Highlights
Tepezza (teprotumumab) is the first medication for the treatment of thyroid eye disease (TED).
Tepezza, offered by Horizon Therapeutics, was approved by the U.S. Food and Drug Administration (FDA) in late January 2020.
The list price for a 500-mg vial of Tepezza is declared to be $14,900. A full six-month course of treatment for American patients will average $200,000 (taking into account 75%–80% adherence to therapy and typical discounts and benefits); eight infusions of the drug in a weight-dependent dose, each administered once every three weeks.

What Is Thyroid Eye Disease?
Thyroid eye disease (TED), also called endocrine orbitopathy, endocrine ophthalmopathy, thyroid ophthalmopathy, thyroid-associated orbitopathy, Graves’ ophthalmopathy, Graves’ orbitopathy, autoimmune ophthalmopathy, is a rare (16 and 3 cases per 100,000 women and men, respectively) autoimmune inflammatory disease of the orbit and periorbital tissues characterized by retraction of the upper eyelid, edema, erythema, conjunctivitis, and proptosis (eye-bulging, exophthalmos). Although the pathology often occurs with Graves’ disease and hyperthyroidism, it may be of an independent nature. As the disease progresses, symptoms worsen: proptosis intensifies, strabismus (misalignment of the eyes) and diplopia (double vision) appears, and the risk of serious visual impairment increases.
Existing approaches to therapy of thyroid eye disease assume obligatory restoration of normal thyroid function (euthyroidism) and smoking cessation. Among symptomatic medications: artificial tears (saline eye drops), selenium, glucocorticosteroids as well as (in case of intolerance or ineffectiveness of the latter) mycophenolate, rituximab, tocilizumab. Somatostatin analogs and diuretics have no proper therapeutic effect. In severe cases, external radiation of the orbit and surgical interventions, including surgery on the eyelids, oculomotor muscles, decompression of the orbit by removing bone and/or fat tissue, are resorted to.
Tepezza: Mechanism of Action of Teprotumumab
It is well known that the thyroid-stimulating hormone receptor (TSHR) is a unique target in Graves’ disease, which is targeted by pathogenic autoantibodies, thyroid-stimulating immunoglobulins (TSIs). These, by activating TSHR, provoke the overproduction of thyroid hormones. The above autoantibodies are detected in the majority of patients, both with and without ophthalmopathy. The expression of TSHR by ocular tissues and their infiltrating fibrocytes suggests that it is a contributor to ophthalmopathy. However, the fact that TSIs are not detected in some individuals with ophthalmopathy suggests a pathogenetic contribution from other autoantigens.
Some of these are immunoglobulins that activate insulin like growth factor 1 receptor (IGF1R, CD221) signaling and synergistically amplify the effects of thyroid-stimulating hormone (TSH). The transmembrane receptor tyrosine kinase IGF1R is responsible for development and metabolism by regulating immune functions and therefore may well be an acceptable target in autoimmune disease therapy.
IGF1R is overexpressed by ocular fibroblasts as well as by T and B cells of Graves’ disease patients. IGF1R and TSHR create a signaling complex through which the former is transactivated. The resulting increase in cytokine expression leads to the activation of fibroblasts which begin to synthesize hyaluronan and other glycosaminoglycans that bind water well resulting in an increase in retrobulbar tissue which causes proptosis and optic nerve compression. In parallel, adipogenesis causes an increase in the volume of adipose tissue.
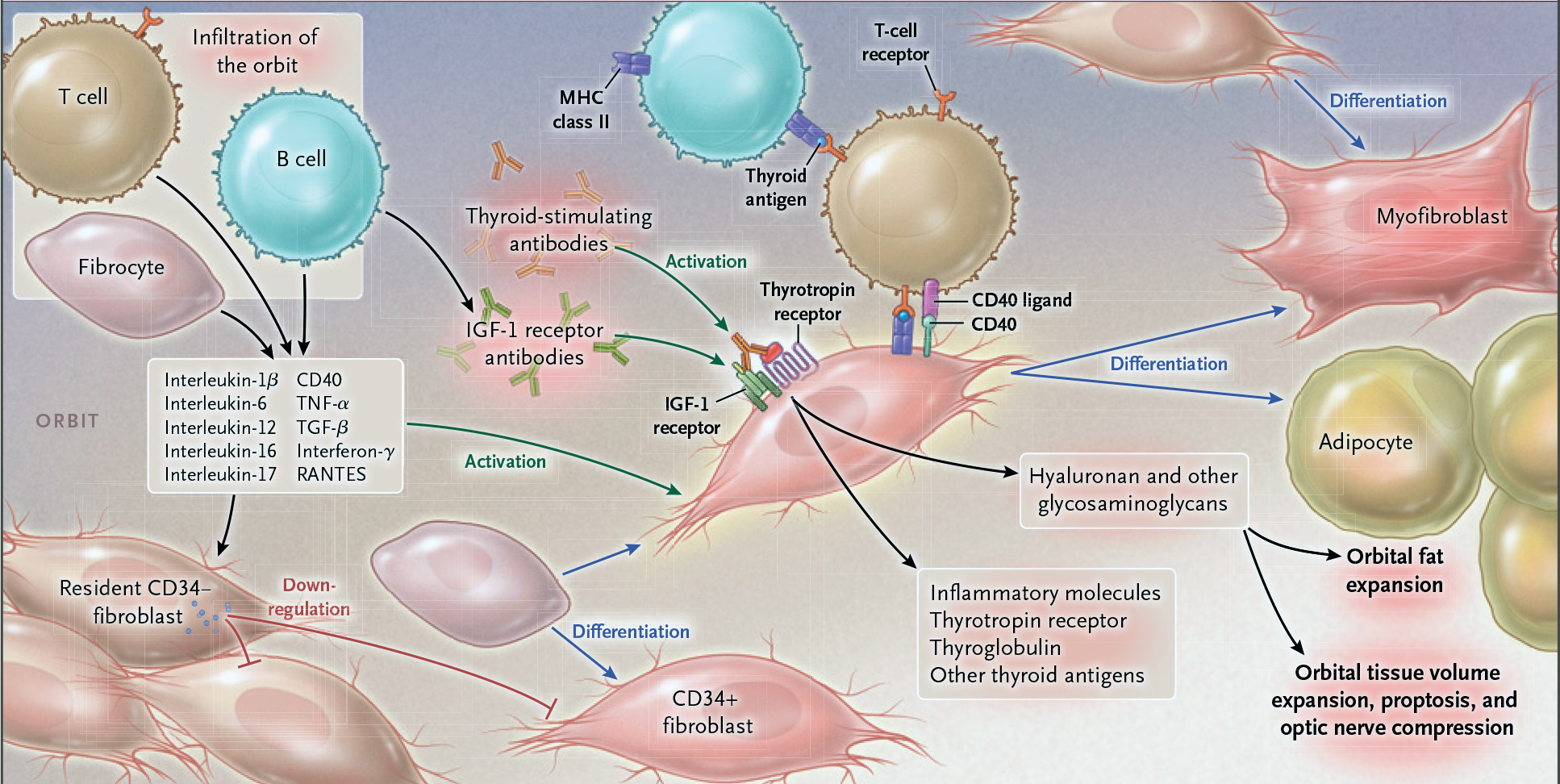
An in vitro study of ocular fibroblasts and fibrocytes showed that IGF1R-inhibiting antibodies attenuated the actions of insulin like growth factor 1 (IGF1), TSH, TSI, and immunoglobulins isolated from Graves’ disease patients. This opened the door for the clinical development of teprotumumumab (R1507), a fully human IgG1 monoclonal antibody against IGF1R.
Teprotumumab targets and binds to IGF1R, inhibits IGF1R autophosphorylation, reduces cell surface expression of IGF1R, and inhibits downstream signaling. Based on its mechanism of action as an IGF1R inhibitor, teprotumumab decreases inflammation and tissue expansion and produces clinically meaningful reductions in the signs and symptoms of thyroid eye disease.
Tepezza: Efficacy and Safety of Teprotumumab for Thyroid Eye Disease
The efficacy and safety of teprotumumab were evaluated in the NCT01868997 phase 2 and OPTIC (NCT03298867) phase 3 clinical trials (randomized, double-blind, placebo-controlled, multicenter) among adult patients (n=170) with Graves’ disease associated with active thyroid eye disease (TED), manifested no earlier than 9 months before randomization.
Participants must not have previously undergone any medical or surgical intervention, other than topical maintenance therapy or oral corticosteroids (at a maximum cumulative dose of no more than 1000 mg of methylprednisolone or equivalent). Among the inclusion criteria: euthyroid state or mild hypo- or hyperthyroidism at screening, which should have been brought to stable euthyroidism throughout the study.
Baseline characteristics of participants: median age 52 years (20–79), majority (73%) female, proptosis in the range 16–33 mm, 73% of patients had diplopia, and 27% were smokers.
For 24 weeks, patients received intravenous infusions of placebo or teprotumumab (initially 10 mg/kg and then 20 mg/kg) every three weeks.
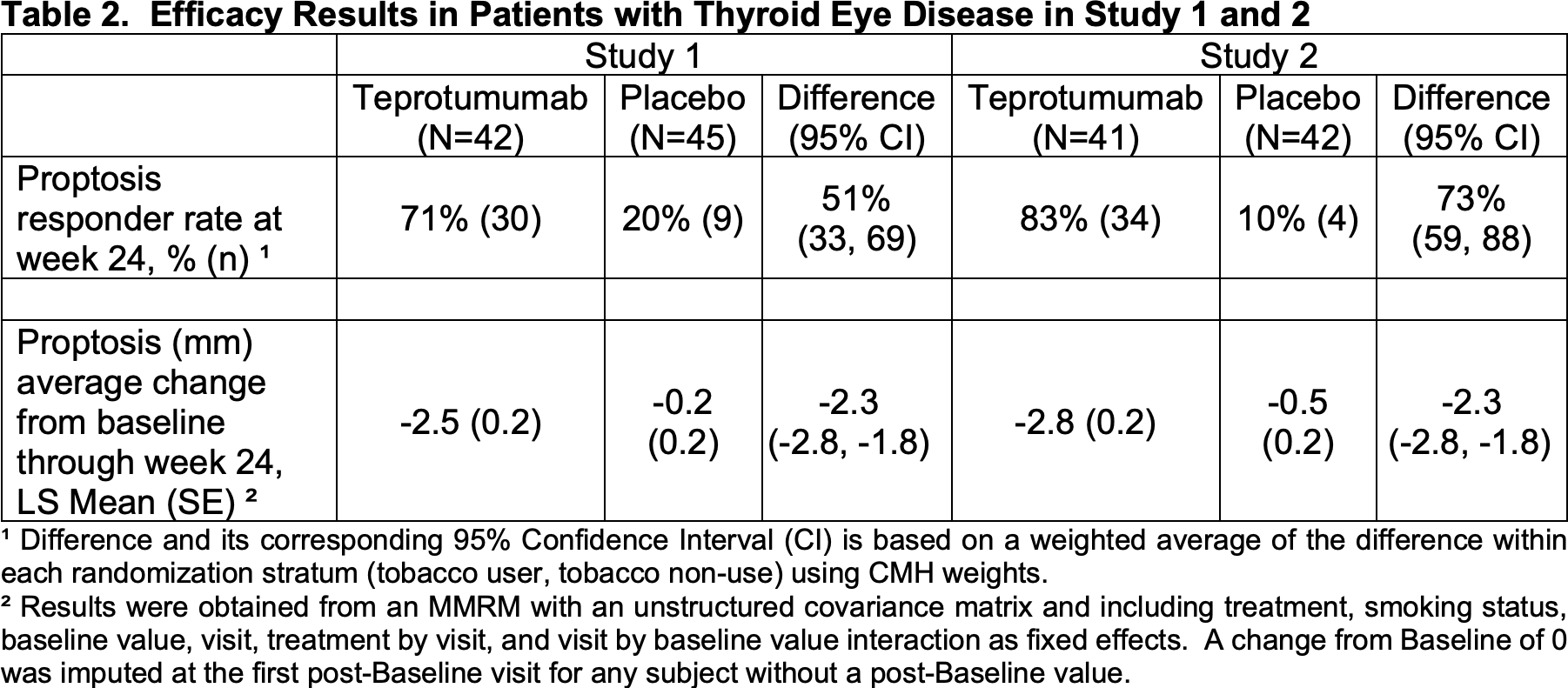
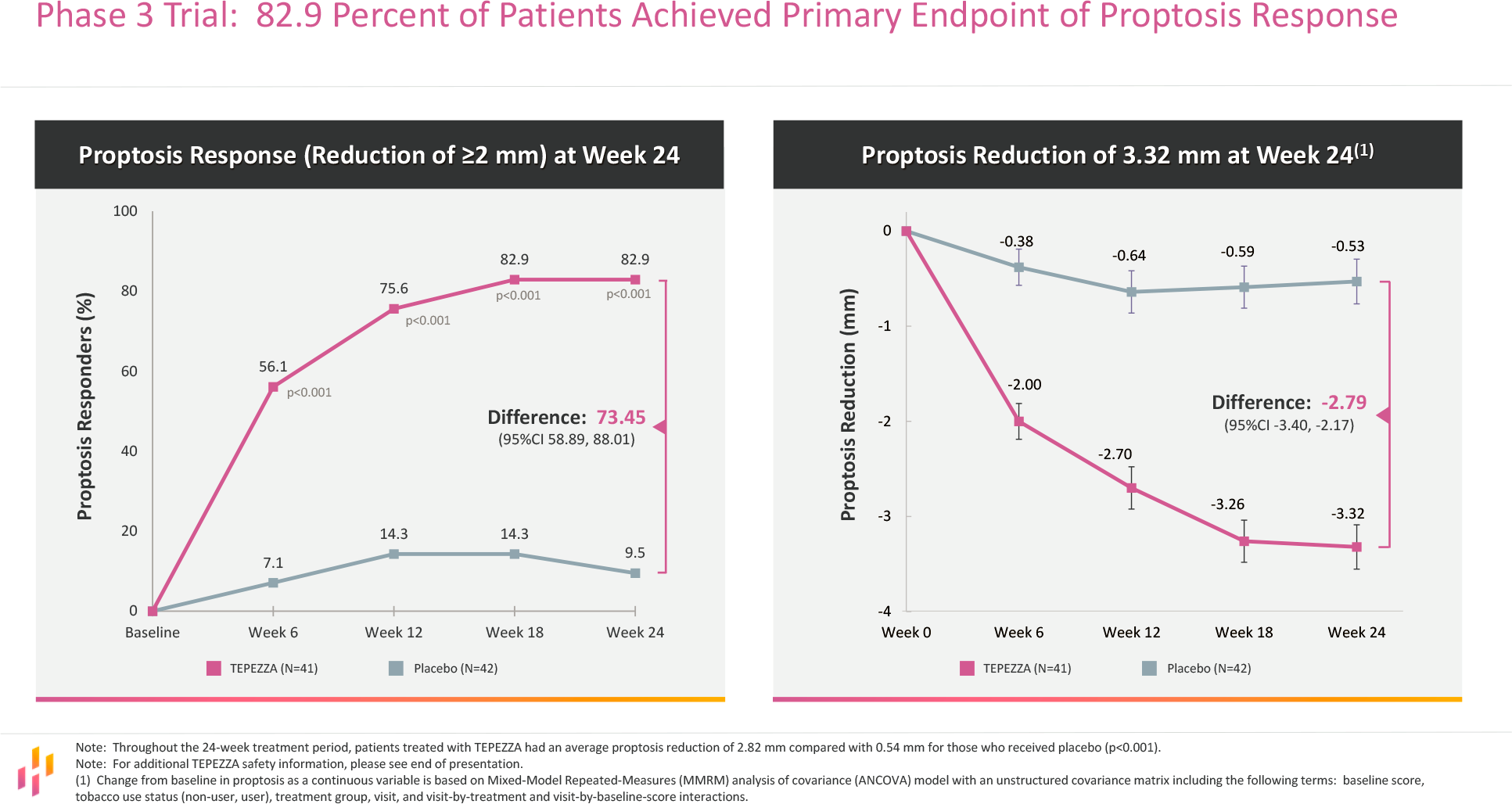
The primary endpoint was the proportion of subjects who gave a response to treatment, which was defined as a decrease in the clinical activity score (CAS) by at least 2 points and a decrease in proptosis in the study eye by at least 2 mm as well as no worsening of the above parameters in the eye that was not subjected to therapy.
In the teprotumumab groups, 71% and 83% of patients reached the declared criterion of therapy success — compared to 20% and 10% in the placebo groups in the first and second studies, respectively. The final difference with placebo was 51% (95% CI: 33 to 69) and 73% (95% CI: 59 to 88). The decrease in proptosis was the mean of 2.5 and 2.8 mm — versus the decrease of 0.2 and 0.5 mm in the control groups.
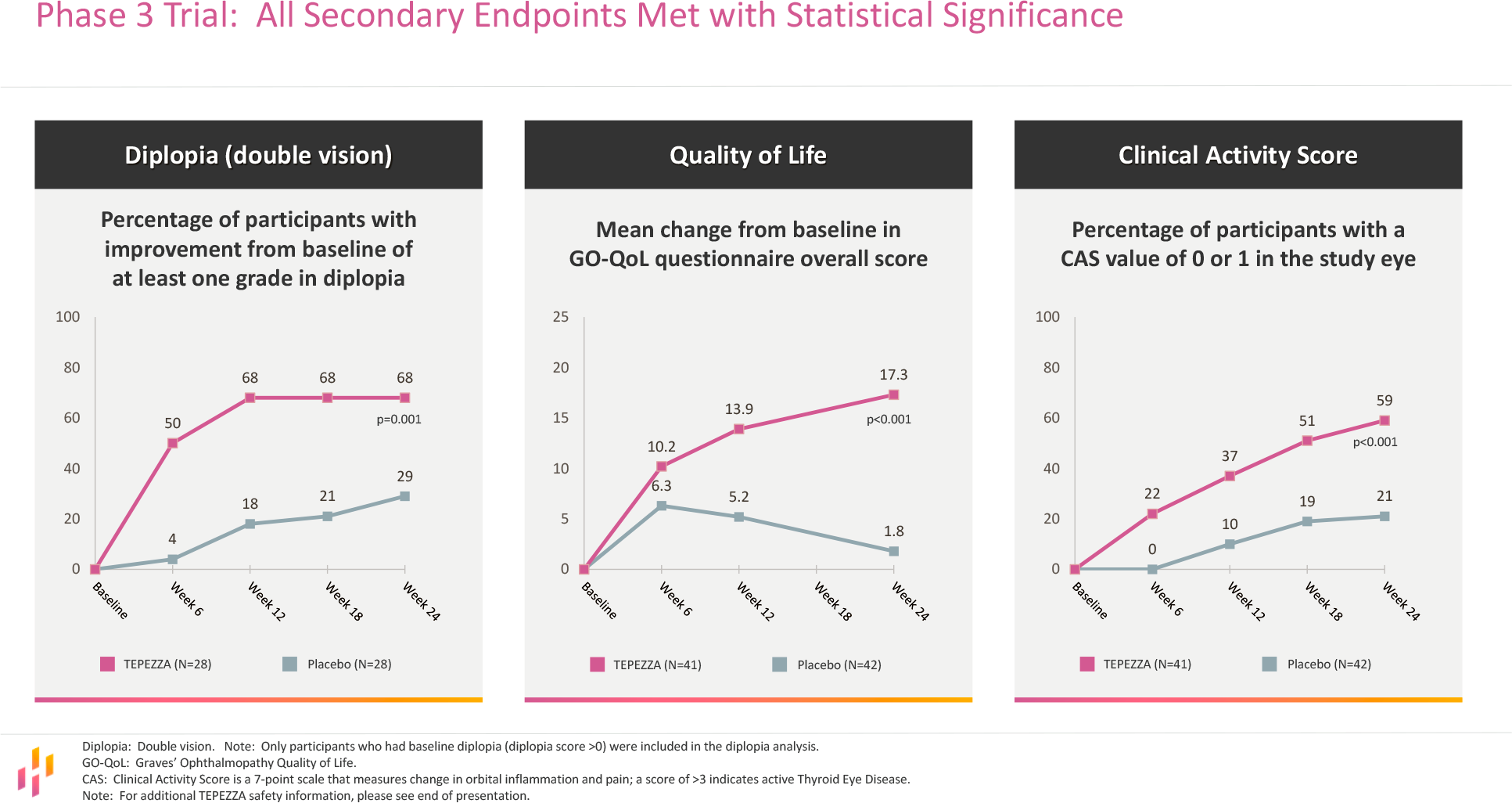
Administration of teprotumumab also improved secondary endpoints including the degree of diplopia (in 53% of patients it completely disappeared), quality of life, and CAS.

Moreover, the first study found that 53% and 67% of patients who recorded improvements in proptosis and diplopia, respectively, remained in response to therapy even after discontinuation, up to 51 weeks after the last teprotumumab infusion.
[twenty20 img1=”1160″ img2=”1161″ offset=”0.5″]The most common adverse events accompanying the use of teprotumumab were muscle spasms (25% of patients), nausea (17%), alopecia (13%), diarrhea (12%), fatigue (12%), hyperglycemia (10%), hearing impairment (10%), dysgeusia (8%), headache (8%), dry skin (8%).
Horizon is committed to conducting post-marketing clinical trials to, first, assess the frequency of need for retreatment with teprotumumab and, second, to further uncover the safety profile of the drug in a broader patient population (to understand the risk of experiencing a hyperglycemic event or exacerbation of a history of inflammatory bowel disease).
Update #1
The therapeutic effect of Tepezza is sustained over the long term. Thus, of those patients who completed the 24-week OPTIC (NCT03298867) pivotal clinical trial and completed a 48-week follow-up, 90% (n=18/20) did not receive any treatment for thyroid eye disease for the next 120 weeks.
Update #2
Tepezza re-prescribing for thyroid eye disease has been confirmed to help those patients who either did not respond to therapy during the first 24-week course or responded but then experienced a relapse (≥ 2 mm increase in proptosis and/or ≥ 2 increase in CAS) during the subsequent 48-week follow-up.
The OPTIC-X (NCT03461211) phase 3 clinical trial, which included the above patients from the OPTIC (NCT03298867) pivotal clinical trial and involved an additional 24-week course of Tepezza, showed that of 5 non-responding patients, 2 responded to treatment, 1 had a 1.5 mm decrease in proptosis (from baseline in OPTIC), and 2 discontinued treatment early. Of those patients (n=8) who experienced a relapse, 5 subjects (63%) responded to treatment (proptosis decreased by a mean of 3.3±0.7 mm).
Update #3
Real clinical practice for the treatment of thyroid eye disease has shown a high adherence of patients to the prescription of Tepezza. Thus, out of 1101 people who started a therapeutic course of 8 infusions of teprotumumab, over 90% passed it completely. Non-compliance with the treatment protocol was recorded in only 1% of patients and 8% of patients discontinued treatment due to adverse events.
Tepezza: Commercial Outlook of Teprotumumab for Thyroid Eye Disease
According to experts, the future of Tepezza appears cloudless. The fact is that traditional invasive surgical interventions for thyroid eye disease, aimed at correcting proptosis and diplopia, are usually not performed until the inflammation of the eye disappears and the disease progresses to the fibrosis stage.
Tepezza’s outlook and existing cash flow from sales of its existing portfolio of drugs, which generated $1.21 billion in 2019 and which includes the antigout drug Krystexxa (pegloticase), allow Horizon not to fear for its business stability. The company is willing to acquire or license any experimental drug compounds in sectors of interest, such as rheumatology, nephrology, endocrinology, and ophthalmology. That’s what happened in mid-March 2021 when at roughly $3 billion Horizon acquired Viela Bio which has Uplizna (inebilizumab) for the treatment of neuromyelitis optica spectrum disorder (NMOSD).
Nothing to say when Tepezza’s sales in 2020 were $820 million, significantly exceeding launch-year expectations. Indeed, EvaluatePharma has predicted that Tepezza sales will reach nearly half a billion dollars only by 2024. The launch of Tepezza has turned out to be one of the most successful rare disease medicine launches ever.
- Tepezza sales in 2021 were $1.66 billion. Peak global demand for Tepezza is expected to exceed $3.5 billion annually.
Horizon took control of teprotumumab in its takeover of River Vision Development for an upfront fee of $145 million in May 2017. The latter licensed the molecule from Roche which in turn obtained it from the originator, Danish Genmab.
In the second quarter of 2021, Horizon expects to initiate a randomized, placebo-controlled trial of Tepezza in patients with chronic thyroid eye disease. Chronic (previously referred to as inactive) thyroid eye disease is no longer progressive; however, significant disease manifestations such as proptosis and diplopia remain.
- The corresponding NCT04583735 phase 4 clinical trial has been started.
By mid-2021, Horizon is planning to initiate an exploratory trial of teprotumumab for diffuse cutaneous systemic sclerosis (dcSSc), a rare, chronic, fibrotic autoimmune disease in which excess collagen production causes large areas of skin to thickening and hardening, or fibrosis, over large areas of the body; usually the fingers, hands, arms, forearms, anterior trunk, legs, and face.
- It is being validated in the NCT04478994 phase 1 clinical trial.
Horizon also wishes to explore Tepezza’s subcutaneous formulation which could provide greater flexibility for patients and physicians. This will be done using ENHANZE, drug delivery technology by Halozyme Therapeutics.

Halozyme: Elegant Transformation of Drugs From Intravenous to Subcutaneous
Easy and quick administration of biological drugs. All for the convenience of patient care.
Tepezza: Market Competitors of Teprotumumab for Thyroid Eye Disease
The high bar of therapeutic efficacy set by teprotumumab leaves few chances for other pharma companies that are developing drugs to treat thyroid eye disease (TED).
Batoclimab
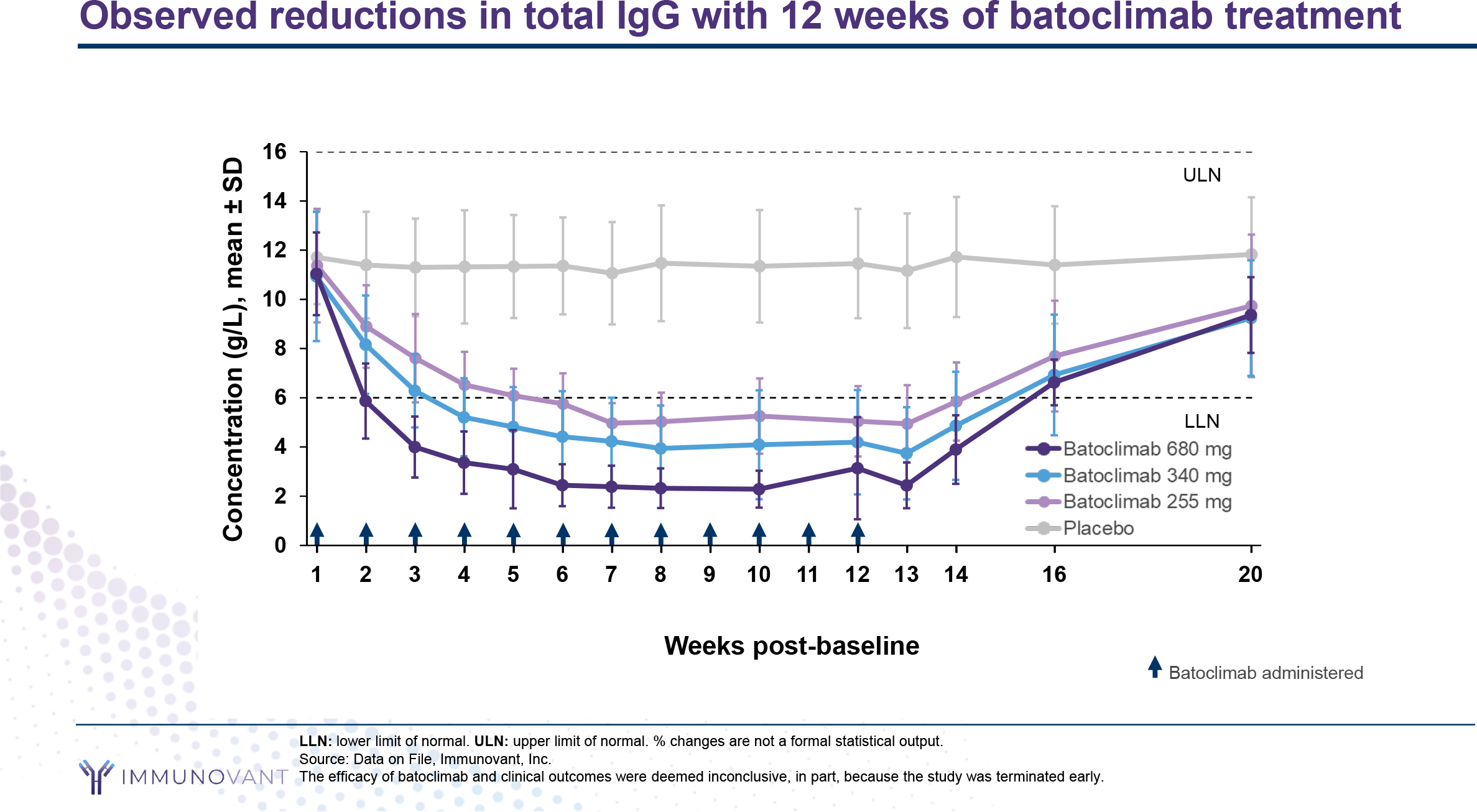
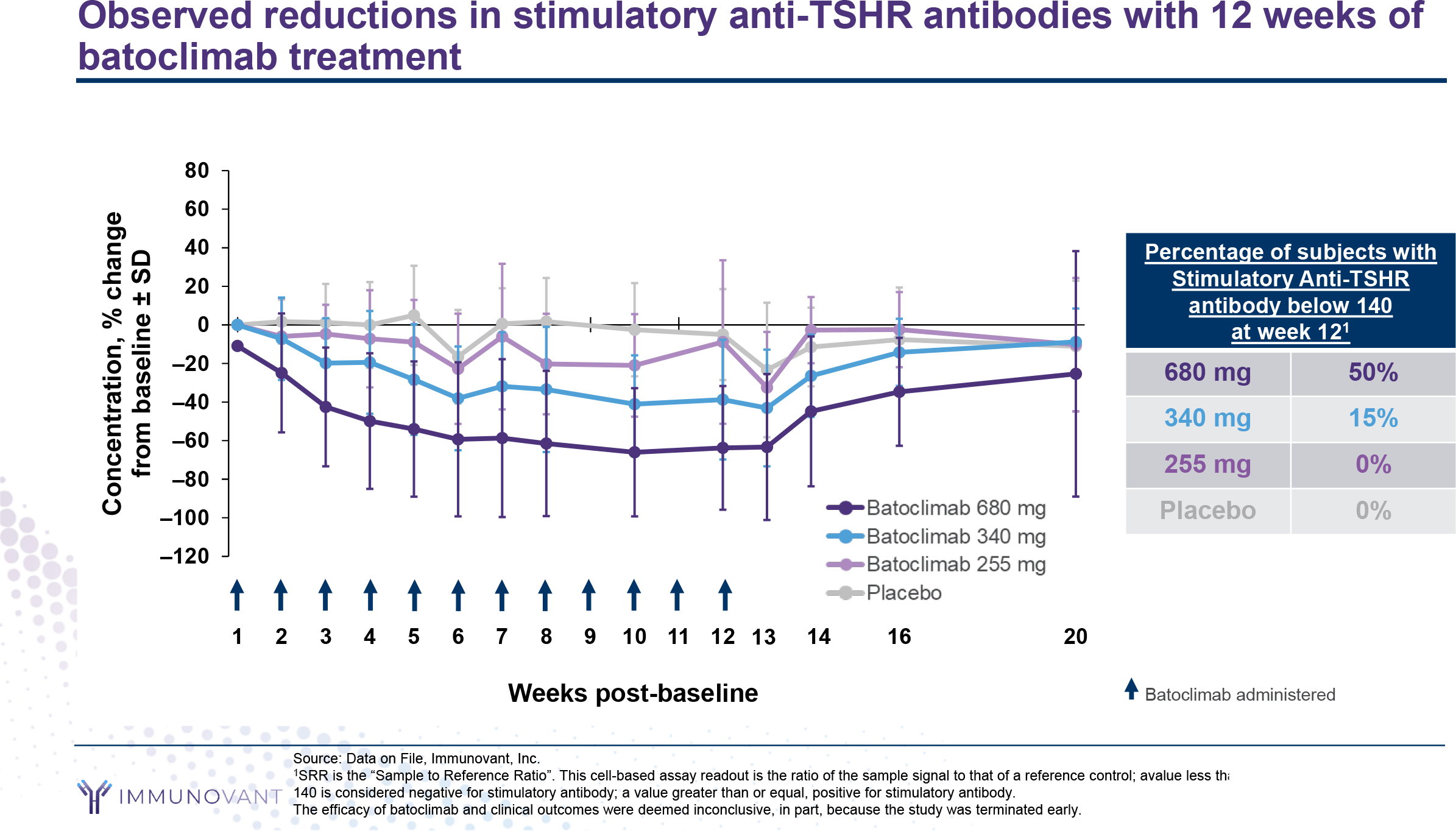
Immunovant, part of Roivant Sciences, is conducting ASCEND GO-1 (NCT03922321) and ASCEND GO-2 (NCT03938545) phase 2a and 2b clinical trials of the experimental batoclimab (IMVT-1401, RVT-1401), a fully human monoclonal antibody against the neonatal Fc receptor (FcRn). The latter actually rescues immunoglobulin G (IgG) from degradation by binding it to endosomes and returning it to the bloodstream, thereby prolonging its half-life. In autoimmune conditions, when the body mistakenly produces pathogenic IgG antibodies to its own tissues, FcRn contributes significantly to the chronic process by preventing lysosomal degradation of said IgG antibodies. Accordingly, it makes sense to block the interaction between FcRn and IgG.
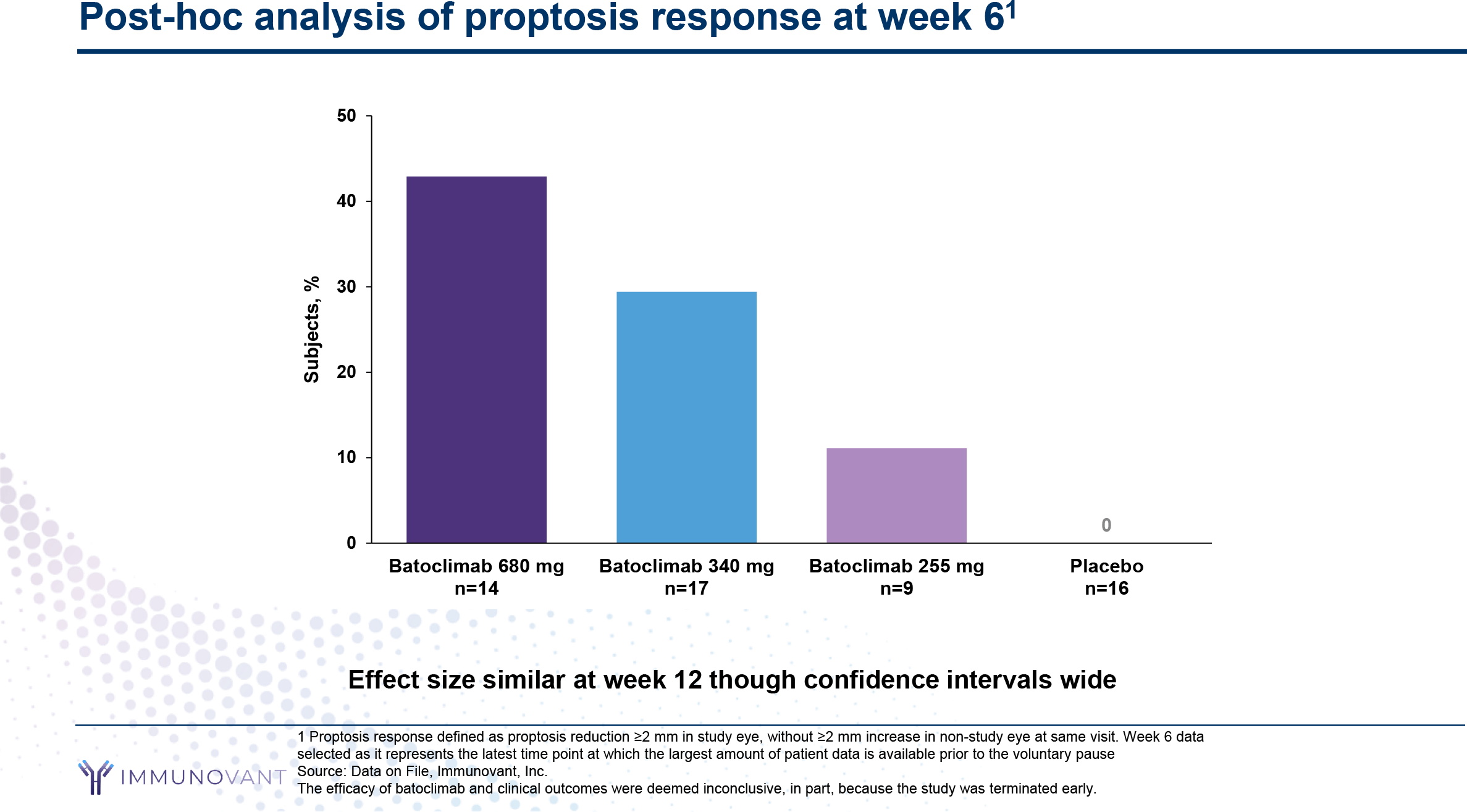
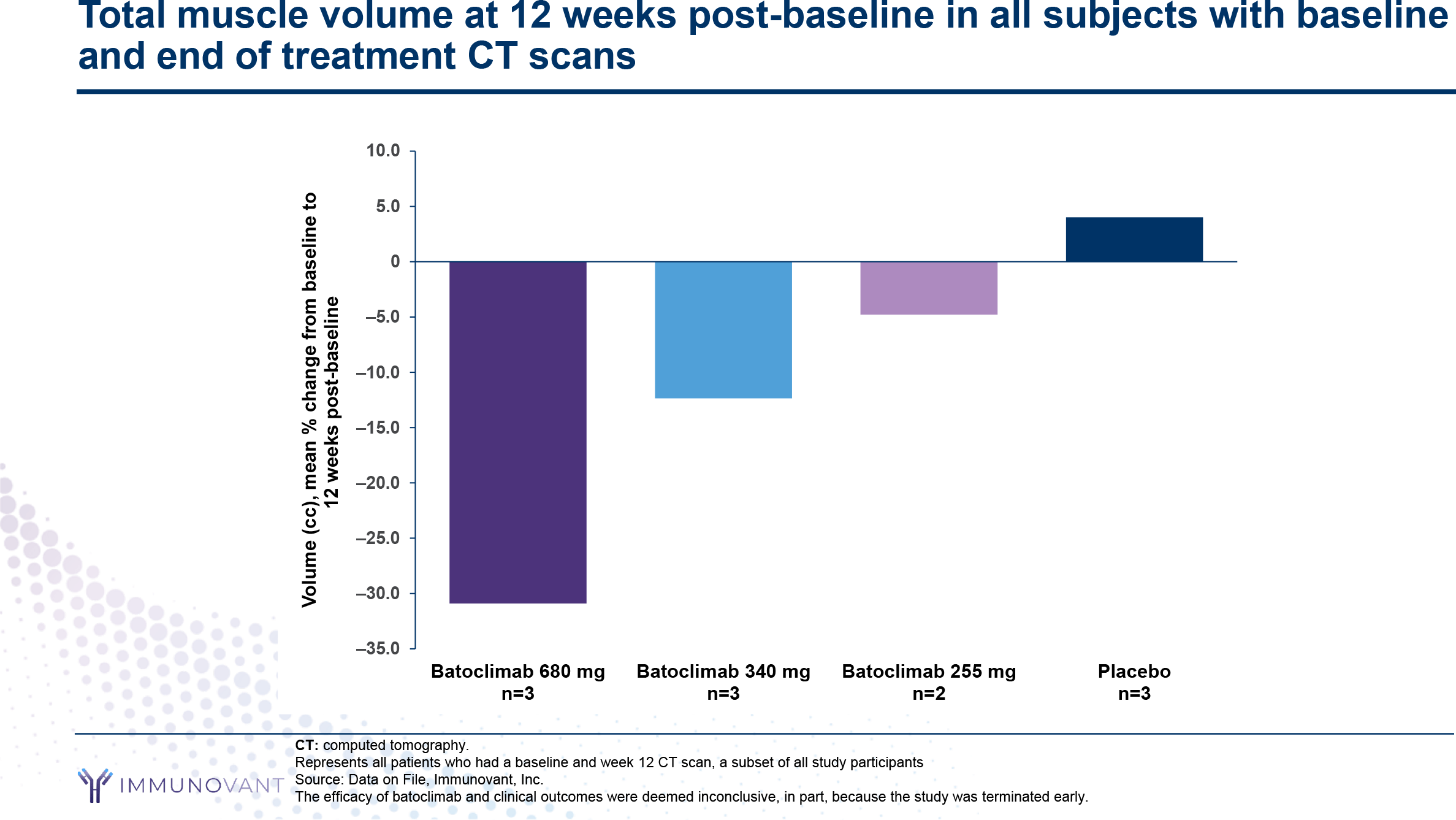
- ASCEND GO-1 was successfully completed, whereas ASCEND GO-2 had to be paused due to elevated total and low-density lipoprotein (LDL) cholesterol levels. Administration of batoclimab to patients with thyroid eye disease resulted in the following positive therapeutic changes. The average decrease in total IgG levels was 65%, a proper decrease in the concentration of antibodies against TSHR was recorded, 57% of patients showed an improvement of 2 points or more on the clinical activity score (CAS), 43% of subjects were in treatment-responsive status (reduction in proptosis by at least 2 mm).
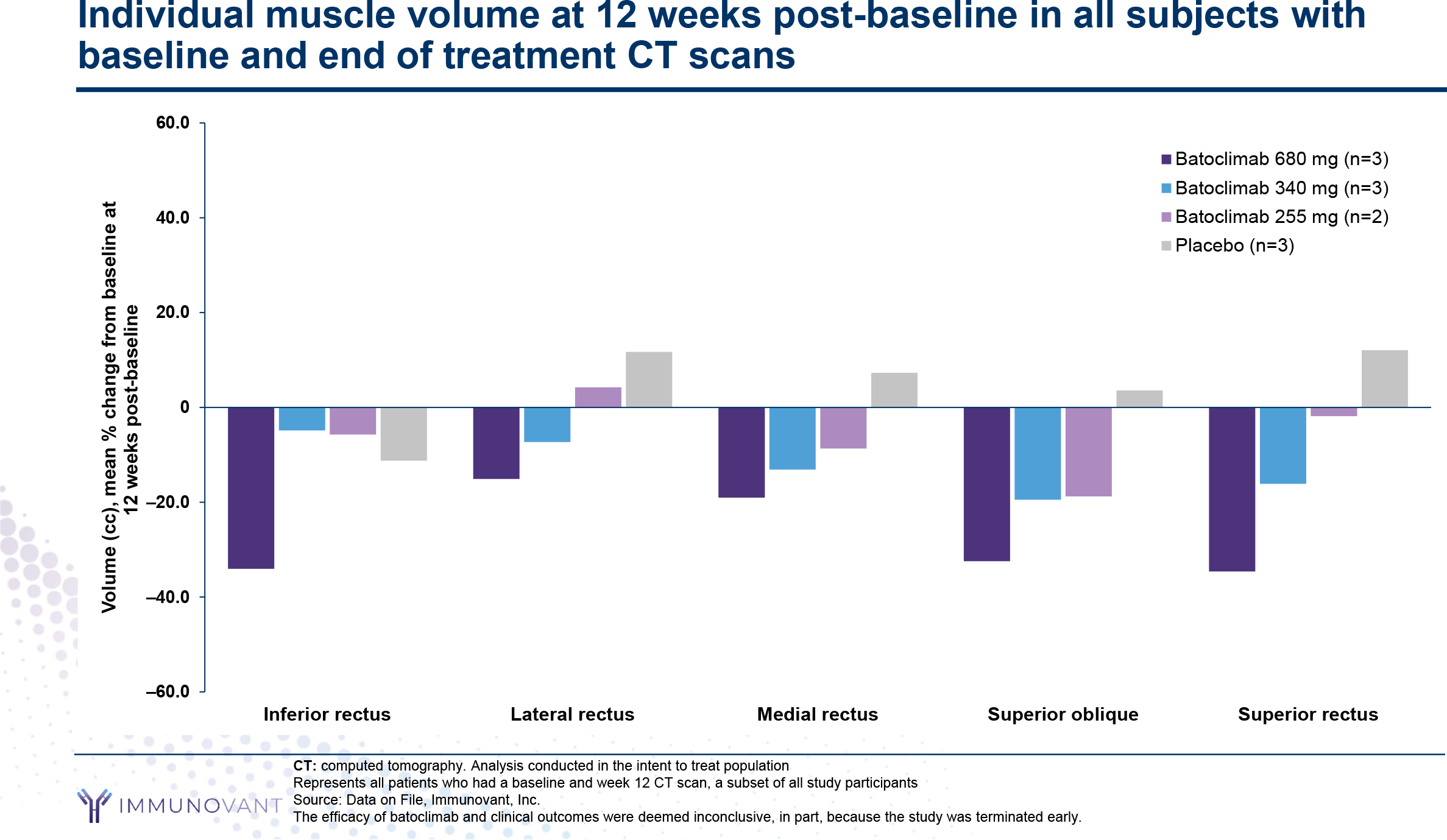
Two similarly designed phase 3 clinical trials, NCT05517421 and NCT05524571, are scheduled to begin in the second half of 2022 to test batoclimab in the treatment of moderate-to-severe TED. The drug will be administered by weekly subcutaneous injections for 24 weeks: 680 mg for the first 12 weeks and 340 mg for the next 12 weeks.
Iscalimab
Despite the success of the NCT02713256 phase 2 clinical trial, Novartis is not yet willing to continue developing iscalimab (CFZ533) for Graves’ disease. The Swiss pharma giant is interested in other autoimmune indications such as hidradenitis suppurativa (HS), kidney or liver transplantation, Sjögren’s syndrome, lupus nephritis (LN), and type 1 diabetes melitus. Iscalimab is a fully human monoclonal antibody that blocks CD40. The CD40-CD154 costimulatory signaling pathway (CD40L) is known to play a significant role in the pathogenesis of Graves’ disease by promoting the activation of autoreactive B cells and encouraging the formation and function of intrathyroid ectopic lymphoid structures.
WP1302/ATX-GD-59
Apitope International, a British-Belgian company that develops the first antigen-specific drug compounds of its class for the therapy of autoimmune diseases, has bet on so-called apitopes — epitopes that do not depend on antigen processing. These are soluble synthetic peptides that mimic naturally occurring epitopes and are designed to rebalance the immune system (return of tolerance to autoantigens). The apitopes are highly selective and modulate only target cells to avoid overall immune suppression. ATX-GD-59 is a peptide mixture of two different immunodominant TSHR apitopes; the drug suppresses CD4+ T cells and T-dependent cellular immune response.
- In the fall of 2021, China’s Worg Pharmaceuticals bought Apitope and will continue to develop WP1302 against Graves’ disease.
K1-70
The fate of K1-70, a fully human monoclonal autoantibody that binds TSHR and inhibits TSH and TSI stimulation of the latter, remains unknown. The autoantibody was isolated from peripheral lymphocytes of a patient with autoimmune thyroid disease and therefore represents a “natural” inhibitor of TSHR stimulation. Behind the molecule is the British AV7.
Extras
Tepezza (teprotumumab). Prescribing information. US. [PDF]
Horizon Therapeutics. Investor presentation. March 8, 2022. [PDF]
Tepezza. Horizon Therapeutics. FDA approval presentation. January 21, 2020. [PDF]
Teprotumumab for treatment of thyroid eye disease. Horizon Therapeutics. FDA Dermatologic and Ophthalmic Drug Advisory Committee (DODAC). December 13, 2019. [PDF]
Teprotumumab for treatment of thyroid eye disease. Sponsor briefing document. FDA Dermatologic and Ophthalmic Drug Advisory Committee (DODAC). December 13, 2019. [PDF]
Teprotumumab for treatment of thyroid eye disease. FDA briefing document. FDA Dermatologic and Ophthalmic Drug Advisory Committee (DODAC). December 13, 2019. [PDF]
Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020 Jan 23;382(4):341-352. [source]
Teprotumumab for thyroid-associated ophthalmopathy. N Engl J Med. 2017 May 4;376(18):1748-1761. [source]
A case of ulcerative colitis associated with teprotumumab treatment for thyroid eye disease. Am J Ophthalmol Case Rep. 2021 Mar 10. [source]
New-onset of inflammatory bowel disease in a patient treated with teprotumumab for thyroid associated ophthalmopathy. Ophthalmic Plast Reconstr Surg. 2021 Mar 8. [source]
Thyroid eye disease, teprotumumab, and hearing loss: an evolving role for otolaryngologists. Otolaryngol Head Neck Surg. 2021 Mar 30. [source]
Teprotumumab and hearing loss: hear the warnings. Orbit. 2021 Feb 23;1-2. [source]
A perspective on the current role of teprotumumab in treatment of thyroid eye disease. Ophthalmology. 2021 Apr 3. [source]
Pharmacokinetics and exposure-response relationship of teprotumumab, an insulin-like growth factor-1 receptor-blocking antibody, in thyroid eye disease. Clin Pharmacokinet. 2021 Mar 26. [source]
Teprotumumab: the first approved biologic for thyroid eye disease. Int Ophthalmol Clin. 2021 Apr 1;61(2):53-61. [source]
Early experience with the clinical use of teprotumumab in a heterogenous thyroid eye disease population. Ophthalmic Plast Reconstr Surg. 2021 Mar 8. [source]
Treatment of moderate to severe orbitopathy: current modalities and perspectives. Ann Endocrinol (Paris). 2021 Mar 4. [source]
Lessons learned from targeting IGF-I receptor in thyroid-associated ophthalmopathy. Cells. 2021 Feb 12;10(2):383. [source]
Targeting TSH and IGF-1 receptors to treat thyroid eye disease. Eur Thyroid J. 2020 Dec;9(Suppl 1):59-65. [source]
Teprotumumab treatment for thyroid-associated ophthalmopathy. Eur Thyroid J. 2020 Dec;9(Suppl 1):31-39. [source]
Graves’ orbitopathy: current concepts for medical treatment. Klin Monbl Augenheilkd. 2021 Jan;238(1):24-32. [source]
Immunovant. Corporate presentation. March 2022. [PDF]
Immunovant. R&D day. March 30, 2022. [PDF]