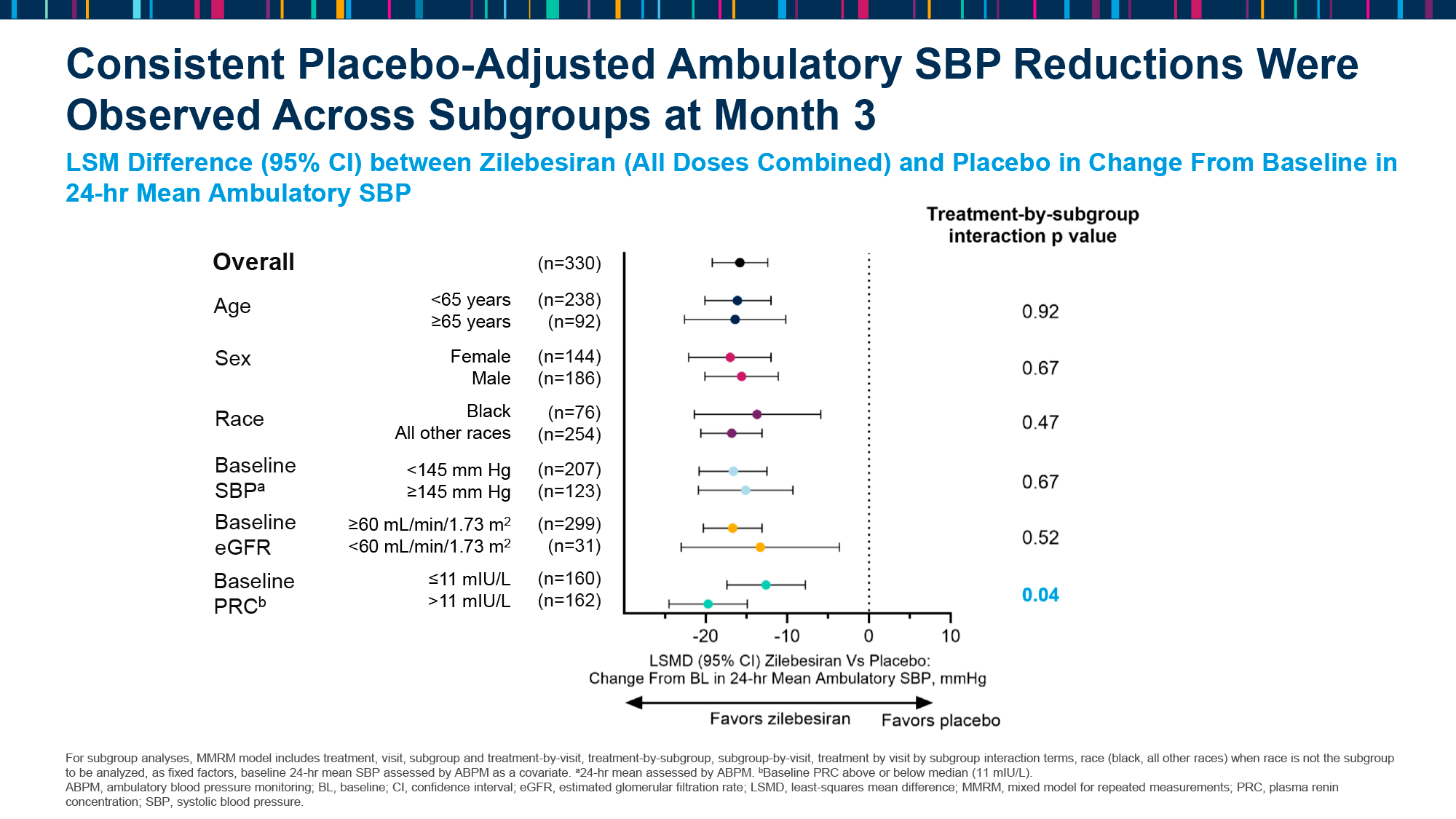
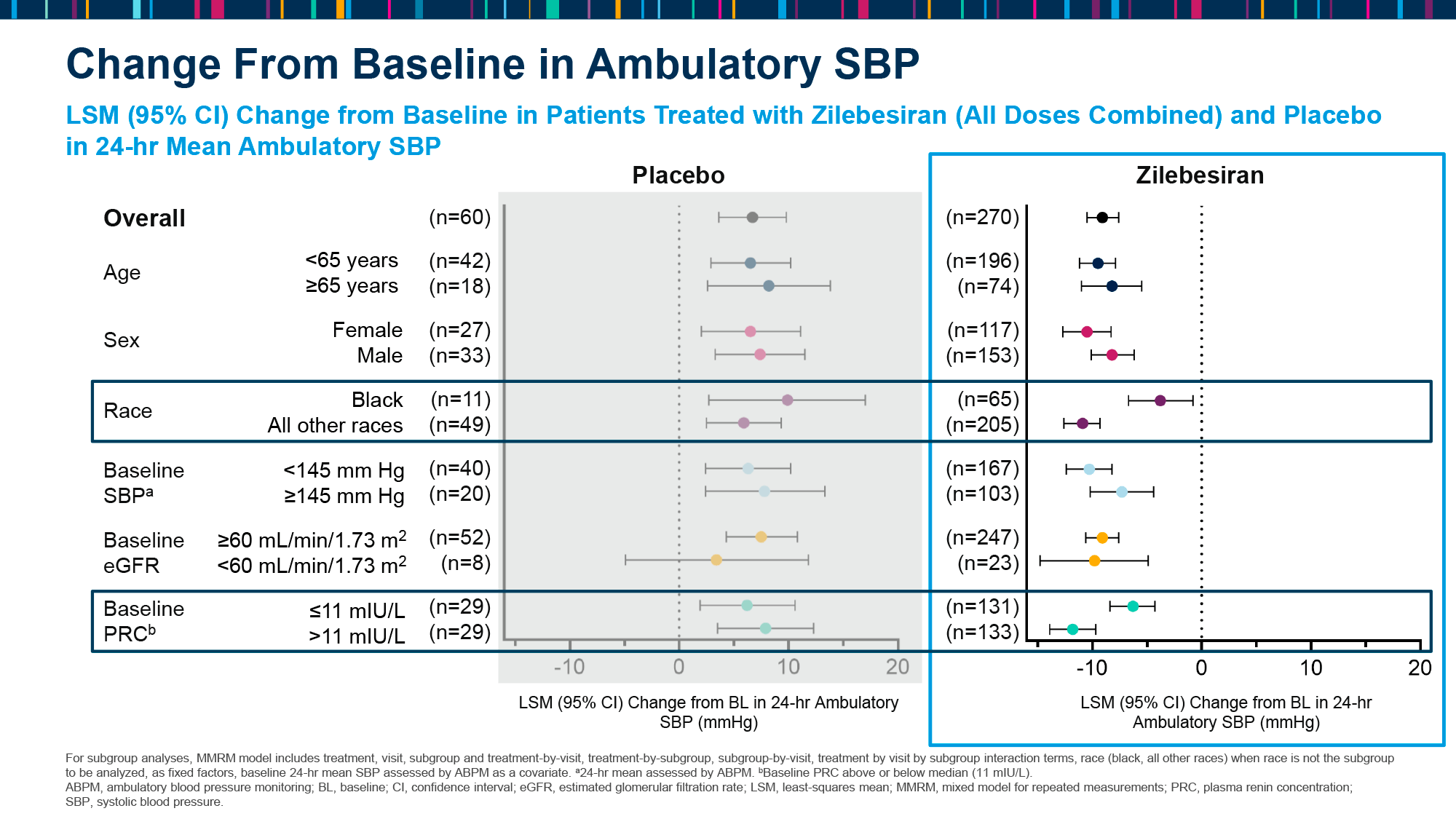
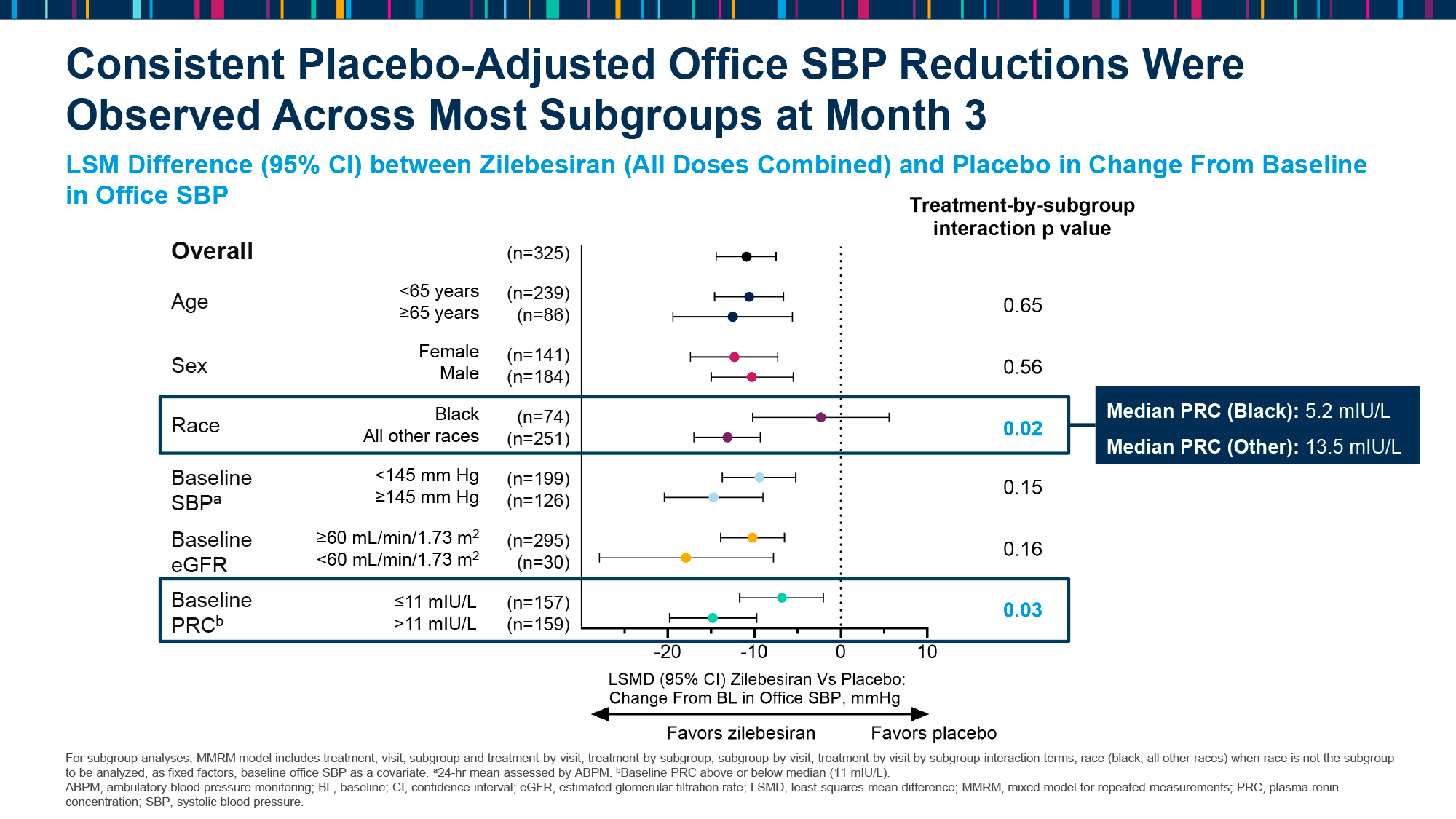
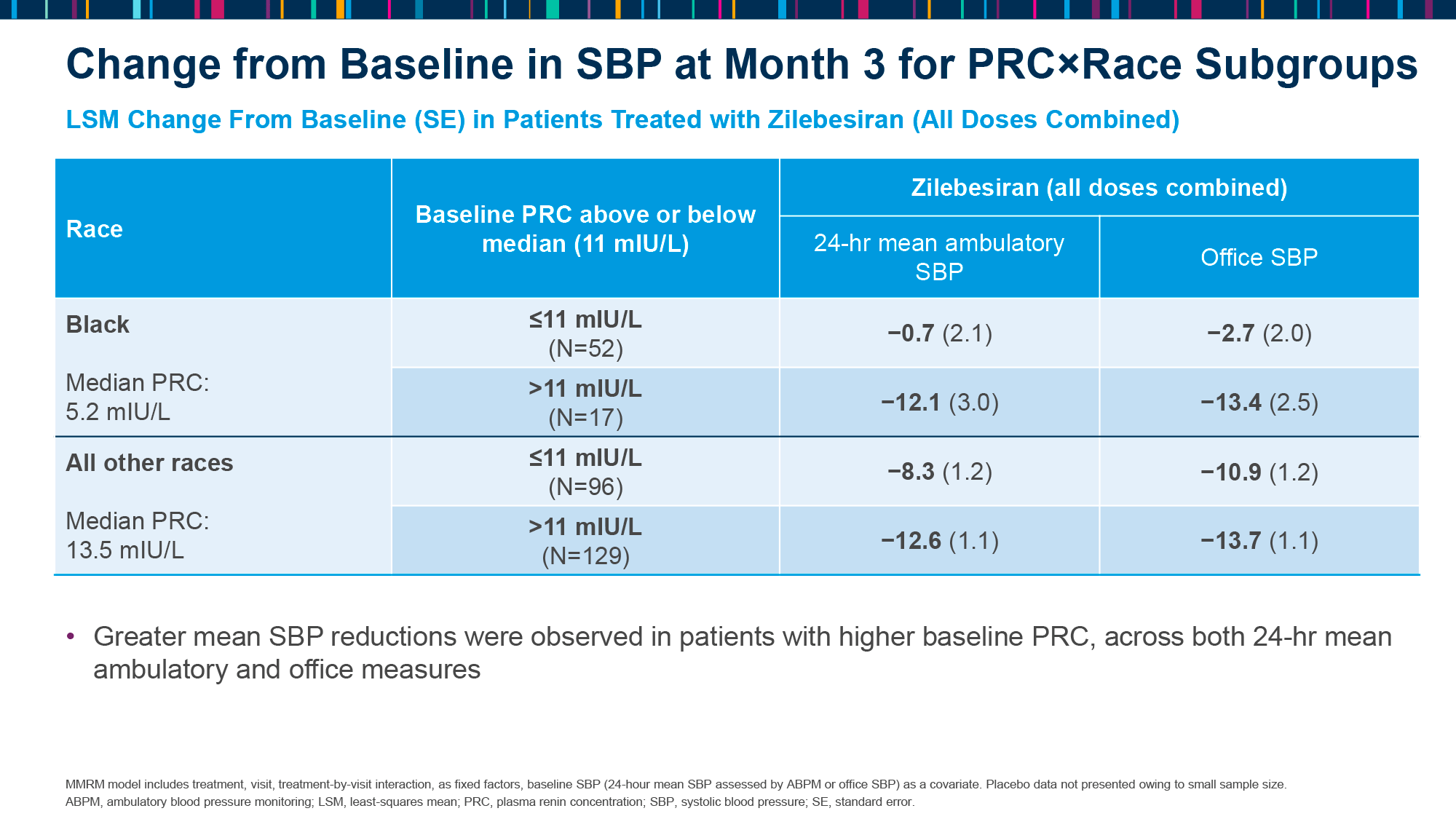
Further analysis revealed that zilebesiran was effective in reducing SBP, regardless of sex, age, race, baseline SBP, or estimated glomerular filtration rate (eGFR). However, initial plasma renin concentration (PRC) in black patients appeared to influence the degree of SBP reduction, with lower PRC resulting in less pronounced blood pressure reductions [5].
KARDIA-2
The KARDIA-2 (NCT05103332) phase 2 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial evaluated the addition of zilebesiran to antihypertensive therapy in adult patients (n=800) with drug-resistant hypertension that inadequately controlled on current medication.
Inclusion criteria included a daytime mean systolic blood pressure (SBP) between 155 and 180 mmHg or 145 and 180 mmHg (for previously untreated hypertension and hypertension treated with one to two antihypertensive drugs, respectively), which had to be reduced to between 130 and 160 mmHg after the run-in period of the study.
The 4-week run-in period required to equalize baseline SBP included a single daily dose of a specific antihypertensive medication: 2.5 mg of the diuretic indapamide, 40 mg of the angiotensin II receptor blocker (ARB) olmesartan, or 5 mg of the calcium channel blocker (CBR) amlodipine [1].
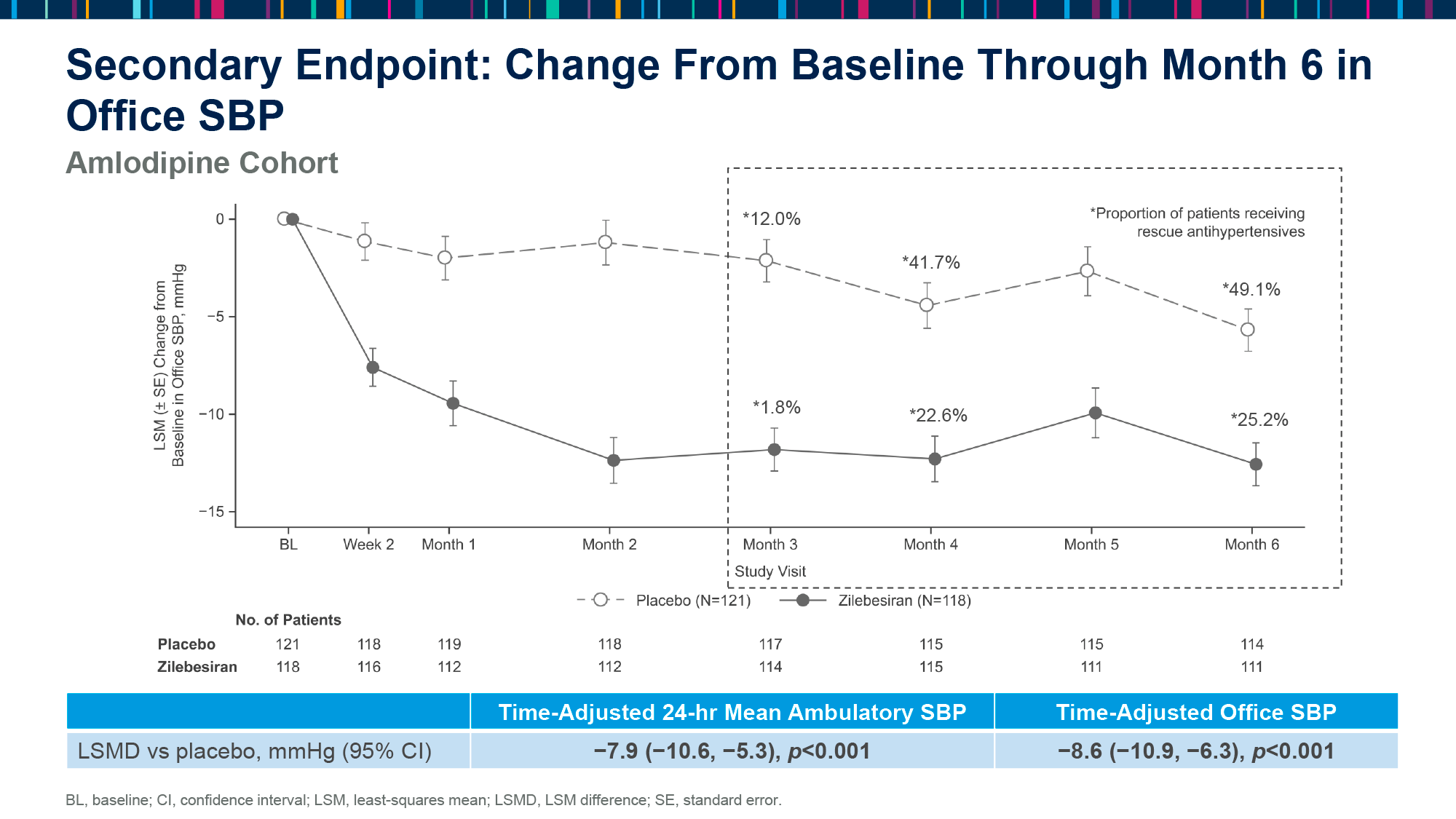
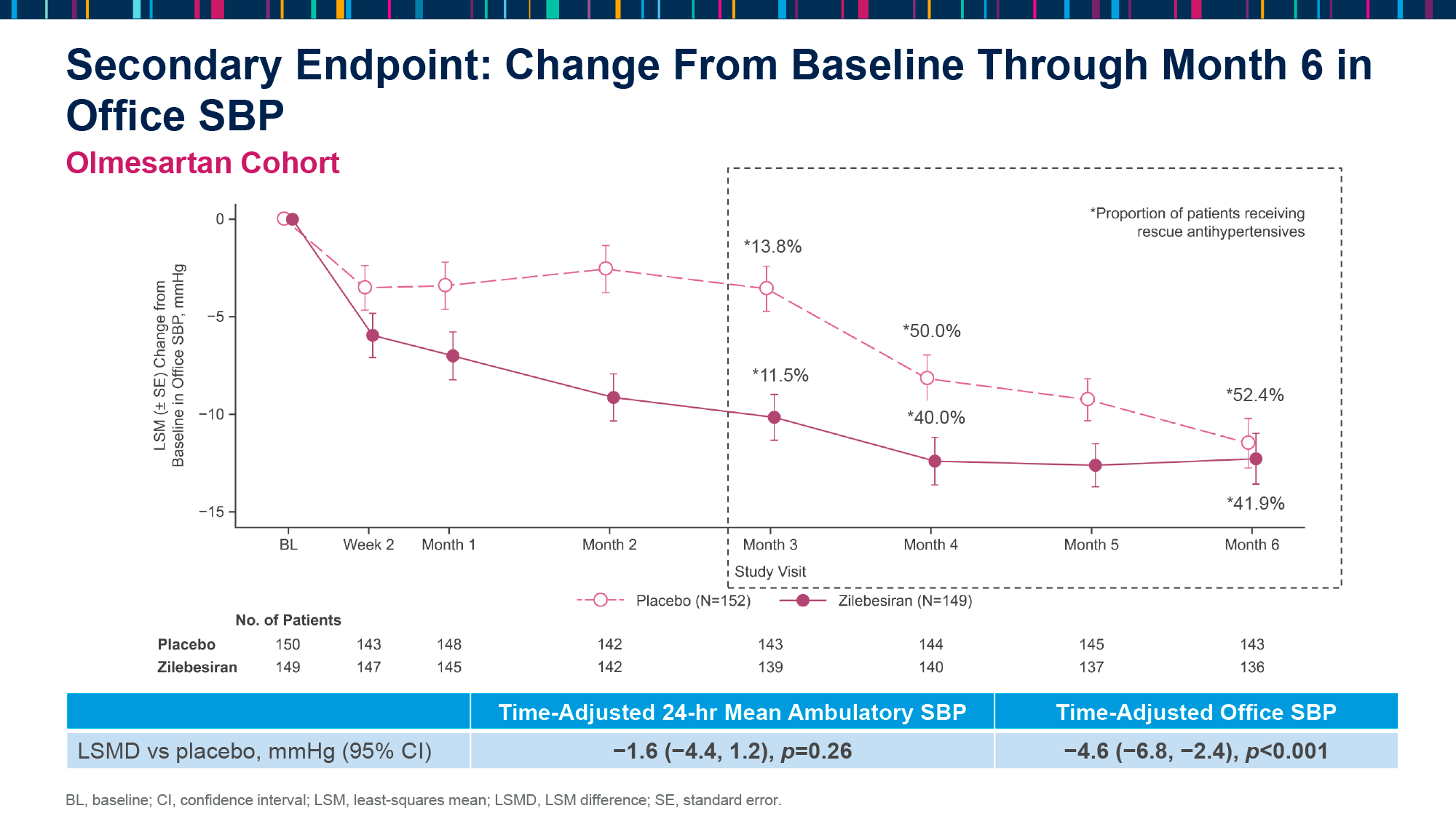
In a subsequent 6-month double-blind period, participants received a single subcutaneous injection of 600 mg of zilebesiran or placebo while continuing to take their previously selected antihypertensive medication daily (additional medication could be added after 3 months if hypertension was not controlled).
Two methods were employed to assess changes in blood pressure (in mmHg) relative to placebo: 24-hour ambulatory blood pressure monitoring (ABPM) and a single blood pressure measurement with a sphygmomanometer (in-office).
The results were as follows [2] [3].
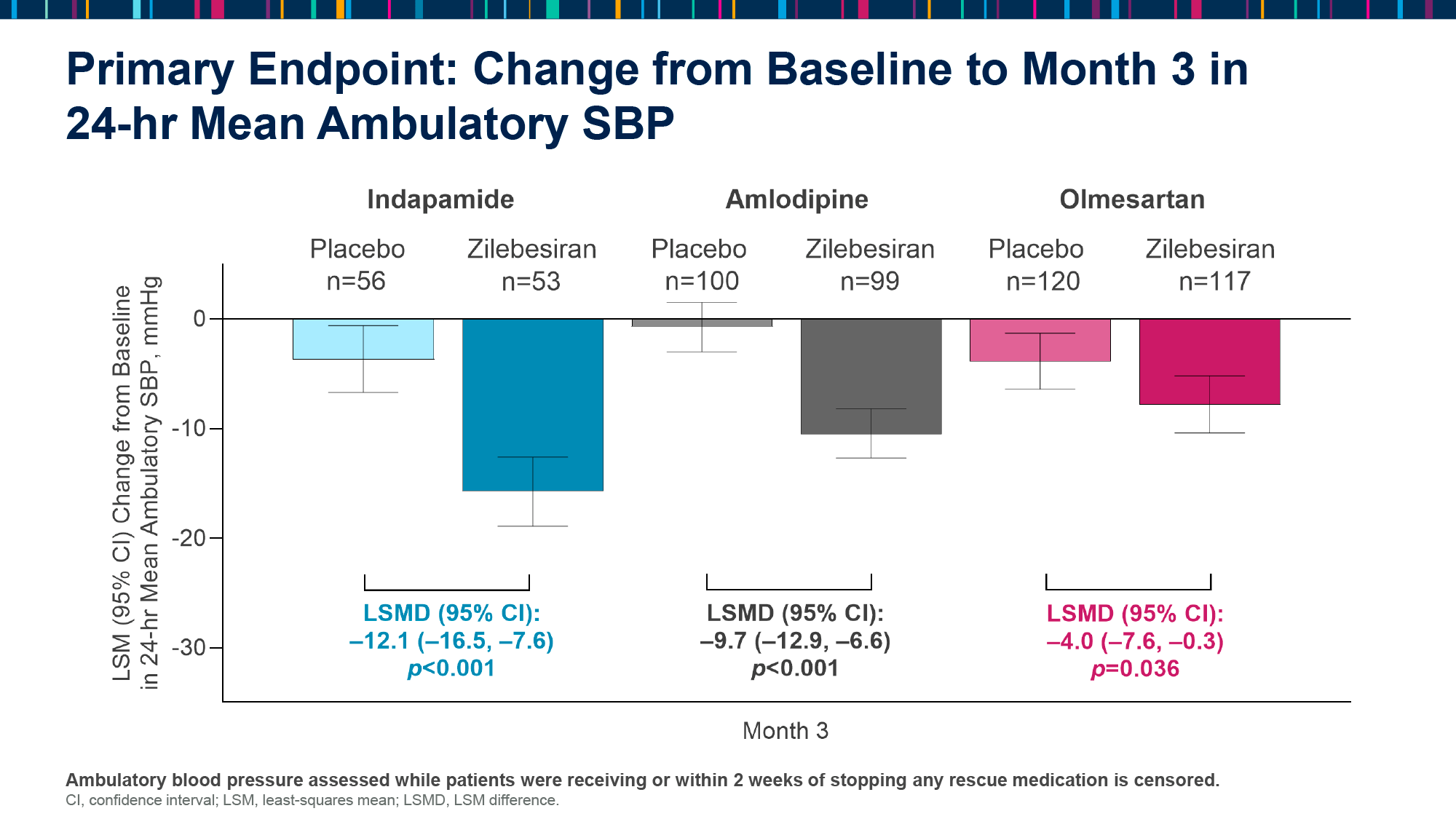
After 3 months, the change in SBP by ABPM was −12.1 (95% CI [hereinafter]: −16.5, −7.6), −9.7 (−12.9, −6.6), and −4.0 (−7.6, −0.3) in subjects receiving zilebesiran and adhering to daily antihypertensive therapy with indapamide, amlodipine, or olmesartan (p<0.001, p<0.001, and p=0.036).
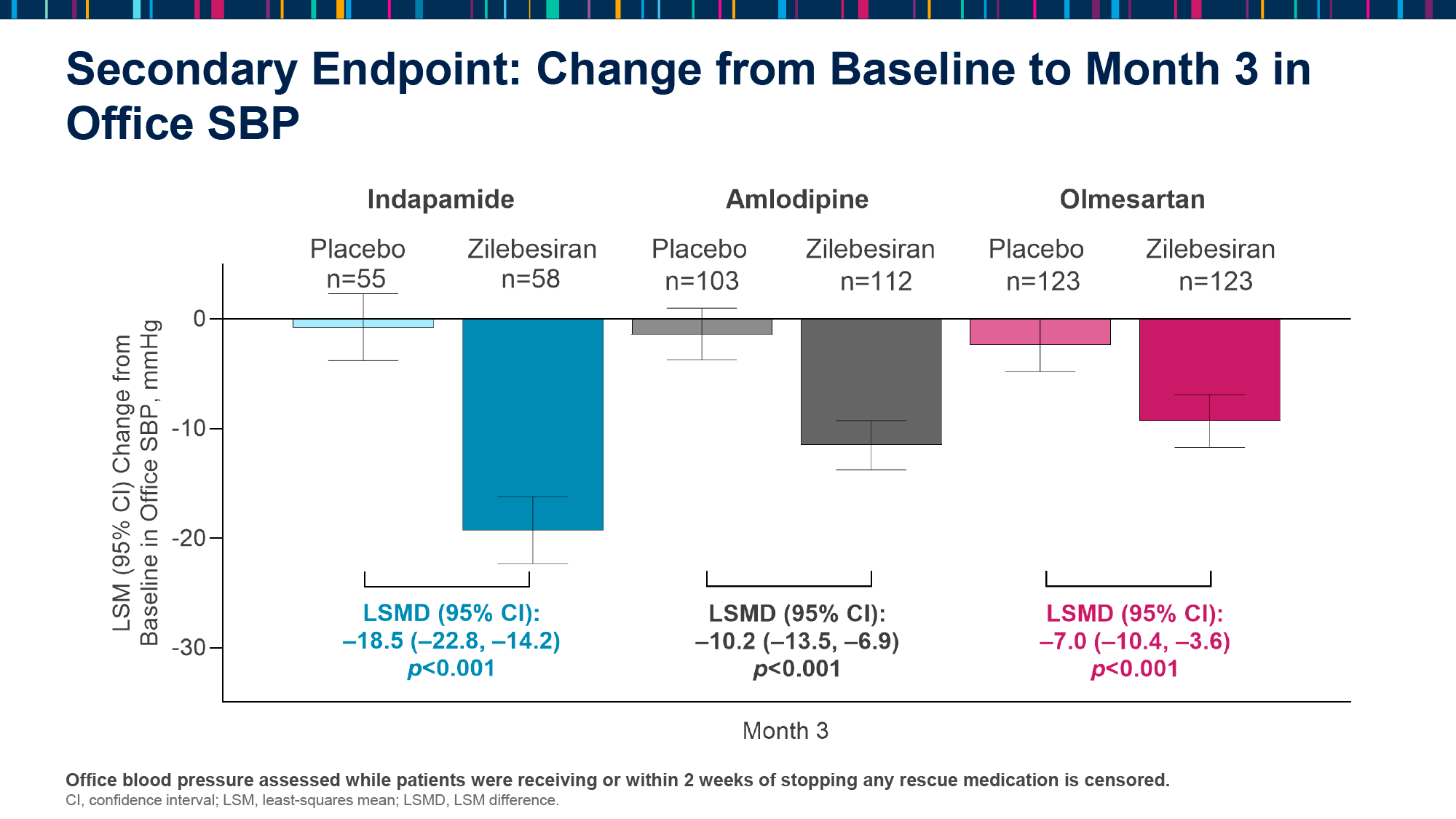
- The change in SBP by in-office was −18.5 (−22.8, −14.2), −10.2 (−13.5, −6.9), and −7.0 (−10.4, −3.6) [p<0.001].
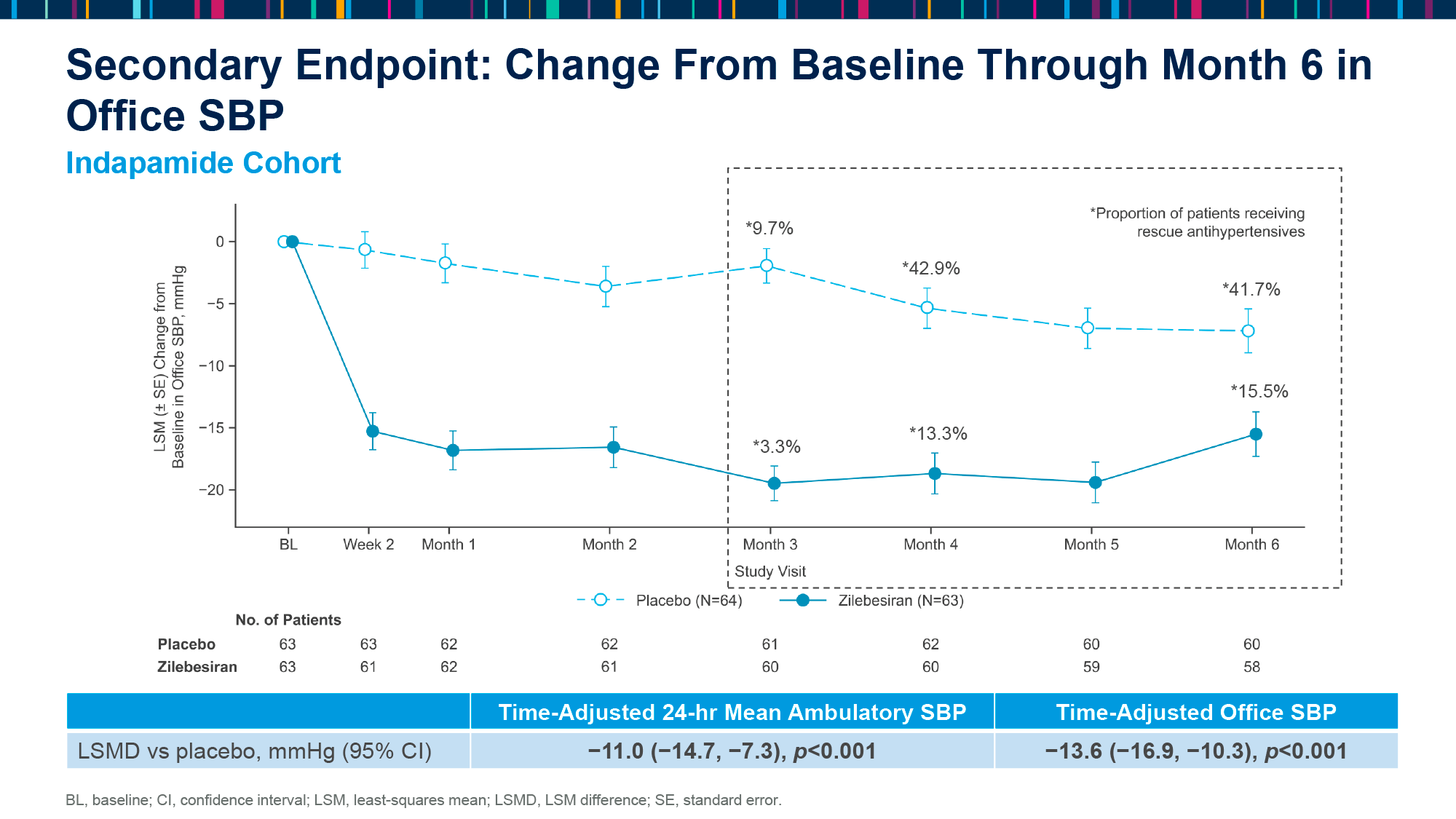
After 6 months, the change in SBP by ABPM was −11.0 (−14.7, −7.3), −7.9 (−10.6, −5.3), and −1.6 (−4.4, −1.2) [p<0.001, p<0.001, and p=0.26].
- The change in SBP by in-office was −13.6 (−16.9, −10.3), −8.6 (−10.9, −6.3), and −4.6 (−6.8, −2.4) [p<0.001].
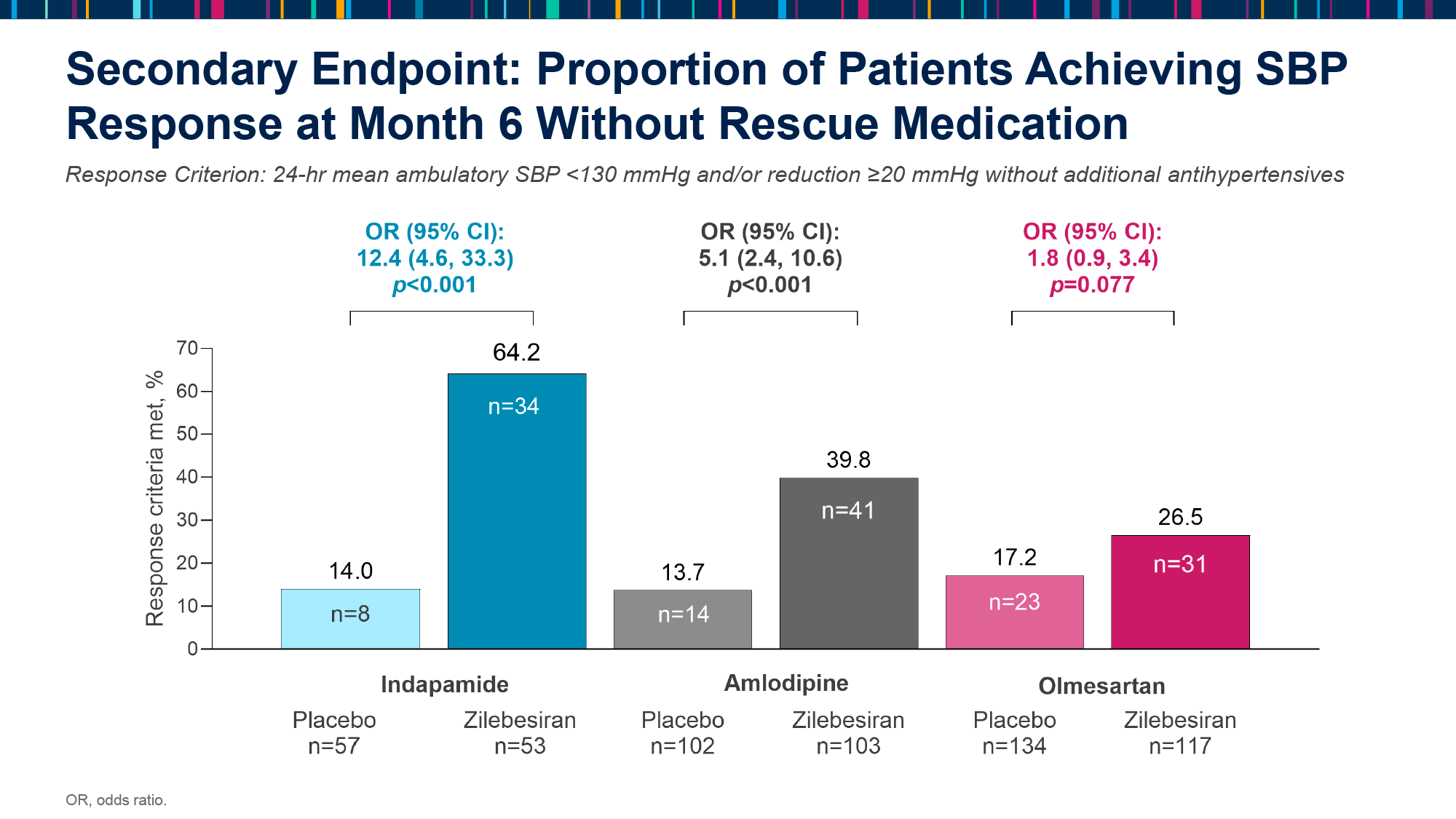
The proportions of patients who responded to treatment, defined as achieving by SBP < 130 mmHg and/or SBP reduction of ≥ 20 mmHg without additional (to already given) antihypertensive medication, at 6 months were 4%, 40%, and 27% in participants who received zilebesiran and then followed indapamide, amlodipine, or olmesartan. In the placebo subgroups, the proportions were 14%, 14% and 17%. The corresponding odds ratios (OR) for achieving a response for the zilebesiran subgroups were 12.4 (4.6–33.3), 5.1 (2.4–10.6), and 1.8 (0.9–3.4) [p<0.001, p<0.001, and p=0.077].
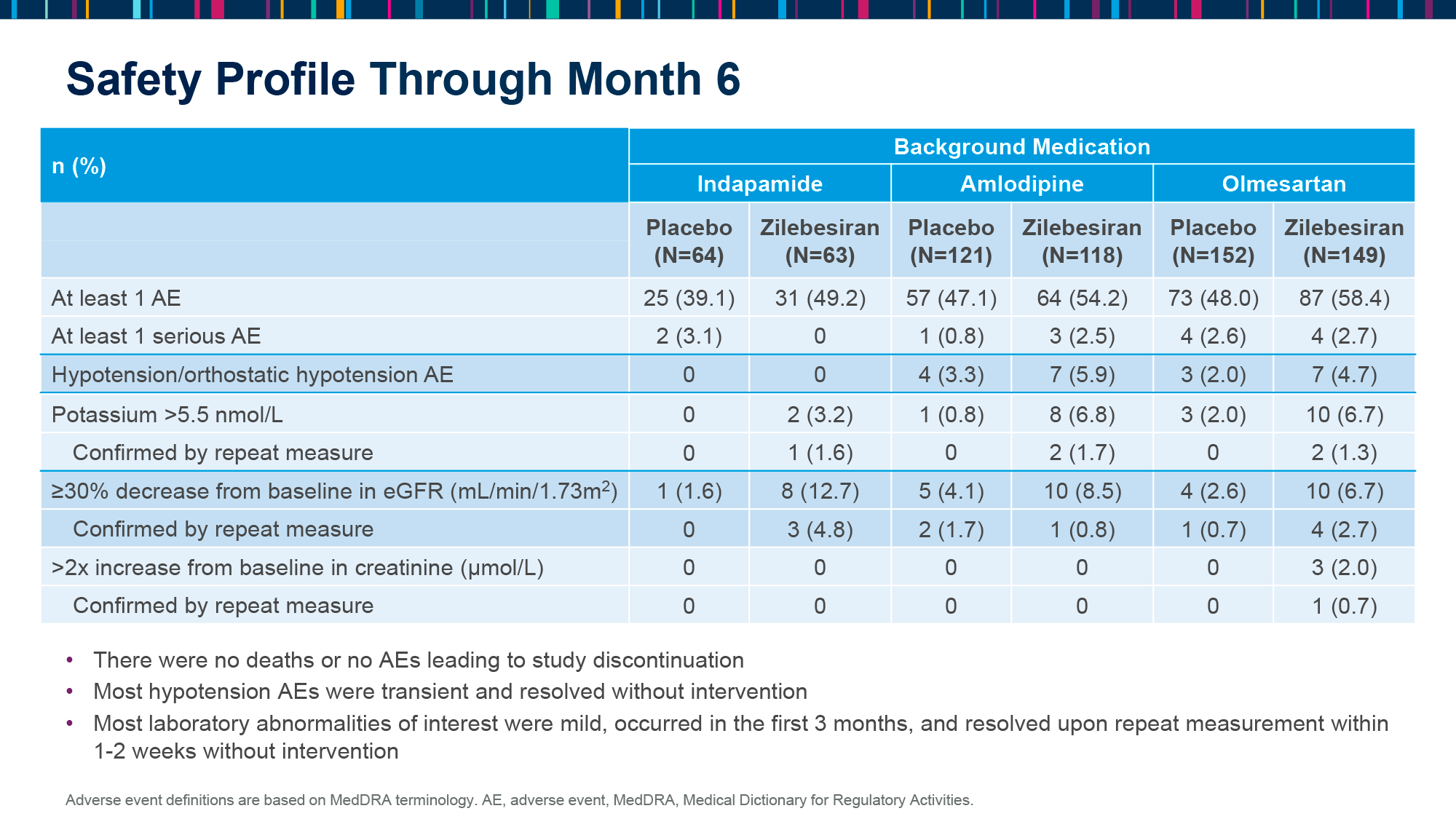
Zilebesiran was well tolerated. Adverse events (AEs), including laboratory abnormalities, were mild, transient, and resolved without intervention. Hypotension or orthostatic hypotension occurred in 0%, 6%, and 5% of patients who received zilebesiran and were subsequently treated with indapamide, amlodipine, or olmesartan, respectively, — versus 0%, 3%, and 3% in the placebo subgroups.
KARDIA-3
The KARDIA-3 (NCT06272487) phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial evaluating the feasibility of zilebesiran as add-on therapy in patients (n=390) with high cardiovascular risk and resistant hypertension (systolic blood pressure between 130 and 170 mmHg) inadequately controlled on 2–4 classes of antihypertensive drugs with different mechanisms of action is ongoing.
Key inclusion criteria include (by choice) a history of cardiovascular disease, high cardiovascular risk, or chronic kidney disease (estimated glomerular filtration rate [eGFR] between 30 and 60 mL/min/1.73 m2).
The study is expected to be completed in spring 2025.
ZILEBESIRAN: OPTIMISTIC PERSPECTIVES
The prevailing view is that a reduction in blood pressure of more than 5 mmHg is clinically significant, and thus the therapeutic benefits provided by zilebesiran appear to be highly compelling. The projected unambiguous commercial success of the drug is primarily due to its very infrequent dosing regimen (once every quarter or six months), as patient adherence to pharmacotherapy for hypertension is notably low.
Zilebesiran is selectively targeted against hepatic angiotensinogen production, which results in minimal alterations of renal angiotensin II. This means that renal compensatory mechanisms are not affected. This improves the therapeutic index, allowing zilebesiran to be administered at higher doses without fear of developing adverse events such as hypotension, hyperkalemia, or acute renal failure, which are often experienced by patients taking standard antihypertensive drugs that block the renin–angiotensin–aldosterone system (RAAS). This is because such drugs target downstream relative to angiotensinogen components of the RAAS pathway.
Once again, zilebesiran will eliminate the redundancy in the number of antihypertensives of different classes used by patients.
It is of paramount importance to consider a number of crucial factors, including the potential loss of efficacy due to the emergence of antibodies to zilebesiran, the long-term safety of the drug, and its broader benefits in the context of comorbidities such as type 2 diabetes mellitus and chronic kidney disease.
Of particular concern is the potential for rapid discontinuation of the therapeutic effect of zilebesiran if required, for example, by an unexpectedly strong and sustained drop in blood pressure. However, the generation of small interfering RNA (miRNA) complementary to the miRNA of zilebesiran does not pose significant challenges.
In addition to an upcoming pivotal phase 3 clinical program that will definitively establish the safety and efficacy of zilebesiran in a broad patient population, Alnylam Pharmaceuticals has envisioned testing its ability to reduce the risk of major cardiovascular events (MACE).
It is presumed that Alnylam will initially focus zilebesiran on the treatment of uncontrolled hypertension, a condition characterized by variability in blood pressure, lack of nighttime dipping, and poor medication adherence. This form of hypertension is typically resistant to the administration of three to four antihypertensives of different classes. It is possible that patients with heart failure or diabetic nephropathy will be added to zilebesiran in the future. Zilebesiran may potentially become a new standard of care for the treatment of primary (essential) hypertension.
The anticipated commercial launch of zilebesiran in the key pharmaceutical markets of the planet (including USA, Europe, Japan) is projected to occur around 2030. This launch will be accompanied by an expanded spectrum of therapeutic indications, including the reduction of cardiovascular morbidity and mortality.
ZILEBESIRAN: ONE MORE THING
At one point, Alnylam Pharmaceuticals had planned to develop an RNA interference drug that would combine two small interfering RNAs (siRNAs) into a single molecule, with the aim of simultaneously silencing two genes: angiotensinogen (ANG) and angiopoietin-like protein 3 (ANGPTL3). The latter is a validated target in the task of reducing atherogenic lipids.
A potential pharmaceutical agent indicated to reduce the risk of major cardiovascular events (MACE) in high-risk patients was required to reduce systolic blood pressure by at least 10 mmHg and low-density lipoprotein (LDL) cholesterol and triglyceride levels by at least 40%.
The silencing of two genes was achieved through the use of the GEMINI technology platform, and extremely infrequent subcutaneous administration was conducted on an annual basis due to the IKARIA technology platform.
The original plan, as outlined in 2021, was to select a candidate drug in 2023. However, the priorities have shifted, with Alnylam now focusing on obesity drugs due to the high demand for such treatments.
IONIS PHARMACEUTICALS AND ADVANCED HYPERTENSION TREATMENT
Ionis Pharmaceuticals first tried to deal with the experimental drug evazarsen, which, similar to zilebesiran by Alnylam Pharmaceuticals, is targeted against angiotensinogen (AGT) in the liver and is indicated for the treatment of resistant hypertension not adequately controlled by standard antihypertensive drugs.
Once sufficient evidence of evazarsen’s therapeutic efficacy had been gathered, Ionis proceeded to develop its improved version, tonlamarsen.
EVAZARSEN: MECHANISM OF ACTION
Subcutaneously administered evazarsen (IONIS-AGT-LRx) is an antisense oligonucleotide (ASO) that inhibits the synthesis of angiotensinogen (AGT) in the liver.
Evazarsen, which is complementary to the messenger RNA (mRNA) encoding AGT, binds to its non-translated region, leading to its own degradation by ribonuclease. As a result, translation is prevented and angiotensinogen synthesis is stopped.
To facilitate targeted delivery of evazarsen to the liver, its ASO sequence is covalently linked to N-acetylgalactosamine (GalNAc) ligand binding asialoglycoprotein receptor 1 (ASGR1) on hepatocytes.
In preclinical studies of evazarsen in rodent models of hypertension or acute renal failure, a 90% drop in circulating AGT levels with sustained reduction in blood pressure was demonstrated [1].
The commercial version of evazarsen was designed for subcutaneous injection once or twice a month.
TONLAMARSEN: MECHANISM OF ACTION
Ionis Pharmaceuticals, aware of the success of competitors, recognized the necessity to optimize the dosing regimen of evazarsen. This was due to the emergence of a direct competitor, zilebesiran, developed by Alnylam Pharmaceuticals, which demonstrated the efficacy of reducing blood pressure through a very rare subcutaneous injection once every six months.
An improved version of evazarsen, tonlamarsen (ION904, AGT-2.5-LRx), was prepared for this purpose.
The antisense oligonucleotide (ASO) tonlamarsen, in contrast to evazarsen, exhibits a greater than 10-fold inhibitory effect on the synthesis of angiotensinogen (AGT) in the liver. Additionally, tonlamarsen can be administered at a much lower frequency, for instance, once every two or three months.
It is conceivable that an oral formulation of tonlamarsen may be developed.
EVAZARSEN: CLINICAL RESULTS
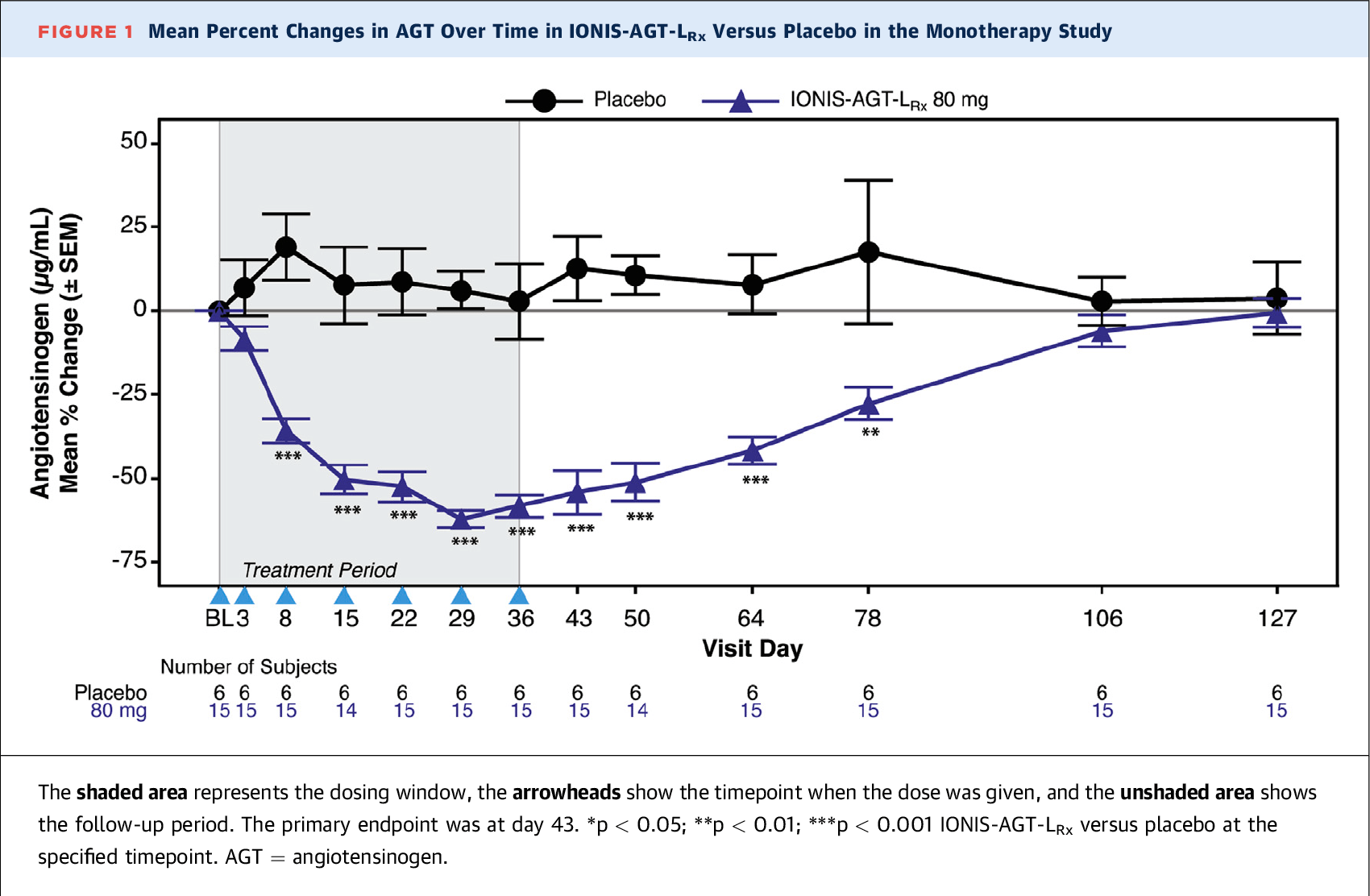
Ionis Pharmaceuticals has completed two phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trials that evaluated the efficacy and safety of evazarsen in the treatment of essential (primary) hypertension. The first trial (NCT03714776) evaluated evazarsen as a monotherapy, while the second (NCT04083222) evaluated it as an add-on to existing antihypertensive medications.
The first study included adult patients (n=25) with hypertension (systolic blood pressure [SBP] 140–165 mmHg) who were adhering to stable therapy with two antihypertensive medications. One of these was an angiotensin-converting enzyme inhibitor (ACEi) or angiotensin II receptor blocker (ARB), while the other was a beta-blocker, calcium channel blocker, or diuretic. It was required that all antihypertensive medications be discontinued by the participants.
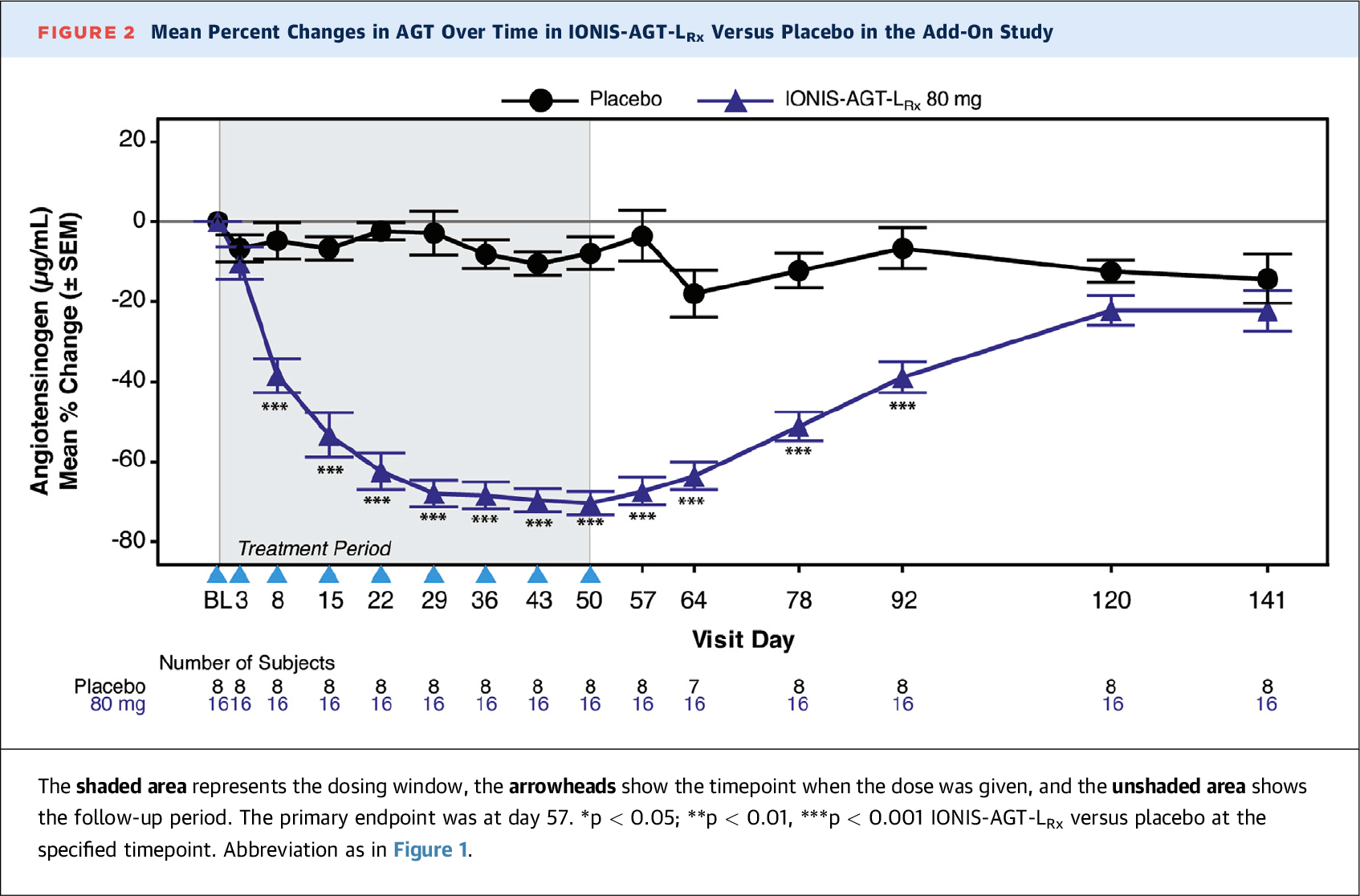
The second study invited adult patients (n=26) with uncontrolled hypertension (SBP 140–170 mmHg) following a stable course of antihypertensive therapy of two to three drugs of different classes. The obligatory ACEi or ARB was to be taken in addition to one or two additional drugs, such as a beta-blocker, calcium channel blocker, or diuretic (non-potassium-sparing). It was required that participants continue their antihypertensive medications.
For 8 weeks, patients were given an 80-mg dose of evazarsen or placebo by subcutaneous injection once a week.
The results were as follows [1].
The serum angiotensinogen (AGT) levels decreased by 54±25% and 67±14% in the evazarsen groups in the first and second studies, respectively — versus to an increase of 3±18% and 13±23% in the placebo groups (p<0.001). A statistically significant difference began to be noted on day 8, remaining so until day 92 and day 78.
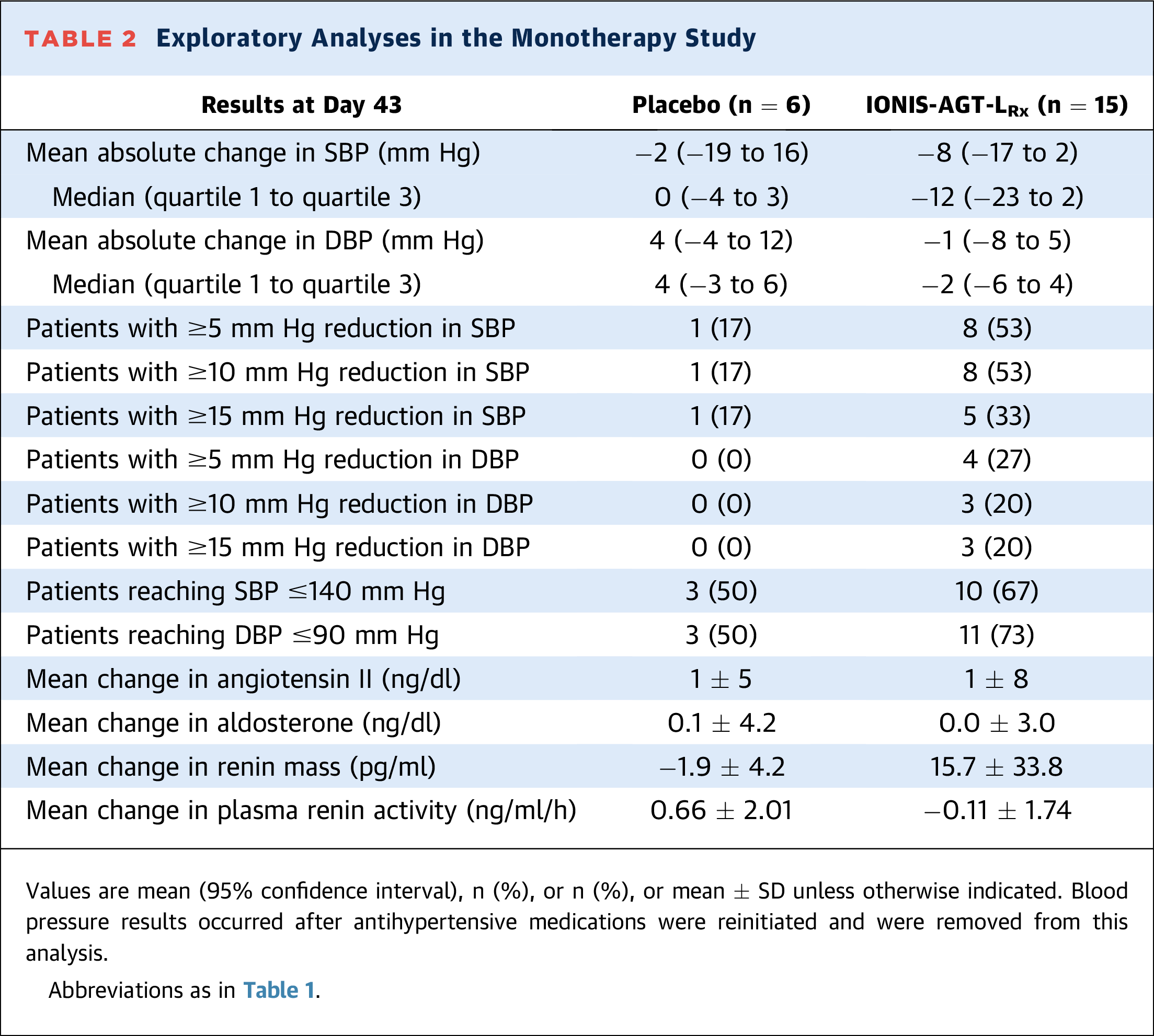
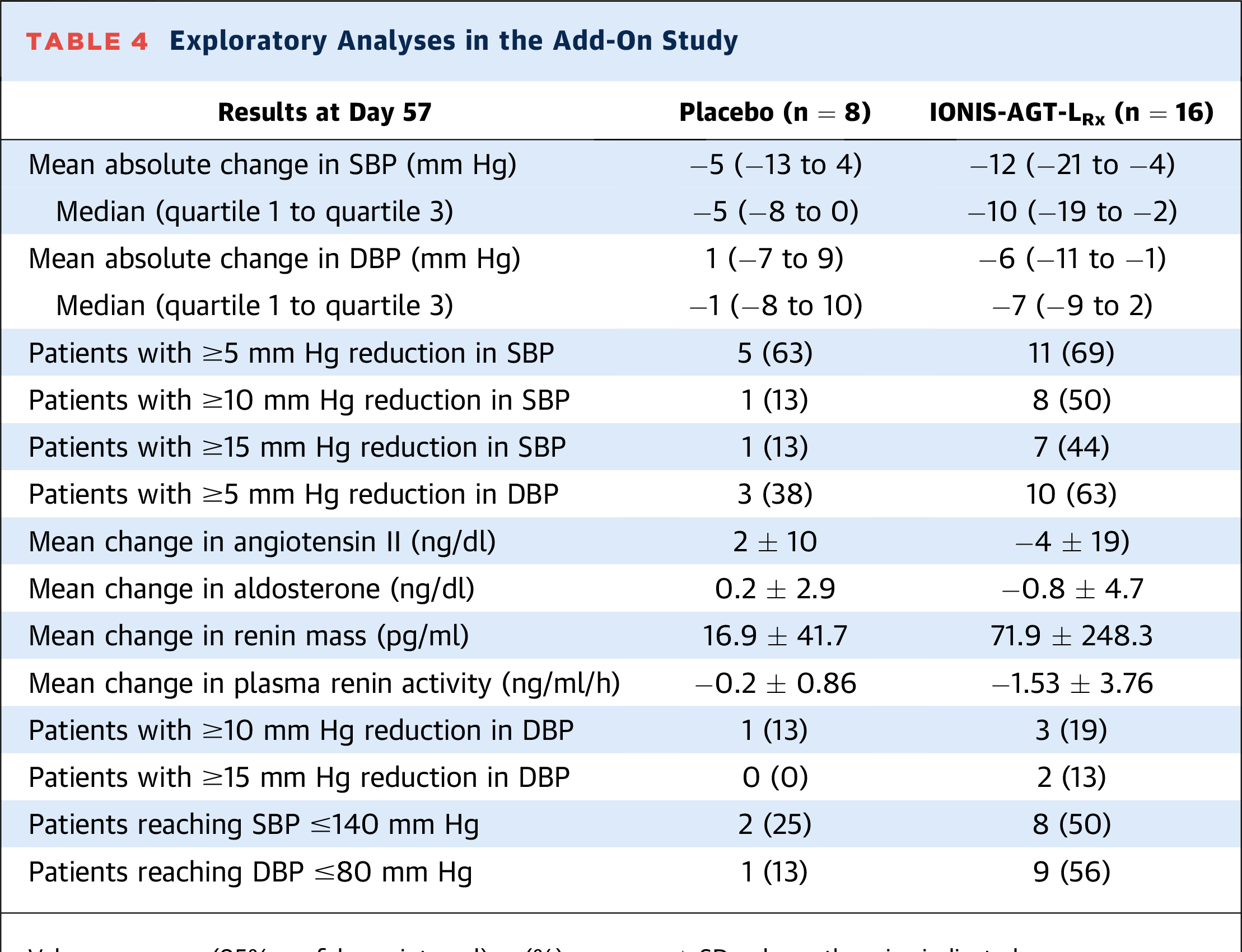
The administration of evazarsen resulted in a numerically greater (although statistically insignificant) reduction in both SBP and diastolic blood pressure (DBP) relative to the placebo. The mean change in SBP (in mmHg) was −8 (95% CI [hereafter]: −17, +2) and −12 (−21, −4), while the mean change in DBP was −1 (−8, +5) and −6 (−11, −1).
In the evazarsen groups, a larger proportion of patients demonstrated reductions in SBP and DBP of at least 5, 10, or 15 mmHg, and reached target values below 140 and 90 mmHg, respectively, than in the control groups.
The second study also showed no significant differences between outcomes depending on whether patients took two (65% of subjects) or three (35%) antihypertensive medications.
The tolerability of evazarsen was found to be acceptable. No hypotensive events, hyperkalemia, or renal impairment were reported.
Additionally, Ionis initiated a pair of phase 2b (randomized, double-blind, placebo-controlled, multicenter) clinical trials to assess the efficacy of weekly subcutaneous administration of evazarsen at different doses and among different patient populations.
In the ASTRAAS (NCT04714320) study, evazarsen was evaluated in patients (n=160) with uncontrolled resistant hypertension who were already taking three or more antihypertensive medications. In the ASTRAAS-HF (NCT04836182) study, evazarsen was tested in patients (n=72) with chronic heart failure with reduced ejection fraction (HFrEF).
The trials have been concluded, but the results have not yet been published.
TONLAMARSEN: CLINICAL RESULTS
Ionis Pharmaceuticals has conducted tonlamarsen through a phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial NCT05314439 among adult patients (n=48) with uncontrolled essential (primary) hypertension (systolic blood pressure [SBP] 130–170 mmHg), stably taking at least one antihypertensive medication.
Participants were administered tonlamarsen (30, 60, or 90 mg) or placebo by subcutaneous injection every 4 weeks for a period of 3 months.
At week 15, a reduction in angiotensinogen (AGT) serum levels of mean 79% and median 86% was observed in the tonlamarsen 90 mg subgroup — versus the reduction of 6% and 5% observed in the placebo group (p=0.001). This finding supports the mechanistic validity of the once-monthly dosing of tonlamarsen [1].
A reduction in SBP of at least 10 mmHg was observed in 42% of patients receiving tonlamarsen — vs. 30% in the control group.
The tolerability of tonlamarsen was acceptable, with no on-target adverse events (AEs) such as hyperkalemia, renal dysfunction, hypotension, or off-target AEs such as hepatic dysfunction, thrombocytopenia, being recorded.
PIPELINE
Currently, Alnylam Pharmaceuticals and its zilebesiran have no competitors.
Given how modest Ionis Pharmaceuticals has been in announcing clinical successes, it seems likely that the evazarsen and tonlamarsen programs will be discontinued. These candidate drugs, while properly blocking angiotensinogen (AGT) in the liver, require substantially more frequent dosing than zilebesiran, i.e., they have no competitive advantage.
The experimental pipeline is represented by countable AGT-targeting molecules being studied in the treatment of hypertension.
Thus, the RNA interference (RNAi) drug candidate BW-00163 by China’s Argo Biopharma is undergoing early-stage clinical testing. In early 2024, Novartis entered into a multi-billion dollar agreement with Argo. It is possible that the arrangements include BW-00163 [1] [2].
China’s Suzhou Ribo Life Science is pursuing the preclinical RNAi drug RBD9079 [3].
China’s Suzhou Senegene Bio and Innovent Biologics are also attempting to develop the preclinical RNAi drug SGB-3908 (IBI-3016) [4] [5].
STP136G and STP237G, RNAi molecules authored by Sirnaomics with offices in the U.S. and China, are in the preclinical stage. The first drug compound targets AGT, while the second targets AGT and apolipoprotein C3 (APOC3) simultaneously [6].
EXTRAS
Corporate
Zilebesiran. KARDIA-2 Phase 2 Results: Investor Event. Alnylam Pharmaceuticals. April 7, 2024. [PDF]
Alnylam R&D Day 2023. December 13, 2023. [PDF]
Alnylam Pharmaceuticals Conference Call to Discuss Zilebesiran Collaboration Agreement with Roche. July 24, 2023. [PDF]
Alnylam R&D Day 2022. December 15, 2022. [PDF]
Alnylam R&D Day 2021. November 19, 2021. [PDF]
KARDIA: Zilebesiran Phase 2 Clinical Development Overview. Alnylam Pharmaceuticals. 2021. [PDF]
RNAi Roundtable: Zilebesiran (ALN-AGT), in Development for the Treatment of Hypertension. Alnylam Pharmaceuticals. June 30, 2021. [PDF]
Alnylam R&D Day 2020. December 15, 2020. [PDF]
RNAi Roundtable: ALN-AGT, in Development for the Treatment of Hypertension. Alnylam Pharmaceuticals. June 23, 2020. [PDF]
Alnylam R&D Day 2019. November 22, 2019. [PDF]
Medical Conferences
Zilebesiran in Combination with a Standard-of-care Antihypertensive in Patients with Inadequately Controlled Hypertension: Primary Results from the Phase 2 KARDIA-2 Study. ACC 2024. [PDF]
Consistent Antihypertensive Efficacy of the RNA Interference Therapeutic Zilebesiran: Subgroup Results from the KARDIA-1 Phase 2 Study in Patients with Hypertension. ACC 2024. [PDF]
Sustained Blood Pressure Reduction with the RNA Interference Therapeutic, Zilebesiran: Primary Results from KARDIA-1, a Phase 2 Study in Patients with Hypertension. AHA 2023. [PDF]
Safety and Tolerability of Zilebesiran, an RNA Interference Therapeutic Targeting Hepatic Angiotensinogen Synthesis, in Obese Patients with Hypertension. AHA 2023. [PDF]
Durable Reductions in Circulating Angiotensinogen and Blood Pressure 6 Months after Single Doses of ALN-AGT, an RNA Interference Therapeutic Targeting Hepatic Angiotensinogen Synthesis, in Hypertensive Patients. AHA 2021. [PDF]
Safety and Tolerability of ALN-AGT, an RNA Interference Therapeutic Targeting Hepatic Angiotensinogen Synthesis, in Hypertensive Patients during Sodium Depletion or Irbesartan Coadministration. AHA 2021. [PDF]
Dose-Related and Prolonged Reductions in Blood Pressure with a RNAi Therapeutic Targeting Angiotensinogen in Hypertensive Patients: Interim Results from a Phase 1 Study with Zilebesiran (ALN-AGT01). OTS 2021. [PDF]
Safety, Pharmacodynamics, and Blood Pressure Effects of ALN-AGT, an RNA Interference Therapeutic Targeting Angiotensinogen, in a Randomized Single Ascending Dose Study of Hypertensive Adults. ESH-ISH 2021. [PDF]
Dose-Related Reductions in Blood Pressure with a RNA Interference (RNAi) Therapeutic Targeting Angiotensinogen in Hypertensive Patients: Interim Results from a First-In-Human Phase 1 Study of ALN-AGT01. AHA 2020. [PDF]
Scientific Publications
Angiotensinogen as a Therapeutic Target for Cardiovascular and Metabolic Diseases. Arterioscler Thromb Vasc Biol. 2024 May;44(5):1021-1030. [Source]
Zilebesiran: A Promising Antihypertensive Therapy Inhibiting Angiotensinogen Synthesis. Cardiol Rev. 2024 Feb 22. [Source]
RNA Interference With Zilebesiran for Mild to Moderate Hypertension: The KARDIA-1 Randomized Clinical Trial. JAMA. 2024 Mar 5;331(9):740-749. [Source]
Molecular Therapies in Cardiovascular Diseases: Small Interfering RNA in Atherosclerosis, Heart Failure, and Hypertension. Int J Mol Sci. 2023 Dec 26;25(1):328. [Source]
Emerging insights and future prospects for therapeutic application of siRNA targeting angiotensinogen in hypertension. Expert Rev Clin Pharmacol. 2023 Jul-Dec;16(11):1025-1033. [Source]
Novel Pharmacological Approaches in the Treatment of Hypertension: A Focus on RNA-Based Therapeutics. Hypertension. 2023 Nov;80(11):2243-2254. [Source]
Zilebesiran, an RNA Interference Therapeutic Agent for Hypertension. N Engl J Med. 2023 Jul 20;389(3):228-238. [Source]
Small Interfering RNA Therapeutics in Hypertension: A Viewpoint on Vasopressor and Vasopressor-Sparing Strategies for Counteracting Blood Pressure Lowering by Angiotensinogen-Targeting Small Interfering RNA. J Am Heart Assoc. 2022 Oct 18;11(20):e027694. [Source]