Highlights
Enjaymo (sutimlimab) is a new drug indicated to decrease the need for red blood cell transfusion due to hemolysis in adults with cold agglutinin disease.
Enjaymo, offered by Sanofi, is approved by the U.S. Food and Drug Administration (FDA) in early February 2022.
Enjaymo could have come sooner, but the FDA rejected its approval in mid-November 2020, citing problems identified with the drug’s contract manufacturer.
For U.S. patients, the list price (excluding discounts and rebates) is billed at $1,800 per vial of Enjaymo. Since six or seven vials of the drug are needed (for patients under or over 75 kg, respectively) in a single intravenous infusion, and these are given every two weeks (after two weekly loading doses), the annual cost of treating cold agglutinin disease with Enjaymo is $291,600 or $340,200.
According to industry forecasts, annual demand for Enjaymo could reach $438 million by 2026.

What Is Cold Agglutinin Disease
Cold autoimmune hemolytic anemia (AIHA) is a condition of acquired uncompensated destruction of red blood cells (RBCs) by autoantibodies to RBC antigens. Autoantibodies bind optimally to RBCs at ambient temperatures of 0–4 ℃ but also become reactive at temperatures above 30 ℃. There are two forms of cold AIHA: cold agglutinin disease (CAD) and paroxysmal cold hemoglobinuria (PCH).
Cold agglutinin disease is a rare autoimmune pathology. The incidence of cold AIHA is 1–3 cases per 100,000 people per year, with a prevalence of 17 per 100,000, with CAD accounting for approximately 15%–20% of cold AIHA cases.
Cold agglutinin disease may be primary (idiopathic), developing without a known cause, or secondary to diseases such as bacterial infections (mycoplasma, infectious mononucleosis, Legionnaires’ disease, syphilis), viral infections (Epstein–Barr virus, cytomegalovirus, mumps, varicella, rubella, HIV, influenza, hepatitis C), parasitic infections (malaria, trypanosomiasis), autoimmune diseases (rheumatoid arthritis, systemic lupus erythematosus), B-cell lymphoproliferative disorders (non-Hodgkin lymphoma, Hodgkin lymphoma, chronic lymphocytic leukemia).
Patients with cold agglutinin disease show symptoms and signs of hemolytic anemia (weakness, dizziness, shortness of breath, pallor) and hemolysis (jaundice, dark urine, left upper quadrant fullness, hepatosplenomegaly). Patients with severe hemolysis have fever, angina, tachycardia, hepatosplenomegaly, and signs of heart failure. At the same time, 40%–90% of patients experience cold-induced circulatory symptoms, ranging from mild acrocyanosis to severe Raynaud’s phenomenon, occurring even with very little exposure to cold. The survival rate after diagnosis is 12.5 years.
CAD is caused by cold agglutinins, IgM autoantibodies that bind to antigen I on RBCs at or below 37 °C, causing them to agglutinate. [1] [2] [3] [4]
The IgM–antigen complex, which is a powerful trigger of the classical complement pathway, binds to the C1 complement complex, leading to the activation of C1s (a C1 complex serine protease), which cleaves C4 and C2; this action, in turn, leads to the formation of C3 convertase C4bC2a. [1] [5]
C3 convertase catalyzes C3 proteolysis to C3a and C3b, which in turn causes opsonization and extravascular hemolysis (clearance of RBCs by phagocytes in the liver, spleen, and lungs); intravascular hemolysis (destruction of RBCs inside blood vessels) mediated by C5b-C9 occurs to a minimal extent due to intact CD55- and CD59-mediated regulation. [1] [5] [6] [7]
All people have circulating antibodies against RBCs, but their concentration is too low to cause disease (titers less than 64 at 4 °C). In people with CAD, these antibodies are in much higher concentrations (titers over 1,000 at 4 °C). More than 90% of patients with primary CAD have clonal expansion of kappa-positive B cells in the bone marrow and monoclonal immunoglobulin M (IgM)-kappa paraprotein.
There is no approved treatment for cold agglutinin disease. [8] Nonspecific methods involve avoiding exposure to cold as much as possible, as well as supportive transfusions of RBCs, administration of corticosteroids or plasmapheresis in case of exacerbation and in severe anemia. Low-molecular-weight heparin (LMWH) for prevention of venous thromboembolism is indicated.
Rituximab, which depletes the B-cell pool, induces a partial response in approximately 50% of patients with cold agglutinin disease after an average delay of 1.5 months, and relapses usually occur within one year. [9]
The addition of cytotoxic bendamustine or fludarabine increases response rates but is accompanied by more serious toxic effects, including severe neutropenia. [10] [11]
Eculizumab, a C5 inhibitor, reduces the need for transfusion and lowers lactate dehydrogenase (LDH) levels but provides only a slight increase in hemoglobin levels because it does not suppress extravascular hemolysis. [12]
Enjaymo: Mechanism of Action of Sutimlimab
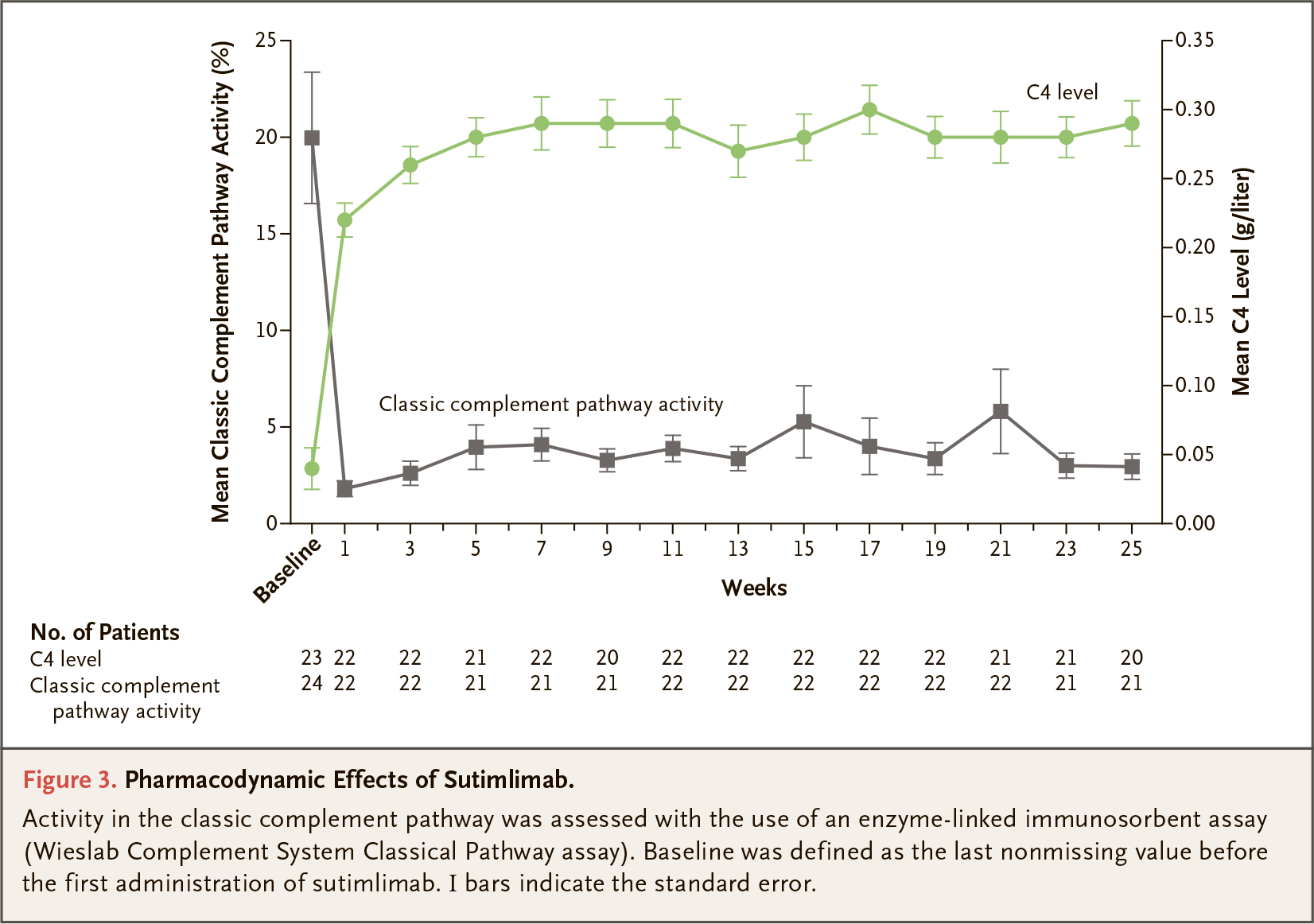
Sutimlimab (BIVV009, TNT009) is a humanized IgG4 monoclonal antibody that specifically binds s subcomponent of complement component 1 (C1s), a serine protease that cleaves complement component 4 (C4), triggering the classical complement pathway. Sutimlimab, by inhibiting the latter and not affecting the alternative and lectin complement pathways, prevents cold agglutinin-mediated deposition of complement opsonins on the red blood cells surface, thereby inhibiting hemolysis in patients with cold agglutinin disease.

Behind the development of sutimlimab is Bioverativ, the hematology division of Biogen, which spun off from its parent company in February 2017 and which Sanofi bought in March 2018 for $11.6 billion. The originator of sutimlimab is True North Therapeutics, which was acquired by Bioverativ in June 2017 for $825 million.
Enjaymo: Efficacy and Safety of Sutimlimab for Cold Agglutininin Disease
Main Results
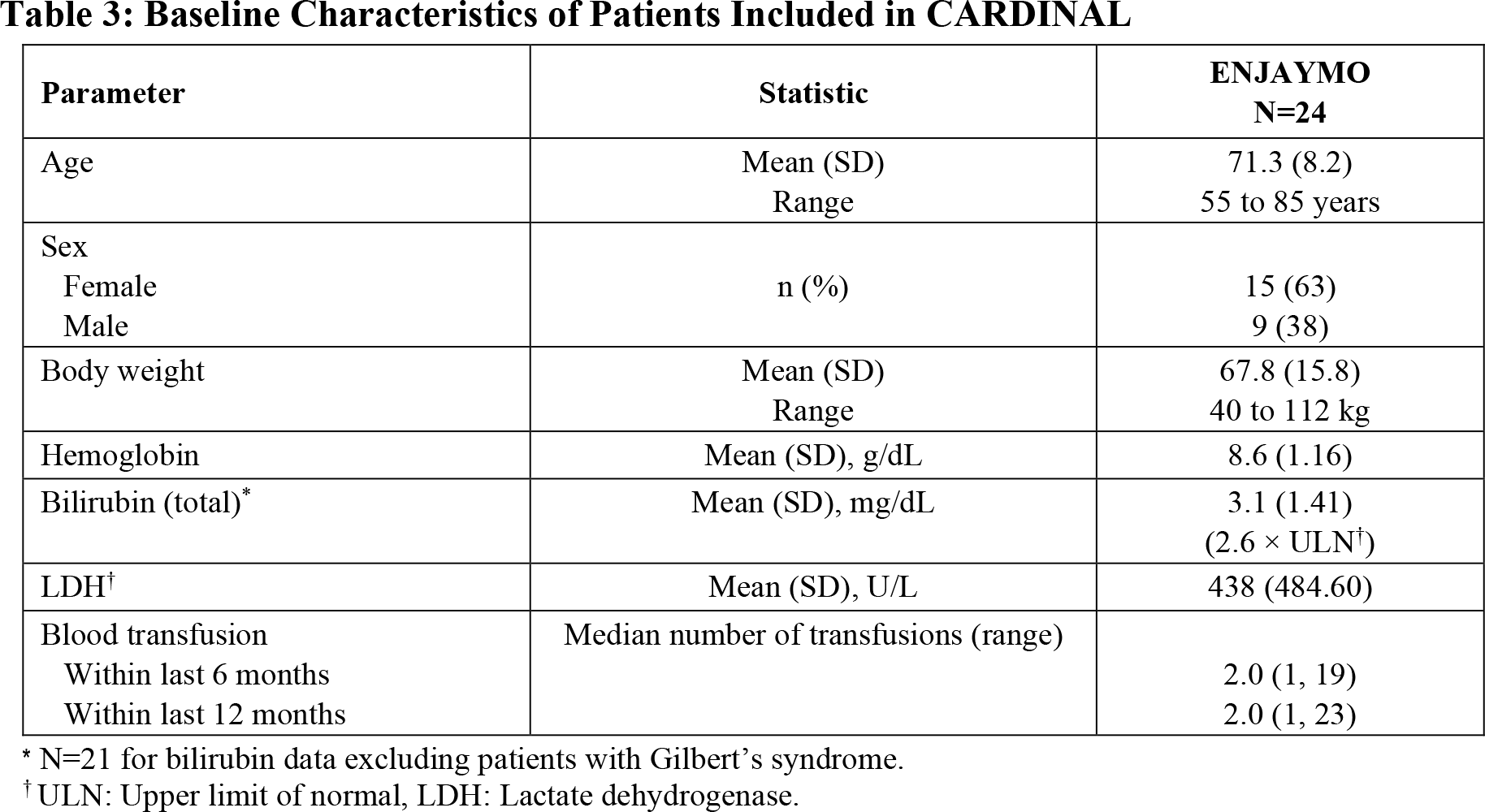
The CARDINAL (NCT03347396) phase 3 (non-randomized, open-label, multicenter, international) clinical trial invited adult patients (n=24) with primary cold agglutinin disease.
Among the main inclusion criteria: at least one episode of blood transfusion within 6 months before trial enrollment, hemoglobin ≤ 10.0 g/dL (≤ 100 g/L), and bilirubin levels above normal (including patients with Gilbert’s syndrome).
Participants received intravenous sutimlimab one dose weekly for the first two weeks and every two weeks thereafter for 26 weeks.
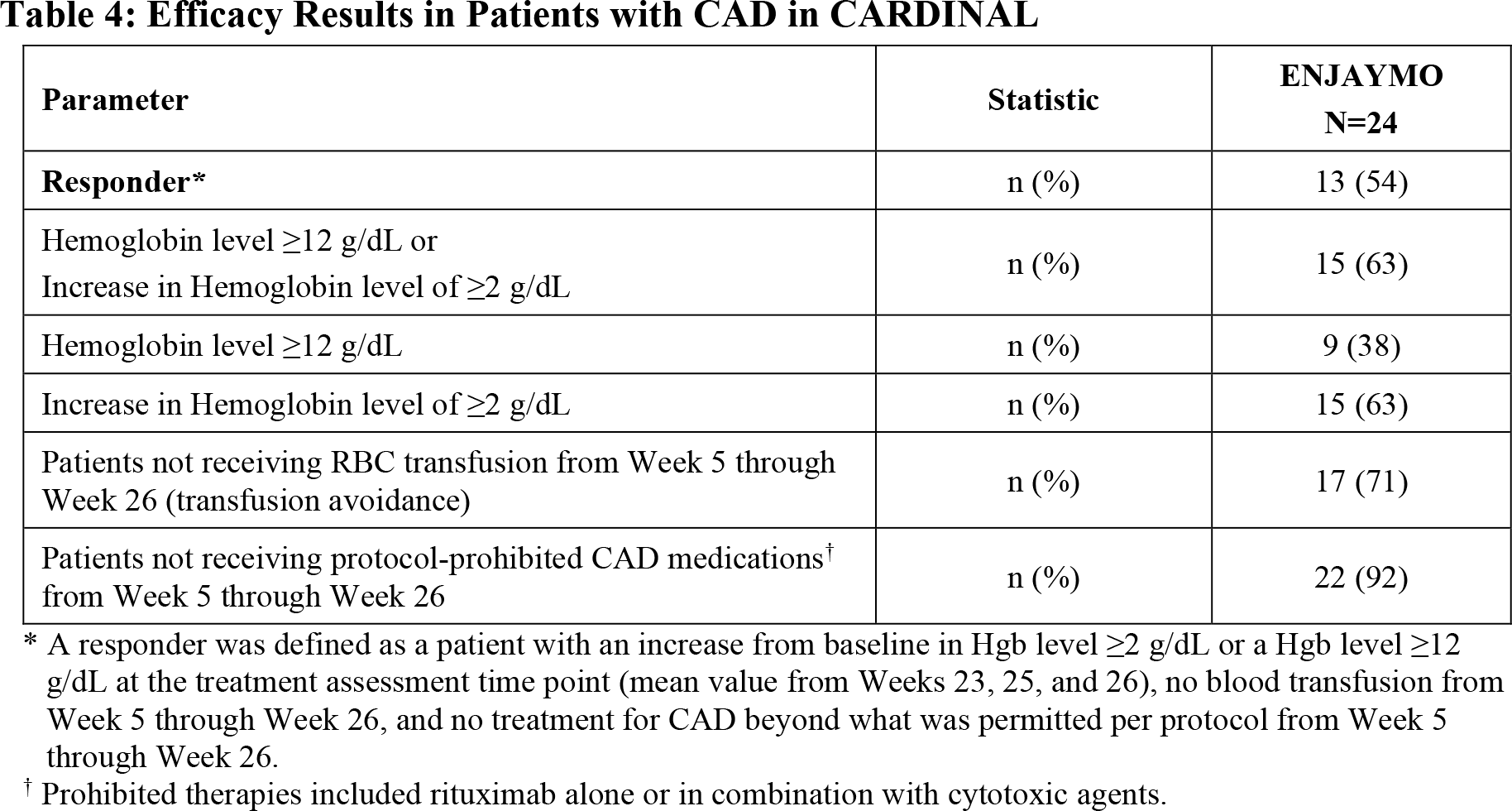
The composite primary efficacy endpoint of treatment was established by the proportion of patients who demonstrated a response, which was defined as the satisfaction of several therapy efficacy criteria simultaneously. First, the absence of the need for transfusion of red blood cells (RBCs) from week 5 to week 26. Second, during the specified therapy period, the subject should not receive cold agglutinin disease treatment beyond what is allowed by the study protocol: for example, rituximab or its combination with cytotoxic drugs. Third, the participant’s hemoglobin level at the end of treatment (averaged over weeks 23, 25, and 26) must meet one of the following criteria: ≥ 12 g/dL or an increase of ≥ 2 g/dL from baseline.
At the endpoint, 54% of subjects responded to cold agglutinin disease treatment with Enjaymo; respondents’ results are as follows:
- hemoglobin level ≥ 12 g/dL or its increase by ≥ 2 g/dL: in 63% of patients
- hemoglobin levels ≥ 12 g/dL: 38%
- increase in hemoglobin levels by ≥ 2 g/dL: 63%
- no need for RBC transfusion: 71%
- no medications received outside the trial protocol: 92%.
The median increase in hemoglobin levels during the treatment period was 2.60 g/dL (95% CI: 0.74–4.46).
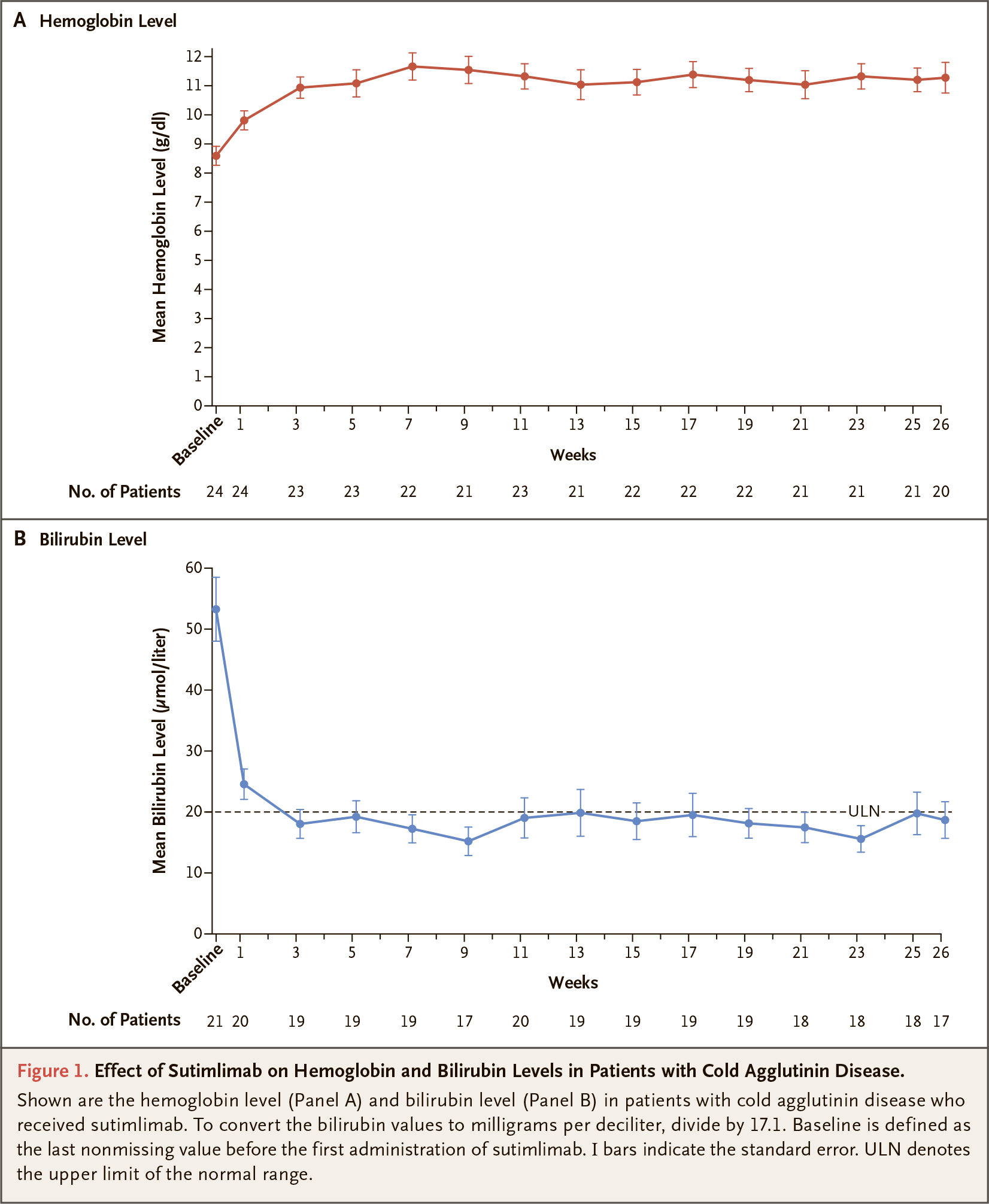
In terms of changes in bilirubin and lactate dehydrogenase levels as biomarkers of extravascular and intravascular hemolysis, respectively, sutimlimab confirmed that it was working properly.
Thus, among the patients (n=14) whose data were collected on the mean change in bilirubin levels, their baseline level was 55.23 μmol/L (2.7-fold the upper limit of normal [ULN]), whereas at the end of treatment it went to 15.56 μmol/L (0.8-fold ULN): a decrease of 38.13 μmol/L (95% CI: −42.58 to −33.86).
Among the patients (n=17) whose mean change in lactate dehydrogenase levels were collected, the baseline level was 424 U/L (1.7-fold ULN), whereas at the end of treatment it fell to 301 U/L (1.2-fold ULN): a decrease of 126 U/L (95% CI: −218 to −35).
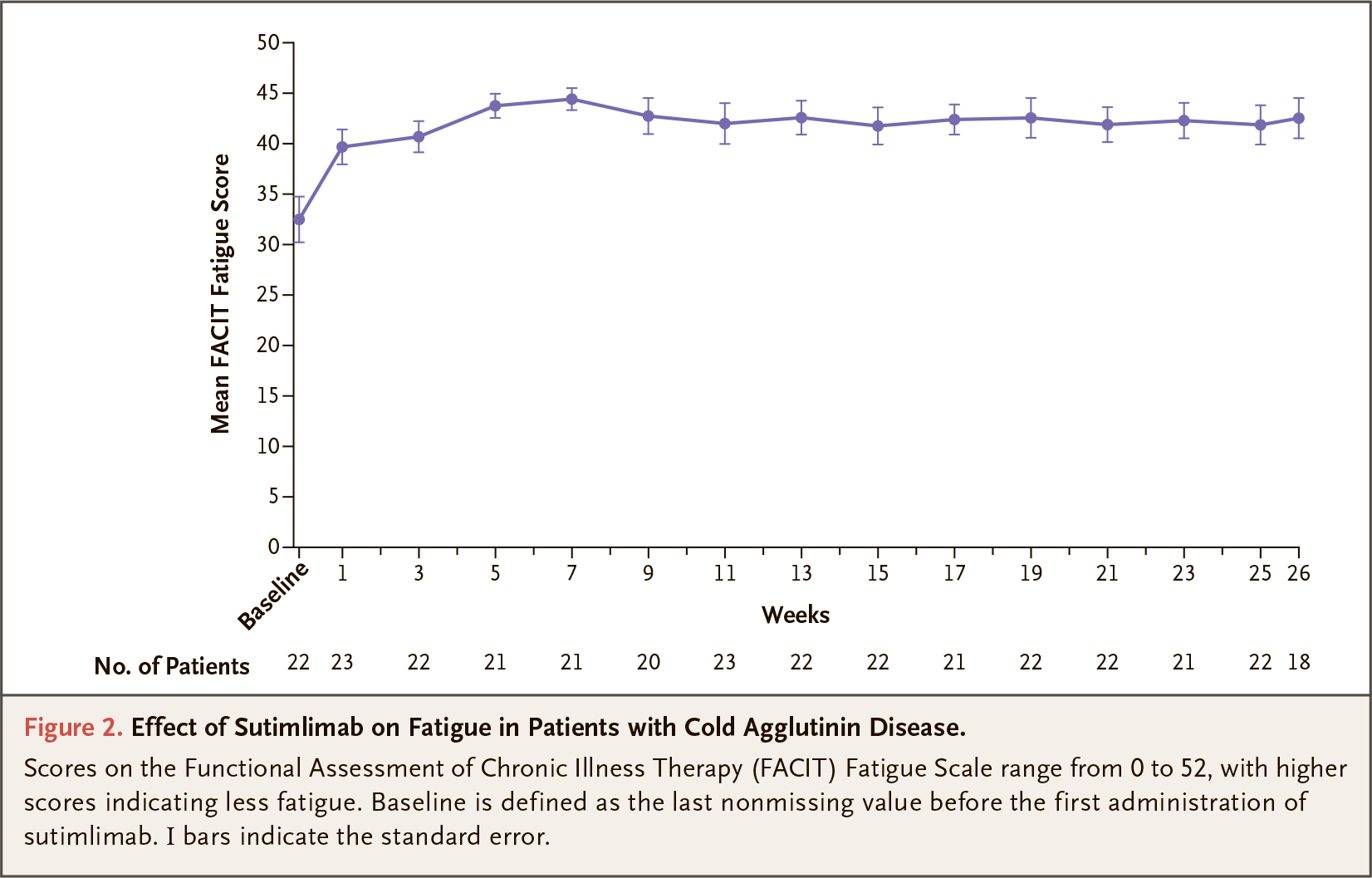
Sutimlimab relieved symptoms of fatigue: according to the Functional Assessment of Chronic Illness Therapy (FACIT) Fatigue Scale (FACIT-F), fatigue was seen to change from an average baseline of 32.5 points to 44.3 points based on patient feedback. The mean change was 10.9 points (95% CI: 8.0-13.7). A change of 3–7 points is considered clinically significant.
The most common adverse reactions to sutimlimab administration included respiratory tract infections (in 24% of patients), viral infections (13%), diarrhea (13%), dyspepsia (13%), cough (13%), arthralgia (13%), peripheral edema (13%), urinary tract infections (8%), bacterial infections (8%), cyanosis (8%), systemic hypertension (8%), gastroenteritis (8%), abdominal pain (8%), fatigue (8%), headache (8%).
Additional Results
The CADENZA (NCT03347422) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial enrolled adult patients (n=42) with primary cold agglutinin disease who, unlike CARDINAL participants, had not had a blood transfusion within 6 months before enrollment in the trial.
The composite primary efficacy endpoint of treatment differed from that of CARDINAL only in assessing hemoglobin levels, which had to rise by at least 1.5 g/dL at the end of therapy.
The results of treatment of cold agglutinin disease with Enjaymo are as follows:
- In the sutimlimab group the proportion of respondents was 73% — versus 15% in the placebo group: odds ratio (OR) 15.9 (95% CI: 2.9–88.0; p<0.001).
- Sutimlimab provided an increase in hemoglobin levels followed by sustained maintenance (mean difference with placebo was 2.6 g/dL (95% CI: 1.8–3.4; p<0.001), and overall mean hemoglobin levels were maintained at or above 11 g/dL for the duration of treatment.
- Sutimlimab relieved symptoms of fatigue: the FACIT-F score increased by 10.8 points — vs. 1.9 points in the control group (mean difference 8.9 [95% CI: 4.0–13.9; p<0.001]).
- Sutimlimab led to a decrease in bilirubin levels of 22.1 μmol/L — vs. a decrease of 1.8 μmol/L in the placebo group; bilirubin levels were maintained below the upper limit of normal for the duration of treatment.
- Administration of sutimlimab was reflected by a decrease in lactate dehydrogenase levels by 150 U/L — vs. an increase of 7.6 U/L in the placebo group.
Treatment-emergent adverse events (TEAEs) that were more frequently reported in the Enjaymo group than in the control group included: headache (in 23% of patients in the sutimlimab group — versus 10% in the placebo group), hypertension (23% vs. 0%), rhinitis (18% vs. 0%), Raynaud’s phenomenon (18% vs. 0%), and acrocyanosis (14% vs. 0%). No deaths or meningococcal infections were reported.
Serious TEAEs occurred in 13.6% of subjects receiving sutimlimab, including one event of cerebral venous thrombosis in a patient with a history of diabetes.
Extras
Enjaymo (sutimlimab). Prescribing information. U.S. [PDF]
Sutimlimab in cold agglutinin disease. N Engl J Med. 2021 Apr 8;384(14):1323-1334. [source]