Highlights
Wegovy (semaglutide) is a new drug indicated for long-term use to correct body weight in adult patients whose body mass index (BMI):
- is equal to or greater than 30 kg/m2 (obesity)
- is within 27–30 kg/m2 (overweight) with at least one comorbidity associated with overweight, such as hypertension, type 2 diabetes mellitus, dyslipidemia, etc.
Wegovy should be prescribed as an adjunct to a low-calorie diet and increased physical activity.
Wegovy, developed by Novo Nordisk (Novo Nordisk), is approved by the U.S. Food and Drug Administration (FDA) in early June 2021.
The price of Wegovy is expected to be comparable to that of Saxenda (liraglutide), a weight-loss drug offered by Novo Nordisk in December 2014. A one-month course of Saxenda for U.S. patients without insurance costs $1,400.

Why Do We Need Medication to Lose Weight?
In short and to the point, scientifically based overview paints the following picture.
Obesity increases the risk of developing type 2 diabetes mellitus and cardiovascular disease, the number one cause of death worldwide.
↓
Reducing body weight by 5–10% alleviates obesity-related complications by improving anthropometric parameters, cardiometabolic parameters (blood glucose levels, blood pressure, plasma triglyceride concentration), and quality of life, and by reducing the risk of cardiovascular complications.
↓
Achieving weight loss with a comprehensive program of lifestyle changes, including diet, exercise, and intensive behavioral therapy, and then maintaining the weight reduction is a challenge.
↓
Adding drugs to lifestyle changes multiplies the likelihood of achieving the desired weight loss goals.
Wegovy: Clinical Efficacy of Semaglutide in Obesity Therapy
The regulatory verdict for Wegovy for weight loss was guided by the results of several 68-week phase 3 clinical trials (randomized, double-blind, placebo-controlled, multicenter, international) in adult patients under the STEP program:
STEP 1 (NCT03548935): therapy for obesity or overweight (n=1961) with an extended study period of one additional year
STEP 2 (NCT03552757): therapy for obesity or overweight (n=1210) with a diagnosis of type 2 mellitus (glycated hemoglobin [HbA1c] in the 7–10% range)
STEP 3 (NCT03611582): therapy for obesity or overweight (n=611) with intensive behavioral therapy focused on lifestyle changes
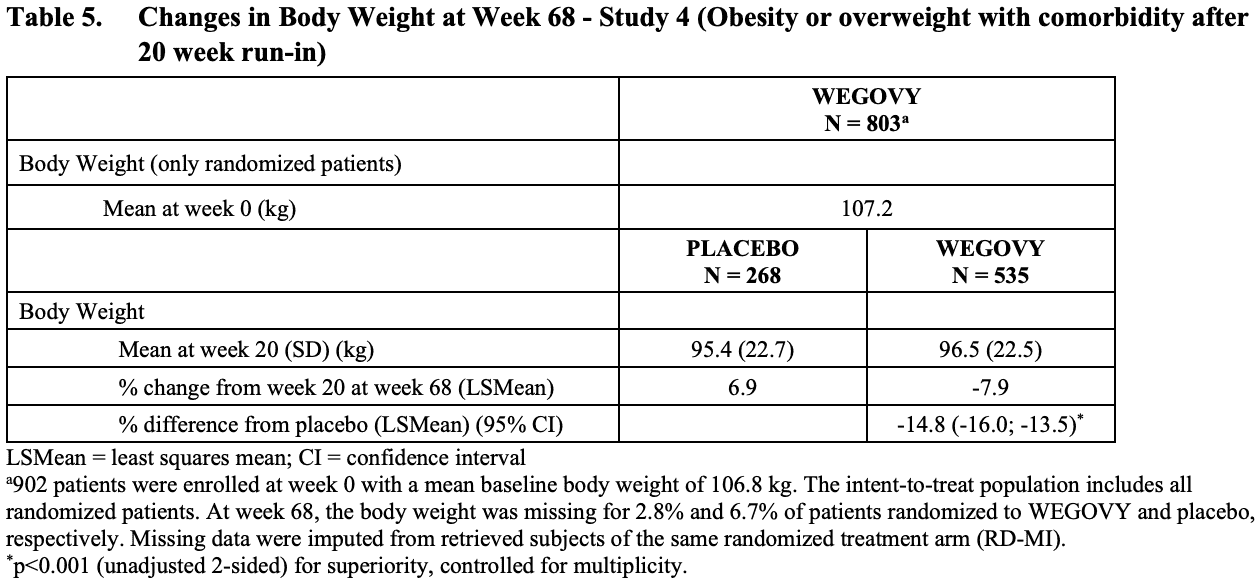
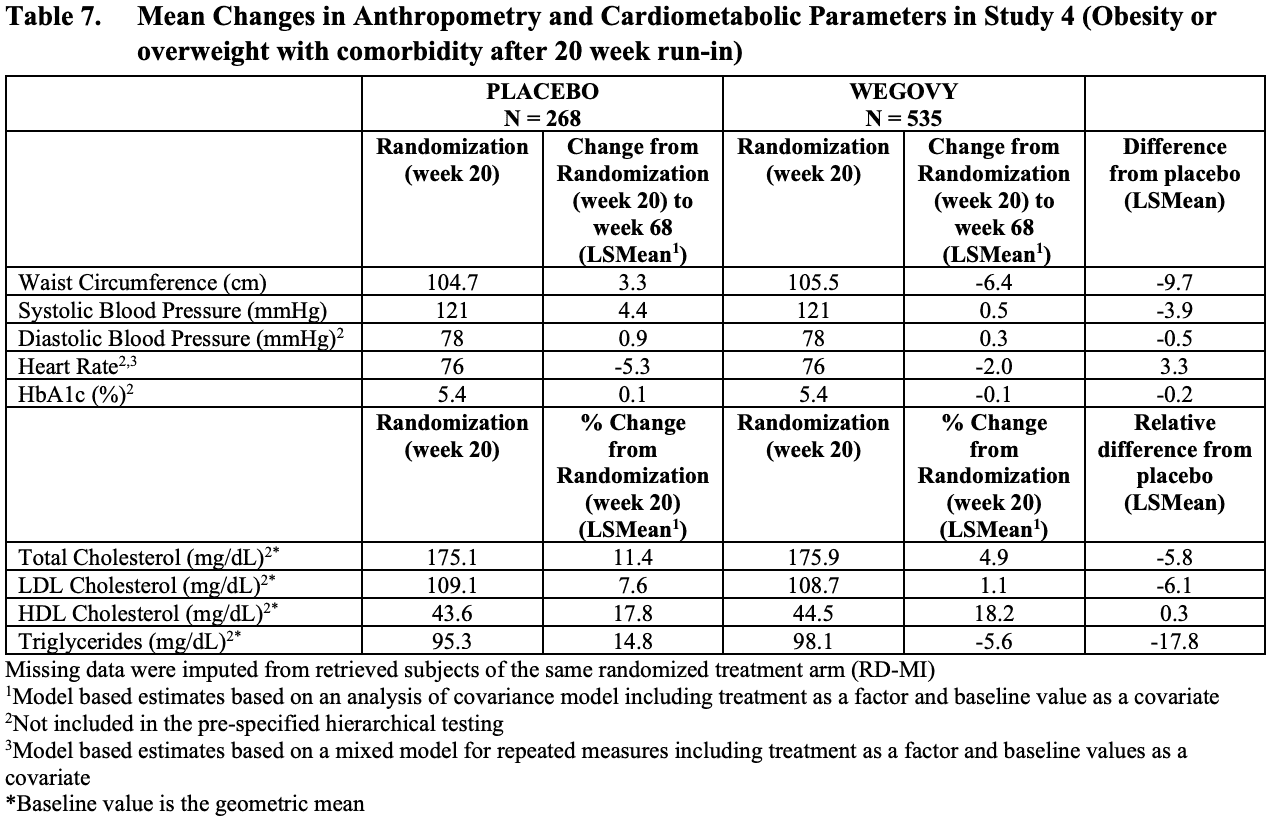
STEP 4 (NCT03548987): therapy for obesity or overweight (n=1964) among patients who reached the target weekly dose of semaglutide of 2.4 mg after a 20-week run-in period.
In STEP 1, STEP 2, and STEP 4 trials, patients were instructed to reduce caloric intake (the deficit was approximately 500 kcal/day) and increase physical activity (minimum 150 min/week). In the STEP 3 trial, participants were initially instructed to follow an 8-week low-calorie diet (total energy intake of 1000–1200 kcal/day) and then switch to a reduced-calorie diet (1200–1800 kcal/day) and increased physical activity (100 min/week with a gradual increase to 200 min/week).
Patients were given weekly injectable semaglutide (with a gradual increase in dose to avoid side effects) or placebo.
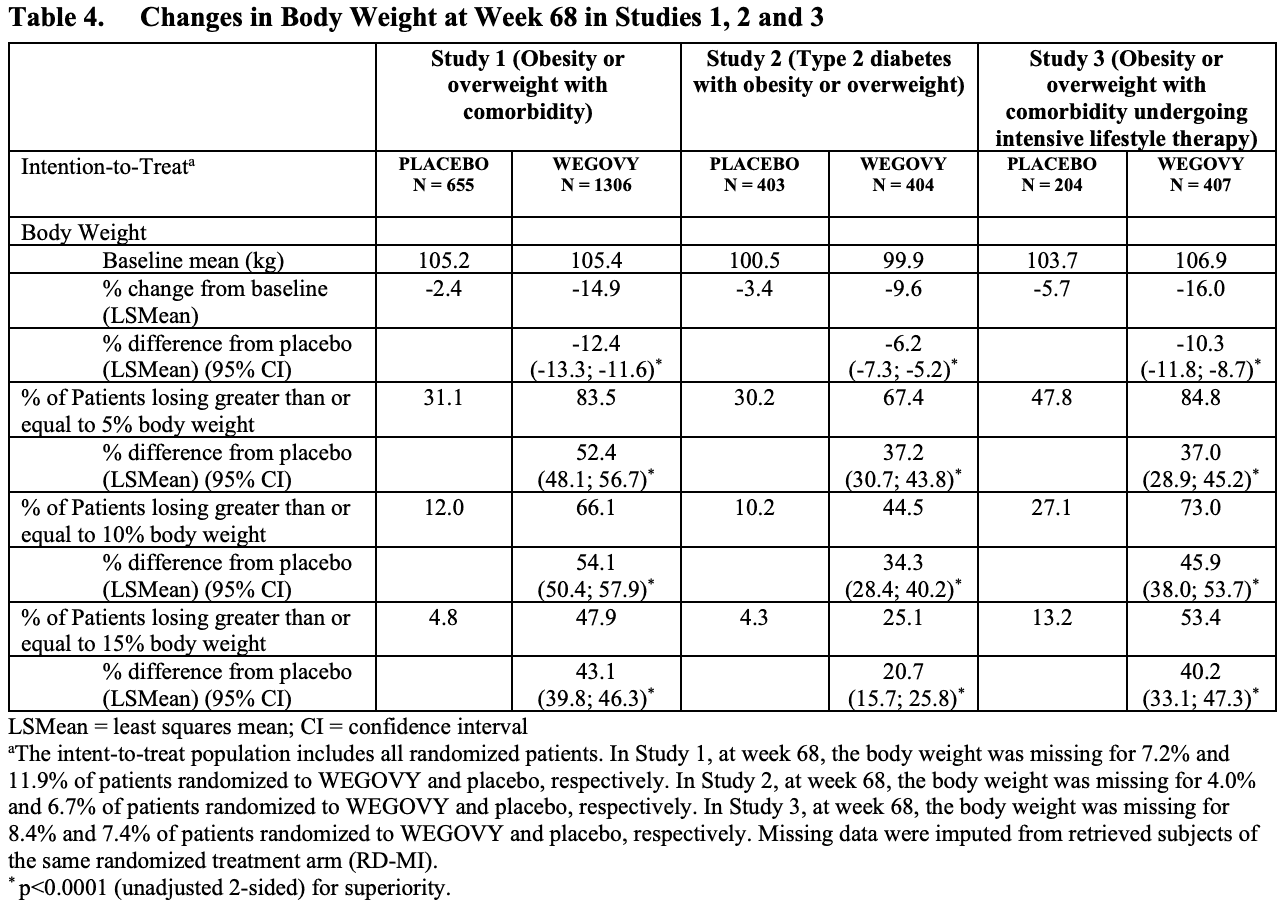
At the end of the trials, Wegovy was statistically significantly superior to placebo providing proper weight loss and deriving a decent proportion of patients to eliminate 5%, 10%, and 15% of excess body weight.
Clinical efficacy of Wegovy (semaglutide) for treating obesity
| STEP 1 | STEP 2 | STEP 3 | STEP 4 | |
|---|---|---|---|---|
| Baseline weight, kg | 105.3 | 99.8 | 105.8 | 107.2 |
| Weight loss, % (first evaluation method) | 14.9 | 9.6 | 16.0 | 17.4 |
| Weight loss, % (second evaluation method) | 16.9 | 10.6 | 17.6 | 18.2 |
| Patients who lost at least 5% of baseline weight, % | 83.5 | 67.4 | 84.8 | |
| Patients who lost at least 10% of baseline weight, % | 66.1 | 44.5 | 73.0 | |
| Patients who lost at least 15% of baseline weight, % | 47.9 | 25.1 | 53.4 |
- The first method for assessing therapeutic efficacy does not take into account treatment adherence (compliance) and does not take into account the facts of whether patients have taken other weight-loss medications. In other words, it refers to “normal” patients whose behavior is closer to reality.
- The second method for assessing therapeutic efficacy considers only patients who strictly followed the treatment protocol throughout the clinical trial and did not use additional weight-loss medications. In other words, we are talking about “ideal” patients.
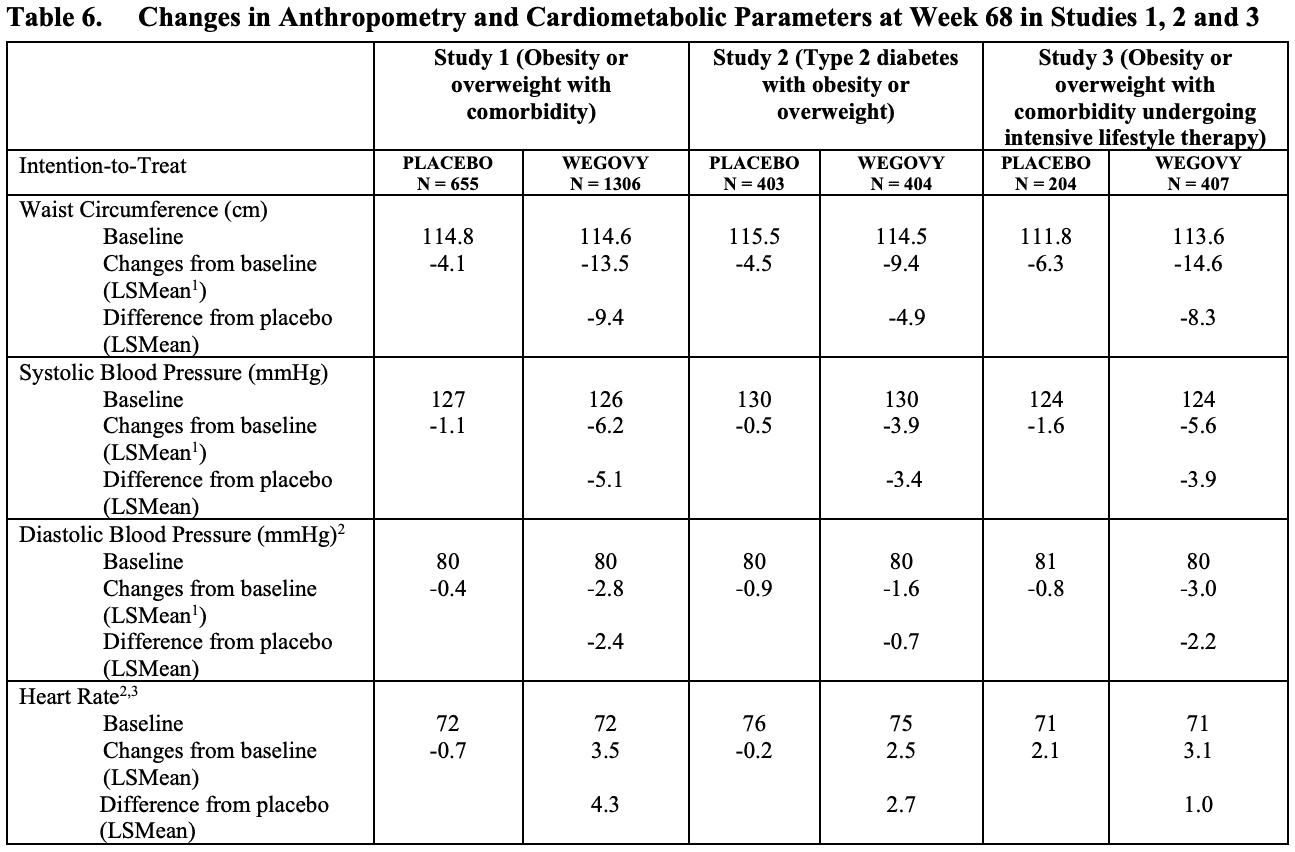
The loss of extra pounds was observed in all subjects regardless of age, sex, race, ethnicity, baseline BMI and weight, and degree of kidney function impairment.
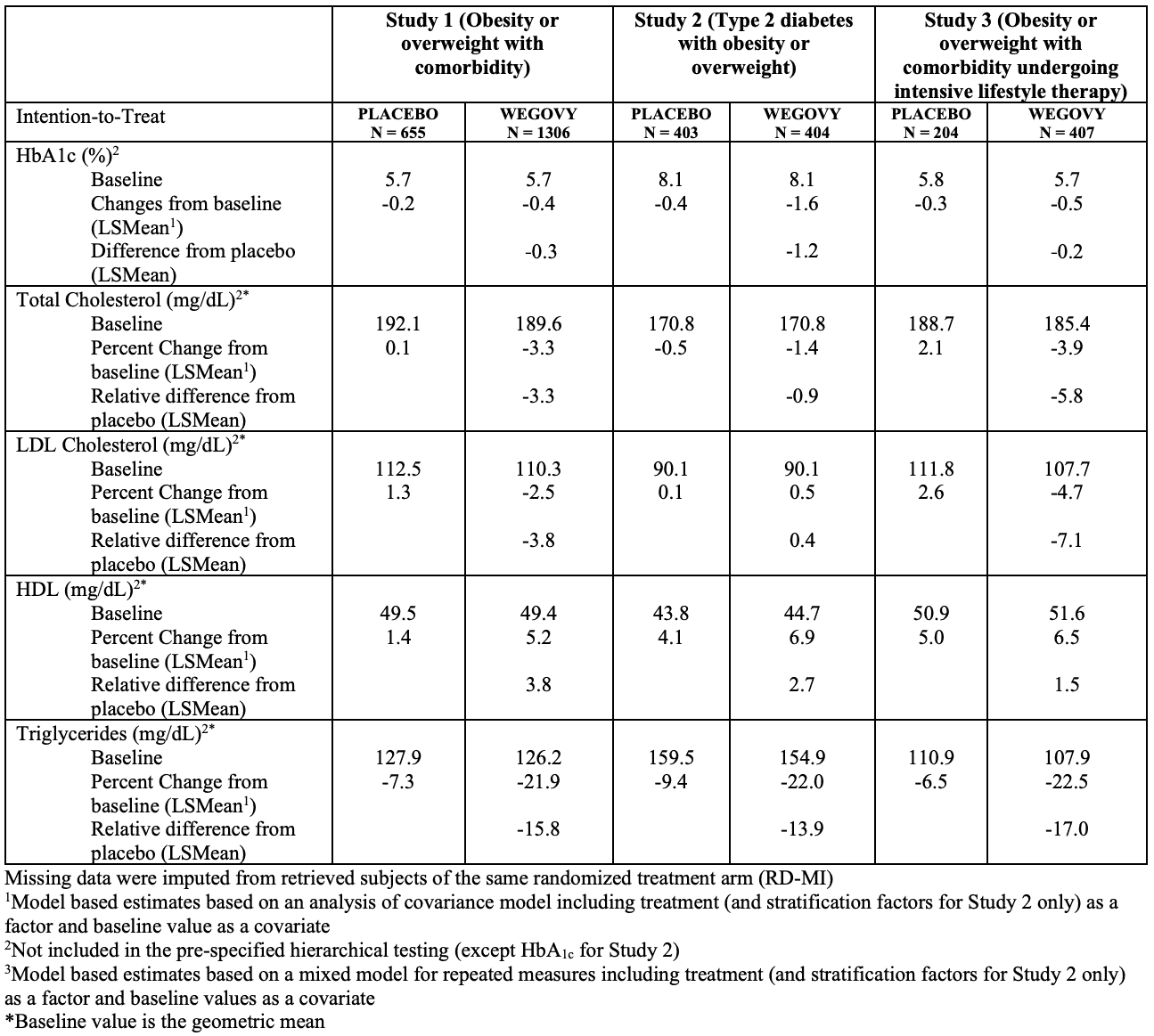
Other favorable effects of Wegovy include improvements in anthropometric parameters such as waist circumference and blood pressure, and improvements in cardiometabolic parameters, including levels of HbA1c, total cholesterol, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol, triglycerides.
Given that semaglutide in the form of the drug Ozempic, approved for therapy of type 2 diabetes mellitus, is permitted to reduce the risk of major adverse cardiovascular events (MACE) in adult patients with a history of type 2 diabetes and a history of cardiovascular disease, it is safe to assume that Wegovy also has the power to reduce MACE risks such as non-fatal myocardial infarction, non-fatal stroke, and cardiovascular death.
Wegovy: Safety of Semaglutide for Weight Loss
Among the most common adverse reactions to Wegovy prescription compared to placebo: nausea (44% versus 16%), diarrhea (30% vs. 16%), vomiting (24% vs. 6%), constipation (24% vs. 11%), abdominal pain (20% vs. 10%), headache (14% vs. 10%), fatigue (11% vs. 5%), dyspepsia (9% vs. 3%).
As we can see, the adverse events of using Wegovy come mainly from the gastrointestinal tract. In most cases, they are mild to moderate in severity, reach their peak during increasing the dose of semaglutide, are transient, and almost disappear during stable therapy.
Prescribing information for Wegovy, as well as all other analogs of glucagon-like peptide-1, has a black-boxed warning: semaglutide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC), as well as those with multiple endocrine neoplasia syndrome type 2 (MEN 2). In rodent trials, semaglutide led to the development of thyroid C-cell tumors.
Wegovy: How Semaglutide Works to Treat Obesity and Weight Loss
Semaglutide, being a biological drug, is a glucagon-like peptide-1 receptor (GLP-1R) agonist.
Glucagon-like peptide-1 (GLP-1) belongs to the incretins, a group of metabolic hormones that stimulate blood glucose lowering. The incretins are released after meals, by a glucose-dependent mechanism, enhancing the production of insulin secreted by the beta cells of the islets of Langerhans in the pancreas.
GLP-1 is a peptide hormone secreted by enteroendocrine L-cells in the mucosa of the distal ileum and in the colon and by certain neurons of the solitary tract in the brainstem. Agonist activation of GLP-1R signaling has an insulinotropic effect that promotes insulin secretion in response to food intake. GLP-1R is expressed in pancreatic beta cells, various types of gastrointestinal cells, and neurons of the central and peripheral nervous systems.
Additional effects of GLP-1R agonism, beneficial in the therapy of obesity and overweight, are manifested by delayed gastric evacuation, decreased gastric juice secretion, and weakened gastric motility. All this leads to a suppression of appetite and a decrease in the postprandial rise in blood glucose levels. Among other things: decrease in plasma glucagon levels (glucagon raises blood glucose concentration and promotes gluconeogenesis and glycogenolysis) and activation of anorexigenic pathways in the brain (mediates weight loss).
The metabolic effects of GLP-1R agonism are not accompanied by a risk of hypoglycemic events in diabetics.
Wegovy: The Best Weight Loss ‘Pill’
If we evaluate the effectiveness of semaglutide on average, that is, regardless of the presence or absence of diabetes, whether or not to follow a program of lifestyle changes, the degree of treatment adherence, it turns out that one year of stable therapy (plus 4 months of gradual adjustment of the dose) with Wegovy can achieve the removal of 15.2% of excess body weight. And this is the best performance relative to other existing pharmacological interventions.
It is appropriate to give general data on the effectiveness of all other medications for the fight against overweight and obesity. It should be understood that the information is for reference purposes only and is not intended to make any comparisons between weight-loss drugs, as it would be methodologically incorrect to do so because of the differences between both the design of the clinical trials themselves and the baseline characteristics of their participant populations. For example, the pooled data included results from studies in which obese patients may concomitantly have type 2 diabetes mellitus and therefore followed background hypoglycemic therapy. Again, the ultimate efficacy of any weight-loss drug considerably varies from patient to patient and is independent of the degree of obesity, age, or prior dietary habits.
One more thing: the results cited excluded the totals of “ideal” patients who strictly adhered to a given course of treatment. In other words, the effectiveness of pharmacological correction of excessive weight given below can move up (by a few percent) if the prescribed therapy regimen (not skipping the next dose and completing the entire course of treatment) and its features (such as including a dietary regimen or physical activity) are clearly followed.
Wegovy joined the following drugs for chronic weight management:
- Qsymia (phentermine + topiramate). A combination of a sympathomimetic amine (similar to amphetamine) and an anticonvulsant developed by Vivus.
- Saxenda (liraglutide). Glucagon-like peptide-1 receptor agonist (GLP-1RA) made by Novo Nordisk.
- Xenical/Alli (orlistat). A reversible inhibitor of gastric and pancreatic lipases promoted by Roche and GlaxoSmithKline.
- Meridia (sibutramine) [banned in most countries]. Norepinephrine and serotonin reuptake inhibitor marketed by Abbott Laboratories.
- Contrave/Mysimba (bupropion + naltrexone). A combination of opioid receptor antagonist and norepinephrine and dopamine reuptake inhibitor by Orexigen Therapeutics, now run by Nalpropion Pharmaceuticals.
- Belviq (lorcaserin) [withdrawn from the market due to safety concerns]. Selective serotonin 5-HT2C receptor agonist by Arena Pharmaceuticals and later by Eisai.
Therapeutic efficacy of weight-loss drugs indicated for long-term use to correct body weight
| Drug | Weight loss in 1 year of stable therapy, % | Patients who lost at least 5% of baseline weight in 1 year, % | Patients who lost at least 10% of baseline weight in 1 year, % |
|---|---|---|---|
| Wegovy (semaglutide) | 15.2 | 79 | 61 |
| Qsymia (phentermine + topiramate) | 10.4 | 68 | 48 |
| Saxenda (liraglutide) | 8.1 | 61 | 32 |
| Xenical/Alli (orlistat) | 7.5 | 51 | 27 |
| Meridia (sibutramine) | 7.0 | 57 | 29 |
| Contrave/Mysimba (bupropion + naltrexone) | 6.3 | 52 | 28 |
| Belviq (lorcaserin) | 5.5 | 46 | 21 |
- Percentages of patients are averaged, based on data from an array of relevant clinical trials.
Wegovy for Weight Loss: What’s Next
Novo Nordisk, wanting to gather more evidence in favor of semaglutide in confronting obesity and overweight in adult patients, is conducting series of additional clinical trials comparing 2.4-mg semaglutide to placebo (unless otherwise stated):
- STEP 5 (NCT03693430) [completed]: therapy for obesity or overweight (n=304) over two years (104 weeks)
- STEP 6 (NCT03811574) [completed]: therapy for obesity or overweight (n=400) for 68 weeks among patients from Japan and Korea with semaglutide at a dose of 1.7 or 2.4 mg, for participants from Japan a diagnosis of type 2 diabetes mellitus is allowed
- STEP 7 (NCT04251156) [ongoing]: therapy for obesity or overweight (n=375) for 44 weeks, allowed participants with a diagnosis of type 2 diabetes mellitus
- STEP 8 (NCT04074161) [completed]: therapy for obesity or overweight (n=1964) for 68 weeks, comparison group receives Victoza (liraglutide) at a daily dose of 3.0 mg
- NCT04102189 [completed]: therapy for obesity or overweight in adolescents (n=1964) for 68 weeks.
In the Name of Weight Loss: Coup de Grâce
Novo Nordisk is preparing to deliver a decisive blow to obesity. A phase 3 clinical trial is scheduled for the second half of 2021 to test a weekly combination of Wegovy and an experimental cagrilintide.
The rationale for the combination of semaglutide and cagrilintide was shown in the NCT03600480 phase 1b clinical trial (randomized, double-blind, placebo-controlled) involving adult patients who were overweight or obese. After 20 weeks, the group of participants who received 2.4 mg each of injectable semaglutide and cagrilintide weekly recorded a 17.1% weight loss.
Such impressive results of the semaglutide and cagrilintide cocktail, fast and powerful, suggest a future slogan: “Two drugs — lose two pounds a week.”
BioPharma Media
Importantly, the combination therapy was marked by acceptable tolerability: the most common adverse events in the form of gastrointestinal disorders, such as nausea and vomiting, were characterized by a mild to moderate severity. Simultaneously, their frequency was comparable to that observed with GLP-1R agonists like semaglutide. In other words, no serious safety problems with cagrilintide have been identified so far.
Cagrilintide (AM833, NN9838) is an amylin receptor (AMYR) agonist that regulates energy homeostasis and triggers a satiation signal resulting in reduced food intake and increased energy expenditure while decreasing adiposity. Cagrilintide is thought to affect the homeostatic and hedonic areas of the brain, inducing a feeling of satiety and, furthermore, influencing specific food choices, which contribute to changes in eating behavior. Because cagrilintide and semaglutide act in different areas of the brain, their combined administration leads to an additive effect on appetite regulation.
In the 26-week NCT03856047 phase 2 clinical trial (randomized, double-blind, placebo-controlled, active-control, multicenter, international) among adult patients (n=706) with obesity or overweight and without type 2 diabetes mellitus, there was a statistically significant benefit of weekly mono-administration of cagrilintide over placebo or Victoza.
The weight loss provided by cagrilintide was 6.0–10.8% (dose-dependent: 0.3, 0.6, 1.2, 2.4, or 4.5 mg) and was not characterized by a plateau reaching by the end of the study. In the placebo and liraglutide groups: 3.0% and 9.0%. In the maximum 4.5-mg dose cagrilintide group, weight loss of at least 5%, 10%, or 15% was noted for 88.7%, 53.5%, and 18.7% of patients. Adverse reactions to cagrilintide, coming with acceptable tolerability, occurred mainly from the gastrointestinal tract.
Market Prospects for Semaglutide
According to Evaluate Pharma, sales of semaglutide for treating obesity are projected to reach $2.4 billion by 2026, far surpassing demand for other weight-loss drugs.
Semaglutide belongs to an extensive class of injectable glucagon-like peptide-1 receptor agonists (GLP-1RAs) ubiquitously and successfully used in the therapy of type 2 diabetes mellitus. Such drugs include Trulicity (dulaglutide), Ozempic (semaglutide), Victoza (liraglutide), Byetta (exenatide), Bydureon/Byetta Long (exenatide), Adlyxin/Lyxumia (lixisenatide). Standing alone is oral Rybelsus (semaglutide). Worldwide sales of GLP-1RAs exceeded $10.6 billion in 2019 and $12.8 billion in 2020.
Global sales of glucagon-like peptide-1 receptor agonists (GLP-1RAs), million dollars
| Drug | INN | Originator | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 |
|---|---|---|---|---|---|---|---|---|
| Trulicity | Dulaglutide | Eli Lilly | 926 | 2030 | 3199 | 4128 | 5068 | 6472 |
| Ozempic | Semaglutide | Novo Nordisk | 285 | 1685 | 3243 | 5359 | ||
| Victoza | Liraglutide | Novo Nordisk | 2979 | 3511 | 3856 | 3288 | 2867 | 2393 |
| Saxenda (for weight loss) | Liraglutide | Novo Nordisk | 234 | 388 | 613 | 851 | 857 | Combine 1335 |
| Wegovy (for weight loss) | Semaglutide | Novo Nordisk | ||||||
| Bydureon/Byetta Long | Exenatide | AstraZeneca | 578 | 574 | 584 | 549 | 448 | 385 |
| Rybelsus | Semaglutide (oral) | Novo Nordisk | 7 | 286 | 769 | |||
| Byetta | Exenatide | AstraZeneca | 254 | 176 | 126 | 110 | 68 | 55 |
| Adlyxin/Lyxumia | Lixisenatide | Sanofi | 36 | 30 | 11 | |||
| Tanzeum/Eperzan (withdrawn) | Albiglutide | GlaxoSmithKline | 165 | 113 | 41 | |||
| Mounjaro | Tirzepatide | Eli Lilly |
- In August 2017, GlaxoSmithKline announced that sales of Tanzeum/Eperzan (albiglutide) had been stopped for economic reasons; it could not survive the competition.
- As of 2019, sales of Adlyxin/Lyxumia (lixisenatide) are too insignificant for Sanofi to include their volumes in the financial annual report.
Wegovy’s launch seriously strengthened Novo Nordisk’s metabolic business, which is forming around semaglutide. Thus, in December 2017, Ozempic (semaglutide) appeared, indicated to improve glycemic control in adult patients with type 2 diabetes mellitus. In January 2020, Ozempic expanded its range of indications: it can now be used to reduce the risk of major adverse cardiovascular events (MACE) in adult patients with type 2 diabetes mellitus and a history of cardiovascular disease.
Ozempic actually acted as a replacement for Novo Nordisk’s Victoza (it is more effective and is used once a week rather than once a day) and a direct competitor to the weekly Trulicity promoted by Eli Lilly, which took the top spot in 2019 GLP-1RAs sales ahead of Victoza. Novo Nordisk’s position in the GLP-1RA market, though, is leading the way. Thus, between 2016 and 2017, global sales of GLP-1RA class drugs totaled $44.2 billion, of which $25 billion came from the Danish drugmaker: Ozempic, Victoza, Saxenda (liraglutide) [for weight loss], and Rybelsus.
It is appropriate to draw a parallel between the pairs of drugs: Victoza and Saxenda, Ozempic and Wegovy. Thus, in the first pair, liraglutide was first started for therapy of diabetes and then connected overweight patients. Semaglutide did a similar job. In all cases, therapy for obesity involves prescribing an increased dose of the drug compared to therapy for diabetes. The maximum maintenance doses of Victoza and Saxenda are 1.8 and 3 mg while Ozempic and Wegovy are 1,0 and 2.4 mg.
To the point, at the end of January 2021, Novo Nordisk sent a label expansion application to the FDA for the possibility of increasing the weekly dose of Ozempic to 2 mg. But at the end of March, the regulator refused citing the need to provide additional data regarding the new manufacturing site. Novo Nordisk resubmitted the application in late May hoping for regulatory approval within a maximum of 10 months.
Novo Nordisk needs a doubled dose of Ozempic for the reason that the colossus Eli Lilly, which is preparing to offer tirzepatide in 2022, is looming behind it. The upcoming antidiabetic drug has a dual action: a glucose-dependent insulinotropic polypeptide receptor (GIPR) agonist is added to the standard GLP-1RA. The resulting efficacy is very powerful in the task of reducing blood glucose levels and body weight.

Tirzepatide: New Dual-Action Drug Against Type 2 Diabetes Mellitus
Eli Lilly has developed a powerful antidiabetic drug. It will be available in 2022.
Since tirzepatide succeeded ahead of Ozempic on all fronts, an alarmed Novo Nordisk is pressing ahead with the results of the SUSTAIN FORTE (NCT03989232) phase 3b clinical trial, which showed that the 2-mg dose of semaglutide statistically significantly outperformed the current 1-mg in terms of HbA1c reduction and greater weight loss; while the available safety profile was almost unimpaired.
Moreover, Novo Nordisk believes that semaglutide can be used for treating other diseases. For example, therapy of non-alcoholic steatohepatitis (NASH) seems promising. First, semaglutide has already demonstrated some success on its own, so it is continuing to be tested in the ESSENSE (NCT04822181) clinical trial phase 3 against NASH (stage 2–3 fibrosis).
Second, in the second half of 2021, in collaboration with Gilead Sciences, a 24-week phase 2b clinical trial of an experimental treatment for NASH with compensated cirrhosis (stage 4 fibrosis) will be conducted with a three-drug cocktail: semaglutide, cilofexor, a nonsteroidal agonist of farnesoid X receptor (FXR), and firsocostat, an acetyl-CoA carboxylase (ACC) inhibitor.

Lipaglyn: World’s First Drug to Treat Non-Alcoholic Steatohepatitis and Non-Alcoholic Fatty Liver Disease
Saroglitazar by Zydus Cadila has opened the doors to a new multi-billion dollar sector of NASH and NAFLD pharmacological treatments.
Meanwhile, the 52-week STEP-HFpEF (NCT04788511) phase 3 clinical trial was launched, testing the hypothesis that semaglutide would have beneficial effects in obese (BMI ≥30 kg/m2) patients with heart failure (NYHA class II–IV) with preserved ejection fraction (HFpEF).
As for Rybelsus, which debuted in September 2019 to improve glycemic control in adults with type 2 diabetes mellitus. It is the world’s first GLP-1RA implemented in an oral formulation and therefore has made all other oral antidiabetic competitors shudder, including many gliptins and gliflozins — members of the dipeptidyl peptidase-4 (DPP-4) inhibitors and sodium-glucose cotransporter 2 (SGLT2) inhibitors, respectively.
In April 2021, Novo Nordisk announced the launch of a 68-week phase 3a pivotal clinical trial of oral semaglutide’s suitability for overweight and obesity therapy. Rybelsus, similar to other GLP-1RAs, will be studied at an increased dose: instead of the maximum antidiabetic 14-mg dose, 50 mg of the drug will be tested. The trial will begin in the second half of the year.
The large-scale trials of oral 14-mg semaglutide in diabetes therapy found that for 52 weeks it reduced weight by 3.8–5.1% and 4.1–6.1% (an average of 4.3% and 5.2%) among “normal” and “ideal” patients, respectively. Assuming that the increased dose of the drug is twice as effective, we can expect to reduce the body weight in the range of 8.6% and 10.4%. And this is quite good.
Finally, Novo Nordisk believes that oral semaglutide may help with Alzheimer’s disease; the two-year phase 3 clinical trials EVOKE (NCT04777396) and EVOKE Plus (NCT04777409) are recruiting patients with early-stage Alzheimer’s manifesting as mild cognitive impairment (MCI) or mild dementia. The premise that GLP-1R agonism can help is abundant. For example, post hoc analysis of pooled data from nearly 16,000 patients with type 2 diabetes mellitus who underwent clinical trials of liraglutide and semaglutide found that these drugs reduced the risk of dementia by 53% (hazard ratio [HR] 0,47 (95% CI: 0.25–0.86).
Extras
Wegovy (semaglutide). Prescribing information. U.S. [PDF]
Novo Nordisk. Wegovy (semaglutide) approved in the U.S. Investor conference call. 7 June, 2021. [PDF]
Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021 Mar 18;384(11):989. [source]
Semaglutide 2.4 mg for the treatment of obesity: key elements of the STEP trials 1 to 5. Obesity (Silver Spring). 2020 Jun;28(6):1050-1061. [source]
Novo Nordisk. Conference call on decision to enter phase 3 development in early Alzheimer’s disease and GLP-1 R&D strategy update. 16 December, 2020. [PDF]
Novo Nordisk. Investor presentation Full year 2020. [PDF]
Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2·4 mg for weight management: a randomised, controlled, phase 1b trial. Lancet. 2021 May 8;397(10286):1736-1748. [source]
Cagrilintide plus semaglutide for obesity management. Lancet. 2021 May 8;397(10286):1687-1689. [source]
Efficacy and safety of AM833 for weight loss: a dose-finding trial in adults with overweight/obesity. [PDF]
AM833 is a novel agonist of calcitonin family G protein-coupled receptors: pharmacological comparison with six selective and nonselective agonists. J Pharmacol Exp Ther. 2021 Jun;377(3):417-440. [source]
Amylin and calcitonin: potential therapeutic strategies to reduce body weight and liver fat. Front Endocrinol (Lausanne). 2021 Jan 8;11:617400. [source]