Highlights
Tecvayli (teclistamab) is a new drug indicated to treat relapsed or refractory multiple myeloma (RRMM) in adult patients who have received at least three prior therapies, including an immunomodulatory agent, a proteasome inhibitor and an anti-CD38 antibody, and whose disease has progressed since their last therapy.
Tecvayli was developed by Janssen, part of Johnson & Johnson.
Tecvayli received marketing authorization from the European Medicines Agency (EMA) at the end of August 2022. The marketing authorization is conditional, which means that the drug has yet to prove its efficacy.
Approval by the U.S. Food and Drug Administration (FDA) is also just around the corner.
The pharmacological armamentarium for the treatment of multiple myeloma includes a wide range of drugs, but new drugs are constantly needed because of the characteristics of this disease, which is generally incurable, prone to relapse, and has a high frequency of development of resistance to the prescribed treatment.
Tecvayli: Mechanism of Action of Teclistamab
Teclistamab (JNJ-64007957) is a bispecific humanized monoclonal antibody that simultaneously binds to CD3, a T-cell surface antigen, and B-cell maturation antigen (BCMA), a tumor-associated antigen (TAA) expressed on plasma cells, including malignant myeloma cells. The cross-linking of T cells and tumor cells orchestrated by teclistamab induces a response by cytotoxic T lymphocytes (CTLs) mediating the lysis of myeloma cells. In other words, teclistamab redirects CD3+ T cells toward BCMA+ myeloma cells to be lysed and killed. Fc function silencing eliminates Fc-dependent immune effector functions. [1] [2]
B-cell maturation antigen is a transmembrane signaling protein that is expressed predominantly on mature B lymphocytes and is involved in their maturation and immune response formation.
BCMA along with B-cell activating factor receptor (BAFF-R, TNFRSF13C, CD268) and transmembrane activator and CAML interactor (TACI, TNFRSF13B, IGAD2, CD267) also belonging to the tumor necrosis factor receptor superfamily (TNFRSF), plays a critical role in the regulation of B cell proliferation and survival, maturation and differentiation into plasma cells (PCs). A trio of these functionally coupled receptors supports the long-term survival of B cells at various stages of their development through binding to their cognate ligands, B-cell activating factor (BAFF, BLyS, TNFSF13B, TALL-1, THANK, CD257) and/or a proliferation-inducing ligand (APRIL, TNFSF13, TALL-2, CD256). [3] [4] [5] [6]
BCMA is expressed on the surface of plasmablasts and differentiated PCs but not on memory B cells, naïve B cells, CD34+ hematopoietic stem cells (HSCs), and other healthy tissue cells. [7] [8] [9] [10] [11] [12] [13] [14] At the same time, mRNA and BCMA protein itself are characterized by much higher expression on malignant rather than normal PCs. [7] [15] [16] [17]
Cell lines of multiple myeloma and patients with the disease showed significantly higher concentrations of BCMA transcripts, the protein itself, and serum BCMA compared to cells from healthy donors. Serum BCMA levels directly correlate with disease status and prognosis. [17] [18] [19] [20] [21]
Teclistamab was developed by Denmark’s Genmab, which licensed it to Johnson & Johnson as part of a DuoBody proprietary technology platform agreement executed in mid-July 2012, providing for payments of up to DKK 1.062 billion ($145 million) per drug program and royalties from sales of the finished drug.
Tecvayli: Efficacy and Safety of Teclistamab for Multiple Myeloma Treatment
The efficacy and safety of teclistamab have been tested in the ongoing MajesTEC-1 clinical trial (non-randomized, open-label, multicenter, international), split into two phases, phase 1 (NCT03145181) and 2 (NCT04557098).
The study invited adult patients (n=165) with multiple myeloma whose disease was relapsed or refractory to standard therapy or who were characterized by intolerance to such therapy. Prior treatment had to include, in any order, administration of an immunomodulatory drug, a proteasome inhibitor, and an antibody against CD38.
Among the main characteristics of the participants: patients had previously received a median of 5 (2–14) lines of therapy; 70% had received at least two immunomodulatory agents, two proteasome inhibitors, and one anti-CD38 antibody; 90% were resistant to prior therapy; 78% had disease refractory to three drug classes and 30% to five drug classes.
Subjects were injected subcutaneously with teclistamab at 1.5 mg/kg once weekly (preceded by a period of step-up doses) until disease progression, unacceptable toxicity, or a maximum of 2 years.
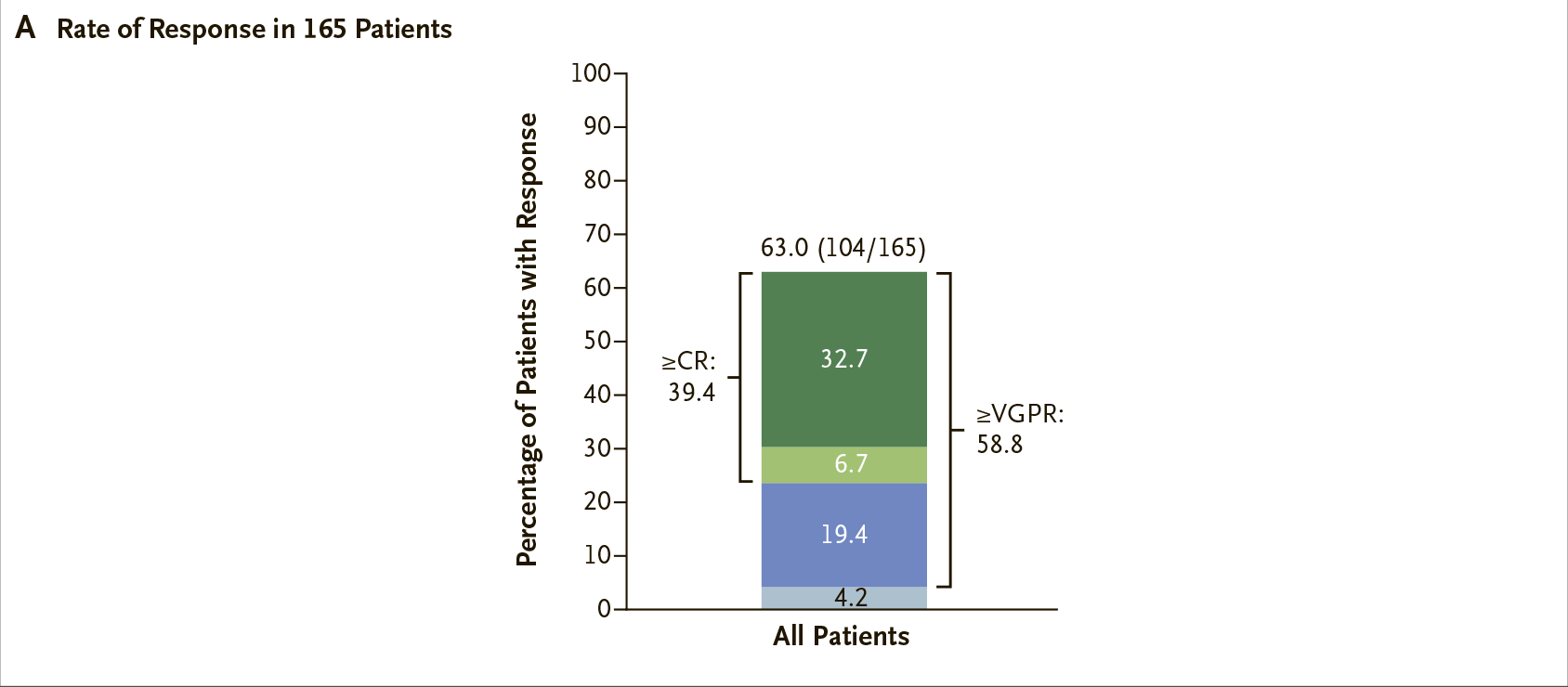
After a median of 14.1 months (0.3–24.4) of follow-up, the overall response rate (ORR) was 63.0% (95% CI: 55.2 to 70.4) including 39% complete responses (CR) or better and 59% very good partial responses (VGPR) or better.
In more detail, administration of Tecvayli resulted in 33% strict complete responses (sCR), 7% CR, 19% VGPR, and 4% partial responses (PR).
Negative minimally residual disease (MRD) status was reported for 27% (95% CI: 20.1 to 34.1) of patients, whereas among patients with CR or better in status without MRD there were 46%.
The median time until the first response was 1.2 months (0.2–5.5).
Response rates were lower in patients with extramedullary disease, stage III disease, and bone marrow replacement with plasma cells by at least 60%, but higher in those who underwent no more than three lines of therapy. Otherwise, response rates were similar in most clinically relevant subgroups, including patients with cytogenetic high-risk abnormalities and those refractory to five classes of drugs.
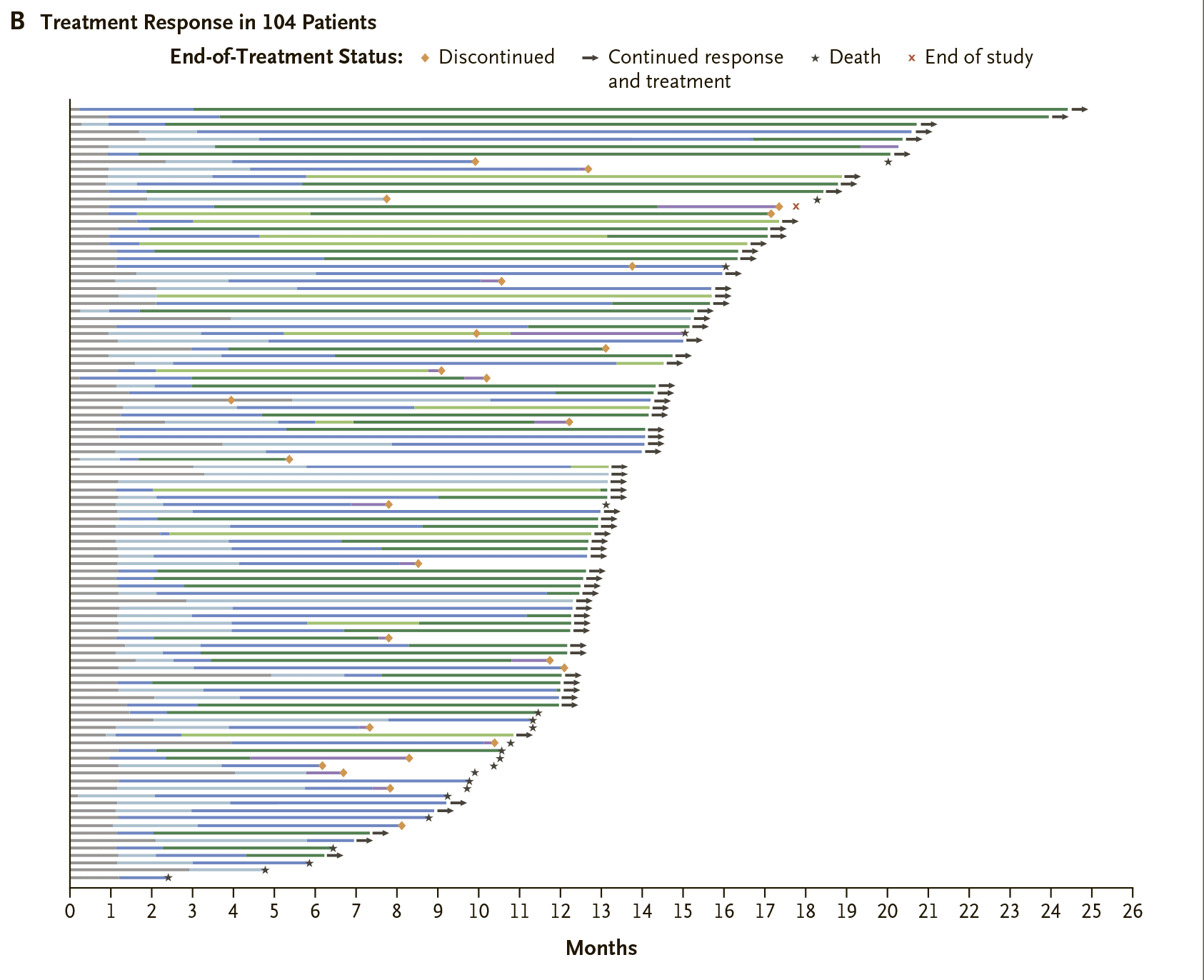
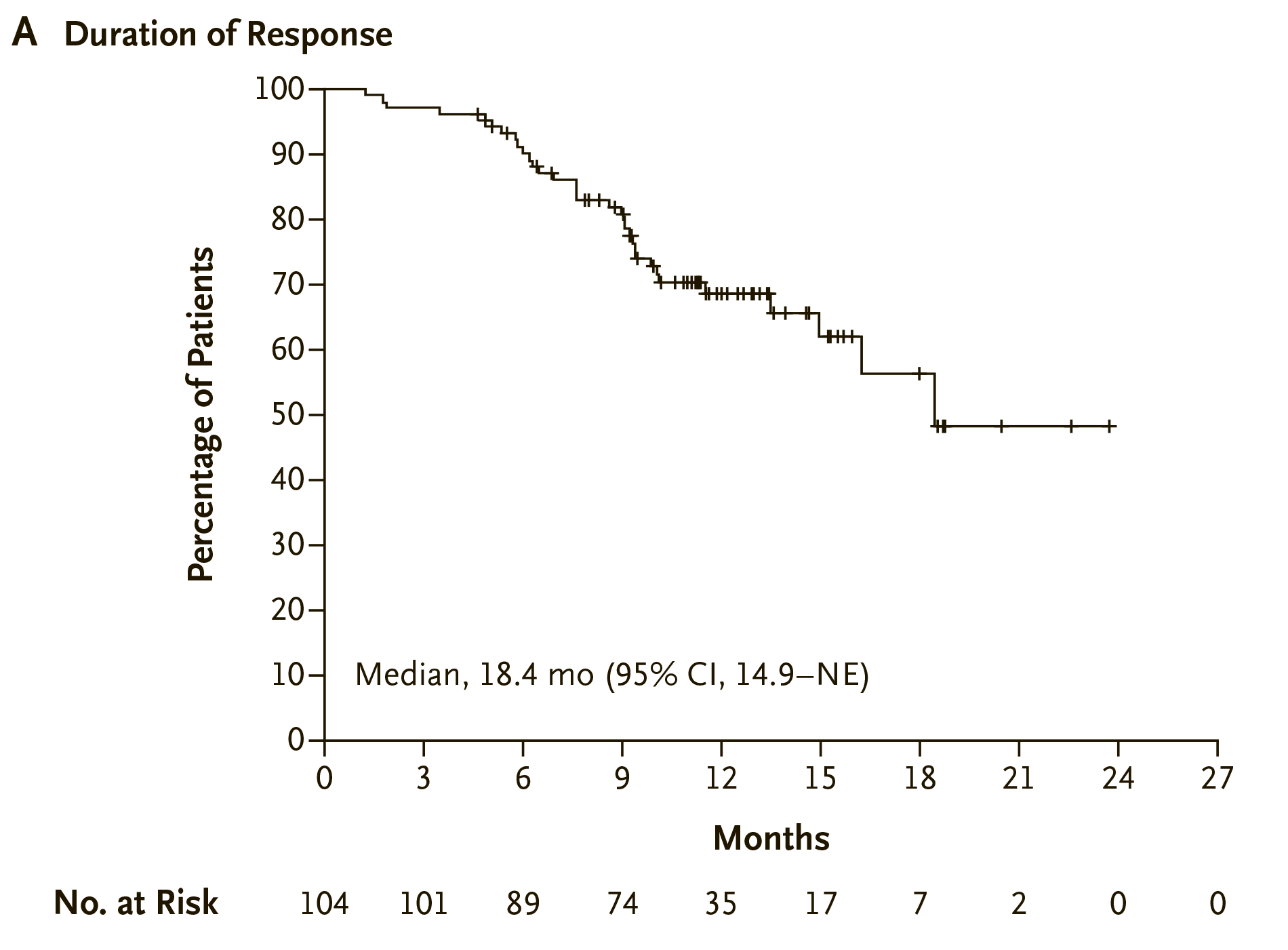
Responses to multiple myeloma therapy with teclistamab were durable and deepened over time. The median duration of response (DoR) was 18.4 months (95% CI: 14.9 to NE). The estimated probability of maintaining a response for at least 12 months was 68.5% (95% CI: 57.7 to 77.1).
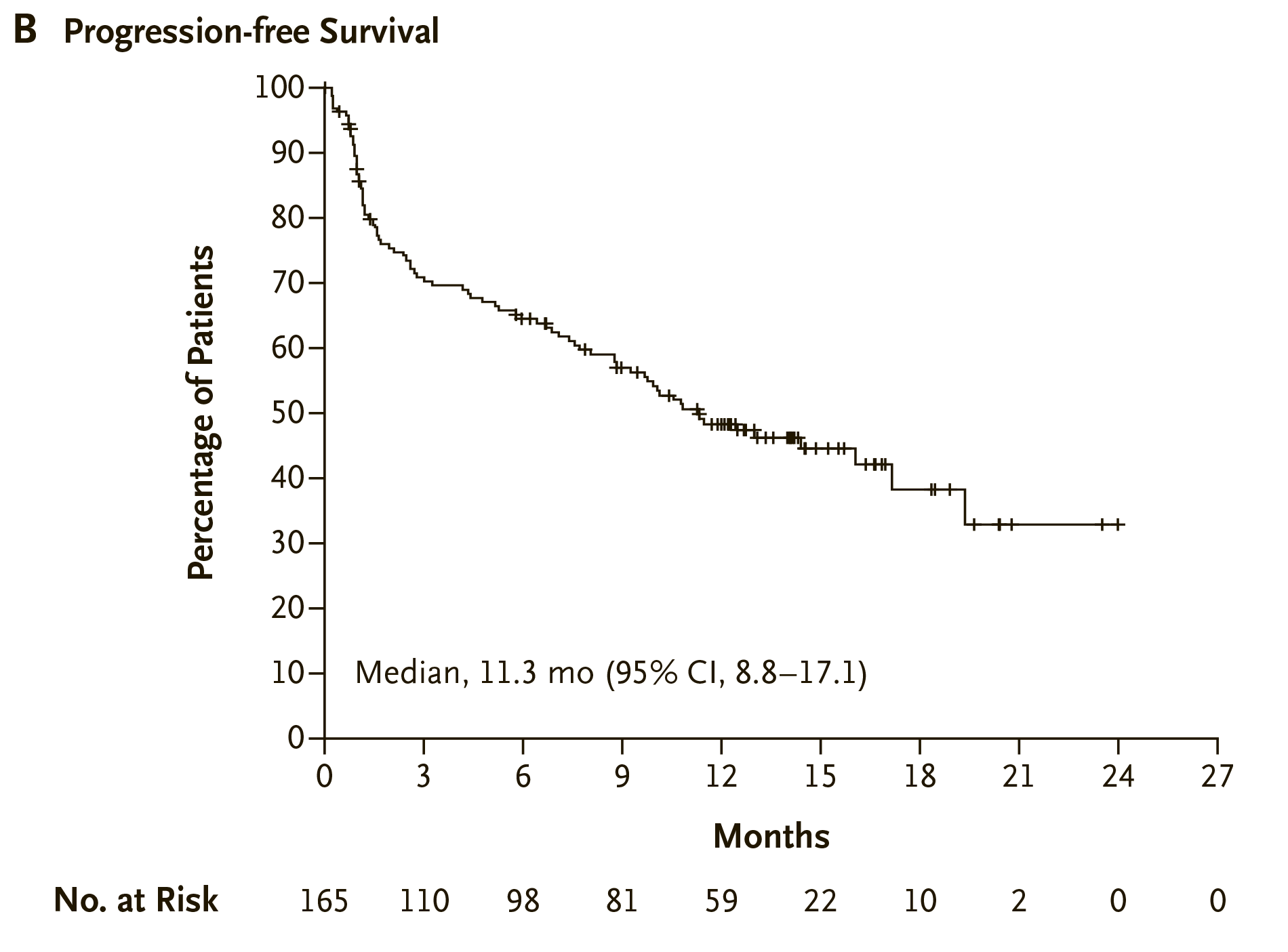
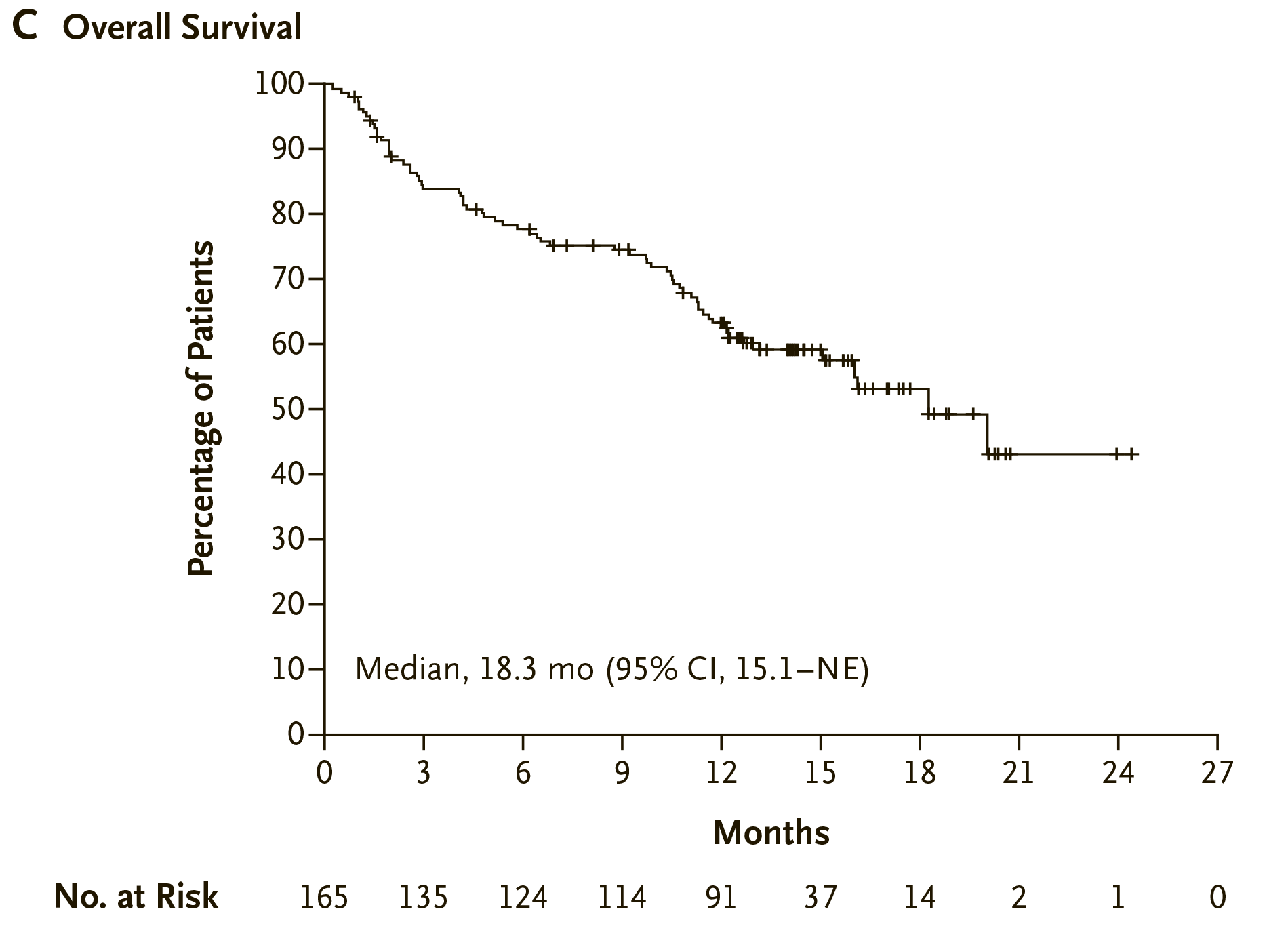
Median progression-free survival (PFS) came out to 11.3 months (95% CI:8.8 to 17.1). Median overall survival (OS) reached 18.3 months (95% CI: 15.1 to NE).
The administration of Tecvayli was accompanied by adverse events (AEs), the most common of which were diarrhea (in 29% of patients), fatigue (28%), nausea (27%), pyrexia (27%), injection-site erythema (26%), headache (24%), arthralgia (22%), constipation (21%), cough (20%), pneumonia (18%), bone pain (18%), and back pain (16%).
Hematologic changes were noted: neutropenia (71%), anemia (52%), thrombocytopenia (40%), lymphopenia (35%), leukopenia (18%).
All patients experienced AEs, and in 95% of them the severity of AEs was severe or life-threatening. For this reason, two-thirds of patients (63%) had to skip the next dose of teclistamab. 78% of patients with neutropenia were treated with granulocyte colony stimulating factor (G-CSF). Three-quarters of patients (75%) had hypogammaglobulinemia (antibody deficiency) and half of them (53%) had to receive intravenous immunoglobulin (IVIG).
Cytokine release syndrome (CRS), mostly mild-to-moderate in severity, was reported in 72% of patients and was mostly encountered at the beginning of treatment. Tocilizumab, low-flow oxygen, and glucocorticoids were used to control it. None of the CRS cases forced treatment discontinuation.
Neurotoxic events, including immune effector cell–associated neurotoxicity syndrome, occurred in 15% of patients. For the most part, their severity was mild-to-moderate.
During the clinical trial, 41% of patients died, of which 5 deaths were related to teclistamab: deaths due to progressive multifocal leukoencephalopathy, COVID-19, hepatic failure, and streptococcal pneumonia.
Expert Comments
Standard treatment for multiple myeloma includes the use of immunomodulatory agents, proteasome inhibitors, and monoclonal antibodies against CD38 that prolong patients’ overall survival (OS). [1] [2] [3]
If after their administration the disease continues to progress, which happens quite often, the available treatment options are limited and are usually characterized by unsatisfactory outcomes: refractoriness to the drugs develops, each subsequent line of therapy becomes less and less effective. [4] [5] [6] [7]
Thus, a retrospective analysis of patients who underwent median four lines of therapy and refractory to anti-CD38 antibodies showed that the overall response rate (ORR) to follow-up treatment was 31%, median progression-free survival (PFS) came out to 3.4 months, median OS was fixed at 9.3 months. [8]
In July 2019, Karyopharm Therapeutics launched Xpovio/Nexpovio (selinexor) to treat completely hopeless patients with relapsed or refractory multiple myeloma, that have undergone at least four lines of therapy and are refractory to at least two proteasome inhibitors, at least two immunomodulators, and an anti-CD38 monoclonal antibody. Selinexor, being a selective inhibitor of nuclear export (SINE) tested in patients who had already received median eight lines of therapy, had the following efficacy rates: ORR of 25%, including strict complete response (sCR) in 1% of patients, median PFS of 3.7 months, median OS of 8.6 months. [9]
The pharma industry then switched to B-cell maturation antigen (BCMA), which is widely expressed on myeloma cells and therefore represents a promising therapeutic target in multiple myeloma, releasing three drugs targeted for BCMA: GlaxoSmithKline’s antibody–drug conjugate Blenrep (belantamab mafodotin) and the CAR T cell therapeutics Abecma (idecabtagene vicleucel) by Bluebird Bio/Celgene/Bristol-Myers Squibb and Carvykti (ciltacabtagene autoleucel) by Nanjing Legend Biotech/Janssen/Johnson & Johnson.
The efficacy of the mentioned anti-BCMA drugs administered to patients with relapsed or refractory multiple myeloma who have undergone at least four lines of therapy is as follows. Blenrep achieved an ORR of 31% including an sCR of 2% [10]. Abecma brought these results to 72% and 28% and Carvykti improved ORR and sCR to an impressive 98% and 78%. [11] [12] [13] However, such therapeutically powerful CAR-T therapy is not suitable for all patients and its use is accompanied by serious and severe adverse events, which can be fatal.
The emergence of Tecvayli has opened up new treatment options for advanced multiple myeloma that has become refractory to available therapeutic options. Because there is no comparison group in the MajesTEC-1 clinical trial of teclistamab, it is appropriate to compare its efficacy with outcomes obtained in real-world clinical practice for the treatment of relapsed or refractory multiple myeloma in those patients who meet the MajesTEC-1 participation criteria and who have received at least three lines of therapy. The administration of teclistamab has been found to be more effective than existing treatment options. Thus, Tecvayli provided a median OS of 18.3 months (95% CI: 18.3 to NR) — versus 13.2 months (95% CI: 10.6 to 18.7) in real-world practice: a hazard ratio (HR) of 0.67 (95% CI: 0.43 to 1.05; p=0.08). Median PFS was 10.1 months (95% CI: 8.1 to NR) — vs. 3.4 months (95% CI: 3.0 to 4.3): HR 0.42 (95% CI: 0.30 to 0.58; p<0.0001). [14] [15]
An indirect comparison of the efficacy of Tecvayli with the outcomes generated by Xpovio/Nexpovio or Blenrep in the treatment of relapsed or refractory multiple myeloma that does not respond to the administration of three different drug classes (immunomodulatory agent, proteasome inhibitor, anti-CD38 antibody) again shows in favor of teclistamab. At the same time, the clinical successes of teclistamab are more pronounced in comparison with selinexor than with belantamab mafodotin. [16] [17]
The extremely strong CAR-T therapies Abecma and Carvykti definitely lead the way, but their introduction into clinical practice for treating relapsed or refractory multiple myeloma is difficult. The main obstacle to CAR-T therapy is the need for access to specialized medical centers and a one-month wait until a cell-based drug is ready and personalized for each patient. Perhaps this will change with the appearance of “off-the-shelf” and therefore less expensive allogeneic CAR-T drugs from T cells of healthy donors designed with a view to eliminating the risk of rejection of the cell product due to the development of acute graft-versus-host disease (GVHD). The question with the response durability remains open, allogeneic CAR-T therapy is likely to be inferior to autologous therapy in terms of the duration of response to treatment.
Related work is being done by Allogene Therapeutics, Poseida Therapeutics, Autolus Therapeutics, Precision BioSciences, Crispr Therapeutics, and Celyad Oncology testing BCMA-targeted allogeneic CAR-T therapies ALLO-715/ALLO-605, P-BCMA-ALLO1/P-BCMACD19-ALLO1, AUTO8, PBCAR269A/PBCAR269B, CTX120, and CYAD-211, respectively. [18] [19] [20] [21] [22] [23] France’s Cellectis is studying the allogeneic CAR-T drug UCARTCS1, targeting, similarly to Empliciti (elotuzumab) by Bristol-Myers Squibb , the surface antigen SLAMF7 (CS1, CD319). [24]
Meanwhile, Johnson & Johnson continues to clinically validate teclistamab in earlier treatments for multiple myeloma. It is possible that the T cell pool, not yet severely depleted by the long-lasting disease, should be expected to produce excellent therapeutic results. So, the MajesTEC-4 (NCT05243797) phase 3 clinical trial is testing a combination of teclistamab with lenalidomide as maintenance therapy for previously untreated multiple myeloma following autologous stem cell transplantation. The MajesTEC-3 (NCT05083169) phase 3 is testing a combination of teclistamab with daratumumumab in relapsed or refractory multiple myeloma that has received no more than three lines of therapy. A cocktail of two drugs seems to make sense: In addition to direct cytotoxic activity, daratumumumab has immunomodulatory effects, including stimulation of T cell expansion and depletion of CD38+ suppressive immunoregulatory cells, as reflected by enhanced teclistamab-mediated myeloma cell lysis. [25]
Johnson & Johnson is also checking out the highly intriguing hypothesis of adding experimental nirogacestat (PF-03084014) to teclistamab, behind which Pfizer, which in September 2017 put it into the hands of its own startup, SpringWorks Therapeutics. Nirogacestat, as a gamma secretase inhibitor, in addition to its primary task of treating desmoid tumors, has the ability to cleave BCMA resulting in the release of its extracellular domain (ECD) from the cell surface. If this function is suppressed, BCMA expression on plasma cells will be preserved (increasing the density of BCMA as a therapeutic target) and the level of soluble ECD BCMA (can serve as a decoy receptors for BCMA-targeting therapy) will decrease. As a result, there are opportunities for enhancing the therapeutic activity of BCMA-targeted drugs and reducing their dosage, in order to improve efficacy and reduce toxicity. [26] [27] [28]
The pharmaceutical industry understands that the niche of bispecific antibodies that bind BCMA and CD3 is promising and profitable, and therefore other players are developing drugs whose mechanism of action is similar to teclistamab. Thus, elranatamab (PF-06863135), linvoseltamab (REGN5458) and ABBV-383B (TNB-383B) are bringing Pfizer, Regeneron Pharmaceuticals and AbbVie to the fore. Amgen, behind bispecific monoclonal antibodies called Bi-specific T-cell engagers (BiTEs), is studying pavurutamab (AMG 701). Harpoon Therapeutics is trying its hand with a three-domain antibody, HPN217, designed within the modality of the Tri-specific T cell–Activating Construct (TriTAC).