Highlights
The experimental drug baxdrostat has been successful in mid-stage clinical trials treating resistant or uncontrolled hypertension in which blood pressure cannot be kept normal even by adhering to appropriate antihypertensive therapy.
Baxdrostat, developed by CinCor Pharma, has been shown to reduce systolic blood pressure (SBP) and diastolic blood pressure (DBP) by an absolute 20.3 mmHg and 14.3 mmHg in patients taking three to four antihypertensive medications of different classes that do not help much.
In patients taking one or two antihypertensive drugs, baxdrostat reduced SBP by an absolute 26.8 mmHg.
Such highly effective control of blood pressure opens up a decidedly new chapter in the treatment strategy for resistant hypertension that cannot be adequately controlled by existing antihypertensives.
If further clinical validation proves successful, baxdrostat will take the position of a highly sought-after drug, quite relevant in the absence of any new breakthrough medications for the treatment of hypertension for many years.
BrigHTN
The BrigHTN (NCT04519658) phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial invited adult patients (n=248) with resistant hypertension, adherent to a stable regimen of at least three antihypertensive drugs (including diuretic) and with blood pressure above 130/80 mmHg.
Main patient characteristics: mean age 62 years, 56% male, mean body mass index (BMI) 32.6 kg/m2, mean SBP 148 mmHg.
Participants were given placebo or baxdrostat daily in three different doses (0.5 mg, 1.0 mg, or 2.0 mg) — for 12 weeks and with the existing treatment regimen.
The efficacy endpoints of resistant hypertension treatment were established by changes in SBP and DBP.
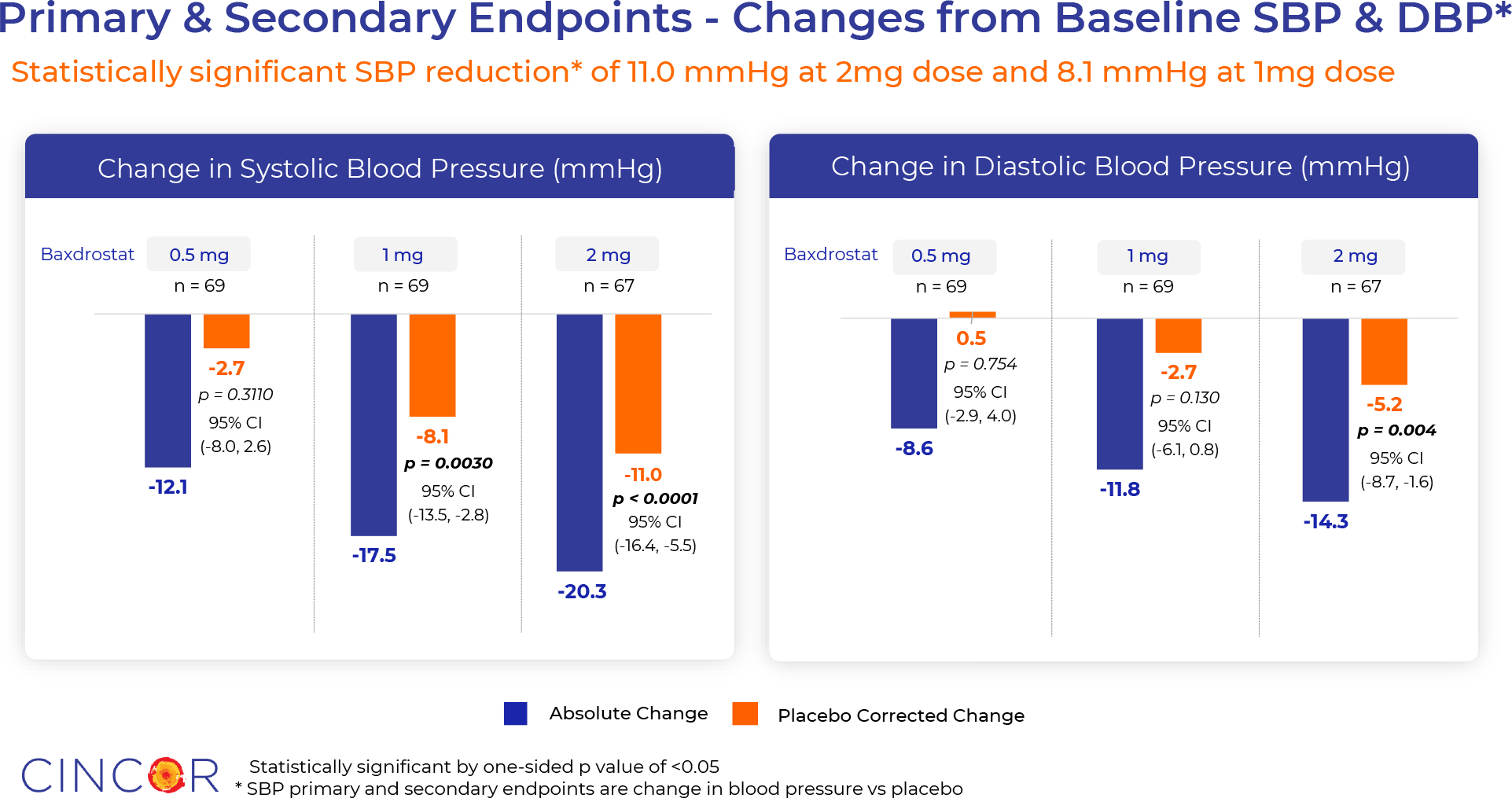
Use of baxdrostat provided mean SBP reductions of 20.3 mmHg, 17.5 mmHg, and 12.1 mmHg — respectively in the 2.0-, 1.0-, and 0.5-mg drug subgroups. In the placebo group, the decrease was 9.4 mmHg (p=0.311, p=0.003, and p<0.0001).
Baxdrostat reduced DBP by 14.3 mmHg, 11.8 mmHg, and 8.6 mmHg — versus a decrease of 9.2 mmHg in the control group (p=0.754, p=0.130, and p=0.004).
Thus, administration of baxdrostat at a dose of 2.0 mg resulted in a decrease in SBP and DBP of 11.0 mmHg and 5.2 mmHg relative to placebo. At the same time, 46% of patients reached their target SBP of less than 130 mmHg.
Baxdrostat was characterized by acceptable tolerability. The frequency of adverse events (AEs) was dose-dependent: while in the 1.0- and 2.0-mg subgroups 52% and 48% of subjects experienced AEs, in the 0.5-mg subgroup 35% experienced AEs. The majority of AEs (62%) were mild, and 89% were unrelated to the administration of baxdrostat or placebo. The most common AEs included urinary tract infections, hyperkalemia, headache, and fatigue. No cases of adrenocortical insufficiency have been reported.
HALO
The HALO (NCT05137002) phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled adult patients (n=227) with uncontrolled hypertension for which blood pressure cannot be adequately reduced by one or two antihypertensive medications.
Main patient characteristics: mean age 60 years, 53% male, mean body mass index (BMI) 32.2 kg/m2, mean SBP 147 mmHg.
Subjects received placebo or baxdrostat daily in three different doses (0.5 mg, 1.0 mg, or 2.0 mg) — for 8 weeks and with the existing treatment regimen.
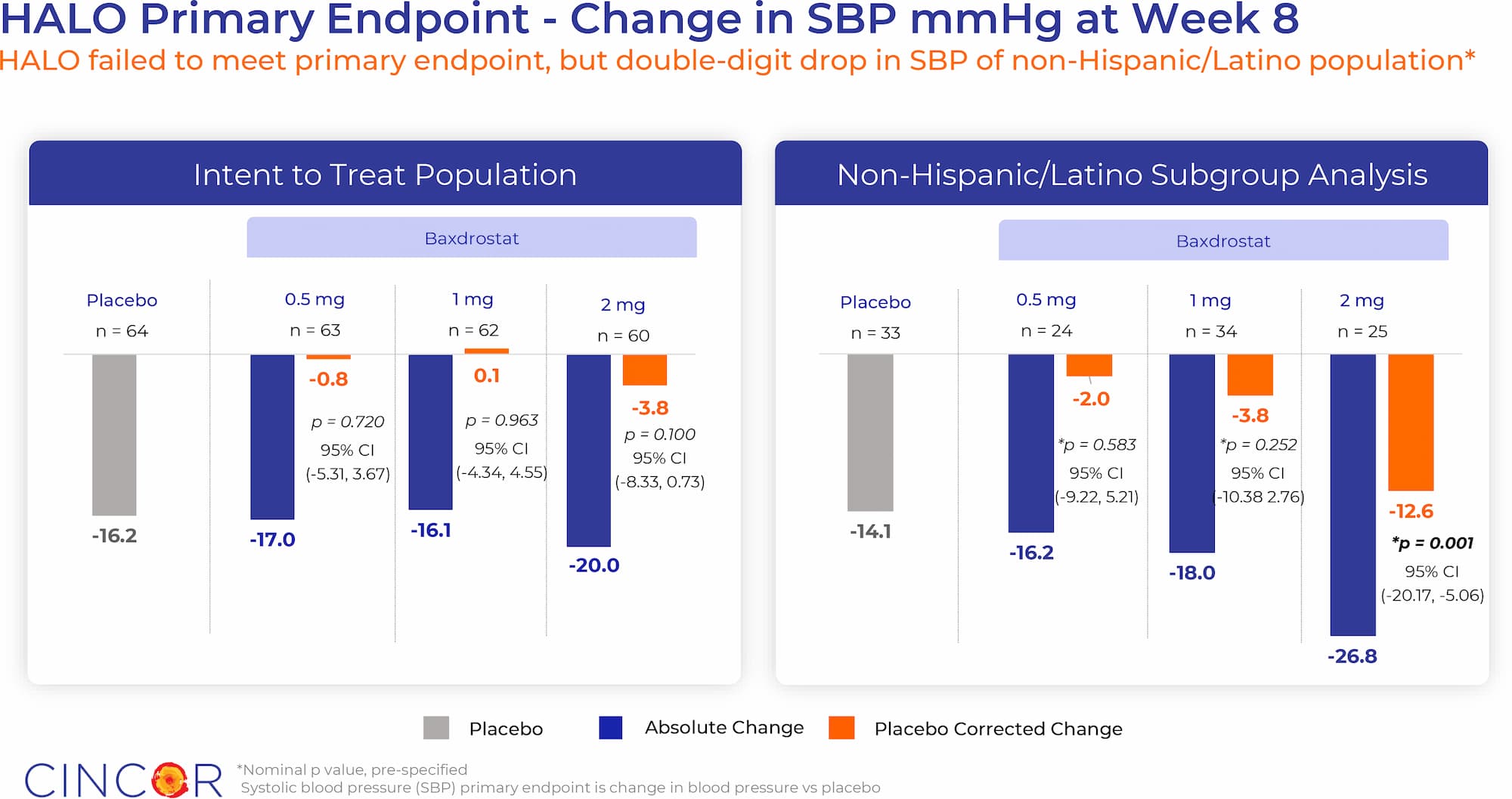
Baxdrostat failed to reach the primary endpoint, set by a statistically significant difference with the placebo group in terms of reduction of SBP. It decreased by 17.0 mmHg, 16.1 mmHg, and 20.0 mmHg — versus changes of −0.8 mmHg, +0.1 mmHg, and −3.8 mmHg in the placebo subgroups (p=0.720, p=0.963, and p=0.100).
However, when data from Hispanic/Latino patients were excluded from the analysis, the baxdrostat all worked out. SBP decreased by 16.2 mmHg, 18.0 mmHg, and 26.8 mmHg — vs. decreases of 2.0 mmHg, 3.8 mmHg, and 12.6 mmHg in the placebo subgroups (p=0.583, p=0.252, and p=0.001).
Thus, daily administration of 2-mg baxdrostat provided an absolute 26.8 mmHg and and a relative 12.6 mmHg reduction in SBP.
According to pharmacokinetic measures, Hispanic/Latino subjects were characterized by insufficient treatment adherence, which skewed the therapeutic efficacy of baxdrostat. In addition, the renin response in this patient population differed significantly from that in non-Hispanic/Latino. Again, according to CinCor, non-Hispanic/Latino patients account for 81%–89% of hypertensive patients in the United States.
With this in mind, baxdrostat was successfully clinically validated.
Baxdrostat was characterized by acceptable tolerability. No serious adverse events (AEs) were observed, none of the patients discontinued treatment due to AEs. Three cases of moderate hyperkalemia were reported.
Baxdrostat: Mechanism of Action
Baxdrostat (CIN-107, RO6836191) is an oral small-molecule inhibitor of aldosterone synthase, the enzyme responsible for aldosterone synthesis and encoded by the CYP11B2 gene [1] [2].
Baxdrostat is highly selective to aldosterone synthase and has a low affinity for steroid 11β-hydroxylase (“cortisol synthase”), the enzyme responsible for cortisol synthesis and encoded by the CYP11B1 gene. The corresponding selectivity ratio of baxdrostat is 100:1. This selectivity is remarkable: During the development of the molecule, it was taken into account that it should not affect cortisol synthesis, although aldosterone synthase and 11ß-hydroxylase are 93% homologous.
The originator of baxdrostat is Roche, which licensed the molecule to CinCor in mid-May 2019.
Suppression of the renin–angiotensin–aldosterone system (RAAS) is the leading therapeutic strategy for treating chronic heart and kidney diseases. Existing first-line drugs for treating hypertension include diuretics, angiotensin-converting enzyme (ACE) inhibitors, and/or angiotensin receptor blockers (ARBs) [3].
Despite appropriate treatment, some patients with hypertension have elevated plasma aldosterone levels, causing a loss of therapeutic efficacy, forcing the addition of the mineralocorticoid receptor antagonist spironolactone or eplerenone [4].
Chronically elevated aldosterone levels are reflected by hypokalemia, sodium reabsorption, and fluid retention, which is manifested by an increase in blood pressure.
Regardless of blood pressure, elevated aldosterone levels lead to inflammation, target organ damage, fibrosis, cardiovascular events (ventricular hypertrophy) and adverse renal events (increased urinary albumin excretion, progression of renal failure) [5].
The association between high plasma aldosterone levels and decreased long-term survival has been demonstrated in patients with congestive heart failure, acute myocardial infarction, and coronary heart disease (CHD) [6] [7] [8] [9] [10] [11].
Thus, inhibition of aldosterone synthase, an enzyme that limits the rate of aldosterone synthesis, is a promising therapeutic approach to control blood pressure and inhibit target organ damage [12].
Baxdrostat: What’s Next
In the first half of 2023, CinCor will launch two phase 3 clinical trials designed to definitively confirm the efficacy and safety of baxdrostat in the treatment of resistant and uncontrolled hypertension.
The 26-week FigHtn-CKD (NCT05432167) phase 2 clinical trial investigating baxdrostat in the treatment of patients with uncontrolled hypertension and chronic kidney disease is ongoing. Results are expected in the second half of 2023.
The 12-week Spark-PA (NCT04605549) phase 2 clinical trial, which is testing baxdrostat for lowering blood pressure in patients with primary aldosteronism, is underway. The results will be summarized in the second half of 2023.
Expert Comments
Two phase 2 clinical trials have confidently confirmed the high therapeutic efficacy of baxdrostat in the treatment of resistant and uncontrolled hypertension. The decrease in blood pressure was associated with a decrease in plasma aldosterone levels and a compensatory increase in plasma renin activity, while there was no decrease in cortisol levels. Overall, baxdrostat had an acceptable safety profile, and none of the patients discontinued the study because of hyperkalemia.
- It should be understood that a decrease in systolic blood pressure, even by a seemingly insignificant 5 mmHg, results in a 10% reduction in the relative risk of major adverse cardiovascular events (MACE). The risks of stroke, heart failure, ischaemic heart disease, and cardiovascular death are reduced by 13%, 13%, 8%, and 5% [1].
- Baxdrostat reduced systolic blood pressure by an absolute 20.3/26.8 mmHg and relative to placebo by 11.0/12.6 mmHg.
It is widely believed that a large number of cases of resistant hypertension is associated with a lack of compliance (treatment adherence). However, there is growing evidence that this view is not valid: In compliant patients, resistant hypertension is believed to be a special subtype of hypertension that responds poorly to standard medications due to its pathogenesis [2] [3].
Thus, the results of the PATHWAY-2 (NCT02369081) clinical trial, combined with the findings from three mechanistic sub-tests, support the hypothesis that resistant hypertension is related to autonomous aldosterone production. This well explains the fact that spironolactone, a mineralocorticoid receptor antagonist, provides greater efficacy in the task of lowering blood pressure compared with a number of other antihypertensives [4] [5].
Spironolactone in terms of safety cannot be called successful. Its extrargetary blockade of numerous steroid hormone receptors leads to adverse events, such as gynecomastia in men and menstrual irregularities and postmenopausal bleeding in women. In addition, the risk of hyperkalemia with spironolactone is mirrored by its reduced use [6].
An alternative strategy of blockade of mineralocorticoid receptors is implemented by reducing aldosterone levels through aldosterone synthase inhibition. However, the development of such a drug is complicated by the 93% similarity between the CYP11B2 and CYP11B1 gene transcripts encoding aldosterone synthase and 11β-hydroxylase.
Osilodrostat (LCI-699), the first aldosterone synthase inhibitor to enter clinical development for the treatment of hypertension, resulted in extrargeted inhibition of cortisol synthesis. Eventually, Novartis and Italy’s Recordati repurposed it to treat Cushing’s syndrome (Cushing’s disease), a severe neuroendocrine condition characterized by increased secretion of the adrenocorticotropic hormone, which stimulates cortisol synthesis [7].
Isturisa (osilodrostat) received regulatory approvals from the European Medicines Agency (EMA) and the U.S. Food and Drug Administration (FDA) in January and March 2020.
Because of its selective mechanism of action, baxdrostat avoids the risks of adrenal insufficiency and loss of blood pressure lowering efficacy that can result from the accumulation of steroid precursors that activate mineralocorticoid receptors that is seen with first-generation aldosterone synthase inhibitors [7] [8].
Mild hyperkalemia is common in patients taking renin–angiotensin–aldosterone system inhibitors. In a clinical trial of baxdrostat, recurrent hyperkalemia was observed in very few patients, and such cases of elevated potassium levels quickly resolved without changes in drug dose or specific interventions beyond the usual dietary recommendations.
Nevertheless, an 8- and 12-week study of baxdrostat is too short a period to draw definitive conclusions about the efficacy and safety of this drug.
Extras
CinCor Pharma. HALO program update. November 28, 2022. [PDF]
CinCor Pharma. BrigHtn program update. August 8, 2022. [PDF]