Highlights
TG Therapeutics has disclosed the results of two pivotal clinical trials evaluated experimental ublituximab in the therapy of relapsing forms of multiple sclerosis.
It was more than successful, and TG intends to send the Biologics License Application (BLA) for ublituximab to regulators in the third quarter of 2021.
- In mid-December 2021, the U.S. Food and Drug Administration (FDA) accepted the BLA for ublituximab. The regulator’s decision will be issued by the end of September 2022.
- At the end of May 2022, it became known that the FDA postponed the deadline for the BLA for ublituximab. The regulator will make its decision by the end of December 2022.
Commercial launch of ublituximab is expected in late 2022 or early 2023.
The drug will most likely be named Ublyxi. Ublituximab, however, can be labeled by other names: Ublixi, Ublyx, or just Ubli.
Ublyxi, if approved, would directly compete with two already existing highly effective disease-modifying therapy (DMT) for multiple sclerosis, Ocrevus (ocrelizumab) and Kesimpta (ofatumumab), promoted by Roche and Novartis, because it has a similar mechanism of action and similar efficacy.

Kesimpta: Highly Effective New Drug for Multiple Sclerosis
Ofatumumab by Novartis is as good and convenient as Ocrevus by Roche against multiple sclerosis.
Ublyxi: Multiple Sclerosis Treatment Efficacy
The ULTIMATE I (NCT03277261) and ULTIMATE II (NCT03277248) phase 3 (randomized, double-blind, active-controlled, multicenter, international) clinical trials, identical in design, examined ublituximab in the therapy of relapsing forms of multiple sclerosis in adult (18–55 years) patients (n=1094).
Among the main inclusion criteria for the trials were:
- Disease in active form (relapsing-remitting multiple sclerosis or active secondary progressive multiple sclerosis).
- Extended Disability Status Scale (EDSS) score between 0 to 5.5.
- Either at least 1 relapse in 1 year before the screening, or at least 2 relapses in 2 years before the screening, or presence of brain inflammation on gadolinium-enhanced T1-weighted MRI images in 1 year before the screening.
A comparison was performed with Aubagio (teriflunomide), a DMT by Sanofi.
Intravenous ublituximab (450 mg) was administered once every 6 months (after two loading doses, 150 mg on day 1 and 450 mg on day 15). Oral teriflunomide was administered daily (14 mg).
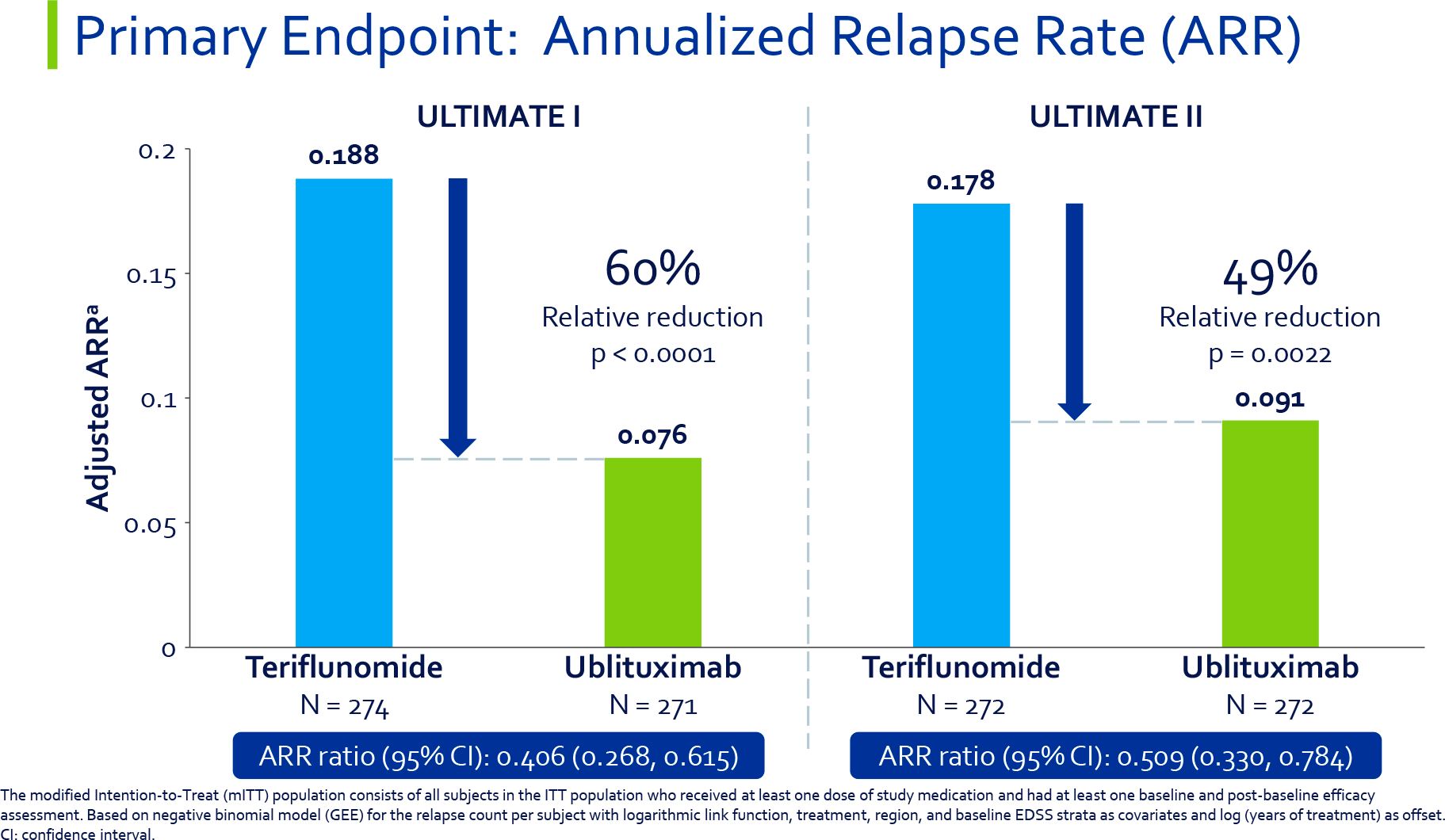
After 96 weeks of treatment, the ublituximab groups statistically significantly outperformed the teriflunomide groups on the primary endpoint, defined by the annualized relapse rate (ARR).
Among those receiving ublituximab, the ARR was 0.076 and 0.091 — compared with 0.188 and 0.178 among those prescribed Aubagio. The hazard ratio (HR) between the groups was 0.406 (95%: 0.268–0.615) and 0.509 (95%: 0.330–0.784), equivalent to a relative risk reduction of 60% (p<0.0001) and 49% (p=0.0022) for relapse of multiple sclerosis supported by ublituximab.
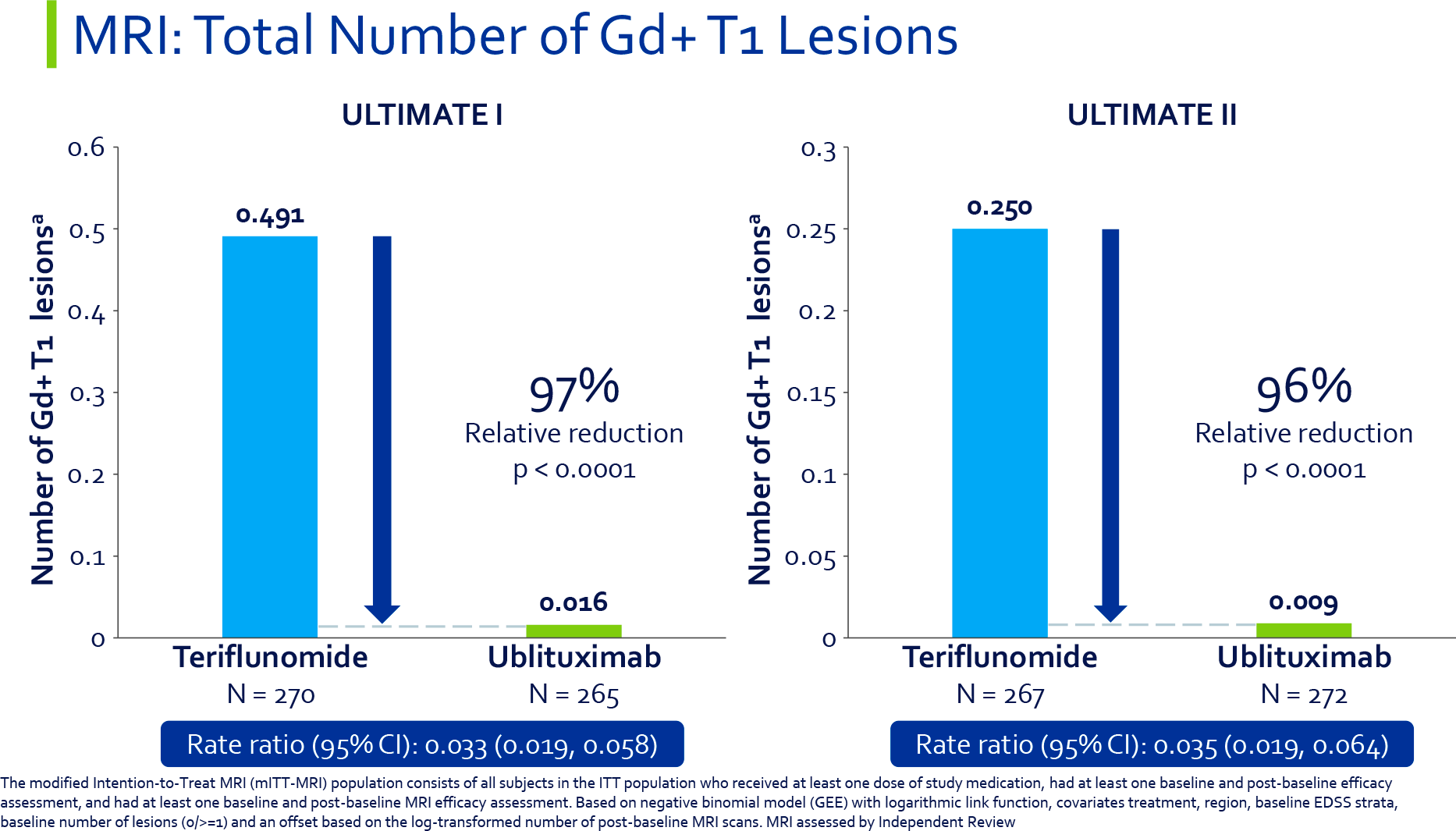
The ublituximab groups recorded 97% and 96% elimination of brain lesions on gadolinium-enhanced T1-weighted MRI images (they reflect the presence of an active inflammatory process) — relative to teriflunomide (p<0.0001).
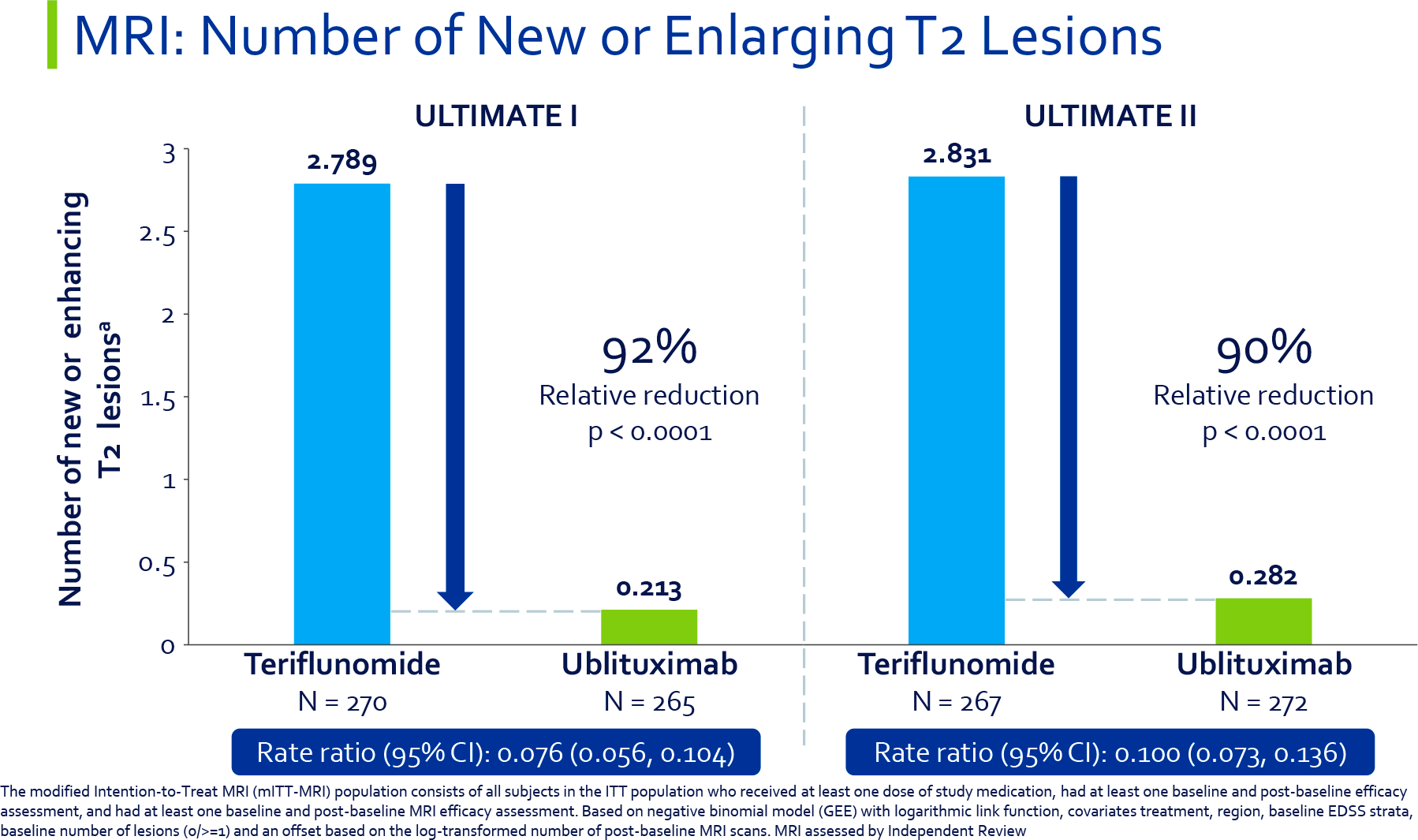
Ublituximab reduced the number of new or increasing brain lesions on T2-weighted MRI images (these are indicative of demyelination) by a relative 92% and 90% (p<0.0001).
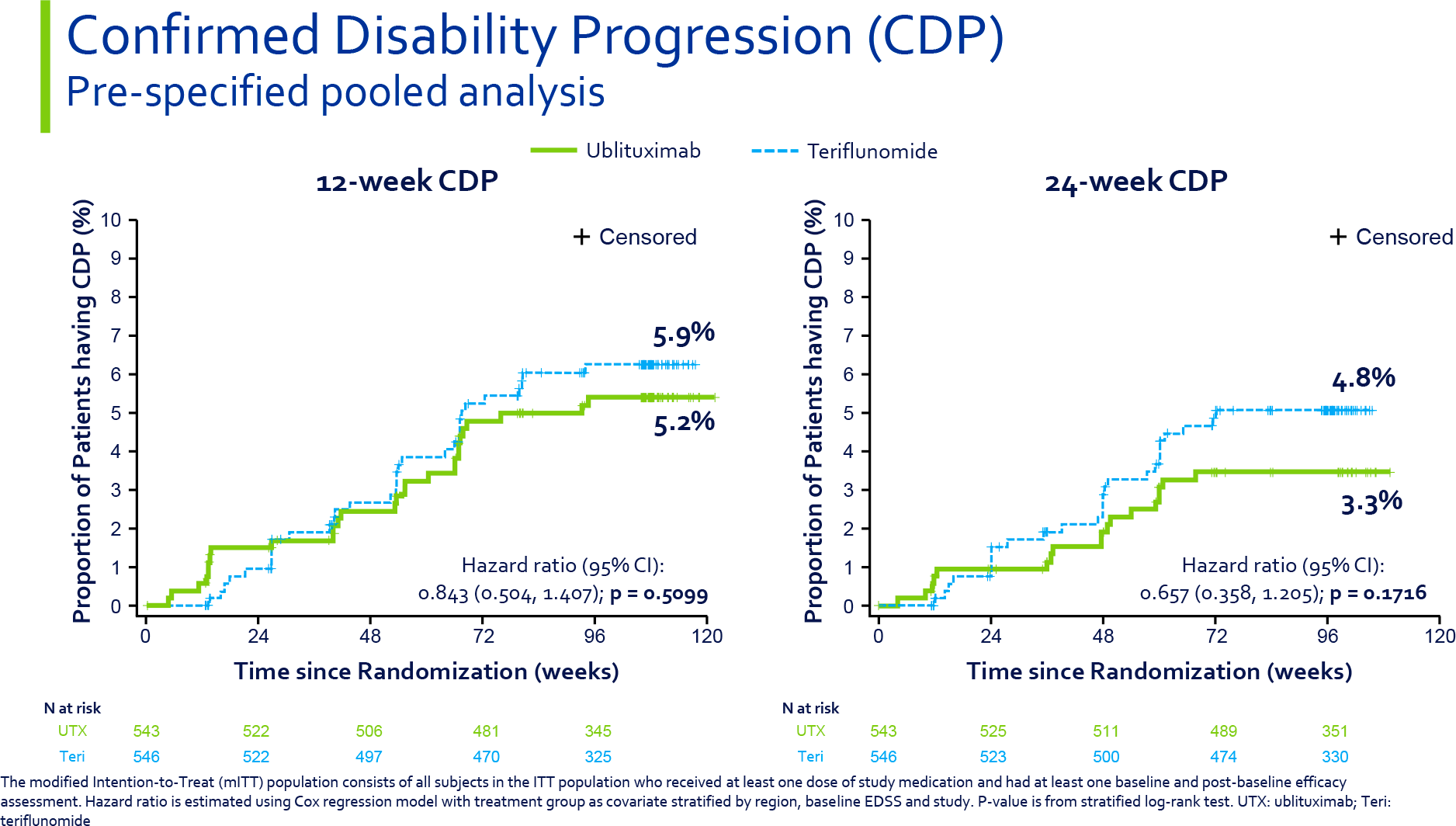
In the ublituximab groups, a smaller proportion of patients than in the teriflunomide groups experienced confirmed disability progression (CDP), which was defined as a ≥1.5, ≥1, or ≥0.5 point increase in EDSS score (respectively among those subjects whose baseline EDSS score was 0, 1–5, or ≥5.5 points) that persisted for 3 months (3mCDP) and 6 months (6mCDP) of treatment. However, there was no statistically significant difference with Aubagio (p=0.5099 and p=0.1716).
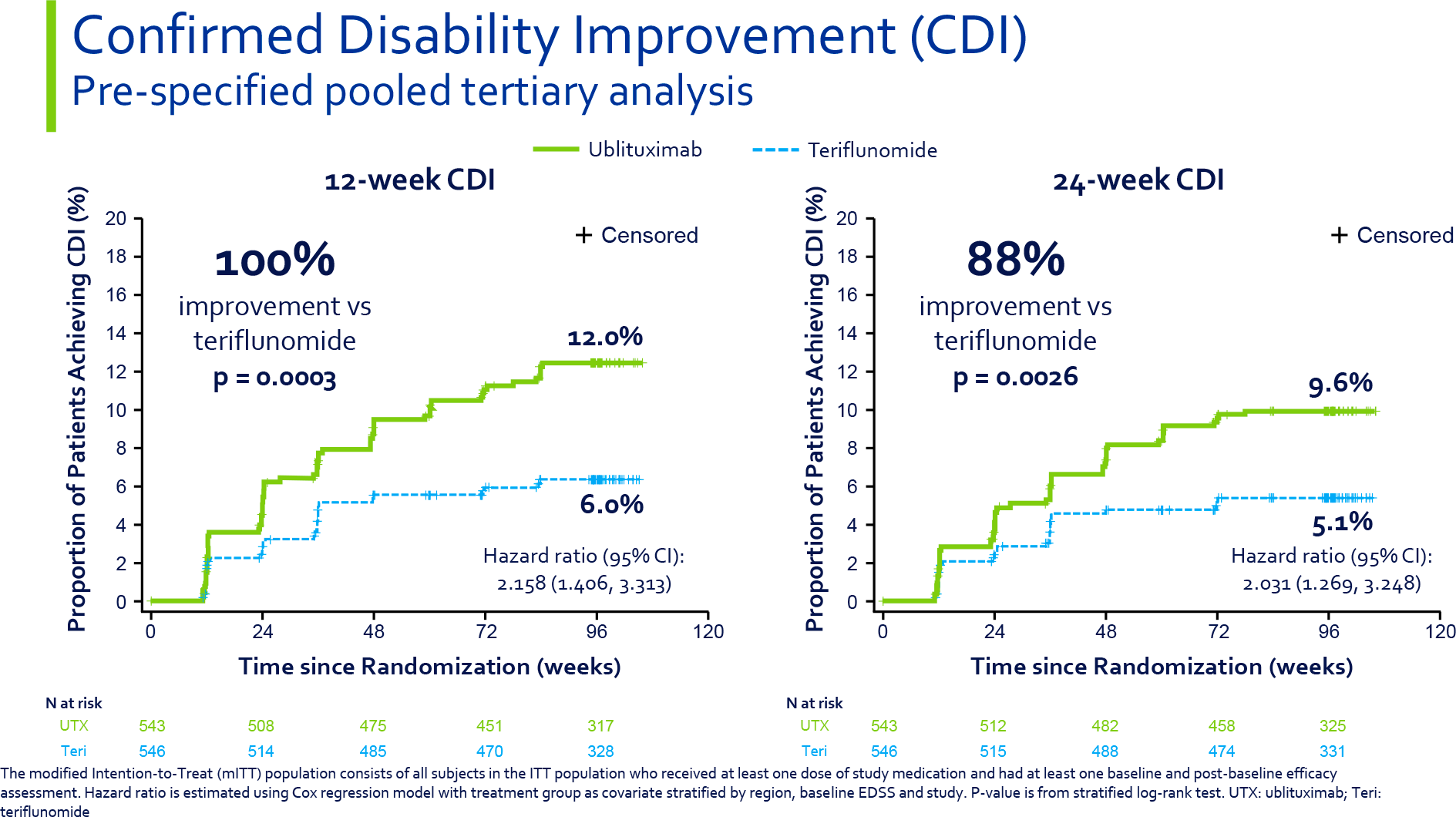
But ublituximab statistically significantly doubled the odds of patients’ exit to confirmed disability improvement (CDI) declared by a decrease in EDSS score, which persisted for 3 months (3mCDI) and 6 months (6mCDI) of therapy. Thus, this was true for 12.0% and 9.6% of subjects treated with ublituximab — versus 6.0% and 5.1% of participants treated with teriflunomide (p=0.0003 and p=0.0026).
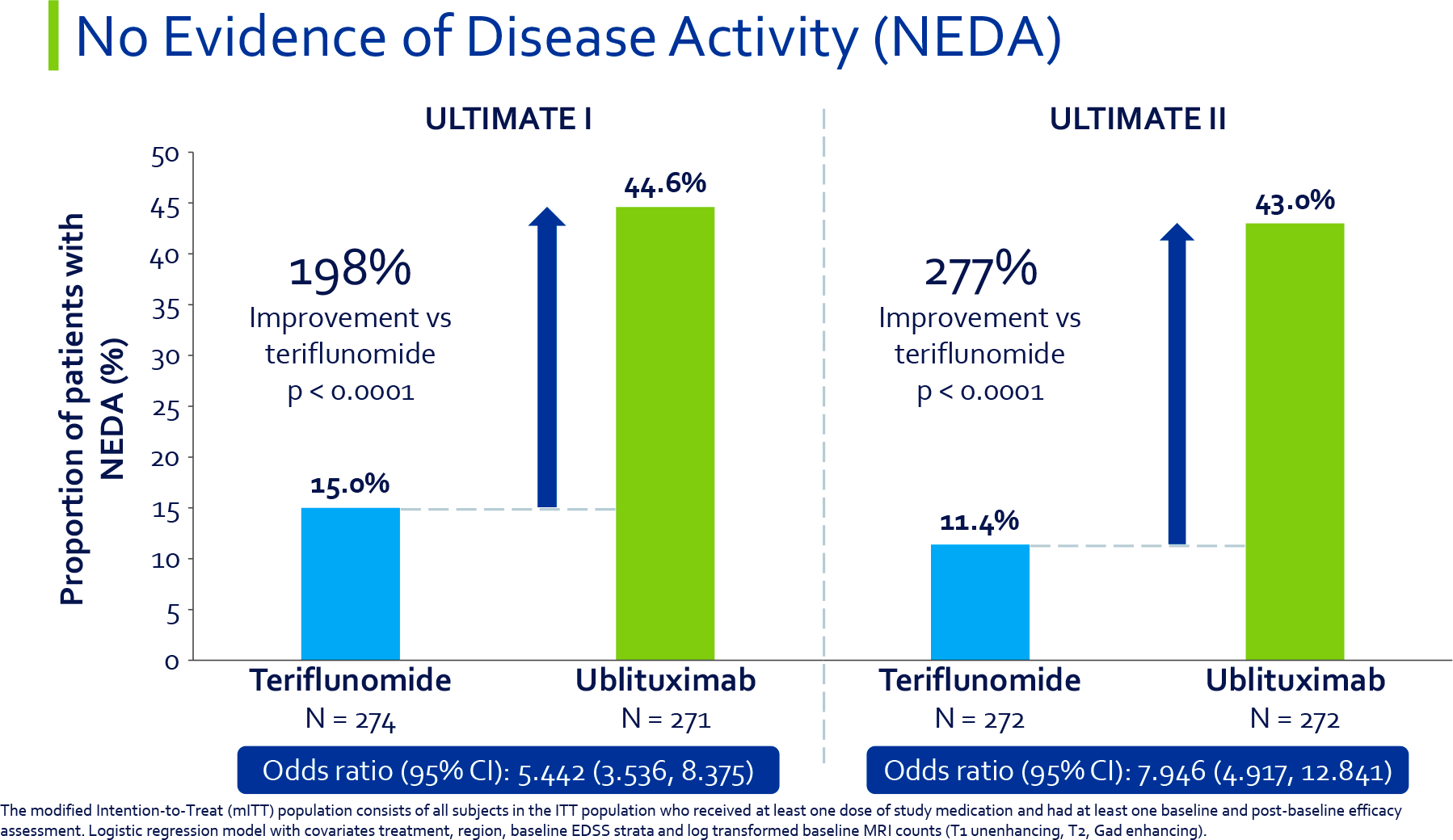
The no evidence of disease activity (NEDA) status, taken between weeks 24 and 96 of therapy, reached 44.6% and 43.0% of patients in the ublituximab groups — vs. 15.0% and 11.4% in the teriflunomide groups (p<0.0001).
- NEDA status was defined as no 6mCDP and no recurrence of multiple sclerosis confirmed clinically or on MRI images (no new or enlarging T2 lesions in the brain, no new T1 lesions in the brain).
Ublyxi: Multiple Sclerosis Treatment Safety
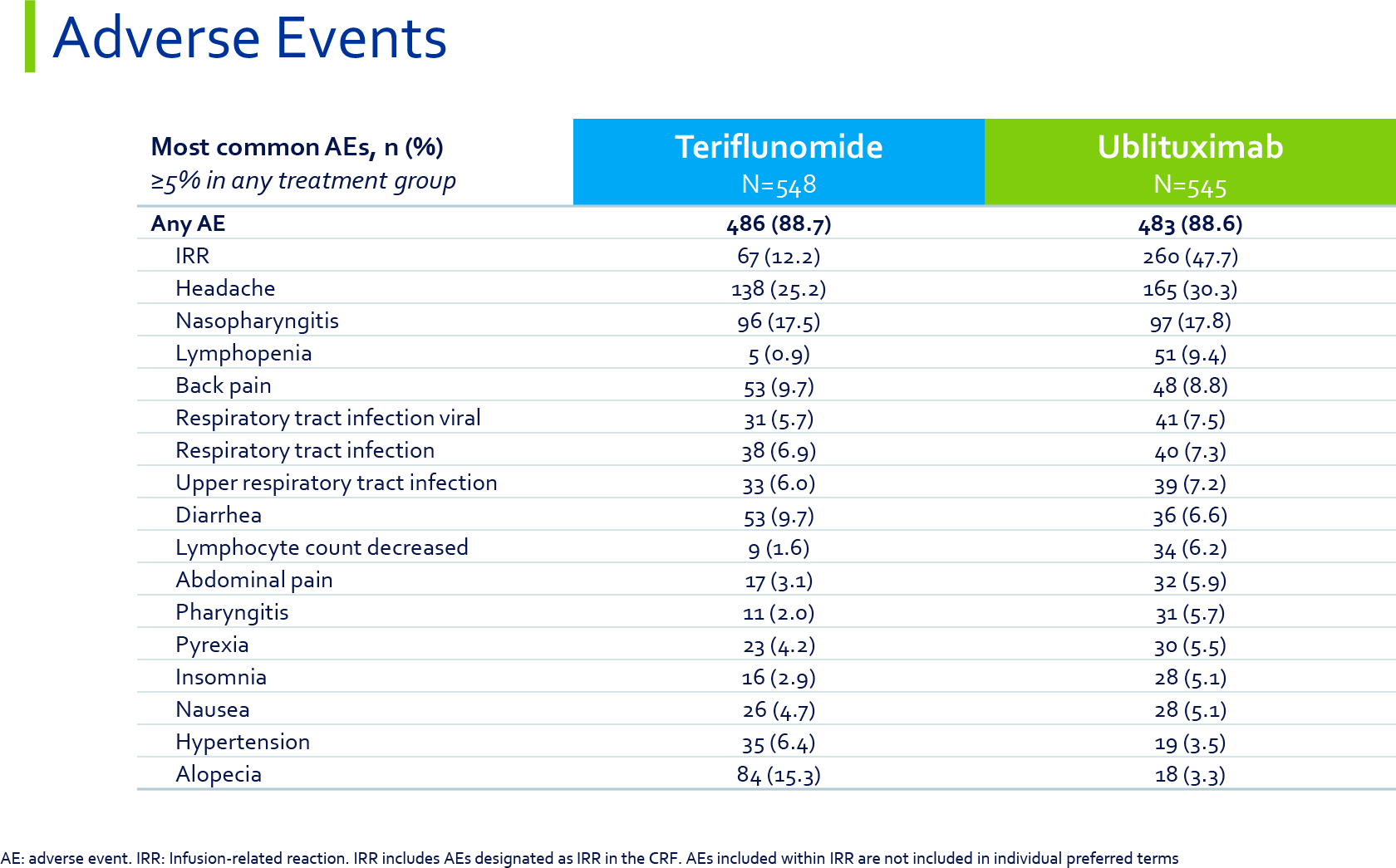
Ublituximab had an acceptable safety profile: The incidence of adverse events was comparable to that of Aubagio, in 88.6% of patients versus 88.7%.
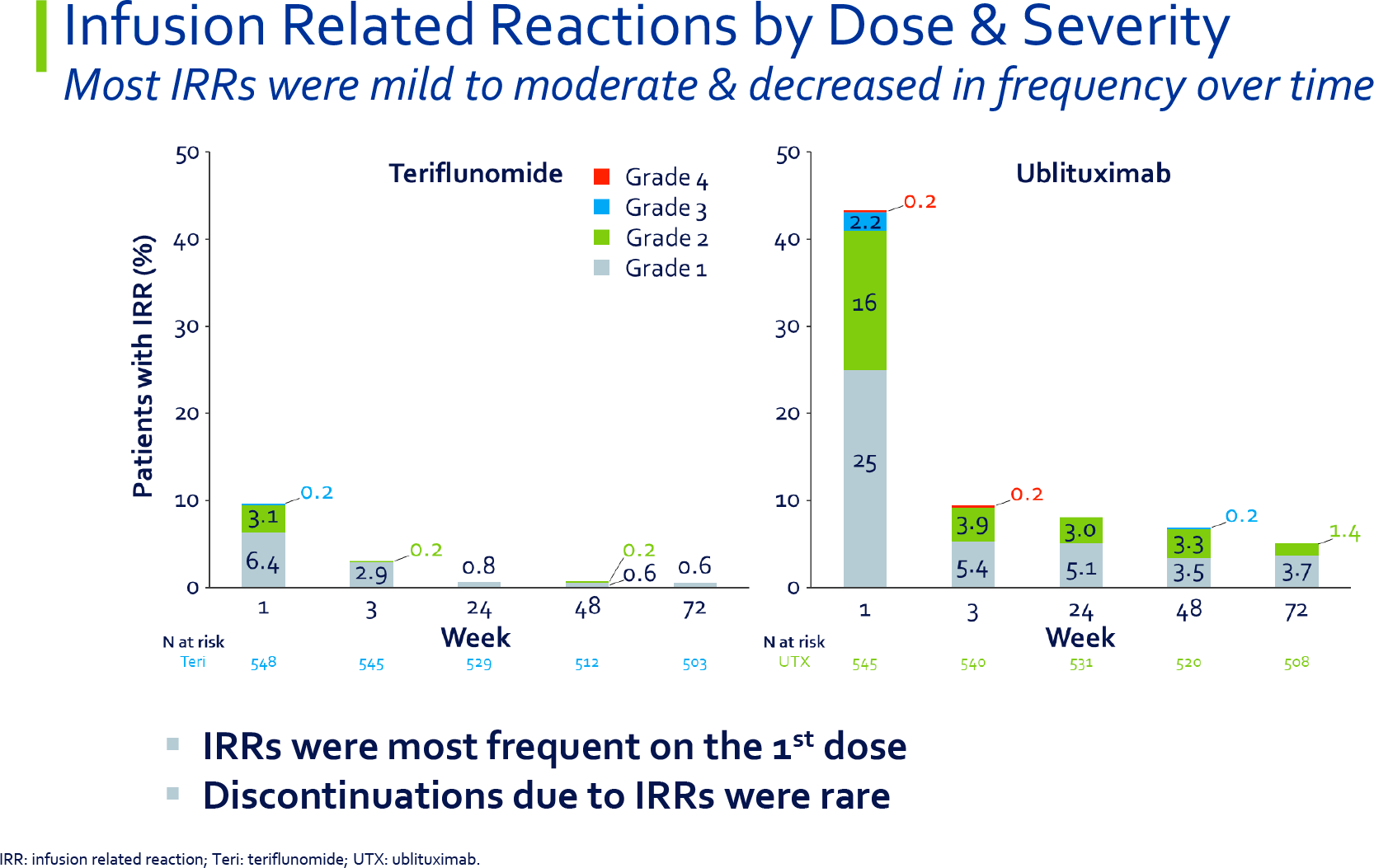
Most often (48% of cases) patients experienced adverse local reactions to ublituximab administration, such as itching, rash, urticaria, erythema, bronchospasm, flushes, etc. In general, they were mild-to-moderate in severity and occurred mostly only after the first infusion of the drug; with subsequent infusions of ublituximab, their frequency decreased sharply.
Other adverse events to ublituximab included headache (in 30% of subjects), nasopharyngitis (18%), lymphopenia (9%), back pain (9%), viral respiratory tract infections (8%), respiratory tract infections (7%), upper respiratory tract infections (7%), diarrhea (7%), lymphopenia (6%), abdominal pain (6%), pharyngitis (6%), pyrexia (6%), insomnia (5%), and nausea (5%).
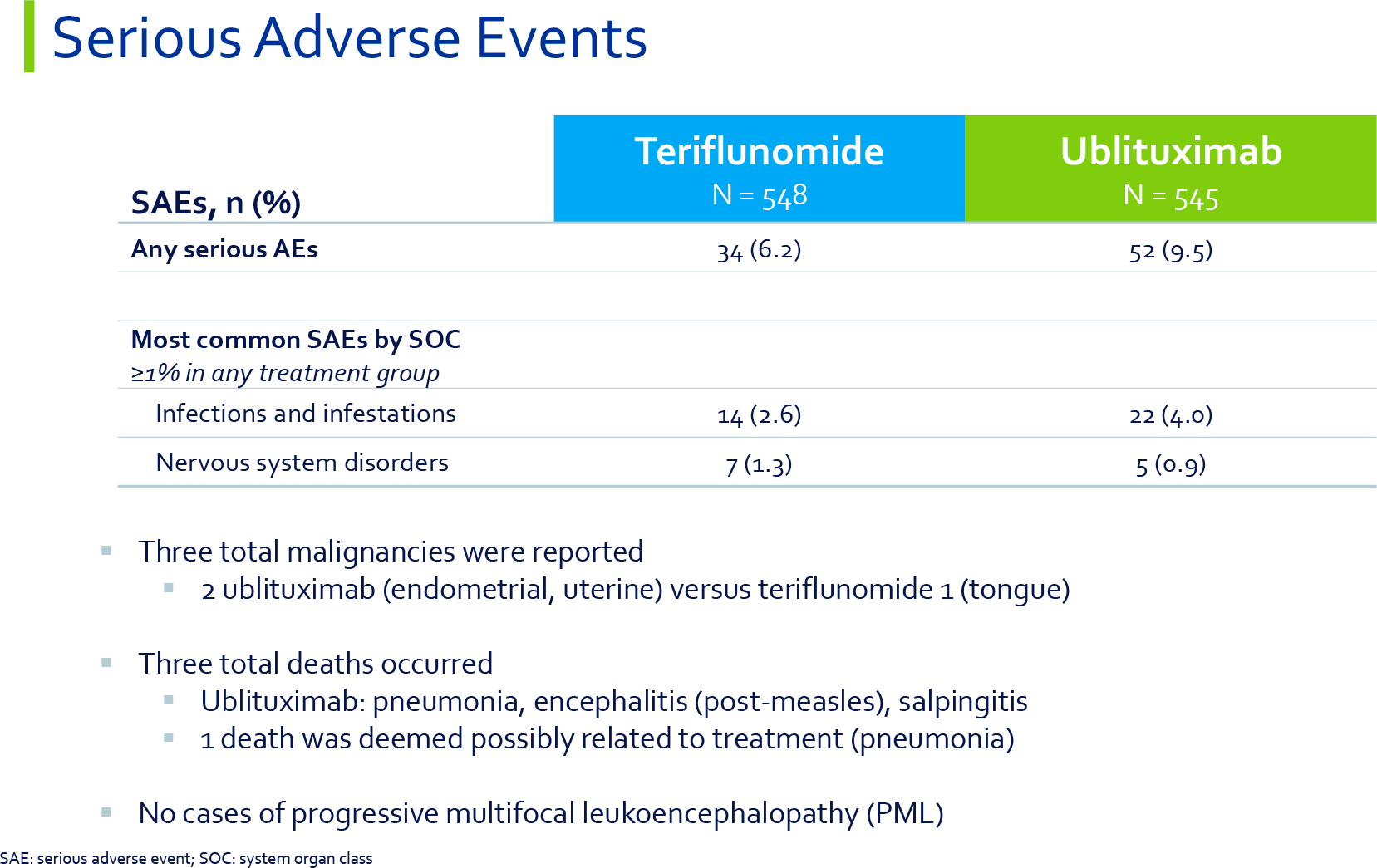
Serious adverse events were reported in 9.5% of patients treated with ublituximab and the most common were infections and infestations (4.0%), and nervous system disorders (0.9%). Two cases of malignancies (endometrial cancer, uterine cancer) and three deaths were recorded, one of which was attributed to treatment (pneumonia). There were no cases of progressive multifocal leukoencephalopathy (PML).
Ublyxi: Mechanism of Action of Ublituximab in Multiple Sclerosis
Ublituximab is a chimeric monoclonal IgG1 antibody targeting a specific epitope of the CD20 surface antigen that is expressed on B cells at all stages of development (except the first and last).
Ublituximab binds to CD20 thereby activating the immune system that carries out B cell lysis via complement-dependent cytotoxicity (CDC), antibody-dependent cell-mediated cytotoxicity (ADCC), and phagocytosis. The resulting depletion of the B-cell pool has an appropriate therapeutic effect in multiple sclerosis.
The molecule (LFB-R603), developed by LFB Biotechnologies (France) and originally targeted at the treatment of chronic lymphocytic leukemia (CLL), belongs to the third generation of drugs in this class. In early March 2012, TG acquired a worldwide license for ublituximab.
Thanks to a modified glycosylation scheme due to the crystallizing fragment (Fc) with low fucose content, increased affinity to all Fc-gamma receptor IIIA (FcγRIIIA, CD16a) variants is realized. As a result of enhanced binding to the latter on effector cells such as macrophages, T helpers, and natural killer (NK) cells, ublituximab is characterized by multiply enhanced ADCC directly affecting B lymphocytes depletion. Such engineering solves one of the problems of monoclonal antibodies when they have insufficient therapeutic efficacy despite their high specificity to target cells. This is true for ublituximab in comparison with other CD20-targeted drugs already approved for multiple sclerosis therapy such as Ocrevus (ocrelizumab) by Roche and Kesimpta (ofatumumab) by Novartis.
For example, in vitro on donor cells from healthy people and patients with CLL, ublituximab demonstrated 100 times more NK-mediated ADCC activity than rituximab. In vitro, ocrelizumab showed two to five times greater ADCC activity against CD20-expressing cells compared to rituximab.
Ublyxi vs. Ocrevus and Kesimpta
Overall, barring minor differences, the therapeutic efficacy and safety of ublituximab are identical in comparison to those of ocrelizumab and ofatumumab.
TG desperately needs marketing leverage to challenge the Swiss colossuses Roche and Novartis. Ublituximab will be promoted among doctors and patients pedaling, obviously, the following positions.
- Ublituximab provided a greater reduction in the annualized relapse rate (ARR) of multiple sclerosis. In absolute numbers, ublituximab reduced the ARR to 0.076–0.091 after 2 years of its administration. Ocrevus reduced this rate to 0.155–0.156 and Kesimpta reduced it to 0.10–0.11.
- Ublituximab was more successful than Ocrevus and Kesimpta in controlling the confirmed disability progression (CDP) in multiple sclerosis. Thus, 3mCDP and 6mCDP statuses were fair for 5.2% and 3.3% of patients who adhered to treatment with ublituximab. More patients, 9.8% and 7.6%, reached the indicated statuses in Ocrevus clinical trials. The Kesimpta trials presented 3mCDP and 6mCDP to an even higher proportion of patients, 10.9% and 8.1%.
- Ublituximab is administered once every 6 months intravenously in a maintenance regimen, with infusions lasting 1 hour. Ocrevus, similarly administered once semiannually, is infused for 3.5 to 4 hours, or 2 hours if the patient has had no serious adverse reactions to prior infusions of the drug.
- Ublituximab and ocrelizumab require premedication to reduce the risk of adverse reactions to infusions of the drug: Patients receive an oral antihistamine and corticosteroid 30 minutes before administration of the former; patients receive an oral antihistamine and paracetamol and an intravenous corticosteroid 30 minutes before administration of the latter. Kesimpta, marketed as an autoinjector for subcutaneous injections, is used by patients themselves once a month; premedication is not necessary.
- TG has repeatedly said that it intends to make ublituximab more affordable than Ocrevus. This is understandable; since ublituximab is effective at lower doses than ocrelizumab (450 mg versus 600 mg), its cost is lower. Right now, a year’s course of maintenance therapy for multiple sclerosis with Ocrevus costs American patients $75,000, and Kesimpta costs $95,000.
If we set aside TG’s understandable desire to highlight its drug in a favorable light, the picture does not look so rosy. Yes, in the first couple of years of therapy, ublituximab did indeed reduce ARR more than the competitors’ anti-CD20 drugs did. But TG reported nothing about the change in ARR during follow-up treatment. Ocrevus is known to have continued to lower the ARR to 0.103, 0.080, 0.065, 0.044, and 0.040 after 3, 4, 5, 6, and 7 years of treatment, respectively, over the course of its continued use. However, the fact that ublituximab does a better job than other anti-CD20 drugs at the beginning of treatment in controlling relapses of multiple sclerosis suggests that it will be beneficial in delaying the worsening of disability later on.
Ublituximab was more effective in protecting patients from the risk of multiple sclerosis progression: A relatively smaller proportion of patients, than adherents of Ocrevus or Kesimpta, experienced a worsening of the disease course. This is thought to be due to the unique mechanism of action of ublituximab, which allows it to deplete the pool of B lymphocytes (in this case pathogenic) as deeply as possible and maintain the proper level of depletion for a long time (until the next infusion of the drug).
Roche understands this and has therefore started the phase 3 clinical trials, NCT04544436 and NCT04548999, in relapsed multiple sclerosis (RMS) and primary progressive multiple sclerosis (PPMS), respectively, which will test doubled and tripled doses of ocrelizumab (1200 and 1800 mg, for patients weighing less than or over 75 kg) to see if a higher B cells depletion will have a beneficial effect on the course of multiple sclerosis without compromising treatment safety.
Ublituximab infusions are faster but Ocrevus is no slouch either. Thus, in a substudy ENSEMBLE PLUS of the phase 3 clinical trial ENSEMBLE (NCT03085810) among patients with early relapsing-remitting multiple sclerosis, it was confirmed that ocrelizumab can be infused faster in 2 hours. As a result, in mid-December 2020, the new dosing regimen was included in the prescribing information of Ocrevus. To be fair, plus or minus a few hours makes absolutely no difference given the need for only one dose every six months.
To summarize, the only thing that ublituximab can do for its successful launch and decent lifecycle is to dramatically lower the cost of treating multiple sclerosis with highly effective DMTs. But the future never turns out to be optimistic: Single players in the global pharmaceutical industry are able to hold back the greed of their investors who want to get rich quickly.
Extras
TG Therapeutics. ULTIMATE I & II data preview call. April 2021. [PDF]
TG Therapeutics. Efficacy and safety of ublituximab vs teriflunomide in patients with relapsing multiple sclerosis: Results from two phase 3 studies ULTIMATE I & ULTIMATE II. AAN 2021. [PDF]
A phase 2 multicenter study of ublituximab, a novel glycoengineered anti-CD20 monoclonal antibody, in patients with relapsing forms of multiple sclerosis. Mult Scler. 2021 Mar;27(3):420-429. [source]