Highlights
The experimental oral drug molnupiravir has nearly halved the risk of hospitalization or death among high-risk patients with mild-to-moderate COVID-19 infection. When it comes to the risk of death, it has decreased by an impressive 94%.
- Updated data on the therapeutic efficacy of the drug showed that molnupiravir performed significantly worse against COVID-19 than originally reported. So, molnupiravir reduced the risk of hospitalization or death by 30% and the risk of death by 89%.
The drug is being developed by Merck & Co., which bought the rights to it from Ridgeback Biotherapeutics, which in turn licensed the molecule from Emory University.
The United Kingdom was the first country in the world to officially approve Lagevrio (molnupiravir) for treatment of mild-to-moderate COVID-19 in adult patients with risk factors for developing severe disease.

Lagevrio: New Antiviral Drug to Treat COVID-19
The oral antiviral drug molnupiravir by Merck & Co.
Other countries, including the U.S. and the European Union, continue to review the application for molnupiravir. For example, the U.S. Food and Drug Administration (FDA) will meet on November 30 for approval of molnupiravir.
- The FDA’s Advisory Committee voted to approve molnupiravir for the outpatient treatment of COVID-19. However, the experts, first, still haven’t figured out the reason why the effectiveness of molnupiravir has dropped dramatically, and second, they called for some caution with the drug.

Molnupiravir: What U.S. Experts Said
FDA scientists took a detailed look at molnupiravir for treating COVID-19.
Pricing remains an open question: it is not yet known exactly how much molnupiravir will cost in any given country. First, Merck & Co. has notified that the price of molnupiravir will be flexible, depending on the economic status and purchasing power of a particular country. Second, Merck & Co. granted non-exclusive voluntary licenses to Indian generic drug makers so that cheap copies of molnupiravir would appear in more than a hundred lower-middle-income countries (LMICs). Third, Merck & Co. licensed molnupiravir to the Medicines Patent Pool (MMP) of UNITAID, which again means that generics of this anti-COVID-19 drug will be affordable in a hundred poor nations.
According to expert estimates, the cost of producing a therapeutic 5-day course of molnupiravir starts at $17.74 and falls to $3.86–6.84 when the synthesis process is optimized. But that doesn’t mean that everyone can buy molnupiravir inexpensively.
Industry observers predict that molnupiravir, marketed in an easy-to-use oral formulation for home administration, is well-positioned to reach $10 billion a year in earnings. Merck & Co. itself expects revenue from molnupiravir to be in the range of $5 billion to $7 billion in 2022.
The closest competitor to molnupiravir is Pfizer’s oral antiviral drug Paxlovid, which has demonstrated significantly better efficacy in treating COVID-19.

Paxlovid: New Cure for Coronavirus
Pfizer’s oral antiviral drug reduced the risk of hospitalization or death from COVID-19 by 89%.
Lagevrio and Paxlovid are the world’s first really working anti-COVID-19 drugs in a convenient oral formulation. And this is quite a remarkable achievement: first, COVID-19 can be effectively treated at home; second, it will reduce the burden on the health care system, which is bogged down by the flow of patients; and third, it will somehow help those who oppose vaccination or cannot be vaccinated for medical reasons.
Therapeutic Efficacy of Molnupiravir
Molnupiravir Against COVID-19: Main Clinical Trial
The MOVe-OUT clinical trial (NCT04575597) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) enrolled non-hospitalized adult patients (n=1433) with a laboratory-confirmed diagnosis of COVID-19 with mild-to-moderate severity.
Among the mandatory criteria for inclusion in the trial: absence of COVID-19 vaccination; at least one risk factor for poor outcomes (age 60 years or older, diabetes mellitus, obesity, chronic kidney disease, serious cardiovascular disease, chronic obstructive pulmonary disease, cancer in active stage); period of manifestation of disease symptoms not longer than 5 days before randomization.
Main characteristics of participants: median age 44 years (18–88); 49% received molnupiravir or placebo within 3 days of the manifestation of COVID-19 symptoms; major risk factors were obesity in 77% of subjects, age 60 years or older in 14%, and diabetes mellitus in 14%.
Patients were given placebo or 800 mg molnupiravir — orally every 12 hours for 5 days.
The primary endpoint was the proportion of participants hospitalized and/or who died from the time of randomization to day 29 of the study.
Interim Results
According to an interim analysis of the data collected, there were 7.3% of patients (n=28/385) in the molnupiravir group — versus 14.1% in the placebo group (n=53/377) who experienced these outcomes. Administration of molnupiravir provided an absolute 6.8% reduction in risk of hospitalization or death (95% CI: −11.3 to −2.4), equivalent to a risk reduction relative to placebo of 48% (p=0.0012): risk ratio (RR) 0.52 (95% ДИ: 0.33–0.80; p=0.0012).
There were no fatalities among those receiving molnupiravir, compared to 8 in the control group. Administration of molnupiravir resulted in a relative 94% reduced risk of death: RR 0.06 (95% CI: 0.00–1.01).
The therapeutic efficacy of molnupiravir was independent of the duration of COVID-19 symptoms or the specificity of the risk factor, including patient age. Molnupiravir demonstrated consistent efficacy against viral variants, including the Gamma, Delta, and Mu strains of SARS-CoV-2, which accounted for nearly 80% of MOVe-OUT infections.
The safety profile of molnupiravir was generally not different from that of placebo: 35% and 40% of subjects experienced adverse reactions, with adverse events caused by administration of the drug in 12% versus 11% in the control group.
Among the most common adverse events in the molnupiravir group were: diarrhea (in 3% of patients), nausea (2%), dizziness (1%), and headache (1%). All adverse reactions were mild-to-moderate in severity.
Full Results
Based on analysis of all 1408 subjects, the main characteristics of participants were as follows: median age 43 years (18–90); 47% received molnupiravir or placebo within 3 days of the manifestation of COVID-19 symptoms; major risk factors were obesity in 74% of subjects, age 60 years or older in 17%, and diabetes mellitus in 16%.
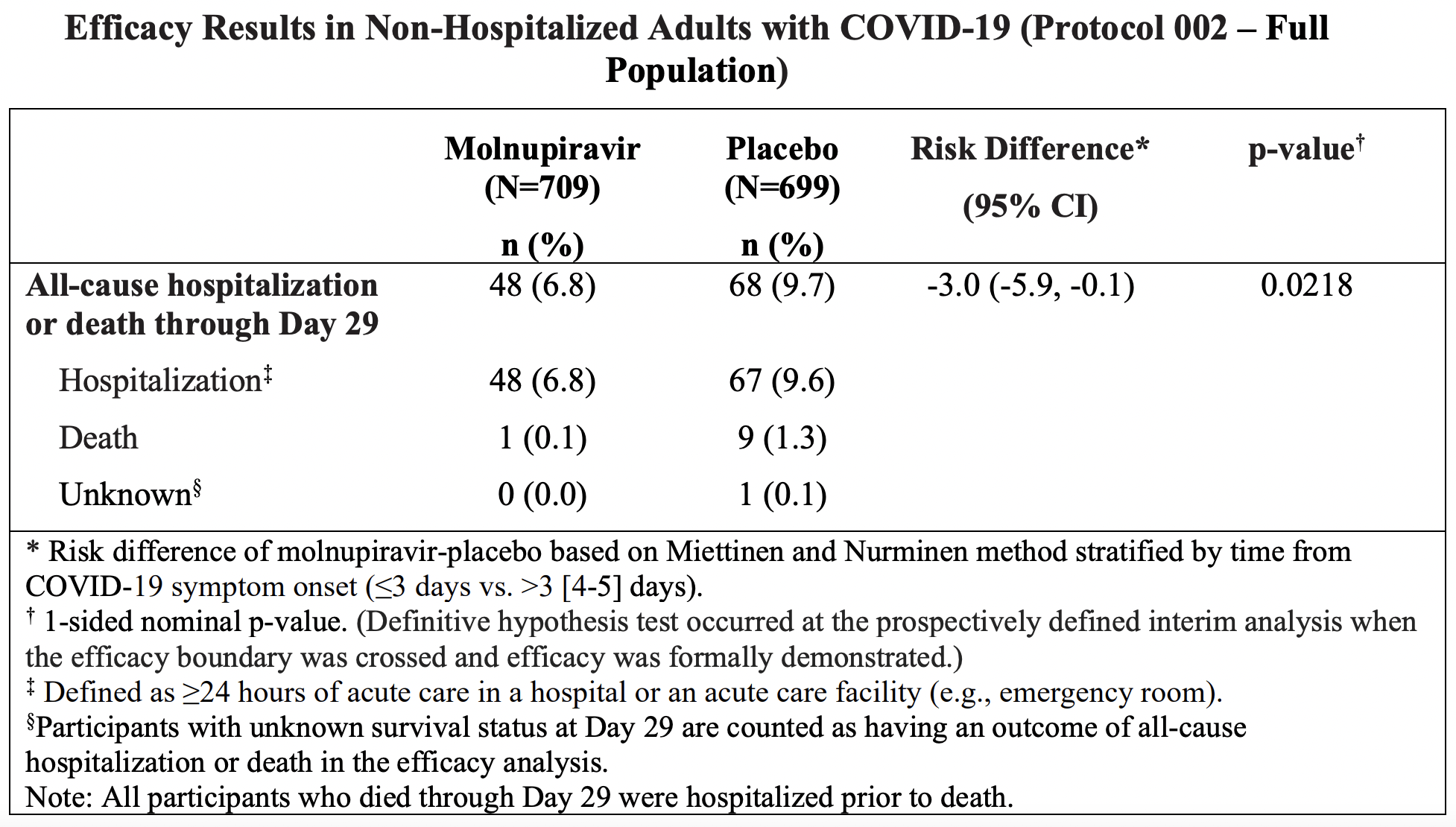
In the molnupiravir group, 6.8% (n=48/709) of patients experienced hospitalization and/or death — versus 9.7% (n=68/699) in the placebo group. Administration of molnupiravir resulted in an absolute 3.0% (95% CI: 0.1–5.9) reduction in risk of hospitalization or death, equivalent to a 30% reduction in risk compared with placebo: RR 0.70 (95% CI: 0.49–0.99).
There was 1 death among those receiving molnupiravir compared to 9 in the placebo group. The use of molnupiravir reduced the risk of death by a relative 89%: RR 0.01 (95% CI: 0.01–0.86).
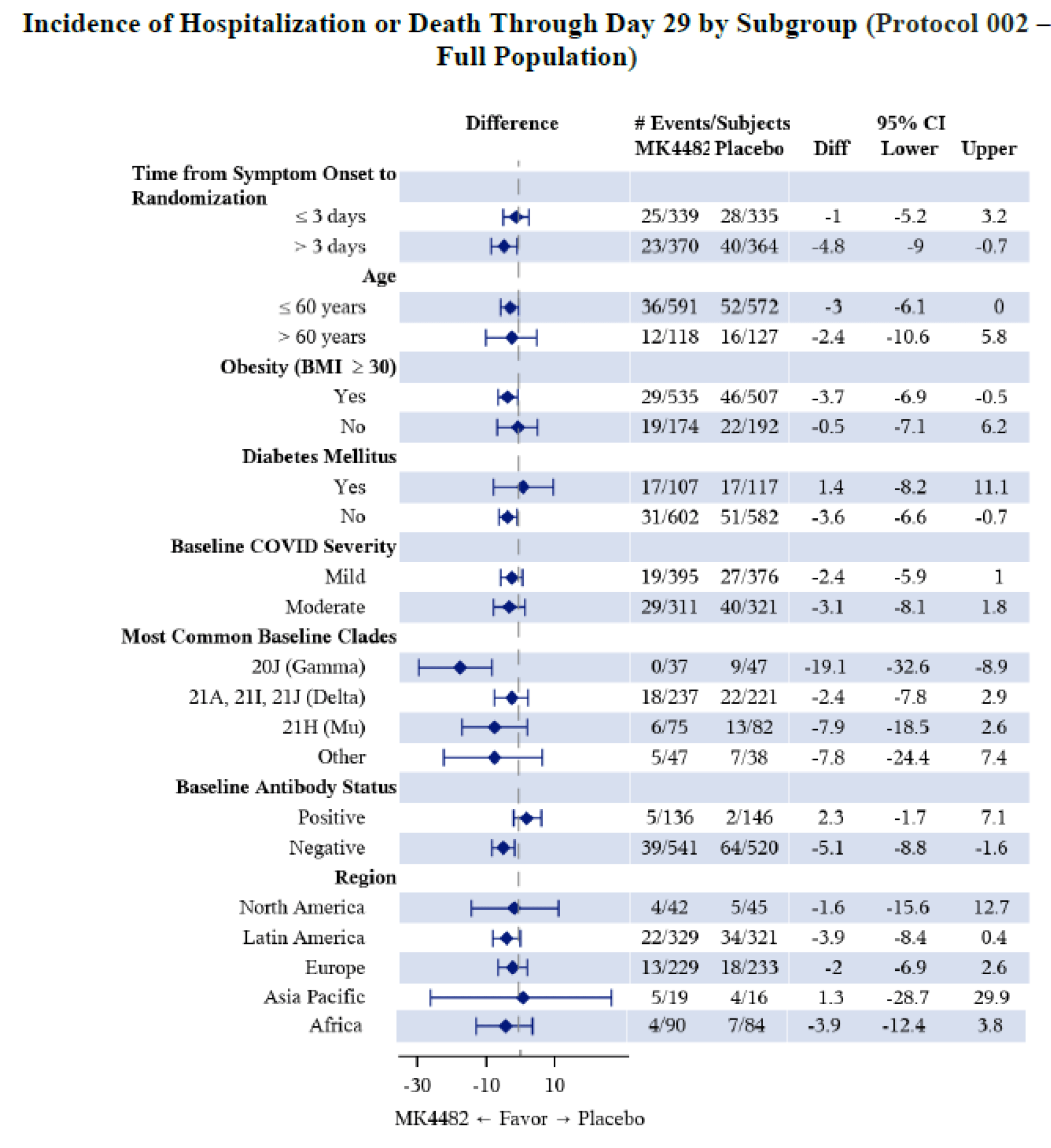
Molnupiravir worked best in patients with the Gamma variant of SARS-CoV-2: the above outcomes were seen in 0% (n=0/37) of patients — vs. 19.1% (n=9/47) in controls. In the case of the Delta variant of SARS-CoV-2, the preventive efficacy of molnupiravir was very mediocre: 7.6% of subjects (n=18/237) — vs. 10.0% (n=22/221) experienced the indicated outcomes.
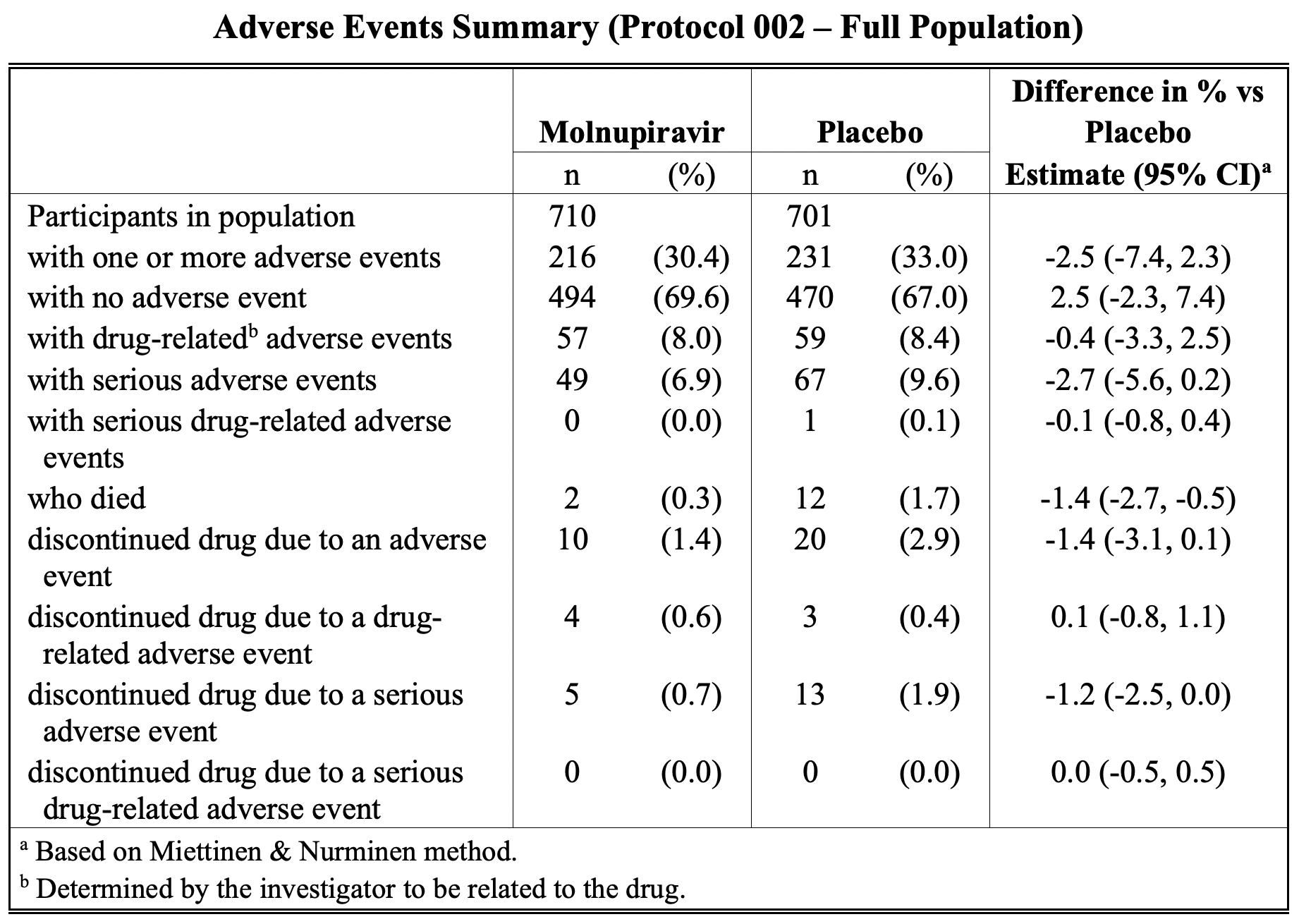
Molnupiravir was characterized by acceptable tolerability. Thus, serious adverse events were noted for 7% of participants receiving molnupiravir — vs. 10% in the placebo group. At the same time, there were no adverse events related directly to the treatment in the molnupiravir group at all —vs. 1 case in the control group.
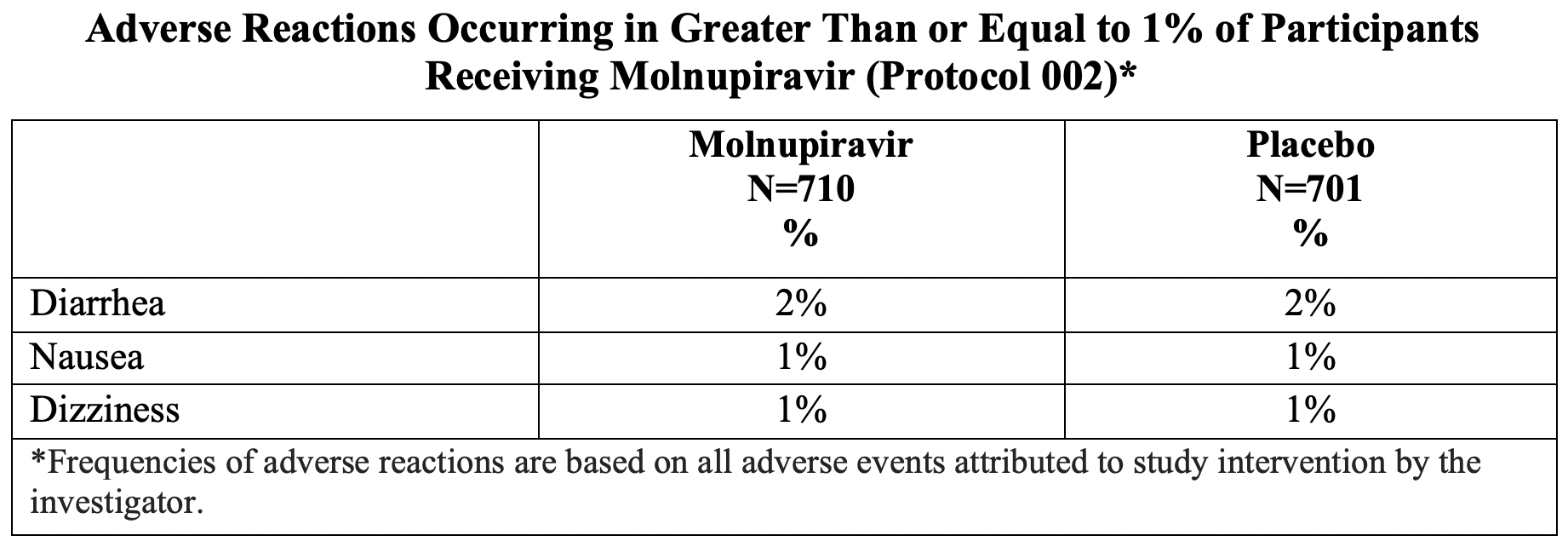
The safety profile of molnupiravir was generally not different from that of placebo. The most common adverse events in the molnupiravir and placebo groups included: diarrhea (in 3% of patients), nausea (1%), and dizziness (1%). All adverse reactions were mild-to-moderate in severity.
Molnupiravir for Treatment of COVID-19: Additional Evidence of Efficacy
India’s Hetero Labs conducted its own CTRI/2021/07/034588 phase 3 (randomized, open-label, placebo-controlled, multicenter) clinical trial among ambulatory adult patients (n=1218) with COVID-19 in the mild form. Mandatory inclusion criteria: positive PCR test results for SARS-CoV-2 obtained no later than 5 days before randomization, a risk factor for disease progression to severe form (e.g., diabetes mellitus, hypertension, etc.).
Participants who received standard COVID-19 treatment were additionally treated with placebo or 800 mg molnupiravir — every 12 hours for 5 days.
The interim results, covering data from 741 patients, are as follows:
- Molnupiravir accelerated clinical improvement (reduction of 2 points on the WHO Clinical Progression Scale): after 5 days of treatment, that was seen in 63.4% of patients — versus 22.3% in the placebo group (p≤0.0001), after 10 days in 79.0% — vs. 49.5% (p≤0.0001), after 14 days in 81.6% — vs. 73.2% (p=0.0150).
- The median time to clinical improvement in the molnupiravir group was 8 days — vs. 12 days in the placebo group (p=0.0001).
- Molnupiravir accelerated seroconversion: a negative PCR test for SARS-CoV-2 was recorded after 5 days in 77.4% of subjects — vs. 26.1% in the control group (p≤0.0001), 10 days in 94.0% — vs. 57.2% (p≤0.0001), 14 days in 97.0% — vs. 85.2% (p≤0.0001).
- During the 14-day follow-up, the proportion of hospitalized patients in the molnupiravir group was significantly lower than in the placebo group: 1.9% (n=7) — vs. 6.2% (n=23) [p=0.0027].
- No deaths were reported in the molnupiravir and placebo groups.
- Adverse reactions were not serious, manifested mildly, and did not lead to discontinuation of treatment with molnupiravir. Among the most common adverse events: nausea, diarrhea, and headache.
In parallel, Hetero is continuing a phase 3 (randomized, open-label, placebo-controlled, multicenter) clinical trial, CTRI/2021/08/035424, testing the suitability of molnupiravir in the treatment of patients with COVID-19 presenting with moderate severity.
Molnupiravir for Coronavirus Treatment: Everything Works
India’s Optimus Pharma has notified positive results from the CTRI/2021/06/033992 phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial that tested the effectiveness of adding molnupiravir to standard treatment for mild COVID-19.
It demonstrated that 5-day administration of molnupiravir at a dose of 800 mg every 12 hours provided a negative PCR test for SARS-CoV-2 RNA in 78% of subjects — versus 48% in the placebo group.
After another 5 days of follow-up, the absence of new coronavirus RNA was noted in 92% of participants — vs. 43% in the control group.
Because Optimus does not have a voluntary license agreement with Merck & Co., it had to develop the formulation of the drug called Molcovir on its own. Merck & Co. has no patent in India for the drug substance molnupiravir, it only has one for the composition.
Optimus, which produces molnupiravir active pharmaceutical ingredient (API) itself, is ready to produce 10 million capsules in two weeks and 40 million capsules in four to six weeks. It would take about three months to install additional equipment capable of increasing production to 80 million molnupiravir capsules per month.
Optimus has set the cost per molnupiravir capsule at 40 cents, meaning a five-day course of treatment would cost $16.
Molnupiravir and Accelerated Elimination of SARS-CoV-2
The NCT04405570 phase 2a (randomized, double-blind, placebo-controlled, multicenter) clinical trial examined the antiviral efficacy of molnupiravir by evaluating the drug’s ability to eliminate the new coronavirus SARS-CoV-2 from the body.
Outpatient adult patients (n=202) with a confirmed diagnosis of COVID-19 and symptoms manifesting no later than 7 days before randomization were invited for this study. Participants were administered placebo or molnupiravir in various doses — for 5 days.
A subgroup of subjects who received 800 mg of molnupiravir twice a day showed the best results. Thus, after 3 days of treatment the presence of viral load confirmed by PCR test for viral RNA in nasopharyngeal swabs was found for 1.9% of patients (n=1/53) in the molnupiravir group — versus 16.7% (n=9/54) in the placebo group (p=0.02). After 5 days of therapy, these rates were 0.0% (n=0/53) — vs. 11.1% (n=6/54) [p=0.03].
The median time required for viral RNA clearance in nasopharyngeal swabs was 14 days for the 800-mg dose of molnupiravir — vs. 27 days for placebo (p=0.001). In other words, the drug did twice as well in eliminating SARS-CoV-2 from the body.
The 800-mg dose of molnupiravir was 3.5 times more effective compared to placebo in reducing the viral load after 5 days of treatment: with differences in the least squares means in its change from the baseline was −0.547 log10 viral copies/mL (p=0.006).
Molnupiravir Helped Treat Only Mild Form of COVID-19
India’s Aurobindo Pharma and MSN Laboratories have stopped the CTRI/2021/08/035424 and CTRI/2021/05/033864 phase 3 (randomized, open-label, placebo-controlled, multicenter) clinical trials of molnupiravir in the treatment of COVID-19 running with moderate severity. The reason is that the experimental drug did not demonstrate “significant efficacy”. The pharma companies, however, will continue to test molnupiravir in the population of patients with a mild course of COVID-19 — in the framework of similar by design clinical trials CTRI/2021/07/034588 and CTRI/2021/05/033904 of phase 3, the more so that a corresponding favorable tendency on the efficiency indicator was noted.
Why molnupiravir did not work in the aforementioned patients can be explained as follows. First, according to the study design, they did not exclude hospitalized patients on whom Merck & Co. had previously reported that molnupiravir was insufficiently effective.
Second, Merck & Co. and Indian pharmaceutical companies have different definitions of moderate COVID-19. For example, the American pharmaceutical giant relies on an FDA guideline that the moderate course of COVID-19 must be accompanied by a blood oxygen level no lower than 93%, while the Indian manufacturers are relying on this figure in the 90–93% range. In other words, the patient population could have included severe patients, according to the FDA.
Molnupiravir for COVID-19 Prevention
The MOVe-AHEAD (NCT04939428) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial is ongoing to test whether molnupiravir works as a preventive drug against coronavirus infection COVID-19.
Adult volunteers (n=1332) living in the same household as persons infected with the new coronavirus SARS-CoV-2 (with laboratory-confirmed diagnosis) and exhibiting at least one of the signs or symptoms of COVID-19 (these should not last more than 5 days) are invited to participate.
Among the exclusion criteria: vaccination against COVID-19, prior history of SARS-CoV-2 infection (with or without symptoms), any signs or symptoms of COVID-19.

Famotidine for Treatment of COVID-19: Hope or Hype? The Most Comprehensive Review
Can a popular heartburn drug Pepcid help fight SARS-CoV-2?
Molnupiravir: Highlights of Chronology
Merck & Co., without waiting for the results of the MOVe-OUT clinical trial, has already set up production of molnupiravir: 10 million therapeutic courses of the drug will be produced by the end of this year 2021, and next 2022, the volumes will at least double.
Supply and purchase agreements for molnupiravir have been signed with the governments of several countries. Pricing policy promises to be flexible: it is stated that the cost of COVID-19 treatment with molnupiravir will be based on the economic status and purchasing power of a particular country.
April 2021
Merck & Co. granted non-exclusive voluntary licenses to five Indian generic drug manufacturers: Cipla, Dr. Reddy’s Laboratories, Emcure Pharmaceuticals, Hetero Labs, and Sun Pharmaceutical Industries. A little later, three more Indian companies joined: Aurobindo Pharma, Torrent Pharmaceuticals, and Viatris. This was done so that low-cost copies of molnupiravir appeared in more than a hundred lower-middle-income countries (LMICs). Such territories, according to the World Bank classification, include many countries in Africa, Asia, and South America.
June 2021
Merck & Co. agreed to supply about 1.7 million courses of molnupiravir to the U.S. government, for which it would be paid somewhere around $1.2 billion. Thus, a 5-day course of COVID-19 treatment with molnupiravir would cost U.S. citizens $712. Meanwhile, this does not mean that this is the list price of molnupiravir that will be fixed thereafter.
October 2021
According to an interim analysis of data from the main clinical trial of molnupiravir, it reduced by 48% the risk of hospitalization and/or death among high-risk patients with COVID-19 infection, caused by SARS-CoV-2 coronavirus and occurring with mild-to-moderate severity. When it comes to the risk of death, it has decreased by an impressive 94%.
↓
South Korea contracted a shipment of molnupiravir from Merck & Co. It turned out that one course of treatment costs $760.
↓
Merck & Co. licensed molnupiravir to the Medicines Patent Pool UNITAID (MMP), which aims to increase access to medicines for poor countries. The action by Merck & Co. is the first of its kind: until now, no pharmaceutical company has shared with MMP any medical technology aimed at combating COVID-19. All of the previous licensing developments that have been issued to MMP have involved drugs against HIV, hepatitis C, and tuberculosis.
November 2021
Bangladesh-based Beximco Pharmaceuticals offered the world’s first generic of molnupiravir. The drug is called Emorivir. A course of treatment with molnupiravir would cost $33, based on a price of 70 Bangladeshi taka per molnupiravir capsule.

↓
Bangladesh-based Eskayef Pharmaceuticals introduced its generic version of molnupiravir, Monuvir. One capsule of the drug costs 50 Bangladeshi taka, the equivalent of $23 for a course of treatment with molnupiravir.

↓
The U.S. government ordered another 1.4 million courses of molnupiravir from Merck and Co. at a cost of $1 billion. In the future, the United States could purchase more than 2 million additional courses of the drug.
↓
The Japanese government has contracted with Merck & Co. to supply 1.6 million courses of molnupiravir for which it is willing to pay $1.2 billion, the equivalent of $750 per course of treatment with molnupiravir.
↓
The United Kingdom is the first country in the world to approve Lagevrio (molnupiravir), an oral antiviral drug for the treatment of COVID-19 infection caused by the new coronavirus SARS-CoV-2 and presenting with mild-to-moderate severity. Lagevrio is approved for use in adult patients with at least one risk factor for developing severe illness.
↓
Sri Lanka approved the use of molnupiravir for the treatment of COVID-19.
↓
It became known that Sun Pharmaceutical Industries would produce a generic copy of molnupiravir under the brand name Molxvir.
↓
The European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) has recommended Lagevrio (molnupiravir) for treatment of adult patients with COVID-19 who do not require supplemental oxygen and who are at risk of developing severe disease. Molnupiravir is not yet approved in European Union countries, but the recommendations are needed to support national regulators, who can possibly make their own decisions about the use of the drug without waiting for a final pan-European EMA verdict.
↓
Updated data on the therapeutic efficacy of molnupiravir have shown that the drug performs significantly worse against COVID-19 than originally announced. Thus, molnupiravir reduced the risk of hospitalization and/or death by 30% and the risk of death by 89%. All of the above is true relative to the placebo.
↓
The FDA’s Advisory Committee voted to approve molnupiravir for outpatient covid treatment. However, the experts, first, still haven’t figured out why the effectiveness of molnupiravir has declined dramatically, and second, have urged some caution about the drug from a safety standpoint.
December 2021
In total, Merck & Co. has signed contracts with various countries for the supply of almost 8 million therapeutic courses of molnupiravir. In comparison, Pfizer has signed agreements for nearly 12 000 courses of Paxlovid.
↓
France has refused to treat COVID-19 patients with molnupiravir, which is already available through an early access program. The local regulator cited evidence of the availability of more effective drugs, including monoclonal antibodies. Again, an oral Paxlovid by Pfizer is coming, which is supposedly much more effective than molnupiravir. Earlier, France ordered 50 000 treatment courses of molnupiravir from Merck and Co. It seems that it will not have to pay for them.
Molnupiravir: Mechanism of Action
Oral molnupiravir (MK-4482, EIDD-2801) is an experimental drug compound developed at Emory University (USA) and licensed by Ridgeback Biotherapeutics. Molnupiravir was originally positioned as an anti-influenza drug.
Molnupiravir, being a prodrug of the synthetic nucleoside analogue β-D-N4-hydroxycytidine (NHC), acts by inhibiting RNA-dependent RNA polymerase (RdRp, RNA replicase), which causes RNA mutagenesis.
- The enzyme RdRp is critical to the life cycle of the virus. It catalyzes RNA replication — the synthesis of new RNAs complementary to the existing RNA matrix encoded in the virus genome. Problem-free RNA replication is necessary for further synthesis of viral components (structural and nonstructural proteins, genome) and virion assembly.
In the body, molnupiravir is converted to NHC (EIDD-1931), which is then phosphorylated by kinases to the active drug form, NHC-triphosphate (EIDD-1931-triphosphate). The latter functions as an alternative/competitive substrate for viral RdRp, which leads to the suppression of its normal functioning: RdRp begins generating mutant RNA copies of SARS-CoV-2 in which cytidine triphosphate or uridine triphosphate is replaced by NHC. The process of accumulation of multiple mutations in the viral genome, the number of which exceeds an acceptable threshold (the so-called viral error catastrophe), leads to a significant disruption or complete loss of the replication ability of the virus. Molnupiravir acts more as an electron donor than as an electron acceptor, and hence this reducing property contributes to the antiviral activity, as it affects the conditions necessary for viral infection.
Importantly, molnupiravir, according to in vitro studies and several clinical trials, maintains high antiviral activity against various variants of SARS-CoV-2 including the highly contagious Delta strain.
- The impressive effectiveness of molnupiravir determined its name, inspired by the hammer of the Scandinavian god Thor — Mjöllnir, a powerful and versatile weapon. Indeed, molnupiravir works equally well against all variants of SARS-CoV-2.
The activity of NHC has been studied on cell cultures infected with SARS-CoV-2. Thus, the EC50 (effective concentration of the drug required to suppress viral replication by 50%; the lower this figure, the more effective, that is, at lower concentrations, the drug compound works) fell within the range of 0.67–2.66 μmol for the A-549 cell line and 0.32–2.03 μmol for the Vero E6 cell line. NHC activity against SARS-CoV-2 variants was similar, with EC50 values of 1.59, 1.77, 1.32, and 1.68 μmol in the B.1.1.7 (Alpha), B.1351 (Beta), P.1 (Gamma), and B.1.617.2 (Delta) cell strains, respectively. No effect was observed on the antiviral activity of NHC in the presence of other drugs such as abacavir, hydroxychloroquine, lamivudine, nelfinavir, remdesivir, ribavirin, sofosbuvir, tenofovir, emtricitabine.
Molnupiravir: Market Outlook
Following the announcement of positive results from the clinical trial of molnupiravir against COVID-19, Merck & Co.’s share price immediately added 10%, the largest surge in its stocks in the past 12 years. This reflects Wall Street’s favorable sentiment: investors see commercial prospects and an optimistic future for molnupiravir.
Looking at the United States market as the most attractive for any pharmaceutical or biotech product (due to higher than high prices, which are not controlled in any way), molnupiravir could become the first oral drug for COVID-19 therapy.
- In some countries, including Russia, such oral anti-COVID-19 drugs as Arbidol (umifenovir) and favipiravir sold under the brands Areplivir, Avifavir, Avigan, Coronavir, Covidolek, FabiFlu, Favibirin, Favipira, Favipiravir have found clinical use. However, these cannot be positioned as drugs that are unequivocally effective against SARS-CoV-2 and COVID-19, since the conducted clinical trials either have not demonstrated proper and unconditional therapeutic efficacy or have serious methodological flaws.
The position of molnupiravir in terms of clinical trial results is still stronger. However, it would not be right to make too bright expectations until the respective results are published in a peer-reviewed medical journal, which would then undergo rigorous analysis by independent industry experts.
If molnupiravir proves to be highly effective against COVID-19, its developers will make billions of dollars. First, Veklury (remdesivir) promoted by Gilead Sciences is implemented in an intravenous formulation and is indicated for use only in hospital settings. Molnupiravir, in contrast, is made in an oral formulation (capsules), allowing it to be prescribed in the home setting.
Second, there are many effective monoclonal antibodies that are indicated for patients at risk for severe COVID-19, but all are made in intravenous formulations that require physician monitoring in an outpatient setting: bamlanivimab + etesevimab, casirivimab + imdevimab, sotrovimab, regdanvimab, tixagevimab + cilgavimab.
Third, despite the ongoing active vaccination of the world’s population, too many people refuse to be vaccinated against COVID-19, either because they do not trust the quality and effectiveness of the respective vaccines, or because they cite conspiracy theories, or because they belong to the category of people who are not able to be vaccinated for health reasons. Molnupiravir can be a conditional rescue when another case of COVID-19, already symptomatic, can be cured without making the disease severe, requiring costly hospitalization, and at the same time acquire appropriate post-infection immunity, even if not as strong as the post-vaccine immunity.
Fourth, if molnupiravir proves its potential in preventing COVID-19, it will further strengthen the confidence of patients and doctors in it. The situation is common: if a family (or household) member suddenly becomes ill with COVID-19, all other theoretically healthy and cohabiting people need to do is prescribe molnupiravir to ensure that COVID-19 is prevented.
From History of Molnupiravir Development
The history of molnupiravir began a few years before the pandemic of the new coronavirus SARS-CoV-2, and George Painter plays a key role in its development.
Painter, a virologist and chemist by education, has devoted his career to working on antiviral drugs, coauthoring several approved drugs for HIV and hepatitis B. In 2013, after decades in the industry, he joined as CEO of Drug Innovation Ventures at Emory (DRIVE), a nonprofit biotech venture owned by Emory University, and incidentally led the Emory Institute for Drug Development (EIDD). The goal of DRIVE and EIDD is to move candidate drugs from early-stage development and preclinical research into human clinical trials.

In 2014, Painter and colleagues at Emory University embarked on a project funded by the Defense Threat Reduction Agency (DTRA) at the U.S. Department of Defense (DoD) to find a drug compound that could fight the Venezuelan equine encephalitis virus (VEEV). During the Cold War, VEEV was studied by the U.S. and the Soviet Union as a potential biological weapon. VEEV, usually transmitted through mosquito bites, causes flu-like symptoms such as fever, headaches, and sometimes encephalitis, a brain swelling that can be fatal.
Scientists at Emory began selecting molecules, focusing on nucleosides (purine or pyrimidine bases attached to sugars), which are common motifs in antiviral compounds. It was necessary to find something active, with a high barrier to resistance and capable of penetrating the blood-brain barrier since VEEV is an encephalitic disease.
Screening efforts led to β-D-N4-hydroxycytidine, a low-molecular-weight compound called EIDD-1931. In the late 1970s, Russian and Polish scientists considered it as a possible drug to treat smallpox infection.
EIDD-1931 exists in two forms. In one form, the molecule mimics cytidine with a single bond between the carbon and the N-OH group. In the other form, which mimics uridine, EIDD-1931 includes an oxime with a double bond between the carbon and the N-OH group. These two forms are known as tautomers, and switching between them causes divergence during transcription. During viral RNA replication in the presence of EIDD-1931, the viral enzyme RNA-dependent RNA polymerase (RdRP) reads this compound as uridine instead of cytidine and therefore inserts adenosine where guanosine should be. The misreading creates a huge number of mutations in the viral genome: copies of viruses cannot function properly.

In experiments on mice infected with VEEV, the molecule EIDD-1931 was able to penetrate the brain and stop viral replication. And because the compound targets the enzyme RdRP, a characteristic of many viruses, Painter and his colleagues thought it could fight more than just VEEV.
Then, the researchers ran into a problem: EIDD-1931 worked quite well in mice and dogs, but not in monkeys. It was found that the 5′-OH in the molecule was phosphorylated, causing it to be trapped in the cells lining the monkeys’ intestines, meaning that the ability to fight the virus in infected cells was disabled.
To get around the problem, Emory’s team developed EIDD-2801 (a prodrug of EIDD-1931), an inactive molecule until it is metabolized. Using the ester group to block 5′-OH, where phosphorylation occurs, meant that enough of the molecule could enter the bloodstream, where enzymes would break down the ester and release the active form of the molecule.
Understanding that EIDD-2801 and its active metabolite, triphosphate of EIDD-1931, could effectively counteract other RNA viruses, Painter and collaborators set up tests against respiratory syncytial virus, norovirus, hepatitis C, Ebola, chikungunya and influenza A and B viruses. And it worked. For example, just three doses of EIDD-2801 saved ferrets (animals commonly used to study human respiratory viruses) infected with the “swine” flu A/H1N1 pandemic in 2009.
The success prompted Emory’s team to turn to researchers at Vanderbilt University and the University of North Carolina at Chapel Hill in 2015 to determine whether EIDD-1931 and EIDD-2801 were suitable for treating coronavirus infections. Colleagues were shocked after confirming that EIDD-1931 is as effective as remdesivir at killing SARS-CoV coronavirus, which causes severe acute respiratory syndrome, and MERS-CoV coronavirus, which causes Middle East respiratory syndrome.
In late 2019, Painter signed a contract with the U.S. National Institute of Allergy and Infectious Diseases (NIAID) to bring EIDD-2801 into phase 1 clinical trials against influenza. The plan was to submit an Investigational New Drug (IND) application to the U.S. Food and Drug Administration (FDA) and in the process find a partner to help with the clinical work.
Just as the team was thinking about their next steps, news reports emerged about the spread of an unknown virus in Wuhan, China. Remarkably, just in late 2019, Painter’s team published a paper demonstrating that EIDD-1931 effectively suppresses the replication of coronaviruses, with mutations of the latter having no way to counteract this molecule.
In early March 2020, the research team tested EIDD-1931 on human cells infected with the new coronavirus SARS-CoV-2. The compound was not only able to effectively kill the pathogen, but also demonstrated that it could eliminate remdesivir-resistant coronaviruses.
Work on bringing EIDD-2801 to clinical trials for the experimental treatment of SARS-CoV-2 was accelerated many times over. For example, the IND was prepared in 48 hours and then reviewed by FDA experts in just one week.
In March, DRIVE licensed EIDD-2801 to Ridgeback Biotherapeutics for human clinical trials. In April, the FDA and the UK Medicines and Healthcare products Regulatory Agency (MHRA) authorized the start of phase 1. In late May, Ridgeback transferred the license for EIDD-2801 to Merck & Co.
Despite very encouraging results from experiments on cell cultures and mice, it was clear that EIDD-2801 should be used as early as possible after the fact of SARS-CoV-2 infection. If you do it too late, it won’t work. Yes, EIDD-2801 will kill the virus regardless of the timing of the infection, but here it is appropriate to draw a comparison with a burning hand, which can be put out with a fire extinguisher, but it cannot be cured completely because the damage caused by fire is irreparable and there is no way to fix it.
Generally, the fact that EIDD-2801 is active against a wide range of viruses is extremely rare. Moreover, EIDD-2801 is characterized by a high barrier to resistance. The bottom line is that drugs can make viruses mutate rapidly so that the former ceases to act on the latter. In laboratory tests, whatever mutagenic efforts were used, EIDD-2801 worked equally effectively on both wild-type and mutant virus strains. Even if SARS-CoV-2 ever becomes resistant to EIDD-2801, it would likely result in a drastic reduction in its ability to replicate.
Extras
Prescribing Information
Lagevrio (molnupiravir): summary of product characteristics. [PDF]
Lagevrio (molnupiravir): patient information leaflet. [PDF]
FDA Antimicrobial Drugs Advisory Committee (ADAC) Meeting. November 30, 2021
Molnupiravir. FDA Introductory Remarks. [PDF]
Molnupiravir. FDA Briefing Information. [PDF]
Molnupiravir. Addendum to the FDA Briefing Information. [PDF]
Molnupiravir. Errata to the FDA Briefing Document. [PDF]
Molnupiravir. Merck Briefing Information. [PDF]
Molnupiravir. Addendum to the Merck Briefing Information. [PDF]
Molnupiravir. Merck Briefing Document. [PDF]
Scientific Publications
Molnupiravir for oral treatment of Covid-19 in nonhospitalized patients. N Engl J Med. 2021 Dec 16. [source]
Discovery, development, and patent trends on molnupiravir: a prospective oral treatment for COVID-19. Molecules 2021, 26(19), 5795. [source]
Molnupiravir promotes SARS-CoV-2 mutagenesis via the RNA template. J Biol Chem. 2021 Jul; 297(1): 100770. [source]
Mechanism of molnupiravir-induced SARS-CoV-2 mutagenesis. Nat Struct Mol Biol. 2021; 28(9): 740–746. [source]
Molnupiravir: coding for catastrophe. Nat Struct Mol Biol. 2021 Sep;28(9):706-708. [source]
Molnupiravir, an oral antiviral treatment for COVID-19. medRxiv. 2021 Jun 17;2021.06.17.21258639. [source]
Therapeutically administered ribonucleoside analogue MK-4482/EIDD-2801 blocks SARS-CoV-2 transmission in ferrets. Nat Microbiol. 2021 Jan;6(1):11-18. [source]
Molnupiravir maintains antiviral activity against SARS-CoV-2 variants in vitro and in early clinical studies. IDWeek 2021. [source]
Small-molecule antiviral β-d-N4-Hydroxycytidine inhibits a proofreading-intact coronavirus with a high genetic barrier to resistance. J Virol. 2019 Dec 15; 93(24): e01348-19. [source]