Kesimpta (ofatumumab) is a new drug indicated for the treatment of adult patients with relapsing-remitting forms of multiple sclerosis including clinically isolated syndrome (CIS), relapsing-remitting multiple sclerosis (RRMS), and secondary progressive multiple sclerosis (SPMS) in its active form.
Kesimpta, offered by Novartis, is approved by the U.S. Food and Drug Administration (FDA) in August 2020.
Marketing approval from the European Medicines Agency (EMA) was granted in March 2021: Kesimpta is indicated for therapy of adult patients with relapsing-remitting forms of multiple sclerosis with the active disease according to clinical course and MRI imaging.
Kesimpta is a disease-modifying therapy (DMT) of multiple sclerosis and a direct competitor to Ocrevus (ocrelizumab), the best-selling drug from Roche. The main difference between ofatumumab and ocrelizumab is the route and regimen of administration. Whereas Ocrevus is administered in the inpatient setting by intravenous infusions (every 6 months — after 2 loading doses with 2 weeks in between), Kesimpta is administered at home by the patient themself by subcutaneous injections (every 4 weeks — after 3 loading doses with 1 week in between). In addition, infusions of Ocrevus require some premedication including a corticosteroid, antihistamine, and antipyretic.

Kesimpta for Multiple Sclerosis: Ofatumumab’s Mechanism of Action
There is ample unequivocal evidence for the essential contribution of B cells both in the regulation of normal autoimmunity and in the pathogenesis of immune-mediated diseases including multiple sclerosis. In the case of the latter, the profile of B cells is biased toward a pro-inflammatory phenotype, while they contribute to the progression of multiple sclerosis through a number of mechanisms such as antibody production, antigen presentation, T cell stimulation and activation, driving autoproliferation of brain-homing autoreactive CD4+ T cells, production of pro-inflammatory cytokines, and formation of ectopic meningeal germinal centers that drive cortical pathology and contribute to neurological disability.
Ofatumumab is a fully human monoclonal antibody against the surface antigen CD20 that is expressed on B cells at all stages of their development (except the first and last), with the level of expression gradually increasing as the B cells mature. Ofatumumab binds to CD20, thereby activating the immune system that performs B cell lysis through complement-dependent cytotoxicity (CDC), antibody-dependent cell-mediated cytotoxicity (ADCC), and phagocytosis. The resulting depletion of the B-cell pool has an appropriate therapeutic effect in multiple sclerosis.
It should be understood that ofatumumab is not a new drug at all: the Swiss pharma giant commercialized Arzerra (ofatumumab) back in October 2009 when it received FDA approval for its use in the therapy of chronic lymphocytic leukemia (CLL). In January 2018, Novartis withdrew Arzerra from sale in all countries except the U.S. deeming demand insufficient due to intense pressure from other much more effective CLL-drugs.
A certain parallel between ofatumumab and ocrelizumab is obvious: Roche’s drug is a modified version of Rituxan/MabThera (rituximab), which is allowed in the treatment of CLL, non-Hodgkin lymphoma, and several autoimmune pathologies, and which before the debut of Ocrevus was widely used off-label in multiple sclerosis.
Novartis acquired the rights to ofatumumab for cancer in a complex asset swap with GlaxoSmithKline in 2014. The former bought the oncology business from the latter for $16 billion and sold it a portfolio of vaccines (except flu vaccines) for $7.1 billion; the companies’ over-the-counter medicines were combined.
Later, the Basel-based pharma giant bought the rights to all other potential indications for the applicability of ofatumumab, for $1.034 billion plus a 12% royalty on sales of the drug in autoimmune disease therapy. Novartis will also give a 10% royalty to Genmab (Denmark), the originator of ofatumumab.
Kesimpta for Multiple Sclerosis Therapy: Clinical Efficacy of Ofatumumab
The efficacy of ofatumumab in the treatment of relapsing-remitting forms of multiple sclerosis has been studied in two identical phase 3 (randomized, double-blind, active-control, multicenter, international) clinical trials ASCLEPIOS I (NCT02792218) and ASCLEPIOS II (NCT02792231) among adult (18-55 years old) patients (n=1881) with relapsing-remitting multiple sclerosis or active secondary progressive multiple sclerosis.
The main eligibility requirements included either at least one relapse in the previous year, or at least two relapses in the past couple of years, or presence of brain inflammation lesions on gadolinium-enhanced T1-weighted MRI images in the previous year; a score on the Expanded Disability Status Scale (EDSS) between 0–5.5.
Comparison was made with oral Aubagio (teriflunomide), DMT by Sanofi. The maximum duration of the trials was 30 months.
In both studies, ofatumumab groups reached the primary endpoint demonstrating a statistically and clinically significant reduction in annualized relapse rate (ARR) to 0.11 and 0.10 — versus 0.22 and 0.25 in the teriflunomide groups. The relative reductions in ARR were 50.5% (hazard ratio [HR] 0.495 [95% CI: 0.374–0.654]; p<0.001) and 58.8% (HR 0.415 [95% CI: 0.308–0.559]; p<0.001).

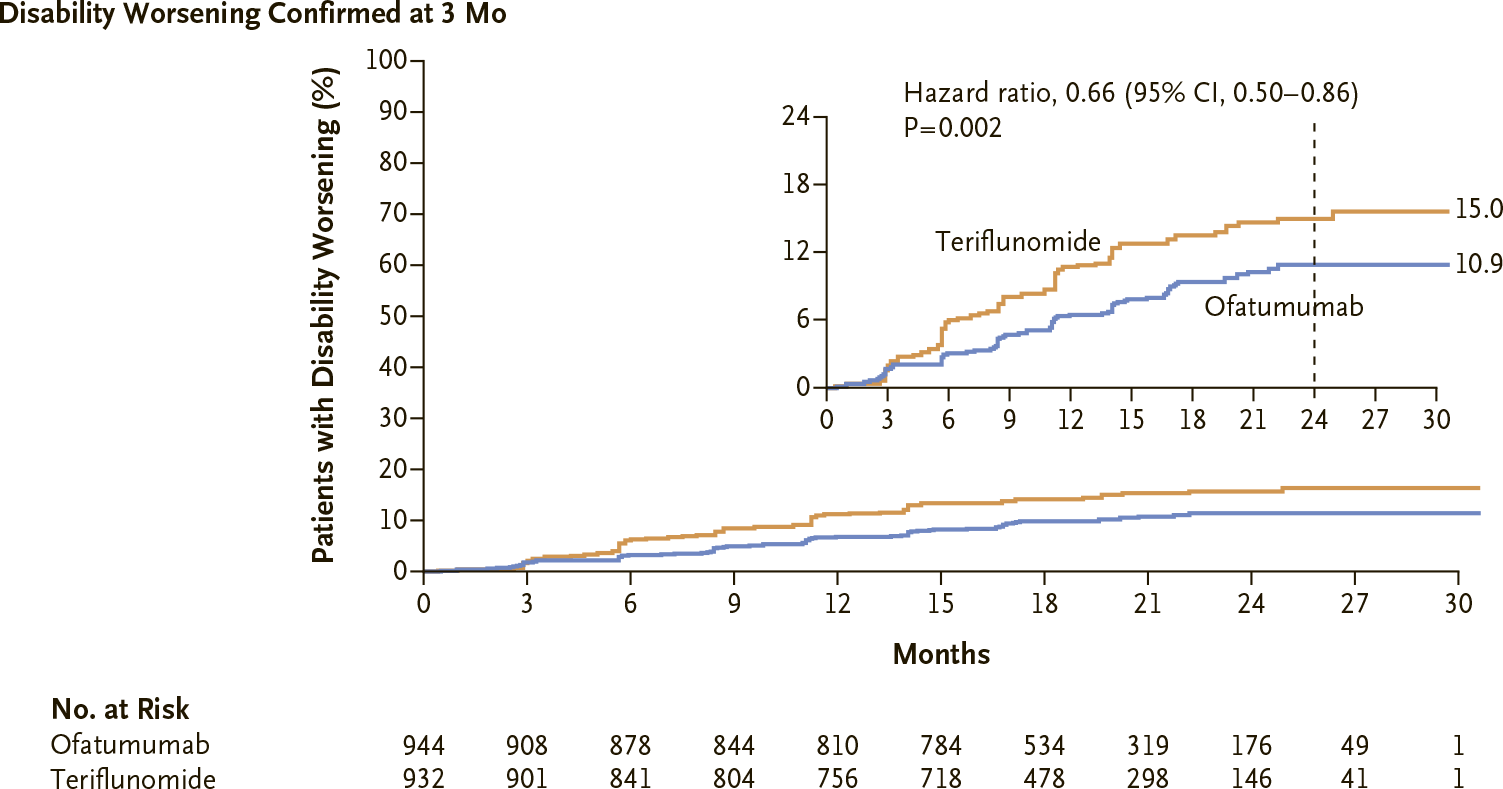
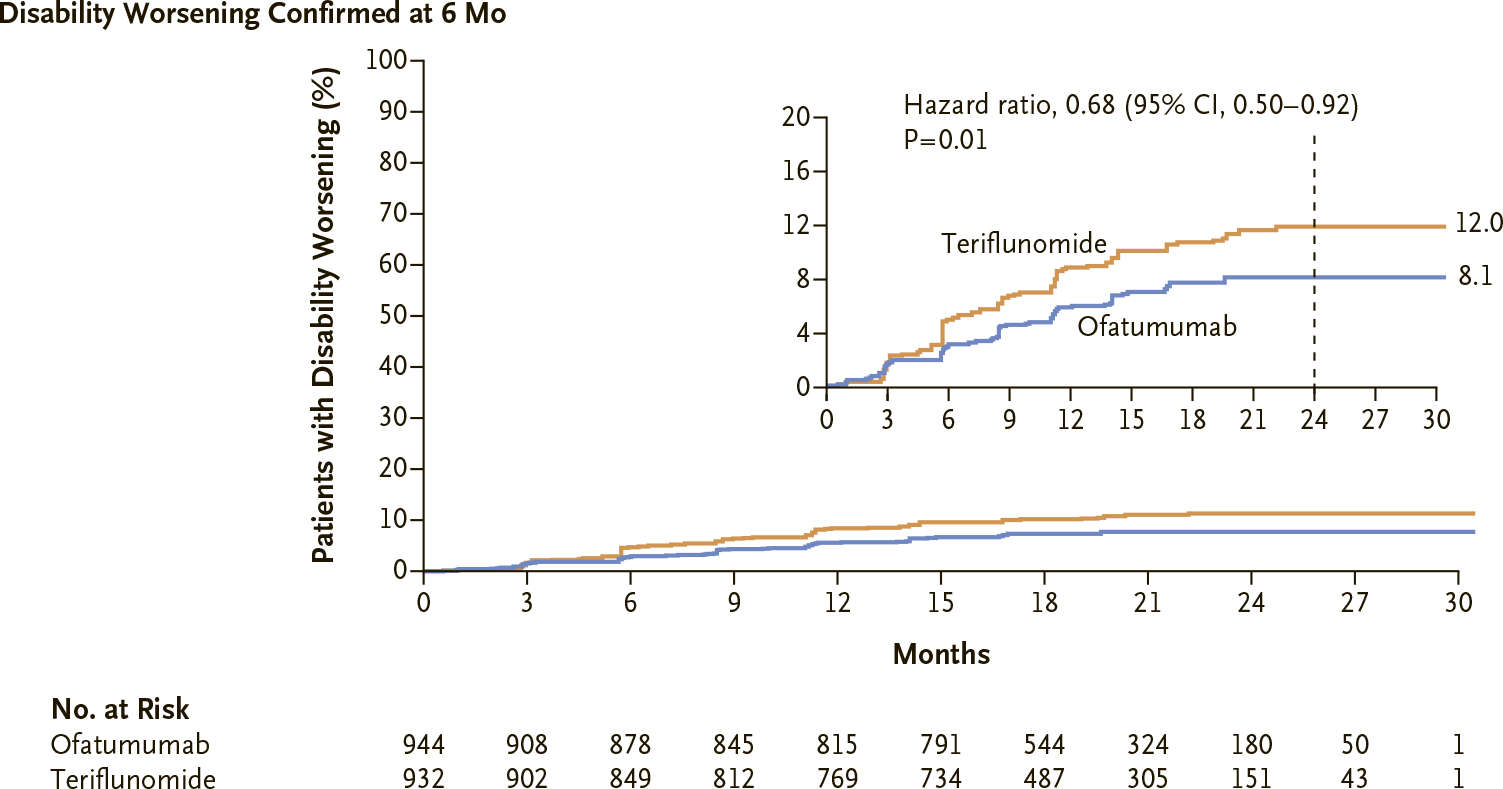
Ofatumumab provided a relative reduction in the risk of confirmed disability progression (CDP) defined as an increase in EDSS score of ≥1.5, ≥1, or ≥0.5 points (among those subjects whose baseline EDSS score was 0, 1–5, or ≥5.5 points, respectively) that persisted through 3 and 6 months of treatment: 34.4% (HR 0.656 [95% CI: 0.499–0.862]; p=0.002) and 32.5% (HR 0.675 [95% CI: 0.498–0.916]; p=0.012).
Kesimpta groups showed a 35.2% increased chance of confirmed disability improvement (CDI) in this case stated by a reduced EDSS score maintained over 6 months of treatment. This status was achieved by 11.0% of patients — vs. 8.1% in Aubagio groups. However, the difference could not be called statistically significant (HR 1.352 [95% CI: 0.950–1.924]; p=0.094).

There was 97.5% and 93.8% elimination of brain lesions on gadolinium-enhanced T1-weighted MRI images (they reflect the presence of an active inflammatory process) — relative to teriflunomide (p<0.001).

Ofatumumab reduced by a relative 82.0% and 84.5% (p<0.001) the number of new or increasing brain lesions on T2-weighted MRI images (these are indicative of demyelination).

Kesimpta for Multiple Sclerosis Therapy: Safety of Ofatumumab
The most common adverse events for the administration of ofatumumab compared to teriflunomide are upper respiratory tract infections (39% versus 38%), systemic reactions after injection (21% vs. 13%), headache (13% vs. 12%), local reactions after injection (11% vs. 6%), urinary tract infections (10% vs. 8%), back pain (8% vs. 6%), and reduced blood immunoglobulin M (6% vs. 2%).
The prescribing information for Kesimpta gives an indication that two serious events should be monitored: reactivation of viral hepatitis B and the development of progressive multifocal leukoencephalopathy (PML) as an opportunistic infection of the brain caused by JC virus. No, there were no reported cases of such adverse events during clinical trials of Kesimpta. However, patients have experienced them while using ofatumumab to treat chronic lymphocytic leukemia (at higher doses than multiple sclerosis therapy but with a short course); they have also been reported among patients receiving other monoclonal antibodies against CD20.
Thus, as of the end of December 2020, there were 10 cases of PML among patients with multiple sclerosis treated with Ocrevus. At the same time, 8 of these cases were in patients with antibodies against the JC virus who had previously received Tysabri (natalizumab), one in a person who had previously received Gilenya (fingolimod), and another in a patient who had not previously received any DMTs although the age status (78 years) and low absolute lymphocyte count before therapy contribute to the bias in the direct association with ocrelizumab.

Kesimpta in Multiple Sclerosis Treatment: What’s Next for Ofatumumab
Novartis continues to conduct numerous clinical trials examining the applicability ofatumumab in the therapy of relapsing forms of multiple sclerosis:
- ALITHIOS (NCT03650114) phase 3 (non-randomized, open-label, multicenter, international). Study ofatumumab’s safety and efficacy in the long-term treatment period (up to 5 years). In parallel, it evaluates the effects ofatumumab on antibody response after administering vaccines such as tetanus toxoid containing vaccine, 13-valent pneumococcal conjugate vaccine, 23-valent pneumococcal polysaccharide vaccine, or seasonal quadrivalent influenza vaccine, as well as neoantigen keyhole limpet hemocyanin (KLH) administration. Such testing is necessary because, in the VELOCE (NCT02545868) phase 3 clinical trial, Roche found that in patients with multiple sclerosis on ocrelizumab therapy, the humoral immune response to non-live vaccines is attenuated although it can still be expected to show its protective properties.
- STHENOS (NCT04788615) phase 3 (randomized, rater-blind, active-control, multicenter). This study will compare ofatumumab versus platform first-line self-administered DMTs — Copaxone (glatiramer acetate), Tecfidera (dimethyl fumarate), Aubagio (teriflunomide), or interferon — in treatment naïve patients with multiple sclerosis.
- ARTIOS (NCT04353492) phase 3 (non-randomized, open-label, multicenter). Evaluation of the efficacy of ofatumumab among patients with multiple sclerosis who are on therapy with oral DMTs, Gilenya (fingolimod) or Tecfidera (dimethyl fumarate), but have chosen to withdraw from them due to breakthrough disease as evidence by clinical relapses or images.
- OLIKOS (NCT04486716) phase 3 (non-randomized, open-label, multicenter). Evaluation of therapy in patients who previously received anti-CD20 therapy with intravenous ocrelizumab or rituximab and then switched to treatment with subcutaneous ofatumumab.
- KYRIOS (NCT04869358) phase 4 (non-randomized, open-label). An immune response study among patients who have received the COVID-19 mRNA vaccine and who have not yet started or are already following therapy for multiple sclerosis with ofatumumab. Two other trials, NCT04878211 and NCT04847596, are being organized in parallel to sort out the immune response in SARS-CoV-2 vaccination.
- NCT04667117 phase 4 (non-randomized, open-label, multicenter). It is necessary to find out whether patients who are about to or are already on therapy for multiple sclerosis with ofatumumab have an adequate immune humoral response to the inactivated quadrivalent influenza vaccine.
- TIMIOS (NCT04676555). This is an observational cross-sectional study of Ocrevus or Kesimpta administrations. The goal is to clarify the economic picture of the costs of these drugs. To do this, the direct costs incurred by the U.S., U.K., and Australian health care systems will be identified in terms of the time required to prepare and administer the drugs, followed by patient follow-up, and the resources needed to manage adverse events. Indirect costs related to patient impairment will be established.
Kesimpta for Multiple Sclerosis: Market Landscape
Kesimpta, as stated at the beginning, has taken a direct competition position with Ocrevus, which was the first among the anti-CD20 drugs to enter the multiple sclerosis market. Ocrevus, approved by the FDA in late March 2017, quickly became a blockbuster earning CHF 869 million, CHF 2.35 billion, CHF 3.71 billion, and CHF 4.33 billion between 2017 and 2020. (The Swiss franc exchange rate is stable fluctuating between 0.9 and 1.0 per dollar.)
The highest demand for ocrelizumab is understandable because Ocrevus is decisively superior to conventional platform interferon therapy, has a beneficial effect on cognitive function, reduces brain tissue damage, holds down the activity and progression of multiple sclerosis, and is generally suitable for most patients. There is still no reliable evidence, however, that ocrelizumab works effectively in the therapy of primary progressive multiple sclerosis.
Industry experts predict that Kesimpta will achieve best-seller status as early as 2022, crossing the $1 billion mark in annual sales.
Novartis is betting on an injectable subcutaneous formulation of ofatumumab (OMB157): patients themselves inject the drug offered in the form of a convenient auto-injector. This will have to be done once a month whereas therapy with Ocrevus involves its intravenous infusion once every six months.
In addition to not requiring a visit to a medical facility and mandatory premedication in the case of Ocrevus (which, by the way, can be optimally modified), the subcutaneous formulation of the anti-CD20 drug Kesimpta has one important advantage. A reduced dose of ofatumumab allows multiple sclerosis therapy to be paused: for example, when an infection needs to be treated — the B-cell population will recover approximately twice as quickly as with ocrelizumab.
Multiple Sclerosis Treatment: Kesimpta vs. Ocrevus
It would not be methodologically correct to directly compare the efficacy of Kesimpta to that of Ocrevus because, of course, different patients participated in the clinical trials. Although however, given the large sample of patients enrolled in these trials, a comparison can still be made.
Thus, ocrelizumab tested in two identical phase 3 (randomized, double-blind, multicenter, international) OPERA I (NCT01247324) and OPERA II (NCT01247324) clinical trials among adult patients (n=1656) with relapsing forms of multiple sclerosis and compared to Rebif (interferon beta-1a) from Merck KGaA, reduced the annualized relapse rate (ARR) to 0.156 and 0.155 — a relative reduction in ARR of 46% and 47% (p<0.0001).
In other words, the efficacy of Kesimpta’s therapy for multiple sclerosis is in no way inferior to Ocrevus.
Meanwhile, ublituximab, which is backed by TG Therapeutics, is pulling up. This anti-CD20 monoclonal antibody, which has completed a pair of phase 3 pivotal clinical trials comparing it to teriflunomide, successfully passed them achieving an ARR of less than 0.10.
Ublituximab, like ocrelizumab, is administered every 6 months but its intravenous infusions are faster: within 1 hour instead of 3.5 hours (or 2 hours if there were no serious adverse reactions to the Ocrevus infusion previously).
Kesimpta and COVID-19: Anti-CD20 Therapy in SARS-CoV-2 Pandemic
There is an opinion about the potential risk of COVID-19 in a more severe form on the background of anti-CD20 therapy. Thus, an Italian retrospective study of 784 people with multiple sclerosis and confirmed SARS-CoV-2 infection found an odds ratio (OR) of 2.59 (p=0.002) for COVID-19 with the severe course for those on ocrelizumab or rituximab therapy. The American COViMS Registry studied 858 anti-CD20 treated patients with multiple sclerosis and COVID-19 whose multivariate logistic regression analysis of the data resulted [LB1242] in an OR of 2.31 (p<0.002).
It is possible that monoclonal antibodies against CD20, which deplete the pool of B lymphocytes, indeed more than doubles the likelihood of death, intensive care, or hospitalization due to COVID-19 — compared to therapy with other DMTs. However, even on the basis of the above data, it is too early to draw any unequivocal conclusions especially since the analysis performed is in no way characterized by a reliable denominator.
Again, interesting is the case of a 51-year-old multiple sclerosis patient who, on treatment with ofatumumab, became infected with SARS-CoV-2 but remained asymptomatic, while she developed antiviral IgM and IgG antibodies. In other words, an effective humoral response to COVID-19 infection is quite possible even in the complete absence of CD19+ B cells in the blood.
Extras
Kesimpta (ofatumumab). Prescribing information. U.S. [PDF]
Kesimpta (ofatumumab). Prescribing information. Europe. [PDF]
Kesimpta (ofatumumab). EMA. European Public Assessment Report (EPAR). [PDF]
Ofatumumab versus teriflunomide in multiple sclerosis. N Engl J Med. 2020 Aug 6;383(6):546-557. [source]
Anti-CD20 B cell treatment for relapsing multiple sclerosis. Front Neurol. 2021 Jan 22;11:595547. [source]
Comparison of the efficacy and safety of anti-CD20 B cells depleting drugs in multiple sclerosis. Mult Scler Relat Disord. 2021 Apr;49:102787. [source]