Highlights
Apogee Therapeutics is developing monoclonal antibodies for the treatment of inflammatory and autoimmune diseases.
A key advantage of the experimental drugs lies in their ability to be dosed very infrequently in a maintenance therapeutic regimen. Thus, APG777, a monoclonal antibody against interleukin 13 (IL-13) being studied in the treatment of atopic dermatitis (eczema) and asthma (eosinophilic subtype), has the potential to be administered by subcutaneous injection once every quarter or six months. At least this follows from the interim results of the first clinical trial.
In comparison, maintenance treatment of eczema with the monoclonal antibodies Dupixent (dupilumab) and Ebglyss (lebrikizumab) requires subcutaneous injections every two and four weeks, respectively.
Apogee has other monoclonal antibodies with extended half-life in hand, targeting other targets relevant in the treatment of inflammatory and autoimmune diseases.
On the wave of positive news, Apogee stock quotes added 40%.

Innovative Treatment for Hypertension: One Shot Every Quarter or Even Six Months
Arterial hypertension is waiting for a major pharmacological breakthrough. Hundreds of millions of people will be saved.
APG777: Mechanism of Action
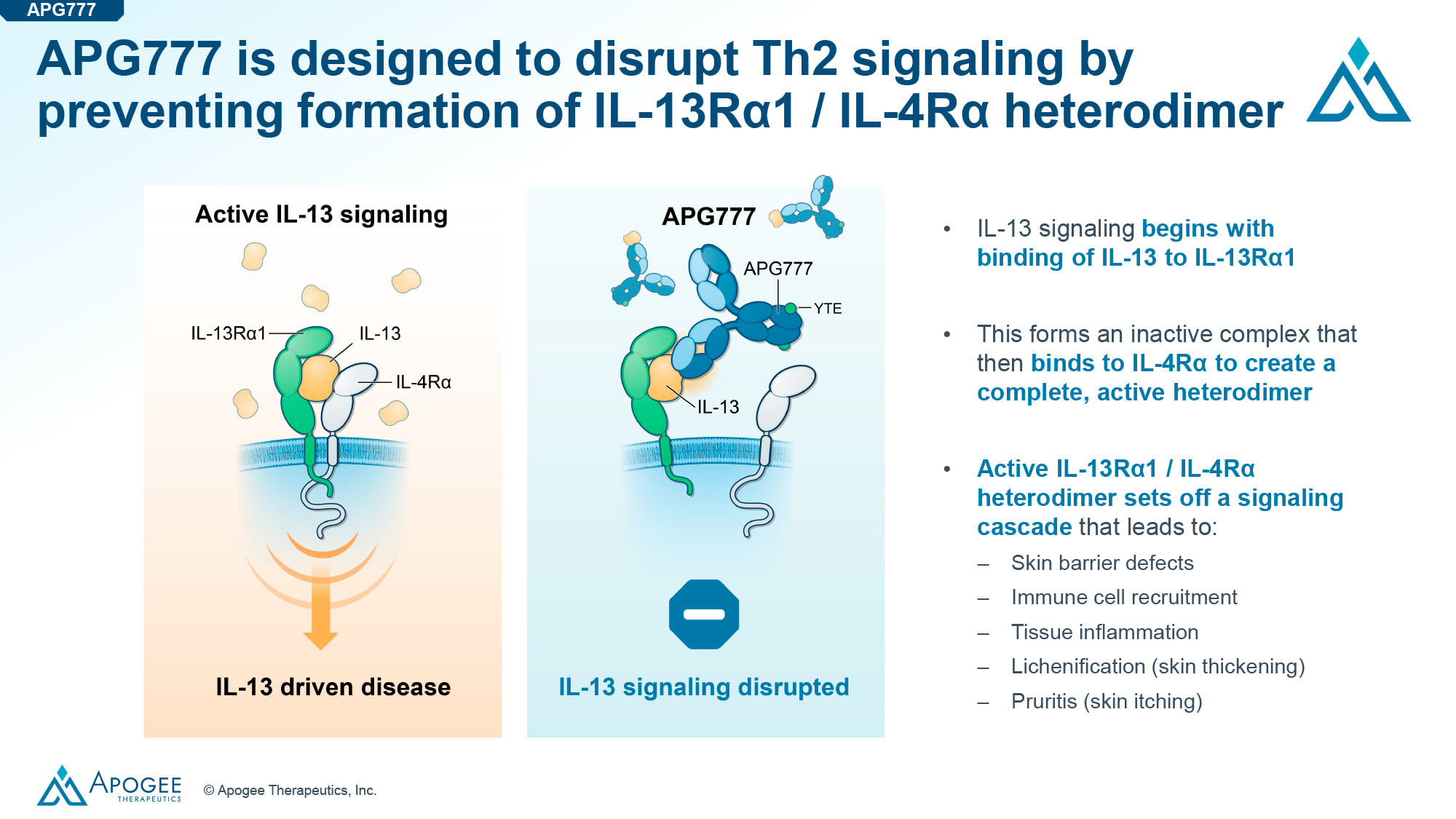
Interleukin 13 (IL-13) is a cytokine secreted predominantly by T helper type 2 (Th2) cells and plays a key role in the pathogenesis of atopic dermatitis (eczema), asthma and other inflammatory and autoimmune diseases [1] [2] [3].
The experimental drug APG777, developed by Apogee Therapeutics, is a humanized monoclonal IgG1 antibody with high affinity for IL-13. By binding to the latter, APG777 blocks heterodimerization of the signaling complex consisting of IL-13 and its two receptor subunits, interleukin 13 receptor alpha 1 (IL-13Rα1) and interleukin 4 receptor alpha (IL-4Rα). The result is the interruption of downstream signaling of type 2 inflammation [4].
The fragment crystallizable (Fc) region of APG777 contains a triple amino acid modification (YTE) intended to prolong the half-life by enhancing binding to the neonatal Fc receptor (FcRn) under acidic pH conditions. Additionally, Fc region contains two amino acid modifications (LALA) designed to ablate Fc and complement effector functions [4] [5].
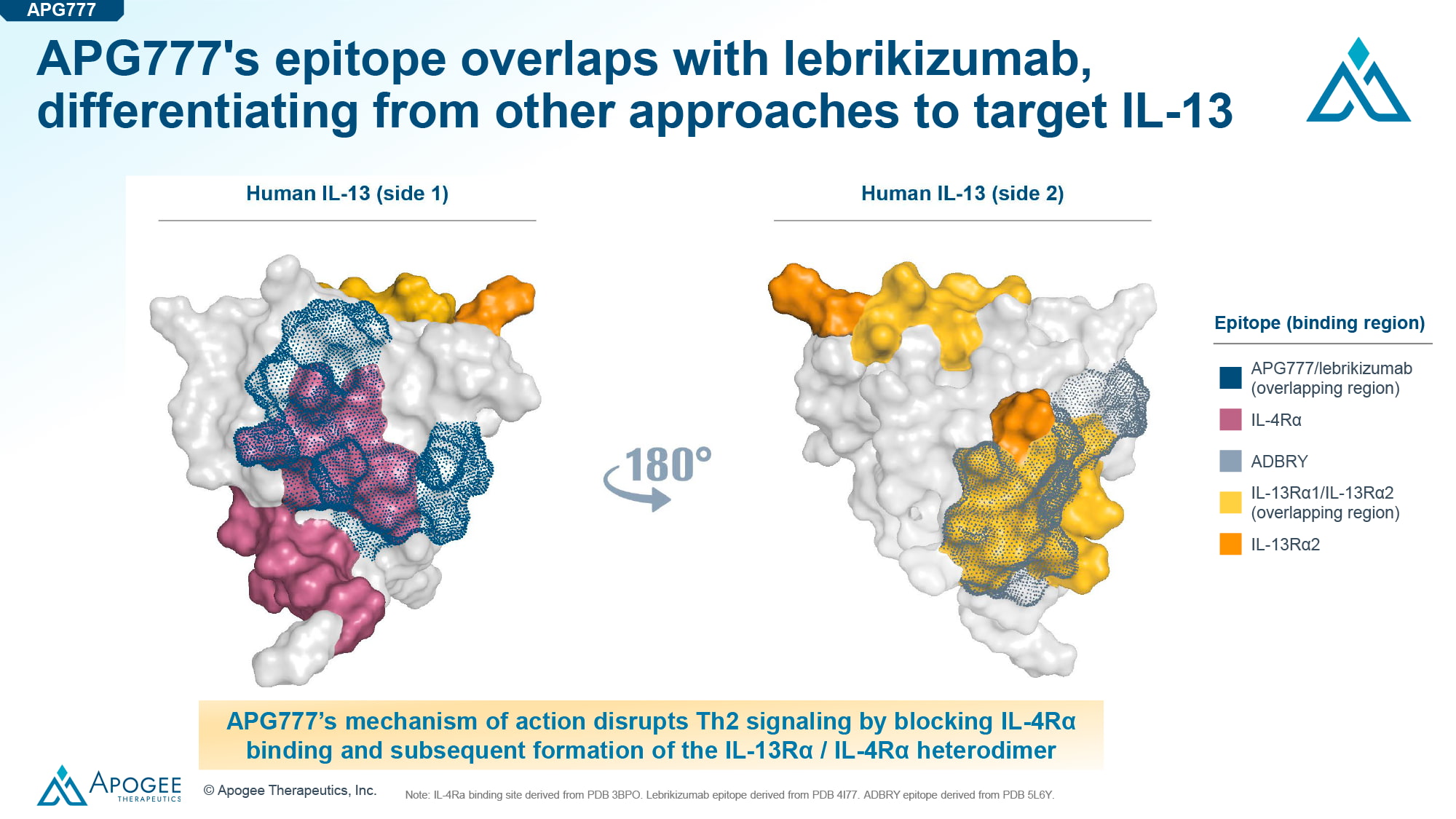
APG777 exhibits affinity for IL-13 at a level comparable to other anti-IL-13 monoclonal antibodies such as lebrikizumab and tralokinumab, commercialized by Spain’s Almirall, which acquired European rights from Eli Lilly, and Danish Leo Pharma under the brand names Ebglyss and Adbry / Adtralza for the treatment of atopic dermatitis [6].
The potency of APG777 is comparable to that of lebrikizumab and dupilumab, promoted by Sanofi and Regeneron Pharmaceuticals as Dupixent, a monoclonal antibody against IL-13 and interleukin 4 (IL-4).
There is no doubt about the therapeutic efficacy of APG777 when one considers a purely mechanistic argument: The monoclonal antibody binds to an epitope on IL-13 that overlaps with the binding epitope of lebrikizumab.
APG777: Clinical Details
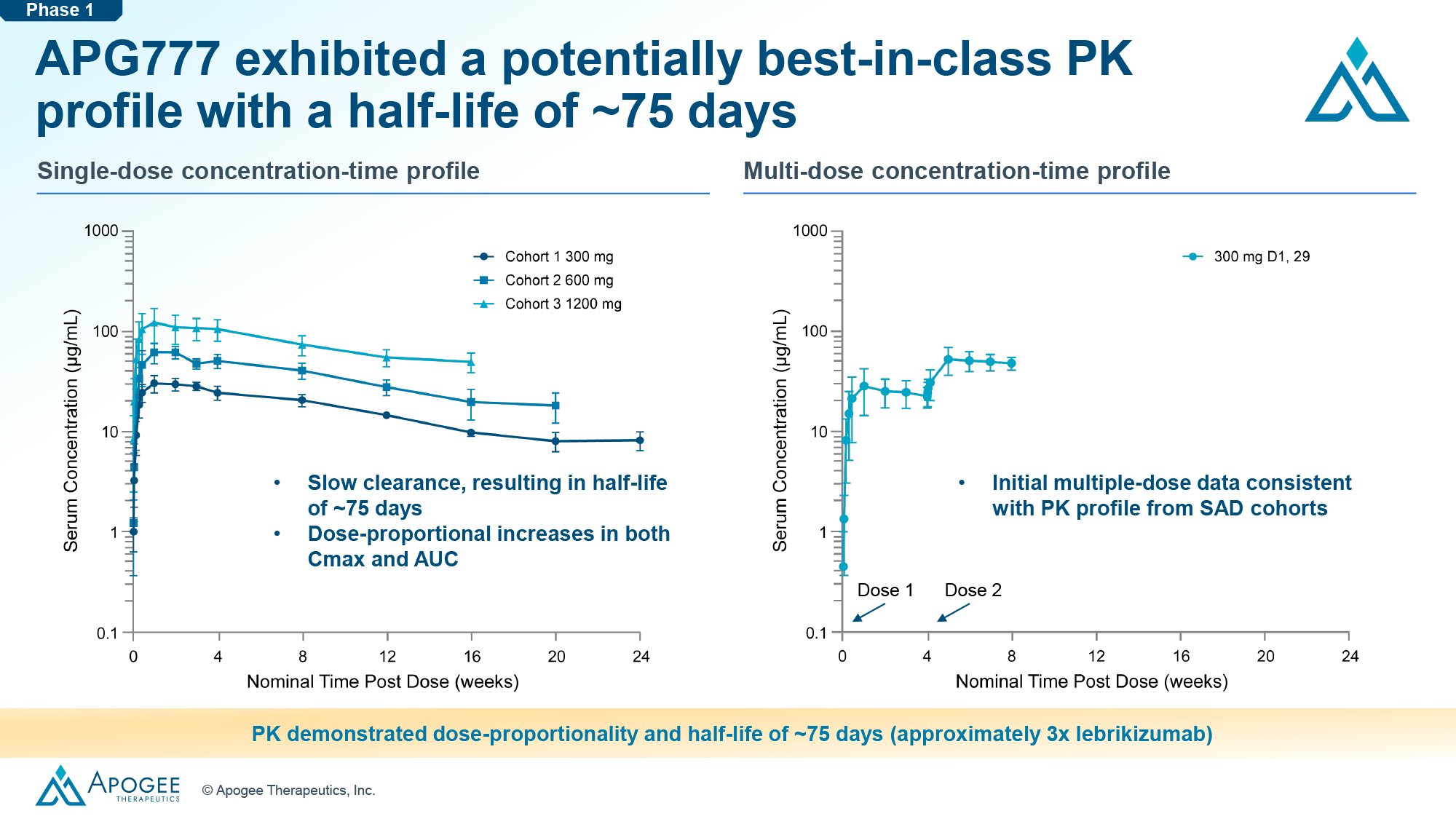
Apogee Therapeutics emphasizes that APG777 is superior to lebrikizumab in every way possible, thus pushing for direct competition with it.
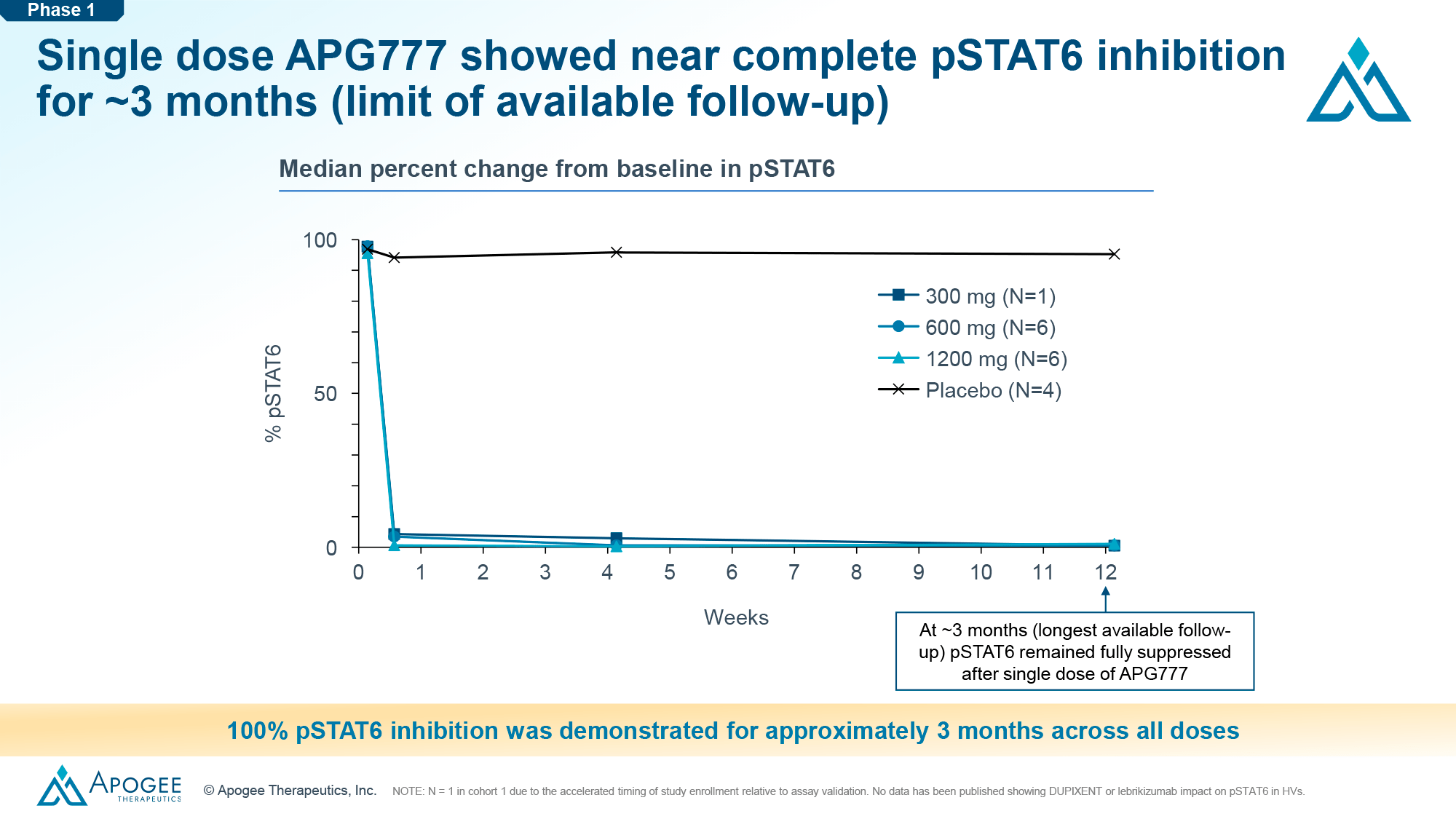
Thus, a phase 1 clinical trial found that the half-life of APG777 is approximately 75 days, which is about three times longer than that of lebrikizumab.
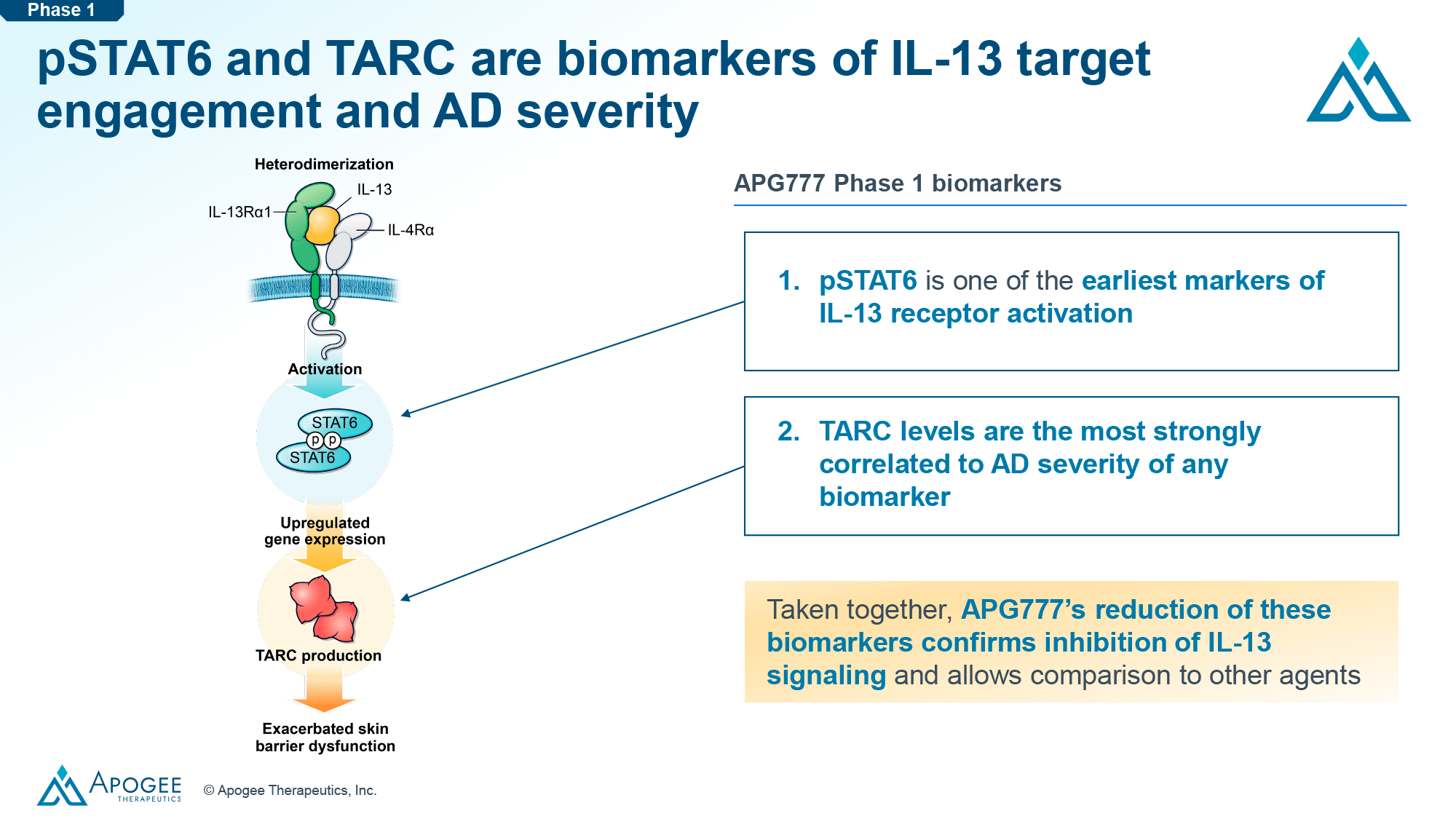
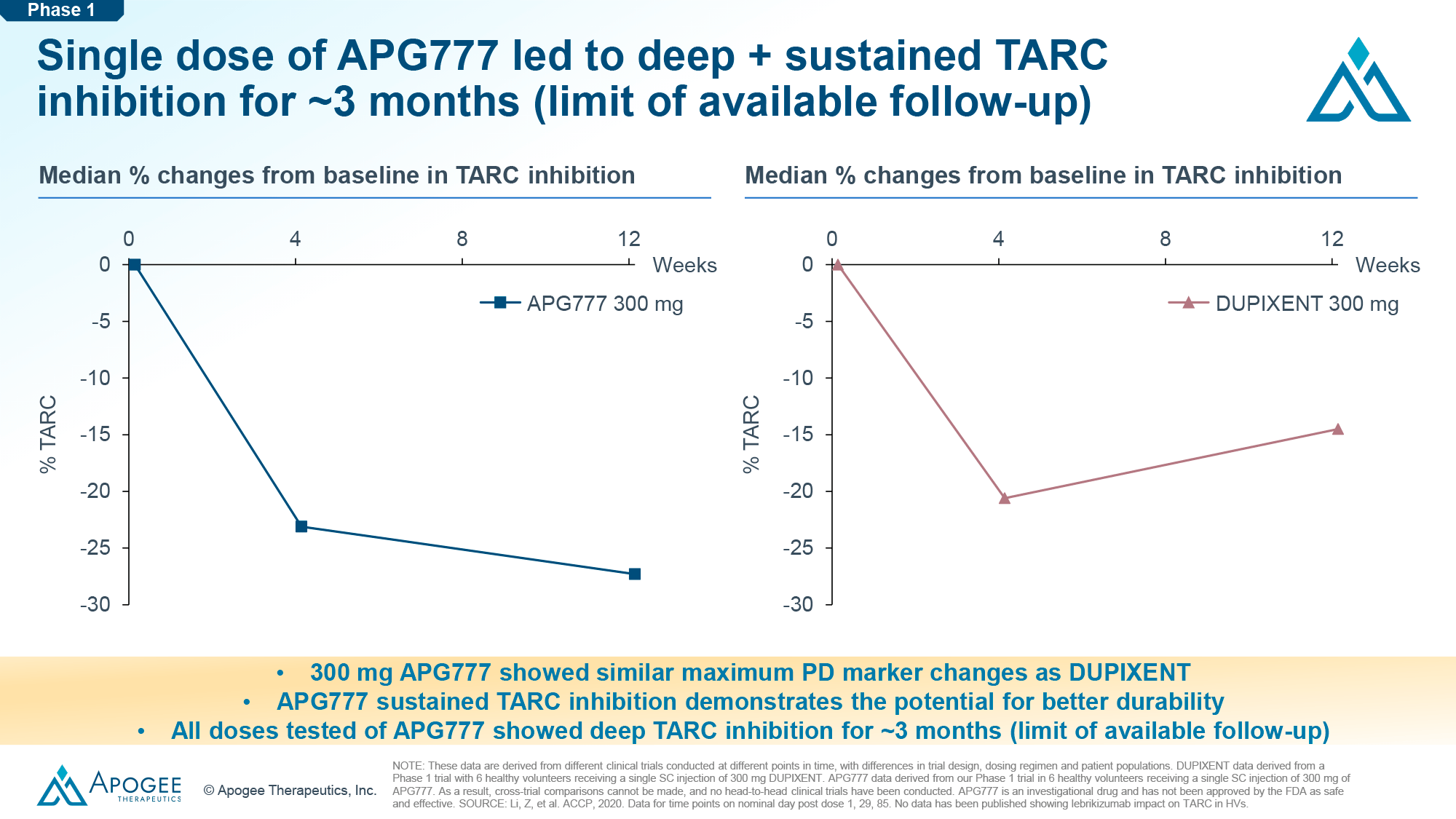
Over a period of 3 months following a single subcutaneous dose of APG777, almost 100% inhibition of phosphorylated transcription factor STAT6 (pSTAT6) and profound and sustained inhibition of C-C motif chemokine ligand 17 (CCL17, TARC), biomarkers respectively of interleukin 13 (IL-13) uptake as a target and severity of the course of atopic dermatitis (eczema), were observed.
A phase 2 clinical trial will begin in the first half of 2024 to test APG777 in the treatment of moderate-to-severe atopic dermatitis among adult patients.
In Part A of the study (n=110), the 16-week induction therapy involves subcutaneous administration of four doses of APG777 (720 mg at weeks 0 and 2, 360 mg at weeks 4 and 12), whereas in the subsequent maintenance therapy, APG777 will be administered once every 3 or 6 months (presumably 360 mg or 720 mg).
First results are expected in the second half of 2025.
In a parallel Part B (n=360), the 16-week induction therapy will test three APG777 dosing options (high, medium, and low dose) and compare efficacy with placebo.
Apogee faces two challenges. First, according to data on lebrikizumab, there is a correlation between the level of exposure to the drug and the strength of response to treatment (therapeutic efficacy) in the induction period of eczema treatment. That is, at this short initial phase of therapy it makes sense to reach a concentration of APG777 higher than that of lebrikizumab. There are all possibilities for this: 180-mg/mL formulation of APG777 allows to get a 44% higher dose than the same amount of lebrikizumab. And it is realized by four injections of APG777 instead of nine injections of lebrikizumab.
Second, since the above correlation was not observed during lebrikizumab maintenance therapy, in this long-term treatment period, APG777 exposure can be kept at a level similar to that of lebrikizumab, i.e., a very infrequent dosing regimen, where APG777 is administered once every quarter or six months: two to four APG777 injections per year instead of 13 injections of lebrikizumab or 26 injections of dupilumab.
As for the efficacy of APG777 for the treatment of atopic dermatitis, it should be no worse than that of lebrikizumab and dupilumab, which bring just over a third of patients (37%–38%) to IGA 0/1 (clear or almost clear skin) status in 16 weeks of treatment.
Apogee, depending on further success in the development of APG777, intends to take it through clinical validation in the treatment of other autoimmune diseases such as asthma (eosinophilic subtype), alopecia areata (AA), chronic rhinosinusitis with nasal polyps (CRSwNP), chronic spontaneous urticaria (CSU), eosinophilic esophagitis (EoE), and prurigo nodularis (PN).
What Else
The pipeline of Apogee Therapeutics has assembled other monoclonal antibodies with an extended half-life, which allows their use in a very rare mode.
Thus, APG808 blocks interleukin 4 (IL-4) and interleukin 13 (IL-13) signaling by binding the interleukin 4 receptor alpha subunit (IL-4Rα) common to them, similar to the mechanism of action of Dupixent (dupilumab). A clinical trial in patients with chronic obstructive pulmonary disease (COPD) of eosinophilic subtype is planned for 2025. In maintenance treatment, subcutaneous injections of APG808 can be given once every six or eight weeks — versus every two weeks with dupilumab.
APG990 binds to OX40L, thereby blocking its interaction with OX40, which is reflected by a rebalancing of the cellular immune response in atopic dermatitis (eczema). It is known that in this autoimmune disease there is an imbalance of the OX40–OX40L signaling axis and consequently an imbalance between pro-inflammatory and anti-inflammatory T cells involved in pathogenesis [1].
It is possible that APG990 will also establish itself in the treatment of asthma, hidradenitis suppurativa (HS), alopecia areata (AA), celiac disease (CD), and systemic sclerosis (SSc).
APG222 exerts dual inhibition of OX40L and IL-13, and such synergy should enhance the efficacy of atopic dermatitis treatment.