Highlights
Kerendia (finerenone) is a new drug indicated for adult patients with chronic kidney disease (CKD) associated with type 2 diabetes mellitus and is intended to reduce the following risks: sustained decline of estimated glomerular filtration rate (eGFR), development of end-stage kidney disease (ESKD), cardiovascular death, nonfatal myocardial infarction, and hospitalization for heart failure.
Kerendia, approved by the U.S. Food and Drug Administration (FDA) in July 2021, is developed by Bayer.
In February 2022, the European Medicines Agency (EMA) granted Kerendia marketing authorization: finerenone is approved for the treatment of adult patients with chronic kidney disease (stage 3 and 4 with albuminuria) associated with type 2 diabetes.
Kerendia will take its rightful place in the pharmacological armamentarium in the fight against diabetic kidney disease (DKD). Industry observers forecast that finerenone will be a blockbuster by 2026, reaching $1.2 billion in annual sales.

Chronic Kidney Disease and Diabetes
Type 2 diabetes mellitus is the leading cause of chronic kidney disease (CKD) worldwide. [1] There are over 200 million patients who suffer from CKD and diabetes at the same time [2] [3] [4] and, when paired, these diseases shorten life expectancy by 16 years. [5] Up to 40% of diabetics end up with CKD. [6]
International guidelines for the treatment of CKD in patients with type 2 diabetes recommend controlling hypertension and hyperglycemia and using renin–angiotensin system (RAS) blockers such as angiotensin-converting-enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs). Recently, recommendations for the use of sodium/glucose cotransporter 2 (SGLT2) inhibitors have been added. [7] [8]. Nevertheless, despite the recommended treatment, the risk of progression of CKD remains [9], and therefore new therapies are needed.
Kerendia: Mechanism of Action of Finerenone
Finerenone (BAY 94-8862) is an oral small-molecule highly selective non-steroidal mineralocorticoid receptor (MR) antagonist.
Evidence suggests a pathophysiological role for excessive activation of mineralocorticoid receptors in cardiorenal diseases, including CKD and diabetes: the inflammation and fibrosis it mediates lead to progressive renal and cardiovascular dysfunction. [1] [2] [3] [4]
Suppression of aldosterone- and cortisol-induced MR overactivity leads to inhibition of the pathological processes of inflammation, fibrosis, blood pressure increase, and ventricular hypertrophy.
Unlike all existing MR blockers such as spironolactone, eplerenone, or canrenone, finerenone has a unique pharmacological profile. [5]
First, finerenone does not affect glucocorticoid, androgen, progesterone, or estrogen receptors in any way, thus avoiding common MR antagonist side effects such as gynecomastia, impotence, and decreased libido.
Second, finerenone is not a steroid (it is a dihydropyridine derivative), which allows it to bind with high affinity to MR and more effectively suppress transcriptional coactivators involved in the expression of hypertrophic and profibrotic genes.
Third, finerenone is relatively equally distributed between cardiac and renal tissues.
In preclinical models finerenone had more potent anti-inflammatory and antifibrotic effects than steroidal MR antagonists. [6] [7] [8] [9]
Finerenone reduced the urinary albumin-to-creatinine ratio (UACR) in patients with chronic kidney disease receiving renin–angiotensin system blockers, while having less effect on serum potassium levels than spironolactone. [10] [11]
Kerendia: Efficacy and Safety of Finerenone for Diabetic Kidney Disease
Bayer has conducted two large-scale clinical trials of finerenone in diabetic kidney disease (DKD). One clinical trial examined Kerendia in type 2 diabetes mellitus with advanced chronic kidney disease (CKD): mainly at stage 3 or 4 and with severe albuminuria. A second study tested Kerendia among diabetics with less advanced CKD: either stage 2–4 and moderate albuminuria or stage 1–2 and severe albuminuria.
FIDELIO-DKD
The FIDELIO-DKD (NCT02540993) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial invited adult patients (n=5674) with diabetic nephropathy and persistent high albuminuria.
Among the main inclusion criteria:
- type 2 diabetes mellitus
- chronic kidney disease
- either persistent high albuminuria (urinary albumin-to-creatinine ratio [UACR] between 30 and 300 mg/g), estimated glomerular filtration rate (eGFR) between 25 and 60 mL/min/1.73 m2 and diabetic retinopathy, or persistent very high albuminuria (UACR ≥ 300 mg/g) and eGFR between 25 and 75 mL/min/1.73 m2
- previous treatment with angiotensin-converting-enzyme (ACE) inhibitors and/or angiotensin II receptor blockers (ARBs)
- serum potassium ≤ 4.8 mmol/L.
Among the main characteristics of the subjects:
- mean age 66 years, 70% male
- mean eGFR 44 mL/min/1.73 m2, 55% had eGFR below 45 mL/min/1.73 m2
- median UACR 852 mg/g (interquartile range [IQR] 446–1634)
- 46% had a history of atherosclerotic cardiovascular disease
- 99.8% were receiving ACE inhibitors or ARBs
- 97% were on antidiabetic therapy: 64% received insulin, 44% metformin, 7% glucagon-like peptide-1 receptor (GLP-1) agonists, 5% sodium/glucose cotransporter 2 (SGLT2) inhibitors
- 74% were on statins, 57% antiaggregants.
Participants received placebo or finerenone daily on top of standard therapy involving hypoglycemic drugs and a maximum tolerated dose of ACE inhibitors or ARBs.
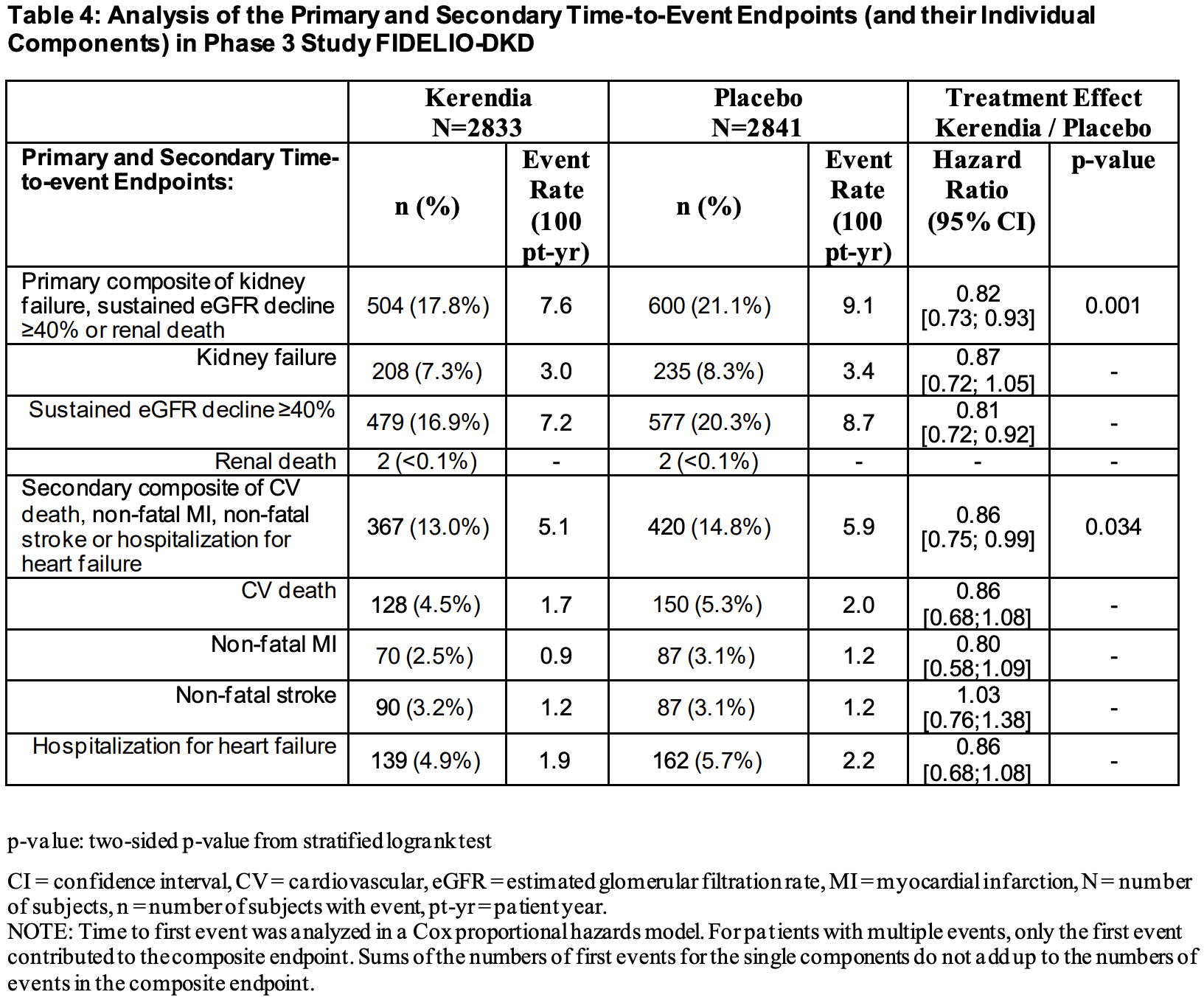
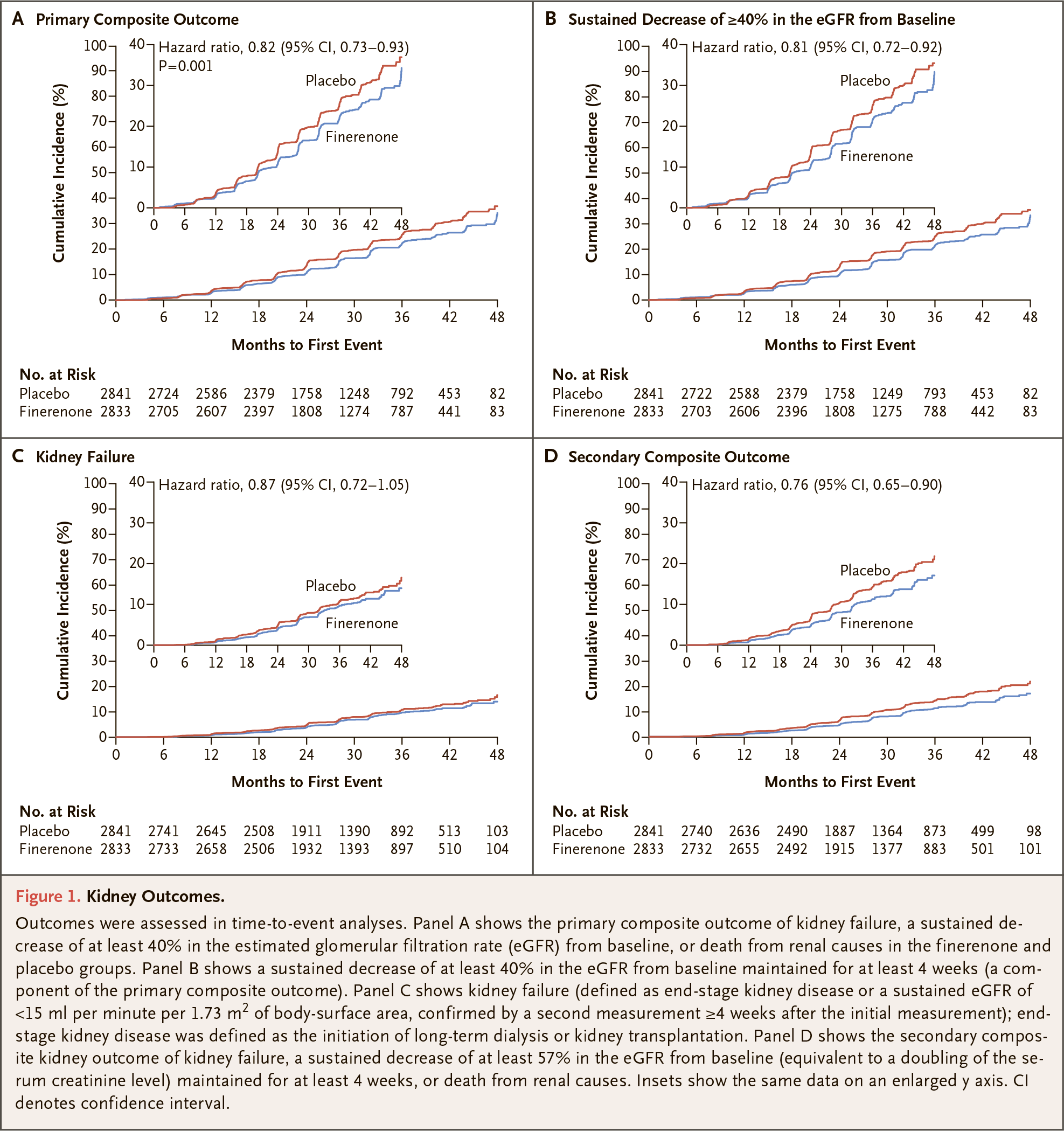
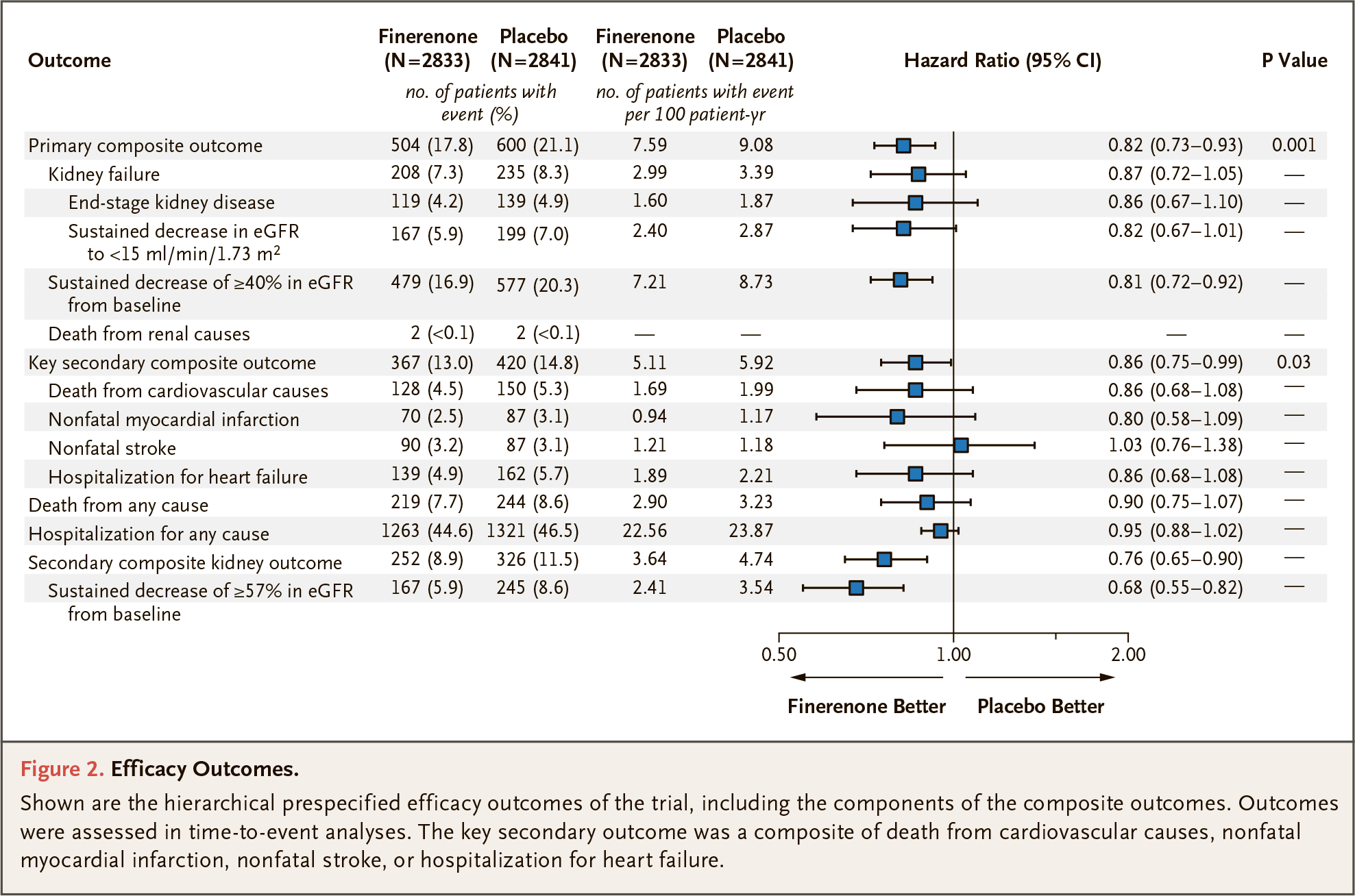
During the 2.6-year follow-up, finerenone slowed the progression of chronic kidney disease by providing a statistically significant delay in the time to first occurrence of kidney failure, a sustained decrease of eGFR (by 40% or more over a minimum of 4 consecutive weeks), or renal death. There was an 18% reduction in the probability of said composite risk compared with placebo: a hazard ratio (HR) of 0.82 (95% CI: 0.73–0.93; p=0.001).
In terms of individual event risk reductions, it was 13% (HR 0.87 [95% CI: 0.72–1.05]) for kidney failure and 19% (HR 0.81 [95% CI: 0.72–0.92]) for sustained decrease of eGFR.
Finerenone statistically significantly attenuated the composite risk of cardiovascular events (cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) by 14% relative to placebo (HR 0.86 [95% CI: 0.75–0.99; p=0.034]).
The incidence of individual events was lower with finerenone than with placebo, with the exception of nonfatal stroke, the incidence of which was similar in both groups. Thus, the hazard ratios for cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, and hospitalization for heart failure were 0.86 (95% CI: 0.68–1.08), 0.80 (95% CI: 0.58–1.09), 1.03 (95% CI: 0.76–1.38), and 0.86 (95% CI: 0.68–1.08).
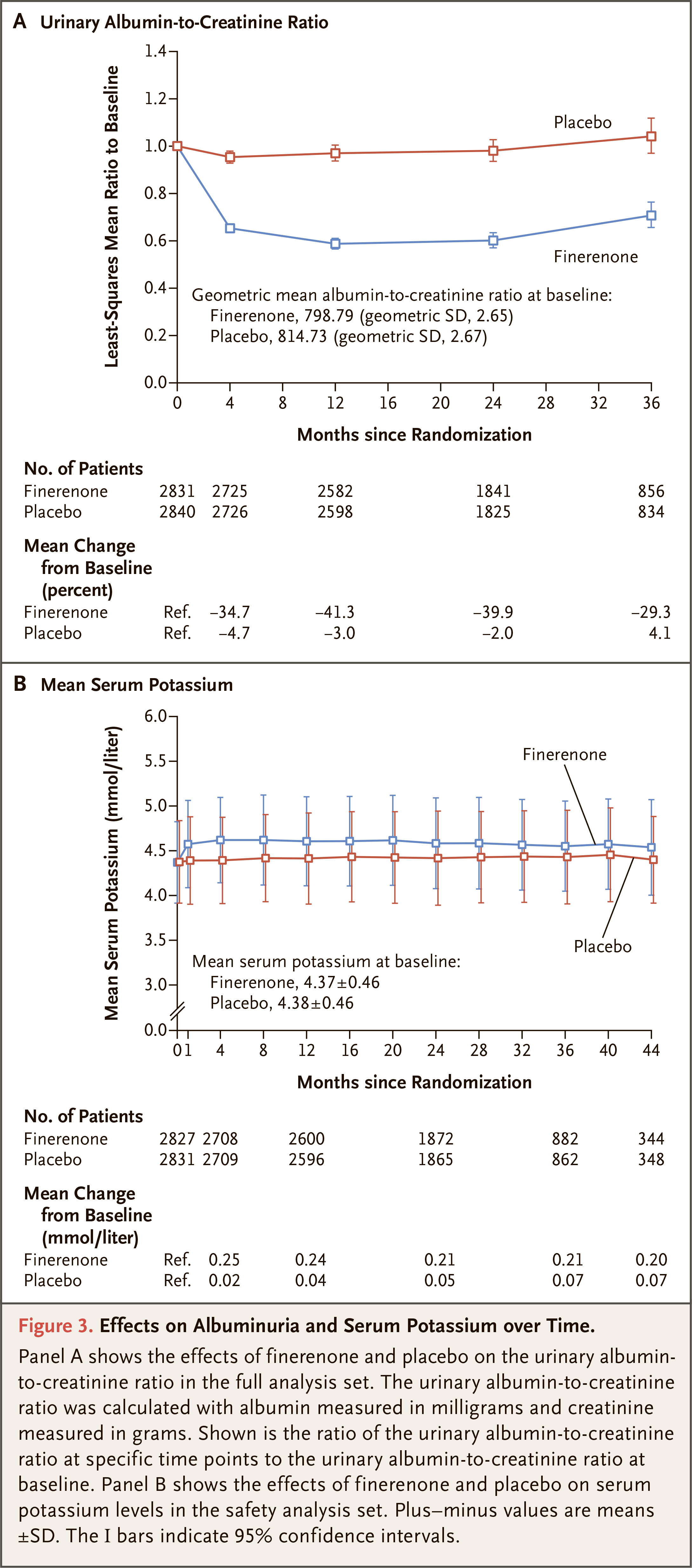
Among the most common adverse reactions in response to Kerendia administration were hyperkalemia (in 18.3% of patients — versus 9.0% in the placebo group), hypotension (4.8% vs. 3.4%), and hyponatremia (1.4% vs. 0.7%). Hyperkalemia caused 2.3% of subjects to discontinue treatment completely — vs. 0.9%. Hospital admissions due to hyperkalemia were experienced by 1.4% of patients receiving finerenone — vs. 0.3% in the control group.
FIGARO-DKD
The FIGARO-DKD (NCT02545049) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial invited adult patients (n=7352) with diabetic nephropathy and persistent high albuminuria.
The main inclusion criteria were identical to those of FIDELIO-DKD, except that there was one difference:
- either persistent high albuminuria (UACR between 30 and 300 mg/g) and eGFR between 25 and 90 mL/min/1.73 m2, or persistent very high albuminuria (UACR ≥ 300 mg/g) and eGFR at least 60 mL/min/1.73 m2.
Among the main characteristics of the subjects:
- mean age 64 years, 69% male
- mean eGFR 68 mL/min/1.73 m2, 62% had eGFR ≥ 60 mL/min/1.73 m2, 83% had eGFR ≥ 45 mL/min/1.73 m2
- median UACR 308 mg/g (IQR 108–740)
- 99.9% were receiving ACE inhibitors or ARBs
- 98% were on antidiabetic therapy: 54% received insulin, 8% GLP-1 receptor agonists, 8% SGLT2 inhibitors
- 71% were on statins, 48% diuretics.
Participants received placebo or finerenone daily on top of standard therapy involving hypoglycemic drugs and a maximum tolerated dose of ACE inhibitors or ARBs.
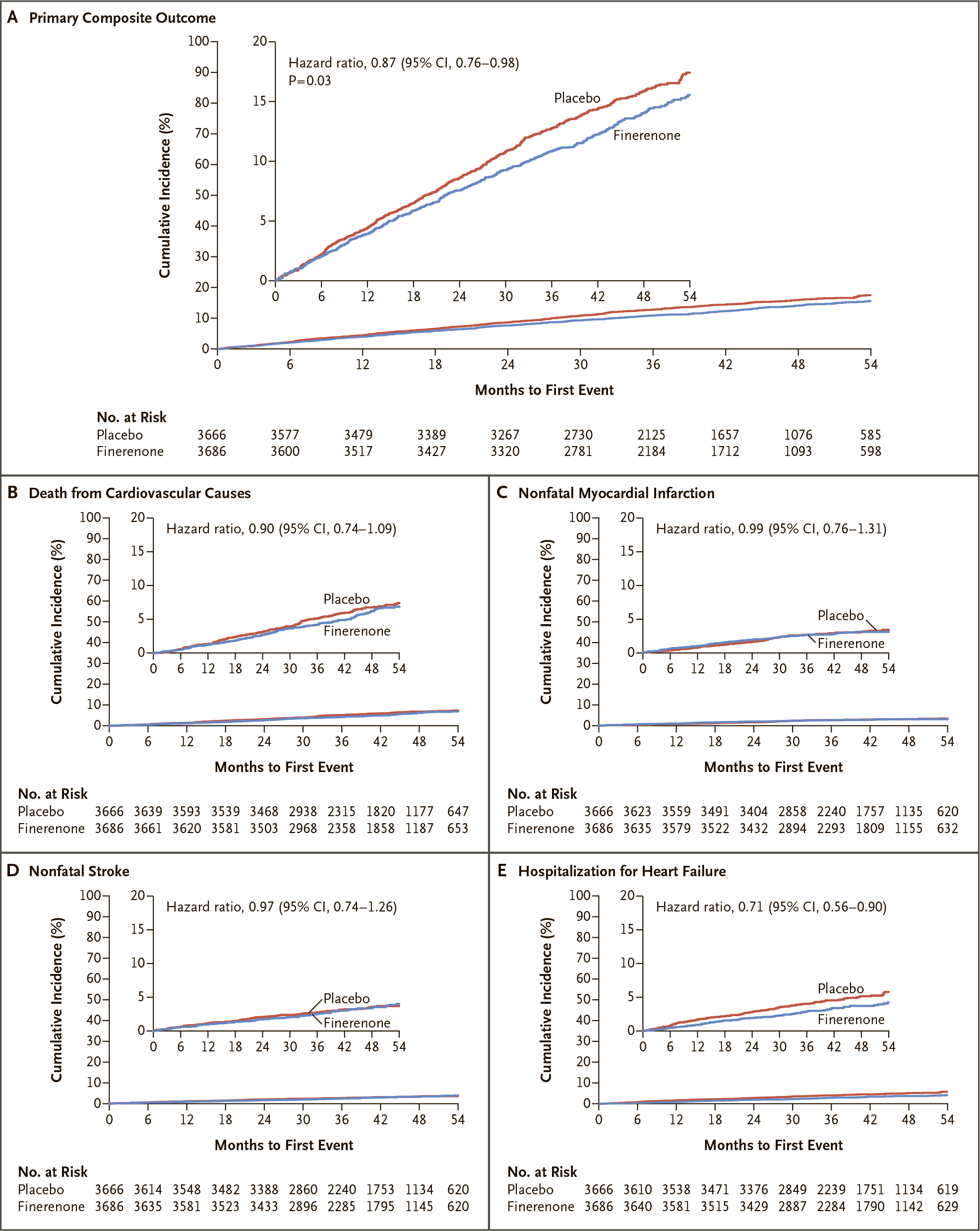
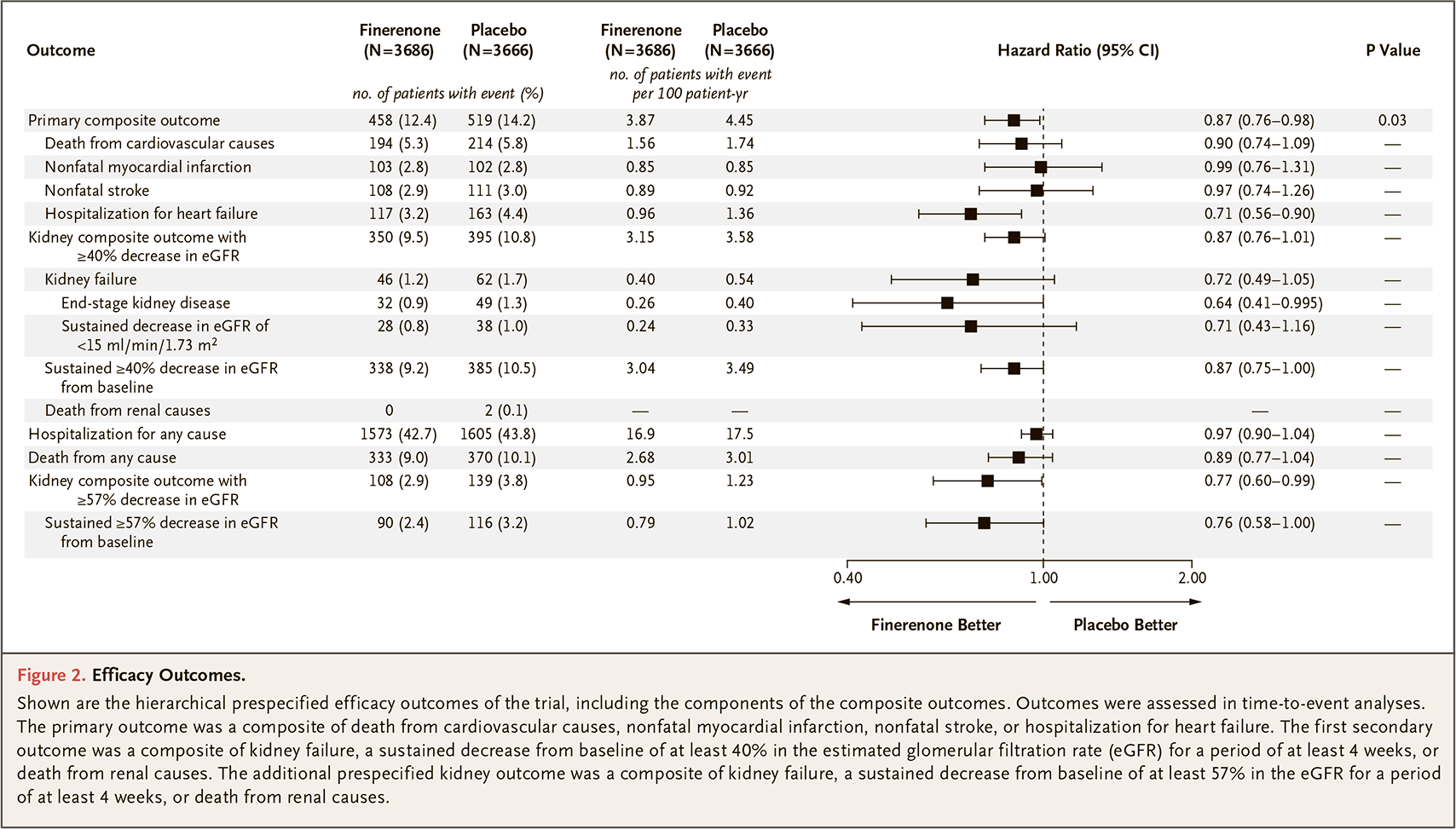
During an follow-up median of 3.4 years, finerenone statistically significantly reduced the risk of an outcome to the composite endpoint represented by one of the cardiovascular events, such as cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure. There was a 13% reduction in the probability of the indicated composite risk compared with placebo: HR 0.87 (95% CI: 0.76–0.98; p=0.03).
Individual event rates were lower with finerenone than with placebo: HRs for cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, and hospitalization for heart failure reached 0.90 (95% CI: 0.74–1.09), 0.99 (95% CI: 0.76–1.31), 0.97 (95% CI: 0.74–1.26), and 0.71 (95% CI: 0.56–0.90).
Finerenone reduced by 13% the probability of a composite risk consisting of events such as kidney failure, a sustained decrease of eGFR (by 40% or more over a period of at least 4 consecutive weeks), or renal death: HR 0.87 (95% CI: 0.76–1.01).
Hazard ratios for individual events were as follows: kidney failure 0.72 (95% CI: 0.49–1.05), end-stage kidney disease (ESKD) 0.64 (95% CI: 0.41–0.995), sustained decrease in eGFR of < 15 mL/min/1.73 m2 0.71 (95% CI: 0.43–1.16), sustained decrease in eGFR of ≥ 40% 0.87 (95% CI: 0.75–1.00), sustained decrease in eGFR of ≥ 57% 0.76 (95% CI: 0.58–1.00).
Among the most common adverse reactions in response to Kerendia administration was hyperkalemia (in 10.8% of patients — versus 5.3% in the placebo group). Serum potassium levels over 5.5 mmol/L were reported in 13.5% — vs. 6.4%, and over 6.0 mmol/L in 2.3% — vs. 1.2%. Hyperkalemia caused complete discontinuation of treatment in 1.2% of subjects — vs. 0.4%. Hospitalization due to hyperkalemia was experienced by 0.6% of patients receiving finerenone — vs. 0.1% in the control group.
Finerenone: What’s Next
Bayer continues to study finerenone in the following phase 3 clinical trials:
- FIND-CKD (NCT05047263) among adult patients (n=1580) with chronic kidney disease (CKD) not associated with diabetes mellitus: can finerenone slow the progression of CKD.
- FINEARTS-HF (NCT04435626) among adult patients (n=5500) with heart failure with moderately reduced or preserved left ventricular ejection fraction (≥ 40%): can finerenone reduce cardiovascular events and deaths.
- FIONA (NCT05196035) among pediatric (age 6 months to 17 years) patients (n=219) with CKD: can finerenone slow the progression of CKD.
Finerenone: Expert Comments
Chronic kidney disease (CKD) exacerbates the cardiovascular risk associated with type 2 diabetes mellitus. [1] The risk of cardiovascular events and first-time heart failure increases as the urinary albumin-to-creatinine ratio (UACR) exceeds 10 mg/g and the estimated glomerular filtration rate (eGFR) falls below 75 mL/min/1.73 m2. [1] [2] [3] [4] Most patients with CKD have a higher risk of cardiovascular events than the risk of developing kidney failure [5]. This is why it is important to identify and treat CKD to reduce the high burden of cardiovascular events and heart failure associated with CKD in patients with type 2 diabetes. [1] [6]
However, patients with high UACR but normal eGFR are not always identified because the UACR assay is not routinely performed, although it is the gold standard for identifying kidney damage. And this is a problem both for patients who are not properly treated and for Bayer, which has an interest in promoting finerenone.
Long-term clinical trials of finerenone, launched in 2015, came at a time when sodium/glucose cotransporter type 2 (SGLT2) inhibitors were beginning to move beyond treating diabetes alone. In late September 2019, for example, Invokana (canagliflozin), which Janssen at Johnson & Johnson is behind, was approved to reduce the risk of developing end-stage kidney disease (ESKD), doubling of serum creatinine, cardiovascular death, and hospitalization for heart failure in adult patients with type 2 diabetes and diabetic nephropathy with albuminuria.
Then, in late April 2021, Farxiga/Forxiga (dapagliflozin), offered by AstraZeneca, was approved to reduce the risk of sustained eGFR decline, ESKD, cardiovascular death, and hospitalization for heart failure in adult patients with CKD at risk of progression.
These SGLT2 inhibitors have set a high bar for therapeutic efficacy in CKD, and finerenone has failed to surpass this bar. If we compare the respective clinical outcomes of Kerendia, Invokana, and Farxiga/Forxiga, all evidence is not in favor of finerenone. It should be understood, however, that such comparisons are often methodologically flawed due to differences in patient populations and clinical trial protocols.
Due to the different mechanisms of action, finerenone is thought to be appropriate for use in combination with SGLT2 inhibitors or glucagon-like peptide-1 receptor (GLP-1) agonists such as Ozempic (semaglutide) or Trulicity (dulaglutide), which Novo Nordisk and Eli Lilly have developed and which have a clear cardiovascular benefit. Bayer, however, is unlikely to agree to clinical trials of such combinations: huge sums of money are needed to detect a possibly not so significant additive effect, with finerenone patent protection expiring in 2029.
Extras
Kerendia (finerenone). Prescribing information. U.S. [PDF]
Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020 Dec 3;383(23):2219-2229. [source]
Finerenone and cardiovascular outcomes in patients with chronic kidney disease and type 2 diabetes. Circulation. 2021 Feb 9;143(6):540-552. [source]
Finerenone reduces new-onset atrial fibrillation in patients with chronic kidney disease and type 2 diabetes. J Am Coll Cardiol. 2021 Jul 13;78(2):142-152. [source]
Finerenone in predominantly advanced CKD and type 2 diabetes with or without sodium-glucose cotransporter-2 inhibitor therapy. Kidney Int Rep. 2021 Oct 14;7(1):36-45. [source]
Design and baseline characteristics of the finerenone in reducing kidney failure and disease progression in diabetic kidney disease trial. Am J Nephrol. 2019;50(5):333-344. [source]
Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med. 2021 Dec 9;385(24):2252-2263. [source]
Finerenone reduces risk of incident heart failure in patients with chronic kidney disease and type 2 diabetes: analyses from the FIGARO-DKD trial. Circulation. 2022 Feb 8;145(6):437-447. [source]
Design and baseline characteristics of the finerenone in reducing cardiovascular mortality and morbidity in diabetic kidney disease trial. Am J Nephrol. 2019;50(5):345-356. [source]
Mineralcorticoid receptor blockers in chronic kidney disease. Nefrologia (Engl Ed). May-Jun 2021;41(3):258-275. [source]
Investigating new treatment opportunities for patients with chronic kidney disease in type 2 diabetes: the role of finerenone. Nephrol Dial Transplant. 2020 Dec 6;gfaa294. [source]