Highlights
China’s Hua Medicine has developed the drug dorzagliatin, which can “functionally cure” type 2 diabetes mellitus, that is, bring it into long-term and sustained remission, which lasts without taking any blood glucose-lowering medications. Remission refers to normal or nearly normal blood glucose levels.
It refers to patients diagnosed with diabetes recently, a population of patients whose disease has not yet progressed to a very advanced stage.
Dorzagliatin works by modulating glucokinase (“glucose sensor”), which controls key functions impaired in type 2 diabetes such as insulin and glucagon secretion by the pancreas and glycogen storage in the liver.
In early October 2022, dorzagliatin, for which an application was sent in March 2021, received marketing approval in China.
The drug, called HuaTangNing (华堂宁), is approved for use either monotherapeutically by previously untreated patients with type 2 diabetes or in combination with metformin by diabetics already receiving hypoglycemic therapy. No dose adjustment is required in the presence of chronic kidney disease (CKD).
Bayer has been selected as a strategic partner, which has obtained exclusive marketing and promotional rights for the drug and has already paid Hua 300 million yuan ($47.5 million) upfront, promising up to 4.18 billion yuan ($661.4 million) more as dorzagliatin is sold.
In the United States, Hua intends to promote dorzagliatin to treat not only type 2 diabetes, but also type 1 diabetes. One of the main issues of the latter is the daily fluctuation of blood glucose levels, when patients do not manage to keep their blood glucose levels within the normal range for as long as possible throughout the day (time in range, TIR). Hua is going to conduct clinical trials of dorzagliatin in the context of type 1 diabetes, first, to improve glycemic control and protection against hypoglycemia and, second, to preserve beta-cell function in an attempt to delay or prevent the progression of type 1 diabetes.

Twymeeg: Completely New Drug for Treatment of Type 2 Diabetes Mellitus
Imeglimin is a universal anti-diabetic drug that incorporates the power of all existing glucose-lowering drugs.
Dorzagliatin and Remission of Type 2 Diabetes Mellitus
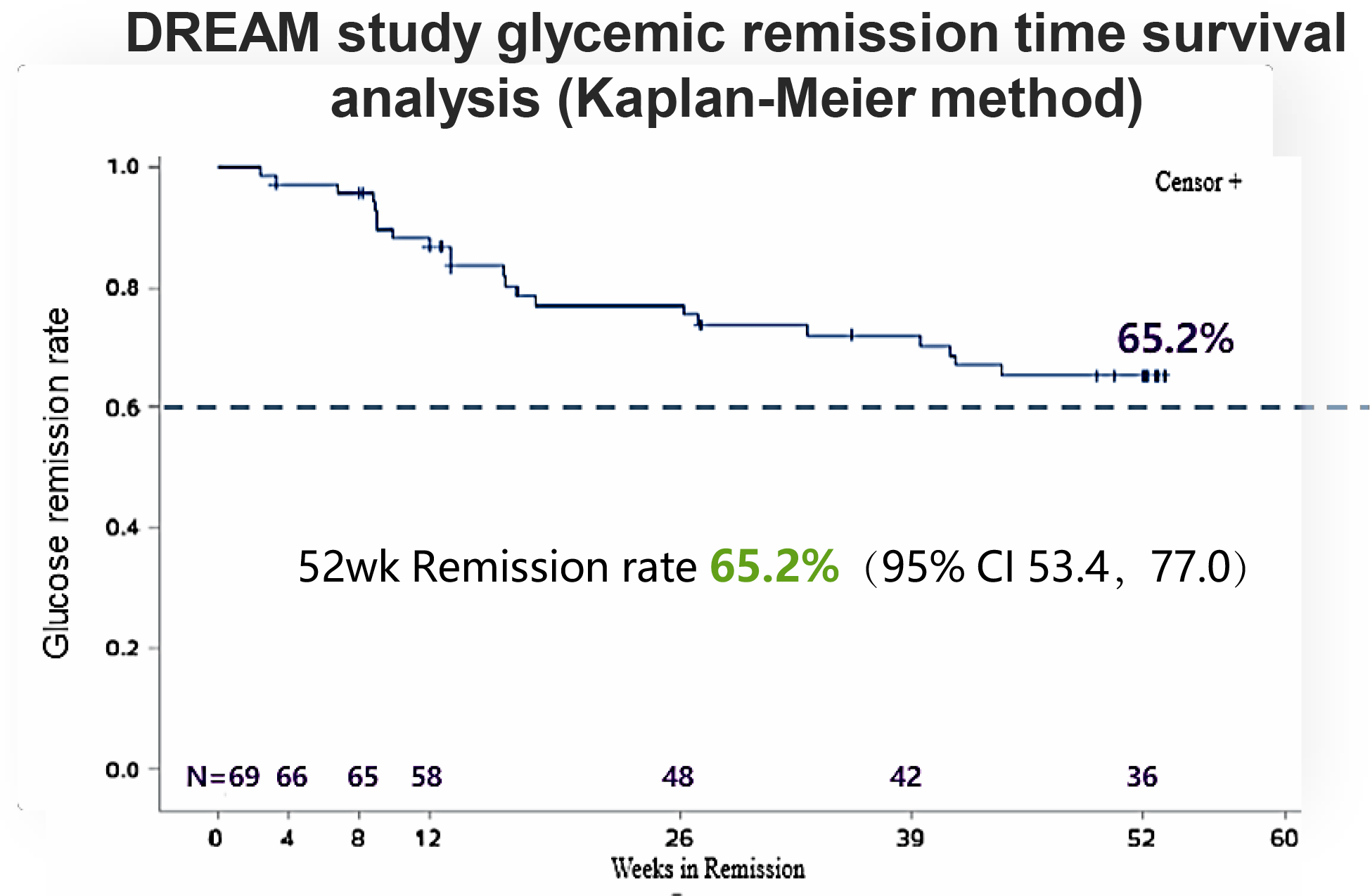
The DREAM (NCT03141073) phase 3 (observational, non-pharmacological, non-interventional) clinical trial aimed to follow patients who had completed the SEED (NCT03173391) phase 3 clinical trial and who had achieved glycemic control (glycated hemoglobin [HbA1c] < 7.0%). SEED participants with previously untreated type 2 diabetes were treated with dorzagliatin for 52 weeks.
After 52 weeks of follow-up of 69 patients who did not take any blood glucose-lowering drugs but adhered to a diet and increased physical activity, it was found that two-thirds of the subjects remained in clinical remission of type 2 diabetes, which meant maintaining HbA1c at or close to normal levels. While at the beginning of DREAM the HbA1c level was 6.61%, it stopped at 6.92% upon completion.
At the end, the reported remission rate for type 2 diabetes after 52 weeks of follow-up was 65.2% (95% CI: 53.4–77.0).
Remission was confirmed by the 2-hour postprandial glucose (2h-PPG) test: Its level at the beginning of DREAM was 250 mg/dL (13.87 mmol/L) and at the end was 234 mg/dL (12.98 mmol/L). This also proved to be true in terms of reduced insulin resistance index and improved beta-cell function: At the 52-week DREAM follow-up period, HOMA2-IR changed from 1.58 to 1.46 (less is better) and HOMA2-β changed from 43.80 to 56.6 (more is better).
- Homeostatic Model Assessment (HOMA) is a method for quantifying insulin resistance and pancreatic beta cell function as a percentage of the normal control population. The method is based on computer modeling and is driven by fasting glucose, insulin, and C-peptide levels. HOMA2 is an advanced computer model that takes into account factors of hepatic and peripheral insulin resistance and a physiological measure of glucose homeostasis.
According to a consensus decision adopted in late August 2021 by the U.S., European, and British diabetic physician organizations, remission of type 2 diabetes is defined as reaching near-normal HbA1c levels (< 6.5%), or fasting plasma glucose levels (< 126 mg/dL, < 7.0 mmol/L), measured at least 3 months after stopping any anti-diabetic medication.
Based on this consensus, the clinical remission status of type 2 diabetes mellitus within DREAM was recorded with a frequency of 52.0% (95% CI: 31.2–69.2).
Because the patients who participated in SEED were newly diagnosed with type 2 diabetes (on average, one year ago) and had not previously received any anti-diabetic treatment, Hua believes that the data collected in DREAM support the rationale for the earliest possible therapy of diabetes to increase the chance of clinical remission. The idea is that urgent pharmacological intervention in the progression of diabetes can stop the degeneration of the “glucose sensor” and restore and enhance its function thereby preventing disruption of pancreatic beta cells function.
Now the leading approaches to providing diabetes remission status are the following: bariatric surgery (worldwide), radical weight loss (in Western countries), intensive insulin therapy (in China).
Follow-up of the DREAM participants is ongoing: the duration of clinical remission of type 2 diabetes needs to be clarified.
Be that as it may, it is already clear that dorzagliatin is the first and only drug that has succeeded in bringing early diabetes into sustained remission. Similar attempts with other blood glucose-lowering drugs (metformin, liraglutide, insulin) have failed.
Dorzagliatin: Mechanism of Action
Continuous deterioration of beta-cell function is a common problem in type 2 diabetes mellitus. Reduced beta-cell mass and disruption of their normal processes lead to changes in the threshold of glucose-stimulated insulin secretion and homeostasis status. A large number of different anti-diabetic drugs (10 classes at present) aimed at reducing blood glucose levels have been proposed for the therapy of this disease. However, none of the existing drugs, even in combination with others, is able to stop the progression of diabetes. This is why there is a great need for new medications with an alternative mechanism of action.
Oral dorzagliatin (dorzagliatin, HMS5552, RO5305552), formerly known as sinogliatin, is a dual glucokinase activator (GKA) and is the fourth generation drug in this class, intended to restore impaired glucose homeostasis, providing proper glycemic control without the risk of hypoglycemia, dyslipidemia, liver damage, or weight gain. Dorzagliatin targets glucokinase both in pancreas and liver. Dorzagliatin belongs to full glucokinase activators: it increases the maximum enzymatic reaction rate (Vmax) of glucokinase.
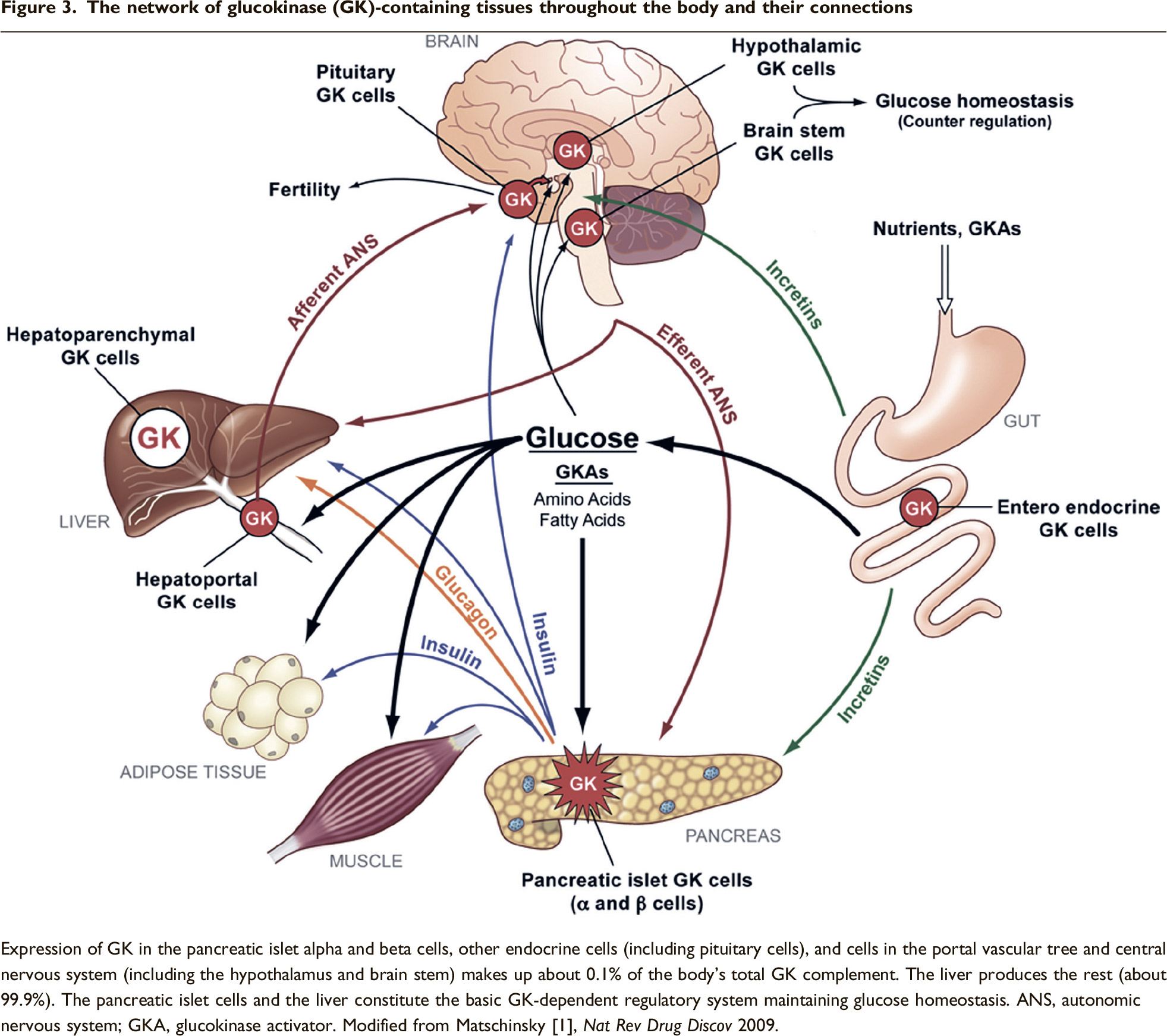
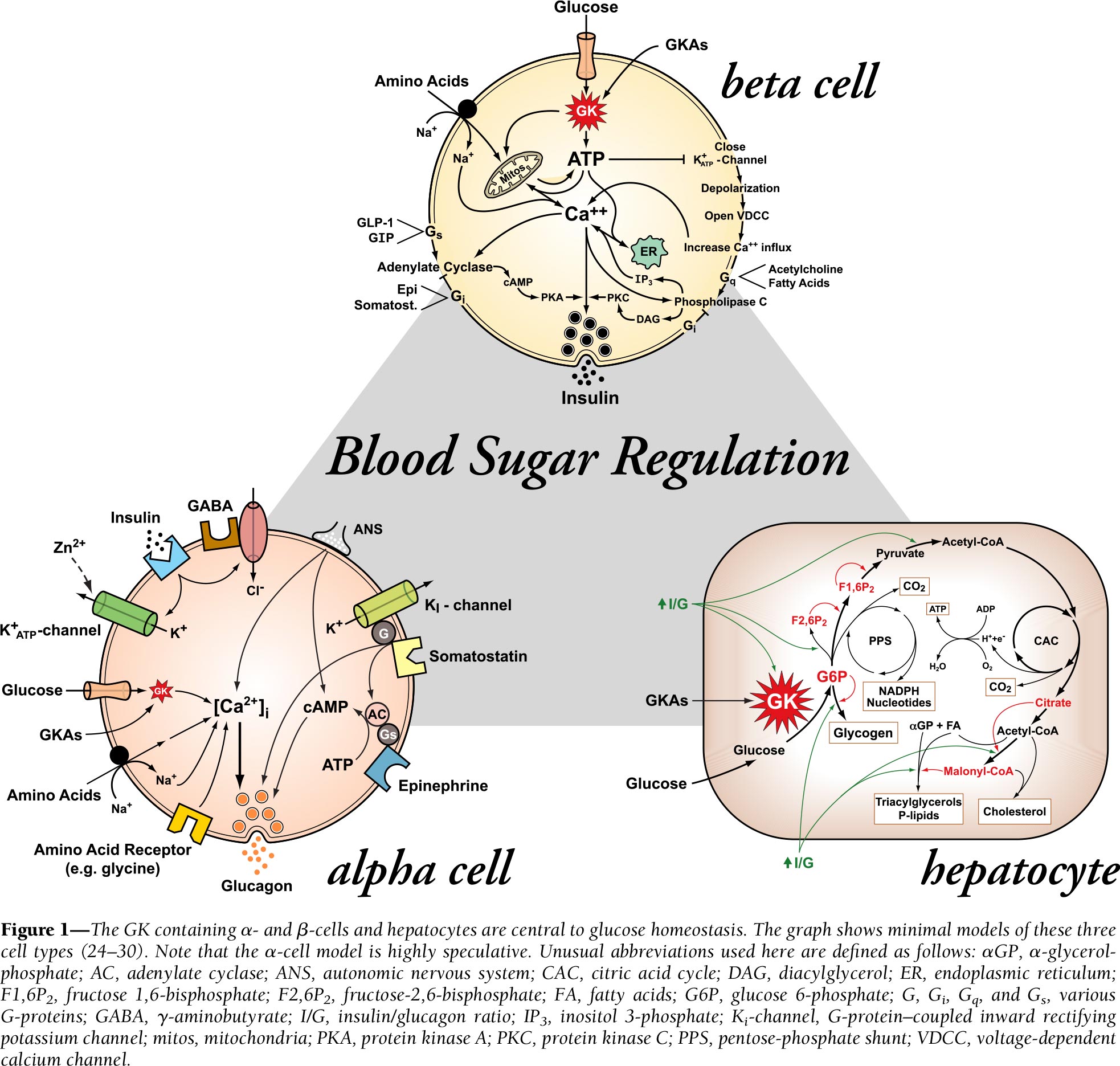
Glucokinase plays a decisive role in glucose homeostasis maintaining blood glucose levels within a narrow range. Glucokinase expression is limited to glucose-sensitive and glucose-dependent tissues in the pancreas (islet alpha and beta cells), liver (hepatocytes), brain (glucose-sensitive neurons in the ventromedial and arcuate nuclei of the hypothalamus), and gastrointestinal tract (K and L cells). In pancreatic alpha and beta cells, glucokinase, acting as a “glucose sensor,” responds to changes in glucose concentration by controlling the release of its dependent hormones such as insulin and glucagon. In hepatocytes, glucokinase, working as a “gatekeeper” of glucose, in the presence of insulin regulates the absorption of glucose received from food and converting it into accumulated glycogen. Glucose-sensitive neurons regulate glucose homeostasis (especially reaction to hypoglycemia), energy expenditure, satiety, appetite, and weight maintenance. Glucokinase in enteroendocrine cells provides an early metabolic response realized by the secretion of incretins.
The net effect of the above glucokinase-mediated pathways is to reduce blood glucose levels by both direct (insulin-mediated) and indirect pathways. Therefore, pharmacological control of glucokinase activity is a workable method to intervene in glucose homeostasis since glucokinase activation leads to a decrease in glucose levels while glucokinase activity is reduced in patients with type 2 diabetes.
It is known that inactivating glucokinase mutations lead to hyperglycemia; activating mutations lead to hyperinsulinemia and hypoglycemia. Disruption of glucokinase expression and activity is closely linked to the loss of pharmacological control of type 2 diabetes — due to the disappearance of glucose and insulin sensitivity in the pancreas and liver. Nevertheless, pathological glucokinase alterations may well be reversed by medication.
Glucokinase activators like dorzagliatin are turning to “glucose sensor” modulation in an attempt to regain control of impaired functions in type 2 diabetes such as insulin and glucagon secretion in the pancreas and glycogen accumulation in the liver.
It is possible that glucokinase activators could have a more pronounced beneficial effect on the course of diabetes than in the case of mechanisms to suppress high blood glucose levels through traditional stimulation of insulin production or promotion of glucose excretion or uptake, which are handled, for example, by biguanides (metformin), gliptins (dipeptidyl peptidase-4 [DPP4] inhibitors), gliflozins (sodium-glucose co-transporter type 2 [SGLT2] inhibitors), and glucagon-like peptide-1 receptor (GLP-1R) agonists.
Hua licensed dorzagliatin from Roche in December 2011, paying $2 million up front. The Swiss pharma giant will receive a certain royalty from the sale of the finished drug.
Dorzagliatin for Treatment of Type 2 Diabetes Mellitus: Clinical Trials
The dorzagliatin’s application sent by Hua to the Chinese regulator in March 2021 included data from two successful pivotal clinical trials that examined the drug’s monodosing and its combination with metformin.
Monotherapy of Diabetes With Dorzagliatin
The SEED (NCT03173391) phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial invited adult patients (n=463) from China with previously untreated type 2 diabetes.
Among the trial inclusion criteria: an HbA1c between 7.5% and 11.0% and a body mass index (BMI) in the range of 18.5–35.0 kg/m2.
Participants adhering to diet and physical activity were given 75-mg dorzagliatin or placebo twice daily.
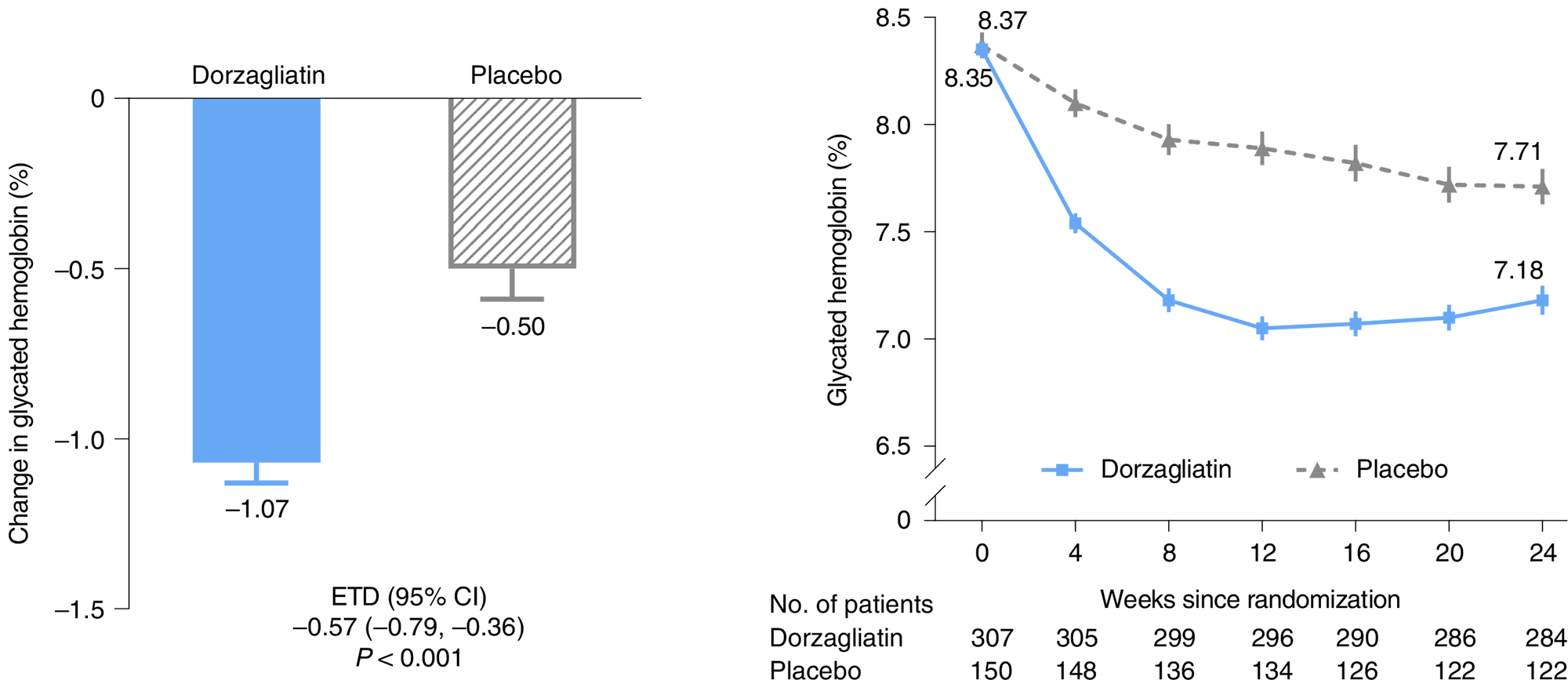
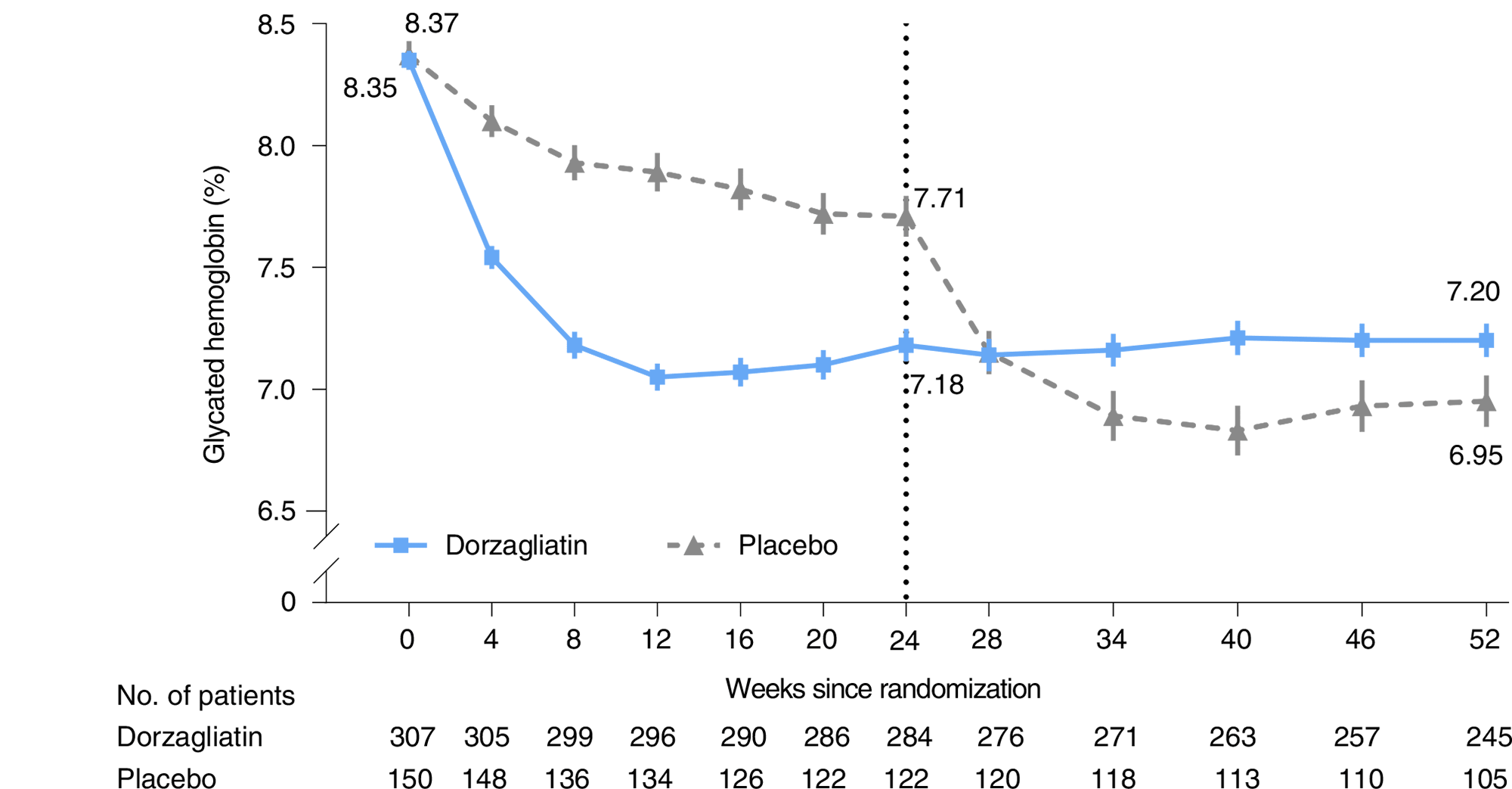
After 24 weeks of double-blind period of SEED, the HbA1c reduction in the dorzagliatin group was 1.07% (95% CI: 0,95 to 1,19) — versus 0.50% (95% CI: 0,32 to 0,68) in the placebo group; the difference was 0.57% (95% CI: 0,36 to 0,79) [p<0.001].
Simultaneously, 42.5% of patients receiving dorzagliatin reached the target HbA1c level below 7.0% — vs. 17,3% in the control group (p<0.001): the odds ratio (OR) was 4.20 (95% CI: 2.51 to 7.02).
The therapeutic effect of dorzagliatin was characterized by rapidity: by the 8th week of treatment, an HbA1c level below 7.0% was registered in 40.8% of patients — vs. 10.0% in the placebo group.
Dorzagliatin administration demonstrated a decrease in insulin resistance, as measured by HOMA2-IR, and an improvement in beta-cell function, as measured by HOMA2-β: a decrease of 0.21 — vs. a decrease of 0.15 and an increase of 2.56 — vs. a decrease of 0.72, respectively.
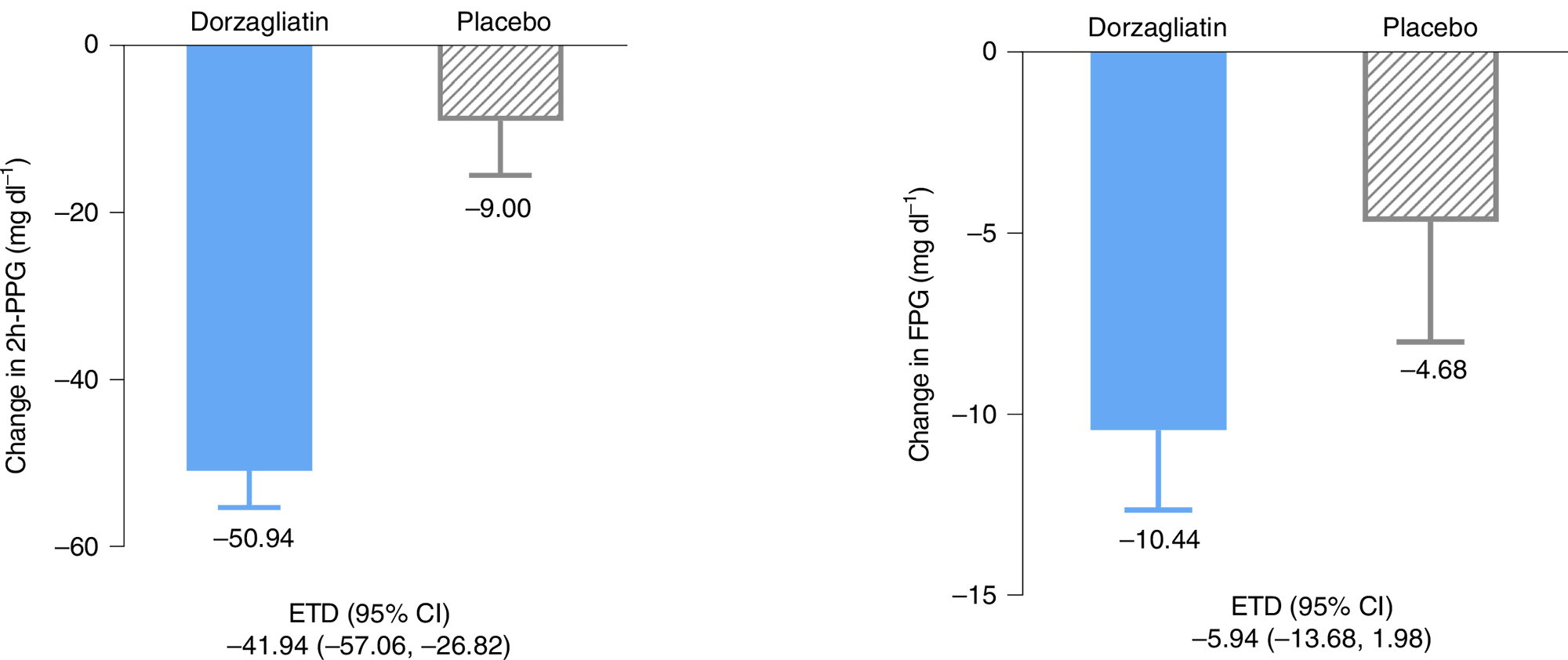
In the dorzagliatin group, there was a decrease in two-hour postprandial glucose (2h-PPG) test: by 50.94 mg/dL (2.8 mmol/L) — vs. 9.00 mg/dL (0.5 mmol/L) [p<0.001]. There was a decrease in fasting plasma glucose (FPG): by 10.44 mg/dL (0.6 mmol/L) — vs. 4.68 mg/dL (0.3 mmol/L).
The safety profile of dorzagliatin was favorable: acceptable tolerability, most adverse reactions were mild in severity, no tendencies for abnormal changes in laboratory parameters and ECG, hypoglycemia events was reported in 1 of 310 patients (0.3%), no cases of severe hypoglycemia were recorded.
At the end of the 28-week SEED’s open-label period that followed, when all subjects were prescribed dorzagliatin, the picture that emerged was as follows. The group that originally received dorzagliatin maintained the same HbA1c level (7.20%), whereas the placebo group that switched to the drug showed a decrease in HbA1c to 6.95%.
Combination Treatment of Diabetes With Dorzagliatin and Metformin
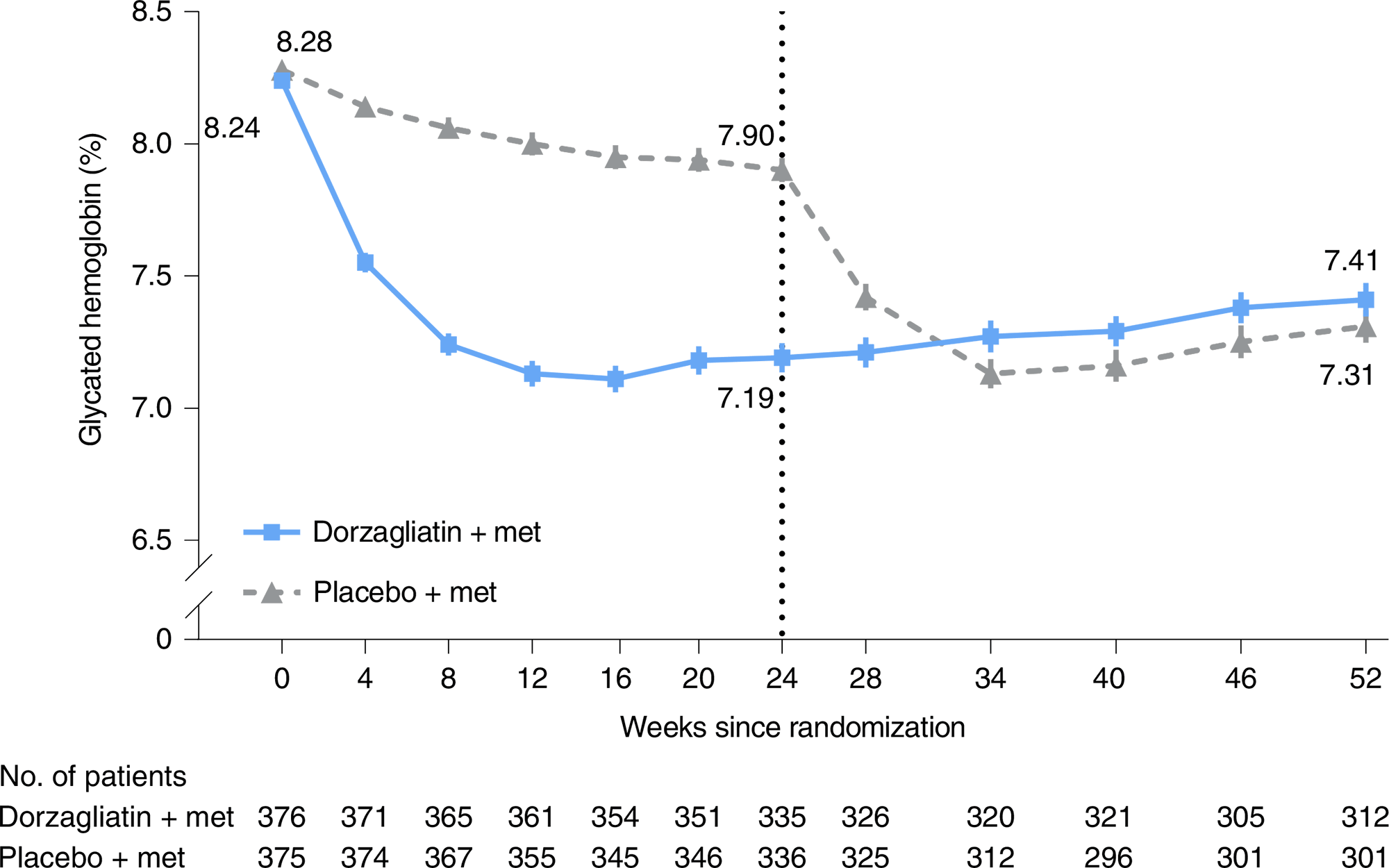
The DAWN (NCT03141073) phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial invited adult patients (n=767) from China who were not able to control glucose levels with the maximum-tolerated dose of metformin (≥ 1500 mg/day).
Among the trial inclusion criteria: an HbA1c between 7.5% and 10.0%, BMI in the range of 18.5–35.0 kg/m2.
Participants adhering to diet and physical activity were given 75-mg dorzagliatin or placebo twice daily — on a background of metformin at a dose of 1,500 mg/day.
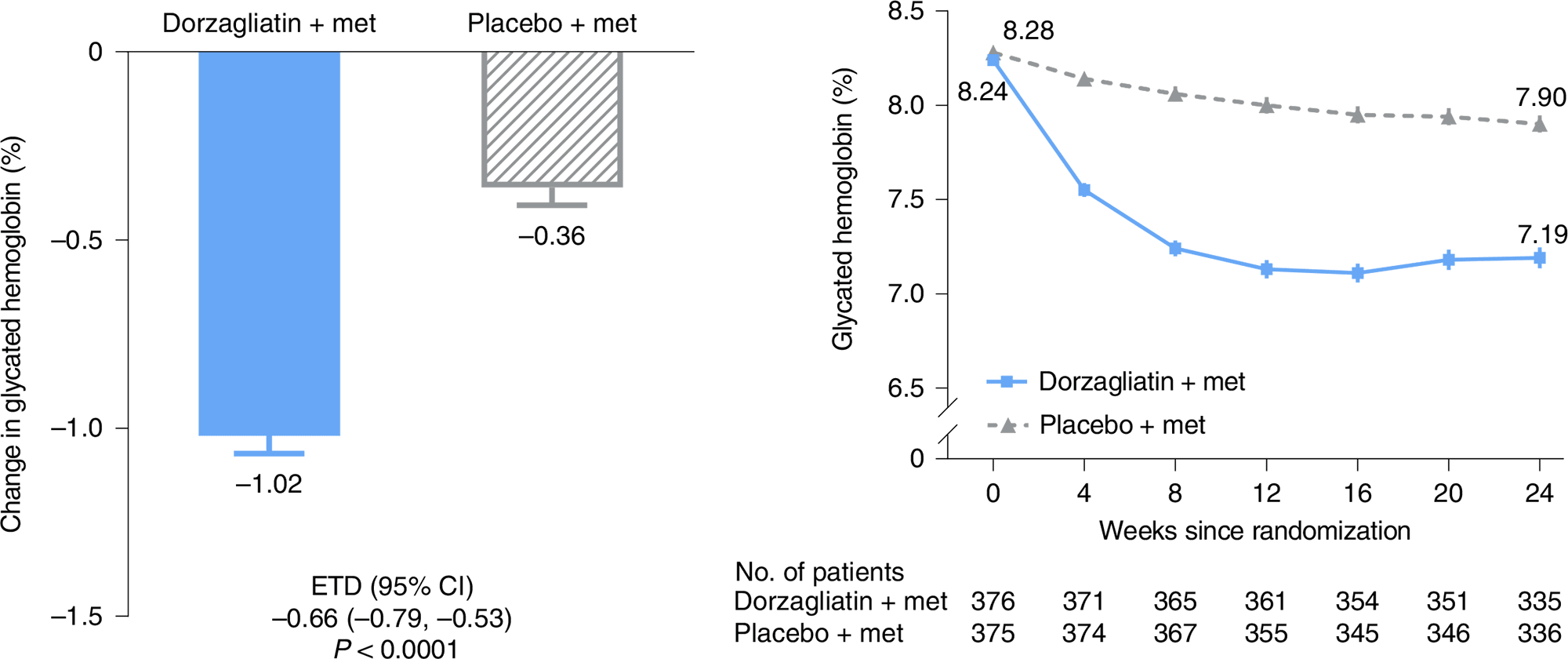
After 24 weeks of double-blind period of DAWN, the HbA1c reduction in the dorzagliatin group was 1.02% (95% CI: 0.93 to 1.11) — versus 0.36% (95% CI: 0.26 to 0.45) in the placebo group; the difference was 0.66% (95% CI: 0.53 to 0.79) [p<0.0001].
Among other efficacy measures:
- 44.4% of patients reached the target HbA1c level less than 7.0% — vs. 10.7%: OR 7.60 (95% CI: 5.05 to 11.42)
- HOMA2-IR: −0.17 — vs. −0.09
- HOMA2-β: +3.82 — vs. +1.40
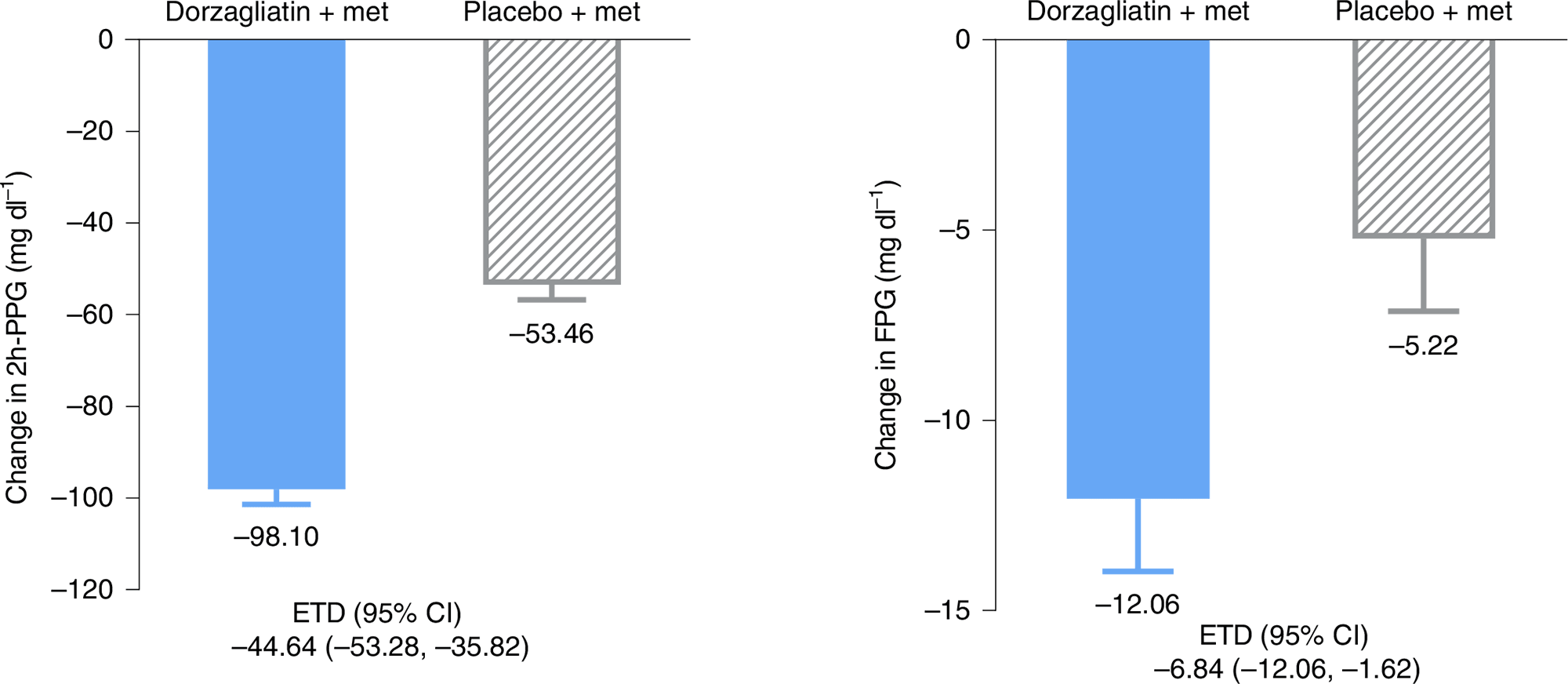
- 2h-PPG: −92.2 mg/dL (−5.1 mmol/L) — vs. −104.9 mg/dL (−5.8 mmol/L)
- FPG: −12.1 mg/dL (−0.7 mmol/L) — vs. −5.2 mg/dL (−0.3 mmol/L).
No significant safety problems with dorzagliatin were identified.
At the end of the 28-week DAWN’s open-label period that followed, when all subjects prescribed dorzagliatin, the groups initially receiving dorzagliatin and placebo were nearly equal showing HbA1c levels of 7.41% and 7.31%, respectively.
Diabetic Kidney Disease
The clinical trial NCT04324424 phase 1 (open-label, non-randomized) investigated the suitability of dorzagliatin in renal failure, which in the form of diabetic kidney disease (diabetic nephropathy) is one of the most common complications of type 2 diabetes. It has been demonstrated that dorzagliatin is safe in impaired renal function: the drug can be prescribed without any adjustment of the therapeutic dose.
Dorzagliatin: What’s Next
Hua hopes to bring dorzagliatin into clinical practice as widely as possible, and therefore continues to build up the range of relevant clinical trials for this drug.
Thus, Hua anticipates that dorzagliatin will prove useful in combination with other blood glucose-lowering drugs. For example, its combination with empagliflozin, an SGLT2 inhibitor, should increase the beneficial cardiological effect of the latter in terms of reducing the risk of major adverse cardiovascular events (MACE) such as hospitalization for heart failure, non-fatal heart attack, or non-fatal stroke.
A cocktail of dorzagliatin and insulin might help in severe diabetes mellitus types 1 and 2.
The combination of dorzagliatin and a GLP-1R agonist seems interesting in the context of Alzheimer’s disease treatment. Novo Nordisk is testing oral semaglutide for the early form of this neurodegenerative pathology for nothing.
Dorzagliatin in combination with pioglitazone might also be found in the treatment of nonalcoholic steatohepatitis (NASH).
Dorzagliatin: Expert Comments
Dorzagliatin’s therapeutic success could still be better because in phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial NCT02561338 in a subgroup of previously untreated patients with type 2 diabetes the drug demonstrated a much more pronounced anti-diabetic effect providing an HbA1c difference from placebo of 1.04% (p=0.0002) over 12 weeks.
It is possible, however, that the results of the SEED (NCT03173391) were biased by the high response in the control group. It is quite possible: a systematic meta-analysis of clinical trials of DPP4 inhibitors found that the decrease in HbA1c among placebo-treated patients with type 2 diabetes was significantly more dramatic when it came to Chinese patients — compared to patients from Western countries. This can be explained by the fact that Chinese residents, first, are willing to strictly follow the study protocol as they also have access to additional medical care, which would otherwise be difficult to achieve. And second, the Chinese are turning to Traditional Chinese Medicine (TCM) in parallel and almost in droves: some herbs have been proven to lower blood glucose levels.
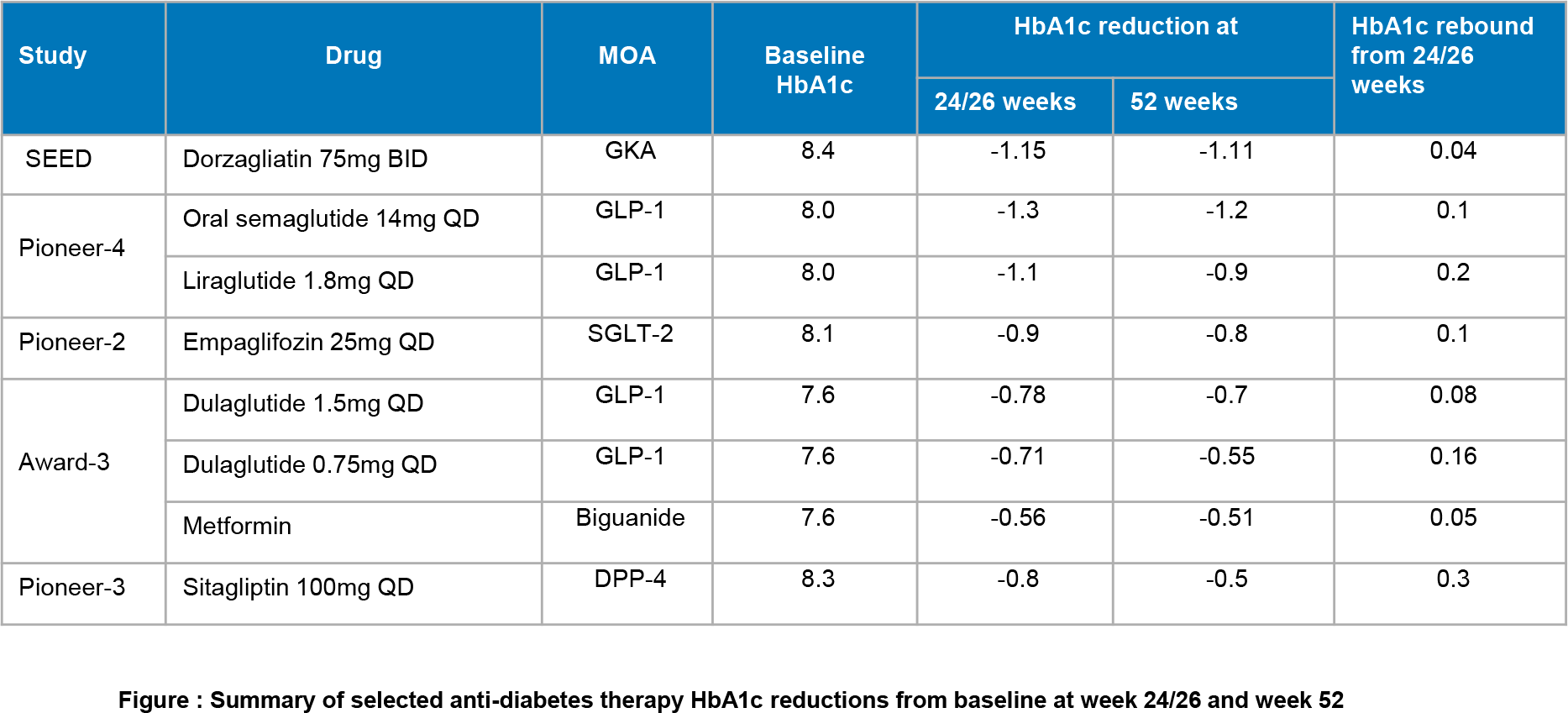
Again, the therapeutic efficacy of dorzagliatin is not beyond that of the GLP-1R agonists and SGLT2 inhibitors that exist in abundance on the market, which can lower HbA1c by a relative 0.3%–0.7% and 0.6%–1.16%, respectively.
In any case, despite the rich pharmacological armamentarium of anti-diabetic drugs (there are 10 classes of such medicines), dorzagliatin will take its rightful place. An indirect comparison of its blood glucose-lowering efficacy with other drugs proves this.
Two decades in a row many pharmaceutical companies tried to bring glucokinase activators to commercial readiness but nothing came out of it; only dorzagliatin was able to complete pivotal clinical trials of phase 3. The development of glucokinase activators is accompanied by the need to solve two major problems related to overcoming rapid development of drug resistance (reflected by insufficient reduction of HbA1c) and reducing the frequency of adverse reactions due to treatment (hypoglycemia, rise in serum triglycerides, increase in blood pressure, appearance of a large number of unwanted metabolites, etc.).
In the case of dorzagliatin, it was possible to develop a molecule that enhances the enzymatic activity of glucokinase at therapeutically effective concentrations while preserving the glucose-sensitive function of glucokinase and without disturbing its glucose-dependent activity. At the same time, dorzagliatin starts to act only when blood glucose levels exceed the normal level of 4 mmol/L, thus avoiding hypoglycemia.
Glucokinase activators, as a pharmacological class of drugs, can be divided into two groups:
- Dual glucokinase activators that target glucokinase in both the pancreas and the liver. Dual-acting molecules are subdivided, depending on their kinetic properties, into:
- Full glucokinase activators that increase the maximum enzymatic reaction rate (Vmax) of glucokinase: piragliatin (RO4389620), MK-0941, AMG 151 (ARRY-403), globalagliatin (LY2608204), and dorzagliatin by Roche, Merck & Co., Amgen/Array BioPharma, Yabao Pharmaceutical/Eli Lilly, and Hua Medicine.
- Partial glucokinase activators that reduce Vmax: e.g., AZD1656 and PF-04937319 (PB-201) by AstraZeneca and Pfizer/PegBio.
- Selective glucokinase activators that work exclusively with this enzyme in the liver: e.g., PF-04991532, TTP399 (GK1-399), and GKM-001 (ADV-1002401) by Pfizer, vTv Therapeutics, and Impetis Biosciences/Advinus Therapeutics.
The closest competitors of dorzagliatin are PB-201 and TTP399 with high therapeutic activity and low toxicity. Both have successfully passed phase 2 clinical trials: the first in the treatment of type 2 diabetes, the second in combination with insulin therapy of type 1 diabetes.
Extras
Dorzagliatin in drug-naïve patients with type 2 diabetes: A randomized, double-blind, placebo-controlled phase 3 trial. Nat Med. 2022 May;28(5):965-973. [source]
Dorzagliatin add-on therapy to metformin in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled phase 3 trial. Nat Med. 2022 May;28(5):974-981. [source]
Hua Medicine. 2021 Annual results presentation. March 17, 2022. [PDF]
Hua Medicine. Company presentation. December 15, 2021. [PDF]
Glucokinase as an emerging anti-diabetes target and recent progress in the development of its agonists. J Enzyme Inhib Med Chem. 2022 Dec;37(1):606-615. [source]
A comprehensive review on glucokinase activators: Promising agents for the treatment of type 2 diabetes. Chem Biol Drug Des. 2022 Feb;99(2):247-263. [source]
Recent clinical advances of glucokinase activators in the treatment of diabetes mellitus type 2. Pharmazie. 2020 Jun 1;75(6):230-235. [source]
Glucokinase activators for type 2 diabetes: Challenges and future developments. Drugs. 2020 Apr;80(5):467-475. [source]
Dorzagliatin monotherapy in Chinese patients with type 2 diabetes: A dose-ranging, randomised, double-blind, placebo-controlled, phase 2 study. Lancet Diabetes Endocrinol. 2018 Aug;6(8):627-636. [source]
Dorzagliatin (HMS5552), a novel dual-acting glucokinase activator, improves glycaemic control and pancreatic β-cell function in patients with type 2 diabetes: A 28-day treatment study using biomarker-guided patient selection. Diabetes Obes Metab. 2018 Sep;20(9):2113-2120. [source]
Development of a physiologically based pharmacokinetic model for sinogliatin, a first-in-class glucokinase activator, by integrating allometric scaling, in vitro to in vivo exploration and steady-state concentration-mean residence time methods: Mechanistic understanding of its pharmacokinetics. Clin Pharmacokinet. 2018 Oct;57(10):1307-1323. [source]
Effect of renal impairment on the pharmacokinetics and safety of dorzagliatin, a novel dual-acting glucokinase activator. Clin Transl Sci. 2022 Feb;15(2):548-557. [source]