Highlights
Paxlovid (nirmatrelvir + ritonavir) is a drug indicated for the treatment of mild-to-moderate COVID-19 infection.
Paxlovid, developed by Pfizer, is one of the most effective drugs for COVID-19 in the world.
Paxlovid successfully treats COVID-19 caused by the Omicron variant of the SARS-CoV-2 coronavirus that now dominates the entire planet.
Paxlovid is taken orally for five days.
Paxlovid, which debuted in the United States in late December 2021, is used to treat mild-to-moderate COVID-19 infection (confirmed by SARS-CoV-2 testing) in adults and children (12 years and older weighing at least 40 kg) who are at high risk for progression to severe disease, including hospitalization or death.

Paxlovid Approved in the U.S.
Pfizer’s oral antiviral drug has entered the world’s main pharmaceutical market.
The European Union, which issued marketing authorization for Paxlovid in late January 2022, approved its use to treat COVID-19 infection in adults who do not require supplemental oxygen and who are at increased risk of progression to severe disease.
The World Health Organization’s (WHO) position on the use of Paxlovid, issued in late April 2022, is as follows: The drug should be used to treat patients with non-serious COVID-19 infection and a high risk of hospitalization.
Risk of Severe COVID-19
There is a category of vulnerable patients whose COVID-19 infection is characterized by an increased risk of severe outcomes, such as hospitalization, admission to the intensive care unit (ICU), need for intubation or mechanical ventilation, and death.
High-risk patients worldwide are estimated to number approximately half of the total population.
High-risk COVID-19 patients should include people who meet at least one criterion:
- Age 50 and older
- Unvaccinated, under-vaccinated, or overdue booster doses of vaccine
- Racial or ethnic minority
- A history of a certain disease (condition):
- Obesity (body mass index [BMI] ≥30 kg/m2)
- Type 1 diabetes mellitus, type 2 diabetes mellitus
- Kidney diseases: chronic kidney disease (CKD)
- Lung diseases: cystic fibrosis, interstitial lung disease, pulmonary embolism, pulmonary hypertension, bronchiectasis, chronic obstructive pulmonary disease (COPD)
- Cardiovascular diseases: heart failure, coronary heart disease, cardiomyopathies
- Cerebrovascular diseases
- Cancer
- Liver diseases: cirrhosis, non-alcoholic fatty liver disease (NAFLD), alcoholic liver disease, autoimmune hepatitis
- Mental health disorders: mood disorders (including depression), schizophrenia spectrum disorders
- Disabilities: attention deficit hyperactivity disorder (ADHD), cerebral palsy, congenital malformations, limitations with self-care or activities of daily living, intellectual and developmental disabilities, learning disabilities, spinal cord injuries
- Other diseases: asthma, HIV, tuberculosis, primary immunodeficiencies, dementia
- Other conditions: pregnancy (including recent pregnancy), physical inactivity, smoking (current or past), solid organ or hematopoietic cell transplantation, use of corticosteroids or other immunosuppressive medications.
People who are overweight (BMI between 25 and 29 kg/m2), have hypertension, hepatitis B, hepatitis C, sickle cell disease, thalassemia, alpha-1 antitrypsin deficiency, bronchopulmonary dysplasia, or substance use disorder are also at increased risk for severe COVID-19.
Features of Paxlovid usage
Paxlovid is not used to treat patients in the standard risk group.
Paxlovid is not indicated to treat patients requiring hospitalization due to severe or critical COVID-19.
Paxlovid is not used for pre-exposure or post-exposure prophylaxis of COVID-19.
Paxlovid should be administered as soon as possible after the diagnosis of COVID-19 and within a maximum of 5 days after manifestation of disease symptoms. If time is missed, the drug is unlikely to help.
Paxlovid, which is available as a set of nirmatrelvir and ritonavir tablets, is taken orally every 12 hours (two 150-mg nirmatrelvir tablets and one 100-mg ritonavir tablet), for 5 days and no longer than that.
For moderate renal insufficiency (estimated glomerular filtration rate [eGFR] in the range of 30–60 ml/min/1.73 m2), the dose of nirmatrelvir should be halved.
Paxlovid is not recommended in severe renal insufficiency (eGFR < 30 mL/min/1.73 m2) or severe hepatic impairment (Child–Pugh class C).
Due to the presence of ritonavir in Paxlovid, its drug interactions with other drugs should always be taken into account, since the consequences can be serious. For an appropriate list of “problematic” drugs that are contraindicated or should be prescribed with caution, see the instructions for medical use of Paxlovid, a special checklist, or a third-party list that provides alternative substitutions for drugs with undesirable interactions.
“Paxlovid Mouth”
Unpleasant taste in the mouth is one of the common side effects that occur during treatment of COVID-19 infection with Paxlovid. Some people experience only slight changes in their taste sensation, while others experience very pronounced dysgeusia (taste disorder). This nauseating effect, dubbed “Paxlovid mouth,” is described by Reddit users in vivid terms: sun-heated slop from garbage bags, dirty coins from the bottom of ashtrays, addled soy milk, rotten grapefruit with soap, rancid vomit, acetone, bleach, glue from hundreds of envelopes, stale black pepper, old dusty aspirin, Malört liqueur…
One Redditor didn’t skimp on the following description of a “Paxlovid mouth”: as if a grapefruit ate a diaper it found on the beach and then crawled into the mouth to die; a graveyard on fire; a pile of iron filings after a nuclear disaster; 16 bottom fish that died ten years ago and were resurrected by an inexperienced necromancer obsessed with excrement.
Sometimes a “Paxlovid mouth” turns away from eating food altogether, as it tastes like garbage.
Dysgeusia is caused by the combination of nirmatrelvir and ritonavir in Paxlovid. Nirmatrelvir, being the main active ingredient, is itself bitter, while ritonavir, which acts as a booster (enhancer) of nirmatrelvir, preventing it from being metabolized prematurely by the body, actually preserves this bitterness. Nirmatrelvir and ritonavir can be excreted with saliva, causing it to reenter the mouth. The process of chemesthesia may be triggered when another sensation is confused with taste: for example, the sharpness of jalapeño peppers is not a taste, but a physical pain on the tongue caused by capsaicin.
Those who are not able to endure the problem with nauseating taste sensations on their own during the 5-day treatment with Paxlovid, because it can be so serious that it interferes with sleep, should try to mask the horrible taste in the mouth with mints, lollipops or candies, cough drops, cinnamon gum. If they do not help, no one forbids experimenting with interrupting the “Paxlovid mouth” with other pronounced flavors like candies with sourness, lemon, salty snacks, orange ice cream, chocolate or almond milk, strawberry and banana smoothies, candied ginger, cranberry juice, hot sauce, energy drink, etc.
One of the techniques of cognitive behavioral therapy (CBT) will be helpful. Reframing negative thinking associated with a bad taste in the mouth involves evaluating the situation in a positive way: The unpleasant effects are a consequence of the fact that Paxlovid is successfully working, keeping you from going to the hospital and dying there.
Even if relief comes, it will be only temporary, the unbearable taste is sure to return.

Paxlovid: Efficacy and Safety of COVID-19 Treatment
Main Study
The EPIC-HR (NCT04960202) phase 2/3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial enrolled unvaccinated adult patients with laboratory-confirmed COVID-19.
Among the main criteria for participation: manifestation of COVID-19 symptoms no later than 5 days before randomization; course of COVID-19 with mild-to-moderate severity and not requiring hospitalization; at least one risk factor for severe COVID-19.
Risk factors included the following: age 60 or older, overweight, smoker status, chronic kidney disease (CKD), diabetes mellitus type 1 or 2, immunosuppressive disease, chronic lung disease, cancer (except skin cancer) in an active stage.
Subjects were given placebo or Paxlovid — orally every 12 hours for 5 days.
The primary endpoint was the proportion of patients who required hospitalization or who died of any cause at 28 days of follow-up from the start of treatment.
Interim Results
According to a planned interim analysis of data from patients (1219 of the 3000 to be included in the study) treated within the first 3 days of COVID-19 symptoms, 0.8% of patients (n=3/389; no deaths) were hospitalized in the Paxlovid group — versus 7.0% of patients (n=27/385; 7 deaths) in the placebo group.
Thus, administration of Paxlovid in the early stages of COVID-19 infection reduced the risk of hospitalization or death by 89% compared with placebo: risk ratio (RR) 0.11 (95% CI: 0.03–0.36; p<0.0001). The risk of death decreased by a relative 93%: RR 0.07 (95% CI: 0.00–1.16).
In patients who started treatment within the first 5 days of COVID-19 symptoms, 1.0% (n=6/607, no deaths) and 6.7% (n=41/612; 10 deaths) of the Paxlovid and placebo groups, respectively, experienced hospitalization.
In other words, later use of Paxloid reduced the risk of hospitalization or death by a relative 85%: RR 0.15 (95% CI: 0.06–0.34; p<0.0001). Reduced risk of death came out to 95%: RR 0.05 (95% CI: 0.00–0.81).
The frequencies of treatment-emergent adverse events (TEAEs) were comparable in Paxlovid and placebo groups: 19% and 21% of subjects, respectively, experienced them, most TEAEs were mild. Serious TEAEs were recorded in 1.7% and 6.6% of participants, and 2.1% and 4.1% discontinued treatment because of TEAEs.
Final Results
According to a final analysis of patients (n=2246), administration of Paxlovid within 3 days after manifestation of COVID-19 symptoms resulted in an 89% reduction in the risk of hospitalization or death compared with placebo (p<0.0001). The risk of hospitalization was reduced by 89% (risk ratio [RR] 0.11 [95% CI: 0.04–0.28]) and the risk of death by 95% (RR 0.05 [95% CI: 0.00–0.90]).
- In the Paxlovid group, 0.7% of patients were hospitalized (n=5/697; no deaths) — versus 6.5% of patients in the placebo group (n=44/682; 9 deaths).
Administration of Paxlovid for 5 days after COVID-19 symptoms manifested reduced the risk of hospitalization or death by 88% relative to placebo (p<0.0001). The risk of hospitalization was reduced by 88% (RR 0.12 [95% CI: 0.06–0.25]) and the risk of death by 96% (RR 0.04 [95% CI: 0.00–0.68]).
- In the Paxlovid group, 0.8% of patients were hospitalized (n=8/1039; no deaths) — vs. 6.3% of patients in the placebo group (n=66/1046; 12 deaths).
In a subgroup of elderly patients (65 years and older), a population particularly at high risk of hospitalization or death, Paxlovid reduced these risks by a relative 94% over the 28-day follow-up period (p<0.0001).
- In the Paxlovid group, 1.1% of patients were hospitalized (n=1/94; no deaths) — vs. 16.3% of patients in the placebo group (n=16/98; 6 deaths).
Paxlovid was slightly less effective among patients younger than 65 years of age, the risk of hospitalization or death was reduced by 85%.
In the entire population of subjects followed up for 28 days, no deaths were reported among those receiving Paxlovid — vs. 12 deaths (1.2%) in the placebo group.
Paxlovid, which was started within 3 or 5 days of the onset of COVID-19 symptoms, provided a 7-fold (by 0.868 log10 viral copies/mL) and 5-fold (by 0.695 log10 viral copies/mL) reduction in viral load relative to placebo, from baseline to assessed at day 5 of treatment, thereby attesting to its powerful activity against the SARS-CoV-2.
The frequencies of treatment-emergent adverse events (TEAEs), which were mostly mild-to-moderate in severity, were almost identical, with 23% of patients in the Paxlovid group — vs. 24% in the placebo group. Administration of Paxlovid resulted in fewer serious TEAEs (1.6% of subjects) and discontinuation of treatment (2.1%) — vs. the placebo group (6.6% and 4.2%, respectively).
Paxlovid Against Omicron
The main clinical validation of Paxlovid was performed at a time when the Delta variant (B.1.617.2) of the SARS-CoV-2 coronavirus dominated. Due to the fact that the Omicron variant now dominates, it is necessary to find out how well this antiviral drug copes with it.
U.S.
The administration of Paxlovid between early January and mid-May 2022 to U.S. patients (n=6036) aged 50 years and older (mean age 62 years) in real-world Omicron (subvariants BA.1.1, BA.2 and BA.2.12.1) dominant conditions was found to reduce the risk of hospitalization within 14 days of manifestation of COVID-19 symptoms by 45%: risk ratio (RR) 0.55 (95% CI: 0.38–0.80; p=0.002).
Those who benefited most from Paxlovid administration were, first, those who were not fully vaccinated (84% risk reduction; p=0.052) and, second, those who were obese (79% risk reduction; p=0.007).
Although the efficacy of Paxlovid against Omicron was halved when compared to the therapeutic strength against Delta demonstrated in the EPIC-HR (NCT04960202) phase 2/3 clinical trial, no deaths were reported in the 28-day period among those receiving nirmatrelvir with ritonavir.
It should not be assumed that nirmatrelivir seems to have lost its antiviral activity against Omicron. The decrease in efficacy is solely due to the specifics of the patient population that was mostly vaccinated. In other words, the reduction in risk of hospitalization provided by Paxlovid cannot be greater than a certain threshold if the patient has been vaccinated, which has already provided some level of protection against COVID-19. This is confirmed by the high risk reduction among under-vaccinated individuals.
For reference, among those treated with Paxlovid, 76.6% received a third (booster) dose of the vaccine, 17.4% were fully vaccinated, 1.6% were partially vaccinated, 4.5% were not vaccinated, and 79.9% received their last dose of vaccine more than 20 weeks ago.
Israel #1
An analysis of the efficacy of Paxlovid, which was given to Israeli patients (n=4737) aged 60 years or older (mean age 68.5 years) between early January and late February 2022 in a real-world setting dominated by Omicron (subvariant BA.1), showed a 46% reduction in risk of severe COVID-19 or death: hazard ratio (HR) 0.54 (95% CI: 0.39–0.75; p<0.001).
Among vaccinated (including those who received a booster dose) and unvaccinated (including those who were not fully vaccinated), the reported risk reduction was 38% (HR 0.62 [95% CI: 0.39–0.98]) and 48% (HR 0.52 [95% CI: 0.32–0.82]), respectively.
In an analysis of only that population of patients diagnosed with COVID-19 after mid-January 2022, when the Omicron variant prevailed, the efficacy of Paxlovid in preventing progression of coronavirus infection to severe or fatal was 57% (HR 0.43 [95% CI: 0.85–0.64]).
The decreased therapeutic efficacy of Paxlovid in the setting of Omicron variant infestation, when compared with the results of the clinical trial EPIC-HR (NCT04960202) phase 2/3, is due to several factors. First, infection with Omicron suggests a less severe course of the disease. Second, the drug was administered according to a positive laboratory test result for SARS-CoV-2, whereas in the study it was administered in the presence of symptoms. Because symptoms usually precede laboratory confirmation, treatment in the trial started earlier and was therefore more effective. In addition, COVID-19 in some of the patients in the Israeli analysis most likely had already lasted more than 5 days, meaning that Paxlovid did not have the proper beneficial effect due to the advanced nature of the disease.
Remarkably, the presence of vaccination (and 77.8% of patients were vaccinated) had no effect on the therapeutic efficacy of Paxlovid.
Israel #2
Administration of Paxlovid between early January and mid-March 2022 to Israeli patients (n=3939), 78.1% of whom were vaccinated (or had previously had COVID-19), in a real-world setting dominated by the Omicron variant (sublineage B.1.1.529) was reflected in the following results:
- In patients aged 65 years or older, nirmatrelvir with ritonavir reduced the risk of hospitalization by 67% (hazard ratio [HR] 0.33 [95% CI: 0.19–0.55]) and death by 81% (HR 0.19 [95% CI: 0.05–0.76]).
- In patients aged 40–64 years, nirmatrelvir with ritonavir reduced the risk of hospitalization by 22% (HR 0.78 [95% CI: 0.40–1.53]) and had no effect on reducing the risk of death (HR 1.64 [95% CI: 0.40–12.95]).
The insignificant efficacy of Paxlovid in the younger age group is mainly due to the non-serious course of COVID-19 infection caused by Omicron. Nevertheless, even in this patient population, nirmatrelvir with ritonavir reduced the risk of hospitalization by 79% (HR 0.21 [95% CI: 0.03–1.53]) in the absence of immunity to SARS-CoV-2.
Hong Kong
The use of Paxlovid from late February to late April 2022 in the treatment of COVID-19 infection in Hong Kong patients (n=890) in a real-world setting dominated by the Omicron variant (subvariant BA.2) resulted in the following:
- Paxlovid reduced the risk of disease progression (death from any cause, need for invasive mechanical ventilation, transfer to the ICU) by 43% (hazard ratio [ HR] 0.57 [95% CI: 0.45–0.72]; p<0.0001) relative to those who were not treated with it.
- Paxlovid reduced the risk of death from any cause by 66% (HR 0.34 [95% CI: 0.23–0.50]; p<0.0001).
- Paxlovid reduced the risk of needing supplemental oxygen by 27% (HR 0.73 [95% CI: 0.54–0.97]; p=0.032).
- Paxlovid reduced the risk of needing invasive mechanical ventilation by 3% (HR 0.97 [95% CI: 0.31–3.03]; p=0.96).
- Paxlovid accelerated viral load reduction by one-third (HR 1.38 [95% CI: 1.07–1.79]; p=0.013).
- Paxlovid reduced hospital stay by an average of 0.43 days (95% CI: −1.29 to −0.42]; p=0.32).
The mean age of patients was 77 years, 83% were older than 65 years, and 10.5% were fully vaccinated. Paxlovid was administered after a median of 1 day (1–3) after manifestation of covid symptoms.
Paxlovid for Everyone
Pfizer, hoping to significantly expand the population of patients who could benefit from Paxlovid, has tested its efficacy among unvaccinated individuals at standard risk, that is, at low risk of hospitalization or death.
According to the interim results (n=854) of the corresponding EPIC-SR (NCT05011513) phase 2/3 clinical trial, the primary efficacy point of treatment was not reached. Administration of Paxlovid did not result in a statistically significant difference with placebo in terms of sustained relief of COVID-19 symptoms over four consecutive days.
However, use of Paxlovid was reflected in a relative 70% reduction in hospitalizations and no deaths from any cause (p=0.051). Nirmatrelvir with ritonavir provided a 10-fold (by 1 log10 viral copies/mL) reduction in viral load.
According to the final results (n=1145), Paxlovid reduced the risk of hospitalization or death by a statistically insignificant 51% relative to placebo. In the included cohort of vaccinated patients with a risk factor for progression to severe COVID-19 (n=721), the risk reduction was a statistically insignificant 57%.
Other outcomes in the Paxlovid group included a 62% reduction in the number of COVID-19-related health care visits (p=0.0228), a 72% reduction in the average number of days in hospital (if hospitalization was still required), no ICU admissions (3 cases in the placebo group), and no fatal outcomes (1 case in the placebo group).
Paxlovid for COVID-19 Prophylaxis
The EPIC-PEP (NCT05047601) phase 2/3 clinical trial challenged to test Paxlovid in the task of post-exposure prophylaxis to prevent COVID-19 in a high-risk setting for potential SARS-CoV-2 infection.
A trial was conducted among individuals (n=2957) with a negative SARS-CoV-2 rapid antigen test result who had contact with a family member who was SARS-CoV-2 positive and symptomatic with COVID-19 during the 4 days prior to randomization.
Prophylactic administration of Paxlovid was found to reduce by statistically insignificant 32% and 37% the risk of confirmed and symptomatic COVID-19, respectively, among those who had taken the drug for 5 and 10 days.
COVID-19 Rebound After Paxlovid Treatment
In late May 2022, the U.S. Centers for Disease Control and Prevention (CDC) issued a warning regarding the possibility of recurrence of COVID-19 infection successfully treated with Paxlovid.
COVID-19 recurrence, or COVID-19 rebound, occurs between 2 and 8 days after initial recovery and is characterized by the reappearance of COVID-19 symptoms and/or a positive test for SARS-CoV-2 after being negative. Such relapse does not result from reinfection with SARS-CoV-2 nor from the development of resistance to Paxlovid. [1] [2]
COVID-19 rebound after Paxlovid treatment occurs in 1%–2% of cases. (In reality, it occurs more frequently, but is usually not recorded, for example, because of mild symptoms.) Recurrence can occur even in those who have been vaccinated or have received a booster dose of the vaccine.
Patients who experience COVID-19 rebound have an extremely low chance of the disease progressing to a severe form. [3]
There is no need for additional treatment of COVID-19 that has relapsed after Paxlovid treatment: In the median 3 days, the condition will improve or the illness will disappear completely. However, patients with viral rebound should take precautions to prevent infection of others.
Pfizer, however, is not against having patients with COVID-19 rebound undergo a second course of treatment with Paxlovid: if the coronavirus is not completely suppressed, it should be done. Regulators have not yet reached any consensus on re-prescribing the drug.
↓
It is possible that the recurrence of clinical disease after treatment with Paxlovid for COVID-19 infection is related, first, to the initially high viral load and, second, to the still active viable virus, which can cultivate for two weeks after completion of therapy. In other words, a 5-day course of nirmatrelvir with ritonavir is not enough in some cases. [4]
↓
The increase in total T lymphocytes and virus-specific T lymphocytes, T cell activation biomarkers, and antibodies detected during viral rebound suggests that symptoms of relapsed COVID-19 infection may be due in part to an emerging immune response against residual viral antigens, which may have been released from dying infected cells due to cytotoxicity and tissue repair throughout the respiratory tract. Symptoms may be more clinically pronounced after the use of potent antiviral treatment with rapid clinical improvement and reappearance of the antigen during the maturation of the immune response. [5]
The hypothesis that taking an antiviral drug early in COVID-19 development leads to interference with adaptive immune responses, the disruption of which contributes to symptomatic relapse, should be rejected.
↓
According to a retrospective data analysis of patients (n=11270) who were treated with Paxlovid from early January to early June 2022, the recurrence rate of COVID-19 in the 7- and 30-day periods after successful completion of therapy was 3.5% and 5.4% for infection and 2.3% and 5.9% for COVID-19 symptoms. At the same time, 0.4% and 0.8% of patients experienced a need for hospitalization. [6]
A generally similar risk of COVID-19 rebound was observed with molnupiravir.
It is possible that the increased rate of COVID-19 rebound, when compared with earlier observations, was influenced by the fact that the data analyzed were obtained during the period of dominance of the Omicron variant, which is less sensitive to neutralizing antibodies and is therefore characterized by a longer elimination time from the body.
↓
According to a retrospective study examining the administration of Paxlovid between early May and mid-July 2022 to patients (n=15,913) in an environment dominated by the Omicron variant, those infected with now ubiquitous BA.5 subvariant than BA.2.12.1 subvariant were a third more likely to experience COVID-19 rebound: hazard ratio (HR) 1.32 (95% CI: 1.06–1.66) for recurrent infection and HR 1.32 (95% CI: 1.04–1.68) for recurrent symptoms. [7]
It has been suggested that due to the high mutational nature of SARS-CoV-2, emerged and established variants of the virus are endowed with an improved ability to evade neutralizing antibodies, and therefore a longer treatment with Paxlovid should be considered in order to guarantee suppression of the virus.
↓
COVID-19 rebound can also occur without any treatment. In the ACTIV-2 (NCT04518410) phase 2/3 platform clinical trial, which tested various treatments for COVID-19, among participants who received placebo, that is, their disease proceeded naturally, at day 5, viral rebound (an increase in viral RNA levels of ≥ 0.5 log10 copies/mL) occurred in 12%, while symptom rebound after initial improvement occurred in 27% and symptom rebound after resolution occurred in 10%. A rare combination of viral rebound with a high viral load (viral RNA level ≥ 5.0 log10 copies/mL), mediating an increased risk of transmission from patients to healthy individuals, with symptom rebound after improvement was seen in 1%–2%. [8]
COVID-19 rebound may have a multifactorial nature, the components of which include spread of the virus over time to different anatomical regions (causing a developing series of symptoms), infection with two different variants of the virus (rare), co-infection with another respiratory virus, and recurrence of symptoms of non-infectious etiology.
Paxlovid and Treatment Resistance
From the very beginning, it was clear that the widespread introduction of Paxlovid into clinical practice for COVID-19 treatment would lead to the emergence of resistant strains of the virus. This is not surprising: With the ubiquitous prevalence of SARS-CoV-2 on the planet, its rapid replication with generational changes and high mutability, the formation of resistance to nirmatrelvir with a decrease in therapy efficacy is only a matter of time.
The traditional way to circumvent the issue of antiviral drug resistance is to use a drug cocktail that affects the pathogen through different mechanisms simultaneously. This idea is the basis of combined treatment of HIV and chronic hepatitis C, which involves the continuous administration of several drugs that work in different ways at once.
Ideally, treatment of COVID-19 with nirmatrelvir, a protease inhibitor, would be combined with molnupiravir, a viral polymerase inhibitor. According to a study in mice, the combination of nirmatrelvir with molnupiravir significantly improves treatment efficacy, which cannot be said about the combination of nirmatrelvir with remdesivir. [1] In practice, this is not the case, and therapeutic control of COVID-19 is carried out with either one or the other drug, i.e. the potential threat of drug resistance formation is picked up from different directions.
No clinical trials testing a cocktail of nirmatrelvir and molnupiravir have yet been registered. Moreover, Pfizer refuses to make nirmatrelvir available to researchers for any clinical trials combined with other drugs, and does so without reasonable explanation. The Drugs for Neglected Diseases initiative (DNDi) would like to test nirmatrelvir in combination with the inhaled corticosteroid budesonide or possibly the antidepressant fluoxetine in order to extend the five-day therapy window by at least two days, when Paxlovid could still work. This is relevant, because in low- and middle-income countries, more than half of COVID-19 patients seek treatment after five days due to weak SARS-CoV-2 testing infrastructure and a number of bureaucratic issues. With limited access to vaccines, Paxlovid would come in handy. Working with generic copies of nirmatrelvir in the combination direction faces additional obstacles in the form of unclear licensing conditions and bioequivalence difficulties. [2] [3]
A number of in vitro studies simulating the development of drug resistance in humans have confirmed that SARS-CoV-2 relatively easily acquires resistance to nirmatrelvir, which reduces the susceptibility of the coronavirus to the drug by many tens of times. [4] [5] [6]
The list of SARS-CoV-2 mutations responsible for nirmatrelvir resistance continues to grow. [7] [8] [9]
So far, it is reassuring only that, first, Paxlovid is not yet taking enough people to make the virus unequivocally and universally mutate, and second, judging by Pfizer statements, the prescribed dose of nirmatrelvir is many times greater than what is needed to prevent viral replication, which means that it theoretically minimizes the potential for mutation. In addition, many factors must coincide whereby drug resistance mutations to Paxlovid will not negatively affect coronavirus characteristics such as replicability, infectivity, infectiousness, transmissibility, virulence, pathogenicity, and lethality, upsetting their acceptable balance, otherwise the virus will simply not register them by discarding them.
Paxlovid: Mechanism of Action
Paxlovid is an oral antiviral drug indicated for the treatment of COVID-19 infection caused by the SARS-CoV-2 coronavirus.
Paxlovid combines two drug compounds, nirmatrelvir and ritonavir [NIR/r].
Nirmatrelvir (PF-07321332) is a reversible covalent inhibitor of 3C-like protease (3CLpro), also known as main protease (Mpro), an enzyme required by SARS-CoV-2 for replication. [1]
SARS-CoV-2, being an enveloped positive-sense (+) RNA virus, enters host cells by binding its S protein to angiotensin-converting enzyme 2 (ACE2) on the cells and then releasing genomic RNA (gRNA) into the cytoplasm after uncoating. The cell’s ribosomes then translate the gRNA into the two major polyproteins, pp1a and pp1ab. Proteases embedded in viral nonstructural proteins 3 (Nsp3) and 5 (Nsp5), papain-like protease (PLpro) and chymotrypsin-like protease (3CLpro), respectively, cleave pp1a and pp1ab into 16 nonstructural proteins that assemble into replication–transcription complexes (RTCs). The latter produce new gRNAs and a set of subgenomic RNAs (sgRNAs) including open reading frames (ORFs) that encode structural viral proteins such as S protein, membrane (M), envelope (E), and nucleocapsid (N) proteins, as well as a number of accessory proteins. The newly created gRNAs are translated to produce additional nonstructural proteins, serve as a template for further RNA synthesis, or are packaged into new virions.
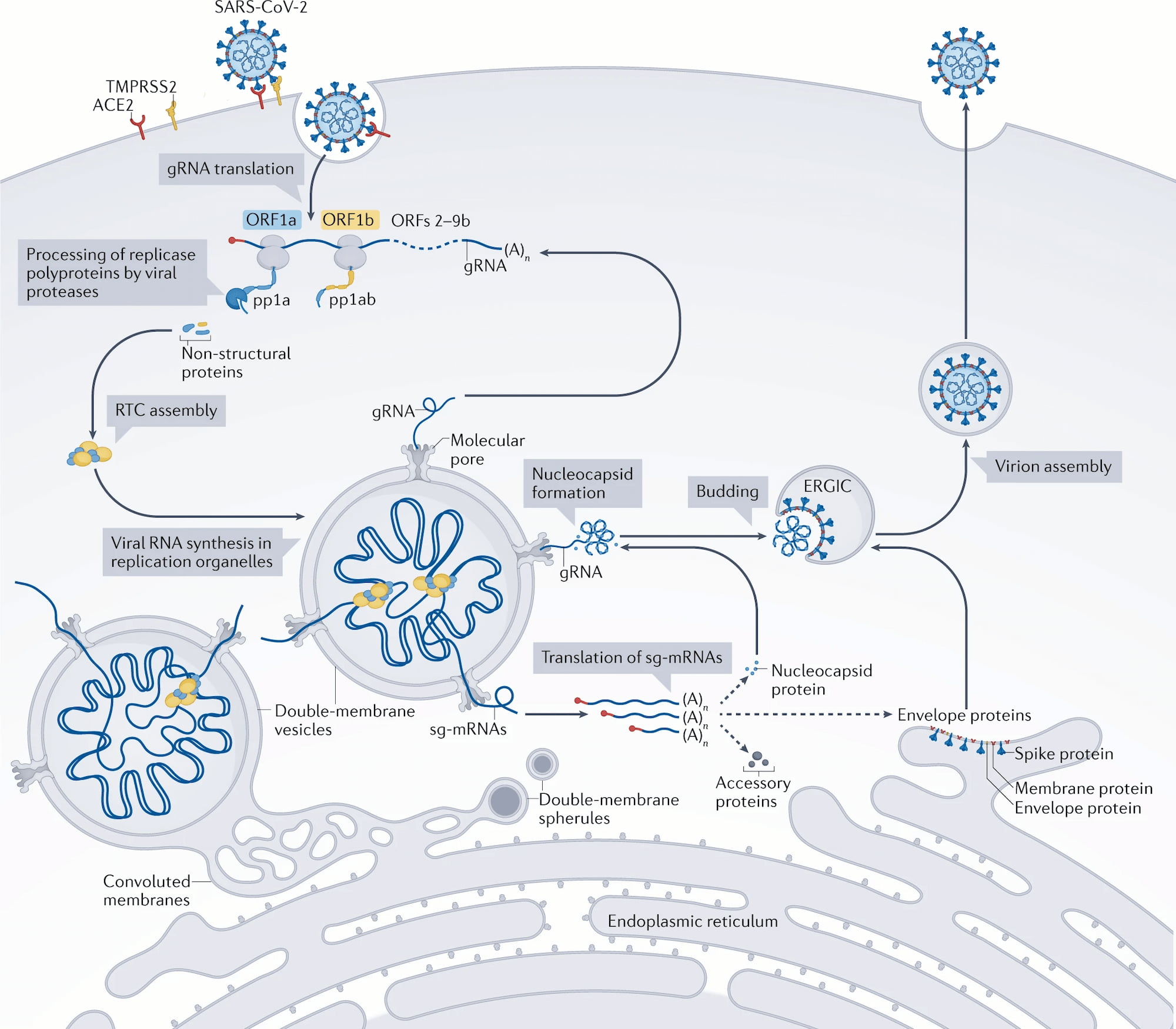
Nirmatrelvir blocks the cysteine residue in 3CLpro, thereby inhibiting its activity at the proteolysis stage. Inhibition of 3CLpro interrupts the life cycle of the virus, preventing it from replicating.
In vitro nirmatrelvir has antiviral activity against coronavirus variants Alpha, Beta, Gamma, Delta, Lambda, and Mu. Nirmatrelvir also works against the Omicron variant. [2] [3] [4] [5]
Ritonavir (ritonavir) is a booster (enhancer) of nirmatrelvir. Ritonavir inhibits cytochrome P450 3A4 (CYP3A4), a hepatic enzyme that metabolizes xenobiotics, that is, it deactivates drug compounds. Adding ritonavir at a low dose increases the bioavailability of nirmatrelvir, helping to slow down the metabolism of this molecule so that it retains its activity in the body for a longer period of time and at higher concentrations. [6]
Paxlovid Pricing
Pfizer’s tiered pricing policy is such that during the COVID-19 pandemic, Paxlovid is offered at prices based on each country’s income level: developed economies pay more than poorer countries.
Obviously, many people will want to buy Paxlovid, which will inevitably lead to the formation of a black market. Speculators and intermediaries will establish illegal channels of supply of copies of Paxlovid from countries where either large-scale production of its generics is organized or the drug is sold without large commercial mark-ups.
The exact price of the Paxloid is a big mystery. Pfizer, it is believed, deliberately does not disclose the financial details of supplying the drug to any country, so as not to agitate the community, already angered by the incredible enrichment of the pharmaceutical business on the pandemic.
↓
In mid-November 2021, the U.S. government awarded Pfizer a $5.29 billion contract to supply 10 million therapeutic courses of Paxlovid. Thus, the price of Paxlovid for U.S. patients is set at $530 per course. It should be understood that Paxlovid is completely free to U.S. citizens along with other COVID-19-relate drugs, vaccines and tests.
According to the terms of the contract, if any of the other countries with strong economies — the G7 countries (Canada, France, Germany, Italy, Japan, the United Kingdom) or Switzerland — order Paxlovid at a lower price than the agreements with the U.S., the latter have the right to a corresponding price reduction. Since Pfizer is unlikely to want to lose revenue, Paxlovid in these countries will in no way be cheaper than in the U.S.
↓
In mid-November 2021, Pfizer signed a voluntary licensing agreement for Paxlovid with the Medicines Patent Pool (MPP) of Unitaid, which aims to increase access to drugs for poor countries. Low-cost generic copies of nirmatrelvir with ritonavir will be distributed in 95 low- and middle-income countries, and Pfizer will not receive any royalties from sales.
↓
In late December 2021, Bangladesh-based Beximco Pharmaceuticals and Eskayef Pharmaceuticals announced the launch of the world’s first generics of Paxlovid, called Bexovid and Paxovir. In pharmacy retail, a 5-day course of treatment will cost BDT 16,000 ($167) and BDT 16,700 ($176), respectively. It is stated that the price will gradually decrease. And so it did: as of mid-August 2022, the price of a course of Bexovid and Paxovir was BDT 12,500 ($132) and BDT 14,500 ($153).
Other generics of Paxlovid soon appeared in Bangladesh. For example, Jupitavir by Incepta Pharmaceuticals, Axlovir by Square Pharmaceuticals, and Nevirax by ACI can be purchased for BDT 16,000 ($169).
↓
At the end of January 2022, the government of Panama placed an order with Pfizer for Paxlovid. Based on the $13.5 million for 54,000 therapeutic courses of the drug, Paxlovid cost $250 per package.
↓
In mid-March 2022, MPP sublicensed the production of generic Paxlovid to 38 pharmaceutical manufacturers from 12 countries: Bangladesh, Brazil, China, the Dominican Republic, India, Israel, Jordan, Korea, Mexico, Pakistan, Serbia, and Vietnam. A little later, Ukraine joined in.
↓
As Doctors Without Borders (Médecins Sans Frontières, MSF), a nonprofit medical humanitarian organization helping people in emergencies, believes, licensing deals like the one between Pfizer and MPP create uncertainty and segmentation for generic production and supply, continuing to fuel persistent inequalities in global access to vaccines and drugs to fight COVID-19. Paxlovid’s voluntary license to 95 countries, home to approximately 53% of the world’s population, has excluded many upper-middle-income countries, such as Argentina, Brazil, China, Malaysia, and Thailand, where established generic drug production exists.
Doctors Without Borders has called for the will of governments to take advantage of all the legal options necessary for successful anti-COVID-19 activities, including the rejection of Pfizer patent applications and suspension of patents, the compulsory licensing of Paxlovid, and controls on drug prices. According to MSF, the best solution is to repeal the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS), which is part of the World Trade Organization (WTO) package. Human lives are more important than the pharmaceutical business.
↓
According to calculations by Knowledge Ecology International (KEI), the 95 countries that have received a voluntary license for Paxlovid are characterized by a combined gross national income (GNI) of 13% of the world total. The contribution of the remaining 122 countries is 87%. In other words, Pfizer is confident that states capable of paying full price for Paxloid will do so anyway.
The picture is paradoxical: for example, Brazil and Mexico are allowed to produce generics of Paxlovid, but are prohibited from selling it on their own territory.
↓
To distribute Paxlovid in economically underdeveloped countries, Pfizer pledged in late March and late June 2022 to provide up to 4 million and 6 million treatment courses of the drug to UNICEF and the Global Fund during the years 2022 and 2022–2023, respectively.
↓
In mid-May 2022, the Clinton Health Access Initiative (CHAI), a Clinton Foundation nonprofit organization dedicated to saving lives and reducing the burden of disease in low- and middle-income countries, agreed with generic manufacturers of Paxlovid to supply the drug to states covered under licensing arrangements between Pfizer and MPP at a ceiling price of $25 per therapy course. This is subject to an annual aggregate order quantity of at least 1 million courses and an individual order quantity of at least 50,000 courses. Due to the higher cost of the drug, CHAI partners will make up the difference in price. For this purpose, generic drug manufacturers have committed to a total of 4.5 million courses of Paxlovid each month.
↓
At the end of May 2022, Pfizer made a commitment to make all of its patented drugs and vaccines available in the U.S. and Europe on a nonprofit basis to 45 low- and lower-middle-income countries. That includes Paxlovid. The list of such countries includes mainly states on the African continent.
↓
According to expert estimates as of the beginning of April 2022, the production cost of a 5-day therapeutic course of Paxlovid is $65. If we talk about the release of its generic copies, the estimated price, which takes into account a 10% profit margin and 27% income tax, is $73. These amounts do not include other costs, including logistics and marketing.
Paxlovid Business
After Paxlovid, which debuted in the United States in late 2021, received its first regulatory approval worldwide, Pfizer projected sales of the drug for all of 2022 at $22 billion. And it doesn’t seem to have been wrong. So, while Paxlovid earned $1.470 billion in the first quarter of 2022, it earned $8.115 billion in the second. The U.S. pharma giant’s current revenue expectations for the antiviral blockbuster are unchanged.
- By comparison, the mRNA vaccine Comirnaty (tozinameran; BNT162b2) put $11.3 billion into Pfizer’s piggy bank in 2021 and $22.075 billion in the first half of 2022. Throughout 2022, Comirnaty should generate $32 billion.
Pfizer expects to release 6 million therapeutic courses of Paxlovid in the first quarter of 2022, 30 million in the first half of the year, and 120 million for the full year.
As of the end of May 2022, Pfizer had shipped more than 12 million therapeutic courses of Paxlovid to nearly 40 countries.
According to industry experts, business of Paxlovid, which at first faced the avalanche demand, will slow down: in 2022, only 50 million therapeutic courses of the drug, which Pfizer intends to produce, will be used. The assumption is based on the fact that as of the mid-August 2022, the U.S., which ordered the drug for 20 million patients and already received 7.1 million of its courses, had distributed the drug among only 3.9 million patients.
The advent of Paxlovid, administered by patients themselves at home, was supposed to relieve the health care system. The initiative encountered numerous obstacles to the active implementation of the drug in clinical practice. Thus, COVID-19 treatment with nirmatrelvir with ritonavir is allowed to start no later than 5 days after the onset of disease symptoms. At the same time, confirmatory testing for SARS-CoV-2 is required. Because Paxlovid is a prescription drug, you must see a physician to obtain it. Prescribing is done, first, in the presence of risk factors for severe COVID-19, second, with laboratory tests that rule out serious kidney and liver problems, and third, with rigorous and mandatory testing of drug interactions of ritonavir with all the drugs the patient is already taking. All of this, along with patients’ traditional inertia in making decisions and the background of the generally milder course of COVID-19 caused by the Omicron variant, leads to inevitable delays in starting treatment when it is too late to take Paxlovid.
In early March 2022, the U.S. government, recognizing this issue, launched the national Test-to-Treat program, which has more than 2,700 sites across the country that offer rapid testing for SARS-CoV-2 and, if positive and eligible for treatment, free oral antiviral medication, Paxlovid or molnupiravir, onsite.
In early July 2022, the FDA allowed pharmacists to prescribe Paxlovid to patients if the above conditions of treatment eligibility are met.
Be that as it may, Paxlovid is projected to make Pfizer a lot of money in 2022, covering 79% of the global market for oral antiviral drugs to treat COVID-19. Next year, 2023, demand will decline decently, as the countries that bought Paxlovid will still have it in stock.
Paxlovid Evolution
In late June 2022, Pfizer sent an application to the U.S. Food and Drug Administration (FDA) for full approval of Paxlovid, which is now approved under the Emergency Use Authorization (EUA). The U.S. regulator’s verdict is expected in the first quarter of 2023.
- The main difference between an Emergency Use Authorization used during a public health emergency and a full regulatory approval has to do with the amount of data from clinical trials. Full-fledged approval, which relies on substantially more data provided than is necessary for an EUA, assumes that the benefits of the drug product are proven to outweigh any potential risks. The clinical data for this must equally encompass a larger number of patients and a longer period of follow-up.
In early March 2022, Pfizer launched the EPIC-PEDS (NCT05261139) phase 2/3 (non-randomized, open-label, multicenter, international) clinical trial testing Paxlovid in the treatment of symptomatic COVID-19 infection in non-hospitalized pediatric (infants to 17-year-olds) patients (n=140) at risk for progression to severe disease.
- Since the beginning of the COVID-19 pandemic in the United States, more than 11,000 children and adolescents have reportedly tested positive for coronavirus, accounting for nearly 18% of all reported infections. This resulted in more than 100,000 hospitalizations. In other words, the pediatric outpatient population is in need of an effective antiviral.
The NCT05438602 phase 2 (randomized, double-blind, multicenter) clinical trial is testing Paxlovid among immunocompromised patients 12 years of age and older. Nirmatrelvir with ritonavir is prescribed for 5, 10 or 15 days.
To address the issue of COVID-19 rebound treated with Paxlovid, Pfizer is to conduct a clinical trial that will answer the question of whether re-prescribing the drug is warranted. The first results will be available by the end of September 2023.
Pfizer is developing a new oral antiviral to replace Paxlovid, which is intended to address the issue of potential treatment resistance due to SARS-CoV-2 mutations. The new drug, which has the same high clinical efficacy, will not contain ritonavir, which means that it will eliminate the issue of Paxlovid incompatibility with many other concomitant medications. By the way, Japan’s Shionogi & Co. has already done this with Xocova (ensitrelvir).
Paxlovid and Patent Litigation
In late June 2022, Enanta Pharmaceuticals sued, accusing Pfizer of infringing patent US11358953B2, describing drugs that inhibit 3C-like protease (3CLpro), an enzyme required by SARS-CoV-2 for replication.
Enanta has asked the court to order Pfizer to compensate it for intellectual property infringement damages and to pay royalties from sales of Paxlovid, which, as a 3CLpro inhibitor, allegedly uses the patented chemical structure of 3CLpro inhibitors and COVID-19 treatment inappropriately. Enanta, however, does not intend to impede or prohibit the sale of Paxlovid in any way.
Enanta is developing EDP-235, an oral reversible competitive peptidomimetic 3CLpro inhibitor that is taken once daily, requires no ritonavir booster and works against all variants of SARS-CoV-2 and any human coronavirus. The antiviral activity of EDP-235 is superior to that of nirmatrelvir and ensitrelvir.
Enanta is not a patent troll, as its expertise in antiviral drug development has already borne fruit in the form of three drugs: Viekira Pak and Viekira XR, combining dasabuvir, ombitasvir, paritaprevir, and ritonavir to treat genotype 1 chronic hepatitis C virus (HCV) infection, and Mavyret/Maviret, which includes glecaprevir and pibrentasvir and targets HCV treatment for all genotypes in a short, 8-week course of therapy if the patient has not previously been treated.
AbbVie, which markets Viekira and Mavyret/Maviret, has licensed paritaprevir and glecaprevir, hepatitis C virus NS3/4A protease inhibitors, from Enanta.