Highlights
Bristol-Myers Squibb has launched Camzyos (mavacamten), a new drug indicated for adult patients with symptomatic (NYHA class II–III) obstructive hypertrophic cardiomyopathy to improve function capacity and symptoms.
Camzyos, approved by the U.S. Food and Drug Administration (FDA) in late April 2022, is the first drug for the specific treatment of obstructive hypertrophic cardiomyopathy.
Hypertrophic cardiomyopathy is a disease in which the myocardium (heart muscle) abnormally hypertrophies (thickens). This causes the internal cavity of the left ventricle to shrink and its walls to lose elasticity, making it less able to relax and fill with blood. The limited pumping function of the heart is reflected by the progression of the disease with the development of debilitating symptoms (chest pain, fatigue, shortness of breath, syncope with exercise) and cardiac dysfunction (heart failure, atrial fibrillation, stroke, sudden death). So far, there are no specialized drugs targeting the pathophysiological processes underlying hypertrophic cardiomyopathy.
There are somewhere between 15–20 million hypertrophic cardiomyopathy patients worldwide, with 160,000–200,000 in the United States and the top five (EU5) most populous European countries (Germany, United Kingdom, France, Italy, Spain).
The cost of a one-year treatment for obstructive hypertrophic cardiomyopathy with Camzyos is $89,500 for U.S. patients. This is the list price, excluding discounts and rebates.
According to the US Institute for Clinical and Economic Review (ICER), the price of Camzyos should not exceed $15,000 per year, based on an optimal balance between treatment costs and the short-term health benefits of the drug. The ICER expert opinion came before Bristol-Myers Squibb disclosed the results of, first, long-term follow-up of patients treated with mavacamten and, second, its use in a severe form of obstructive hypertrophic cardiomyopathy requiring invasive septal reduction therapy. In other words, the ICER assessment needs revision; the bar for the optimal price of Camzyos may be raised.
Bristol-Myers Squibb estimates that mavacamten will cross the $4 billion annual sales threshold by 2029. Outside observers, however, are forecasting lower sales of $2.0 billion to $2.9 billion, apparently because of the complex dosing protocol for Camzyos and the close monitoring of its administration, which requires periodic visits to a hospital facility. Meanwhile, competitors are pushing harder, developing their own equally effective drugs.

What Is Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is a common cardiovascular disease characterized by hypertrophy of the nondilated left ventricle in the absence of any other cardiac or systemic disease (such as hypertension) that could explain the observed hypertrophy, microvascular dysfunction, and myocardial fibrosis.

The prevalence of hypertrophic cardiomyopathy is 0.2% in the general population (one person in every 500).
Left ventricular hypertrophy is defined by a maximal left ventricular free wall thickness ≥ 15 mm (in adults) and a wall thickness ≥ 2 standard deviations above the mean for age, sex, or body size (in children).
Histopathological features of hypertrophic cardiomyopathy include disorganization of muscle fibers and myocardial fibrosis due to microvascular ischemia and cell death.
Hypertrophic cardiomyopathy is caused mainly by inherited autosomal dominant mutations (over 1,400 of them) in ≥ 11 genes encoding thick and thin contractile myofilament proteins of the cardiac sarcomere. It can also be caused by de novo mutations.
Phenotypically, hypertrophic cardiomyopathy can be obstructive (70% of patients), with presence of left ventricular outflow tract (LVOT) obstruction, or nonobstructive (30% of patients).
Complications of hypertrophic cardiomyopathy include syncope, heart failure with reduced left ventricular ejection fraction, atrial fibrillation, and sudden death due to ventricular tachyarrhythmia.
Prognostically, many patients with hypertrophic cardiomyopathy have a normal life expectancy with little or no disability without the need for major therapeutic interventions. Most patients with nonobstructive hypertrophic cardiomyopathy do not transition to progressive heart failure.
Treatment of hypertrophic cardiomyopathy involves: low-intensity exercise, symptomatic medications (beta-blockers, calcium channel blockers [verapamil, diltiazem], sodium channel blockers [disopyramide], oral diuretics), implantable cardioverter defibrillators, major invasive interventions (permanent pacemaker implantation, septal myectomy, alcohol septal ablation, heart transplantation).
Camzyos: Mechanism of Action of Mavacamten
Mavacamten (MYK-461) is an oral slow-molecule compound that is a selective allosteric inhibitor of cardiac myosin ATPase and is designed to reduce the increased left ventricular contractility that is characteristic of the specific pathophysiology of hypertrophic cardiomyopathy.
Mavacamten, through modulation of cardiac myosin function (the motor protein that controls heart muscle contraction), reduces the number of excess actin–myosin cross-bridge formation in the myocardium. Mavacamten targets the sarcomere, where it is to both reduce the force of cardiac contractility and facilitate diastolic relaxation in hypertrophic cardiomyopathy patients. These functions together are thought to lead to improved reduced left ventricular compliance and reduced dynamic left ventricular outflow tract (LVOT) obstruction in hypertrophic cardiomyopathy patients.

Mavacamten was developed by MyoKardia in partnership with Sanofi, which withdrew from the project in January 2019 without explanation. Bristol-Myers Squibb completed its takeover of MyoKardia in November 2020, a purchase that cost $13.1 billion in cash.
By the way, Bristol-Myers Squibb additionally acquired MYK-224, which allows for more flexible dosing due to its improved pharmacokinetic profile compared to mavacamten, and danicamtiv (MYK-491), a cardiac myosin stimulator for the treatment of hereditary dilated cardiomyopathy.
Camzyos: Clinical Trials of Mavacamten
Obstructive Hypertrophic Cardiomyopathy
EXPLORER-HCM: Pivotal Study
The EXPLORER-HCM (NCT03470545) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial enrolled adult patients (n=251) with obstructive hypertrophic cardiomyopathy.
Among the main criteria for inclusion in the trial: peak left ventricular outflow tract (LVOT) gradient ≥ 50 mm Hg (at rest, after Valsalva manoeuvre or exercise), left ventricular ejection fraction (LVEF) ≥ 55%, heart failure NYHA functional class II or III, and resting oxygen saturation ≥ 90%.
Participants received daily oral placebo or mavacamten, the dose (2.5, 5, 10, or 15 mg) of which was titrated to achieve a target reduction in LVOT gradient less than 30 mm Hg and a mavacamten plasma concentration between 350 and 700 ng/mL.
The primary efficacy endpoint of treatment was established by a combined assessment of clinical response, stated as either an increase in peak oxygen consumption (pVO2) of at least 1.5 mL/kg/min, according to the cardiopulmonary exercise testing (CPET), with at least one NYHA functional class reduction, or an increase in pVO2 of at least 3.0 mL/kg/min without NYHA functional class worsening.
After 30 weeks, 37% of patients in the Camzyos group reached the primary endpoint — versus 17% in the placebo group: the difference was 19.4% (95% CI: 8.7 to 30.1; p=0.0005). When the results are broken down according to whether the improvements were symptomatic or cardiac in nature, they are as follows:
- Increase in pVO2 of ≥ 1.5 mL/kg/min with NYHA class improvement of ≥ 1: 33% of subjects in the mavacamten group vs. 14% in the placebo group — 19.3% difference (95% CI: 9.0 to 29.6)
- Increase in pVO2 of ≥ 3.0 mL/kg/min without NYHA class worsening: 24% vs. 11% — 12.6% difference (95% CI: 3.4 to 21.9)
- Increase in pVO2 of ≥ 3.0 mL/kg/min with NYHA class improvement of ≥ 1: 20% vs. 8% — difference 12.5% (95% CI: 4.0 to 21.0)

Among the secondary endpoints of treatment efficacy evaluated after 30 weeks of therapy:
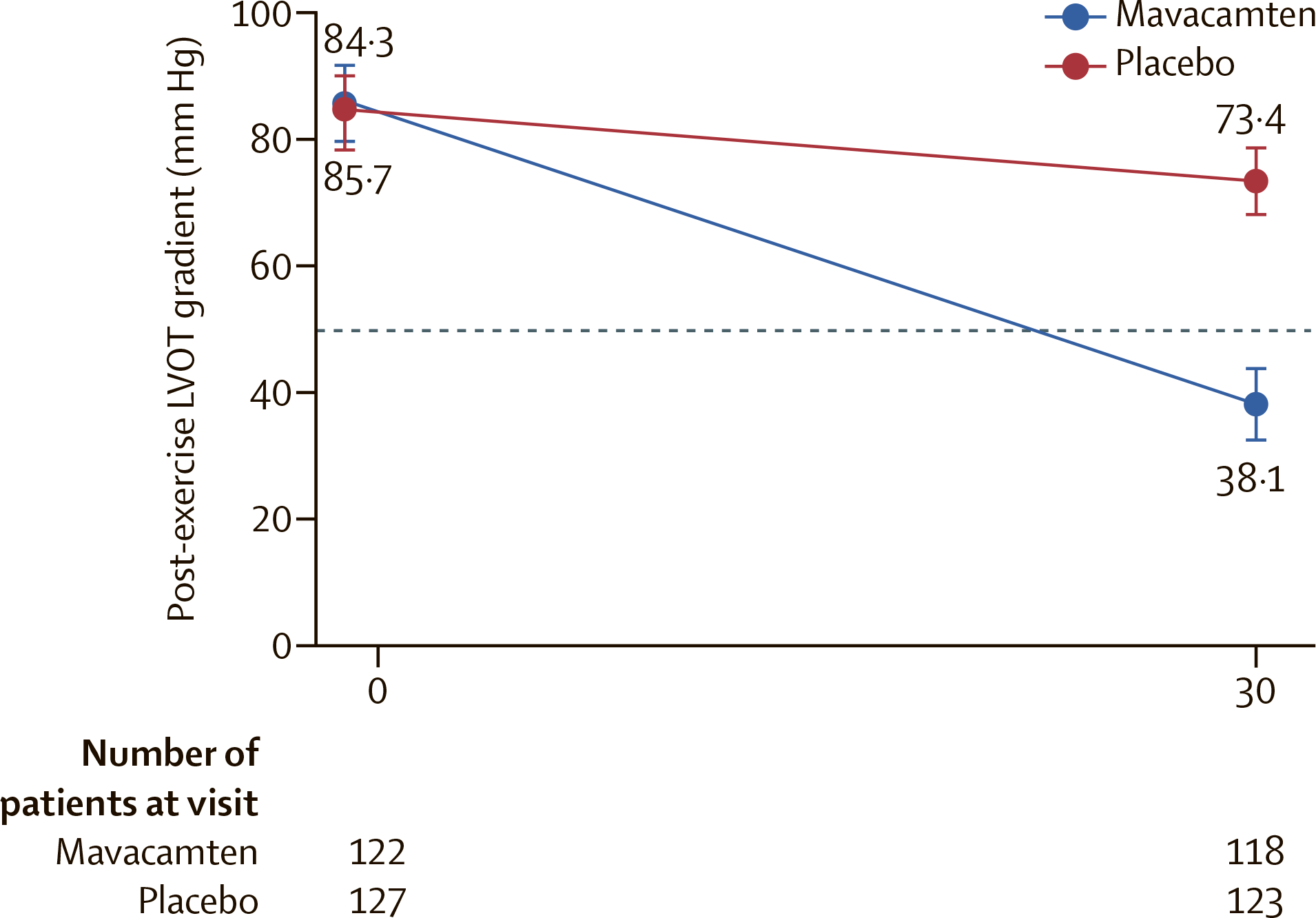
- Change in LVOT gradient after exercise, mm Hg (less is better): average of −47 among those receiving mavacamten vs. −10 in the control group. The difference was −35.6 (95% CI: −43.2 to −28.1; p<0.0001)
- Change in pVO2, mL/kg/min (more is better): mean 1.4 vs. −0.1 — difference 1.4 (95% CI: 0.6 to 2.1; p=0.0006)
- NYHA class improvement of ≥ 1: in 65% vs. 31% of patients — difference 34% (95% CI: 22 to 45; p<0.0001)
- Change in Kansas City Cardiomyopathy Questionnaire — Clinical Symptom Score (KCCQ-CSS) [more is better]: 13.6 vs. 4.2 — difference 9.1 (95% CI: 5.5 to 12.7; p<0.0001)
- Change in Hypertrophic Cardiomyopathy Symptom Questionnaire Shortness-of-Breath (HCMSQ-SoB) subscore (less better): −2.8 vs. −0.9 — difference −1.8 (95% CI: −2.4 to −1.2; p<0.0001)
Complete response, defined as a reduction in all LVOT gradients to less than 30 mm Hg with achievement of NYHA functional class I, was reported in 27% of patients taking mavacamten — versus 1% in the placebo group: a 26.6% difference (95% CI: 18.3 to 34.8).
Administration of mavacamten alleviated LVOT obstruction (post-exercise gradient < 30 mm Hg) in 57% of subjects — vs. 7%: difference 49.6% (95% CI: 39.3 to 34.8). Use of mavacamten reduced the post-exercise LVOT gradient to below the standard threshold at which septal reduction therapy is indicated (< 50 mm Hg) in 74% of patients — vs. 21%: difference 53.5% (95% CI: 42.0 to 65.0).

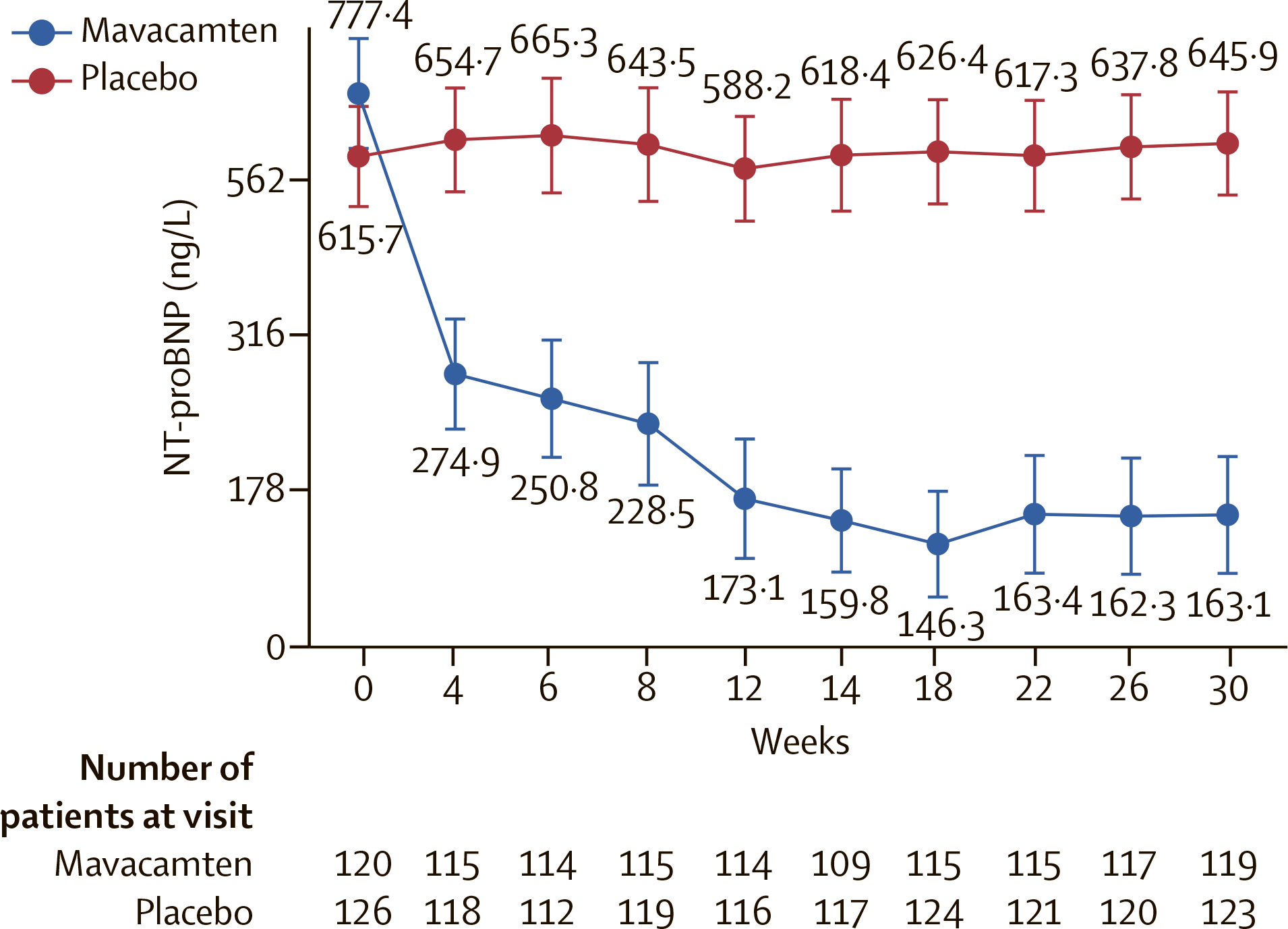
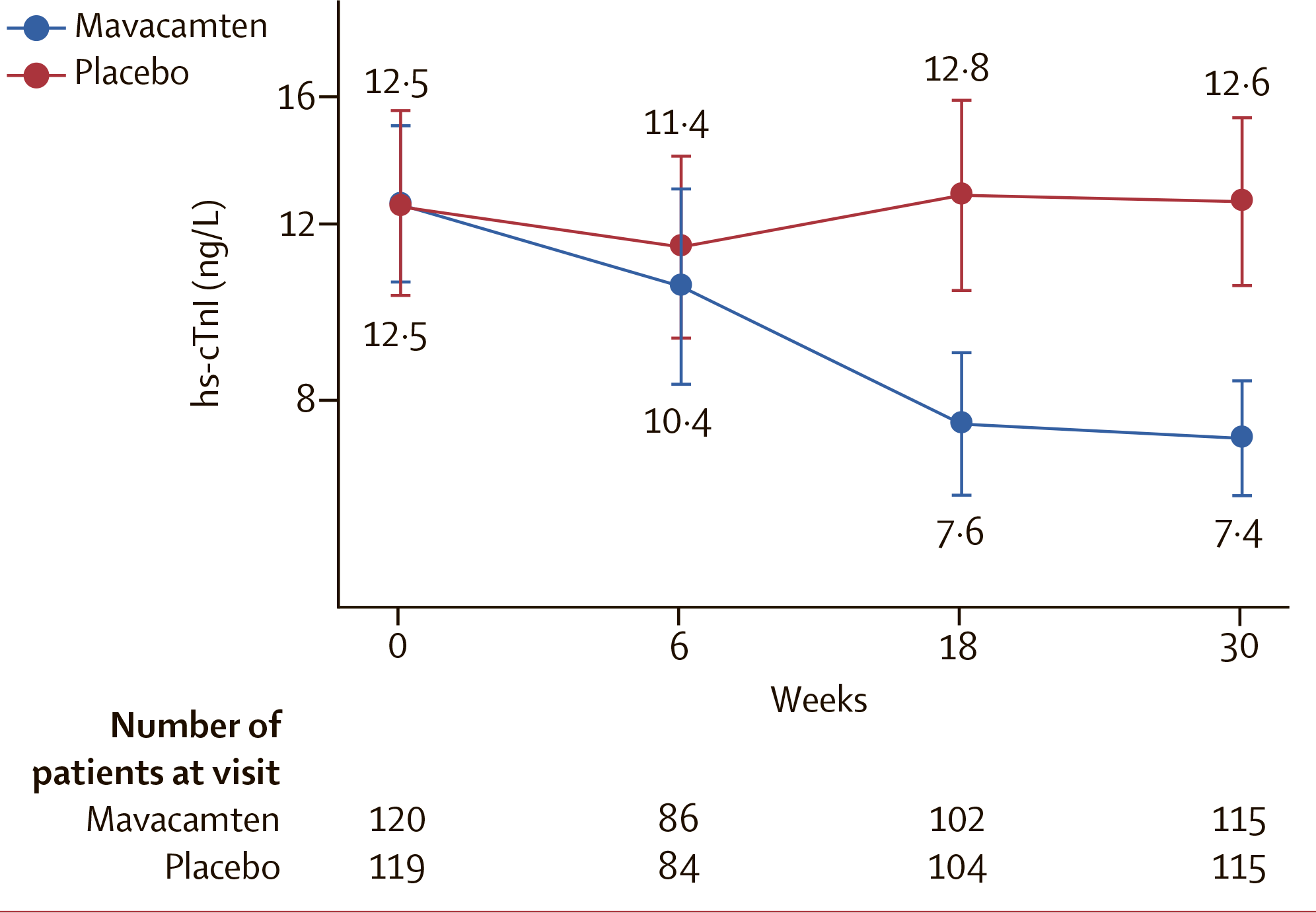
The decrease in cardiac biomarker serum levels in the Camzyos group proved to be rapid and sustained and paralleled the positive hemodynamic changes observed. Thus, the decrease in the N-terminal pro B-type natriuretic peptide (NT-proBNP) after treatment with mavacamten was 80% greater (at an absolute 614 ng/L) than with placebo, and the decrease in high-sensitivity cardiac troponin I (hs-cTnI) was 41% greater (at an absolute 5.1 ng/L).
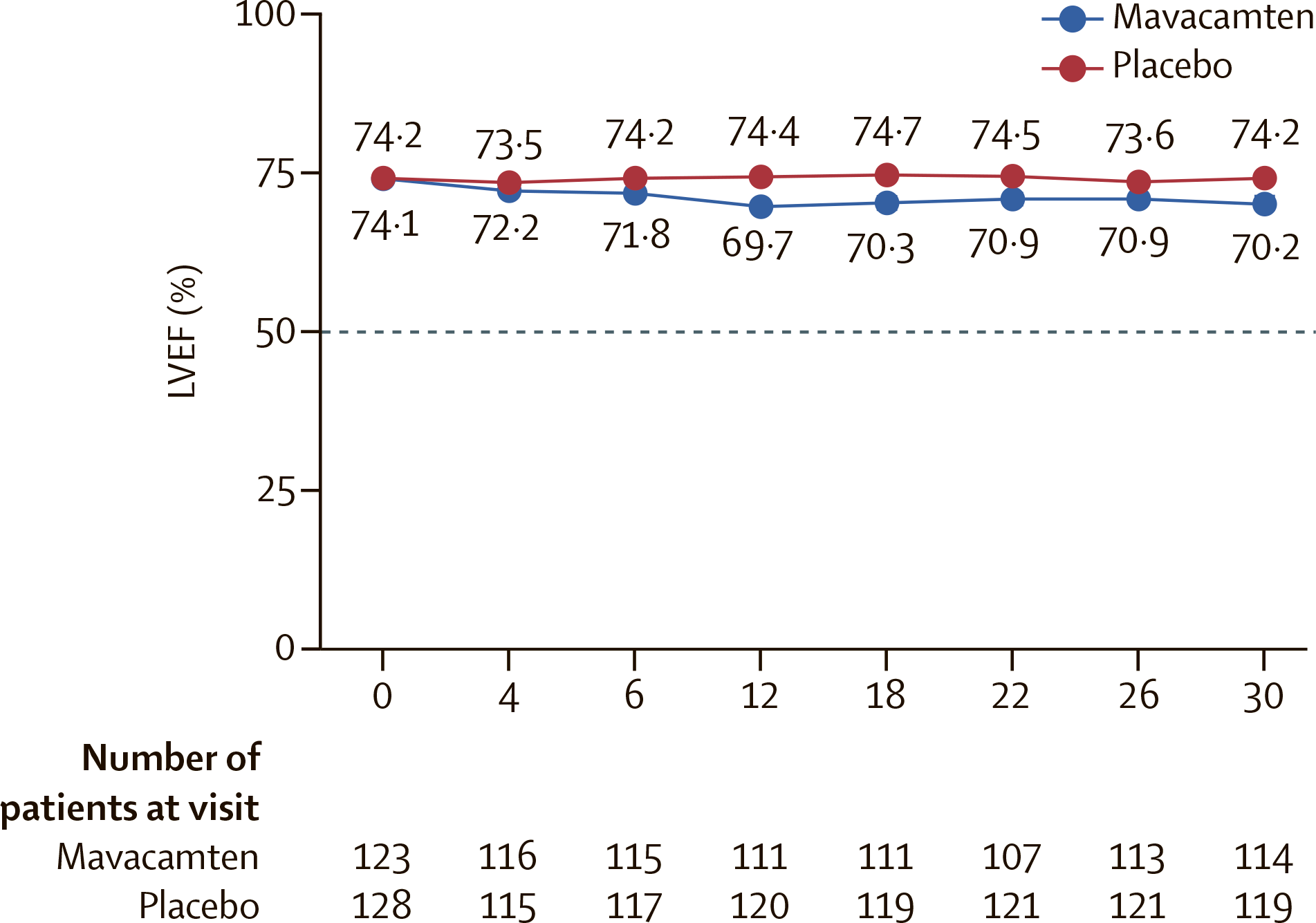
The treatment-emergent adverse events (TEAEs) were generally mild in severity. Serious adverse events occurred in 8% of patients in the mavacamten group and 9% in the placebo group. Among those receiving Camzyos such events included atrial fibrillation (2% of patients), syncope (2%), stress cardiomyopathy (2%), diverticulitis (1%), contusion (1%), forearm fracture (1%). Some patients (6%) receiving mavacamten had a transient decrease in LVEF to less than 50%, they had to stop treatment temporarily and then, after LVEF normalization, resume. The mavacamten and placebo groups did not differ in terms of changes in laboratory values, electrocardiography, or resting vital signs, including changes in heart rate and blood pressure from baseline.
- The prescribing information for Camzyos come with a black box warning regarding the risks of developing heart failure or complete blockage of ventricular function, since mavacamten reduces systolic contraction. Therefore, the patient’s clinical condition should be evaluated before prescribing Camzyos.
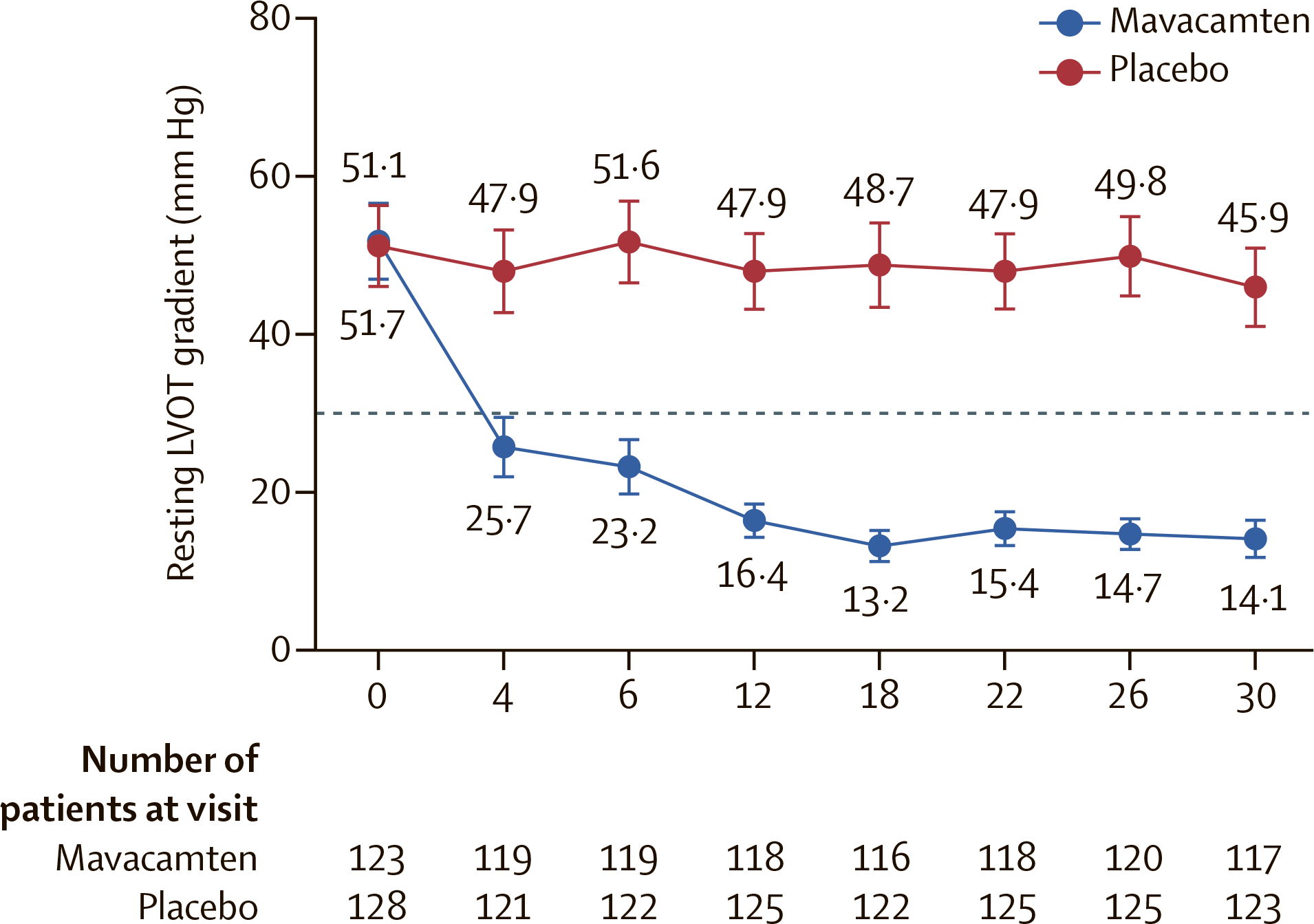
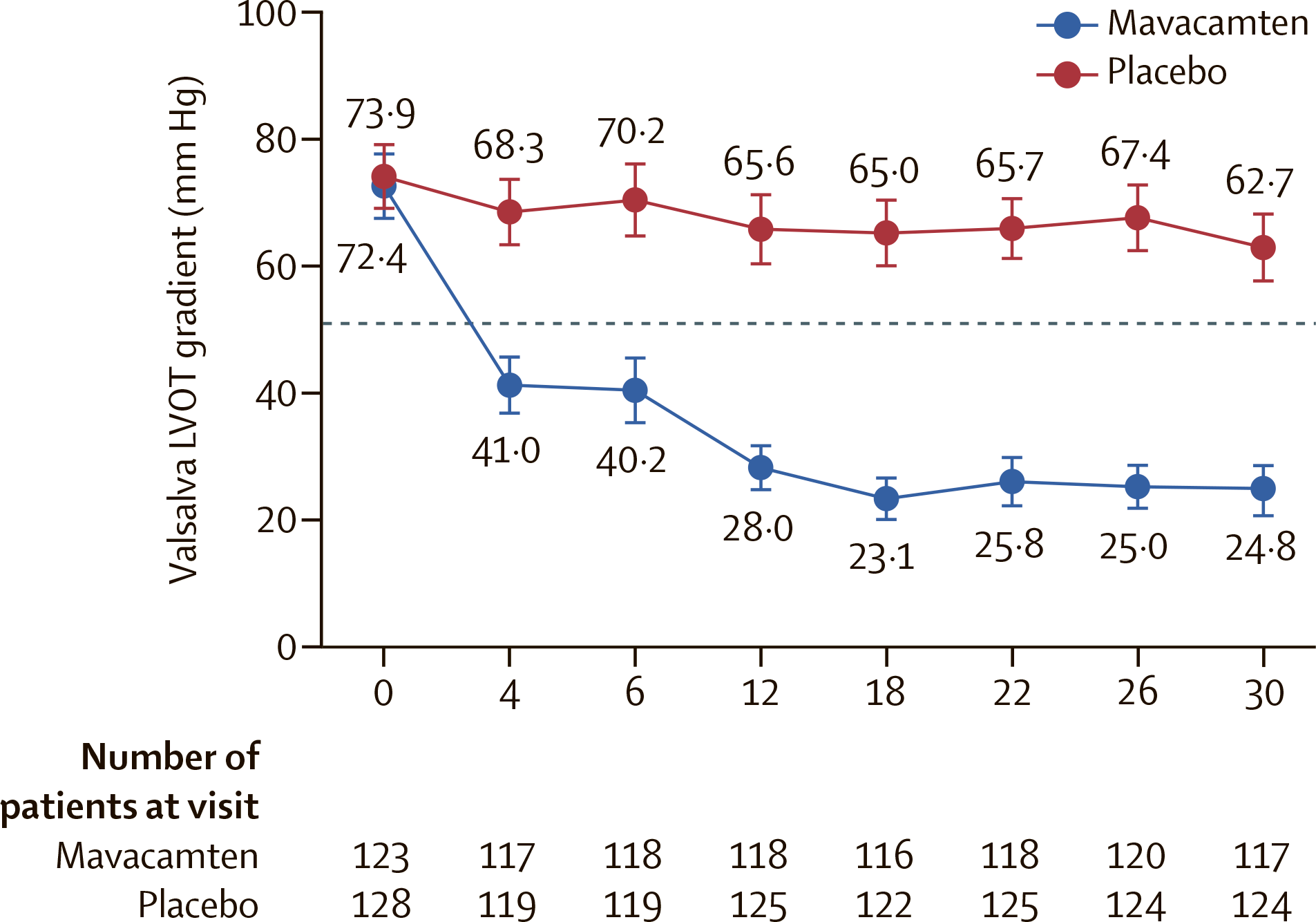
- As obstructive hypertrophic cardiomyopathy is treated with Camzyos, periodic echocardiographic assessment of the left ventricular ejection fraction (LVEF) and Valsalva left ventricular outflow tract (LVOT) gradient should be performed to make a validated decision about gradually increasing the dose of mavacamten to the target maintenance dose.
EXPLORER-LTE: Long-term Study
The MAVA-LTE (NCT03723655) phase 2/3 (non-randomized, open-label, multicenter, international) clinical trial organized a long-term 5-year safety and efficacy study of mavacamten among patients who completed the EXPLORER-HCM (NCT03470545) and MAVERICK-HCM (NCT03442764) clinical trials, the EXPLORER-LTE and MAVERICK-LTE cohorts respectively.
Participants were administered daily oral mavacamten with dose titration (2.5, 5, 10, or 15 mg).
The EXPLORER-LTE cohort demonstrated the following treatment efficacy results after 48 and 84 weeks:
- Change in resting LVOT gradient, mm Hg (less is better): mean of −36 and −33 at weeks 48 and 84
- Change in Valsalva LVOT gradient, mm Hg (less is better): mean of −45 and −46 at weeks 48 and 84
- Decrease in NT-proBNP levels, ng/L (more is better): median of −480 (interquartile range [IQR] −1104 to −179) and −488 (IQR −1098 to −166) at weeks 48 and 84
- Improvement in NYHA functional class ≥ 1: at week 48, 68% of patients, of whom 60% reported improvement by 1 class and 7% by 2 classes, with improvement beginning at week 12. In 31% of patients, the NYHA class did not change
- Resting LVEF change (less is better): mean of −7.0% and −9.0% at weeks 48 and 84
4% of participants discontinued therapy completely because of treatment-emergent adverse events (TEAEs), and 11% temporarily discontinued mavacamten for any reason and then resumed.
VALOR-HCM: Severe Disease
The ongoing VALOR-HCM (NCT04349072) phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial invited adult patients (n=112) with obstructive hypertrophic cardiomyopathy that is severe and requires invasive septal reduction therapy (SRT).
Among the main criteria for inclusion in the trial: peak left ventricular outflow tract (LVOT) gradient ≥ 50 mm Hg (at rest, after Valsalva manoeuvre or exercise), left ventricular ejection fraction (LVEF) ≥ 60%, heart failure NYHA functional class III or IV or class II with exertional syncope or near syncope, resting oxygen saturation ≥ 90%.
Participants received daily oral placebo or titrated dose of mavacamten (2.5, 5, 10, or 15 mg) — on the background of standard therapy from a maximum tolerated dose of beta-blockers, calcium channel blockers, and/or a sodium channel blocker (disopyramide).
The primary efficacy endpoint of treatment was stated to be a composite of the proportion of patients who decided to undergo SRT and the proportion of patients clinically still eligible for SRT.
The 16-week treatment found that administration of Camzyos resulted in a significantly lower proportion of subjects who reached the primary endpoint: 18% — versus 77% in the placebo group. The difference was 59% (95% CI: 43.9 to 73.9; p<0.0001).
Among other findings:
- Change in post-exercise LVOT gradient, mm Hg (less is better): mean of −39 among those receiving mavacamten and −1.8 in the control group (p<0.05)
- NYHA class improvement of ≥ 1: in 63% — versus 21% of patients (p<0.0001)
- NYHA class improvement of ≥ 2: in 27% — vs. 2% of patients (p<0.0001)
- Change in KCCQ-CSS [more is better]: 10.4 — vs. 1.9 (p<0.0001)
- Reduction in cardiac biomarkers NT-proBNP and hs-cTnI levels was 67% and 47% greater in the mavacamten group compared with the placebo group (p<0.0001)
The safety profile of mavacamten was characterized by acceptable tolerability. There were no cases of complete discontinuation of treatment due to a decrease in LVEF to ≤ 30%. No cases of serious adverse events such as congestive heart failure, syncope, and sudden cardiac death were reported.
The VALOR-HCM clinical trial continues with a 16-week double-blind phase followed by a 16-week open trial with all participants receiving mavacamten, followed by a long 96-week open trial.
Nonobstructive Hypertrophic Cardiomyopathy
MAVERICK-HCM: Preliminary Study
The MAVERICK-HCM (NCT03442764) phase 2 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled adult patients (n=59) with nonobstructive hypertrophic cardiomyopathy.
Among the main criteria for inclusion in the trial: peak left ventricular outflow tract (LVOT) gradient < 30 mm Hg (at rest, after Valsalva manoeuvre or exercise), left ventricular ejection fraction (LVEF) ≥ 55%, heart failure NYHA functional class II or III, elevated (≥ 300 pg/mL) levels of N-terminal pro B-type natriuretic peptide (NT-proBNP).
Participants were given daily oral placebo or mavacamten, the dose (2.5, 5, 10, or 15 mg) of which was titrated to achieve plasma concentrations of the drug between 200 ng/mL and 500 ng/mL.
After 16 weeks of treatment, NT-proBNP level decreased by geometric mean of 53% in the mavacamten group compared to 1% in placebo group or, in terms of absolute values, by 435 pg/mL and 6 pg/ml, respectively (p=0,0005).
The decrease in high-sensitivity cardiac troponin I (hs-cTnI) levels was a geometric mean of 34% in the mavacamten group — versus an increase of 4% in the control group, or, in terms of absolute values, −0.008 ng/mL and +0.001 ng/mL (p=0.009).
In terms of the outcome to a composite functional endpoint identical to the primary efficacy endpoint of treatment in EXPLORER-HCM (NCT03470545) clinical trial, there were no clear differences between the Camzyos and placebo groups (p>0.05). However, analysis of a subgroup of participants with baseline elevated hs-cTnI level or baseline averaged echo parameters of diastolic function (ratio between early mitral inflow velocity and mitral annular early diastolic velocity, E/e′) > 14 showed that 33% of patients receiving mavacamten reached it, whereas none in placebo group did it (p=0.03).
90% of patients treated with mavacamten experienced treatment-emergent adverse events (TEAEs). Among the most common were dizziness (in 17.9% of subjects), palpitation (15.4%), fatigue (12.8%). They were mostly mild-to-moderate in severity.
MAVERICK-LTE: Long-term Study
The MAVA-LTE (NCT03723655) phase 2/3 (non-randomized, open-label, multicenter, international) clinical trial organized a long-term 5-year safety and efficacy study of mavacamten among patients who completed the EXPLORER-HCM (NCT03470545) and MAVERICK-HCM (NCT03442764) clinical trials, the EXPLORER-LTE and MAVERICK-LTE cohorts respectively.
Participants were administered daily oral mavacamten with dose titration (2.5, 5, 10, or 15 mg).
The MAVERICK-LTE cohort demonstrated the following treatment efficacy results after 48 weeks:
- NT-proBNP levels decreased by a median of 67% (IQR −78 to −32)
- E/e′ ratio decreased by an average of 2.4±3.1 (95% CI: −3.6 to −1.3)
- Left atrial volume index (LAVI) decreased by a mean of 4.3±7.2 mL/m2 (95% CI: −6.7 to −1.9)
- LVEF changed by an absolute −5.4%±6.0% (95% CI: −7.4 to −3.4)
21% of patients temporarily discontinued treatment because the LVEF fell to less than 50%, with 16% symptomatically unaffected, and 17% returned to treatment (with a reduced dose of mavacamten) after the LVEF (≥ 50%) was restored.
Mavacamten: Competitive Landscape
Mavacamten’s direct competitor is aficamten (CK-3773274, CK-274), a cardiac myosin inhibitor that Cytokinetics is testing in the SEQUOIA-HCM (NCT05186818) phase 3 clinical trial in symptomatic obstructive hypertrophic cardiomyopathy. The trial will be completed by the fall of 2023. In the preceding REDWOOD-HCM (NCT04219826) phase 2 trial, aficamten was confidently confirmed to work, yielding no worse results than mavacamten.
Ninerafaxstat (IMB-101), partial fatty acid oxidation inhibitor (pFOX), being a key drug asset of Imbria Pharmaceuticals, increases myocardial metabolic efficiency. Ninerafaxstat is a cardiac myotrope that shifts myocardial substrate utilization in favor of glucose oxidation to produce more ATP per unit of oxygen consumed, thereby increasing cellular energy metabolism. Ninerafaxstat is being studied in the treatment of nonobstructive hypertrophic cardiomyopathy, angina due to obstructive coronary artery disease, and diabetic cardiomyopathy in the IMPROVE-HCM (NCT04826185), IMPROVE-Ischemia (NCT04826172), and IMPROVE-DiCE (NCT04826159) phase 2 clinical trials, respectively.
Novartis is trying its hand at expanding the prescribing range for Entresto/Yuperio (sacubitril + valsartan), a neprilysin inhibitor with angiotensin II receptor blocker. The NCT04164732 phase 2 clinical trial is testing the drug in the treatment of nonobstructive hypertrophic cardiomyopathy.
Univar Solutions, on the rails of the TEMPEST (NCT04706429) phase 2 clinical trial, is seeking to repurpose trientine, a copper chelating agent used in the treatment of Wilson’s disease, by targeting it against hypertrophic cardiomyopathy.
A gene therapy for hypertrophic cardiomyopathy caused by a mutation in myosin-binding protein C (MYBPC3) is in the early stages of development. In about 30%-40% of cases, the disease develops due to loss of function mutations of this particular gene. Tenaya Therapeutics is behind the creation of TN-201.
Mavacamten: Expert Comments
Current pharmacological approaches to the treatment of obstructive hypertrophic cardiomyopathy are exclusively symptomatic. Invasive procedures like septal reduction therapy (SRT), such as surgical septal myectomy and alcohol septal ablation, indicated in patients with symptoms intractable on maximum tolerated drug doses, are characterized by very decent efficacy, prolonging survival and improving quality of life. However, optimal results from SRT can only be achieved with well-trained medical personnel.
Mavacamten provides a dramatically new method of effective and patient-friendly (oral route of administration) treatment for obstructive hypertrophic cardiomyopathy.
The EXPLORER-HCM (NCT03470545) pivotal clinical trial has proven the unconditional therapeutic efficacy of Camzyos, confirming that the drug improves functional capacity both objectively (pVO2) and subjectively (NYHA class), and in a patient population representative of actual clinical practice.
The clinical effect was characterized by rapid onset and persistence, and it was achieved also with background administration of beta-blockers or calcium channel blockers. The concomitant reduction of serum concentrations of NT-proBNP and hs-cTnI, biomarkers reflecting cardiac wall stress and myocardial damage and prognostic for long-term outcomes, once again confirmed the therapeutic benefit of mavacamten in hypertrophic cardiomyopathy.
Camzyos was generally well tolerated, not particularly different from placebo in terms of safety. Because the mechanism of action of mavacamten is aimed at reducing increased myocardial contractility, there were concerns that use of the drug would result in dangerously low left ventricular ejection fraction (LVEF < 30%). In EXPLORER-HCM, none of the participants experienced such an event, although some had a drop in LVEF below 50%: they had to temporarily stop treatment, wait for LVEF to normalize, and then resume mavacamten at a reduced dose.
Bristol-Myers Squibb intends to address this problem with the Risk Evaluation and Mitigation Strategy (REMS): apparently, with dose titrated by periodic echocardiogram measurements.
The ongoing long-term cohort clinical trial MAVA-LTE (NCT03723655) has demonstrated the validity of continuous prescribing of mavacamten in symptomatic obstructive hypertrophic cardiomyopathy.
Camzyos has also confirmed that it can be a good alternative to the invasive interventions indicated for severe disease. At any rate, the 16-week VALOR-HCM (NCT04349072) demonstrated this, in passing testifying to the possibility of concomitant administration of mavacamten with disopyramide, although there were concerns about enhancing the negative inotropic effect.
The MAVERICK-HCM (NCT03442764) clinical trial of mavacamten laid the groundwork for a large-scale review of its suitability in the treatment of nonobstructive hypertrophic cardiomyopathy. Subsequent long-term testing of MAVA-LTE found a positive trend toward improved outcomes, left ventricular relaxation, and diastolic function based on changes in NT-proBNP, E/e′, and LAVI measures. It is possible that only a certain patient population characterized by a more severe, progression-prone disease will benefit therapeutically.
Finally, Bristol-Myers Squibb’s phase 2a EMBARK-HFpEF (NCT04766892) clinical trial is testing the hypothesis that mavacamten will establish itself in the treatment of a very specific heart disease — heart failure with preserved ejection fraction (HFpEF) in the presence of elevated NT-proBNP. And so a relevant phase 3 clinical trial is scheduled for launch in 2022.
Extras
Camzyos (mavacamten). Prescribing information. US. [PDF]
Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2020 Sep 12;396(10253):759-769. [source]
Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): Health status analysis of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2021 Jun 26;397(10293):2467-2475. [source]
Evaluation of mavacamten in symptomatic patients with nonobstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2020 Jun 2;75(21):2649-2660. [source]
Abstract 9685: Long-term efficacy and safety of mavacamten in patients with non-obstructive hypertrophic cardiomyopathy: Interim results from the MAVERICK-LTE cohort of the MAVA-LTE Study. [source]
The impact of mavacamten on the pathophysiology of hypertrophic cardiomyopathy: A narrative review. Am J Cardiovasc Drugs. 2022 Apr 18. [source]
Mavacamten: A novel disease-specific treatment for hypertrophic cardiomyopathy. Cardiol Rev. 2022 Mar 30. [source]
Myosin modulators: Emerging approaches for the treatment of cardiomyopathies and heart failure. J Clin Invest. 2022 Mar 1;132(5):e148557. [source]
Mavacamten for hypertrophic cardiomyopathy: Effectiveness and value. J Manag Care Spec Pharm. 2022 Mar;28(3):369-375. [source]
Effect of mavacamten on echocardiographic features in symptomatic patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol. 2021 Dec 21;78(25):2518-2532. [source]
Projecting the long-term clinical value of mavacamten for the treatment of obstructive hypertrophic cardiomyopathy in the united states: An assessment of net health benefit. Clin Ther. 2022 Jan;44(1):52-66.e2. [source]
Assessing health-related quality-of-life in patients with symptomatic obstructive hypertrophic cardiomyopathy: EQ-5D-based utilities in the EXPLORER-HCM trial. J Med Econ. Jan-Dec 2022;25(1):51-58. [source]
Myosin modulation in hypertrophic cardiomyopathy and systolic heart failure: Getting inside the engine. Circulation. 2021 Sep 7;144(10):759-762. [source]
Mavacamten — a new disease-specific option for pharmacological treatment of symptomatic patients with hypertrophic cardiomyopathy. Kardiol Pol. 2021;79(9):949-954. [source]
From genetic mutations to molecular basis of heart failure treatment: An overview of the mechanism and implication of the novel modulators for cardiac myosin. Int J Mol Sci. 2021 Jun 21;22(12):6617. [source]
Pathophysiology and treatment of hypertrophic cardiomyopathy: New perspectives. Curr Heart Fail Rep. 2021 Aug;18(4):169-179. [source]
Mavacamten, a novel therapeutic strategy for obstructive hypertrophic cardiomyopathy. Curr Cardiol Rep. 2021 Jun 3;23(7):79. [source]
Myosin modulators: The new era of medical therapy for systolic heart failure and hypertrophic cardiomyopathy. Cardiol Res. 2021 Jun;12(3):146-148. [source]