Highlights
Covovax/Nuvaxovid (NVX-CoV2373), developed by US-based Novavax, is a vaccine to protect against COVID-19 infection caused by the new coronavirus SARS-CoV-2.
Indonesia was the first country in the world to approve the use of Covovax/Nuvaxovid. It was then approved by the Philippines.
Production of the vaccine is being undertaken by the Serum Institute of India (SII), which is prepared to produce approximately 1 billion doses of Covovax/Nuvaxovid.
Novavax has already applied for registration of Covovax/Nuvaxovid in India, as well as for authorization by the World Health Organization (WHO). Applications for approval of the vaccine in the European Union, the United Kingdom, Canada, Australia, and New Zealand have been completed. Plans are underway to send applications for approval of Covovax/Nuvaxovid worldwide in the near future. By the end of the year, an application will be prepared for registration in the United States.
- On December 17, 2021, WHO included Covovax/Nuvaxovid in the list of vaccines recommended for use against SARS-CoV-2 coronavirus. Thus, the world’s main medical regulator has confirmed the quality, safety, and efficacy of Covovax/Nuvaxovid.
- On December 20, 2021, the European Medicines Agency (EMA) approved Covovax/Nuvaxovid for immunization of persons 18 years of age and older to prevent COVID-19 infection. The regulatory verdict is conditional, meaning the vaccine will need to undergo additional clinical evaluation to confirm its efficacy against COVID-19 in order to be fully approved. Covovax/Nuvaxovid is the fifth vaccine for COVID-19 to receive marketing authorization in the European Union; prior to that, vaccines developed by Pfizer/BioNTech, Moderna, AstraZeneca, and Johnson & Johnson’s Janssen were approved.
- Covovax/Nuvaxovid approved in India (Dec. 28, 2021), South Korea (Jan. 12, 2022), Australia (Jan. 19), New Zealand (Feb. 3), United Kingdom (Feb. 3), Singapore (Feb. 14), Canada (Feb. 17), Thailand (April 8), Switzerland (April 13), Japan (April 19), Taiwan (June 23).
- On July 13, 2022, the U.S. Food and Drug Administration (FDA) approved Novavax’s COVID-19 vaccine under its Emergency Use Authorization (EUA). The new vaccine is the fourth to be approved by the U.S. regulator, following vaccines by Pfizer/BioNTech, Moderna, and Janssen/Johnson & Johnson.
Covovax/Nuvaxovid Vaccine: Design and Production Features
Covovax, also known as Nuvaxovid and codenamed NVX-CoV2373, is a vaccine against SARS-CoV-2 coronavirus that includes full-length recombinant S protein trimers of the virus, stabilized in the “pre-fusion” conformation, derived from its original Wuhan-Hu-1 genetic sequence and assembled into nanoparticles. The saponin-based adjuvant Matrix-M is used; this immune stimulant is extracted from the inner bark of the Chilean soap bark tree (Quillaja saponaria).
The U.S. government has invested $1.6 billion to develop a commercial-scale production of NVX-CoV2373.
Covovax/Nuvaxovid is positioned equally as a protein subunit vaccine as a virus-like particle vaccine, although Novavax itself calls it a recombinant nanoparticle vaccine.
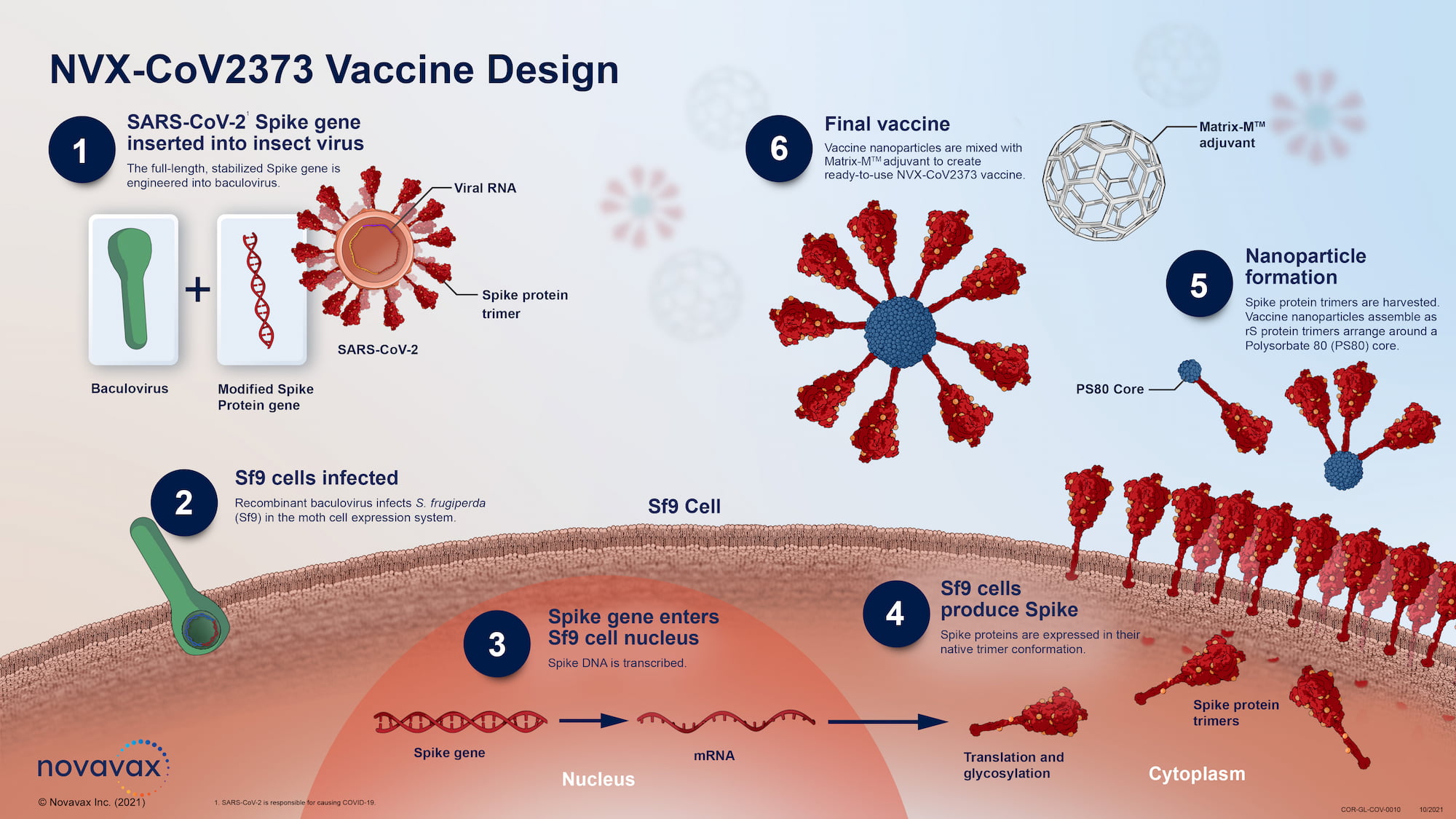

Covovax/Nuvaxovid is produced by creating a modified baculovirus containing the altered S protein gene of SARS-CoV-2. The modification is the inclusion of two proline amino acids to stabilize S protein in “pre-fusion” conformation. Baculovirus infects a culture of Sf9 moth cells, which produce S protein and express it on their cell membranes. S proteins separate and assemble into synthetic lipid nanoparticles about 50 nm in size, each carrying up to 14 S proteins.
- All enveloped viruses, such as coronaviruses, influenza virus or respiratory syncytial virus, require the fusion of the viral membrane and the host cell membrane in order to penetrate and infect the host cell. This process is facilitated by viral fusion proteins; by their own structural rearrangement from a metastable “pre-fusion” conformation to a highly stable “post-fusion” conformation. Viral fusion proteins, or fusogens, are the main targets of the protective reactions of neutralizing antibodies (they block the penetration of the virus into the cell), and therefore they are excellent candidates for subunit vaccines, that is, containing not the entire pathogen (inactivated or attenuated), but only part of it — one or more surface immunogenic proteins. However, the inherent unstable nature of fusogens poses a serious obstacle to the development of an effective vaccine.
- For vaccines, the “pre-fusion” fusogen is preferred. It is the conformation that contains important epitopes that are not present in the “post-fusion” conformation and that induces the production of broadly cross-reactive and highly neutralizing antibodies as part of a strong immune response. Traditional approaches of recombinant expression of viral fusion proteins usually result in premature trigger effects and a conformational shift toward the “post-fusion” structure.
Covovax/Nuvaxovid is stable at 2–8 °C, meaning it can be transported and stored using the available cold chain, which is important in the face of the COVID-19 pandemic and the still-existing vaccine shortage.
The advantage of Covovax/Nuvaxovid is that it addresses a traditional adjuvant platform based on protein subunits, and this may well reduce the degree of anti-vax sentiment along with prolonging the duration of the immune response.
Covovax/Nuvaxovid Vaccine: Protective Efficacy
British Evaluation
The NCT04583995 phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled just over 14,000 UK residents aged 18–84 years without confirmed COVID-19 who were given two doses of NVX-CoV2373 or placebo — 21 days apart.
Among the main characteristics of the participants: median age 56 years; 27.9% were 65 years of age or older; and 44.6% had a severe risk factor for COVID-19 (chronic respiratory, cardiac, renal, neurological, or immunodeficiency conditions, obesity).
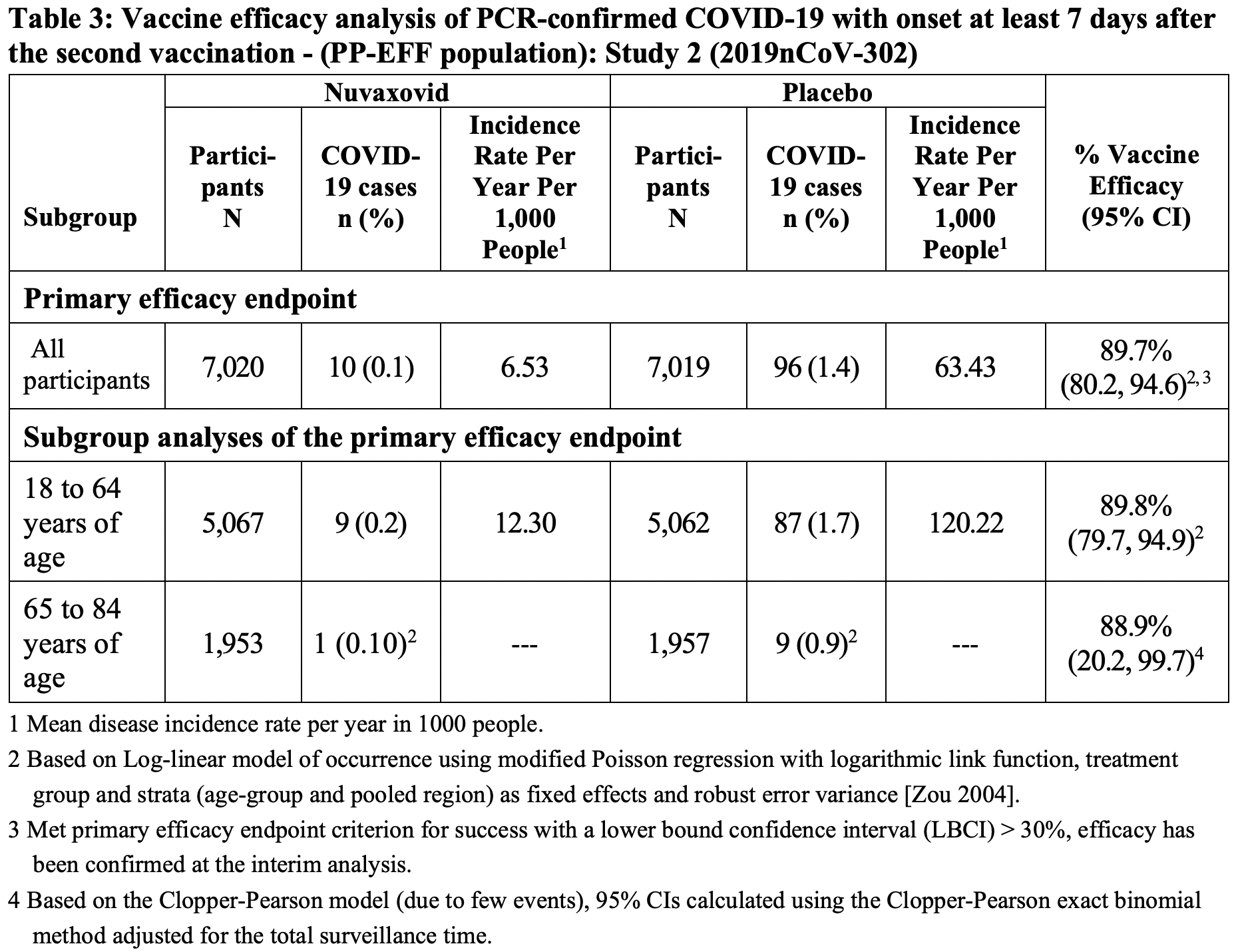
The primary endpoint was a proportion of subjects with virologically confirmed symptomatic COVID-19 infection manifesting at least 7 days after the second dose.
10 people in the vaccine group and 96 in the placebo group experienced COVID-19 infection. The final protective efficacy of Covovax/Nuvaxovid was 89.7% (95% CI: 80.2–94.6).
Of the 10 COVID-19 cases in the vaccine group, 8 were caused by the Alpha variant (B.1.1.7) of SARS-CoV-2, 1 by a non-Alpha variant, and 1 by a variant that could not be identified.
No cases of hospitalization or death were reported in the vaccine group.
5 cases of severe COVID-19 were reported, all in the placebo group.
In the age subgroup of subjects younger than 65 years old, the protective efficacy of Covovax/Nuvaxovid was 89.8% (95% CI: 79.7–95.5), in subjects aged 65 years and older, it was 88.9% (95% CI: 20.2–99.7). The efficacy was 90.9% (95% CI: 70.4–97.2) in the presence of a risk factor for COVID-19 with a severe course, and 89.1% (95% CI: 76.2–95.0) in its absence.
The protective efficacy against SARS-CoV-2 Alpha variant was 86.3% (95% CI: 71.3–93.5), and against the non-Alpha variant was 96.4% (95% CI: 73.8–99.4).
The protective efficacy after 14 days after the first dose of Covovax/Nuvaxovid came out to 83.4% (95% CI: 73.6–89.5).
American Evaluation
The PREVENT-19 (NCT04611802) phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled 25,500 US and Mexican residents aged 18 years or older without confirmed COVID-19 who received two doses of NVX-CoV2373 or placebo — 21 days apart.
Among the main characteristics of participants: median age 47 years; 11.8% were 65 years of age or older; and 47.3% had a risk factor for severe COVID-19 infection.
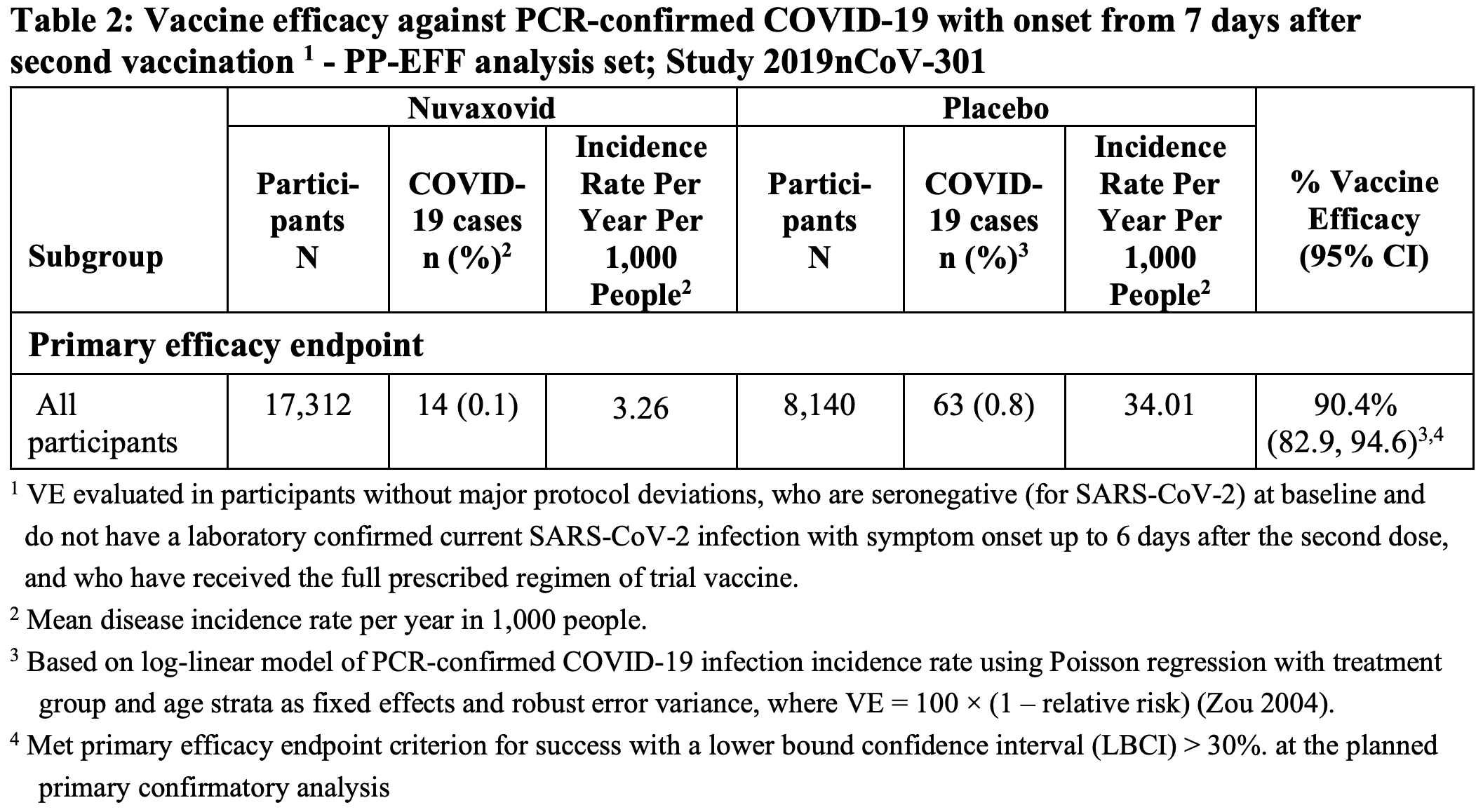
The primary endpoint was the proportion of subjects with virologically confirmed symptomatic COVID-19 infection manifesting at least 7 days after the second dose.
14 people in the vaccine group and 63 in the placebo group experienced COVID-19 infection. The final protective efficacy of Covovax/Nuvaxovid was 90.4% (95% CI: 82.9–94.6).
All COVID-19 cases in the vaccine group were of mild severity. The efficacy of Covovax/Nuvaxovid in preventing the development of COVID-19 in moderate-to-severe form reached 100% (95% CI: 87–100) and in severe form 100% (95% CI: 34.6–100).
In the presence of a risk factor for developing COVID-19 with a severe course, the efficacy of Covovax/Nuvaxovid protection was 91.0% (95% CI: 83.6–95.0).
Beta Variant
The NCT04533399 phase 2a/2b (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled 2770 South Africa residents aged 18 years or older without confirmed COVID-19 who received two doses of NVX-CoV2373 or placebo — 21 days apart.
Participants could have been HIV infected, then they had to be on stable, highly active antiretroviral therapy (HAART), and their viral load had to be less than 1000 copies/mL; 5.5% of the volunteers in the study were HIV infected.
The trial tested the Covovax/Nuvaxovid vaccine at a time when South Africa was dominated by the Beta (B.1.351) variant of SARS-CoV-2.
51 people in the vaccine group and 96 in the placebo group experienced COVID-19 infection. The final protective efficacy of Covovax/Nuvaxovid was 48.6% (95% ДИ: 28.4–63.1).
Omicron Variant
For successful control of the Omicron variant and its subvariants, Covovax/Nuvaxovid vaccine should be used in a booster regimen 6 months after the main vaccination. This follows from tests of its neutralizing activity.
Covovax/Nuvaxovid Vaccine: Safety
British Evaluation
Local adverse events occurred more frequently in the vaccine group than in the placebo group: after the first dose, in 57.6% of participants — versus 17.9%; after the second dose, in 79.6% — vs. 16.4%. The most common adverse events were soreness and pain at the Covovax/Nuvaxovid injection site: respectively, in 53.3% and 29.3% of subjects after the first dose and in 76.4% and 51.2% after the second dose. In most cases, these adverse reactions were mild-to-moderate in severity and disappeared within two to three days.
Systemic adverse events were more common in the vaccine group than in the placebo group: 45.7% of participants after the first dose — vs. 36.3%; 64.0% — vs. 30.0% after the second dose. Among the most common systemic adverse reactions in response to Covovax/Nuvaxovid administration were headache, muscle pain, and fatigue in 24.5%, 21.4%, and 19.4% after the first dose and in 40.0%, 40.3%, and 40.3% after the second dose. Most events were characterized by mild-to-moderate severity and passed within two days.
American Evaluation
Local and systemic adverse events that were mostly mild to moderate in severity and resolved in less than two days were more common in the Covovax/Nuvaxovid group than in the placebo group, and more common after the second dose.
The most common adverse reactions to the vaccine were soreness and pain at the injection site, headache, muscle pain, fatigue, and malaise.
Extras
Covovax/Nuvaxovid. Prescribing information. U.S. [PDF]
Covovax/Nuvaxovid. Prescribing information. Europe. [PDF]
Safety and efficacy of NVX-CoV2373 Covid-19 vaccine. N Engl J Med. 2021 Sep 23;385(13):1172-1183. [source]
Efficacy and safety of NVX-CoV2373 in adults in the United States and Mexico. medRxiv, October 10, 2021. [source]
Efficacy of NVX-CoV2373 Covid-19 vaccine against the B.1.351 variant. N Engl J Med. 2021 May 20;384(20):1899-1909. [source]