The human mind treats a new idea the same way the body treats a strange protein; it rejects it.
Peter Medawar, biologist, Nobel Prize winner
A new scientific truth does not triumph by convincing its opponents and making them see the light, but rather because its opponents eventually die, and a new generation grows up that is familiar with it.
Max Planck, physicist, Nobel Prize winner
Crux of Problem
Progressive multiple sclerosis (PMS), as a severe form of this demyelinating disease, is classified into primary progressive multiple sclerosis (PPMS) and secondary progressive multiple sclerosis (SPMS). The first is true when the course of the disease is continuously worsening by the time of diagnosis (15% of cases). The second begins as relapsing-remitting multiple sclerosis (RRMS) which eventually turns into SPMS in 80% of patients.
Drugs offered by the pharmaceutical industry that alter the course of multiple sclerosis (disease-modifying therapy, DMT) are overwhelmingly aimed at treating RRMS as its most common form (85% of primary diagnoses). For example, Ocrevus (ocrelizumab) promoted by Roche declares that it is suitable for the therapy of patients with both RRMS and PPMS. And while in relapsing-remitting multiple sclerosis it is true that ocrelizumab is a highly effective DMT (although by no means unconditionally), in the case of primary progressive multiple sclerosis we cannot really call Ocrevus working yet. Even the FDA approved ocrelizumab against PPMS with a huge stretch, apparently due to the lack of any other therapy options. However, the Swiss pharma giant continues to look for evidence that its monoclonal antibody against CD20 can also cope with PPMS.
Novartis offers Mayzent (siponimod) which is suitable for patients with SPMS but only in its active form, that is when the inexorably progressive disease continues to be characterized by periods of relapse. Alas, as acceptable efficacy as with RRMS, siponimod could not be arranged for patients with SPMS.

Mayzent: New Drug for Treatment of Secondary Progressive Multiple Sclerosis
Siponimod released by Novartis is an improved version of Gilenya.
Ocrevus and Mayzent only marginally control the deterioration of disability in progressive multiple sclerosis: a tiny 6% difference from placebo no one can ever call evidence of a fundamental change in the course of the disease.

According to global statistics, the worldwide population of patients with multiple sclerosis is broken down as follows: RRMS accounts for 57% of patients, while PMS covers 43%, including 15% of patients with PPMS and 28% with SPMS.
The medical need for new breakthrough and, most importantly, highly effective drugs for the therapy of progressive multiple sclerosis remains unmet. The physician and patient communities dream either of reversing disability followed by sustained maintenance of the gains made, or of at least stably halting the progression of multiple sclerosis.
Hypothesis That Has Found Answer
Atara Biotherapeutics is working on the theory that the Epstein–Barr virus (EBV) is closely linked to the development of multiple sclerosis. And to that end, it is developing a therapy based on T cells as critical components of the body’s immune system that selectively target specific viral antigens. Targeted T cells recognize and eliminate from the central nervous system B lymphocytes and plasma cells infected with Epstein–Barr virus. The result of modulating the pathophysiology of multiple sclerosis is the prevention of subsequent autoimmune attacks and the discovery of the possibility of central nervous system repair through the mechanisms of remyelination, dendritic and axonal sprouting (outgrowth), synaptic remodeling.
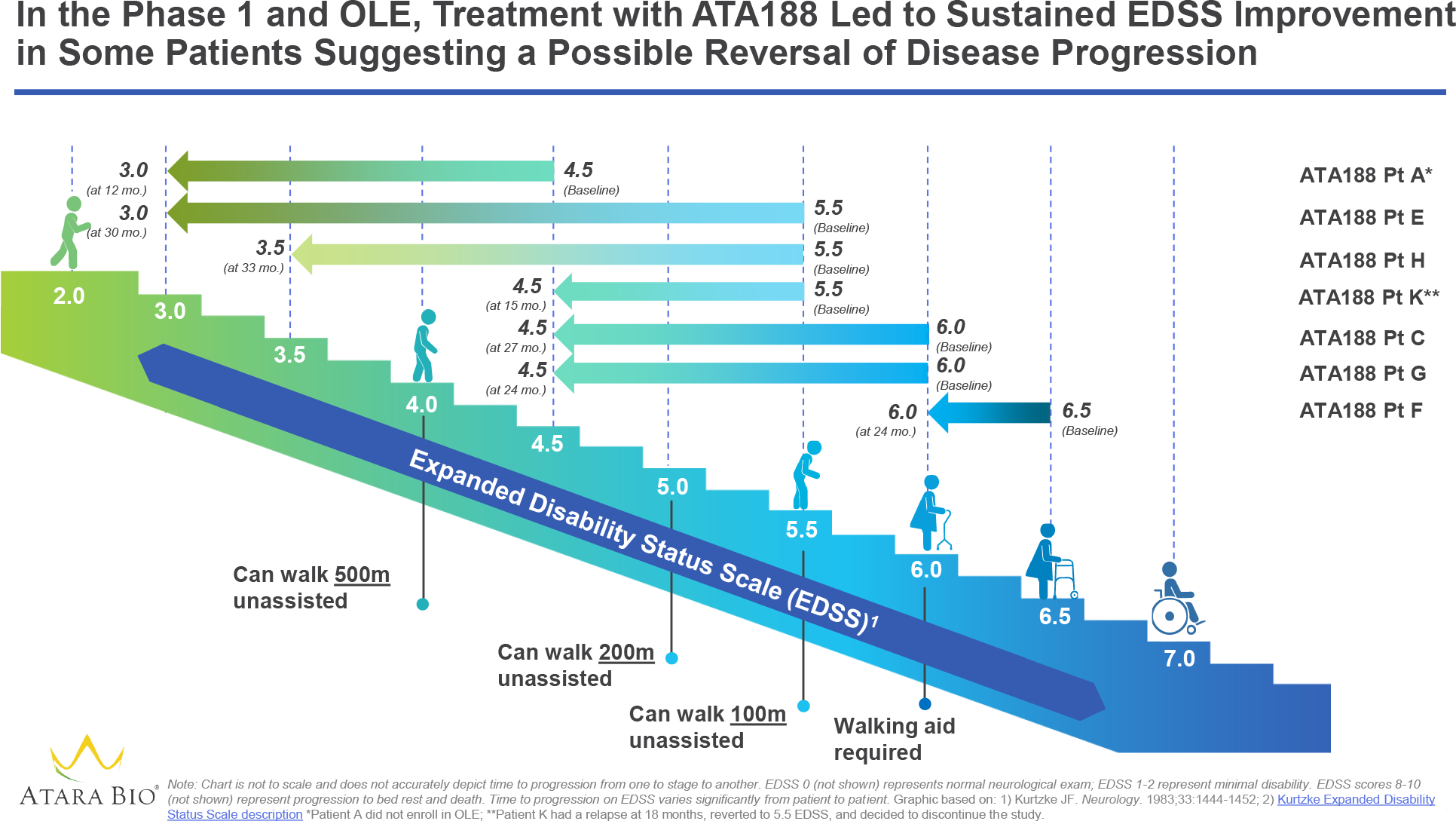
Atara’s achievements, supported by clinical trial data, confirm that its hypothesis is correct. Moreover, the demonstrated clinical efficacy of the experimental treatment of progressive multiple sclerosis is incredible, not only in halting the deterioration of an already serious disease but also in reversing it.
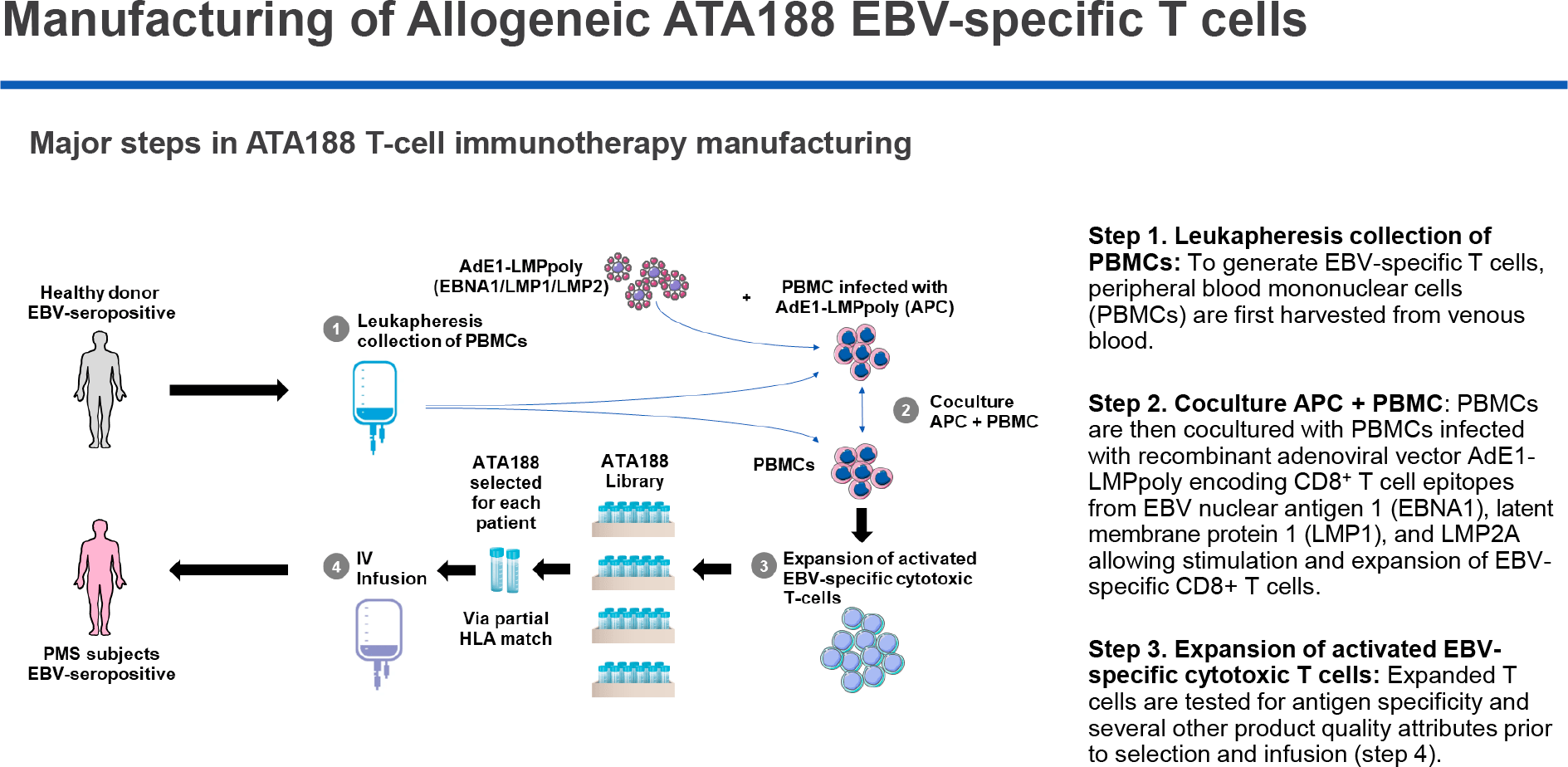
Atara is conducting a clinical trial of ATA188, a T-cell immunotherapy containing cytotoxic T lymphocytes against specific EBV protein antigens. Experimental ATA188 is allogeneic and is produced in advance by in vitro cultivation:
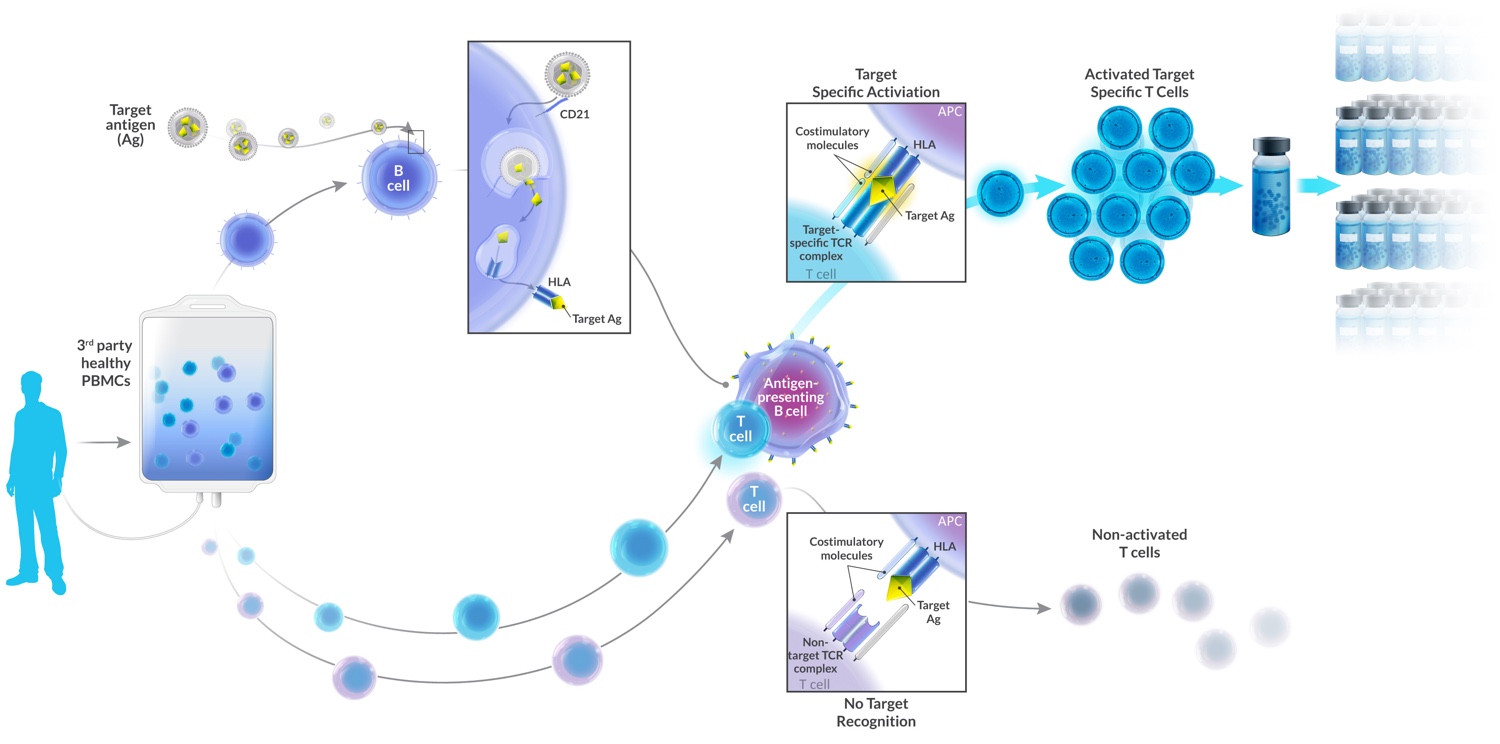
- Peripheral blood mononuclear cells (PBMCs) are collected from EBV-positive immunologically diverse and non-immunocompromised donors (non-multiple sclerosis patients) by leukopheresis. From these, T cells and B cells are isolated, which are then cultured and multiplied.
- B cells are transformed into antigen-presenting cells (APCs) by transfecting them with the recombinant adenoviral vector AdE1-LMPpoly which encodes CD8+ T-cell epitopes relevant to Epstein–Barr virus antigens — EBV nuclear antigen 1 (EBNA1), latent membrane protein 1 (LMP1), latent membrane protein 2A (LMP2A).
- T cells are exposed to APCs that express these EBV antigens. The result is the stimulation and proliferation of EBV-specific CD8+ T cells. Targeted cytotoxic T lymphocytes (CTL) are generated.
- When CTLs are administered intravenously to patients with multiple sclerosis, they destroy the EBV-infected B cells persisting in the central nervous system, which carry the EBV antigens sought.
Since ATA188 is only partially HLA matching, an extensive library of cryopreserved ATA188 products is created. The right one is selected for each patient by matching at least two HLA alleles common to ATA188 and a particular patient.
Previously, Atara tried its forces with autologous T-cell immunotherapy ATA190 but later abandoned it because the manufacture was carried out separately for the specifics of each patient which is very time-consuming and costly.
Possible Victory Over Progressive Multiple Sclerosis
The EMBOLD (NCT03283826) phase 1/2 clinical trial is testing the safety and efficacy of ATA188 administered as monotherapy once a year (multiple cycles) for five years to adult EBV-positive patients (n=97) with progressive forms of multiple sclerosis (primary progressive or secondary progressive).
The trial consists of two parts. Among the inclusion criteria: age 18–66 and 18–56 years, an Expanded Disability Status Scale (EDSS) score of 3.0–7.0 and 3.0–6.5 for parts one and two, respectively.

The first part of the study (open-label, dose-escalation) involved the determination of the effective dose of ATA188. The experimental drug was administered in four different doses: 5×106 cells (cohort 1, n=6), 1×107 cells (cohort 2, n=6), 2×107 cells (cohort 3, n=6), 4×107 cells (cohort 4, n=7). The baseline EDSS score of participants (n=25) was a median of 6.0 (4.0–6.5).
The following changes will be identified in the second part of the study (randomized, double-blind, placebo-controlled): EDSS, Timed 25-Foot Walk (T25FW), Nine-Hole Peg Test (9-HPT), cervical spinal cord and whole-brain MRI volumes, number of brain lesions on gadolinium-enhancing T1-weighted MRI images and number of new or enlarging lesions on T2-weighted MRI images.
Beginning Is Done
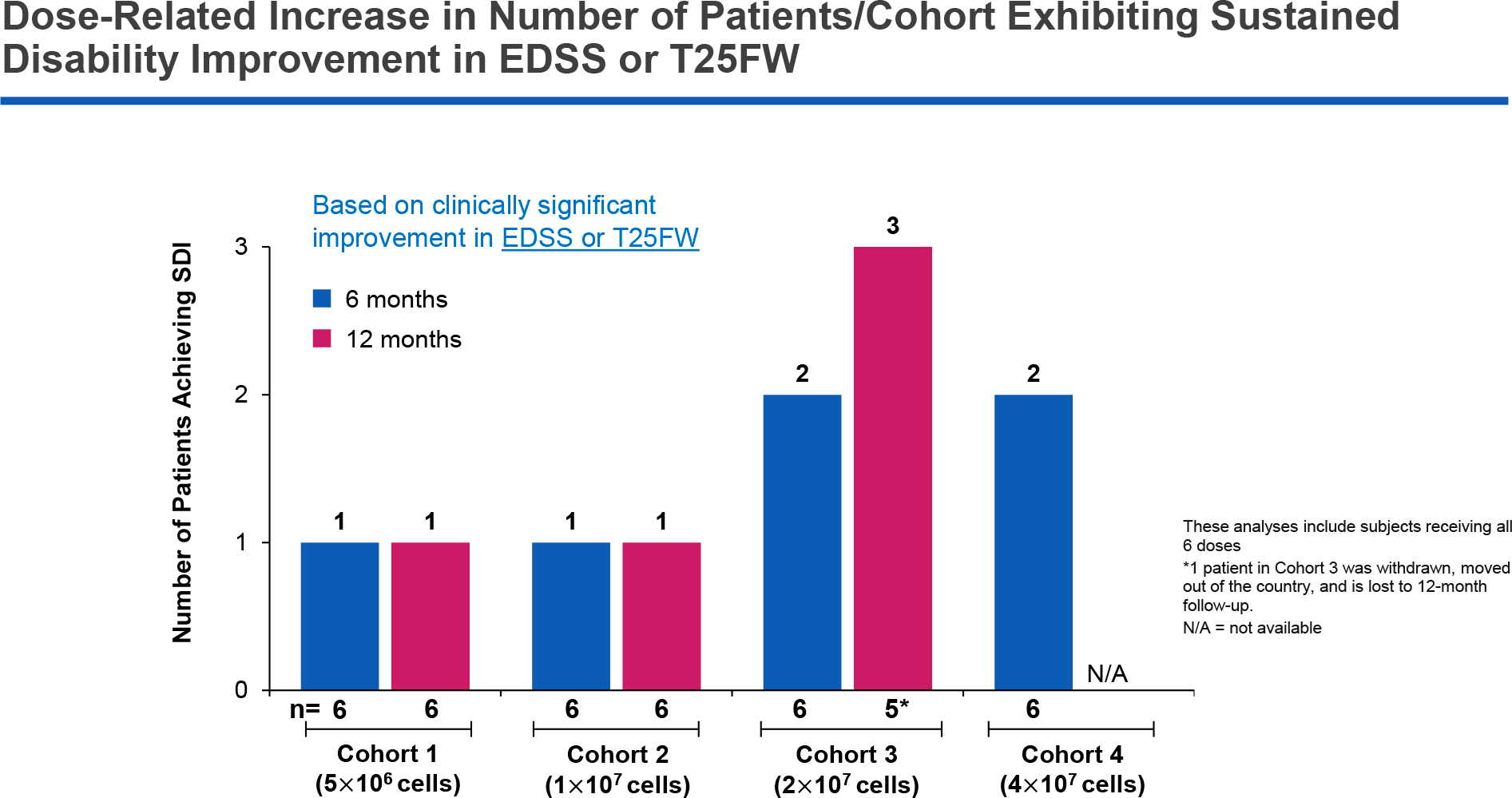
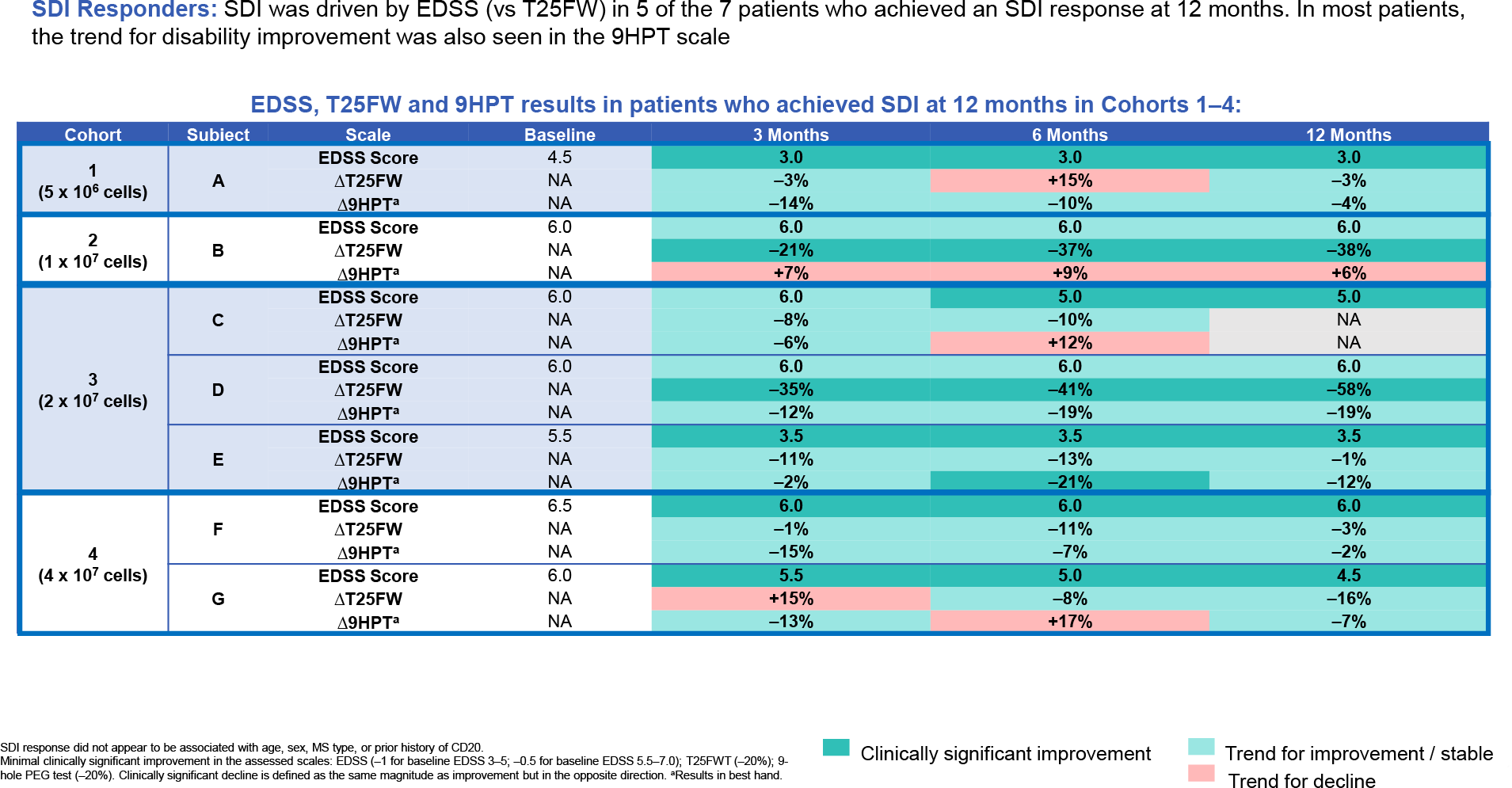
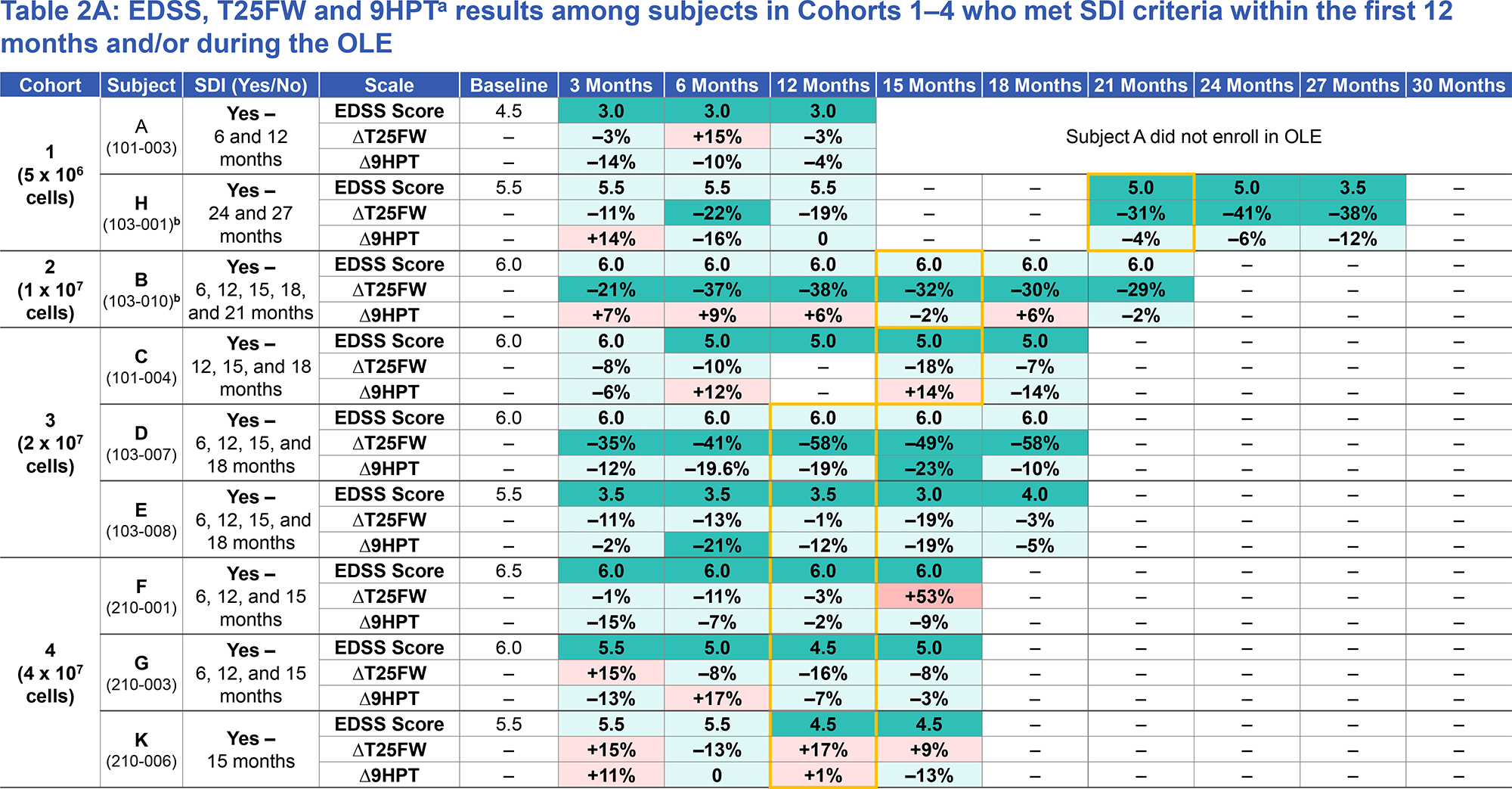
Atara shared 6 and 12 months of ATA188 study data collected in the first part of the trial. For this, a composite measure of therapeutic efficacy was established as Sustained Disability Improvement (SDI). The exit to SDI was confirmed at a minimally clinically significant improvement in EDSS score or T25FW time recorded over a period of two consecutive evaluations: for example, after three and then six months.
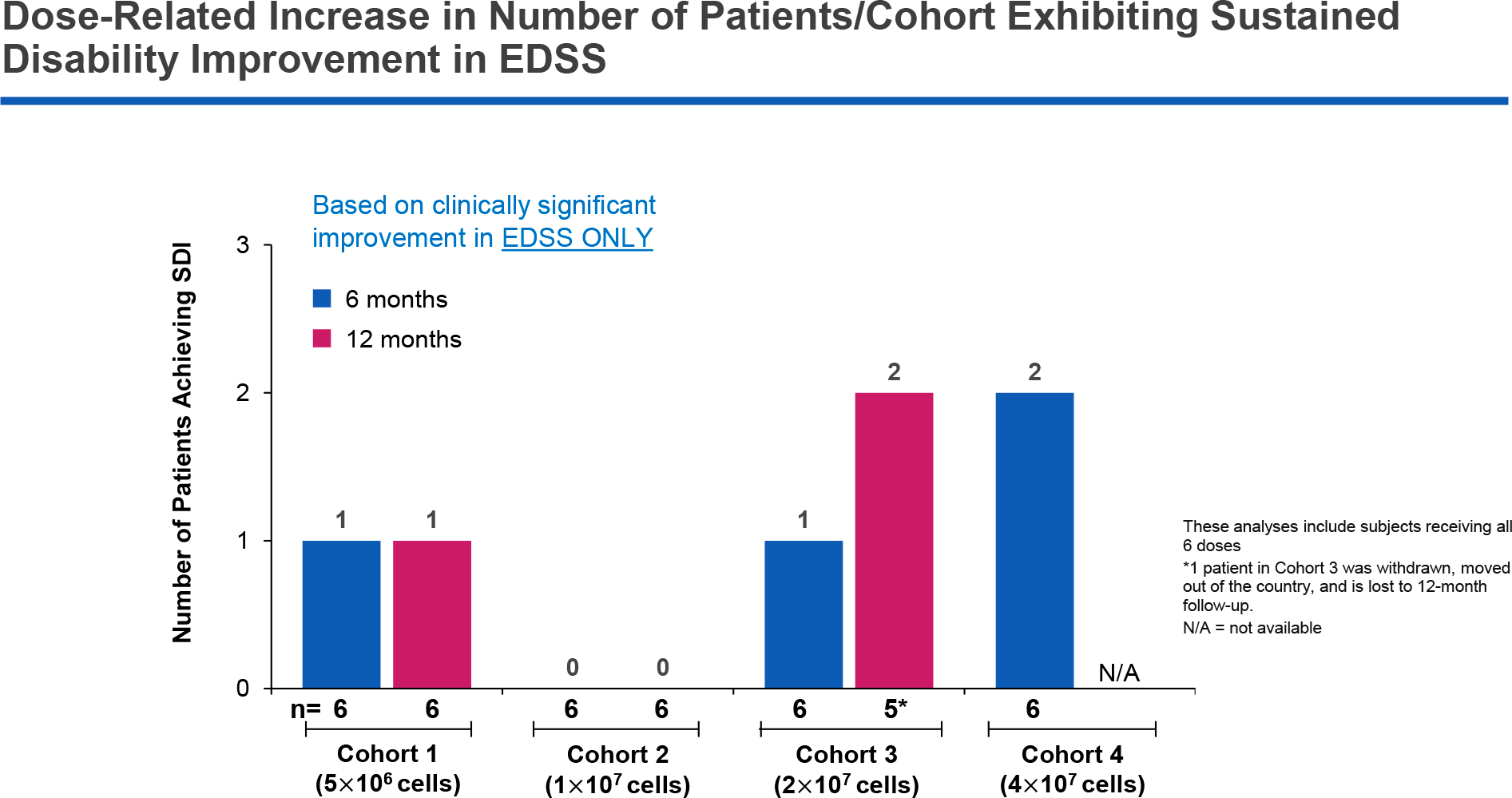
It is stated that the response to treatment deepened with an increasing dose of ATA188. Thus, one patient each in cohorts 1 and 2 and two patients in cohort 3 showed SDI over a period of six months that persisted beyond 12 months. Two participants in maximum dose cohort 4 also showed SDI at 6 months, but their 12-month data have not yet been collected. The main contribution to achieving SDI came from improvements in the EDSS score.
Atara conducted another assessment of the therapeutic efficacy of ATA188 using a composite endpoint designed to detect early indications of efficacy. This was an a priori classification of clinical outcomes assessed on seven scales valid for symptoms, functional capacity and degree of disability in patients with multiple sclerosis. Treatment was required to reach clinical improvement status, which was confirmed if improvement was recorded over a period of two or more consecutive assessments and continued at least at the minimum level for clinical significance.

The scales and necessary changes in their scores are as follows:
- Fatigue Severity Score (FSS): minimum clinical improvement should have been −0.7 points
- Multiple Sclerosis Impact Scale-29 (MSIS-29) [physical ability domain]: −8 points
- T25FW: −20%
- 9-HPT: −20%
- 12-item Multiple Sclerosis Walking Scale (MSWS-12): −8 points
- EDSS: −1 point (if baseline EDSS 3–5 points) and −0.5 points (if baseline EDSS 5.5–7.0 points)
- Visual Acuity (VA) [on the LogMAR scale]: a change of at least −0.1 in each eye.
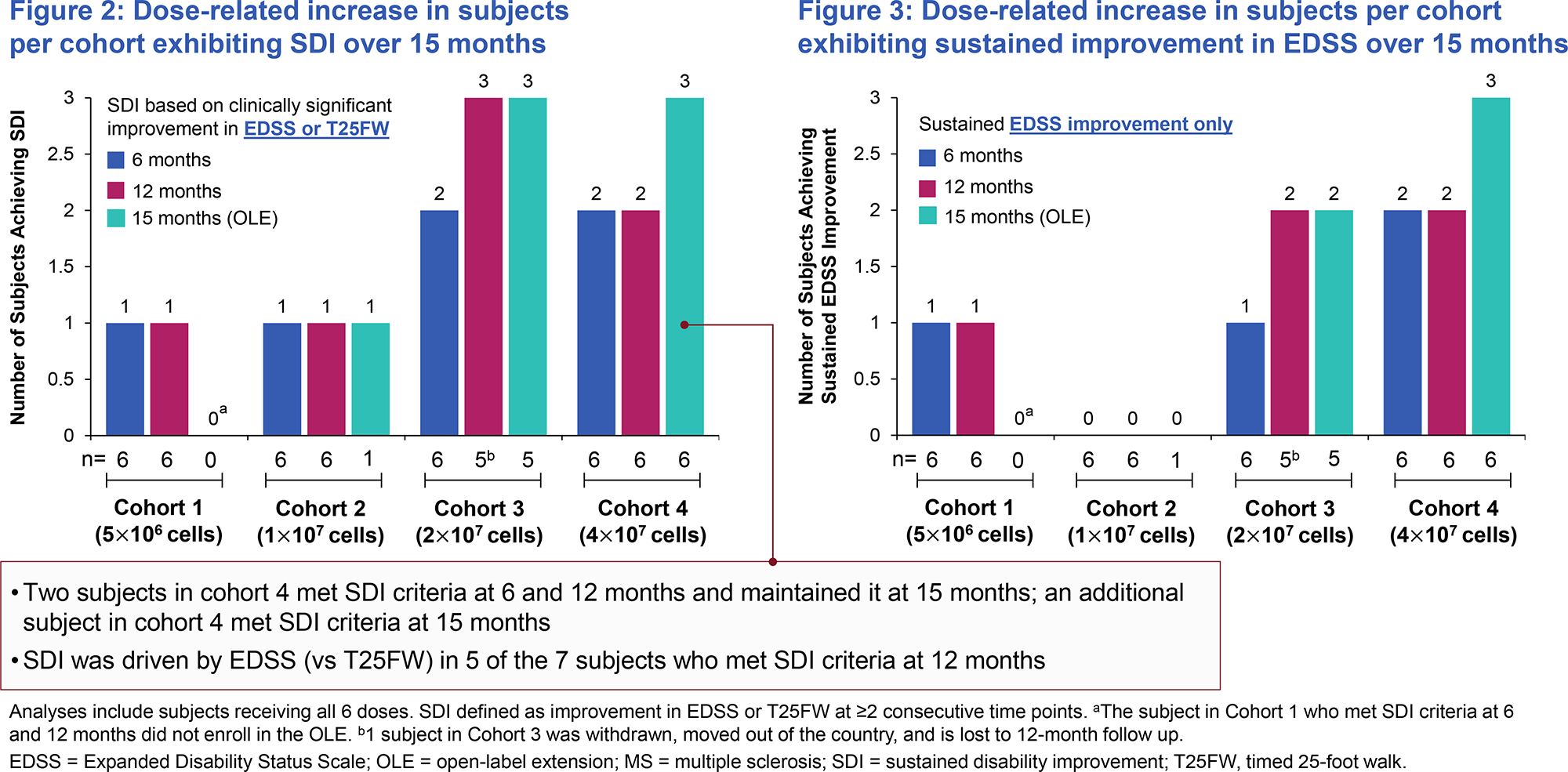
The long-term reported therapeutic efficacy of ATA188 has been confirmed to correlate directly with increasing doses of the drug.

Based on the results, Atara has selected dose cohort 3 for study in part 2 of the clinical trial. It is possible that participants from maximum dose cohort 4 will subsequently be included, as soon as their 12-month data are available.
The safety profile of ATA188 is characterized by the absence of dose-limiting toxicity and fatal adverse reactions. All adverse events associated with therapy were mild to moderate in severity. Although one patient experienced a severe adverse reaction leading to withdrawal from the clinical trial, it occurred against the background of ongoing symptoms of upper respiratory tract infection and possible dental infection. Runny nose was the only adverse reaction reported in more than one subject.
ATA188 had no clinically significant effect on cytokine production, including no cytokine release syndrome.
ATA188 Clinical Trial in Multiple Sclerosis: Data Update #1 [August 2020]
Atara, which continues to collect clinical data on ATA188, has found evidence that increased doses of the experimental drug are reflected by a higher proportion of patients showing sustained improvement in disability status.

Among those who responded to the treatment, such improvements stemmed primarily from lower EDSS scores: over time, therapeutic efficacy is translated into improved T25FW and 9-HPT scores.
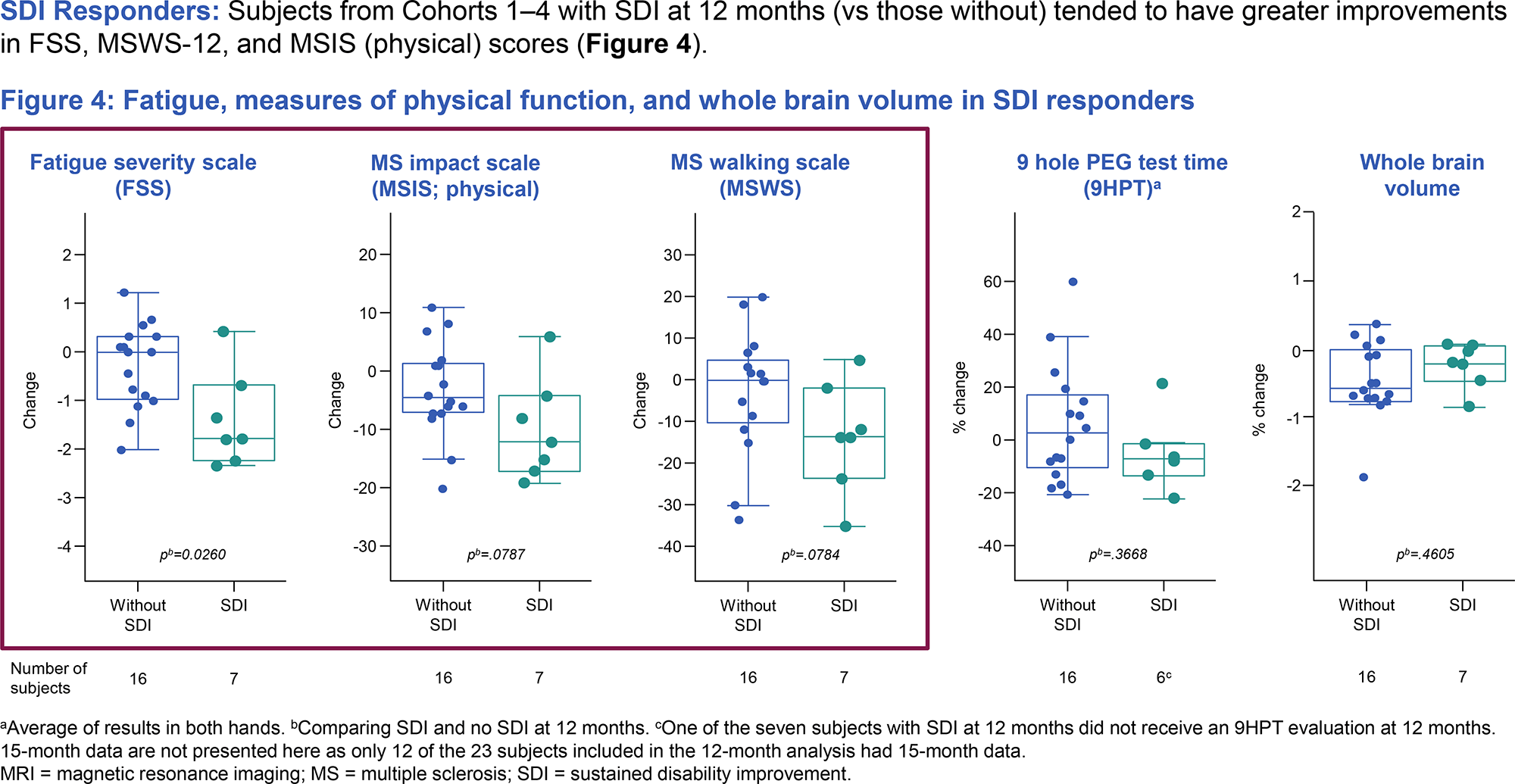
There have been favorable trends toward improved scores on the FSS, MSIS-29, and MSWS-12.

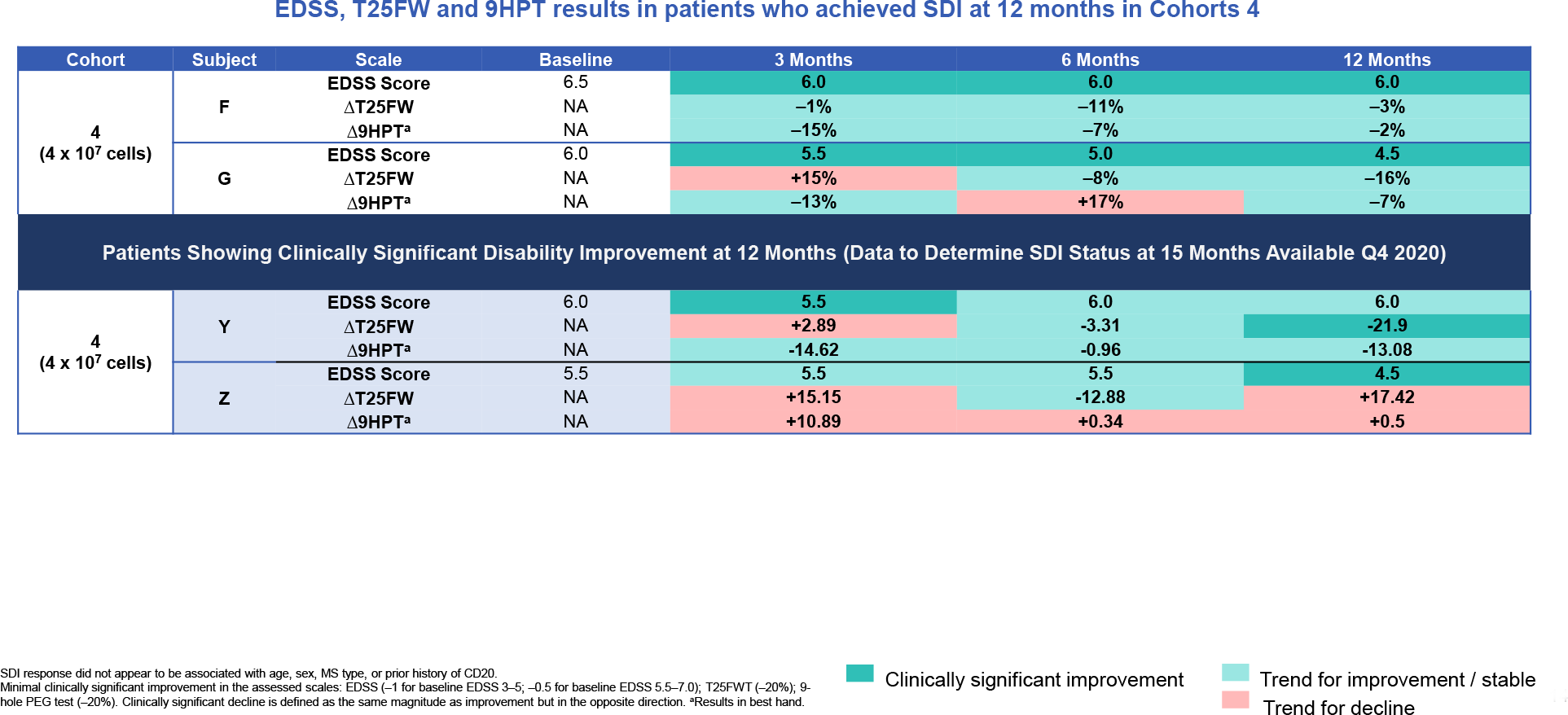
Data from an even longer follow-up of 6 patients revealed the following:
- 3 patients (out of those who reached SDI after 6 and 12 months) maintained it after 15 months
- 1 patient reached SDI after 24 months
- 1 patient remained in SDI between 6 and 18 months.

The conclusions made by Atara are as follows:
- Accumulated clinical trial data from ATA188 confirmed the safety of such an experimental treatment for progressive forms of multiple sclerosis.
- The efficacy of the therapy directly correlates with increasing doses of the drug.
- Patients who have demonstrated sustained improvement in disability status after 12 months are characterized by improvements in measures of fatigue, physical function, and mobility when compared to those patients who have not achieved the specified SDI.
- If a patient is locked into SDI at any particular time point in therapy, he or she remains in SDI.
- Despite the clinical successes of ATA188, experimental therapy for progressive forms of multiple sclerosis still needs to be more thoroughly evaluated in a larger number of patients.
ATA188 Clinical Trial in Multiple sclerosis: Data Update #2 [October 2020]
Further follow-up of the patients proved that a higher dose of ATA188 was of decisive therapeutic importance. Thus, exit to SDI in the two high-dose cohorts (cohorts 3 and 4) was true for 42% (n=5/12) and 50% (n=6/12) of participants after 12 and 15 months, respectively.
Part 2 of the clinical trial initially focused on dose cohort 3 but after cohort 4 (the highest dose) showed similar or even better treatment outcomes the decision was made to switch all participants to it.
ATA188 Clinical Trial in Multiple sclerosis: Data Update #3 [August 2021]
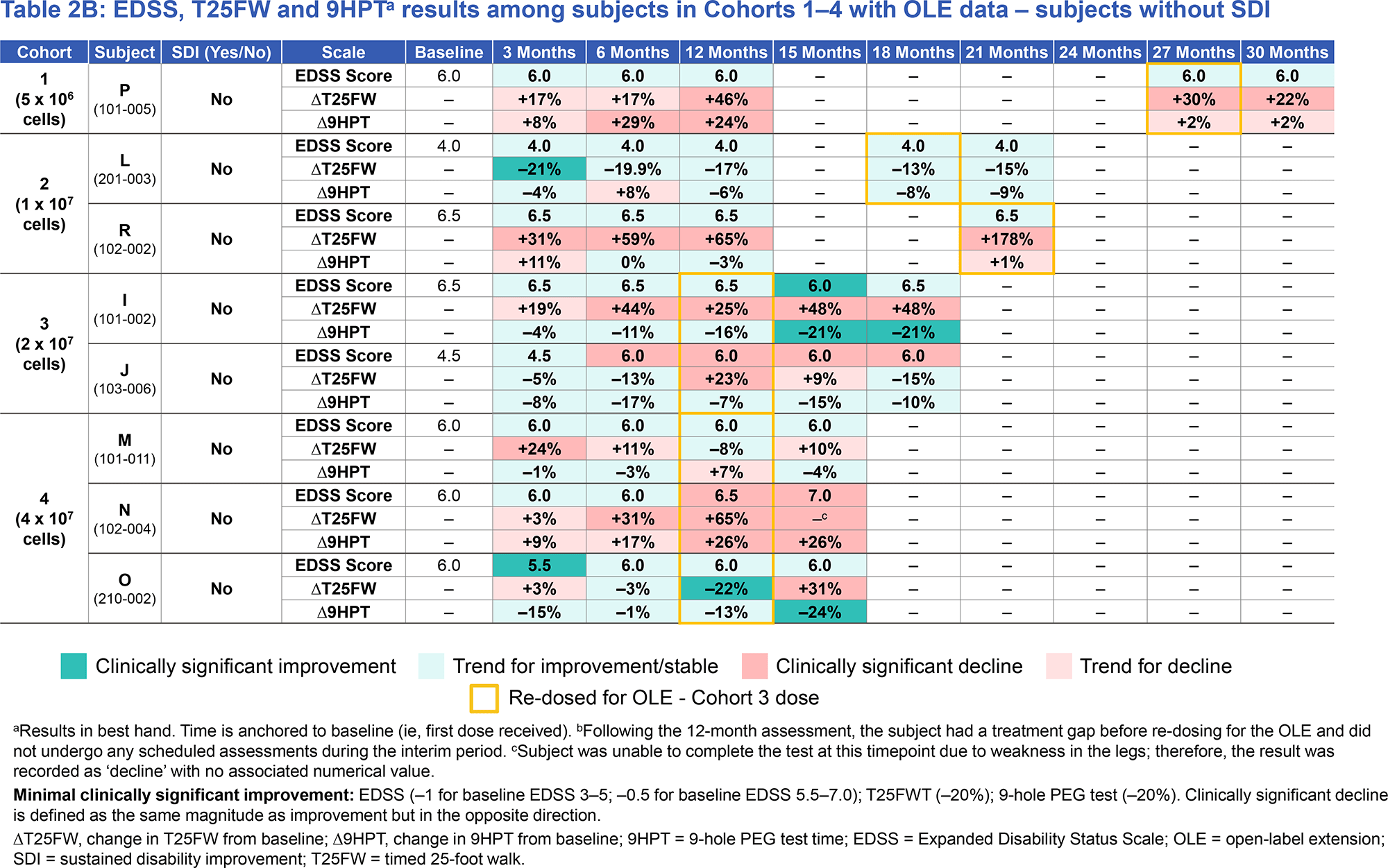
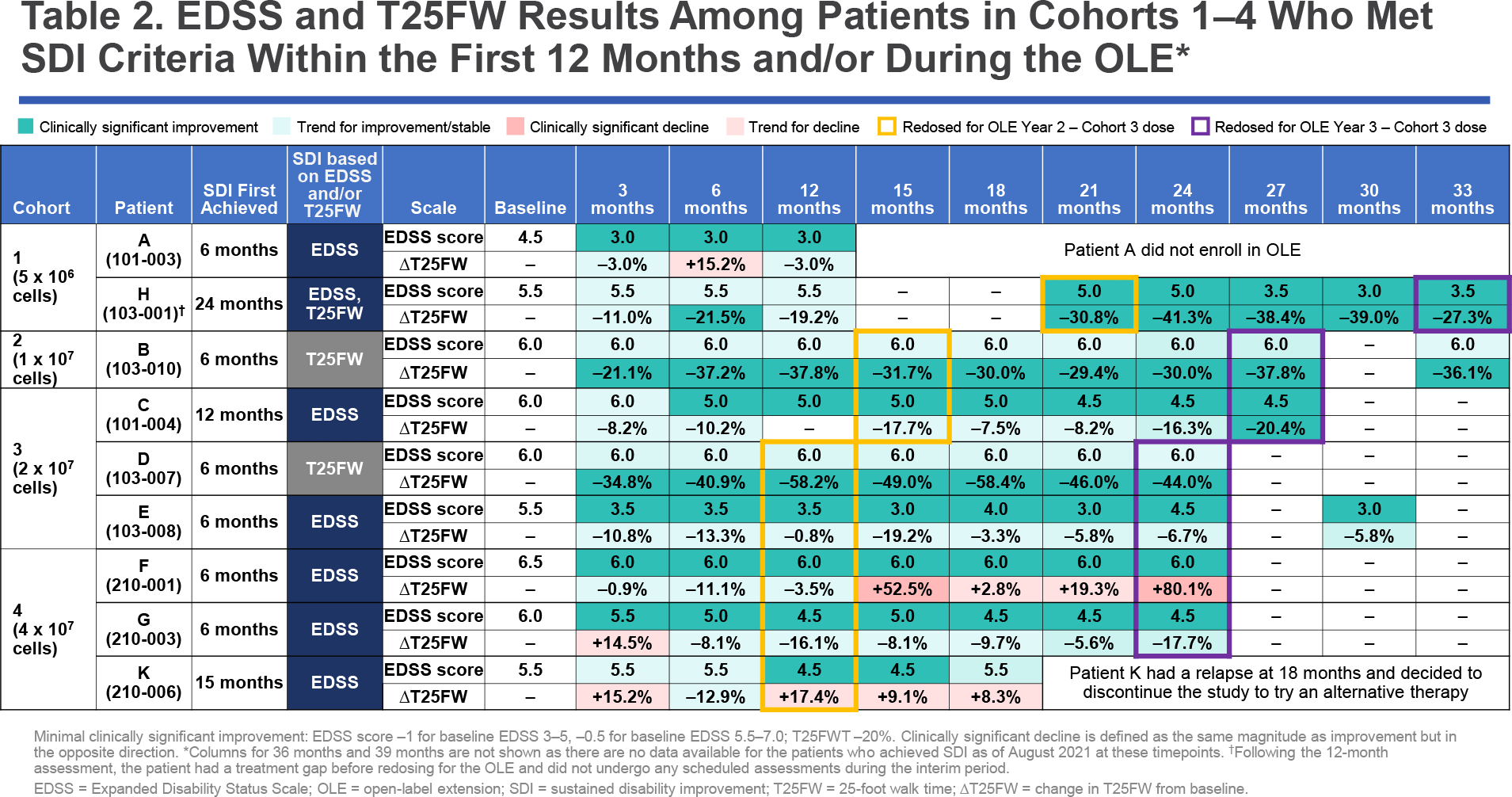
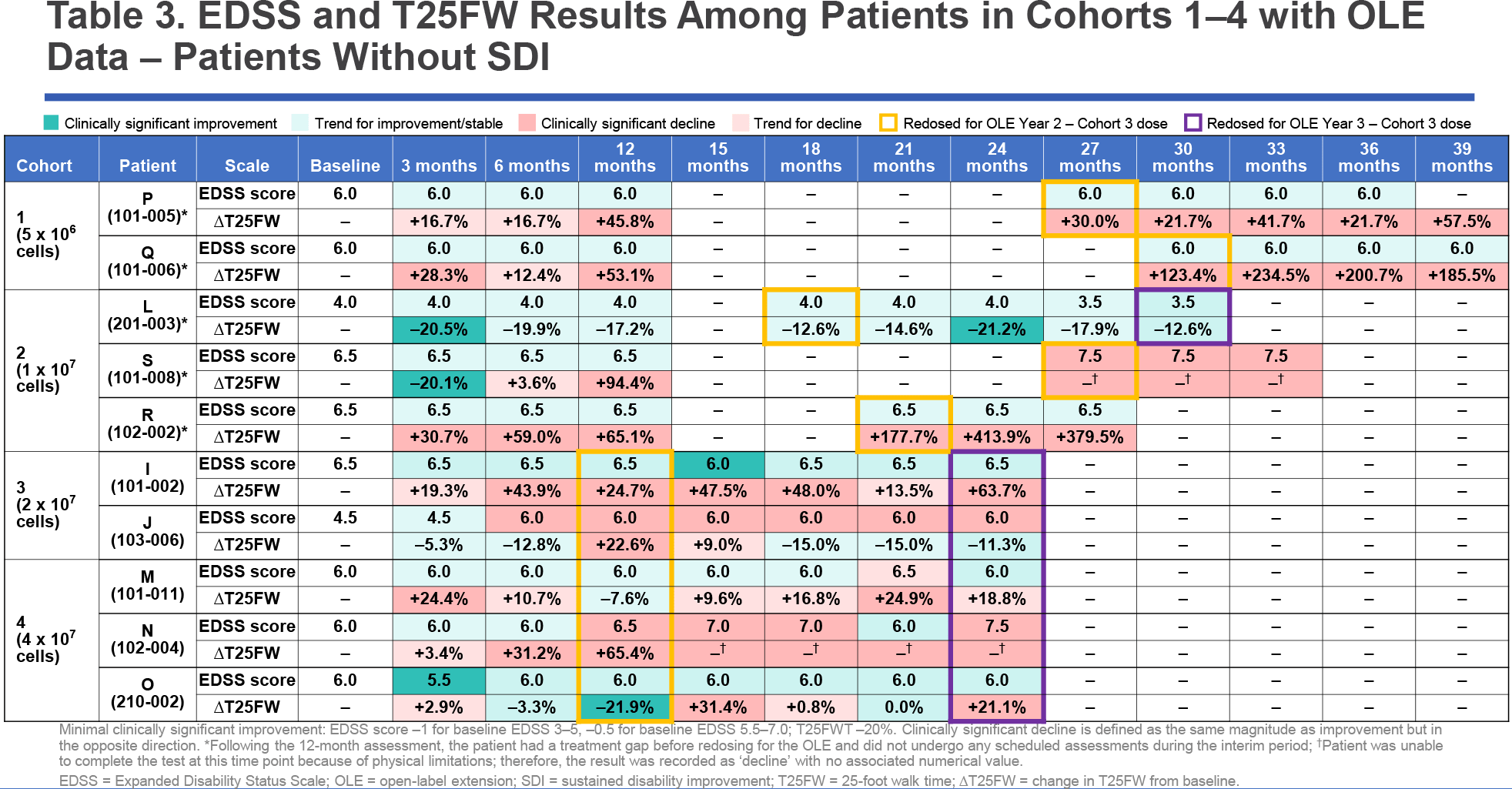
Updated results of ATA188 treatment of progressive forms of multiple sclerosis among patients followed up to 39 months have led to the following conclusions.
First, the majority of patients who achieved SDI at any time point maintained this status at follow-up. The exit to SDI was usually due to sustained improvement in the EDSS score.
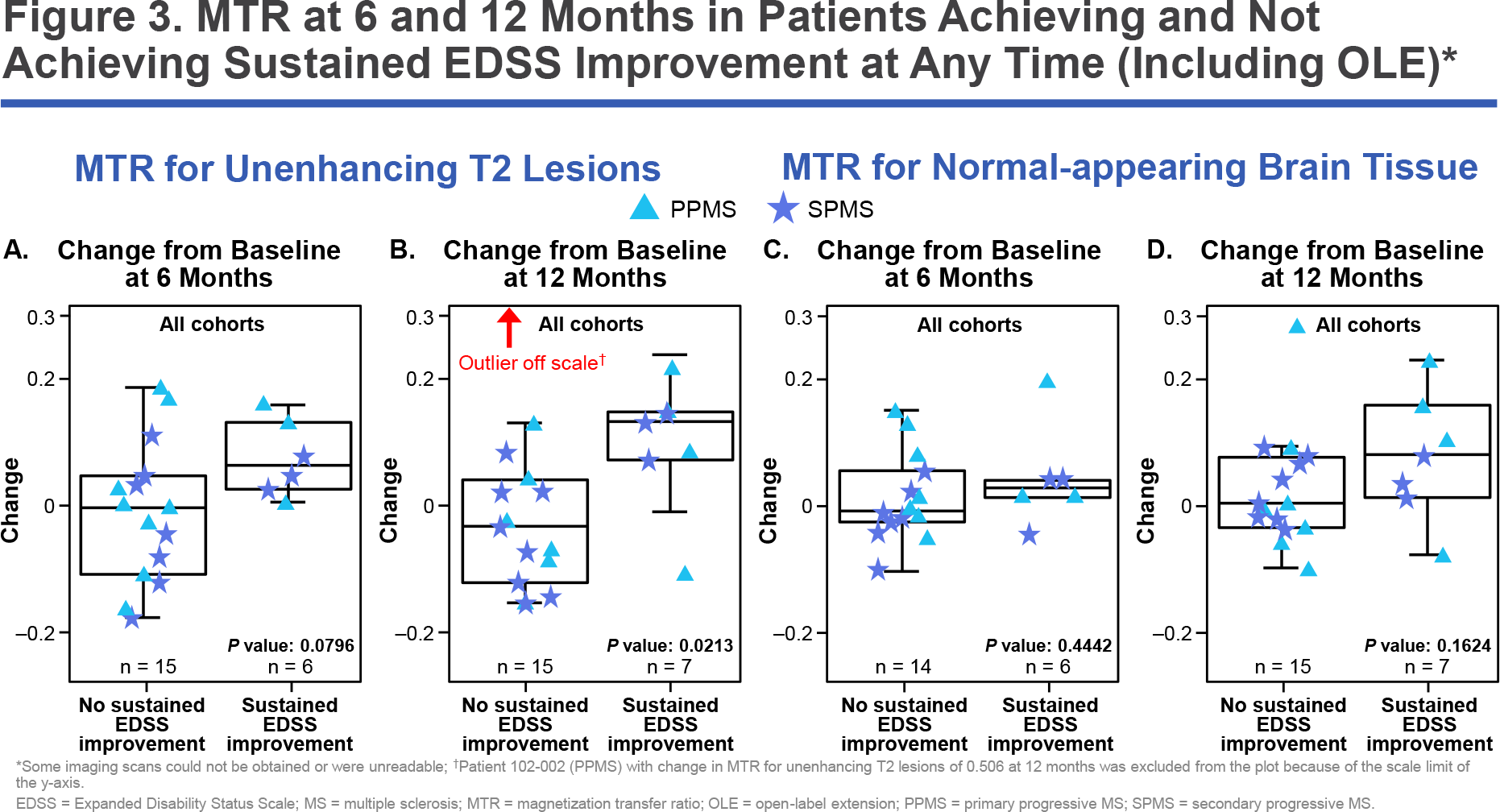
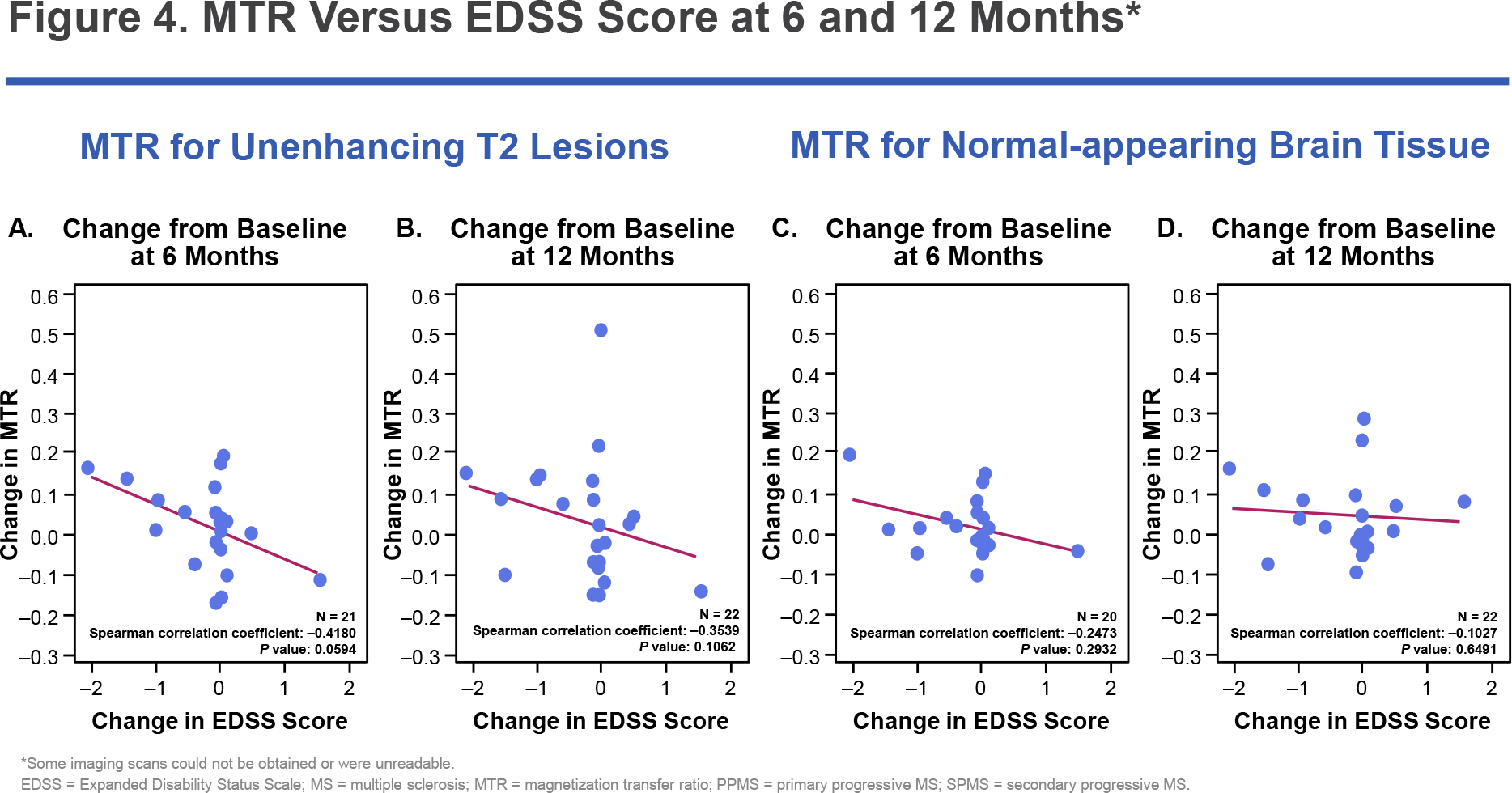
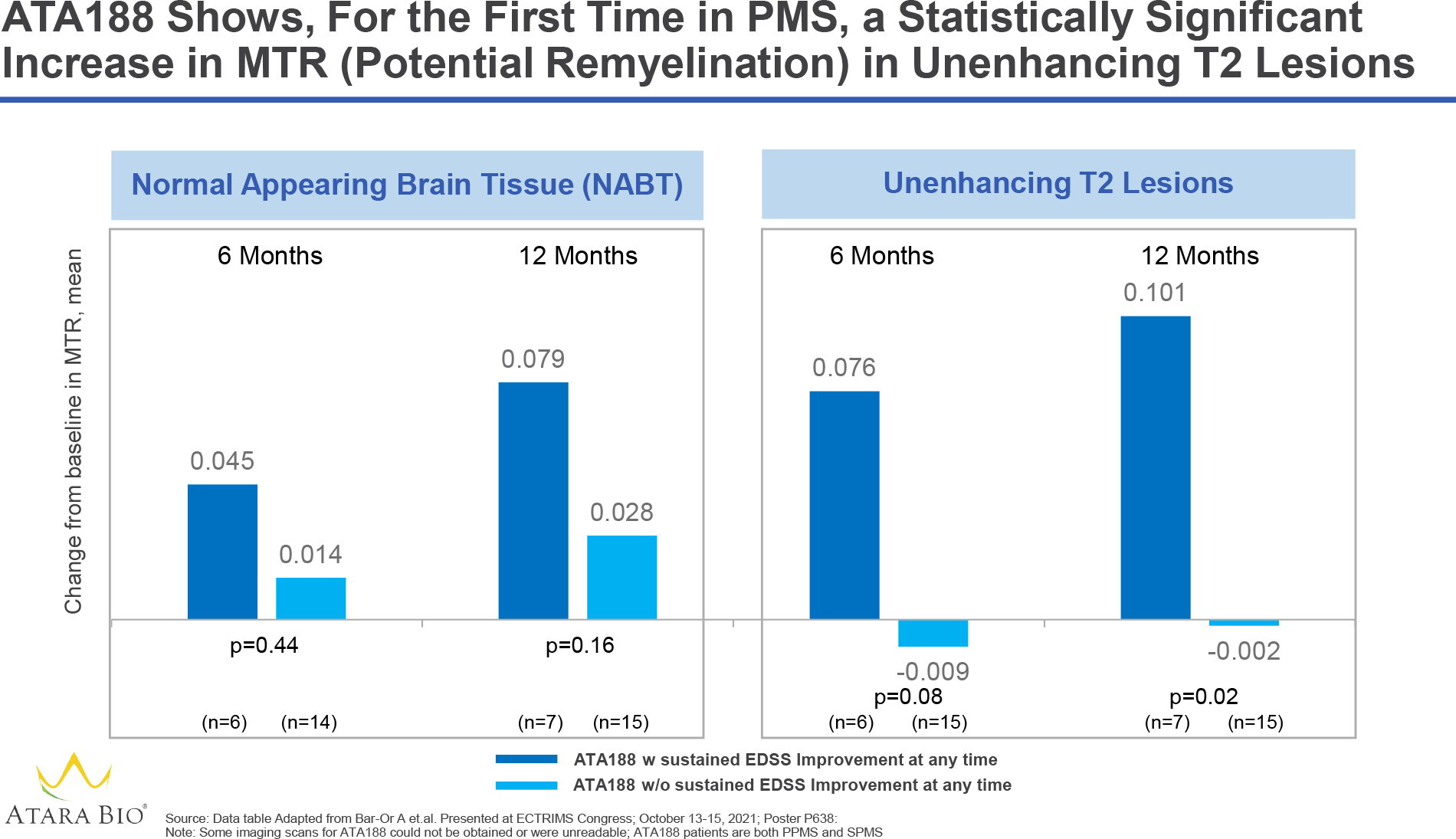
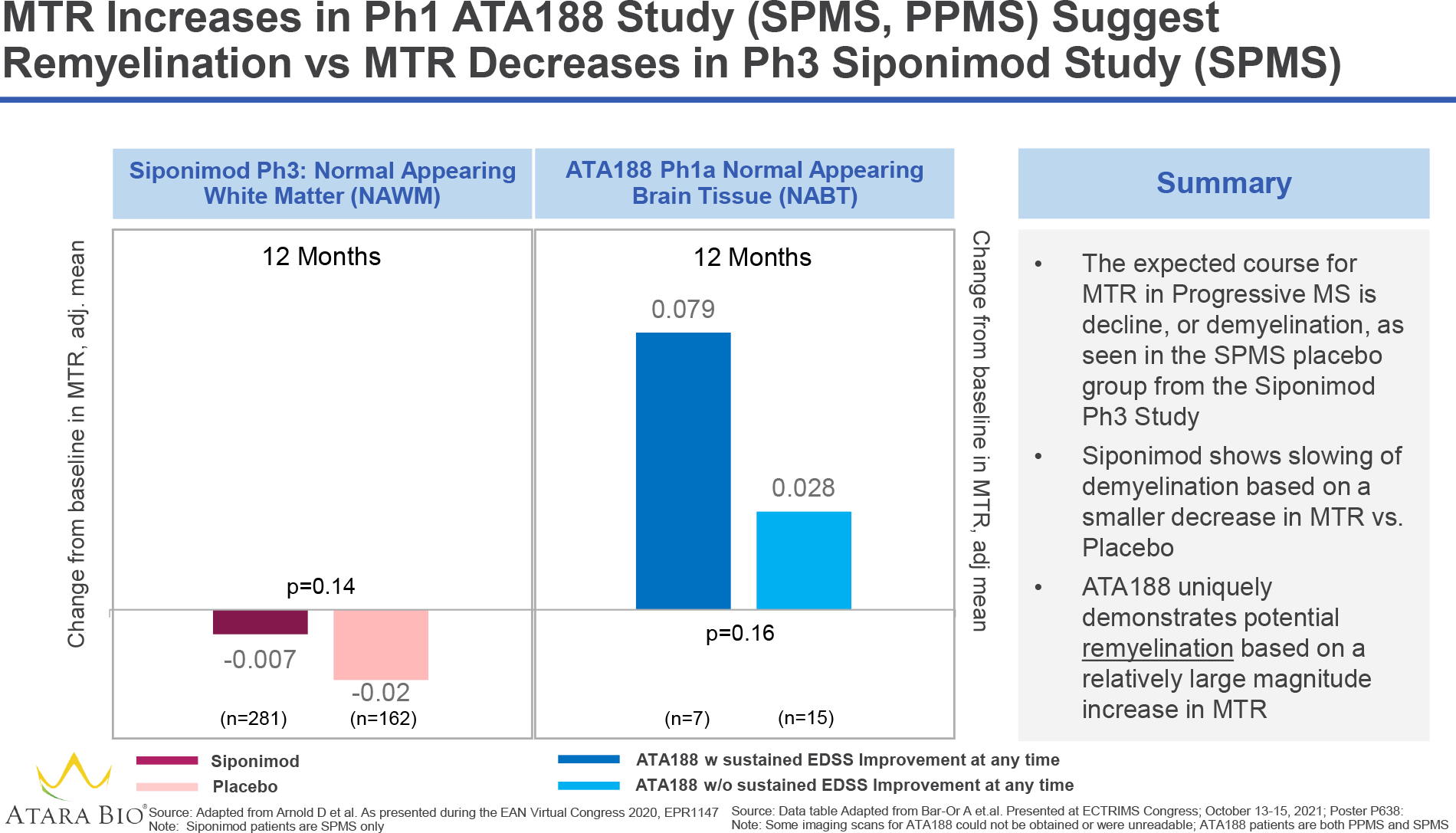
Second, there is evidence of possible remyelination. Thus, patients with a sustained improvement in EDSS score showed a greater (compared to those with no apparent improvement in EDSS score) increase in magnetization transfer ratio (MTR) as a key biomarker of myelination status. In other words, structural changes in brain tissue indicative of remyelination may well be the very driving force that is beneficially shown by the attenuation of the degree of disability in progressive multiple sclerosis.
Third, patients showed a steady improvement in their EDSS score as treatment progressed, suggesting that not only does the progression of multiple sclerosis slow down, but the disease is reversed.
Fourth, no major safety or tolerability issues with ATA188 have been identified.
Be that as it may, despite the encouraging results of experimental treatment of progressive forms of multiple sclerosis, they need to be confirmed in a randomized placebo-controlled clinical trial. Atara is doing just that: relevant interim data from part 2 of the EMBOLD study will be available in the first half of 2022.
Atara has planned two pivotal phase 3 clinical trials that will study ATA188 in two patient populations: those with non-active secondary progressive multiple sclerosis (SPMS) and those with non-active primary progressive multiple sclerosis (PPMS). There is no approved therapy for the first population and one of very poor efficacy for the second.
More Than Hope
Although the development of multiple sclerosis is probably driven by more than one causative factor, the Epstein–Barr virus is the only risk factor known to date that is mandatory for the manifestation of the disease. It has been proven that 100% of multiple sclerosis patients have been exposed to EBV. Moreover, EBV-infected cells, especially memory B cells, which have become immortal due to viral infection, are believed to play a critical role in the immune cascade responsible for relapsing and progressive forms of multiple sclerosis. The success of current pharmacotherapy, which depletes the pool of all peripheral B cells, once again demonstrates the key position of these cells in the pathophysiology of multiple sclerosis. It is shown that continuation of experiments with ATA188, a cytotoxic T-cell therapy selectively targeted against EBV-infected B cells and plasma cells both circulating in the body and persisting in the central nervous system, is warranted for multiple sclerosis therapy.
Some observations are that the efficacy of ATA188 in improving disability status seems to depend on the baseline EDSS score: the more advanced the disease, the less (or slower) the curative power of the treatment appears. Still, even a one-point improvement in the EDSS score is remarkable. For instance, if a patient originally walked with a cane, he was able to walk on his own after ATA188 therapy.

Clinical trials of the autologous ATA190, which Atara abandoned due to manufacturing difficulties, at their time pointed to the fact that in patients with severe neurological disability (baseline EDSS score of 8.0) irreversible axonal degeneration and neuronal loss limit therapeutic options for improvement, even if autoimmune attacks on the central nervous system are prevented by EBV-specific T-cell therapy. Nevertheless, even in such advanced patients, treatment has had a favorable effect on general condition, physical and cognitive ability, and physiologically, including bladder function, visual acuity, and spasticity.
Available pharmaceutical drugs can only mildly hold back the deterioration of progressive multiple sclerosis, they cannot stop or reverse the disease. If ATA188 does achieve this in a strictly controlled part 2 clinical trial, an evolution in the treatment paradigm for progressive and other forms of multiple sclerosis awaits us.
Multiple Sclerosis and Epstein–Barr Virus
Genetic and environmental factors are thought to contribute to the risk of multiple sclerosis, a chronic inflammatory demyelinating disease of the central nervous system that causes progressive disability. Over the past four decades, a growing body of evidence has emerged that Epstein–Barr virus plays a significant role in the development of multiple sclerosis. The assumption is supported by a number of independent research reports indicating a widespread presence of the infection in patients and high titers of serum antibodies against EBV both during the clinical course of multiple sclerosis and before its manifestation.

Epstein–Barr virus (EBV), also known as Human gammaherpesvirus 4 and Human herpesvirus 4 (HHV-4), is unique in many ways. In order to colonize the body, it infects B lymphocytes, activates and promotes their clonal proliferation, and then persists as a latent infection in memory B cells carrying the phenotype of resting cells throughout the human life span. The virus, switching from a latent (dormant) to a lytic (replicative) form through modulation of its nuclear genes, latent membrane proteins (LMP) 1, 2A and 2B, and the viral precursor protein BZLF1 (ZEBRA), reactivates in plasma cells and tonsil epithelial cells, make its own transmission to other organisms through saliva and genital secretions.
Although approximately 95% of the world’s adult population is infected with this DNA double-stranded gammaherpesvirus, the number of EBV-infected cells in the body is kept under strict immune control, including by EBV-specific CD8+ cytotoxic T lymphocytes that destroy proliferating and lytic-infected cells.
In some cases, the immunological surveillance of EBV is weakened, which is manifested by the development of various diseases. Epstein–Barr virus is known to cause infectious mononucleosis. It is associated with certain cancers, including Hodgkin’s lymphoma, Burkitt’s lymphoma, gastric cancer, and nasopharyngeal carcinoma. Epstein–Barr virus has been linked to childhood disorders like Alice in Wonderland syndrome and acute cerebellar ataxia. It is thought to increase the risks of autoimmune pathologies, including dermatomyositis, systemic lupus erythematosus, rheumatoid arthritis, and Sjögren’s syndrome.
Regarding multiple sclerosis, in susceptible hosts, EBV infection is thought to confer infected autoreactive B cells an abnormal ability to survive and proliferate. Such latently infected cells accumulate in the lymphoid structures and target organs affected by the disease. In the case of the brain, this leads to a constant production of autoantibodies that attack and damage oligodendrocytes, myelin, and neurons.
Atara’s analysis of autopsy brain samples from multiple sclerosis patients and healthy individuals (without neurological disease) revealed that, despite signs of Epstein–Barr virus infection in both groups, EBV-positive immune cells are more common and densely populate the brains of specifically multiple sclerosis patients.
Atara’s experts who turned to immunohistochemistry, in situ hybridization, optical microscopy, and semi-quantitative analysis studied autopsy brain biopsy specimens from multiple sclerosis patients (n=17) and healthy individuals (n=9). The presence of LMP-1 was detected in 93% of biopsy specimens from the multiple sclerosis group and 78% of controls, while the former showed a significantly higher presence of CD138+ plasma cells and LMP-1-enriched cell populations.
Remarkably, 78% of chronic brain lesion areas in multiple sclerosis and only 33.3% of healthy brain samples contained CD138+ plasma cells in the parenchyma, where they should not be. It is possible that EBV infection is responsible for the extravasation of the latter from the cerebral vascular network endowing the inflammatory process with permanence.
The BZLF1 protein was found in 46% and 44% of the tissues, respectively, whereas in the case of biopsy specimens with multiple sclerosis it was found predominantly in association with areas of chronic brain damage. BZLF1 is thought to be able to inhibit the production of interleukin 2 (IL-2) and interleukin 6 (IL-6). In addition to its involvement in B cell maturation, IL-6 is important for the neuro- and genesis of oligodendroglia under normal conditions and after injury.
In addition, 85% of brain samples from multiple sclerosis patients showed a much more prominent presence of EBV-encoded small RNA-1 (EBER1) immune cells than in biopsy specimens from healthy individuals.
Further Evidence
Antiviral therapy for multiple sclerosis is professed by the Swiss-French GeNeuro with its experimental temelimab. According to one hypothesis, some viruses can give rise to the development of multiple sclerosis.
For instance, the multiple sclerosis–associated retrovirus (MSRV), which belongs to the pathogenic W-family of human endogenous viruses (pHERV-W), can be transactivated by external factors such as Human herpesvirus 6 (HHV-6) or Epstein–Barr virus. This results in the generation of the pathogenic envelope protein MSRV-Env which, by over-activating the endogenous toll-like receptor 4 (TLR4), triggers the pro-inflammatory cascade and suppression of remyelination.
Temelimab (GNbAC1) is a recombinant humanized monoclonal antibody that selectively targets the extracellular domain of MSRV-Env to neutralize it.
Extras
Atara Biotherapeutics. Investor presentation. January 10, 2022. [PDF]
Atara Biotherapeutics. ECTRIMS. Corporate presentation. October 13, 2021. [PDF]
Phase I study of ATA188, an off-the-shelf, allogeneic Epstein–Barr virus-targeted T-cell immunotherapy for progressive forms of multiple sclerosis. [PDF]
Atara Biotherapeutics. Investor presentation. March 1, 2021. [PDF]
Corporate and ATA188 data update. September 11, 2020. [PDF]
ATA 188 data update. May 26, 2020. [PDF]
Epstein–Barr virus in multiple sclerosis: theory and emerging immunotherapies. Trends Mol Med. 2020 Mar;26(3):296-310. [source]
Molecular signature of Epstein–Barr virus infection in MS brain lesions. Neurol Neuroimmunol Neuroinflamm. 2018 Jun 7;5(4):e466. [source]