Highlights
The world community is extremely concerned about the growing threat of the Omicron variant (B.1.1.529) of coronavirus SARS-CoV-2. This is because the new variant is not only spreading rapidly across the planet but is also characterized by an impressive set of mutations. These mutations may well contribute to Omicron becoming more infectious and aggressive, and existing vaccines may not be able to counteract it as effectively, leading to an increase in reinfection.
In the wake of the hype surrounding Omicron, the Internet is overflowing with a slew of disturbing messages. People are worried: “Omicron is more contagious,” “Omicron avoids vaccine-mediated immunity,” “We need new vaccines against Omicron.” Some are more optimistic: “Omicron causes a milder course of the disease,” “Omicron will destroy itself because of the excessive mutations that will eventually render it unable to replicate,” “Omicron is generally harmless.” Others are categorical in their statements: “HIV patients are to blame for the emergence of Omicron.”
Let’s not succumb to panic, but stick to scientific approaches in our assessments.
Omicron Variant: Scientific Timeline
January 2022
January 14
Although a number of vaccine manufacturers are preparing vaccine modifications tailored to the mutational specificity of the Omicron variant of SARS-CoV-2 coronavirus, U.S. health officials believe it is not particularly necessary.
On the one hand, the scientific world and the pharmaceutical industry argue that existing vaccines need to be updated for the specifics of Omicron because their effectiveness drops dramatically in its presence. On the other hand, officials at the U.S. Food and Drug Administration (FDA) and the National Institute of Allergy and Infectious Diseases (NIAID) express doubts about such an initiative: first, by the time new vaccines are ready, the Omicron wave may be over, and second, repeated (booster) doses of vaccines will provide quite reliable protection against Omicron.
There is an opinion that it is wise to wait a couple of months or so to see if Omicron becomes the dominant variant in the long term, competing with Delta, or if it quickly recedes like other SARS-CoV-2 variants like Alpha, Beta, and Gamma.

Universal Coronavirus Vaccine
The biotechnology industry must come up with a comprehensive defense against all coronaviruses.
The current uncertainty with the future of Omicron should not negate the fact that premature promotion of new vaccines is risky and costly because manufacturing processes would have to be restructured, and this would disrupt the production of existing vaccines, causing shortages. Again, it is not known whether Omicron vaccines will be as effective against other strains, since the latter may well break out again or evolutionize into other variants. It would be far better to abandon the pursuit of specific variants of coronavirus and devote resources to the development of a universal vaccine that protects against all SARS-CoV-2 mutations in a long-lasting and effective manner.
January 13
A third (booster) dose of the viral vector vaccine Vaxzevria/Covishield (AZD1222, ChAdOx1 nCoV-19, ChAdOx1-S) by AstraZeneca enhances antibody response to the Omicron (B.1.1.529) variant of SARS-CoV-2 coronavirus.
Vaxzevria/Covishield booster also enhances the immune response to other coronavirus variants, including Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2).
Immunogenicity was evaluated 28 days after the third dose of the vaccine.
This was reported by AstraZeneca, based on preliminary analysis of data collected in the ongoing clinical trial NCT04973449 phase 2/3.
The study is testing the safety and immunogenicity of a booster dose of Vaxzevria/Covishield or AZD2816 experimental vaccine designed to be specific to the Beta variant of coronavirus. Adult volunteers were invited, both unvaccinated and those who had received a full course of two doses of Vaxzevria/Covishield or the mRNA vaccine — Comirnaty (tozinameran; BNT162b2) or Spikevax (elasomeran; mRNA-1273) by Pfizer/BioNTech and Moderna respectively.
January 12
Adagio Therapeutics has notified that ADG20 monoclonal antibody it is developing works against the Omicron (B.1.1.529) strain of SARS-CoV-2 coronavirus.
Thus, the half-maximal inhibitory concentration (IC50) of ADG20 is 0.4–1.1 µg/ml, which compares with that of sotrovimab and Evusheld (AZD7442) as a combination of tixagevimab (AZD8895) and cilgavimab (AZD1061) by GlaxoSmithKline/Vir Biotechnology and AstraZeneca, respectively.

ADG20: Cure for All Mutant Variants of SARS-CoV-2
Adagio Therapeutics’ monoclonal antibody will help fight all strains of the coronavirus.
↓
According to the European Medicines Agency (EMA), frequently repeated vaccinations for COVID-19 infection can negatively affect the immune response by overloading and weakening the immune system, ultimately proving impractical.
According to the regulator, repeated booster doses of the vaccine every four months are too frequent an immunization regimen: revaccination should be less frequent, tying it to the beginning of the winter season in each hemisphere, similar to influenza inoculation.
Regarding the need for universal adoption of the fourth dose of vaccines advocated by Israel, the EMA has so far questioned this approach due to a lack of data that would unequivocally support it. Nevertheless, the regulator continues to study Omicron comprehensively in order to propose the best strategy to combat it. But it is already clear that endless boosters do not provide a way out of a pandemic that is highly desirable to bring to a more endemic nature.
When it comes to vaccines specific to the Omicron mutation set, more data needs to be collected on the effect of the new variant on the vaccines available in the armamentarium and a better understanding of the evolution of the current wave. In other words, a strategy that is not just reactive is needed — an approach suitable for preventing future SARS-CoV-2 variants should be developed.
January 11
The World Health Organization (WHO) reported a record number of people infected with SARS-CoV-2 coronavirus in the history of the pandemic.
During the first full week of January 2022 (January 3 to 9 inclusive), the number of newly infected people exceeded 15 million. This is a 55% increase over the previous week.
The epidemiological situation is due to the rapid spread of the Omicron variant on the background of reduced circulation of the Delta variant and a very low presence of Alpha, Beta, and Gamma variants.
↓
There were 1.35 million new cases of SARS-CoV-2 coronavirus in the United States, the highest daily total of any country in the world. The previous anti-record was set on May 3, 2021 — 1.03 million new cases.
The spike in incidence is due to the continued spread of the Omicron (B.1.1.529) variant of coronavirus.
Although Omicron causes perhaps a less severe course of COVID-19 infection than other variants, the huge flood of patients is putting tremendous pressure on hospital systems.
January 10
An experimental ensovibep, developed by Molecular Partners and Novartis and suitable for fighting the Omicron variant of SARS-CoV-2 coronavirus, provided an 87% reduction in risk of hospitalization and/or death relative to placebo among outpatients with mild-to-moderate COVID-19 infection.

Ensovibep: Drug for All Variants of Coronavirus Including Omicron
Molecular Partners and Novartis believe in the success of DARPins.
December 2021
December 29
The Delta (B.1.617.2) and Omicron (B.1.1.529) variants of the SARS-CoV-2 coronavirus now circulating are twin threats that are causing huge numbers of hospitalizations and deaths. Total vaccination of the world’s population can help control the problem. However, fewer than half of the World Health Organization’s (WHO) member states have met the plan to immunize 40% of their people.

Eliminating Health Disparities Is Key to Ending Pandemic
Misinformation, populism, and self-interest keep the COVID-19 that has enslaved the planet.
According to Tedros Adhanom Ghebreyesus, WHO’s director-general, as the COVID-19 pandemic drags on, new variants of the coronavirus could become completely resistant to existing vaccines, requiring them to adapt accordingly. And any renewal of vaccines potentially means another shortage in supply. Therefore, vaccine production must be ramped up locally. But this is not possible without the consolidation of vaccine technologies when all patents and intellectual property rights become the public domain. This has not happened so far: every pharmaceutical company is busy making crazy profits.
The moment has come when the leaders of the countries must put aside the politics of populism and self-interest.
December 24
Within the next two to three months, 3 billion or more people on the planet will be infected with the Omicron (B.1.1.529) variant of the SARS-CoV-2 coronavirus. This is equivalent to nearly 40% of the world’s population.

Three Billion Omicron Cases
Omicron, a new variant of the SARS-CoV-2 coronavirus, will infect nearly 40% of the world’s population.
According to the predictive model of the Institute for Health Metrics and Evaluation (IHME) at the University of Washington School of Medicine, the accelerated transmissibility (contagiousness) of Omicron will result in multiple increases in reported COVID-19 infections and a global spike in hospitalizations. However, the number of fatalities will not rise significantly.
- COVID-19 results briefing. IHME, December 22, 2021. [PDF]
December 23
Researchers at Oxford University who tested the neutralizing activity of antibodies against the Omicron (B.1.1.529) variant of the SARS-CoV-2 coronavirus made the following conclusions:
- A third (booster) dose of the viral vector vaccine Vaxzevria/Covishield (AZD1222, ChAdOx1 nCoV-19, ChAdOx1-S) promoted by AstraZeneca could potentially protect against Omicron, although the degree of protection would be relatively weak.
- A third dose of the mRNA vaccine Comirnaty (tozinameran; BNT162b2) by Pfizer/BioNTech is quite capable of putting up a strong shield against Omicron.
- The protective immunity developed in unvaccinated individuals after naturally exposed to non-Omicron COVID-19 variants is comparable to that after two doses of AstraZeneca or Pfizer/BioNTech vaccine, which means it will not save them from Omicron — well, except to avoid the development of severe COVID-19 that requires hospitalization.
Thus, 28 days after the third dose of Vaxzevria/Covishield, the titer of Omicron neutralizing antibodies in the sera of the vaccinated increased 2.7-fold compared to their level after 28 days after the second dose. However, the titer after the booster was still 3.6 and 12.7 times lower compared with the booster titer of neutralizing antibodies against the Delta variant and the original non-mutant SARS-CoV-2.

After the Comirnaty booster, the titer of Omicron neutralizing antibodies in the sera of vaccinated subjects increased 34.2-fold compared with their levels after the second dose. At the same time, it was 3.6 and 14.2 times lower relative to the booster titer against Delta and non-mutant coronavirus. It would seem that this reduction is comparable to that for the AstraZeneca’s vaccine, but in absolute terms the level of neutralizing antibodies against Omicron after the third dose of Comirnaty was 11.4 times higher compared to the level after the third dose of Vaxzevria/Covishield.

Looking at titers of Omicron neutralizing antibodies in the sera of unvaccinated and COVID-19 survivors, they, compared with titers against the original coronavirus, dropped significantly — by 16.9, 33.8, 11.8, 3.1, and 1.7 times for COVID-19 caused by non-mutant SARS-CoV-2, its Alpha (B.1 .1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2) variants, respectively. At the same time, their levels in absolute values were comparable to that after the second dose of AstraZeneca or Pfizer/BioNTech vaccine, i.e., decisively insufficient to counteract omicron.

- Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. bioRxiv, December, 22, 2021. [PDF]
↓
Russia has approved MIR 19, a new drug for the treatment of COVID-19 infection caused by the SARS-CoV-2 coronavirus.
MIR 19, which inhibits coronavirus replication and prevents the development of severe COVID-19, including acute respiratory distress syndrome (ARDS), is based on RNA interference (RNAi) technology. Because of its specific mechanism of action, MIR 19 retains antiviral activity regardless of the variant of coronavirus, whether it is Omicron or Delta.
MIR 19, indicated for the treatment of COVID-19 in the non-serious form, is administered by inhalation for 14 days.

MIR 19: Surprising New Drug to Treat Coronavirus
A Russian drug for COVID-19 has adopted a powerful RNA interference technology.
↓
Merck & Co. has offered oral molnupiravir, a new drug indicated to treat mild-to-moderate COVID-19 infection in adult patients who are at high risk for progression to severe disease that requires hospitalization or may end in death.
According to a clinical trial of the antiviral, molnupiravir reduced the risk of hospitalization or death by 30%.
According to Merck & Co., molnupiravir maintains its antiviral efficacy against the Omicron variant.

Molnupiravir: New Effective Pill for Coronavirus. All That We Know
Molnupiravir pills can help COVID-19 patients avoid going to the hospital or dying.
December 22
Pfizer has released oral Paxlovid (nirmatrelvir + ritonavir), a new drug indicated to treat mild-to-moderate COVID-19 infection in adults and children who are at high risk for progression to severe disease that requires hospitalization or may end in death.
Paxlovid is the first oral antiviral drug for home use with reliably proven therapeutic efficacy.
In a clinical trial of the antiviral, Paxlovid reduced the risk of hospitalization or death by 89% and 88% when administered within 3 and 5 days of onset of COVID-19 symptoms, respectively. Among older patients, the risk reduction was even better, at 94%.
According to Pfizer, Paxlovid maintains its highest antiviral efficacy against the Omicron variant.

Paxlovid: New Cure for Coronavirus
Pfizer’s oral antiviral drug reduced the risk of hospitalization or death from COVID-19 by 89%.
↓
Israel became the first country in the world to launch a mass immunization campaign with a fourth dose. The initiative responds to scientific evidence showing that even three doses of vaccines are insufficient to provide reliable protection against the Omicron variant of SARS-CoV-2 coronavirus.
The fourth dose of Pfizer/BioNTech’s mRNA vaccine Comirnaty (tozinameran; BNT162b2) will initially be given to the elderly (60 years and older), those with compromised immune systems, and healthcare workers. To receive it, at least four months must pass after the third dose of inoculation.
In addition, the period between the second and third doses was reduced from five to three months.
Earlier, Israel became the first country in the world to start immunizing its population with the third (booster) dose of the vaccine.
Of Israel’s 9.3 million population, nearly 70% were inoculated with two doses, while 45% received three doses.
↓
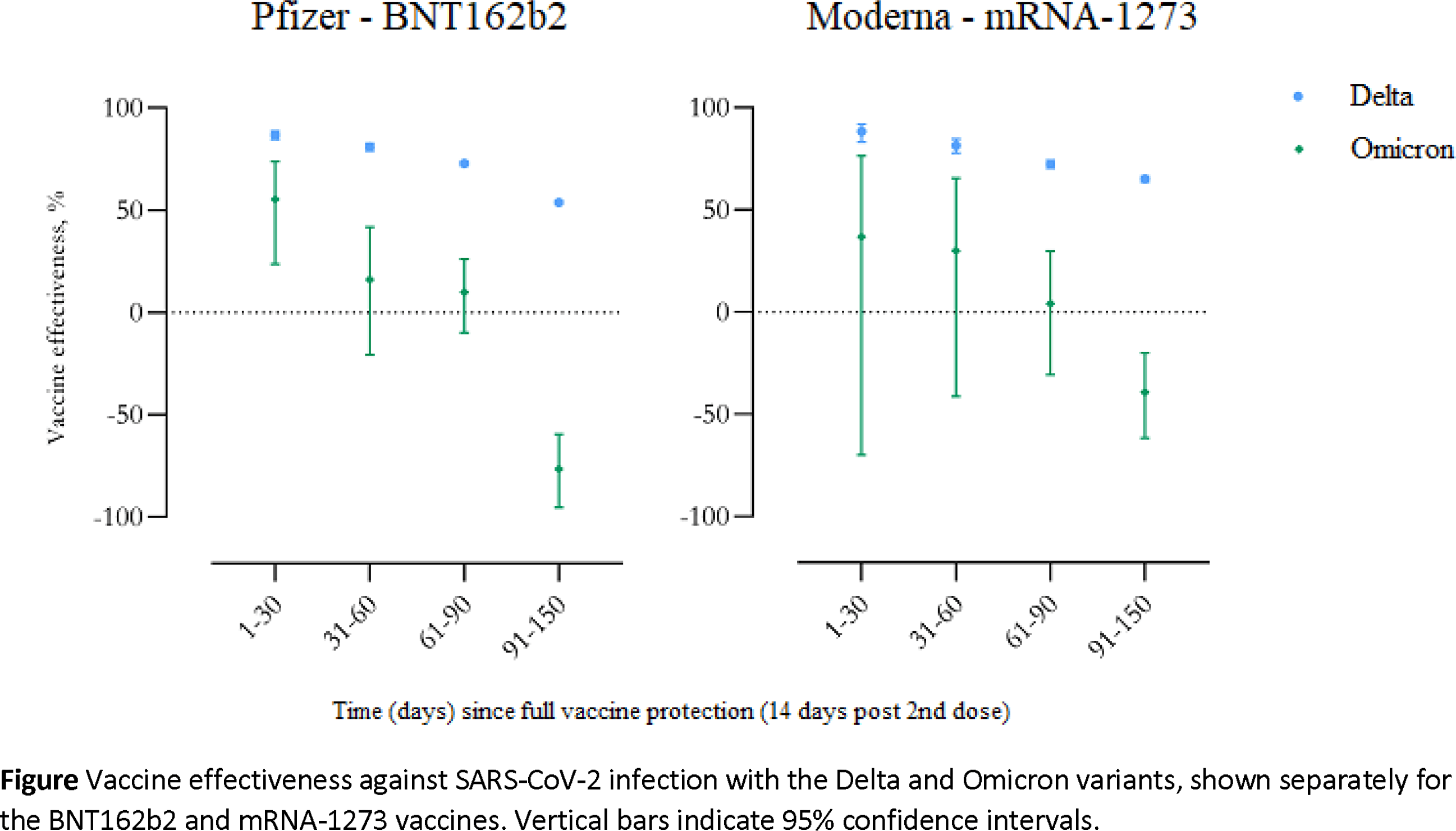
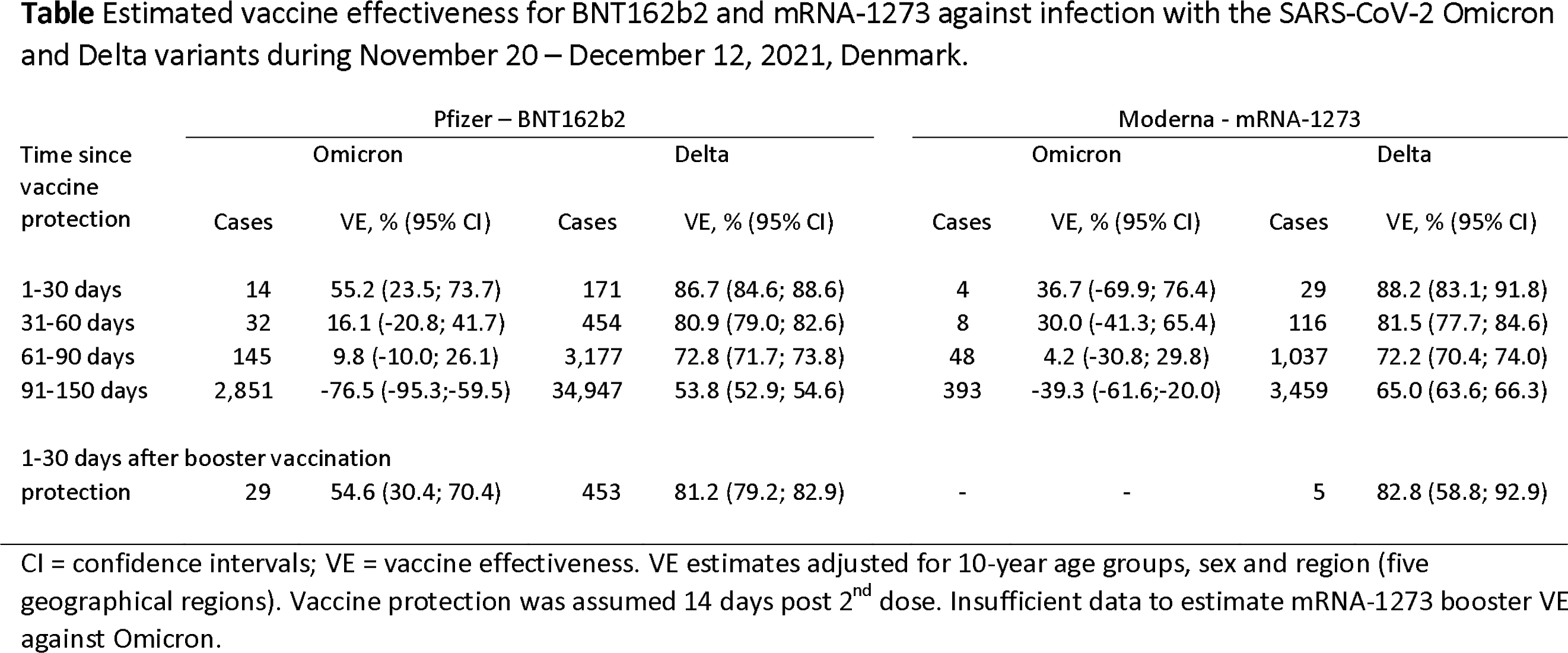
The Danish Staten Serum Institut (SSI) evaluated the protective efficacy of vaccines against the Omicron (B.1.1.529) variant of SASR-CoV-2 coronavirus. mRNA vaccines Comirnaty (tozinameran; BNT162b2) and Spikevax (elasomeran; mRNA-1273) by Pfizer/BioNTech and Moderna were tested.
The effectiveness of mRNA vaccines against Omicron was found to be catastrophically reduced, both disproportionately inferior to protection against the Delta strain (B.1.617.2) and weakening very rapidly over time. And even the third (booster) dose protects against Omicron significantly worse than against Delta.
Thus, immunization with two doses of Comirnaty provided 87%, 81%, 73%, and 54% protection against Delta for up to one month after inoculation, one to two months, two to three months, and three to five months, respectively. In the case of Omicron, vaccine effectiveness was 55%, 16%, 9%, and −77%.
Vaccination with two doses of Spikevax protected against Delta at 88%, 82%, 72%, and 65% in the above periods. The Omicron variant reduced its effectiveness to 37%, 30%, 4%, and −39%.
A third (booster) dose of Comirnaty brought the level of protection against Delta and Omicron to the corresponding 81% and 55% for periods up to one month after its administration.
- Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. medRxiv, December 21, 2021. [PDF]
December 21
According to a study by the Icahn School of Medicine at Mount Sinai (ISMMS), the neutralizing antibody activity of those who recovered from a COVID-19 infection or who received two doses of mRNA vaccines — Comirnaty (tozinameran; BNT162b2) or Spikevax (elasomeran; mRNA-1273) by Pfizer/BioNTech and Moderna — is decidedly insufficient to successfully protect against the Omicron (B.1.1.529) variant of SASR-CoV-2 coronavirus.
However, protection against Omicron will remain (albeit at a decently weakened level) in those who have previously been exposed to coronavirus three or four times: either they were vaccinated with three doses, or they were infected and then vaccinated with two doses, or they were infected and vaccinated with three doses.
The reduction in neutralizing activity of serum antibodies against Omicron was as follows when compared with activity against the original non-mutant SARS-CoV-2 as measured by the 50% inhibitory dose (ID50; the antibody titer required to suppress replication of 50% of the viral culture):
- COVID-19: 11.1-fold reduction — in most cases (73%) the neutralizing activity against omicron was below the limit of detection (LOD)
- two doses of Comirnaty: 23.3-fold (p=0.0043) — 30% LOD
- two doses of Spikevax: 42.6-fold (p=0.0005)
- three doses of Comirnaty: 7.5-fold (p=0.0007)
- three doses of Spikevax: 16.7-fold (p=0.0437)
- COVID-19 and two doses of Comirnaty: 13.7-fold (p=0.0165)
- COVID-19 and two doses of Spikevax: 10.6-fold (p=0.0075)
- COVID-19 and three doses of Comirnaty: 13.1-fold (p=0.0462).
The researchers also examined the binding activity of serum antibodies, one of the correlates of protection against SARS-CoV-2, which provides it through Fc-mediated effector functions. If binding activity to the receptor-binding domain (RBD) of the coronavirus is maintained (even with a significant decrease in antibody titer), it indicates the presence of cognate B cells. The latter can be rapidly activated during infection with a variant of coronavirus or a vaccine specific to it, inducing a strong plasmoblast response that provides control over the spread of the virus. In addition, B cells, characterized by low-affinity binding to proteins of the variant with the antigenic drift, enter the lymph nodes and participate in germinal center reactions leading to the formation of antibodies capable of restoring neutralizing activity due to affinity maturation.
In general, the binding activity of antibodies against Omicron decreased significantly less than the neutralizing activity. It decreased most dramatically (7.5-fold reduction) in previously exposed to COVID-19 but not vaccinated, and in two-thirds to an undetectable threshold. In all other groups, binding was relatively stable, and its reduction ranged from 2.9-fold for two doses of Spikevax to 1.5-fold for three doses of Comirnaty.
Finally, the experts checked serum antibody binding activity to the N-terminal domain (NTD) of the coronavirus, which, in addition to RBD, is the main target of B cells after inoculation with mRNA vaccines. The NTD at Omicron carries a large number of amino acid substitutions, three deletions, and one insertion of three amino acids in length, all of which significantly modify the immunodominant “supersite” binding as well as the neutralizing epitopes beyond it.
As it turned out, antibody binding to NTD was preserved with a relatively small decrease (1.9-fold at most), indicating either the maintenance of binding (e.g., with lower affinity) to the “supersite,” or the presence of a large number of unchanged epitopes in this domain.
- Activity of convalescent and vaccine serum against a B.1.1.529 variant SARS-CoV-2 isolate. medRxiv, December 21, 2021. [PDF]
December 20
Moderna has disclosed preliminary data regarding the efficacy of a third (booster) dose of the mRNA vaccine Spikevax (elasomeran; mRNA-1273) in the task of counteracting the Omicron (B.1.1.529) variant of SARS-CoV-2 coronavirus.
Administration of the booster at a dose of 50 mcg (this dose is officially approved by regulators) resulted (after 29 days) in a 37-fold increase in neutralizing antibody levels against Omicron compared to levels before its administration. A booster at a dose of 100 μg (the doubled dose is experimental) resulted in an 83-fold increase.
Nevertheless, even after the boosters, the level of neutralizing antibodies against Omicron was 2.9 and 3.0 times lower when compared with that after the boosters surrounded by the original coronavirus with the D614G mutation.
- The D614G mutation was previously one of the most common mutations in the world: as of mid-2020 (during the first wave of COVID-19), it was the dominant mutation in the coronavirus pandemic. One of the clinical features of D614G is loss of smell.
A doubled third dose of Spikevax was characterized by acceptable tolerability, although adverse reactions were more frequent than with the standard 50-μg dose.
Moderna is about to complete a clinical trial of the 100-μg booster and then send the collected data to regulators.
In parallel, Moderna is developing mRNA-1273.529, a variant of Spikevax, that takes into account Omicron mutation specificity; appropriate clinical trials will be launched in early 2022.
At the same time, Moderna is studying the possibility of incorporating Omicron mutations into an experimental program of multivalent boosters that take into account the mutational specificities of several coronavirus strains at once, including Delta (B.1.617.2) and Beta (B.1.351).
- Omicron booster strategy update. Moderna, December 20, 2021. [PDF]
December 19
Switzerland-based Molecular Partners reported that an experimental ensovibep (MP0420) being developed with Novartis for the treatment and prevention of COVID-19 infection remains fully functional in the presence of the Omicron (B.1.1.529) variant of SARS-CoV-2 coronavirus.
According to in vitro studies in a pseudoviral system mimicking the Omicron variant, ensovibep retained high neutralizing activity comparable to that against the original non-mutant SARS-CoV-2. Thus, while the half-maximal inhibitory concentration (IC50) of ensovibep against the latter is 1.6 ng/ml, in the case of Omicron it only increases by a factor of 1.3–1.4 to 2.1–2.2 ng/ml.
The neutralizing activity of ensovibep against all other strains of coronavirus, including the variants of concern such as Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2), is very high: IC50 falls within a narrow range of 1–8 ng/ml.
- Ensovibep, a novel trispecific DARPin candidate that protects against SARS-CoV-2 variants. bioRxiv, December 17, 2021. [PDF]
Ensovibep: Drug for All Variants of Coronavirus Including Omicron
Molecular Partners and Novartis believe in the success of DARPins.
December 18
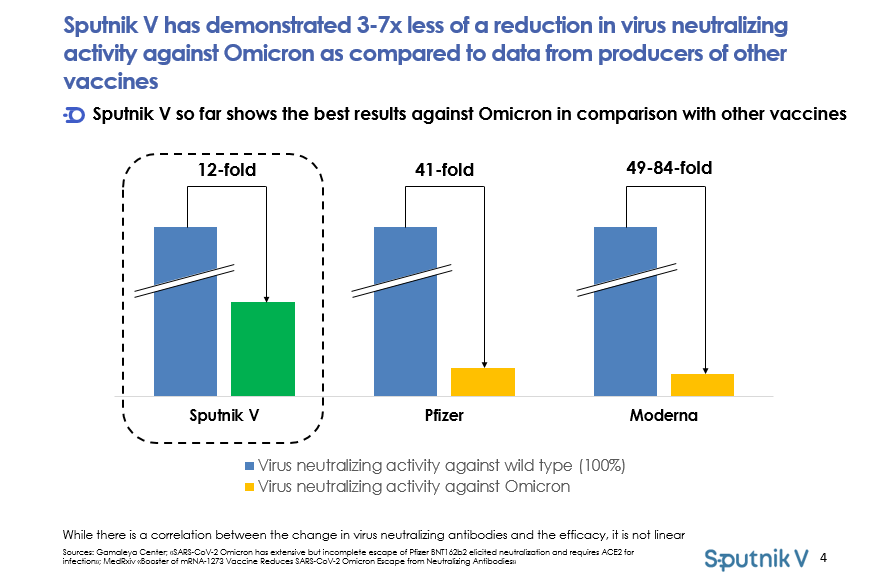
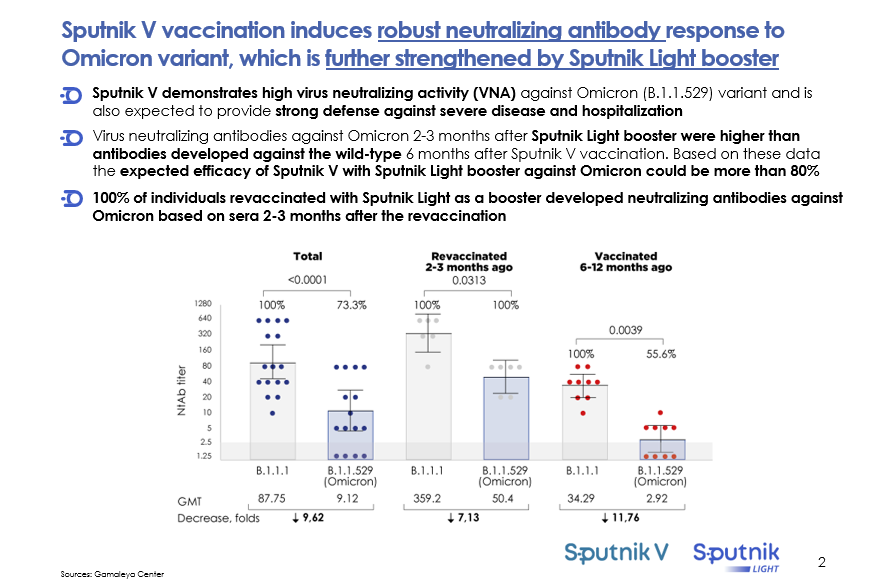
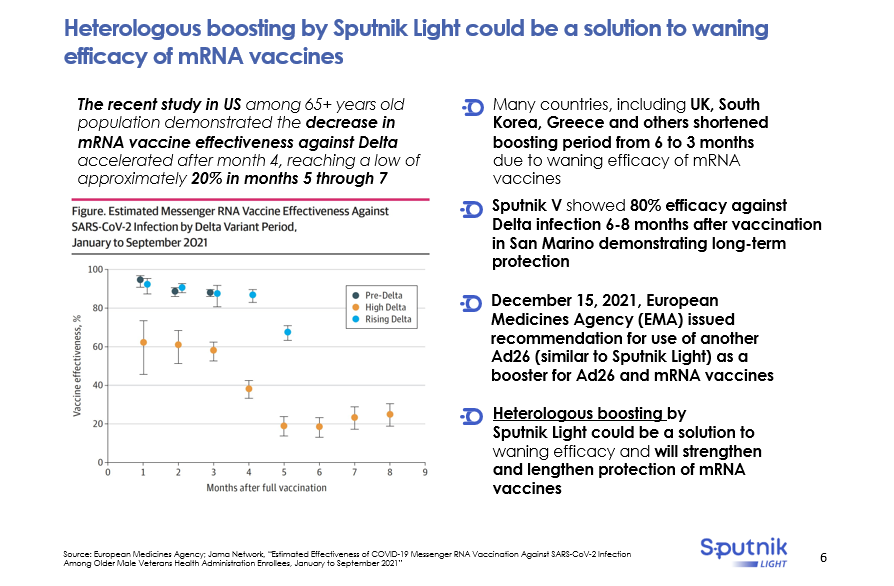
Sputnik V, virus vector vaccine for COVID-19, also known as Gam-COVID-Vac, induces a sustained neutralizing antibody response against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus.
It was announced by Russia’s Gamaleya Research Institute of Epidemiology and Microbiology whose specialists performed a preliminary analysis of the neutralizing activity of Sputnik V and found that it decreases by 11.8 times in the presence of Omicron.
The indicated reduction in the activity of Sputnik V is said to be substantially less than that demonstrated in the case of Comirnaty (tozinameran; BNT162b2) and Spikevax (elasomeran; mRNA-1273), mRNA vaccines for COVID-19 by Pfizer/BioNTech and Moderna, which showed 41- and 49–84-fold reductions, respectively.
- However, revised results for Comirnaty revealed a 21-fold decrease in neutralizing activity.
Moreover, the neutralizing activity of Sputnik V was tested on sera taken more than 6 months after vaccination, while the activity of Comirnaty and Spikevax was tested on sera taken a short period after vaccination, 12–27 and 28 days respectively.
In other words, it is claimed that Sputnik V provides long-term and reliable protection against Omicron.
Finally, the administration of a third (booster) dose of the vaccine, Sputnik Light, is expected to bring protection against Omicron to more than 80%. It is reported that after 2–3 months of administration of Sputnik Light, 100% of those vaccinated had antibodies against Omicron, while the third dose of Comirnaty provided antibodies only in 25% at 3 months after vaccination.
December 17
A study conducted by Imperial College London has come to a conclusion that differs dramatically from the universally replicated one. The course of COVID-19 infection caused by the Omicron variant (B.1.1.529) of SARS-CoV-2 is said to be as severe as that of the Delta variant (B.1.617.2).
It is stated that no evidence has been found that COVID-19 due to Omicron is milder, as judged by the proportion of symptomatic patients and the proportion who sought hospitalization. Despite the still limited data set, the severity of COVID-19 in Omicron is only marginally different from Delta.
- Meanwhile, media outlets around the world have been circulating the idea that Omicron does not pose any threat: they say Omicron is easy and people recover very quickly.
The British experts’ statement may well be correct because even those vaccinated and previously infected with COVID-19 are known to be infected with Omicron much more frequently than during outbreaks caused by other variants of the coronavirus. If the degree of protective immunity against severe COVID-19 still remains at a high level in such patients, the pattern would be that infection with Omicron leads to a milder course of the disease. Conversely, in the case of the unvaccinated and those who have not yet had COVID-19, infection with Omicron may well be as dangerous as other variants of coronavirus.
Of the other findings of the London experts the following:
- the number of Omicron infections doubles every 2.5 days
- the risk of reinfection with Omicron versus Delta is increased by a factor of 5.41 (95% CI: 4.87–6.00), indicating a relatively low level of immunity remaining after earlier COVID-19
- the immunity developed in COVID-19 disease survivors protects by 19% against reinfection under Omicron conditions within 6 months, whereas prior to Omicron, post-COVID-19 immunity protected by 85%
- the Omicron reinfection rates are highest among 18- to 29-year-olds
- the efficacy of vaccines against Omicron was drastically reduced: protective efficacy after two doses of vaccines was 0%–20%, after three doses it was 55%–80%.
- Report 49: Growth, population distribution and immune escape of Omicron in England. Imperial College London, December 16, 2021. [PDF]
- Report 48: The value of vaccine booster doses to mitigate the global impact of the Omicron SARS-CoV-2 variant. Imperial College London, December 16, 2021. [PDF]
↓
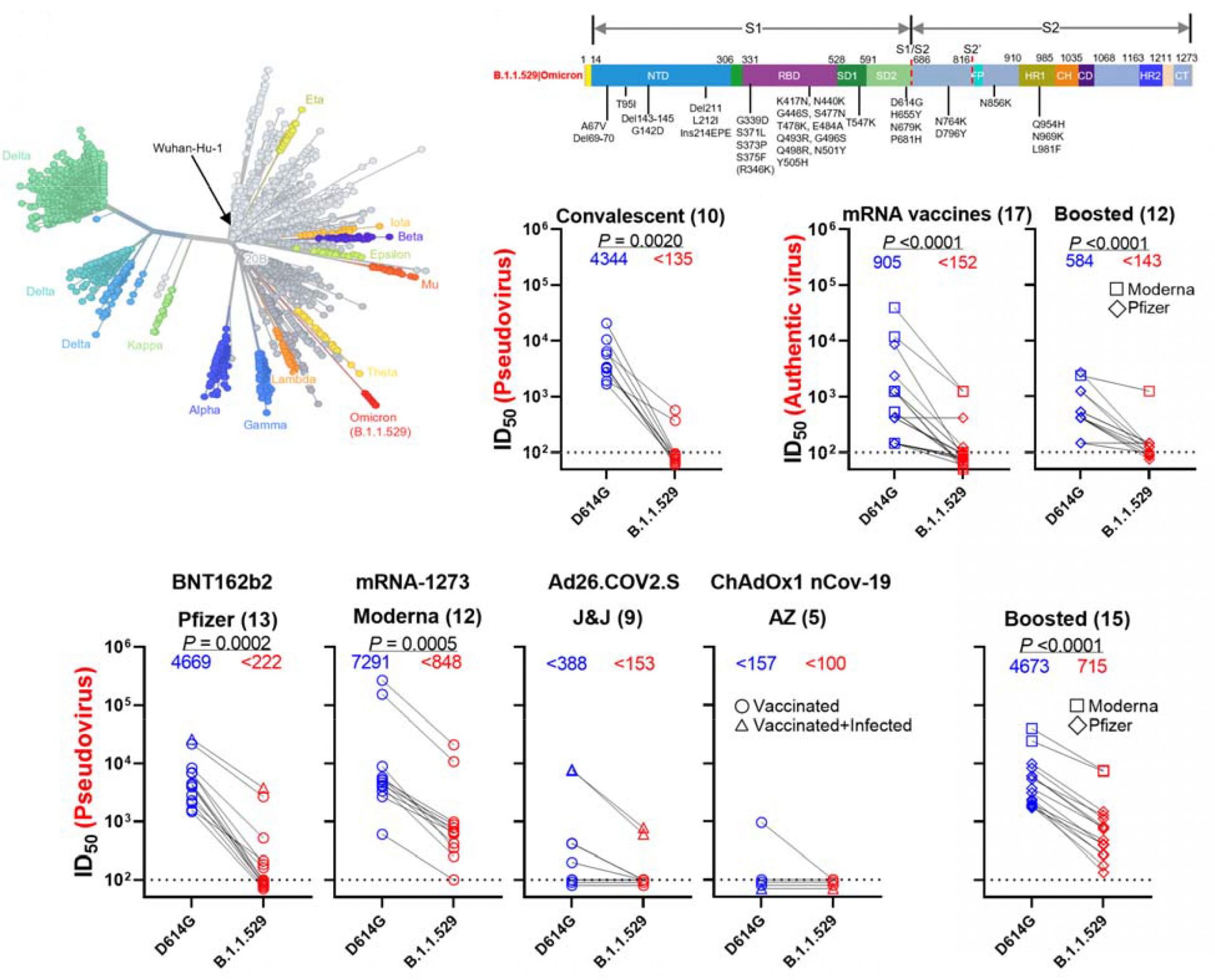
According to a study by American and Hong Kong scientists, the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus seriously suppresses the activity of neutralizing antibodies that are either produced by the body in response to vaccination, are ingested when monoclonal antibody therapeutic or preventative drugs are given, or are produced independently after having had COVID-19 disease. Omicron is a serious threat, raising the question of developing new vaccines and drugs that can deal with it.
First, the neutralizing activity of sera taken from unvaccinated and COVID-19 sufferers, tested in a pseudoviral system, was found to be 32 times reduced in the presence of the Omicron variant when compared to the antibody titer for the original non-mutant SARS-CoV-2 strain. At the same time, only 2 of its 10 samples had an antibody titer that exceeded the detection limit.
Second, the neutralizing activity of the vaccines fell sharply in the presence of Omicron, even if the serum samples were obtained from simultaneously vaccinated and transfected individuals. An additional (booster) dose of vaccine determined a rise in titers, but they were still decently low.
- The vaccines in question are the mRNA vaccines Comirnaty (tozinameran; BNT162b2) and Spikevax (elasomeran; mRNA-1273) by Pfizer/BioNTech and Moderna and the viral vector vaccines Vaxzevria/Covishield (AZD1222, ChAdOx1 nCoV-19, ChAdOx1-S) and Ad26. COV2.S by AstraZeneca and Janssen/Johnson & Johnson.
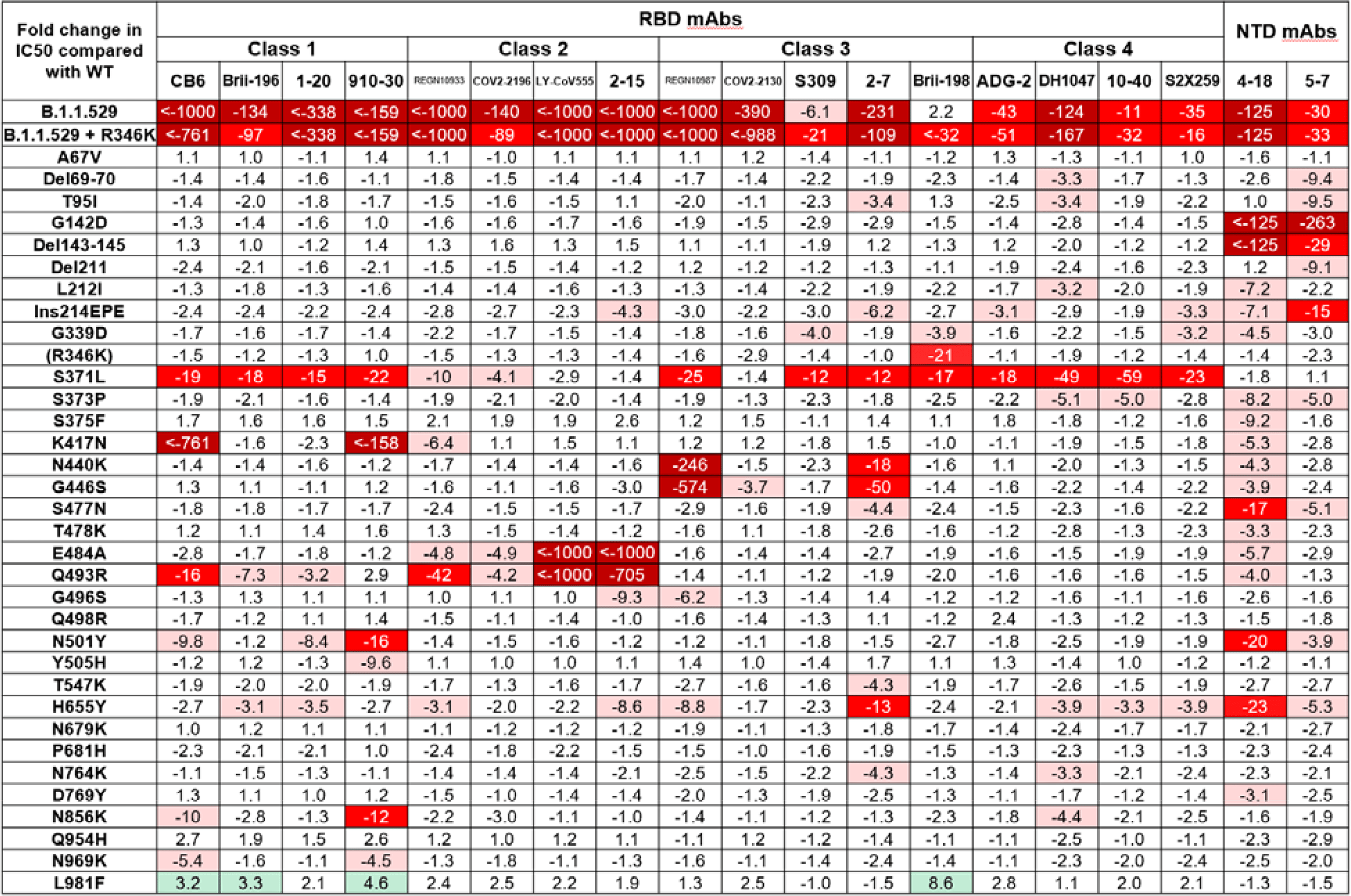
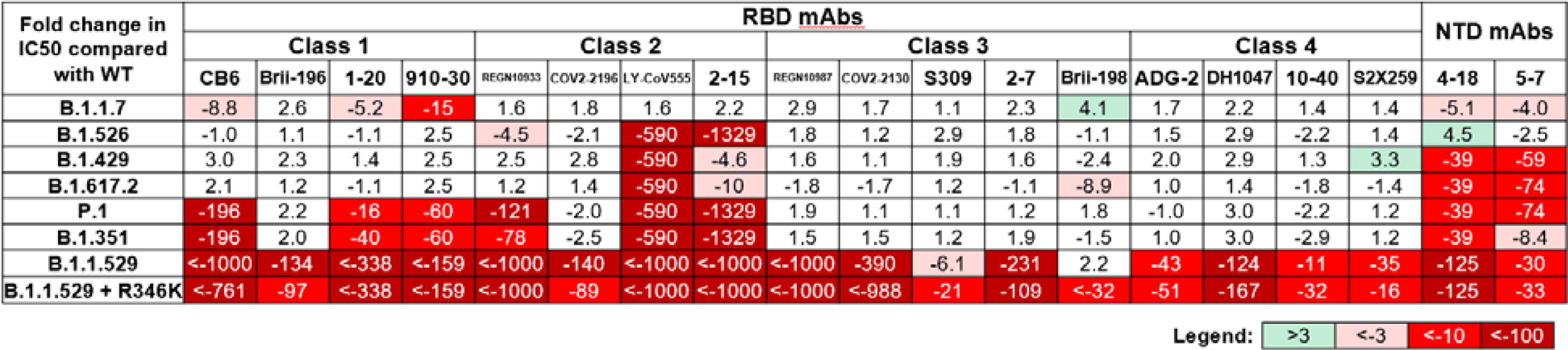
Third, monoclonal antibodies have shown, similar to vaccines, a decided lack of neutralizing activity against Omicron. And only a few have confirmed their ability to fight Omicron — at least their activity has not decreased so much as to speak boldly about the disappearance of efficacy. By the way, the researchers cite data on the change in neutralizing activity according to the presence of each of the three dozen mutations in the Omicron’s S protein.
- Among the monoclonal antibodies working against Omicron are Xevudy (sotrovimab, VIR-7831, GSK4182136), romlusevimab (BRII-198) and Evusheld (AZD7442) as a combination of tixagevimab (AZD8895) and cilgavimab (AZD1061) developed by GlaxoSmithKline/Vir Biotechnology, China’s Brii Biosciences, and AstraZeneca, respectively.
- Striking antibody evasion manifested by the Omicron variant of SARS-CoV-2. bioRxiv, December 15, 2021. [PDF]
December 16
New coronaviruses will continue to infect bats and other animal reservoirs and potentially represent a pandemic threat to humanity. To counter future outbreaks of coronavirus infections, the global scientific and medical research community must focus its efforts on three goals. First, to characterize the range of genetic diversity of coronaviruses in different animal species. Second, to understand the pathogenesis of coronavirus infections. Third, to apply the accumulated knowledge to develop universal coronavirus vaccines.
Universal vaccines that work against all coronaviruses should be ideal.
Leading experts from the National Institute of Allergy and Infectious Diseases (NIAID), part of the U.S. National Institutes of Health (NIH), David Morens, Jeffery Taubenberger, and Anthony Fauci, have urged the global biotechnology industry to develop universal coronavirus vaccines.
Universal Coronavirus Vaccine
The biotechnology industry must come up with a comprehensive defense against all coronaviruses.
↓
Evusheld (AZD7442), an AstraZeneca drug that is a combination of tixagevimab (AZD8895) and cilgavimab (AZD1061) monoclonal antibodies, retains neutralizing activity against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus, according to an FDA study.
The half-maximal inhibitory concentration (IC50), as an indicator of the neutralizing ability of the antibody, for Evusheld under the Omicron conditions decreased dramatically but still fell within the range of 171–277 μg/mL, which is in between neutralizing titers in people previously infected with the coronavirus. By comparison, the IC50 of Evusheld in the original non-mutant SARS-CoV-2 is 1.3–1.5 μg/mL.
Evusheld is approved by FDA for use in pre-exposure COVID-19 prophylaxis in individuals who, for health reasons or immune status, cannot mount an adequate immune response after vaccination against SARS-CoV-2. Evusheld protects against the development of COVID-19 for six months or longer.

Evusheld: First Drug for Strong and Long-Lasting Protection Against Coronavirus
One dose of AstraZeneca’s monoclonal antibody cocktail protects against COVID-19 for six months or longer.
↓
Regeneron Pharmaceuticals reported that its REGEN-COV/Ronapreve (casirivimab + imdevimab) is active against all known SARS-CoV-2 variants of concern, including Omicron (B.1.1.529) and Delta (B.1.617.2). However, casirivimab and imdevimab are less active against Omicron than Delta.
Regeneron is said to have several experimental monoclonal antibodies against SARS-CoV-2 in its hands that neutralize Omicron and Delta. Their clinical trials are scheduled for 2022.
The REGEN-COV/Ronapreve monoclonal cocktail is now being used to treat mild-to-moderate COVID-19 in high-risk patients at danger of hospitalization or death, as well as for post-exposure prophylaxis of COVID-19 in individuals at risk for severe disease.
↓
Specialists at the Li Ka Shing Faculty of Medicine of the University of Hong Kong (HKUMed) have figured out the specifics of how the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus infects human respiratory tracts.
Thus, Omicron infects the bronchi and replicates in them 70 times faster than the Delta variant (B.1.617.2) and the original non-mutant coronavirus do. This fact likely explains why Omicron is transmitted faster from the infected to the healthy.
Omicron replicates 10-fold slower in the lungs compared to the original SASR-CoV-2, and therefore COVID-19 disease is probably milder.
It should be understood, however, that Omicron, while highly contagious, infects many more people and therefore statistically can cause more severe illness and death, even if it is less pathogenic. Given that Omicron, which has an abundance of mutations, is able to evade vaccines and the immunity acquired after suffering COVID-19, the degree to which Omicron threatens humanity is quite significant.

↓
According to the U.S. study, Moderna’s Spikevax (elasomeran; mRNA-1273) mRNA vaccine showed a 49–84-fold decrease in neutralizing activity against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus based on serum samples taken 4 weeks after receiving it in two doses.
The addition of a third (booster) dose of Spikevax increased neutralizing antibody titers, thereby reducing the risk of symptomatic breakthrough COVID-19 infection. However, vaccine activity was still reduced 4.2–6.5-fold.
- Booster of mRNA-1273 vaccine reduces SARS-CoV-2 omicron escape from neutralizing antibodies. medRxiv, December 15, 2021. [PDF]

December 15
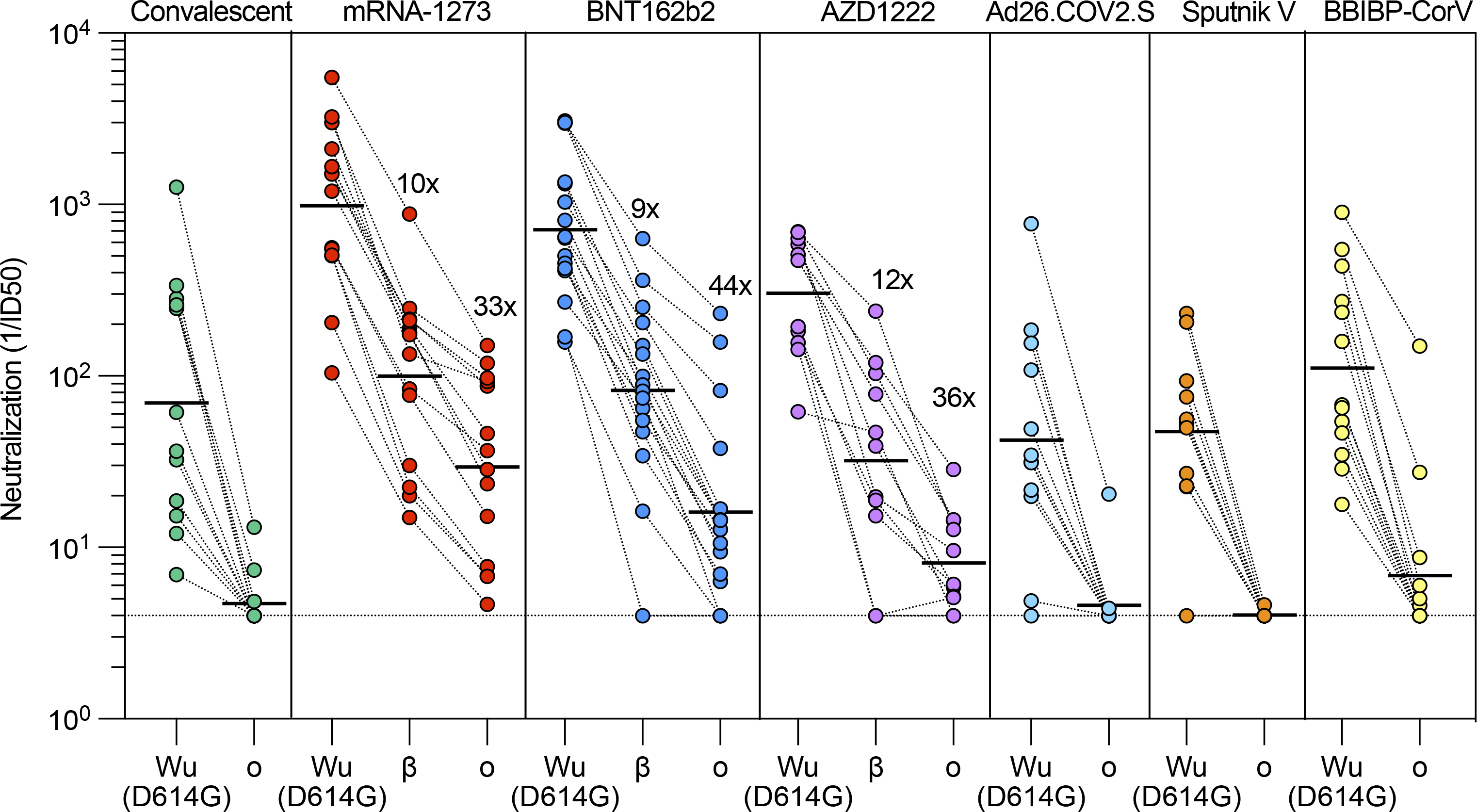
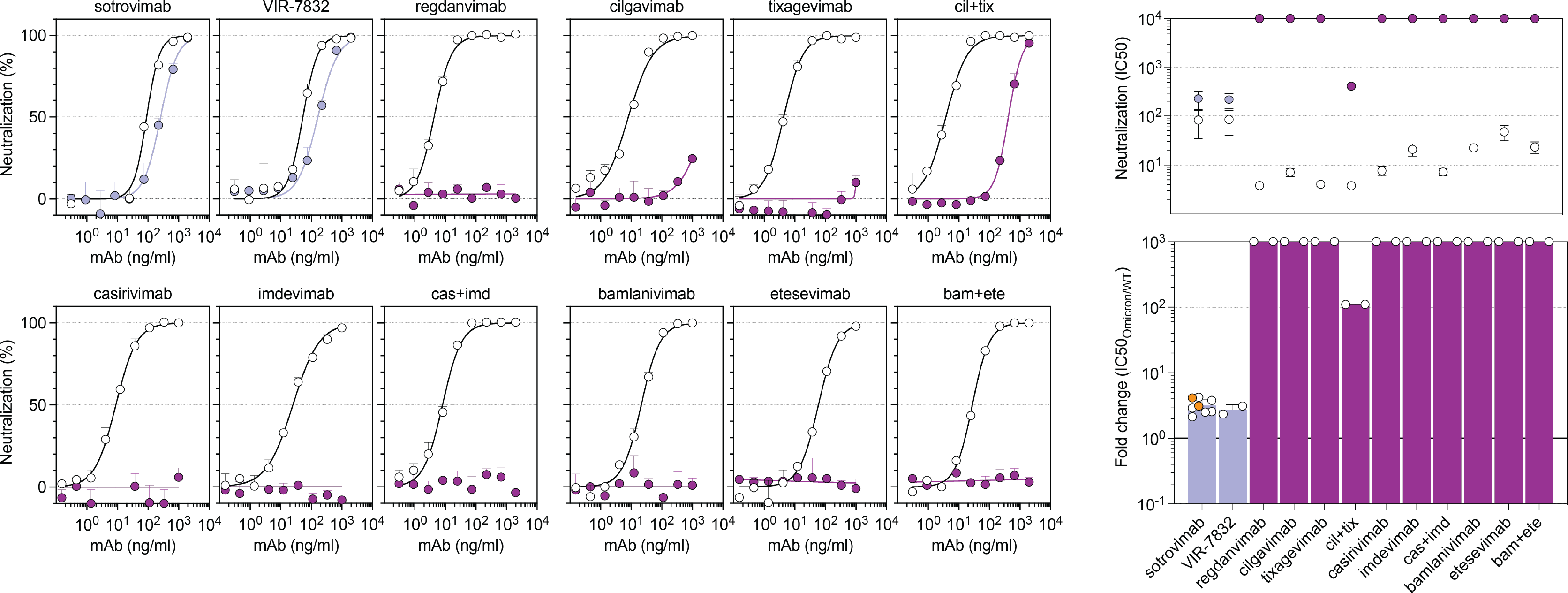
Experts from Humabs BioMed, a Swiss company owned by Vir Biotechnology, analyzed many vaccines and monoclonal antibodies approved by regulators in terms of their ability to fight the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. The efficacy of the vaccines and monoclonal antibodies has been found to drop dramatically in the presence of Omicron. Experts recommend a third (booster) dose of vaccine as a matter of urgency to do something about the situation.
The neutralizing anti-Omicron activity of the following vaccines and monoclonal antibodies was analyzed:
- mRNA vaccine Spikevax (elasomeran; mRNA-1273) by Moderna
- mRNA vaccine Comirnaty (tozinameran; BNT162b2) by Pfizer and BioNTech
- viral vector vaccine Vaxzevria/Covishield (AZD1222, ChAdOx1 nCoV-19, ChAdOx1-S) by AstraZeneca
- viral vector vaccine Ad26.COV2.S by Janssen, part of Johnson & Johnson
- viral vector vaccine Sputnik V (Gam-COVID-Vac) by Russia’s Gamaleya Research Institute of Epidemiology and Microbiology
- inactivated whole-virion vaccine BBIBP-CorV [SARS-CoV-2 Vaccine (Vero Cell), Hayat-Vax] by China’s Sinopharm, also known as the China National Pharmaceutical Group
- monoclonal antibodies bamlanivimab (LY-CoV555) and etesevimab (LY-CoV016) by Eli Lilly, Canada’s AbCellera Biologics, and China’s Shanghai Junshi Biosciences
- monoclonal antibodies casirivimab (REGN-10933) and imdevimab (REGN-10987) — REGEN-COV/Ronapreve by Regeneron Pharmaceuticals
- monoclonal antibodies tixagevimab (AZD8895) and cilgavimab (AZD1061) — Evusheld (AZD7442) by AstraZeneca
- monoclonal antibody regdanvimab — Regkirona by Korea’s Celltrion
- monoclonal antibody sotrovimab (VIR-7831, GSK4182136) — Xevudy by GlaxoSmithKline and Vir Biotechnology.
An in vitro test in a pseudovirus system revealed that a full course of vaccination (two doses each; in the case of Ad26.COV2.S one dose) with Ad26.COV2.S, Sputnik V, or BBIBP-CorV would not protect against the Omicron infection. The titer of neutralizing antibodies produced by the body in response to administration of these vaccines was too low compared to the original non-mutant SARS-CoV-2 to reliably control Omicron. In other words, Ad26.COV2.S, Sputnik V, and BBIBP-CorV vaccines are ineffective against Omicron — in any case without a booster dose.
The Gamaleya Research Institute of Epidemiology and Microbiology in response to the results stated the following:
A recently published small study addresses Sputnik vaccine’s efficacy against Omicron variant deliberately using serum samples that are not representative. For example, this study used Sputnik samples with a lower virus neutralization ability against SARS-COV-2 than AstraZeneca’s vaccine while a much larger study in Argentina based on representative serum samples demonstrated 1.8 times higher virus neutralizing titers against SARS-COV-2 for Sputnik, which is explained by its heterologous boosting advantage. Therefore, conclusions about Sputnik efficacy against Omicron based on wrong serum samples, cannot be made. Within the next 7 days the Gamaleya Center will publish its own positive data based on representative serum samples on Omicron neutralization ability for both Sputnik V vaccine and one-shot Sputnik Light as a booster.
Vaccination with two doses of Spikevax, Comirnaty, or Vaxzevria/Covishield provided antibody activity against Omicron, although the neutralizing antibody titer decreased by a factor of 33, 44, and 36, respectively. Remarkably, the decrease was less pronounced (5-fold) in Comirnaty vaccinated individuals who had been previously infected, indicating an extended antigenic response due to maturation of affinity due to multiple antigenic stimulations.
The neutralizing activity of most monoclonal antibodies proved insufficient to counteract Omicron. Simply put, they are useless against Omicron. Only sotrovimab, Evusheld (tixagevimab + cilgavimab), and the experimental VIR-7832 (GSK4182137) by Vir worked against Omicron.
- Broadly neutralizing antibodies overcome SARS-CoV-2 Omicron antigenic shift. bioRxiv, December 14, 2021. [PDF]
↓
German scientists analyzed the neutralizing activity of a number of monoclonal antibodies, both commercially available and still experimental, assessing their ability to cope with the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus.
The monoclonal antibodies in question are the following:
- bamlanivimab (LY-CoV555) and etesevimab (LY-CoV016) by Eli Lilly, Canada’s AbCellera Biologics, and China’s Shanghai Junshi Biosciences
- casirivimab (REGN-10933) and imdevimab (REGN-10987) — REGEN-COV/Ronapreve by Regeneron Pharmaceuticals
- sotrovimab (VIR-7831, GSK4182136) — Xevudy by GlaxoSmithKline and Vir Biotechnology
- P2B-2F6, Fab2-36, and C102 are being studied in academia [1] [2] [3] [4]
- BI 767551 (DZIF-10c) by Boehringer Ingelheim (development stopped in summer 2021 due to strong market competition).
A study of the Omicron variant in pseudovirus neutralization assays found that in vitro the monoclonal antibodies indicated were very poor at suppressing it. Thus, starting from a half-maximal inhibitory concentration (IC50) exceeding 10 µg/ml, we can safely declare a failure against Omicron. Here too, only sotrovimab and BI 767551 emerged victorious, convincingly defeating Omicron as well as Alpha (B.1.1.7), Beta (B.1.351), and Delta (B.1.617.2) variants.

Sotrovimab Is Effective Against Omicron Variant of Coronavirus
A monoclonal antibody developed by GlaxoSmithKline and Vir Biotechnology successfully counteracts a new strain of SARS-CoV-2.
As shown, bamlanivimab, etesevimab, casirivimab, and imdevimab, actively promoted for the treatment of mild-to-moderate COVID-19 among high-risk patients, could not deal with Omicron.
- mRNA booster immunization elicits potent neutralizing serum activity against the SARS-CoV-2 Omicron variant. medRxiv, December 14, 2021. [PDF]

↓
Adagio Therapeutics reported that experimental monoclonal antibody ADG20 did not work against the Omicron variant. When this drug candidate was tested in vitro on the coronavirus itself and in a pseudovirus system, ADG20’s neutralizing activity against Omicron dropped by more than 300 times. Adagio believes the failure is due to an abundance of mutations in the Omicron’s S protein, a combination of which helps the variant evade ADG20. ADG10, another experimental monoclonal antibody, also failed at suppressing Omicron. The disappointing news collapsed Adagio’s stock price by 75%.
ADG20 was considered a very promising drug for therapy and prophylaxis of any variant of coronavirus, current and upcoming, because, unlike other monoclonal antibodies against SARS-CoV-2, it targets an epitope of the virus that is highly conserved, immunoreactive, and not an easy target for the endogenous neutralizing antibody response.
ADG20: Cure for All Mutant Variants of SARS-CoV-2
Adagio Therapeutics’ monoclonal antibody will help fight all strains of the coronavirus.
December 14
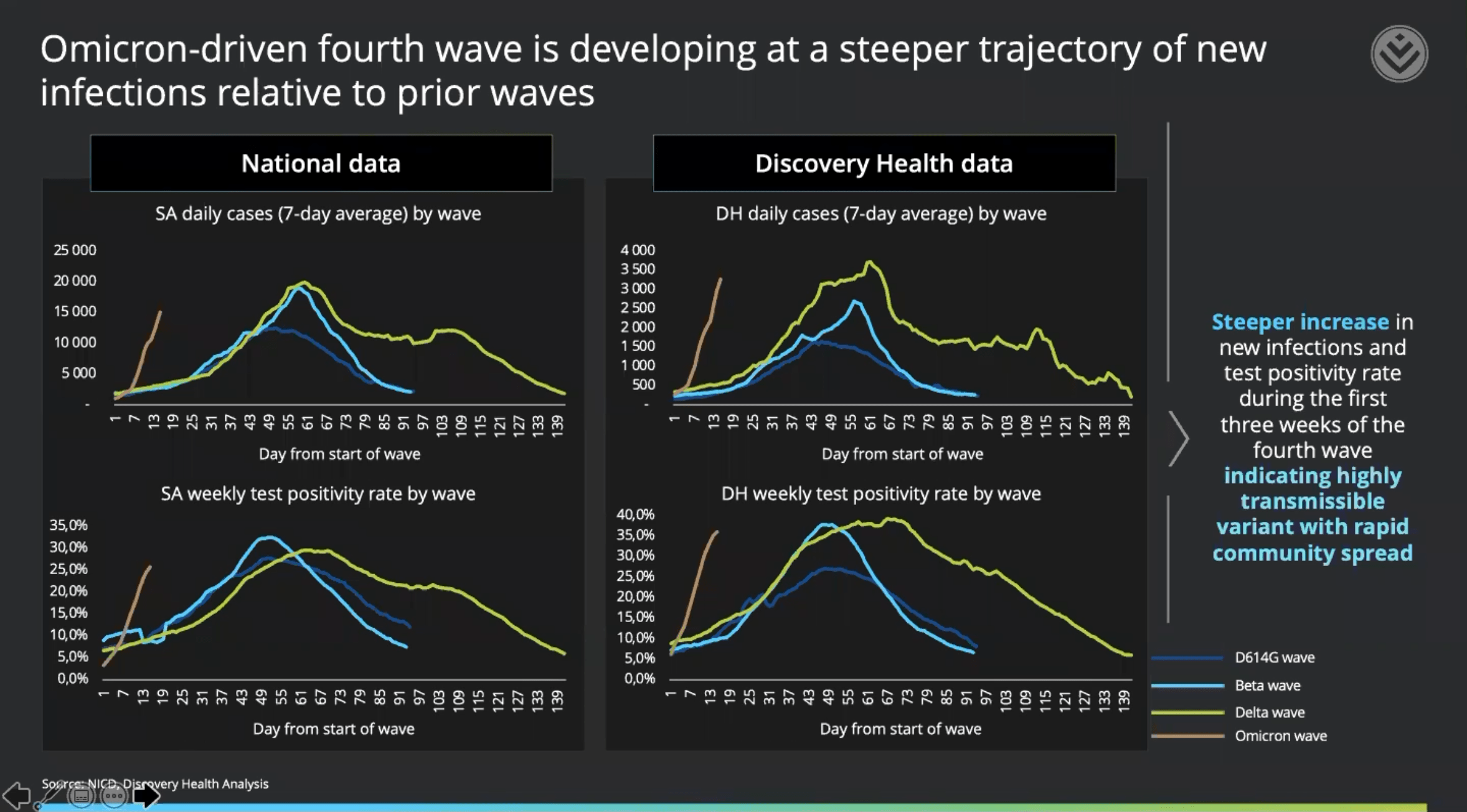
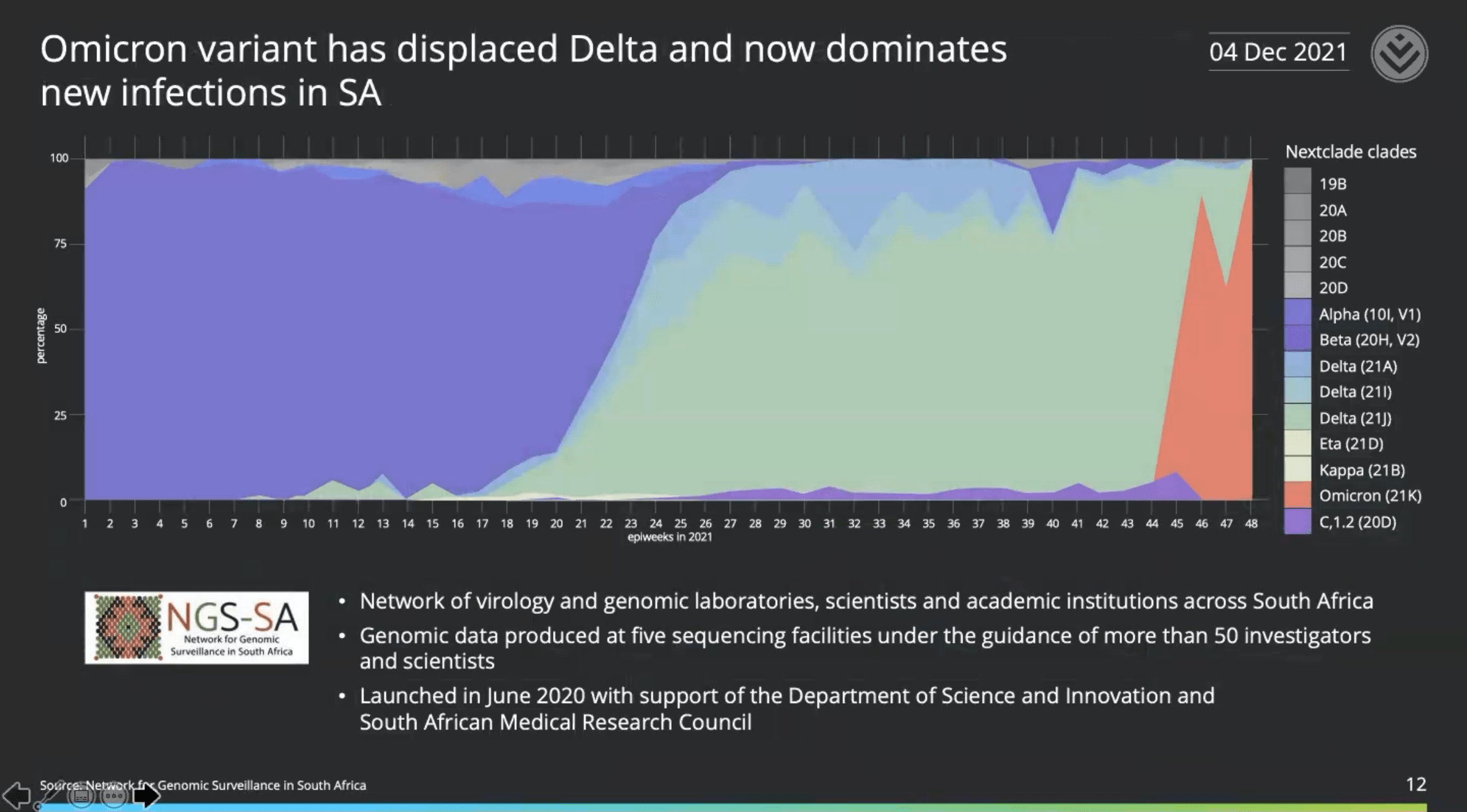
Discovery Health, the largest private health insurance provider in the Republic of South Africa (RSA), has shared the results of a large-scale analysis of the outbreak of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus based on data from over 211 000 tests. The conclusions, based on real data rather than theoretical or laboratory ones, are as follows.
Omicron is now the dominant variant in South Africa, accounting for 90% of new coronavirus cases, with an exponential increase in infections.
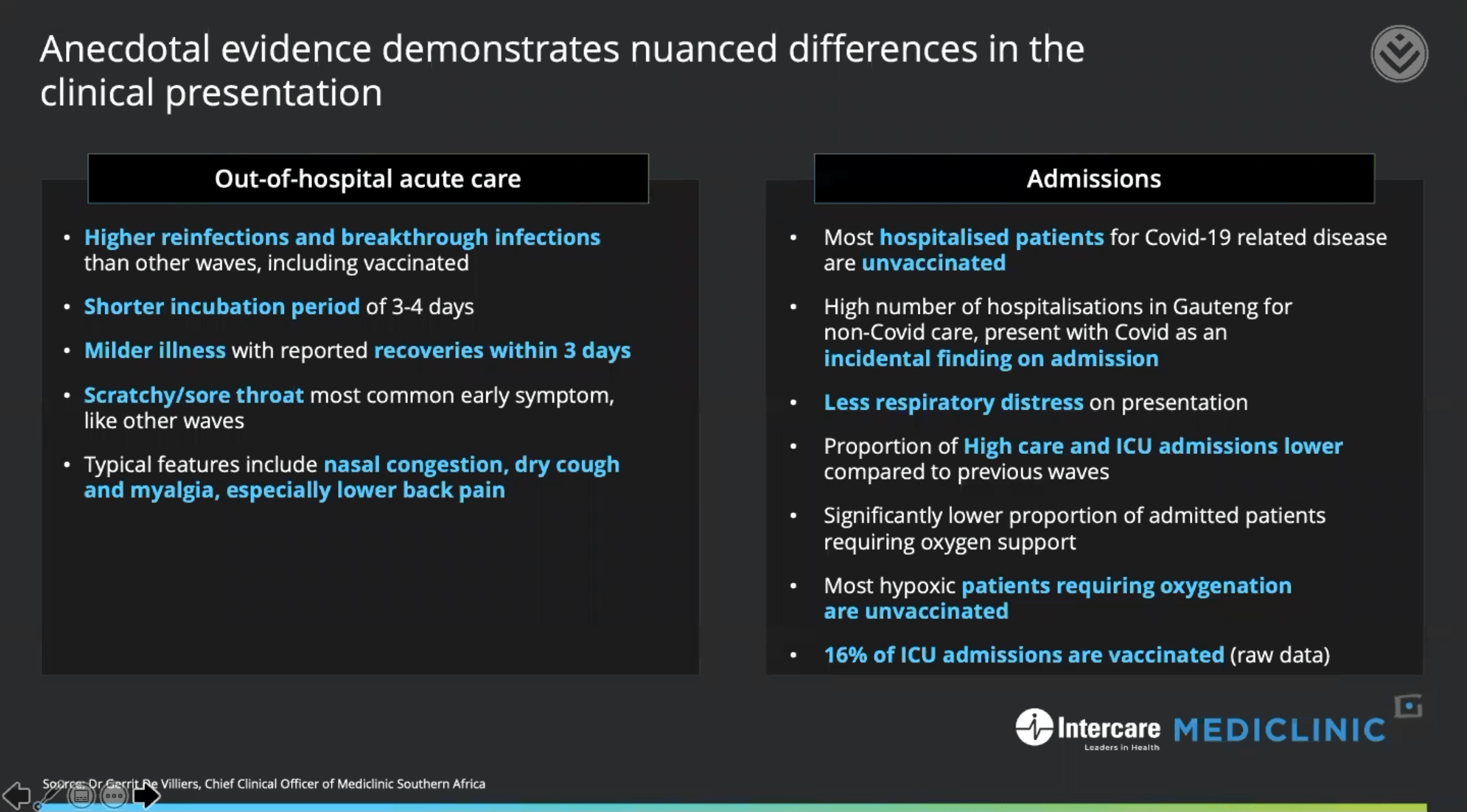
The Omicron outbreak is characterized by a higher number of reinfections and breakthrough infections than other coronavirus variants, including among vaccinated individuals.
Clinical features of Omicron in adults include a shortened incubation period of up to three to four days; a generally mild course of illness with recovery within three days; scratchy and/or sore throat is the most common early symptom (as with other SARS-CoV-2 variants, however); and nasal congestion, dry cough, and myalgia (especially low back pain) among others symptoms of Omicron.
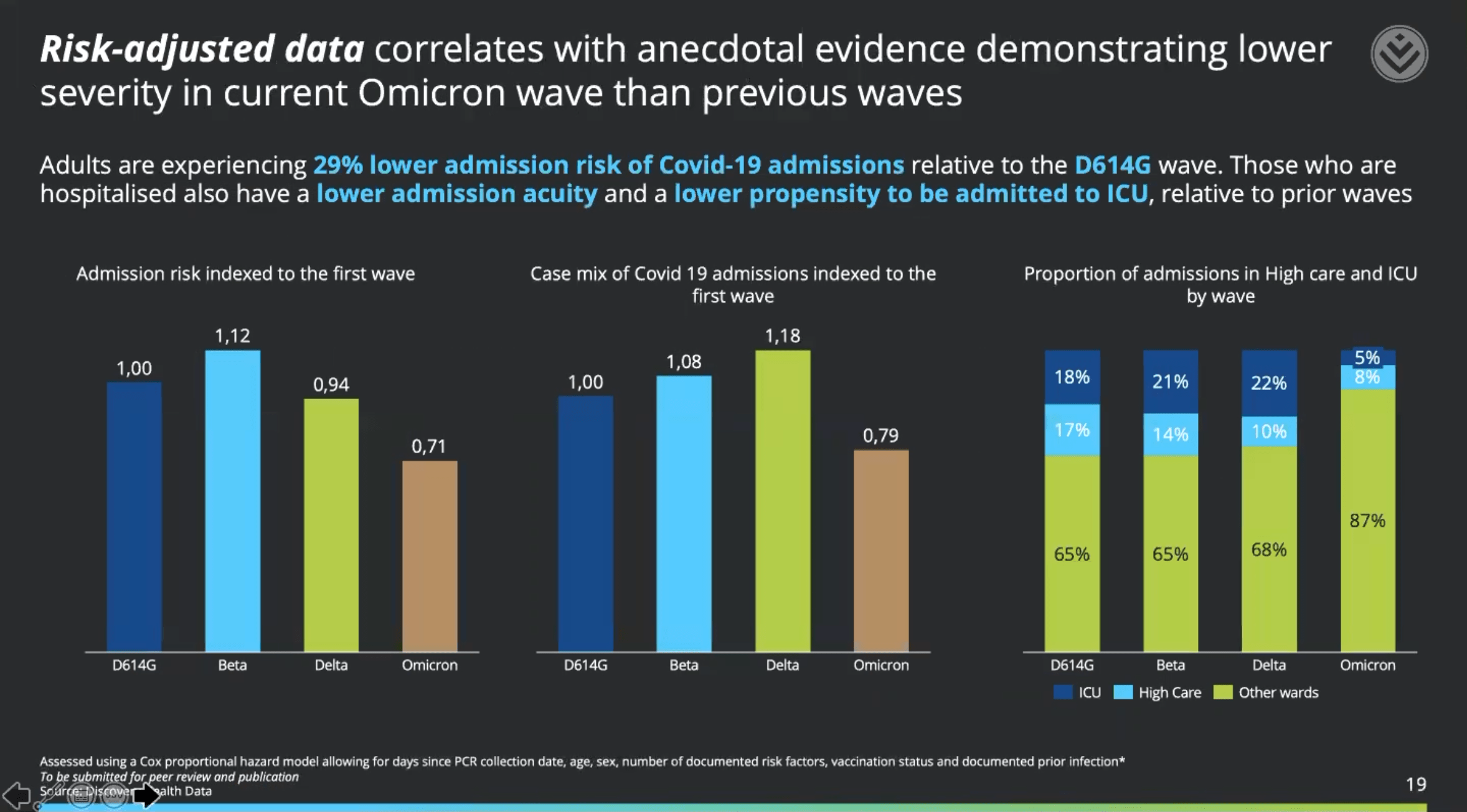
In adults hospitalized with Omicron, there is a reduced incidence of acute respiratory distress syndrome (ARDS); a reduced rate of ICU admission; and a reduced proportion of patients requiring oxygen support, which, if needed, is provided in most cases to the unvaccinated.
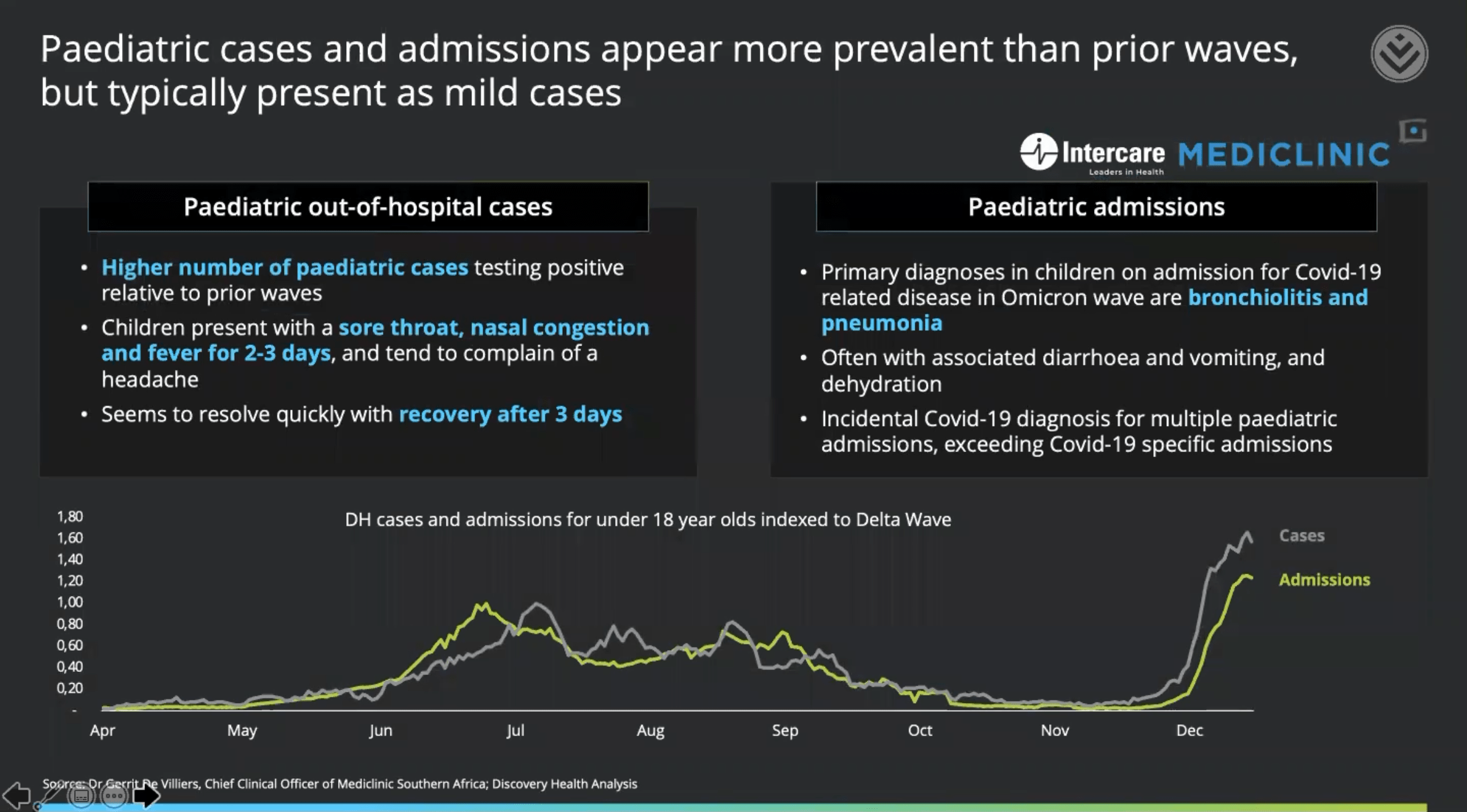
Clinical features of Omicron in children and adolescents, which, incidentally, is diagnosed more frequently than in coronavirus waves of other variants, include mostly mild course of illness with recovery within three days; symptoms of Omicron include sore throat, nasal congestion, headache, and fever for two to three days.
Children and adolescents are hospitalized with Omicron complications such as bronchiolitis and pneumonia; diarrhea, vomiting, and dehydration are common.
Two doses of mRNA vaccine Comirnaty (tozinameran; BNT162b2) by Pfizer and BioNTech provided 70% protection (compared with unvaccinated individuals) against development of Omicron-induced COVID-19 infection that was severe or critical and required hospitalization, and 33% against development of symptomatic COVID-19.
- Against the Delta variant (B.1.617.2), Comirnaty protected better: at 93% and 80%, respectively.
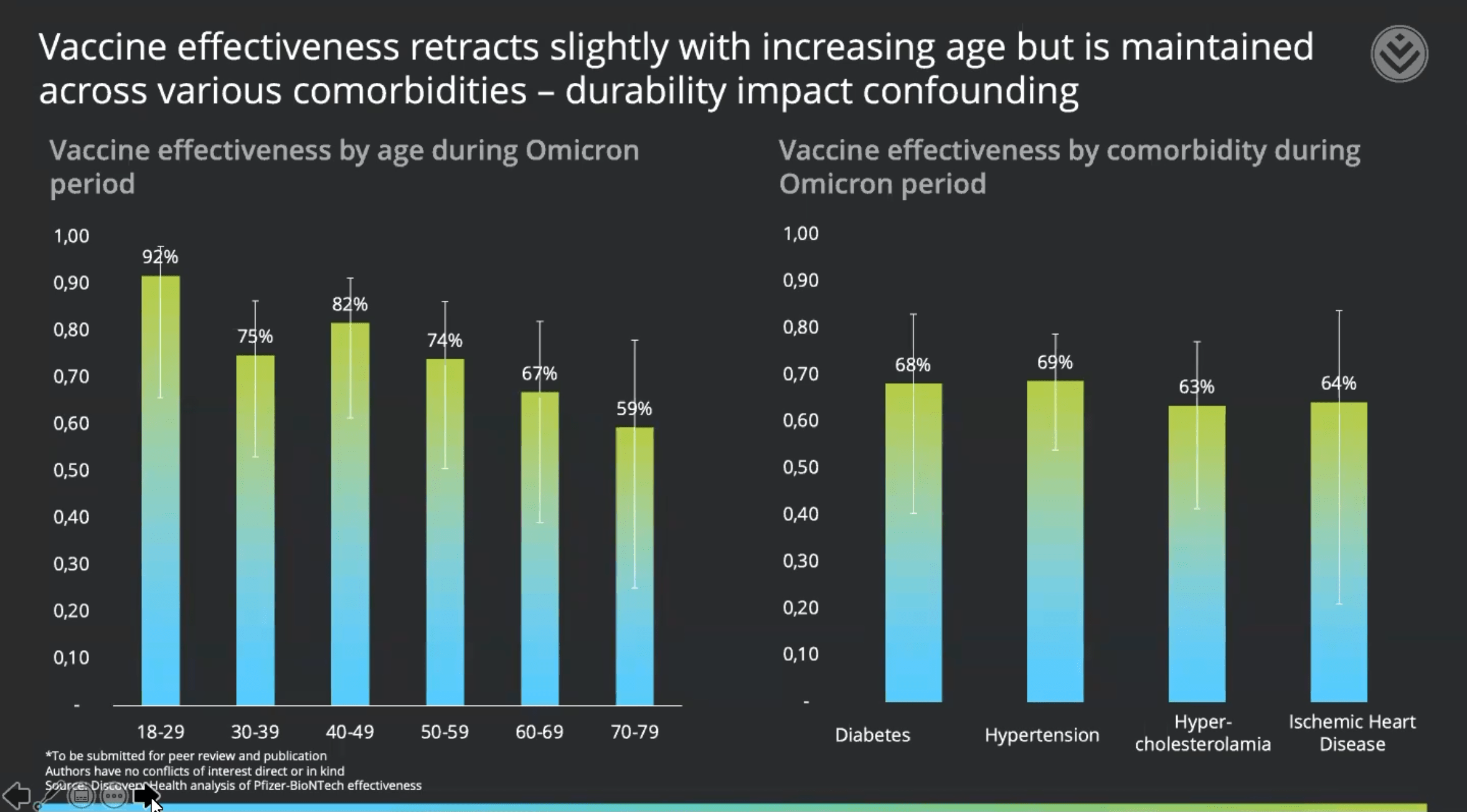
There was a correlation between age and the level of vaccine protection of Comirnaty against Omicron, infection with which led to hospitalization. Thus, the effectiveness of Comirnaty generally fell as a function of age: 82% for ages 40–49 years, 74% for ages 50–59 years, 67% for ages 60–69 years, and 59% for ages 70–79 years.
In the presence of comorbidities contributing to an increased risk of hospitalization due to COVID-19, Comirnaty in the Omicron setting provided the following level of protection: 68% for diabetes mellitus, 69% for hypertension, 63% for hypercholesterolemia, and 64% for coronary heart disease.
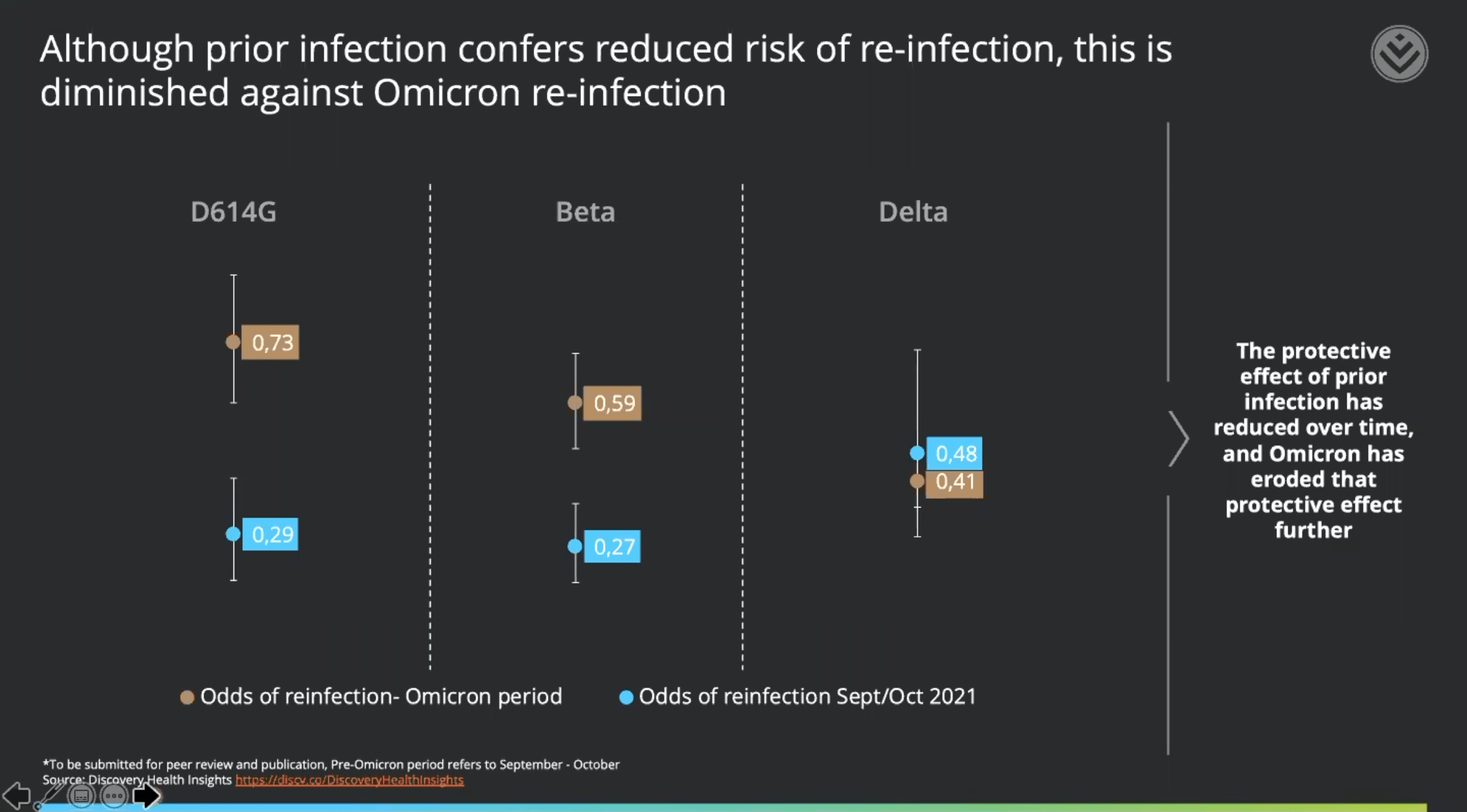
For people who have already been infected with COVID-19, the risk of reinfection with Omicron is significantly higher when compared to other variants of the coronavirus. Thus, among those previously infected with the Delta variant, the risk of reinfection with Omicron increased by 40%, with the Beta variant (B.1.351) by 60%, and with the original coronavirus with the D614G mutation by 73%.
- The D614G mutation was previously one of the most common mutations in the world: as of mid-2020 (during the first COVID-19 wave), it was the dominant mutation in the coronavirus pandemic. One of the clinical features of D614G is loss of smell.
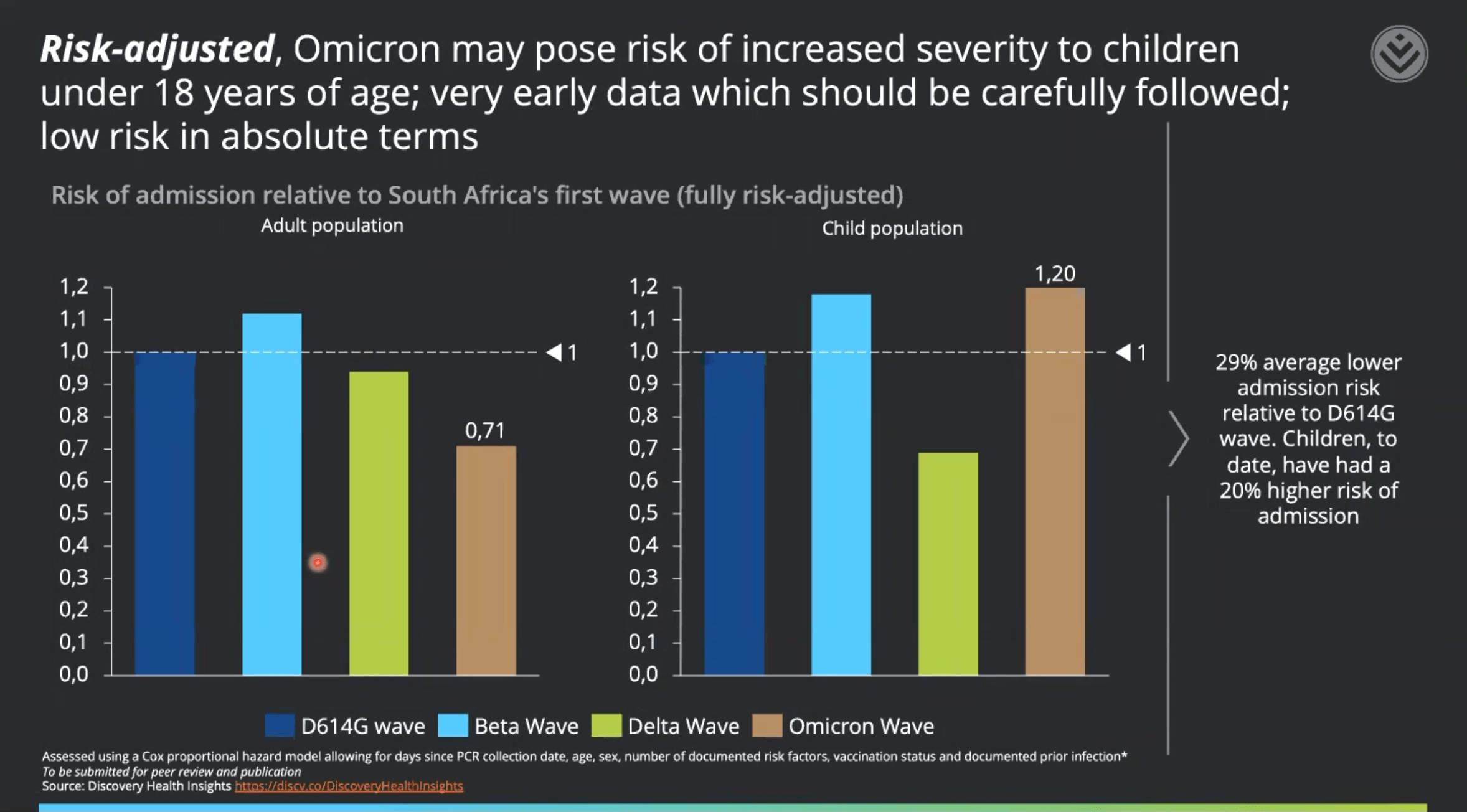
Omicron-infected adult patients have a 29% lower risk of hospitalization when compared to infection with the original coronavirus with the D614G mutation.
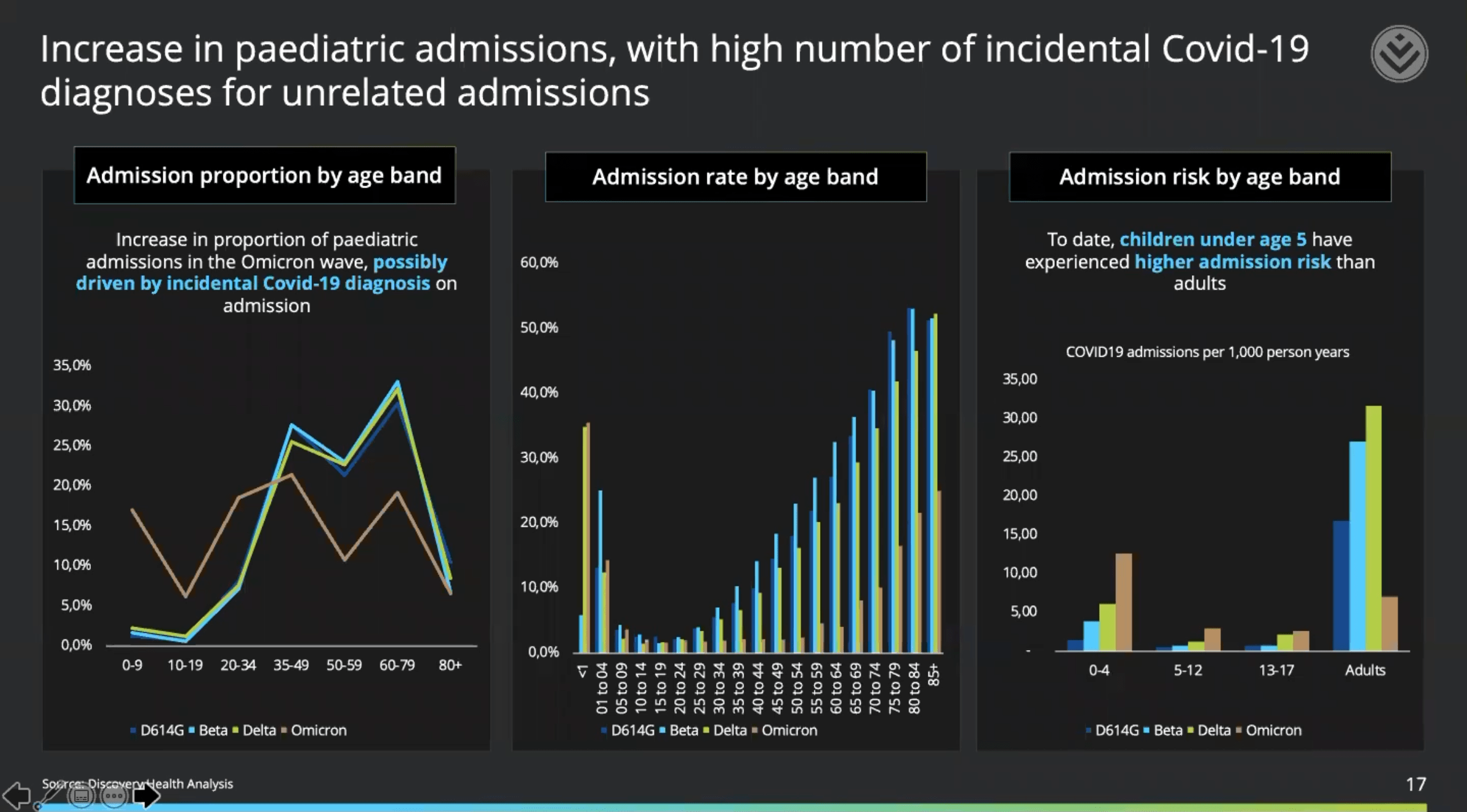
Despite the very low absolute incidence of COVID-19 disease in children and adolescents, preliminary data suggest that those under 18 years of age infected with Omicron have a 20% higher risk of hospitalization when compared with infection with the D614G mutant original coronavirus. At the same time, the maximum risk of hospitalization due to Omicron was recorded for children under 5 years of age.
↓
It should be understood that the conclusions are based on data from the first three weeks of the Omicron outbreak, and therefore are preliminary and may change in the future. The conclusions may have been affected by biases associated with the high prevalence of antibodies against SARS-CoV-2 in the general South African population.
A study conducted by experts at the Li Ka Shing Faculty of Medicine of the University of Hong Kong (HKUMed) found that the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus escapes the neutralizing antibodies produced by the organism after vaccination, and therefore the effectiveness of existing vaccines drops dramatically.
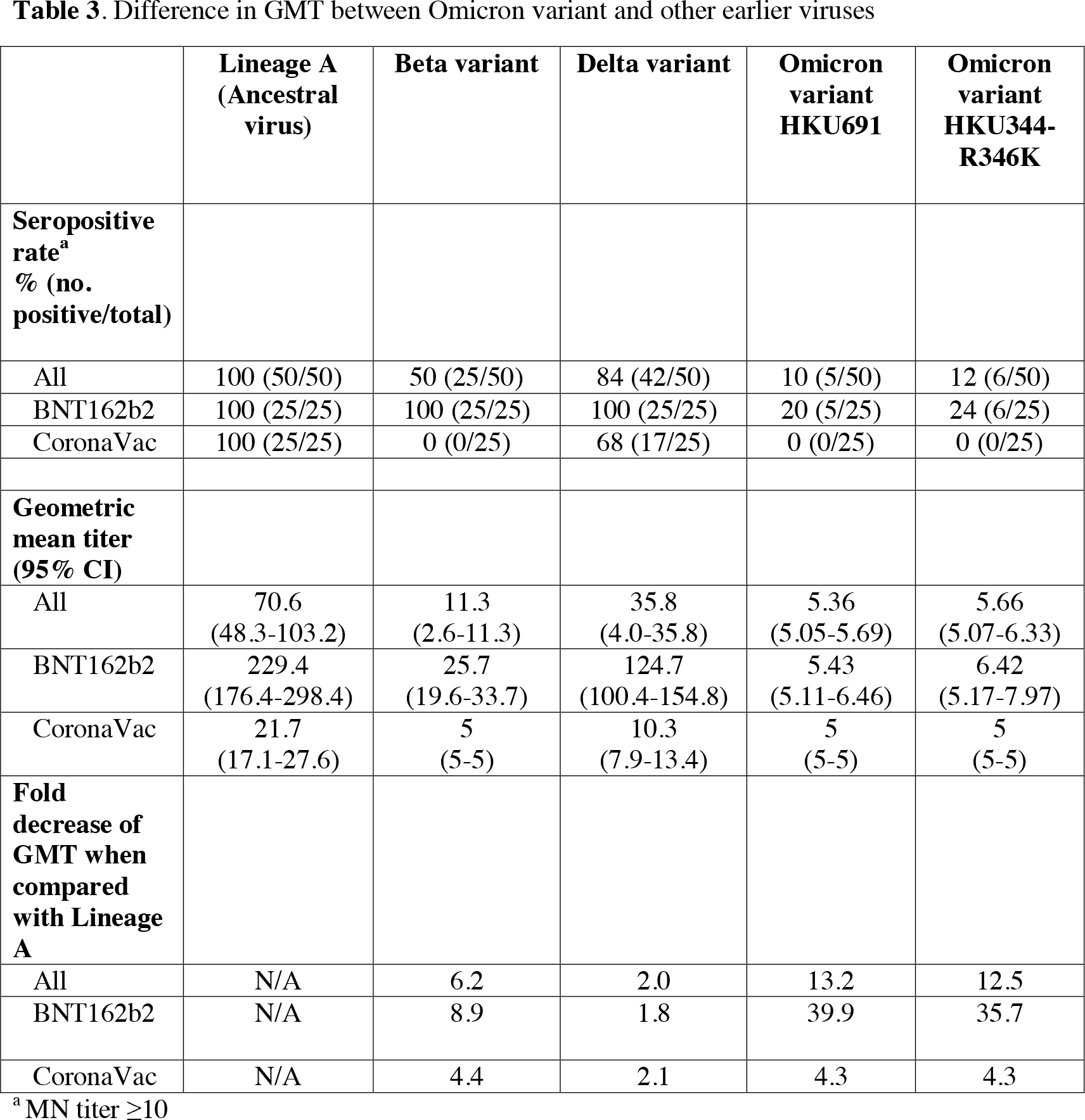
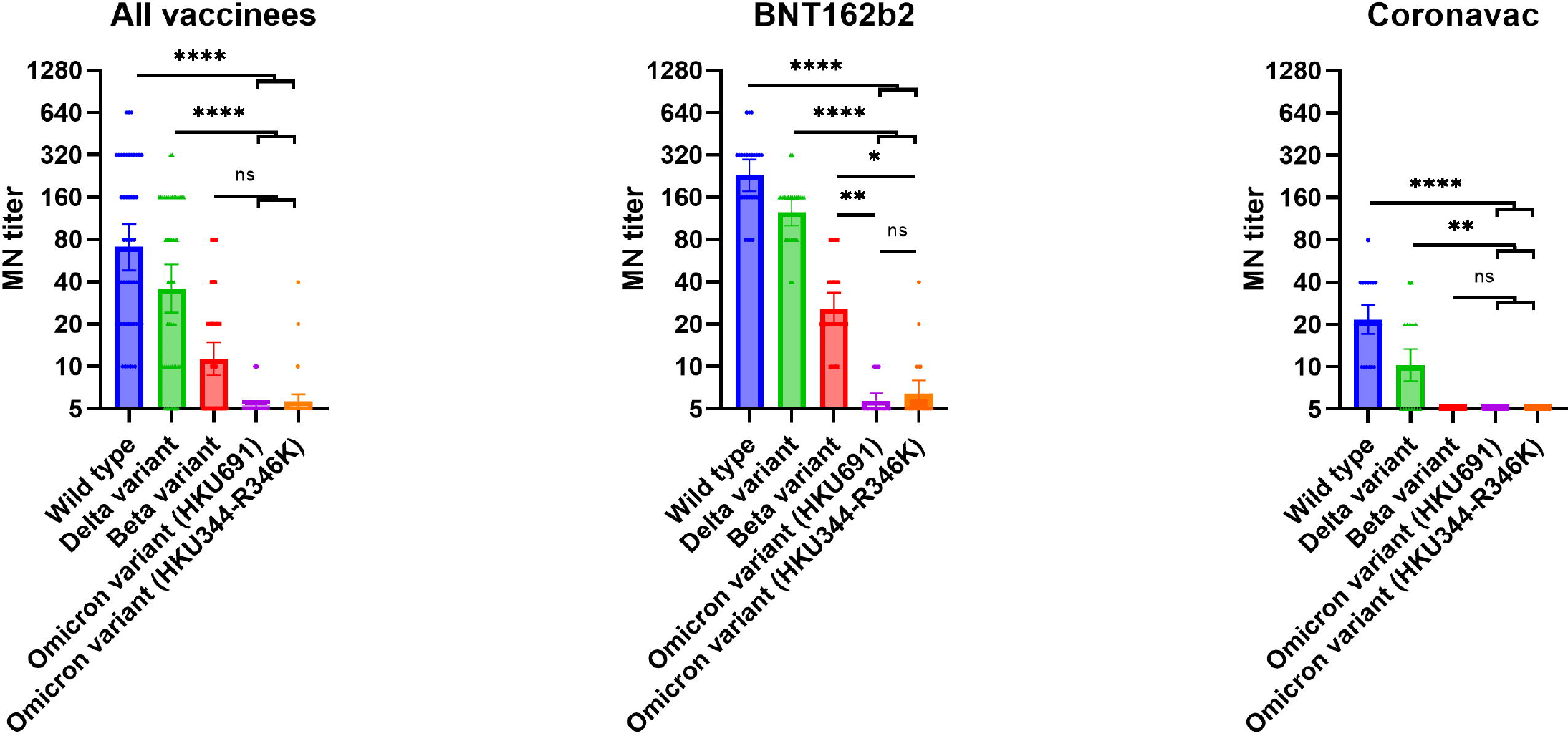
Geometric mean titer (GMT) of neutralizing antibodies in serum samples taken from those vaccinated with two doses of mRNA vaccine Comirnaty (tozinameran; BNT162b2) by Pfizer and BioNTech, was 39.9 and 35.7 times lower in Vero E6 cell culture of Omicron isolates HKU691 and HKU344-R346K when compared with titers in the culture of the original non-mutant coronavirus. At the same time, the seropositive rate (the frequency with which antibodies occur) against these Omicron isolates was only 20% and 24%. The GMT against Beta (B.1.351) and Delta (B.1.617.2) variants decreased 8.9- and 1.8-fold, but the seropositive rate remained 100%.
- Omicron isolates HKU691 and HKU344-R346K differ in two nucleotides: HKU344-R346K contains the nonsynonymous G22599A mutation leading to the R346K mutation in S protein; it was found in 8.5% of sequenced Omicron genomes in the GISAID database as of December 10, 2021. The R346K mutation is of particular concern because it affects receptor-binding domain (RBD), which was once reflected in reduced vaccine efficacy against the Mu variant, which also carries this mutation.
The GMT of neutralizing antibodies in serum samples taken from two doses of inactivated whole-virion vaccine CoronaVac developed by China’s Sinovac Biotech, which is considered to be the most popular in the world, was 4.3 times lower in Vero E6 cell culture of HKU691 and 157 HKU344-R346K Omicron isolates and 4.4 and 2.1 times lower in the culture of Beta and Delta variants when compared with the titer in the culture of the original non-mutant coronavirus. The seropositive rate was zero for Omicron and Beta variants and 68% for Delta variant.
To summarize, the efficacy of Comirnaty vaccine against Omicron decreased dramatically, but was maintained against Delta and Beta. The CoronaVac vaccine against Omicron and Beta did not work at all and was characterized by reduced efficacy against Delta.
- Neutralization of SARS-CoV-2 Omicron variant by sera from BNT162b2 or Coronavac vaccine recipients. medRxiv, December 14, 2021. [PDF]
↓
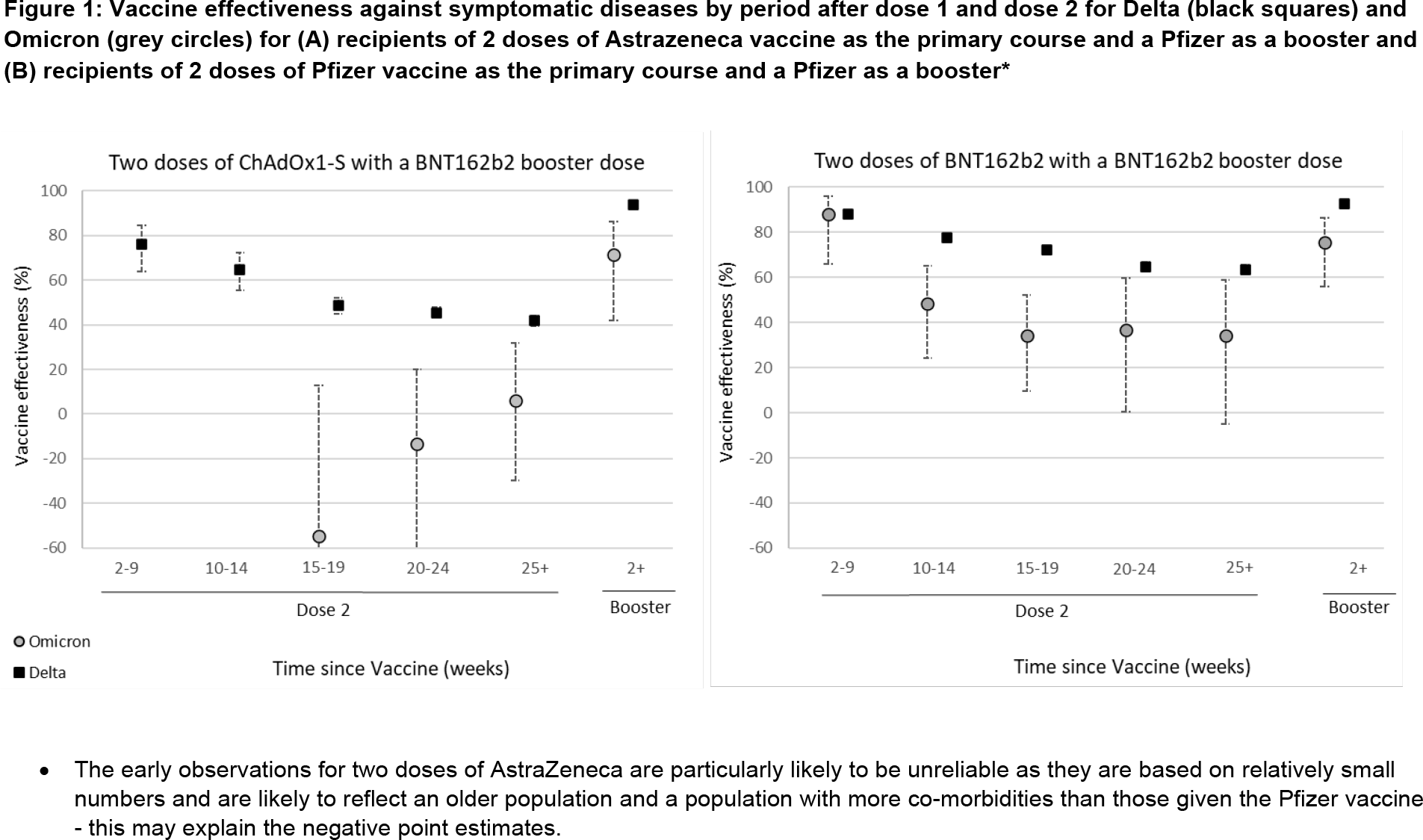
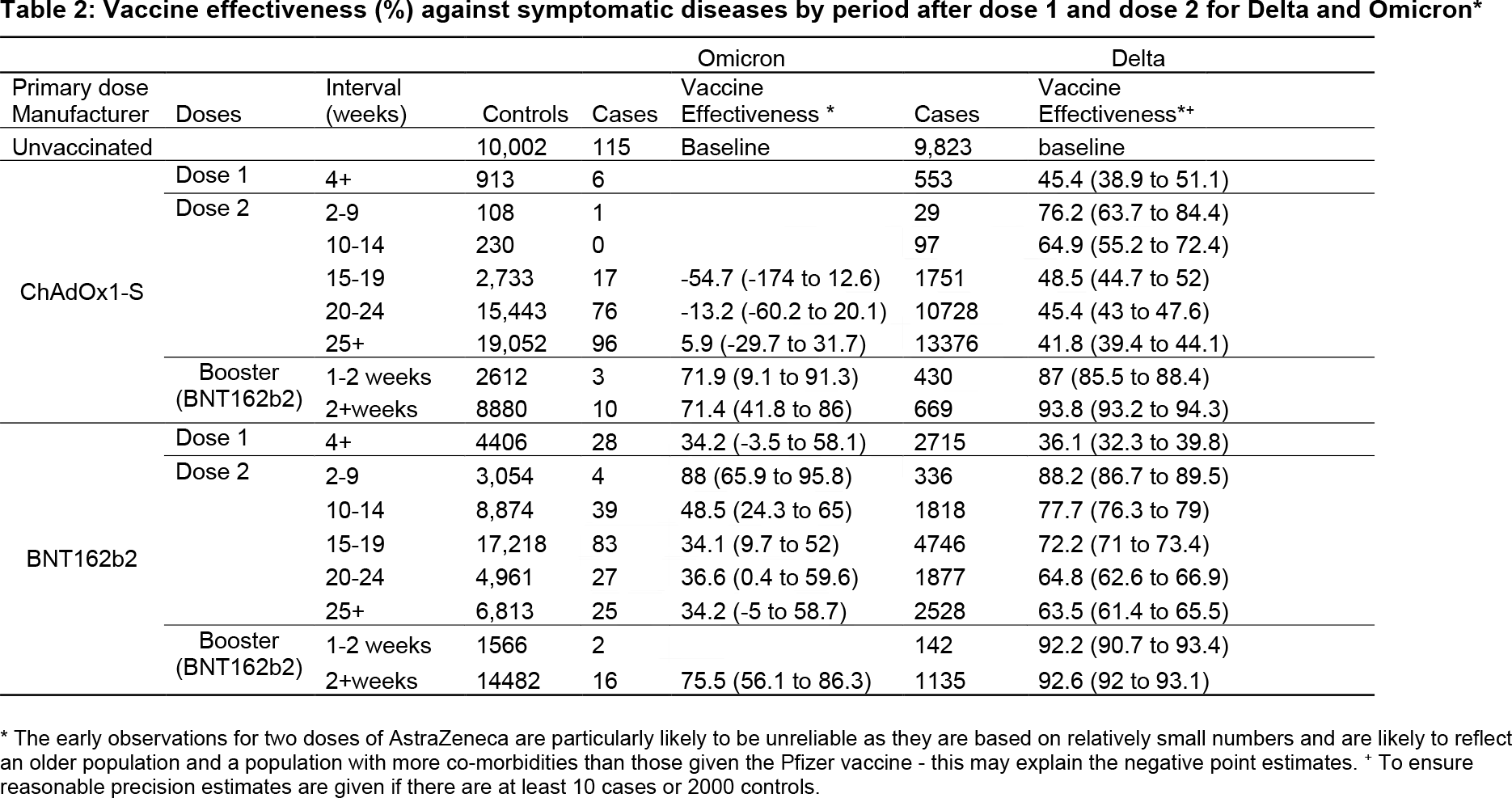
The National Health Security Agency (HSA) of the United Kingdom has conducted a more thorough analysis of vaccines for COVID-19 in terms of their protective effectiveness against the development of symptomatic COVID-19 infection caused by the Omicron (B.1.1.529) and Delta (B.1.617.2) variants strains of SARS-CoV-2 coronavirus.
Two vaccine products were studied: the mRNA vaccine Comirnaty (tozinameran; BNT162b2) by Pfizer and BioNTech and the viral vector vaccine Vaxzevria/Covishield (AZD1222, ChAdOx1 nCoV-19, ChAdOx1-S) by AstraZeneca. One group of people received the full course of two doses of Comirnaty, the second group received two doses of Vaxzevria/Covishield. Everyone then received a third (booster) dose of Comirnaty.
Two doses of Comirnaty were found to be significantly more effective in protecting against Omicron and Delta when compared to the two doses of Vaxzevria/Covishield. However, this is still not enough — the level of protection decreases seriously over time. The third dose of Comirnaty raises the level of protection dramatically. However, we don’t know yet how long it will last.
Thus, 25 weeks or more after receiving two doses of Comirnaty, the level of vaccine protection against Omicron was 34.2% (95% CI: −5.0 to 58.7), and against Delta was 63.5% (95% CI: 61.4 to 65.5). After two doses of Vaxzevria/Covishield, 5.9% (95% CI: −29.7 to 31.7) and 41.8% (95% CI: 39.4 to 44.1), respectively.
After receiving a booster dose of Comirnaty, effectiveness against Omicron and Delta after 2 weeks or more in the group initially vaccinated with Comirnaty increased to 75.5% (95% CI: 56.1 to 86.3) and 92.6% (95% CI: 92.0 to 93.1), respectively, whereas it increased to 71.4% (95% CI: 41.8-86.0) and 93.8% (95% CI: 93.2-94.3) in the group initially vaccinated with Vaxzevria/Covishield.
As we can see, even a third dose of the vaccine does not protect against Omicron at the same level as Delta. At any rate, this is true for protection against mild-to-moderate COVID-19 infection that does not require hospitalization. When it comes to protection against severe or critical COVID-19 leading to hospitalization or death, we would expect the third dose to raise its level even higher. This follows from the observations noted with previous variants of coronavirus. [1] [2]
- Effectiveness of COVID-19 vaccines against the Omicron (B.1.1.529) variant of concern. Preprint. [PDF]
December 13
Boris Johnson, the Prime Minister of Great Britain, has reported the death of a patient from the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. This is the first officially reported death worldwide due to Omicron.
Omicron is so transmissible that the number of cases of this variant doubles every two to three days. The strain is spreading phenomenally fast; it won’t be long before Omicron supplants Delta (B.1.617.2). Among those hospitalized with Omicron, most have received two doses of the vaccine.
Mr. Johnson is pushing for total vaccination with a third (booster) dose: it will be offered by the end of December, with the interval between the second and third doses to be shortened from six months to three.
↓
The Li Ka Shing Faculty of Medicine of the University of Hong Kong (HKUMed) has published new electron micrographs of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus that infected African green monkey kidney epithelial cells (Vero E6 line).
The image on the left (low magnification) shows cells 24 hours after Omicron infection, with a frame highlighting clusters of viral particles in the cytoplasm. The image in the middle (high magnification) shows an enlarged image of aggregates of viral particles in vesicles and on the cell surface. The image on the right (high magnification) frames large aggregates of viral particles with spikes in membrane-bound vesicles.

- A high-resolution image is available here.
↓
Researchers at the University of Oxford analyzed the level of antibody neutralization of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus in the sera of people vaccinated with two doses of vaccines — mRNA vaccine Comirnaty (tozinameran; BNT162b2) by Pfizer and BioNTech and viral vector vaccine Vaxzevria/Covishield (AZD1222, ChAdOx1 nCoV-19, ChAdOx1-S) by AstraZeneca.
In the case of Comirnaty, the neutralizing antibody titer decreased by a factor of 29.8 when compared with the level in the original non-mutant coronavirus, while in one person (n=1/21) it dropped to an undetectable level. In the case of Vaxzevria/Covishield, the titer fell below the detectable threshold in all but one person (n=1/22).
The results indicate that Omicron is much more antigenically distant from the original SARS-CoV-2 than its Beta (B.1.351) and Delta (B.1.617.2) strains. As a result, Omicron, which is spreading across the planet at an incredible speed, will lead to an increase in breakthrough COVID-19 infections in those already infected or twice vaccinated, which will inevitably be reflected in an increased burden on health care systems. It is possible that a third (booster) dose of vaccines could correct the gloomy picture to some extent.
If Omicron displaces Delta, becoming the world’s dominant variant of coronavirus, there will likely be a need to produce vaccines that take into account Omicron’s mutational specificity. However, such vaccines are unlikely to provide protection against previous strains due to the antigenic distancing of Omicron. Therefore, it is appropriate to consider switching from the current strategy of monovalent vaccines to multivalent vaccines for COVID-19, similar to those produced against seasonal influenza.
- Reduced neutralisation of SARS-COV-2 Omicron-B.1.1.529 variant by post-immunisation serum. medRxiv, December 11, 2021. [PDF]
December 12
China’ Brii Biosciences reported that the therapeutic combination of monoclonal antibodies amubarvimab (BRII-196) and romlusevimab (BRII-198) maintained activity against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. In in vitro neutralization tests, amubarvimab was shown to have significantly reduced activity against Omicron, whereas romlusevimab showed adequate activity against this strain. Taken together, the cocktail is effective against Omicron.
A cocktail of amubarvimab and romlusevimab is approved by the Chinese regulator on Dec. 9, 2021, to treat mild-to-moderate COVID-19 infection in patients at high risk of progression to severe disease, which includes hospitalization or death. The combination therapy, which was the first of this class of drugs in China, reduced the risks of these outcomes by 80%.
The U.S. Food and Drug Administration (FDA) is currently reviewing Brii’s application for amubarvimab/romlusevimab.
↓
A study conducted by the Li Ka Shing Faculty of Medicine of the University of Hong Kong (HKUMed) and the Chinese University of Hong Kong (CUHK) found that the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus significantly reduced the ability of Comirnaty (tozinameran; BNT162b2), mRNA vaccine for COVID-19 by Pfizer and BioNTech, to neutralize the virus — by a factor of 32 or more when compared to the original non-mutated coronavirus.
The image clearly shows that Omicron escapes the neutralizing effect of inoculated serum.

The results of a test of CoronaVac, inactivated whole-virion vaccine for COVID-19 by China’s Sinovac Biotech, will be available soon.
It should be understood that we are talking about indirect tests when in vitro study the neutralizing activity of blood sera of vaccinated people. There is no direct data (in clinical trials or real-world practice) on how effective the existing vaccines against Omicron are yet.
According to experts, vaccines are probably still effective in the task of protecting against severe COVID-19 and death. The research team encourages people in high-risk groups (the elderly, immunocompromised, or chronically ill) to get a booster (extra) dose of the vaccine as soon as possible.
December 11
According to researchers at Chaim Sheba Medical Center at Tel HaShomer (Israel), the neutralizing activity of even three doses of Comirnaty (tozinameran; BNT162b2), mRNA vaccine for COVID-19 by Pfizer and BioNTech, is four times lower against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus than against the Delta variant (B.1.617.2), and eight times lower than against the original non-mutant coronavirus.
The neutralizing activity of two doses of Comirnaty was not able to handle Omicron at all, although it did work against Delta.
The Israeli Ministry of Health is considering shortening the time until a third (booster) dose of the vaccine is administered — three months after the second dose. This will still not be enough to fully combat Omicron but the neutralizing activity will increase by a factor of about a hundred, which is encouraging.
- Third BNT162b2 vaccination neutralization of SARS-CoV-2 Omicron infection. medRxiv, December 14, 2021. [PDF]

December 10
The World Health Organization (WHO) has made several assumptions about the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus, based, however, on as yet very limited data on it.
First, Omicron is characterized by a faster spread than Delta (B.1.617.2), regardless of how widely the latter variant is represented in the population. It is unknown whether this is due to the ability of Omicron to evade the immune system or its inherent increased contagiousness.
Second, Omicron-induced COVID-19 infection is probably less severe than Delta-induced one; all reported cases were mild or asymptomatic.
Third, in view of the lack of reliable and peer-reviewed evidence, it cannot be unequivocally stated that the protective efficacy of vaccines will decrease in the case of Omicron. Although the significantly altered antigenic profile of the Omicron’s S protein indicates a potential decrease in vaccine efficacy. This is indirectly confirmed by the increased frequency of reinfection in South Africa, as well as by in vitro data indicating a fall in the neutralizing activity of sera obtained from vaccinated and previously infected individuals.
Fourth, Omicron does not affect the diagnostic accuracy of PCR and antigen-based rapid diagnostic test (Ag-RDT). However, some PCR tests targeting the S protein gene may give false-negative results because of mutations in this gene.
Fifth, the therapeutic interventions for the management of patients with severe or critical COVID-19 are expected to remain unchanged. Except that monoclonal antibodies should be tested separately for their antigen binding and ability to neutralize Omicron.
- Enhancing readiness for Omicron (B.1.1.529): technical brief and priority actions for member states. WHO. December 10, 2021. [PDF]
↓
The National Health Security Agency (HSA) of the United Kingdom has stated that two doses of Comirnaty (tozinameran; BNT162b2), mRNA vaccine for COVID-19 by Pfizer and BioNTech, or Vaxzevria/Covishield (AZD1222, ChAdOx1 nCoV-19, ChAdOx1-S), viral vector vaccine for COVID-19 by AstraZeneca, are not sufficient to provide reliable protection against the development of symptomatic COVID-19 infection caused by the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus as well as its Delta variant (B.1.617.2).
Thus, two doses of Comirnaty granted protection against Delta and Omicron at 60% and 40%, respectively, while Vaxzevria/Covishield gave protection at 40% and 10%. After the third (booster) dose of Comirnaty, the protective efficacy against Omicron increases to 76% among those who have already received two doses of Comirnaty, and to 71% among those initially vaccinated with Vaxzevria/Covishield. Vaccine efficacy against Delta rises to 90% in all cases.
The Omicron variant tends to spread around the Earth very quickly because it is three times more transmissible (contagious) than the Delta variant through close contact, and people who were previously infected with COVID-19 and recovered are twice as likely to reinfect with Omicron as they are with Delta.
- SARS-CoV-2 variants of concern and variants under investigation in England. Technical briefing 31. December 10, 2021. HSA. [PDF]
↓
The U.S. Centers for Disease Control and Prevention (CDC) has released a surveillance report describing 43 cases of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus in 22 states during the first week of December 2021. No deaths or hospitalizations were reported. The majority of cases were in young adults aged 18–39 (58%). Among those who got Omicron, fully vaccinated accounted for 47%, and fully vaccinated people with an additional (booster) dose of the vaccine accounted for another 33%. Thus, 80% of fully vaccinated people became ill with Omicron compared with 19% of unvaccinated people.
December 9
The State Research Center of Virology and Biotechnology VECTOR (Russia) is not going to modify its EpiVacCorona, peptide-based vaccine for COVID-19, to fit the mutational features of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus, since it is claimed to retain its effectiveness against the new strain. However, appropriate evaluation of EpiVacCorona against Omicron has already begun.
↓
According to a study by Hiroshi Nishiura, a scientist from Kyoto University advising the Japanese Ministry of Health, the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus is 4.2 times (95% CI: 2.1–9.1) more transmissible (contagious) in the early stage of COVID-19 infection than the Delta variant (B.1.617.2). Understand, however, that this does not mean that Omicron is more dangerous than Delta.
Nishiura, who specializes in mathematical modeling of infectious diseases, has previously analyzed the Delta variant in the run-up to the Tokyo 2020 Summer Olympics.
- The research. [PDF]
December 8
The Li Ka Shing Faculty of Medicine of the University of Hong Kong (HKUMed) has published electron micrographs of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus that infected African green monkey kidney epithelial cells (Vero E6 line).
The image on the left (low magnification) shows damaged cells with swollen vesicles containing small black virus particles. The image on the right (high magnification) shows clusters of viral particles with crown-shaped spikes on their surface (red frame).

- A high-resolution image is available here.
↓
AstraZeneca has offered Evusheld (tixagevimab + cilgavimab), a cocktail of two monoclonal antibodies, a single injection of which protects against COVID-19 for at least six months. Evusheld is being extensively studied in its ability to protect against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus.
Evusheld: First Drug for Strong and Long-Lasting Protection Against Coronavirus
One dose of AstraZeneca’s monoclonal antibody cocktail protects against COVID-19 for six months or longer.
↓
Pfizer and BioNTech reported that serum antibodies induced by Comirnaty (tozinameran; BNT162b2), mRNA vaccine for COVID-19, neutralized the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus after three doses of the vaccine.
Laboratory studies showed that sera of inoculated individuals taken one month after receiving the third (booster) dose of the Comirnaty vaccine neutralized Omicron to levels comparable to those of the initial non-mutant SARS-CoV-2 after receiving two doses of the vaccine. Without the booster, the level of neutralizing antibodies against Omicron was 25 times lower.
According to Pfizer and BioNTech, a third dose of Comirnaty vaccine is mandatory for reliable protection against Omicron.
At the same time, the partners are developing a version of Comirnaty modified for the mutational features of Omicron. The first batches of the updated vaccine will be ready by March 2022.
- BioNTech. Omicron variant (B.1.1.529). December 8, 2021. [PDF]
December 7
Xevudy (sotrovimab), a monoclonal body developed by GlaxoSmithKline and Vir Biotechnology, has confirmed neutralizing activity against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. At any rate, this follows from its in vitro testing.
Xevudi is used to treat mild-to-moderate COVID-19 in patients at high risk of progression to severe disease, which can lead to hospitalization or death.
- The dual function monoclonal antibodies VIR-7831 and VIR-7832 demonstrate potent in vitro and in vivo activity against SARS-CoV-2. biorxiv, December 07, 2021. [PDF]
- Omicron Conference Call Presentation. Vir Biotechnology, December 7, 2021. [PDF]
Sotrovimab Is Effective Against Omicron Variant of Coronavirus
A monoclonal antibody developed by GlaxoSmithKline and Vir Biotechnology successfully counteracts a new strain of SARS-CoV-2.
↓
Comirnaty (tozinameran; BNT162b2), mRNA vaccine for COVID-19 by Pfizer and BioNTech, provides significantly reduced immunity to the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus but a third (booster) dose may still help.
This follows the results of laboratory tests conducted at the Africa Health Research Institute (AHRI) in Durban (South Africa), which found that the level of neutralizing antibodies against Omicron produced by the vaccine was 41 times lower than that of the original non-mutant coronavirus.
According to experts, under conditions of the Omicron variant, the protection against COVID-19 infection conferred by Comirnaty vaccine would be seriously reduced — its effectiveness would fall to 22.5% (95% CI: 8.5–40.7), but it would remain in terms of preventing the development of severe disease since in this case high levels of neutralizing antibodies are not required due to the postvaccinal T-cell immunity formed.
- SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer BNT162b2 elicited neutralization and requires ACE2 for infection. medRxiv, December 11, 2021. [PDF]
November 2021
November 30
Inovio Pharmaceuticals has shared plans to develop DNA vaccines that address the mutational features of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. These are INO-4800, DNA vaccine for COVID-19, which is still in two phase III clinical trials, and the DNA vaccine candidate INO-4802, which potentially retains efficacy regardless of existing and upcoming coronavirus variants. In the Omicron challenge, the neutralizing activity of serum samples from patients vaccinated with INO-4800 and preclinical samples from animal models tested with INO-4802 will be evaluated.
November 29
China’s Sinovac Biotech could not avoid joining the vaccine race in the fight against omicron. Its CoronaVac, inactivated whole-virion vaccine for COVID-19, is considered the most widely used in the world, with an estimated 943 million doses produced by mid-2021, and more than 2.91 billion doses on offer by year’s end, according to Airfinity. Sinovac is ready to set up production of CoronaVac, optimized for mutation combinations of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus, in three months, but only if needed.
Previously, Sinovac developed versions of CoronaVac that take into account specific features of Gamma (P.1) and Delta (B.1.617.2) variants but did not put them into mass production since the original vaccine copes well with them.
↓
Adagio Therapeutics has notified that the monoclonal antibody ADG20 it is developing against SARS-CoV-2 coronavirus will retain adequate neutralizing activity against its Omicron variant (B.1.1.529). This is possible because ADG20 is targeted to the highly conserved and mutation-avoiding epitope of receptor-binding domain (RBD) of S protein.
If all goes well, ADG20 will go commercial in the second half of 2022. Adagio hopes that a single intramuscular injection of ADG20 will be enough to reliably and long-lasting (at least 6 months) prevent the development of symptomatic COVID-19 infection and to treat it if it does occur.
ADG20: Cure for All Mutant Variants of SARS-CoV-2
Adagio Therapeutics’ monoclonal antibody will help fight all strains of the coronavirus.
↓
Janssen, part of Johnson & Johnson, company behind the development of the Ad26.COV2.S, viral vector vaccine for COVID-19, has begun testing it against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. This involves testing serum from participants in completed and ongoing clinical trials to determine the neutralizing activity of Ad26.COV2.S against Omicron. At the same time, an updated version of the vaccine specific to the Omicron mutational fatures is being developed.
↓
The Gamaleya Research Institute of Epidemiology and Microbiology (Russia) announced that it has begun development of Sputnik V (Gam-COVID-Vac), viral vector vaccine for COVID-19, modified for the mutation features of the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. Its readiness for large-scale production is expected within 45 days. Sputnik Light, single-component viral vector vaccine for COVID-19, is claimed to retain adequate efficacy against omicron.
November 27
Pfizer and BioNTech are ready to offer an updated Comirnaty (tozinameran; BNT162b2), mRNA vaccine for COVID-19, modified to the mutational specificity of Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. It will take approximately 100 days to release the novelty. This is true if the current version of Comirnati proves not to be very effective against Omicron.
November 26
Novavax is testing whether its Covovax/Nuvaxovid (NVX-CoV2373), a recombinant nanoparticle vaccine for COVID-19, is suitable for reliable protection against the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus. Novavax will evaluate both Covovax/Nuvaxovid, already approved in Indonesia and the Philippines, and will begin development of a mutation-specific Omicron vaccine. A proper vaccine could be available in January 2022.

Covovax/Nuvaxovid: Nanoparticle Vaccine for COVID-19
Covovax/Nuvaxovid by Novavax is a protein subunit vaccine from virus-like particles.
↓
Moderna has unveiled a strategy to counteract the Omicron variant (B.1.1.529) of SARS-CoV-2 coronavirus, intending to implement it in three vectors at once.
First, the original Spikevax (elasomeran; mRNA-1273), mRNA vaccine for COVID-19, will be tested in a doubled booster dose (100 µg). Second, two multivalent vaccine booster candidates are being clinically tested: mRNA-1273.211 includes several Omicron mutations that are also present in SARS-CoV-2 Beta variant (B.1.351), and the experimental booster mRNA-1273.213 contains several Omicron mutations that are present in the Delta variant (B.1.617.2). Third, the vaccine booster candidate mRNA-1273.529, which is fully engineered for Omicron specificity, is under study.
An Omicron mutation-matched mRNA vaccine by Moderna could be available in early 2022.
Omicron Variant: Only Facts
Background
The Omicron variant (B.1.1.529 lineage) is a new strain of SARS-CoV-2 coronavirus that was reported to the world on November 24, 2021. The first cases of Omicron began to be documented on November 9. [1] [2] [3] [4]
On November 26, the World Health Organization (WHO) listed Omicron as a variant of concern. [5]
- This list includes SARS-CoV-2 strains that pose a potential risk to humanity because of criteria such as increased transmissibility, morbidity or mortality, ability to evade existing vaccines or antiviral drugs, bypass natural immunity (risk of reinfection) or infect vaccinated individuals, etc.
The Omicron variant, which is thought to be native to the Republic of South Africa (RSA), is spreading rapidly across the planet. It contains over 30 mutations in the S protein of SARS-CoV-2, including mutations found in other strains that are associated with increased transmissibility (contagiousness) of the coronavirus and decreased susceptibility to neutralizing antibodies, including therapeutic monoclonal antibodies.
As of December 20, 2021, the number of confirmed cases of Omicron, was 79,346. [6]
According to European Centre for Disease Prevention and Control (ECDC) estimates as of December 2, 2021, the Omicron variant could become the dominant strain of coronavirus in Europe by March 2022. [7] This is due to the fact that Omicron is three times more contagious than the Delta variant through close contacts, and people who have previously been infected with SARS-CoV-2 and recovered are twice as likely to reinfect with Omicron rather than Delta. [8] In addition, Omicron replicates 70 times faster in the bronchi than Delta and non-mutant original SARS-COV-2, which dramatically increases its infectivity. [9]
- Implications of the further emergence and spread of the SARS-CoV-2 B.1.1.529 variant of concern (Omicron) for the EU/EEA – first update. ECDC. December 2, 2021. [PDF]
- SARS-CoV-2 variants of concern and variants under investigation in England. Technical briefing 31. December 10, 2021. HSA. [PDF]
Genetics Features
The genome of SARS-CoV-2 Omicron variant contains a total of 60 mutations compared with the original virus from Wuhan: 50 nonsynonymous mutations, 8 synonymous mutations, and 2 noncoding mutations.
34 mutations affect S protein (30 amino acid substitutions, 3 small deletions, 1 small insertion), the main antigenic target of antibodies produced by infections and most vaccines. Many of these mutations have not been observed in other strains. Notably, 15 of the 30 amino acid substitutions are in receptor-binding domain (RBD).
- The key amino acid substitutions in S protein (substitutions in RBD are highlighted in bold) are as follows: A67V, del69-70, T95I, del142-144, Y145D, del211, L212I, ins214EPE, G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493R, G496S, Q498R, N501Y, Y505H, T547K, D614G, H655Y, N679K, P681H, N764K, D796Y, N856K, Q954H, N969K, L981F
Several assumptions can be made about the degree of transmissibility (contagiousness) based on omicron mutations. [1] For example, N501Y enhances binding to angiotensin-converting enzyme 2 (ACE2) receptor, which may increase transmissibility, and the combination of N501Y and Q498R further increases binding affinity. However, other substitutions in S protein are thought to reduce binding to ACE2. Thus, affinity binding to ACE2 receptor must be evaluated using the full range of substitutions in Omicron’s S protein.
H655Y and N679K are closer to the furin cleavage site, which is characterized by its polybasic nature, which can enhance S protein cleavage, thereby increasing transmissibility.
P681H enhances S protein cleavage, increasing transmissibility. This mutation occurs in the Alpha variant, while an alternative mutation (P681R) is present in the Delta variant.
Clinical Features
The clinical implications of the combination of mutations in Omicron are not yet precisely clear. According to a limited data set, Omicron, being more contagious, is able to evade humoral immunity formed after a coronavirus infection or induced by a vaccine, and is characterized by an increased risk of reinfection in individuals previously infected with other variants of coronavirus.
Thus, in an unpublished study evaluating national surveillance data in South Africa, the ratio of reinfection (repeat positive test at least 90 days after a previous positive test) to primary infections was higher at the beginning of the disease wave associated with the Omicron variant compared with outbreaks associated with Beta (B.1.351) and Delta (B.1.617.2) variants: 0.25 — versus 0.12 and 0.09. [1]
And while these data suggest that the risk of reinfection may be higher with Omicron, they do not account for the possibility that changes in testing regimens or variable risks of infection may contribute to the differences observed.
The risk of severe illness with Omicron infection may be lower than with infection with other SARS-CoV-2 variants.
An unofficial report from the South African hospital at the center of the outbreak showed that only 33% of 42 patients with COVID-19 required supplemental oxygen (down from the start of previous outbreaks), while 8 of 9 people with COVID-19 pneumonia were unvaccinated. However, it is decidedly premature to draw unqualified conclusions based on these small and early reports. [2]
According to a large-scale analysis of 211,000 Omicron cases in South Africa, its clinical features include a shortened incubation period of three to four days and a mostly mild disease with recovery within three days. [3]
Cases from other countries also show a mild or asymptomatic course of COVID-19 caused by Omicron. [4] [5]
The relatively mild course of the disease may reflect the younger age of those affected at this stage of the Omicron outbreak (or the higher rate of reinfections), and because there is often a delay between the onset of symptoms and the development of respiratory complications, the severity of Omicron’s clinical manifestations may not be evident for several weeks.
Symptoms and Signs
Most of the symptoms of Omicron are the same as those of the common cold. Symptoms and signs of Omicron include the following: runny nose, headache, fatigue, sneezing, scratchy or sore throat, and muscle pain (especially low back pain). [1] [2]
COVID-19 caused by Omicron is significantly less often characterized by classic symptoms such as fever, dry cough, and loss of smell, which have been clearly seen in other variants of the coronavirus.
Diagnostic
One of the mutations in the Omicron variant is a deletion in the S protein, resulting in the inability of some molecular tests for SARS-CoV-2 to detect the corresponding gene encoding the S protein. However, these tests will still be able to detect viral RNA because they use more than one target gene and thus will not lead to false negatives. [1] Although there are still a couple or three tests that fail the Omicron diagnostic. [2]
Such a change in the S protein gene can be used as a marker for detecting Omicron but with the caveat that this change can also occur in other variants, such as Alpha.
Antigen testing, which relies primarily on the detection of its nucleocapsid protein, will not be affected by Omicron.
Treatment Effectiveness
Monoclonal antibodies, which are widely available on the market, are unlikely to help in the treatment or prevention of COVID-19 caused by the Omicron variant of SARS-CoV-2. In any case, their in vitro neutralizing activity drops sharply in the presence of Omicron. [1] [2] [3] [4] [5]
There are, however, several monoclonal antibodies that have confirmed their ability to fight Omicron — at least their neutralizing activity has not decreased so much as to speak of a loss of effectiveness. Among these are the following:
- The monoclonal antibody sotrovimab (VIR-7831, GSK4182136), developed by GlaxoSmithKline and Vir Biotechnology and known by the brand name Xevudy.
- Going by the name Evusheld (AZD7442) is a combination of tixagevimab (AZD8895) and cilgavimab (AZD1061) monoclonal antibodies by AstraZeneca.
- The monoclonal antibody romlusevimab (BRII-198) from China’s Brii Biosciences. It is approved for use together with amubarvimab (BRII-196), but the latter failed to handle Omicron.
Vaccine Effectiveness
The effect of mutations in the Omicron variant on the effectiveness of COVID-19 vaccines is still unclear. Several preliminary unpublished and non-peer-reviewed reports suggest the following. First, in vitro neutralizing activity of sera of vaccinated individuals is 20–40 times lower against Omicron than against the original nonmutant wild-type virus. Second, previously infected vaccinated individuals and individuals who received a booster (third) dose of the vaccine retain adequate neutralizing titers against Omicron. Third, vaccine effectiveness may be reduced, particularly in the task of preventing infection, but not for preventing the development of severe COVID-19 or death. [1] [2] [3] [4]
- Reduced neutralization of SARS-CoV-2 Omicron variant by vaccine sera and monoclonal antibodies. medRxiv, December 11, 2021. [PDF]
- Quantification of the neutralization resistance of the Omicron Variant of Concern. Preprint. [PDF]
- SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer BNT162b2 elicited neutralization and requires ACE2 for infection. medRxiv, December 11, 2021. [PDF]
- BioNTech. Omicron variant (B.1.1.529). December 8, 2021. [PDF]
In any case, the clinical implications of the above findings for vaccines are unknown; particularly because the neutralizing activity may not be the only line of immune defense, as there is also cell-mediated immunity that provides cross-defense against different variants of SARS-CoV-2. [5]
- mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science. 2021 Dec 3;374(6572):abm0829. [PDF]
That said, preliminary data must be confirmed by large-scale studies involving sera from people with different immunological profiles (e.g., who received different vaccine brands or additional vaccine doses, and who had infections of varying severity) as well as sera collected at different times after infection and/or vaccination.
According to a large-scale analysis of 211,000 cases of Omicron in South Africa, two doses of mRNA vaccine Comirnaty (tozinameran; BNT162b2) by Pfizer and BioNTech provided 70% protection (compared with unvaccinated people) against Omicron-induced COVID-19 infection in a severe or critical form requiring hospitalization, and 33% against the development of symptomatic disease. In comparison, against the Delta variant, Comirnaty protected better, at 93% and 80%, respectively. [6]