Highlights
Evusheld (tixagevimab + cilgavimab) is a new drug indicated for pre-exposure prophylaxis of coronavirus disease COVID-19 caused by the new coronavirus SARS-CoV-2.
Evusheld is the first drug designed to prevent COVID-19 rather than treat it.
Evusheld can be used by adults and children (12 years and older, weighing at least 40 kg) who are not currently infected with the coronavirus and who have not had recent exposure to an infected person.
- There is an additional restriction on the use of Evusheld. The drug is indicated either for persons who are immunocompromised (moderately or severely) for health reasons or because of immunosuppressive therapy, unable to respond adequately to the COVID-19 vaccine, or for persons for whom vaccination is not recommended because of a history of severe adverse reactions to the vaccine or its components.
Evusheld should not be used to treat COVID-19 or as post-exposure prophylaxis for it, that is, when contact with a person infected with the coronavirus has been established.
- Evusheld, however, confirmed that it is capable of treating COVID-19 of mild-to-moderate severity. But in the task of post-exposure prophylaxis, it was of no help.
Evusheld is not a substitute for any COVID-19 vaccine.
- This statement is presumably because of limited production capacity and the desire to reduce the cost of insurance reimbursement for expensive drugs, as well as the policy of widespread and universal vaccination.
If Evusheld is to be administered to a vaccinated person, it is necessary to wait at least two weeks after the last dose of vaccine.
Evusheld, developed by AstraZeneca, is approved by the U.S. Food and Drug Administration (FDA) in early November 2021 under the Emergency Use Authorization (EUA).
- The U.S. government has signed a contract with AstraZeneca to supply 700,000 doses of Evusheld. The drug will be distributed at no cost to Americans who need it.
The European Medicines Agency (EMA) granted Evusheld marketing authorization at the end of March 2022. Unlike the U.S. regulator, the European one allowed Evusheld to be used for pre-exposure prophylaxis of COVID-19 without any restrictions on immune system status, meaning in the general population.
There are already monoclonal antibodies against SARS-CoV-2 on the market, but they are all only used to treat COVID-19. These drugs, developed by Eli Lilly/AbCellera Biologics/Shanghai Junshi Biosciences, Regeneron Pharmaceuticals, GlaxoSmithKline/Vir Biotechnology, and Celltrion, include bamlanivimab + etesevimab, REGEN-COV/Ronapreve (casirivimab + imdevimab), Xevudy (sotrovimab), Regkirona (regdanvimab). They are indicated for the treatment of mild-to-moderate COVID-19 infection in people at high risk of progression to a severe form.
- REGEN-COV and the combination of bamlainivimab with etesevimab are additionally approved for post-exposure prophylaxis of COVID-19 in individuals at risk of developing severe disease.

Evusheld and Omicron
According to an FDA study, Evusheld retains neutralizing activity against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus.
Thus, the half-maximal inhibitory concentration (IC50), as an indicator of the neutralizing ability of the antibody, for Evusheld under the Omicron conditions decreased dramatically but still fell within the range of 171–277 μg/mL, which is in between neutralizing titers in people previously infected with the coronavirus. By comparison, the IC50 of Evusheld in the original non-mutant SARS-CoV-2 is 1.3–1.5 μg/mL.
Evusheld’s ability to fight Omicron was previously confirmed in another third-party study.
As for the antiviral activity of Evusheld against Omicron subvariants, studies show that the drug copes with them, although to a lesser extent than in the case of the original non-mutant Omicron. Thus, the neutralizing activity of Evusheld against the original Omicron (BA.1 [B.1.1.529.1]) and its subvariants (BA.1.1 and BA.2 [B.1.1.529.2]) was reduced by 132–183, 424 and 3.2 times in the pseudotypic virus-like particles (VLPs) system, and by 12–30, 176, and 5.4 times in the authentic virus system.
Evusheld maintains antiviral activity against the Omicron subvariants BA.4 and BA.5, despite the fact that it decreased 8.1-fold compared to the activity against BA.2. Thus, in the pseudovirus system, the IC50 of Evusheld against the original coronavirus, its Omicron variant (BA.1) and Omicron subvariants BA.1.1, BA.2, BA.3, BA.4, and BA.5 was 0.001 µg/mL, 0.232 µg/mL, 0.806 µg/mL, 0.008 µg/mL, 0.065 µg/mL, and 0.065 µg/mL, respectively.

Omicron Variant: Latest Scientific News, Findings, Evidence, and Developments
Up-to-date scientific information about the new Omicron variant of SARS-CoV-2/COVID-19.
Evusheld: Mechanism of Action
Intramuscularly administered Evusheld (AZD7442) is a set of two recombinant human IgG1ϰ monoclonal antibodies, tixagevimab (AZD8895) and cilgavimab (AZD1061), which bind to non-overlapping regions of the receptor-binding domain (RBD) of S-protein of SARS-CoV-2, thereby blocking its interaction with angiotensin-converting enzyme 2 (ACE2), the receptor that the virus uses to attach to the cell membrane and then penetrate it.
The amino acid substitutions introduced into the monoclonal antibodies (to reduce binding to Fc-receptor and complement component 1q) almost tripled their half-life, reduced effector function, and minimized the potential risk of antibody-dependent enhancement of disease, a phenomenon in which virus-specific antibodies promote, rather than suppress, infection and/or disease.
Evusheld is claimed to provide robust protection against COVID-19 for at least 6 months. The protection will probably last much longer: based on simulated pharmacokinetic data, the monoclonal shield can last for an entire year.

Sotrovimab Is Effective Against Omicron Variant of Coronavirus
A monoclonal antibody developed by GlaxoSmithKline and Vir Biotechnology successfully counteracts a new strain of SARS-CoV-2.
Tixagevimab and cilgavimab, discovered by Vanderbilt University Medical Center and licensed by AstraZeneca in June 2020, are monoclonal antibodies selected from an extensive library of such, accumulating this class of biomolecules derived from COVID-19 survivors.
Evusheld is declared to retain proper neutralizing activity even in the current glut of the Delta variant of the SARS-CoV-2 and the emerging wave of the Omicron strain.
Evusheld: Efficacy of COVID-19 Prophylaxis
The efficacy and safety of Evusheld were examined in two phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trials, PROVENT (NCT04625725) and STORM CHASER (NCT04625972), that tested the suitability of this drug in preventing the development of symptomatic COVID-19 infection caused by the new coronavirus SARS-CoV-2.
The first trial tested Evusheld to prevent the development of COVID-19 under pre-exposure conditions and the second trial tested it under post-exposure conditions (after exposure to the coronavirus).
Participants with a laboratory-confirmed history of SARS-CoV-2 infection or positive for antibodies against SARS-CoV-2 at the time of screening were excluded.
Subjects were given Evusheld or placebo once intramuscularly.
The primary endpoint was the number of cases of symptomatic disease caused by SARS-CoV-2 and with a positive RT-PCR result occurring up to 183 days after prophylaxis. Follow-up continued for 15 months.
PROVENT
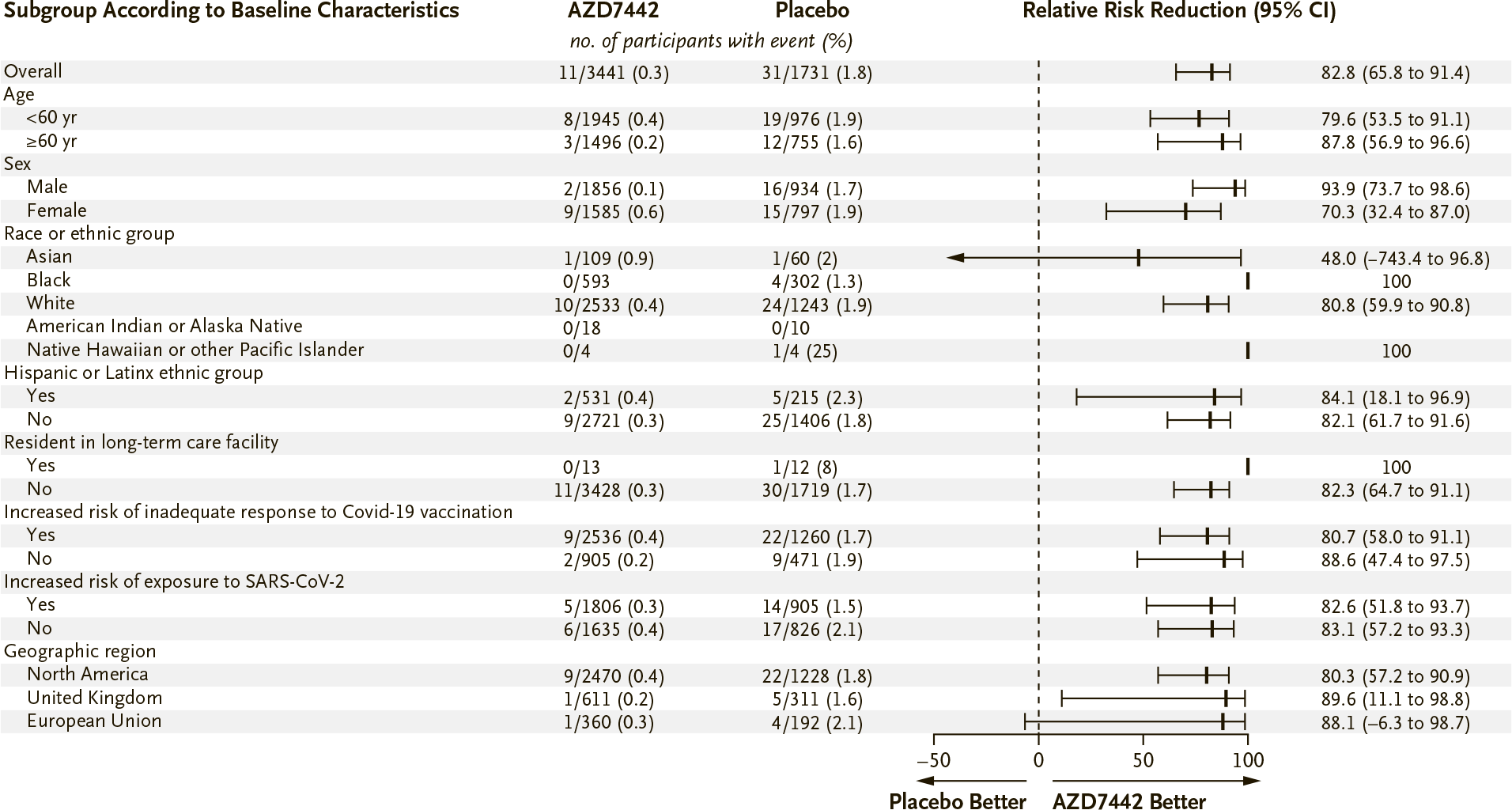
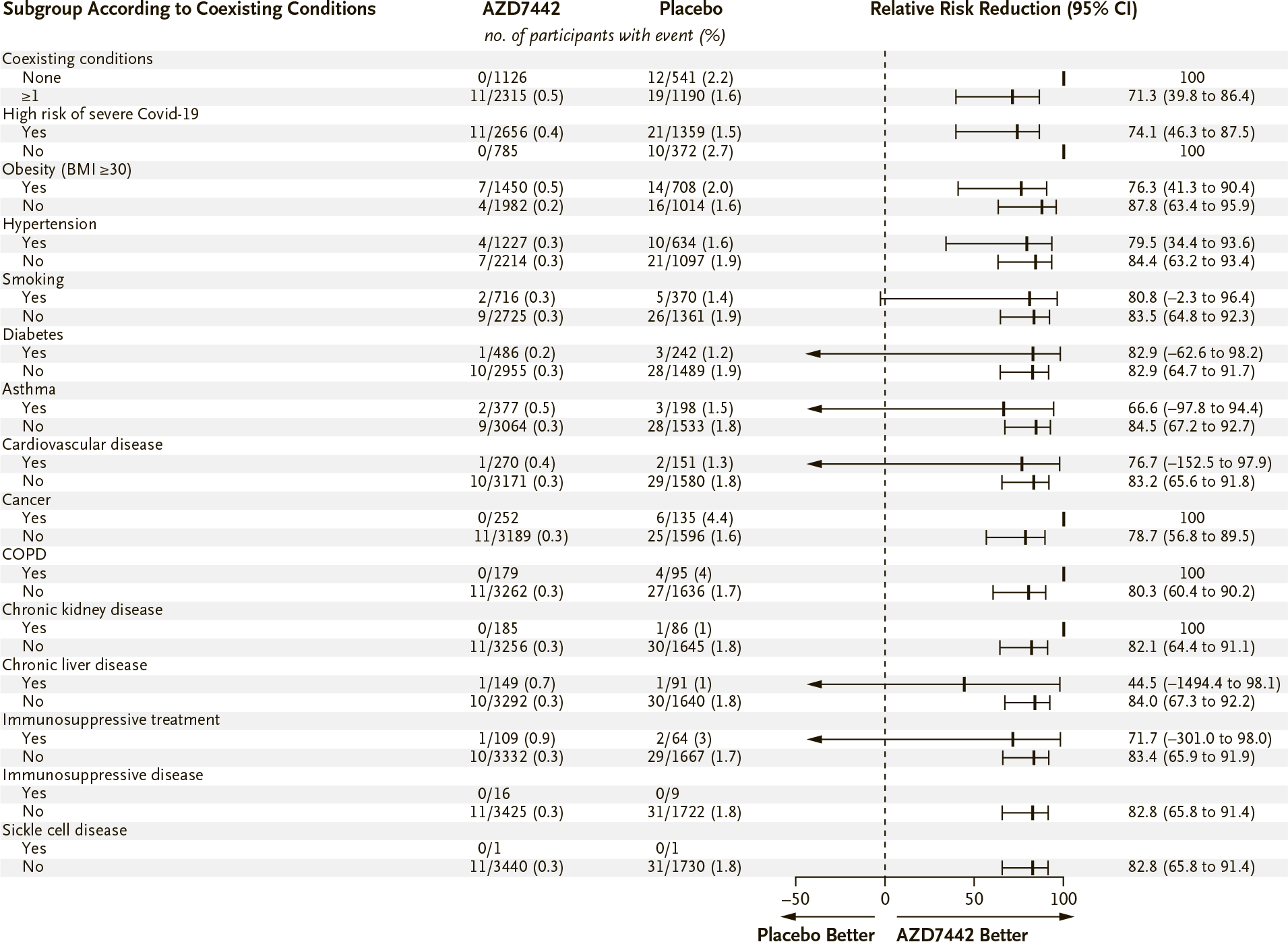
The ongoing PROVENT clinical trial enrolled unvaccinated adult volunteers (n=5172) who were either elderly (60 years or older) and had a co-morbid disease or were at increased risk for SARS-CoV-2 infection because of their living or working conditions.
- Co-morbidities included obesity, congestive heart failure, chronic obstructive pulmonary disease (COPD), chronic kidney disease, chronic liver disease, immune compromise, and severe or serious adverse reactions to COVID-19 vaccine in the history.
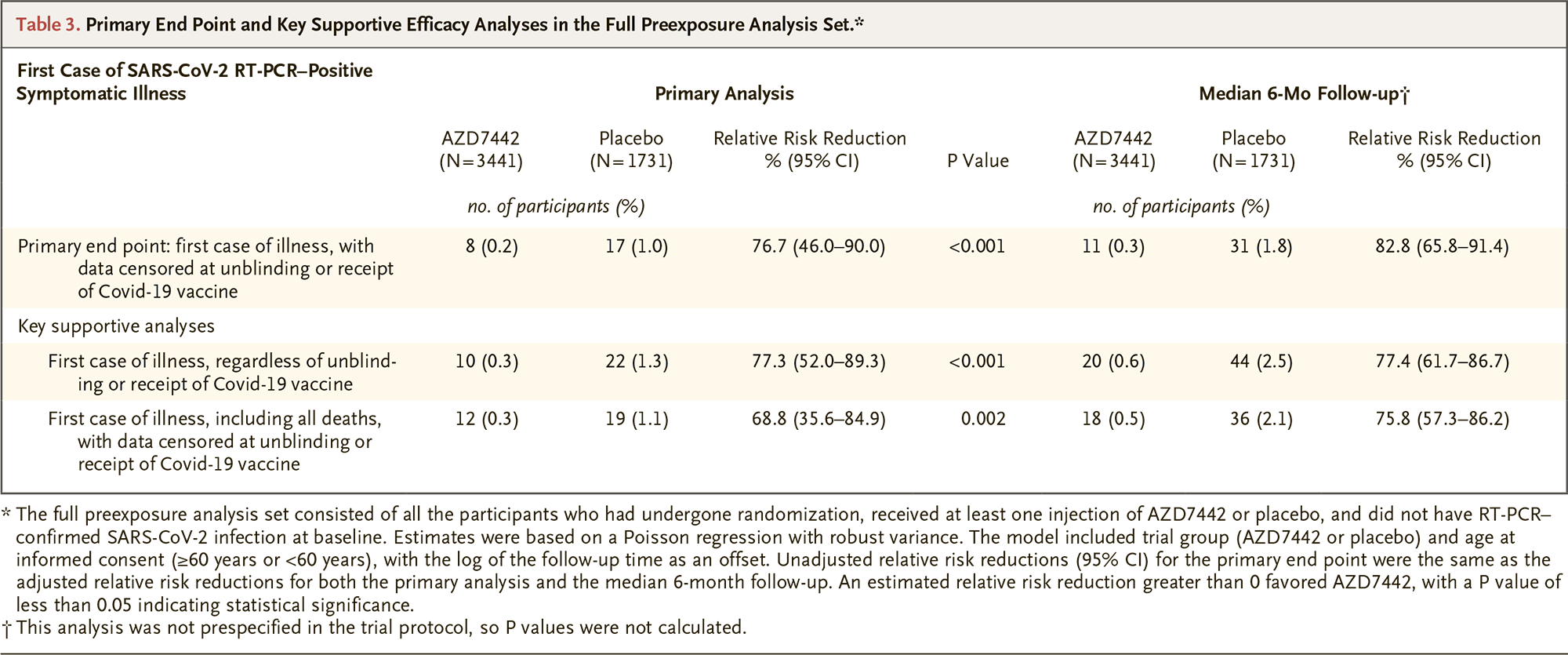
According to an interim analysis of the data, which covered follow-up at a median of 83 days (3–166) after prophylaxis, COVID-19 was encountered by 0.2% of subjects (n=8/3441) in Evusheld group — versus 1.0% (n=17/1731) in the placebo group. Thus, Evusheld reduced the risk of symptomatic COVID-19 infection by 77% (95% CI: 46–90; p<0.001).
No cases of severe or critical COVID-19 were reported among subjects who received Evusheld — vs. 1 case (0.1%) in the placebo group.
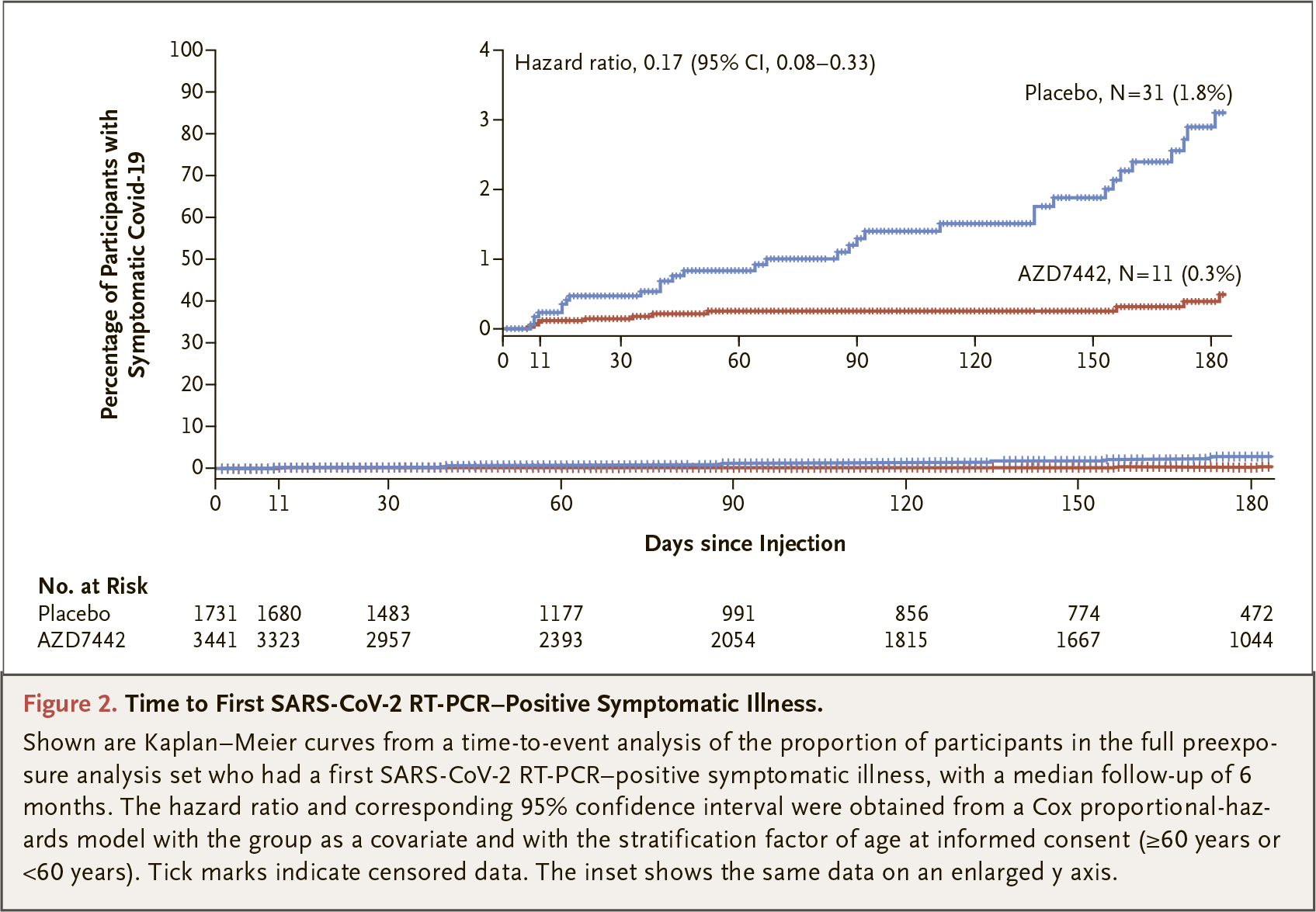
An interim analysis of data over a median follow-up period of 6.5 months (196 days) showed that Evusheld reduced the risk of developing COVID-19 by 83% (95% CI: 66–91): 0.3% (n=11/3441) — vs. 1.8% (n=31/1731) of cases. No severe or critical cases of COVID-19 were reported in the drug group — vs. 5 cases (0.3%) in the placebo group.
STORM CHASER
The ongoing STORM CHASER clinical trial recruited unvaccinated adult volunteers (n=1121) who had been in contact with a person with laboratory-confirmed COVID-19 infection, symptomatic or asymptomatic, and who was at risk for imminent COVID-19 at the time of inclusion in the trial.
- These volunteers included in particular members of the same household or institutional residences, health care or long-term care facility workers, and employees of occupational or industrial settings involving close contact.
During the median 49 day (5–115) follow-up, 3.1% of subjects (n=23/749) in Evusheld group developed symptomatic COVID-19 — versus 4.6% (n=17/372) in the placebo group. Thus, Evusheld showed no statistically significant effect: the reduction in relative risk (RR) was 33% (95% CI: −26 to 65).
However, Evusheld did work when considering cases of symptomatic COVID-19 among subjects who were initially RT-PCR negative, discarding those who were nevertheless infected with the coronavirus at the time of initiation of prophylaxis. Thus, according to planned data analysis, Evusheld reduced the risk of developing COVID-19 by 73% (95% CI: 27–90) relative to placebo.
A retrospective post hoc analysis showed that Evusheld reduced the risk of COVID-19 even further — by 92% (95% CI: 32–99) compared to placebo — for cases reported more than 7 days after prophylaxis, that is, those cases that were most likely related to infection occurring after prophylaxis rather than before it, based on the incubation period features of SARS-CoV-2.
Thus, Evusheld confirmed its protective ability in pre-exposure prophylaxis of COVID-19 but not post-exposure prophylaxis.
Evusheld: Efficacy of COVID-19 Treatment
The TACLE (NCT04723394) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial enrolled unvaccinated adult patients (n=903) with laboratory-confirmed COVID-19 infection, not requiring hospitalization, presenting with mild-to-moderate severity, and manifesting within 7 days of trial initiation.
- Trial participants had to be at high risk of COVID-19 progression to severe disease. Such risk was defined as older age and/or presence of comorbidities, including cancer, diabetes mellitus, obesity, chronic lung disease, asthma, cardiovascular disease, and immunosuppressive condition.
Subjects were given Evusheld or placebo once intramuscularly.
The primary endpoint was established by cases of severe COVID-19 or death from any cause within 29 days of treatment initiation.
In Evusheld group, these events occurred among 4.4% of patients (n=18/407) — versus 8.9% (n=37/415) in the placebo group. Thus, Evusheld reduced the risk of severe COVID-19 or death events by 50% relative to placebo.
According to a further analysis of the data, the risk was reduced by a relative 67% if Evusheld was administered no later than 5 days after the manifestation of COVID-19 symptoms, and by 88% if no later than 3 days.
Extras
Evusheld (tixagevimab + cilgavimab). Prescribing information. U.S. [PDF]
Evusheld (tixagevimab + cilgavimab). Prescribing information. Europe. [PDF]
Intramuscular AZD7442 (tixagevimab–cilgavimab) for prevention of Covid-19. N Engl J Med. 2022 Apr 20;NEJMoa2116620. [source]