Highlights
The Netherlands-based Argenx has launched Vyvgart (efgartigimod), a new drug indicated for the treatment of adult patients with generalized myasthenia gravis (gMG) and autoantibodies to acetylcholine receptor (AChR).
Vyvgart is approved by the U.S. Food and Drug Administration (FDA) in mid-December 2021.
The course of treatment with Vyvgart involves an intravenous infusion of the drug once a week for a month.
Vyvgart, which will go on sale in January 2022, costs $225,000 per year for a typical patient in the U.S. By comparison, a year’s treatment of myasthenia gravis with Soliris (eculizumab) — until now the only specialized drug against this autoimmune disease — costs $470,000.
Approval of Vyvgart in the European Union is expected in the second half of 2022, in Japan in the first quarter of 2022. By the middle of next year, Argenx intends to send the application for Vyvgart approval in China and Israel.
What is Myasthenia Gravis
Myasthenia gravis is a rare (150–250 cases per million) autoimmune disease that affects the neuromuscular synapses and is characterized by pathologically rapid and painless fatigue of the skeletal muscles.
Signs and symptoms of myasthenia gravis occur, often affecting the visual organs, manifesting as ptosis and diplopia. Thymic hyperplasia is found in 60–70% of myasthenia gravis patients and thymoma in 10–12% of cases.
In 85% of patients diagnosed with myasthenia gravis, it progresses within two years to a generalized form involving bulbar disorders and limb musculature problems. In two-thirds of patients, myasthenia gravis reaches its maximum severity within the first year. Myasthenic crisis in the form of respiratory failure occurs in 20% of patients, usually in the first year of the disease.
Myasthenia gravis, being an acquired synopathy, is caused by a B-cell mediated T-cell dependent immunological attack with the production of high-affinity autoantibodies directed against components of neuromuscular synapses and blocking signal transduction in the latter.
Autoantibodies against nicotinic acetylcholine receptors (AChRs) are detected in 80–90% of patients. Autoantibodies cause neuromuscular synapse dysfunction by blocking acetylcholine binding to its receptor, cross-binding and internalizing the AChR, and activating the complement system.
Acetylcholinesterase inhibitors (AChEIs), such as pyridostigmine and neostigmine, are the first-line therapy for myasthenia gravis regardless of its subtype.
Immunosuppressive therapy is recommended for more severe disease or if AChEIs do not work: oral corticosteroids (prednisolone, prednisone, methylprednisolone) and other immunosuppressive drugs (azathioprine, cyclosporine, mycophenolate mofetil, rituximab, cyclophosphamide, methotrexate, tacrolimus).
In myasthenia gravis crisis (severe exacerbations), intravenous immunoglobulins, plasmapheresis, and plasma exchange are used.
Soliris (eculizumab), a monoclonal antibody against complement component (C5) by Alexion Pharmaceuticals, improves the symptomatology of refractory myasthenia gravis and is approved in the therapy of generalized myasthenia gravis with AChR autoantibodies.
Vyvgart: Mechanism of Action of Efgartigimod
Efgartigimod (ARGX-113) is a fragment of a human IgG antibody against the neonatal Fc-receptor (FcRn).
The neonatal Fc receptor, also known as the Brambell receptor and encoded by the FCGRT gene, is a receptor for the Fc fragment of immunoglobulin G (IgG). Its structure is similar to that of the major histocompatibility complex (MHC) class I molecule and is associated with beta-2-microglobulin (B2M). In the early stages of life, FcRn ensures the absorption of IgG antibodies from maternal blood or milk and plays an important role in maintaining the homeostasis of this isotype and serum albumin antibodies in the adult body, protecting them from premature degradation.
FcRn, which is involved in antigen processing and presentation, is involved in activating T lymphocytes CD4+ and CD8+ and triggering stimulation of inflammatory cytokine synthesis and release by these cells. FcRn-mediated antigen presentation also contributes to IgG production by B lymphocytes and maintenance of the immune IgG response.
FcRn actually saves IgG from decay by binding them to endosomes and returning them to the bloodstream, thereby prolonging half-life. In autoimmune conditions, where the body mistakenly produces pathogenic IgG antibodies to its own tissues, FcRn contributes significantly to the chronic process by preventing the lysosomal breakdown of said IgG antibodies. Accordingly, it makes sense to block the interaction between FcRn and IgG.
Efgartigimod, being an Fc fragment of IgG1, acts as a natural FcRn ligand. The molecule is made to have an increased affinity for FcRn compared to endogenous IgG in order to compete with the binding of the latter, resulting in reduced recirculation of IgG and increased degradation.
Vyvgart: Efficacy and Safety of Efgartigimod in Treatment of Myasthenia Gravis
The ADAPT (NCT03669588) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial investigated the efficacy and safety of efgartigimod in the treatment of generalized myasthenia gravis in adult patients (n=167).
Prior to screening, participants were required to adhere to stable therapy for myasthenia gravis with acetylcholinesterase inhibitors, corticosteroids, or non-steroidal immunosuppressive drugs.
Subjects were given intravenous infusions of efgartigimod or placebo.
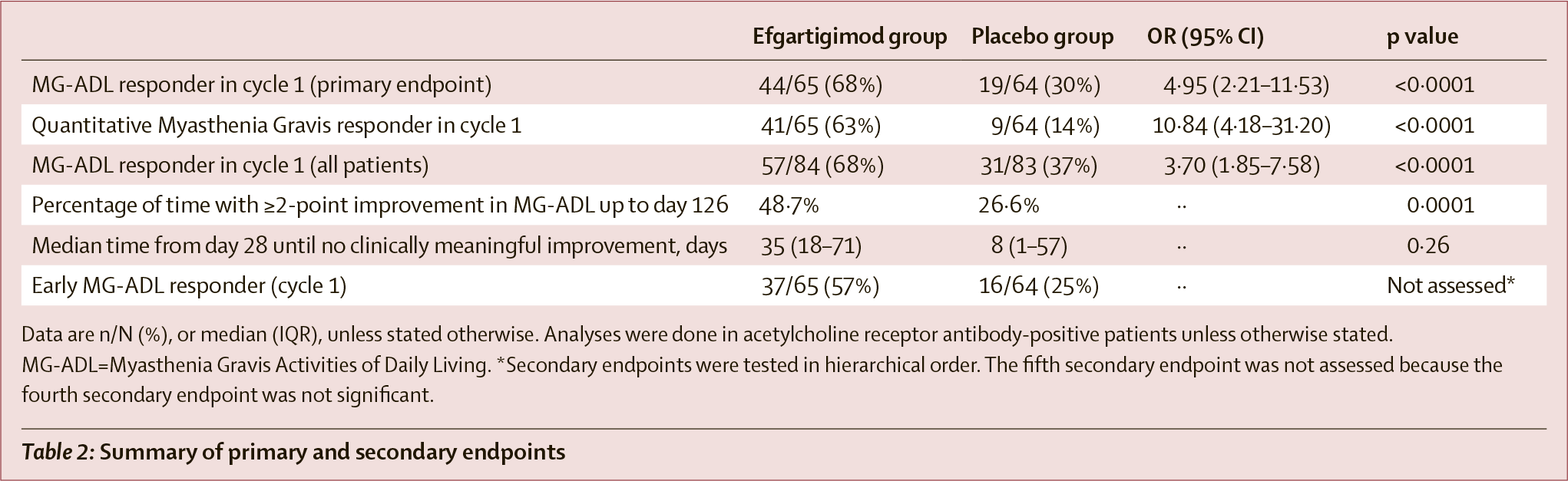
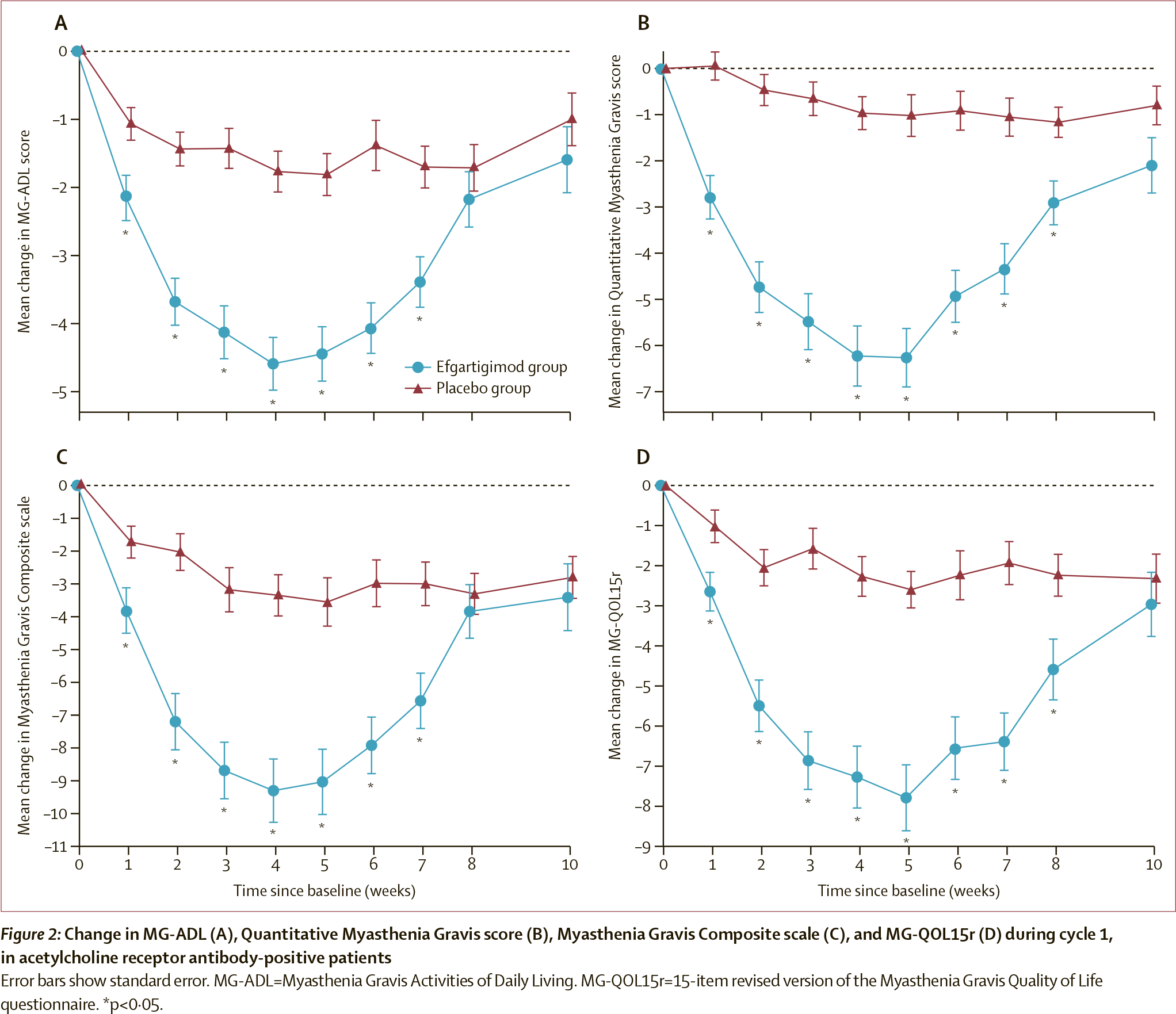
Treatment efficacy was assessed by the change in the total score on the Myasthenia Gravis Activities of Daily Living (MG-ADL) scale among patients with autoantibodies to acetylcholine receptor (AChR). Subjects were considered to have responded to treatment if they showed a decrease in MG-ADL score of 2 points or more, sustained for at least 4 consecutive weeks, with the first such decrease occurring within one week of the last drug infusion in the next therapy cycle.
In the first therapy cycle, the proportion of patients responding to treatment in Vyvgart group was 67.7% — versus 29.7% in the placebo group (p<0.0001). The odds ratio (OR) was 4.95 (95% CI: 2.21–11.53).
In addition, 40% of subjects in efgartigimod group reached an overall MG-ADL score of 0 or 1 (minimal symptom expression) — vs. 11% in the control group (p<0.0001).
Treatment efficacy was also confirmed by a change in the overall score on the Quantitative Myasthenia Gravis (QMG) scale, which assesses muscle weakness. Patients were considered to have responded to treatment if they showed a decrease in QMG score of 3 points or more for at least 4 consecutive weeks, with the first such decrease occurring within 1 week after the last drug infusion in the next therapy cycle.
In the first therapy cycle, the proportion of patients responding to treatment in Vyvgart group was 63.1% — vs. 14.1% in the placebo group (p<0.0001). The OR value came out to 10.84 (95% CI: 4.18–31.20).
Among AChR-positive patients, the mean maximum decrease in immunoglobulin G (IgG) levels was 61.3% and AChR antibodies levels was 57.6%.
The most common adverse reactions to efgartigimod administration included respiratory tract infections (in 33% of patients — versus 29% in the placebo group), headache (32% vs. 29%), urinary tract infections (10% vs. 5%), paresthesia (7% vs. 5%), and myalgia (6% vs. 1%).
Efgartigimod: What’s Next
Argenx continues to pursue a large-scale clinical program of efgartigimod, including testing its more convenient subcutaneous formulation, implemented thanks to ENHANZE drug delivery technology invented by Halozyme Therapeutics.

Halozyme: Elegant Transformation of Drugs From Intravenous to Subcutaneous
Easy and quick administration of biological drugs. All for the convenience of patient care.
Efgartigimod is undergoing a number of clinical trials for the experimental treatment of autoimmune diseases such as primary immune thrombocytopenia (ITP), pemphigus vulgaris, pemphigus foliaceus, chronic inflammatory demyelinating polyneuropathy (CIDP), bullous pemphigoid, idiopathic inflammatory myopathy (IIM; myositis).
Efgartigimod: Market Outlook and Competition
According to industry forecasts, sales of Vyvgart for the treatment of myasthenia gravis will reach $2.1 billion by 2026.
When it comes to the FcRn-targeted drugs being tested in the treatment of myasthenia gravis, efgartigimod’s closest competitor is the experimental rozanolixizumab (UCB7665), a monoclonal antibody against FcRn, which is handled by the Belgium-based UCB. Its “trick” is the subcutaneous route of administration, although the drug is administered daily.
Rozanolixizumab, which has successfully completed the MycarinG (NCT03971422) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial in the treatment of generalized myasthenia gravis, is being prepared for approval: the US, European and Japanese applications are scheduled for submission in the third quarter of 2022.
In the NCT03052751 phase 2 clinical trial, the proportion of patients responding to treatment (change in overall scores by at least 3 points) was greater in rozanolixizumab group than in the placebo group: MG-ADL (48% vs. 14%), QMG (38% vs. 23%), Myasthenia Gravis Composite (MGC) scale (48% vs. 27%).
Janssen as part of Johnson & Johnson is working on nipocalimab (JNJ-80202135, M281), a monoclonal antibody against FcRn developed by Momenta Pharmaceuticals, which was bought in October 2020 for $6.5 billion.
Nipocalimab, which is in the NCT04951622 phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial in the treatment of generalized myasthenia gravis, is administered intravenously once every 2 or 4 weeks.
The Vivacity-MG (NCT03772587) phase 2 clinical trial demonstrated that nipocalimab resulted in a sustained reduction in MG-ADL overall score of at least 2 points in 51.9% of patients — versus 15.4% in the placebo group.
Immunovant, as part of Roivant Sciences, deals with batoclimab (IMVT-1401, RVT-1401, HL161), a monoclonal antibody against FcRn developed by Korea’s HanAll Biopharma, affiliated with Daewoong Pharmaceutical. Batoclimab is administered by subcutaneous injection once weekly or every 2 weeks.
In the ASCEND MG (NCT03863080) phase 2a clinical trial in batoclimab group 60% of patients responded (reduction in MG-ADL overall total score by at least 2 points) to treatment for generalized myasthenia gravis — versus 20% in the placebo group. The phase 3 clinical trial is scheduled to start in early 2022.
Alexion Pharmaceuticals, now owned by AstraZeneca, is trying its hand with orilanolimab (ALXN1830, SYNT-001), a monoclonal antibody against FcRn developed by Syntimmune purchased by Alexion. Orilanolimab is administered by subcutaneous injections.

AstraZeneca + Alexion = Rescue of Both Companies
Alexion Pharmaceuticals, which owns Soliris, one of the most expensive drugs on Earth, has agreed to sell AstraZeneca for $39 billion.
The NCT04982289 phase 2a clinical trial testing orilanolimab in the treatment of generalized myasthenia gravis, temporarily stopped due to the COVID-19 pandemic, will be restarted in 2022.
Extras
Vyvgart (efgartigimod). Prescribing information. U.S. [PDF]
Vyvgart (efgartigimod).FDA approval call. Argenx, December 17, 2021. [PDF]
Argenx. Corporate Presentation, October 2021. [PDF]
Safety, efficacy, and tolerability of efgartigimod in patients with generalised myasthenia gravis (ADAPT): a multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2021 Jul;20(7):526-536. [source]
Efficacy and safety of rozanolixizumab in moderate to severe generalized myasthenia gravis: a phase 2 randomized control trial. Neurology. 2021 Feb 9;96(6):e853-e865. [source]
Nipocalimab. Vivacity-MG phase 2 interim analysis topline results. Momenta Pharmaceuticals, June 15, 2020. [PDF]
Roivant Sciences. R&D Day. September 28, 2021. [PDF]