Highlights
The experimental drug bepirovirsen, being developed by GlaxoSmithKline, has the potential to provide a functional cure for chronic hepatitis B.
It has been demonstrated that weekly subcutaneous injections of bepirovirsen resulted in complete clearance of hepatitis B virus DNA and its surface antigen (HBsAg) in nearly a third of patients after 6 months of treatment.
However, after 6 months of follow-up after completion of therapy, the functional cure status appeared to be true for a significantly smaller proportion of patients. Nevertheless, the therapy can still be called successful when compared with existing medications.
Currently, chronic hepatitis B, which infects 300 million people around the world, is incurable. Lifelong therapy has to be followed, which is not always successful.
In contrast, chronic hepatitis C is considered completely curable. Since the end of 2013, direct-acting antivirals that cure this infectious disease in a few months have been systematically appearing.
Bepirovirsen: Mechanism of Action
Bepirovirsen (GSK3228836, IONIS-HBVRx) is an antisense oligonucleotide (ASO), a single-stranded DNA that is complementary to all hepatitis B virus (HBV) mRNA, including its pregenomic RNA (pgRNA). Binding of bevirovirsen to HBV mRNA and pgRNA results in the formation of a hybrid complex that recruits endogenous ribonuclease H (RNase H). This enzyme cleaves HBV mRNA and pgRNA, thereby preventing translation of the virus proteins. As a result, the amount of HBV RNA, DNA, and proteins, including hepatitis B surface antigen (HBsAg), is reduced. Viral load decreases, HBV infection and replication processes are restrained, there is a chance for functional cure of chronic hepatitis B. [1] [2] Bepirovirsen also exhibits agonist activity to toll-like receptor 8 (TLR8), thereby working as an immunostimulant.
Bepirovirsen was developed by Ionis Pharmaceuticals, which licensed it to GlaxoSmithKline in late August 2019. In return, up to $262 million and royalties from sales of the finished drug were promised.
The validity of the therapeutic paradigm of antisense oligonucleotides is confirmed by a considerable number of already approved drugs aimed at inhibiting the expression of specific proteins pathogenic in a particular disease. For example, Exondys 51 (eteplirsen), Vyondys 53 (golodirsen), Amondys 45 (casimersen), and Viltepso (viltolarsen) are used in the treatment of Duchenne muscular dystrophy, Spinraza (nusinersen) is indicated for the treatment of spinal muscular atrophy, Tegsedi (inotersen) is prescribed for the treatment of polyneuropathy in hereditary transthyretin-mediated amyloidosis.
Bepirovirsen: Efficacy and Safety of Chronic Hepatitis B Treatment
The B-Clear (NCT04449029) phase 2b (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial invited adult patients (n=457) with chronic hepatitis B undergoing or not receiving background treatment with nucleoside/nucleotide analogues (NAs).
For 24 weeks, participants were given bepirovirsen weekly (different regimens) by subcutaneous injection:
- Group 1: 300-mg bepirovirsen for 24 weeks
- Group 2: 300-mg bepirovirsen for 12 weeks, then 150-mg bepirovirsen for 12 weeks
- Group 3: 300-mg bepirovirsen for 12 weeks, then placebo for 12 weeks
- Group 4: placebo for 12 weeks, then 300-mg bepirovirsen for 12 weeks.
Groups 1, 2, and 3 also received loading doses of 300-mg bepirovirsen on days 4 and 11.
The primary endpoint was the proportion of patients who demonstrated a sustained virological response (SVR), which is defined as a decrease in hepatitis B surface antigen (HBsAg) and HBV DNA levels below a high-precision PCR threshold maintained for 24 weeks after treatment completion and assuming no additional treatment with any antiviral medications (if not previously taken) during this period.
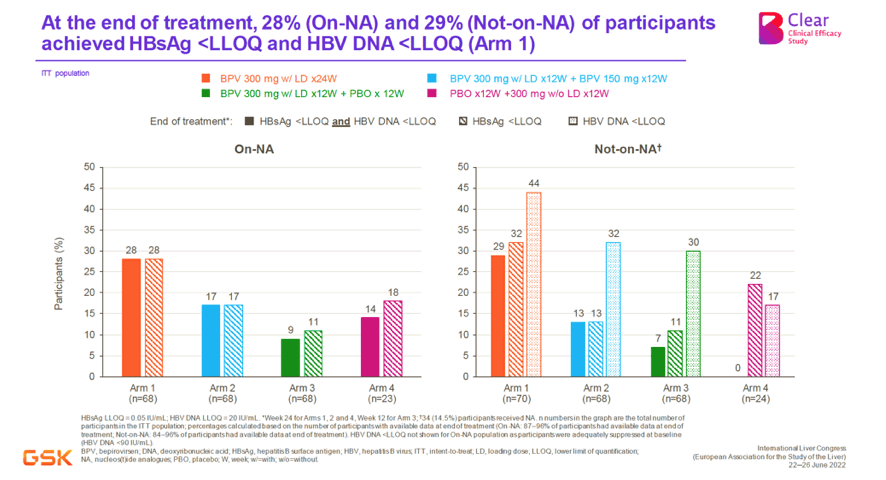
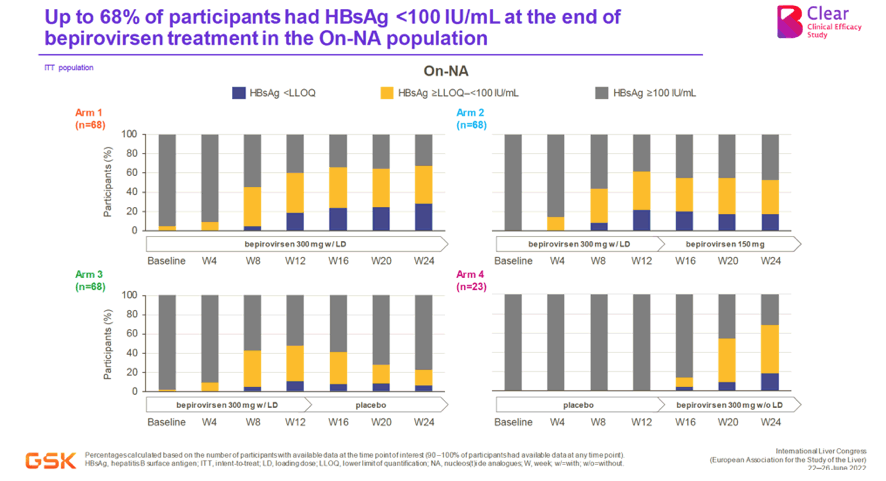
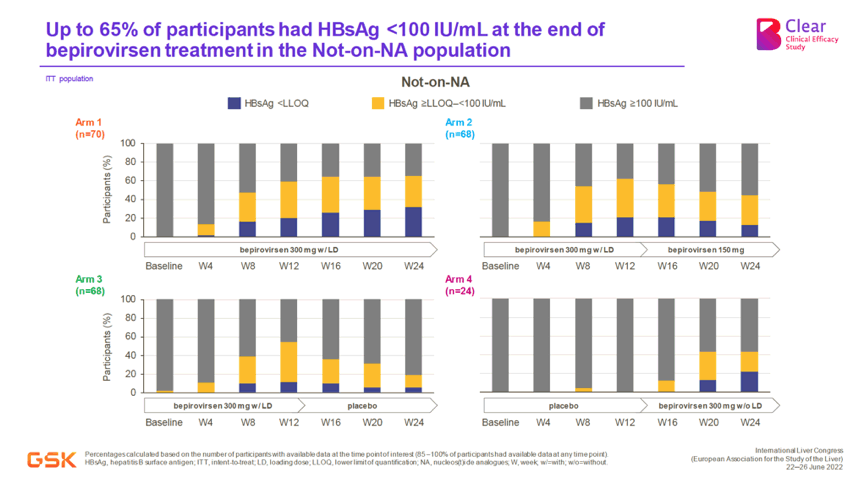
According to interim analysis of collected data, after 24-week therapy of chronic hepatitis B, Group 1 showed the best results. Thus, the simultaneous absence of HBsAg and HBV DNA was documented for 28% and 29% of subjects adhering to NAs background therapy and not taking such drugs, respectively. At the same time, 68% and 65% of participants had HBsAg levels below 100 IU/mL.
The final results of the clinical trial were as follows.
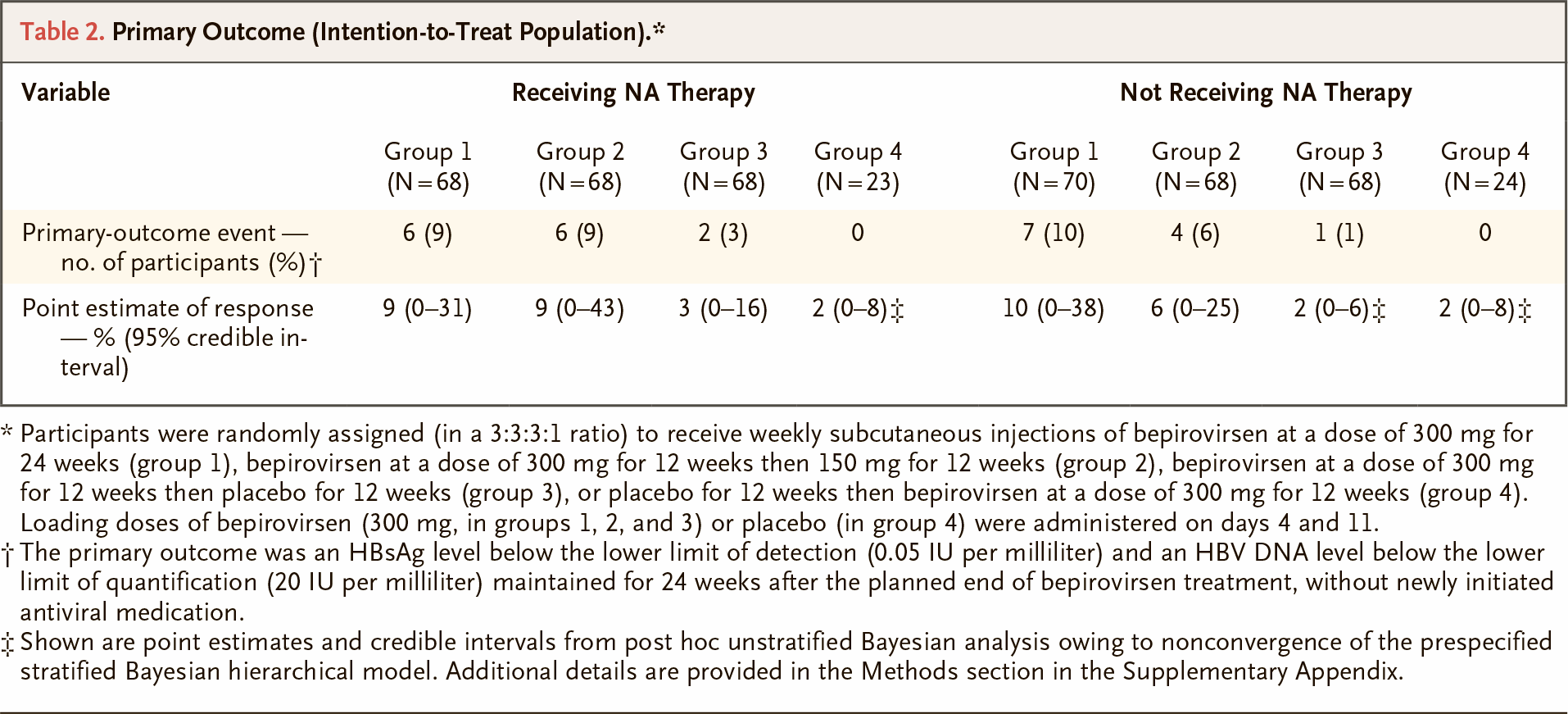
Among those patients who adhered to NAs background therapy, 9%, 9%, 3%, and 0% of participants in Groups 1, 2, 3, and 4 reached the primary efficacy endpoint. Among those who did not receive NAs, the primary efficacy endpoint was reached among 10%, 6%, 1%, and 0% of subjects.
Assuming “blips” in hepatitis B virus activity (single-time-point increases in HBsAg or HBV DNA to levels greater than or equal to threshold levels), that is, somewhat relaxing the exit criteria for the primary endpoint, it was reached in 10%, 9%, 4%, and 2% of patients on background NAs therapy and 14%, 6%, 1%, and 4% of patients without background NAs therapy.
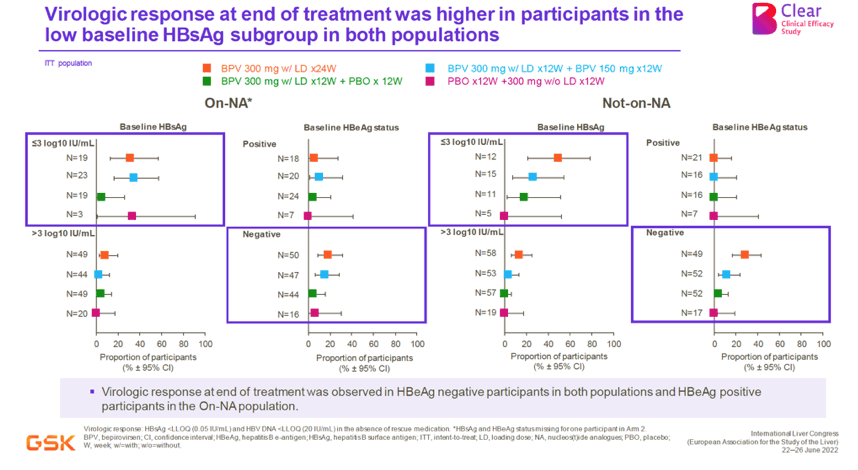
Successful response to bepirovirsen directly depended on the pre-treatment HBsAg level: it was more frequent in subjects with low HBsAg levels (≤ 3 log10 IU/mL) and less frequent in those with high levels (> 3 log10 IU/mL). For example, in Group 1, the primary endpoint was documented in 16% and 25% of patients with low baseline HBsAg levels and in 6% and 7% of patients with high levels, respectively, among those receiving and not receiving background NAs therapy.
Bepirovirsen was characterized by acceptable tolerability. The most common adverse event was injection site reaction.
Bepirovirsen: What’s Next
GlaxoSmithKline is continuing the B-Sure (NCT04954859) phase 2 clinical trial among previously treated with bepirovirsen and responding patients from other trials of the drug: a 33-month follow-up to see how long sustained virological response (SVR) status persists.
A parallel B-Together (NCT04676724) phase 2 clinical trial is testing the 12- or 24-week use of bepirovirsen on nucleoside/nucleotide analogues therapy, followed by a 24-week course of pegylated interferon alfa-2a. The presence of SVR is established after 24 weeks of treatment.
GlaxoSmithKline is also conducting a phase 2 clinical trial, NCT05276297, in which a 12- or 24-week course of bepirovirsen therapy is followed by administration of an experimental GSK3528869 targeted immunotherapy.
GSK3528869A is a three-component therapeutic vaccine:
- ChAd155-hIi-HBV: replication-defective simian (chimpanzee-derived) group C adenovirus serotype 155 viral vector encoding sequences of two HBV protein antigens: the truncated hepatitis B core antigen (HBcAg) and the full-length small hepatitis B surface antigen (S-HBsAg);
- MVA-HBV: encoding the above two HBV protein antigens Modified vaccinia Ankara (MVA), which is a highly attenuated Vaccinia virus strain;
- HBc-HBs/AS01B-4: the above two HBV protein antigens enhanced by the AS01B-4 adjuvant, which is a liposomal combination of 3-O-desacyl-4′-monophosphoryl lipid A (MPL) from Salmonella minnesota and a saponin molecule (QS-21) from plant extract of Quillaja saponaria.
The first component of GSK3528869A is administered on day 1, the second on day 57, and the third on days 113 and 169.
The conceptual idea behind the use of therapeutic vaccines like GSK3528869A is that a lack of induction of HBV-specific B and T cell immunity is responsible for the lack of clearance of hepatitis B virus. [1] [2] [3] [4] The vaccine should trigger the formation of strong virus-specific immunity against HBV antigens, controlling infection by induction of neutralizing antibodies and elimination of infected hepatocytes with the participation of effector T cells. [5] [6]
The NCT05330455 phase 1/2 clinical trial tests a combination of bepirovirsen and GSK3965193, a small-molecule inhibitor of noncanonical atypical poly(A) polymerases 5 and 7 (PAPD5 and PAPD7). These enzymes are required to stabilize HBV RNA through the viral post-transcriptional regulatory element (PRE). [7] [8] [9] Inhibition of PAPD5 and PAPD7 leads to suppression of viral replication and synthesis of viral proteins including HBsAg. [10] [11] [12] In preclinical trials in a mouse model of HBV, the combination of bepirovirsen and GSK3965193 was shown to be justified in terms of enhancing the reduction of HBsAg levels.
Expert Comments
All current treatment strategies for chronic hepatitis B aim at long-term suppression of HBV DNA. Loss of hepatitis B e antigen (HBeAg) in HBeAg-positive patients is highly desirable, as it reflects the presence of partial immune control of the infection. Normalization of ALT levels should be considered as an additional goal. The optimal treatment endpoint is sustained loss of hepatitis B surface antigen (HBsAg), as it indicates profound suppression of HBV replication and viral protein expression, indicating a functional cure of chronic hepatitis B, that is, when the virus is not completely eliminated from the body, but the immune system controls it without any medication. [1] [2]
The available drug approaches to the treatment of chronic hepatitis B, represented by peginterferon therapy and the administration of nucleoside/nucleotide analogues (NAs), cannot boast unequivocal efficacy. The loss of HBsAg is very rare: after 6 months after a one-year course of treatment, this is seen in 3–7% of peginterferon therapy and 0–3% of NAs therapy. If NAs use continues for a long time, say 5–8 years, the likelihood of HBsAg loss increases, but again only slightly: up to 10–12% in initially HBeAg-positive patients and less than 1–2% in HBeAg-negative patients. [1]
Such modest efficacy of chronic hepatitis B treatment is due to the fact that complete eradication of HBV by current drugs is difficult because of the preservation in hepatocytes both covalently closed circular DNA (cccDNA) HBV and HBV DNA integrated into their nucleus, which are transcriptional templates for resumption of replication of HBV DNA. [3] [4]
Attempts at combination therapy have resulted in a loss of HBsAg in 14% of cases if patients are switched to peginterferon therapy after at least 48 weeks of NAs therapy. [5] The direct antiviral activity of NAs, through inhibition of viral DNA polymerase (reverse transcriptase) resulting in virologic suppression and suppression of HBV replication, is thought to partially restore adaptive immunity, thereby improving the immunomodulatory action of peginterferon manifested in the prevention of HBV protein formation and depletionof the intrahepatic pool of cccDNA. [6] [7] [8] [9] Nevertheless, the approach needs further clarification studies.
In addition to the functional cure of chronic hepatitis B, there is the far less achievable goal of a sterile cure, where HBsAg is undetectable and HBV DNA, including cccDNA and integrated DNA, is destroyed.
Bepirovirsen has demonstrated high efficacy based on the fact that loss of HBsAg has been established in nearly one-third of patients after a relatively short 24-week course of treatment.
A virological response was reported among both HBeAg-negative patients and those adhering to NAs treatment HBeAg-positive patients. This suggests that the therapeutic HBV mRNA-sequencing target for bepirovirsen is present even when HBsAg is derived from integrated viral genomes. [10]
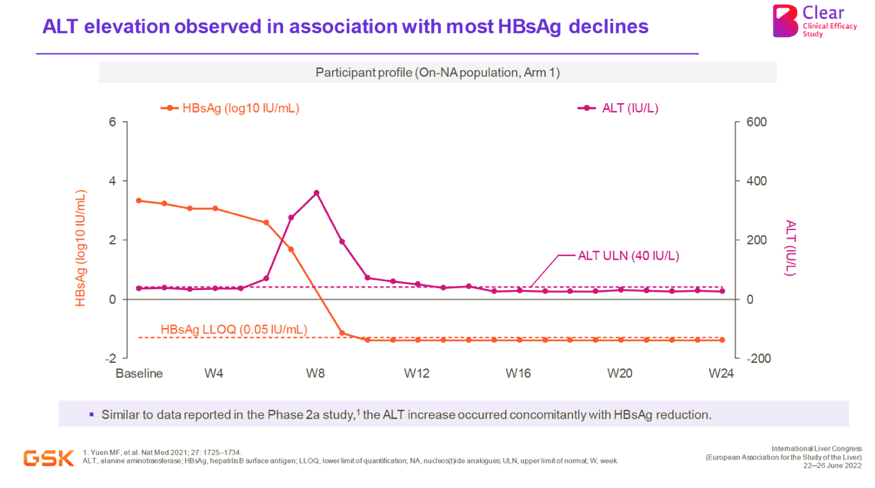
The observed increase of ALT level, accompanied by a decrease of HBsAg level, indicates beneficial immune processes. It is known that the increase in ALT level, a surrogate marker of liver inflammation, indirectly reflects the fact of immune-mediated destruction and clearance of infected hepatocytes and is a predictor of HBsAg loss. [11]
We cannot say that the final results of the clinical trial of bepirovirsen were disappointing. Yes, functional cure status of chronic hepatitis B confirmed by absence of HBsAg and HBV DNA during 6 months after treatment completion was recorded in maximum 10% and 14% of patients, respectively, among those who received background NAs therapy and without it. However, given the short course of therapy, efficacy should be taken with due optimism.
Since bepirovirsen showed the greatest efficacy among patients with baseline low HBsAg levels, one should further consider the latter as a fundamental criterion for the selection of suitable patients who are more likely to benefit from treatment.
In addition, one predictor of success is HBeAg status. In Group 1, among HBeAg-negative participants, 10% and 14% were functionally cured, respectively, among those with and without background NAs therapy. In HBeAg-positive status, cure was noted for 6% and 0%.
Fortunately, there is a trend that most patients with chronic hepatitis B are HBeAg-negative, meaning that HBV DNA sequences are integrated into the host genome and are the primary source of HBsAg. [19] [10]
Despite the many experimental approaches to the treatment of chronic hepatitis B that have been studied, [12] there is a growing criticism of them; they say that most of them are fundamentally flawed. [13] HBV infection is characterized by a very high degree of genetic plasticity (thousands of quasispecies exist in each individual patient), [14] which is the result of lack of HBV reverse transcriptase corrective activity, high turnover of cccDNA, and constant immune pressure exerted on the virus. Considering that even single point mutations of HBV abolish the ability of antisense oligonucleotide (ASO) and small interfering RNA (siRNA) to specifically cleave mRNA, [15] even theoretical validity of these classes of drugs for chronic hepatitis B treatment is questioned.
This is hinted at by the fact that HBsAg reduction provided by bepirovirsen was stronger among patients with initially lower HBsAg levels (≤ 3000 IU/ml), which contradicts the stated mechanism of action of the drug: The strength of HBsAg reduction should not depend on its initial level.
A previous phase 2a clinical trial, NCT02981602, showed a similar pattern. [16] Again, GSK3389404, a variant of bepirovirsen conjugated with N-acetylgalactosamine (GalNAc) for more targeted delivery to hepatocytes, [17] had no significant effect on reducing HBsAg levels. [18]