Unresolved Issue of Small Cell Lung Cancer
Small cell lung cancer (SCLC), which contributes approximately 15% to the total number of lung cancers, is pathologically and clinically decisively different from non-small cell lung cancer (NSCLC). The disease is characterized by rapid growth and early development of metastases, and therefore belongs to the extremely aggressive types of oncology. Most cases diagnosed with SCLC experience distant metastasis: 70% of patients encounter small cell lung cancer in the advanced stage, traditionally referred to as extensive-stage small cell lung cancer.
For several decades, etoposide, a podophyllotoxin derivative, in combination with a platinum-containing drug, cisplatin or carboplatin, has been the standard of care for first-line chemotherapy. Despite a high response rate to treatment, there was almost always a recurrence of the disease, with a median progression-free survival of less than 3 months and a median overall survival of 10 months. The two-year survival rate for chemotherapy treatment of extensive-stage SCLC rarely exceeds 5%.
The rapid ascent of immune checkpoint inhibitors (ICIs) represented by PD-(L)1 blockers, which showed decent therapeutic efficacy against a wide variety of oncology diseases, forced the pharmaceutical industry to implement their large-scale testing in the fight against SCLC. The high mutational nature of small cell lung cancer suggested that its tumors, being immunogenic, would respond to ICIs. Collected clinical data confirmed the validity of prescribing immunotherapy in combination with standard chemotherapy — however, no serious extension of life has yet been achieved.
At the current state of medical science, the following picture is emerging. First-line treatment of small cell lung cancer at the advanced stage is reasonable by adding ICI to standard chemotherapy — not after it has taken place. In addition, it is PD-L1 blockers, not PD-1, that are effective. The latter thing is most likely because tumors characterized by insufficient PD-L1 expression respond better to PD-L1 blockers.
For reference, the tumor PD-L1 expression at least at a minimal level of 1% is found in approximately two-thirds of patients with NSCLC, whereas in SCLC it is found in no more than 20% of cases.
Second-line therapy is still at the mercy of chemotherapy, although there are indications that PD-(L)1 blockers will benefit here in platinum-resistant patients who did not receive them during the first-line treatment. Until recently, third-line treatments for small cell lung cancer were given with PD-1 blockers — a subsequent validation of their therapeutic efficacy failed.
Be that as it may, there is still the highest unmet medical need for new pharmacological options for the first-line treatment of extensive-stage small cell lung cancer.
Tecentriq for Treatment of Small Cell Lung Cancer: First New Drug in 20 Years
In March 2019, Tecentriq (atezolizumab), a PD-L1 blocker developed by Roche (Roche), secured approval from the U.S. Food and Drug Administration (FDA) for use in combination with etoposide and carboplatin in the first-line treatment of extensive-stage small cell lung cancer.

Atezolizumab has become the first immuno-oncology drug approved for first-line treatment of SCLC in the past two decades.
It should be understood, however, that the therapeutic benefit of Tecentriq is extremely mediocre: the IMpower133 (NCT02763579) phase 3 clinical trial showed that adding atezolizumab to standard chemotherapy could prolong overall survival (OS) by a very modest 2 months. The median OS was 12.3 months (95% CI: 10.8–15.9) — versus 10.3 months (95% CI: 9.3–11.3) with standard treatment: hazard ratio (HR) 0.70 (95% CI: 0.54–0.91); p=0.007.
Exploratory analysis found that clinical outcomes were generally independent of PD-L1 tumor expression status or tumor mutational burden (TMB) level.
Extras
First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018 Dec 6;379(23):2220-2229. [source]
Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with atezolizumab, carboplatin, and etoposide (IMpower133). J Clin Oncol. 2021 Feb 20;39(6):619-630. [source]
Imfinzi for Treatment of Small Cell Lung Cancer: Strong Alternative to Tecentriq
In March 2020, exactly one year after the debut of Tecentriq in the first-line treatment of advanced small cell lung cancer, Imfinzi (durvalumab), a PD-L1 blocker from AstraZeneca, got a similar indication.

Durvalumab is prescribed together with standard chemotherapy: etoposide and a platinum-containing agent of choice (carboplatin or cisplatin).
The clinical performance of Imfinzi in the CASPIAN (NCT03043872) phase 3 clinical trial is generally not different from that of Tecentriq. After a median of 14.2 months of follow-up, median OS came out to 13.0 months (95% CI: 11.5–14.8) — versus 10.3 months (95% CI: 9.3–11.2) with standard treatment: HR 0.73 (95% CI: 0.59–0.91); p=0.005.
After a median of 25.1 months of follow-up, the median OS stopped at 12.9 months (95% CI: 11.3–14.7) — versus 10.5 months (95% CI: 9.3–11.2): HR 0.75 (95% CI: 0.62–0.91); p=0.003.
Imfinzi outperforms Tecentriq except in a set of relatively non-critical criteria. First, durvalumab can be used in combination with either carboplatin or cisplatin (no particular difference between the two has been identified): the former is the standard platinum-containing chemotherapy in the US, the latter in Europe. Second, Imfinzi was more effective than Tecentriq in controlling metastasis to the brain. Third, durvalumab has a slightly more acceptable safety profile.
Extras
Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019 Nov 23;394(10212):1929-1939. [source]
Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2021 Jan;22(1):51-65. [source]
Opdivo for Treatment of Small Cell Lung Cancer: It Didn’t Work Out
In August 2018, Opdivo (nivolumab), a PD-1 blocker marketed by Bristol-Myers Squibb, received conditional FDA approval for use in the treatment of metastatic small cell lung cancer that had progressed after platinum-containing chemotherapy and at least one prior line of therapy.

Nivolumab was actually the first new drug against SCLC in the past twenty years.
The regulatory decision was guided by the results of the CheckMate-032 (NCT01928394) phase 1/2 clinical trial: the overall response rate (ORR) was 11.9%, including 0.9% complete response (CR) and 11.0% partial response (PR). Among respondents, the median duration of response (DoR) was 17.9 months. OS frequencies at 12 and 18 months were recorded at 28.3% and 20.0%.
Meanwhile, in December 2020, Bristol-Myers Squibb removed third-line therapy for small cell lung cancer from its list of indications for Opdivo. The decision, made voluntarily, was due to the failures of two confirmatory clinical trials.
Thus, in October 2018, Opdivo failed to stake a claim in second-line therapy for SCLC, which relapsed after platinum-containing chemotherapy. The CheckMate-331 (NCT02481830) phase 3 clinical trial failed to uncover the advantages of nivolumab monotherapy over standard topotecan or amrubicin, as far as prolonging overall survival.
Median OS reached 7.5 months (95% CI: 5.6–9.2) — versus 8.4 months (95% CI: 7.0-10.0): HR 0.86 (95% CI: 0.72–1.04; p=0.11).
Slightly greater OS prolongation was seen in patients either with lactate dehydrogenase levels no higher than the upper limit of normal, or resistant to prioritized platinum-containing chemotherapy, or without liver metastasis.
In November 2018, Opdivo failed to meet the interesting challenge of supporting therapy for advanced small cell lung cancer that had stabilized (not progressed) after first-line platinum-containing chemotherapy. The CheckMate-451 (NCT02538666) phase 3 clinical trial, which checked the consolidating monotherapy of nivolumab or its combination with Yervoy (ipilimumab), a CTLA-4 blocker, found no advantage over placebo.
Median OS was determined at 10.4 months (95% CI: 9.5–12.1) and 9.2 months (95% CI: 8.2–10.2), respectively — versus 9.6 months (95% CI: 8.2–11.0) in the control group: HR 0.84 (95% CI: 0.69–1.02) and HR 0.92 (95% CI: 0.75–1.12; p=0.37).
There was a positive dynamics of OS among those patients who started nivolumab therapy within 5 months after completion of chemotherapy or whose tumors had a relatively high mutational burden.
Extras
Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): a multicentre, open-label, phase 1/2 trial. Lancet Oncol. 2016 Jul;17(7):883-895. [source]
Tumor mutational burden and efficacy of nivolumab monotherapy and in combination with ipilimumab in small-cell lung cancer. Cancer Cell. 2018 May 14;33(5):853-861.e4. [source]
Third-line nivolumab monotherapy in recurrent SCLC: CheckMate 032. J Thorac Oncol. 2019 Feb;14(2):237-244. [source]
Second-line nivolumab in relapsed small-cell lung cancer: CheckMate 331. Ann Oncol. 2021 Feb 1;S0923-7534(21)00099-5. [source]
Nivolumab and ipilimumab as maintenance therapy in extensive-disease small-cell lung cancer: CheckMate 451. J Clin Oncol. 2021 Mar 8;JCO2002212. [source]
Keytruda for Treatment of Small Cell Lung Cancer: Justified Rejection
In June 2019, Keytruda (pembrolizumab), Merck & Co.’s best-selling PD-1 blocker, achieved conditional FDA approval for the same as Opdivo monotherapy in the treatment of metastatic small cell lung cancer that has progressed during or after platinum-containing chemotherapy and at least one prior therapy line.

Regulatory approval came from the KEYNOTE-028 (NCT02054806) phase 1b (cohort C1) and KEYNOTE-158 (NCT02628067) phase 2 (cohort G) clinical trials. Administration of pembrolizumab resulted in an ORR of 19.3%, including a CR of 2.4% and a PR of 16.9%. The median DoR at that time had not yet been established (4.1–35.8+ months).
In March 2021, Merck & Co. notified that it had excluded small cell lung cancer from the wide-ranging list of indications for Keytruda.
The reason was the crash of the KEYNOTE-604 (NCT03066778) phase 3 clinical trial, which tested the addition of pembrolizumab to etoposide with carboplatin or cisplatin in previously untreated extensive-stage SCLC.
Yes, the Keytruda group showed a statistically significant improvement in progression-free survival (PFS) relative to the use of chemotherapy alone (HR 0.75 [95% CI: 0.61–0.91]; p=0.0023). However, pembrolizumab failed to statistically significantly prolong OS: median 10.8 months (95% CI: 9.2–12.9) — versus 9.7 months (95% CI: 8.6–10.7); HR 0.80 (95% CI: 0.64–0.98), p=0.0164 (threshold p=0.0128).
Anyway, Keytruda is a sin to complain about: the immunotherapy drug is firmly established in the first-line treatment of non-small cell lung cancer, demonstrating its own suitability for a wide patient population. And with NSCLC occurring in three-quarters of all lung cancer diagnoses, pembrolizumab raises billions of dollars in revenue for Merck & Co. each year. In 2019 and 2020, for example, Keytruda added $11.1 billion and $14.4 billion to the U.S. drugmaker’s bank account.
Extras
Pembrolizumab in patients with extensive-stage small-cell lung cancer: results from the phase Ib KEYNOTE-028 study. J Clin Oncol. 2017 Dec 1;35(34):3823-3829. [source]
Pembrolizumab after two or more lines of previous therapy in patients with recurrent or metastatic SCLC: results from the KEYNOTE-028 and KEYNOTE-158 studies. J Thorac Oncol. 2020 Apr;15(4):618-627. [source]
Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung cancer: randomized, double-blind, phase III KEYNOTE-604 study. J Clin Oncol. 2020 Jul 20;38(21):2369-2379. [source]
Zepzelca for Treatment of Small Cell Lung Cancer: New Chemotherapy Drug
In June 2020, Zepzelca (lurbinectedin), a new drug designed to treat metastatic small cell lung cancer that has progressed during or after platinum-containing chemotherapy, was released.

Lurbinectedin, formerly known as Zepsyre, is a selective inhibitor of oncogenic transcriptional programs that many solid tumors depend on for survival. Lurbinectedin belongs to the class of alkylating antineoplastic drugs.
Lurbinectedin suppresses active transcription in tumor cells through selective covalent binding to CG-saturated DNA-sequences, irreversible inhibition and degradation of elongating RNA-polymerase II on DNA template, generation of XPF-dependent single- and double-stranded DNA breaks. The result is apoptosis of cancer cells. The molecule does not affect RNA polymerase I or mitochondrial RNA polymerase and has no effect on basal transcription. Lurbinectedin has a selective apoptosis-inducing effect on mononuclear phagocytes and inhibits the production of inflammatory cytokines.

Lurbinectedin, developed by Spain’s PharmaMar and commercialized by Jazz Pharmaceuticals, is conditionally approved by FDA.
Zepzelca has become an alternative second-line therapy for SCLC. Prior to its introduction, the second-line management of this cancer, which is sensitive to chemotherapy with platinum-containing drugs, was with topotecan. There were no treatment options for platinum-resistant small cell lung cancer.
In the NCT02454972 phase 2 clinical trial, monotherapy with lurbinectedin provided median OS of 9.3; 11.9 and 5.0 months, according to interim results, among the entire participant population, patients with platinum-sensitive SCLC and subjects with platinum-resistant SCLC, respectively.
For the sake of clarity, lurbinectedin outperforms topotecan on all key clinical outcomes, including OS, PFS, ORR, and DoR. So, for example, the second-line use of topotecan yields OS within a median of 5.8 months.
A confirmatory phase 3 clinical trial ATLANTIS (NCT02566993) examining the combination of lurbinectedin and doxorubicin in second-line therapy of recurrent small cell lung cancer unresponsive to platinum-containing chemotherapy ended unsuccessfully in December 2020. The comparison was made with topotecan or cyclophosphamide/doxorubicin/vincristine (CAV regimen). As a result, the experimental treatment did not improve OS.
In January 2021, there were encouraging results of the phase 1b/2 clinical trial NCT02611024, which tested the hypothesis of the appropriateness of a synergistic combination of lurbinectedin and irinotecan in extensive-stage SCLC, which have undergone no more than two lines of therapy.
In parallel, the phase 1/2 clinical trial LUPER (NCT04358237) is trying to establish the efficacy of a cocktail of lurbinectedin and pembrolizumab in SCLC relapsed after first-line chemotherapy.
Extras
Lurbinectedin as second-line treatment for patients with small-cell lung cancer: a single-arm, open-label, phase 2 basket trial. Lancet Oncol. 2020 May;21(5):645-654. [source]
Antitumor activity of lurbinectedin in second-line small cell lung cancer patients who are candidates for re-challenge with the first-line treatment. Lung Cancer. 2020 Dec;150:90-96. [source]
Small Cell Lung Cancer: Promising Immuno-Oncologic and Beyond Treatment Attempts
The pharmaceutical industry, unstoppable in developing new modalities for treating small cell lung cancer, has been targeting a variety of immune checkpoints, selecting alternative targets, and testing combination approaches.

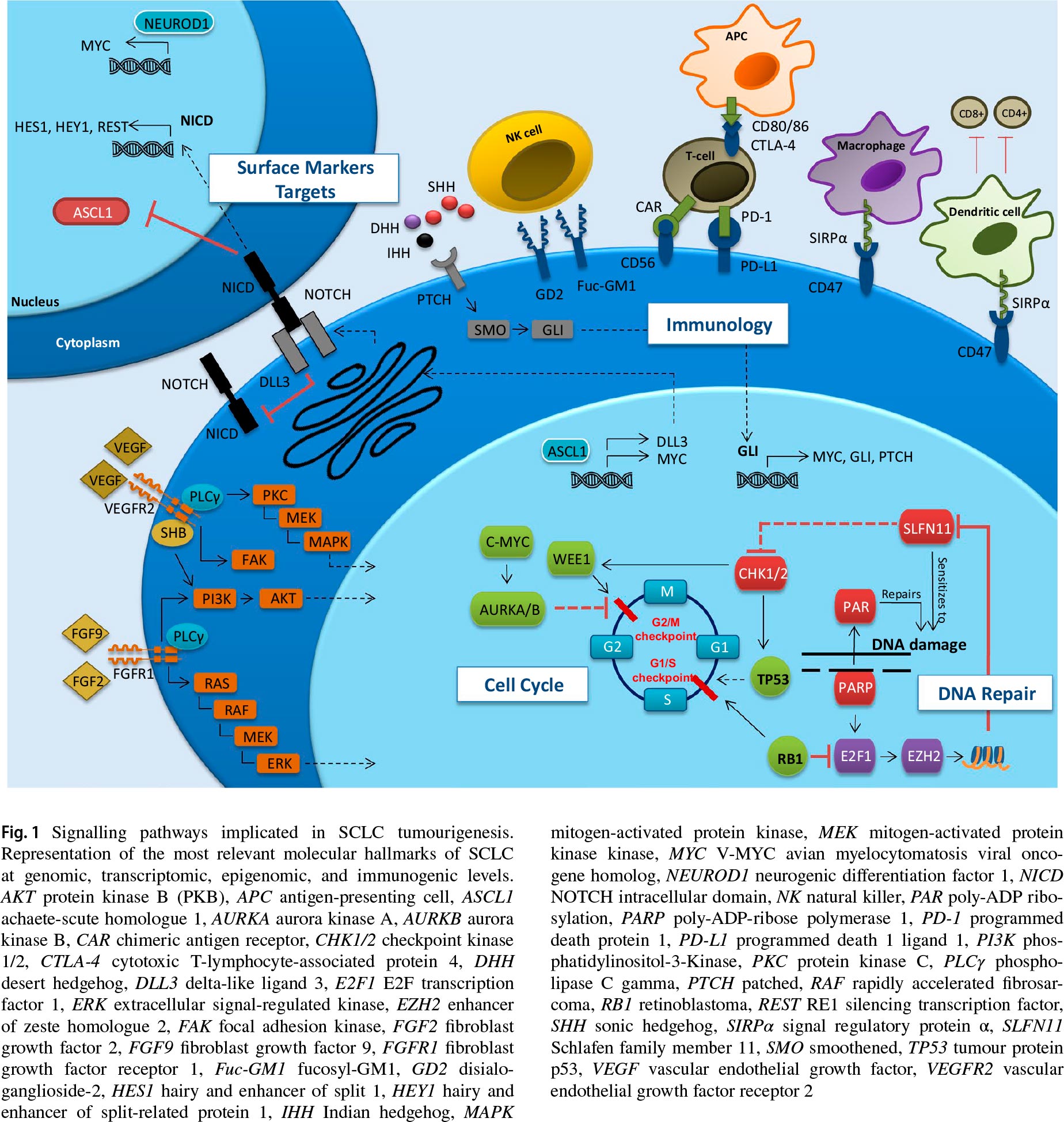
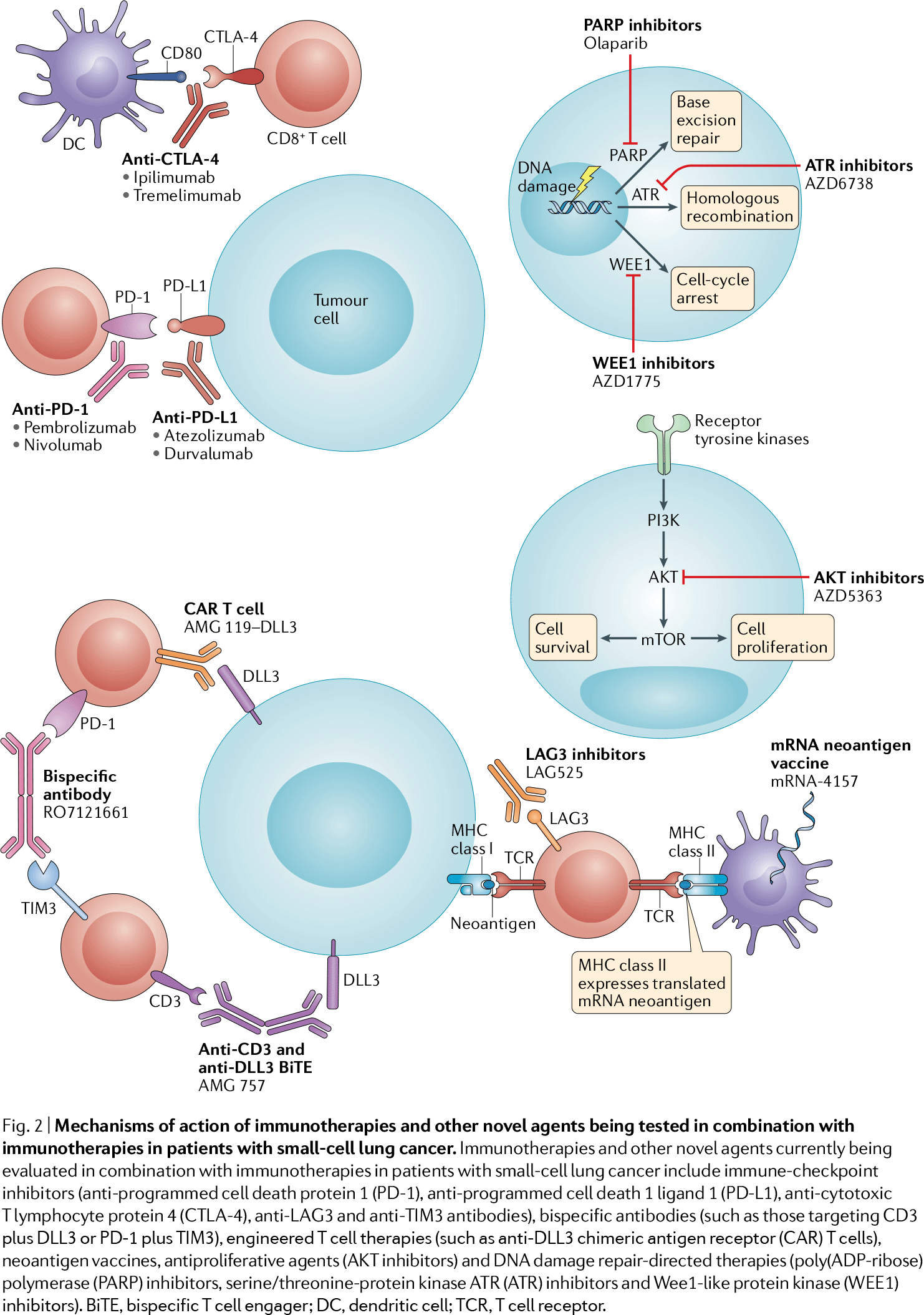
Signaling pathways involved in the oncogenesis of small cell lung cancer. Drugs. 2020 Jan 8. Mechanism of action of immunotherapeutic and other drugs being developed in the treatment of small cell lung cancer. Nat Rev Clin Oncol. 2020 Feb 13.
A key issue for successful SCLC therapy lies in the lack of reliable tumor biomarkers that can be targeted and that can confidently predict clinical outcomes.
For example, when it comes to tumor PD-L1 expression, small cell lung cancer is immunohistochemically closer to triple-negative breast cancer and urothelial carcinoma, in which PD-L1 expression is noted mainly on tumor-infiltrating immune cells (IC) rather than directly on tumor cells (TC). To be clear, in NSCLC, which is significantly better treated with PD-(L)1 blockers than SCLC, PD-L1 expression is observed on both ICs and TCs.
Again, there is a curious paradox associated with the relatively high tumor mutational burden (TMB) in small cell lung cancer: it is probably a reflection of the endless damage caused by carcinogens in tobacco smoking. High TMB, however, is accompanied, first, by low or absent tumor PD-L1 expression and, second, by a very poor response rate (compared with other solid tumors with similar median TMB levels) to the administration of immune checkpoint inhibitors.
Let’s consider the most interesting and significant clinical trials of experimental treatment of small cell lung cancer. Information about them is periodically updated as new data become available.
Targets: 4-1BB, OX40, GITR
Clinical trial JAVELIN Medley (NCT02554812) phase 2
Indication: small cell lung cancer that has progressed after at least one platinum-containing therapy.
Sponsor: Pfizer.
Monoclonal antibody utomilumab (PF-05082566), a costimulatory immune checkpoint 4-1BB agonist, in combination with Bavencio (avelumab), a PD-L1 blocker.
4-1BB (CD137, TNFRSF9) is a surface glycoprotein belonging to the tumor necrosis factor (TNF) receptor superfamily that is expressed on activated CD8+ and CD4+ T lymphocytes and natural killer (NK) cells, acting as an inducible costimulatory receptor that is involved in T cell proliferation, survival and cytolytic activity. Agonist binding to 4-1BB enhances its mediated signaling, induces cytokine production, and promotes T cell-mediated antitumor immune responses.
Clinical trial NCT03241173 phase 1/2
Indication: advanced small cell lung cancer.
Sponsor: Incyte.
Monoclonal antibody INCAGN01949, a secondary costimulatory immune checkpoint OX40 agonist, in combination with Opdivo (nivolumab) or Yervoy (ipilimumab), PD-1 and CTLA-4 blockers, or with a combination thereof.
OX40 (CD134, TNFRSF4) is a surface glycoprotein belonging to the TNF receptor superfamily that is delayedly expressed on resting naive T cells some time after their activation, providing a costimulatory signal for proliferation and survival of activated T cells. Agonist binding to OX40 potentiates T cell receptor (TCR) signaling, inhibits regulatory T cell (Treg)-mediated suppression of effector T cells (Teff), induces proliferation of memory T cells and Teff, and modulates cytokine production.
In addition, the Fc fragment of immunoglobulin G1 (IgG1) monoclonal antibody INCAGN01949 binds and interacts with Fc gamma receptor III (FcγRIII, CD16a) on effector immune cells, which activates FcγRIII-mediated signaling and promotes selective depletion of the intratumor Treg population, thereby enhancing the cytotoxic T lymphocyte (CTL)-mediated response by tumor cells.
Clinical trial NCT03126110 phase 1/2
Indication: advanced small cell lung cancer.
Sponsor: Incyte.
Monoclonal antibody INCAGN01876, a costimulatory immune checkpoint GITR agonist, in combination with Opdivo (nivolumab) or Yervoy (ipilimumab), PD-1 and CTLA-4 blockers, or a combination thereof.
GITR (CD357, TNFRSF18) is a transmembrane receptor molecule belonging to the TNF receptor superfamily that is expressed on multiple immune cells, including Treg, Teff, B cells and NK cells, enhancing T cell survival, proliferation and cytokine production and reducing Treg activity. GITR activation stimulates the immune system, resulting in activation and proliferation of tumor-specific Teff and suppression of the function of activated Treg, which inhibits Teff and TCR signaling.
Targets: CD47/SIRPα, LAG3, TIM-3, TGF-β
Clinical trial REPLATINUM (NCT03699956) phase 3
Indication: small cell lung cancer that has undergone at least two lines of therapy, including platinum drugs and PD-(L)1 blocker.
Sponsor: EpicentRx.
RRx-001 together with etoposide and a platinum-containing chemotherapy drug (cisplatin or carboplatin).
RRx-001 is a low molecular weight pleiotropic immunotherapeutic agent that repolarizes tumor-associated macrophages (TAM) and other immunosuppressed cells into an immunostimulatory phenotype by inhibiting the CD47/SIRPα signaling pathway. In other words, it sensitizes tumor cells, making them more susceptible to chemotherapy. The cell surface molecule CD47 (IAP), which is responsible for the “don’t eat me” signaling, binds to the SIRPα receptor on phagocytic cells, thereby inhibiting phagocytic function. The selection of CD47/SIRPα as an immunotherapeutic target is promising for many cancers.
Clinical trial NCT03365791 phase 2
Indication: advanced small cell lung cancer, recurrent and/or refractory to standard therapy.
Sponsor: Novartis.
A combination of two monoclonal antibodies: leramilimab (LAG525), an activator of inhibitory immune checkpoint LAG3, and spartalizumab (PDR001), a PD-1 blocker.
LAG3 (CD223) is a signaling receptor molecule belonging to the immunoglobulin superfamily (IgSF) that is expressed on the surface of activated CTL and Treg and negatively regulates T cell proliferation and activation. Binding of LAG3 expressed on tumor-infiltrating lymphocytes (TIL) and its subsequent blocking of binding to class II molecules of the major histocompatibility complex (MHC) on the surface of tumor cells leads to activation of antigen-specific T lymphocytes and enhances CTL-mediated lysis of malignant cells.
LAG3 is likely to be a better target than PD-1 or CTLA-4 because antibodies against the latter only activate Teff but do not inhibit Treg activity, while antibodies against LAG3 equally activate Teff and inhibit induced antigen-specific suppressive Treg activity.
Clinical trial NCT03708328 phase 1
Indication: small cell lung cancer, unresponsive, progressive, or with intolerance to standard therapy.
Sponsor: Roche.
RO7121661 (RG7769) is a bispecific monoclonal antibody against PD-1 and the inhibitory immune checkpoint TIM-3.
TIM-3 (HAVCR2, CD366) is a transmembrane protein expressed on CD4+ and CD8+ T cells, Treg, and cells of the innate immune system (dendritic cells, NK, monocytes) responsible for promoting immunosuppression by mediating depletion of the CD8+ T cell pool. Co-expression of TIM-3 and PD-1, often observed on tumor-antigen-specific T cells, results in high rates of dysfunction and depletion of the pool of tumor-infiltrating Teff.
Simultaneous PD-1 and TIM-3 blockade reverses T-cell suppression, activates antigen-specific T lymphocytes, and enhances CTL-mediated lysis of malignant cells.
Clinical trial NCT03554473 phase 1/2
Indication: recurrent small cell lung cancer.
Sponsor: National Cancer Institute (NCI).
Monotherapy with bintrafusp alfa (M7824) or its combination with topotecan or temozolomide.
Bintrafusp alfa, developed by Merck KGaA and GlaxoSmithKline, is a bifunctional hybrid protein that, as a dual inhibitor of immune checkpoints, is composed of a heavy chain of a fully human monoclonal IgG1 antibody against PD-L1 attached to the extracellular domain of two transforming growth factor beta receptor II (TGFβRII) molecules.
TGFβRII, acting as a trap for all three isoforms of transforming growth factor beta (TGF-β), neutralizes the latter, thereby enhancing the penetration of T cells into the tumor microenvironment and increasing its susceptibility to anti-PD-L1 therapy. Signaling of pleiotropic cytokine TGFβRII in the tumor microenvironment promotes disease progression: by suppressing the immune response, promoting tumor angiogenesis, inducing epithelial-mesenchymal transition (leading to metastasis and resistance to treatment), and fibrosis (reflected by preventing access of drug molecules).
Targets: p53, tumor neoantigens
Clinical trial NCT03406715 phase 2
Indication: recurrent small cell lung cancer.
Sponsors: H. Lee Moffitt Cancer Center & Research Institute, MultiVir, Bristol-Myers Squibb.
A cocktail of INGN-225 and Opdivo (nivolumab) plus Yervoy (ipilimumab), PD-L1 and CTLA-4 blockers.
INGN-225 (Ad.p53-DC) is a dendritic cell vaccine against the tumor suppressor p53, whose dysfunction (due to point mutations in the TP53 gene or abnormalities in degradation of wild-type p53 protein), noted in half of all cancers and over 90% of SCLC cases, is manifested by loss of apoptosis regulation and abnormal cell proliferation. The p53 protein is considered an “ideal” tumor-associated antigen (TAA). First, it and its derived epitopes accumulate on the surface of most tumor cells. Second, the latter, even if restored to wild-type p53 status (without the loss of antigenicity variants) are unlikely to escape anti-p53 CTL attack, since mutant forms of p53 lead to oncogenic gain-of-function mutations.
Nonreplicating adenovirus particles with the wild-type TP53 gene transfect the patient’s autologous dendritic cells ex vivo. The latter (after intradermal injection) synthesize, process, and present p53 peptides (epitopes) recognized by naive T cells, which, upon activation, begin to proliferate and differentiate into Teff capable of identifying and destroying p53-overexpressing malignant cells.
Clinical trial KEYNOTE-603 (NCT03313778) phase 1
Indication: inoperable (locally advanced or metastatic) small cell lung cancer.
Sponsors: Moderna and Merck & Co.
mRNA-4157 with Keytruda (pembrolizumab), a PD-1 blocker.
mRNA-4157 is a personalized anti-cancer mRNA vaccine encoding up to three dozen tumor neoantigens, both those discovered during ex vivo experiments on patient immune cells and those predictably immunogenic according to bioinformatics algorithms, which means they can initiate beneficial immunostimulatory reactions in the body. Delivery of a variety of tumor-specific antigens (TSA) to the body at once should dramatically increase the probability of successful clinical outcomes, as the immune system begins to generate a multidirectional T-cell response (from cytotoxic CD8+ T cells and memory CD4+ T cells) to the neoantigen peptides that have been presented to it.
Targets: PARP, VEGFR
Clinical trial NCT03516084 phase 3
Indication: maintenance therapy of extensive-stage small cell lung cancer after first-line platinum-containing chemotherapy.
Sponsor: Zai Lab (China).
Zejula (niraparib), a poly (ADP-ribose) polymerase (PARP) inhibitor.
The clinical trial was interrupted before its completion: due to the changed paradigm of treatment of extensive-stage SCLC, recruitment of participants was significantly delayed.
According to the data that were collected, maintenance administration of niraparib failed: overall survival was not prolonged.
Clinical trial MENDIOLA (NCT02734004) phase 1/2
Indication: platinum-sensitive recurrent small cell lung cancer.
Sponsor: AstraZeneca.
Lynparza (olaparib), a PARP inhibitor, plus Imfinzi (durvalumab), a PD-L1 blocker.
Clinical trial NCT02498613 phase 2
Indication: metastatic or inoperable small cell lung cancer (stage III or IV) treated with platinum-containing chemotherapy.
Sponsors: National Cancer Institute (NCI), AstraZeneca.
A combination of the PARP inhibitor Lynparza (olaparib) and cediranib, a tyrosine kinase inhibitor of vascular endothelial growth factor receptor (VEGFR).
Clinical trial NCT03672773 phase 2
Indication: extensive-stage small cell lung cancer recurrent after and/or refractory to first-line platinum-containing therapy.
Sponsors: Jonsson Comprehensive Cancer Center (JCCC), Pfizer.
PARP inhibitor Talzenna/Talcenna (talazoparib) combined with temozolomide.
Targets: tyrosine kinases, LXR-β, Wee1, ATR, CDK4/CDK6, PI3Kδ, FucGM1, GD2, DLL3
Clinical trial NCT04234607 phase 3
Indication: previously untreated extensive-stage small cell lung cancer.
Sponsor: Chia Tai Tianqing Pharmaceutical Group (China).
A combination of the multi-target tyrosine kinase inhibitor Focus V (anlotinib), the PD-L1 blocker TQ-B2450 (CBT-502, APL-502), the chemotherapeutic etoposide and carboplatin.
Clinical trial NCT02922764 phase 1
Indication: extensive-stage small cell lung cancer that has progressed after first-line platinum-containing chemotherapy with or without a PD-(L)1 blocker.
Sponsor: Rgenix.
RGX-104, a nuclear liver X receptor beta (LXR-β) agonist, and docetaxel.
Clinical trial NCT02937818 phase 2
Indication: extensive-stage small cell lung cancer recurrent after and/or refractory to first-line platinum-containing therapy.
Sponsor: AstraZeneca.
Three different combinations are being tested:
- Imfinzi (durvalumab), a PD-L1 blocker, and tremelimumab, a CTLA-4 blocker
- adavosertib (AZD1775), a Wee1-like protein kinase inhibitor, and the chemotherapeutic carboplatin
- ceralasertib (AZD6738), an ATR serine/threonine protein kinase inhibitor, and Lynparza (olaparib), a PARP inhibitor.
Clinical trial NCT03085849 phase 1
Indication: extensive-stage small cell lung cancer that has progressed or recurred after first-line platinum-containing chemotherapy.
Sponsor: Columbia University Irving Medical Center (CUIMC).
A cocktail of Imfinzi (durvalumab), a PD-L1 blocker, tremelimumab, a CTLA-4 blocker, and guadecitabine (SGI-110), a next-generation hypomethylating chemotherapy.
Clinical trial NCT03041311 phase 2
Indication: first-line treatment of extensive-stage small cell lung cancer.
Sponsor: G1 Therapeutics.
Tecentriq (atezolizumab), a PD-L1 blocker, over chemotherapy (etoposide plus carboplatin) along with or without trilaciclib, a cyclin-dependent kinase 4 and 6 (CDK4 and CDK6) inhibitor.
Clinical trial NCT02646748 phase 1
Indication: advanced or metastatic small cell lung cancer recurrent after and/or refractory to first-line platinum-containing therapy or with intolerance to standard therapy.
Sponsor: Incyte.
Parsaclisib (INCB050465), a highly selective inhibitor of the delta isoform of phosphoinositide 3-kinase (PI3Kδ), together with Keytruda (pembrolizumab), a PD-1 blocker.
Clinical trial NCT02247349 phase 1/2
Indication: small cell lung cancer recurrent and/or refractory to first-line treatment with platinum-containing chemotherapies.
Sponsor: Bristol-Myers Squibb.
Monotherapy with BMS-986012 or its combination with Opdivo (nivolumab), a PD-1 blocker.
BMS-986012 is a monoclonal antibody against ganglioside fucosyl-GM1 (FucGM1), a sphingolipid monosialoganglioside and tumor-associated antigen (TAA) overexpressing on tumor cells, including SCLC.
Clinical trial DISTINCT (NCT03098030) phase 2/3
Indication: small cell lung cancer recurrent or progressive during or after first-line platinum-containing chemotherapy.
Sponsor: United Therapeutics.
Unituxin (dinutuximab) with irinotecan — comparison with irinotecan or topotecan monotherapy.
Dinutuximab is a monoclonal antibody against disialoganglioside GD2, a tumor-specific antigen (TSA) overexpressed on cells of various neuroectodermal tumors, including SCLC.
In early February 2020, United reported that a clinical trial of the experimental therapy was unsuccessful: it failed to extend overall survival relative to irinotecan.
Clinical trial NCT03392064 phase 1
Indication: extensive-stage small cell lung cancer recurrent after and/or refractory to first-line platinum-containing chemotherapy.
Sponsor: Amgen.
Adoptive CAR-T therapy AMG 119, targeting delta-like canonical Notch ligand 3 (DLL3), which is associated with cancer stem cells and is expressed on the cell surface in more than 80% of tumors in SCLC.
By the way, AbbVie’s tremendous efforts to clinically test rovalpituzumab tesirine (Rova-T), a monoclonal antibody conjugate carrying the cytotoxic pyrrolobenzodiazepine (PBD) and targeting DLL3, failed miserably.
Clinical trial NCT03319940 phase 1
Indication: extensive-stage small cell lung cancer, either recurrent after and/or refractory to first-line platinum-containing chemotherapy, or its maintenance therapy after response to the latter.
Sponsor: Amgen.
AMG 757, a bispecific monoclonal BiTE antibody targeting DLL3 and CD3, administered alone or in combination with Keytruda (pembrolizumab), a PD-1 blocker.