Monkeypox Prevention
General Information
The smallpox vaccine prevents infection with monkeypox and alleviates its symptoms.
A number of countries have strategic stocks of smallpox vaccines. Even if they are not available, mass production can be established without much trouble.
Smallpox vaccines are characterized by a number of adverse reactions, generally similar to those of other vaccines. However, some of the adverse events, although very rare, are serious and sometimes fatal.
Denmark’s Bavarian Nordic has developed a third-generation smallpox vaccine Jynneos/Imvanex/Imvamune, which, firstly, is the first and so far the only vaccine approved against monkeypox and, secondly, has a much better safety profile than previous generations of smallpox vaccines.
OrtopoxVac, the world’s first officially approved fourth-generation smallpox vaccine, will soon be licensed in Russia. The powerful and maximally safe smallpox vaccine was developed by the State Research Center of Virology and Biotechnology VECTOR.
In case of contact with an infected person it makes sense to consider post-exposure smallpox vaccination as early as possible.
Active Immunization for Monkeypox
Persons who have had smallpox develop long-term and often lifelong immunity to reinfection, which, however, sometimes occurs, although their frequency does not exceed 1 per 1000 for 15–20 years. [1]
Smallpox vaccination confers persistent immunity with a protective efficacy of 80%–95%. Those who need it are advised to revaccinate every 10 years, although protection can last substantially longer. [2]
Pre-immunization with smallpox vaccine reliably prevents infection with monkeypox and significantly alleviates clinical symptoms of the disease if it does manifest. This is possible due to the formation of persistent and high-quality cross-immunity organized by all orthopoxviruses. Simultaneous epidemics of smallpox and monkeypox have never been reported. [3]
According to data collected from 1980–1984 in the Democratic Republic of Congo (DRC), which is enzootic for monkeypox, smallpox vaccination provides 85% protection against monkeypox. [4]
Trend analysis of monkeypox incidence in the DRC, showed that those vaccinated against smallpox had a 5.2 times lower risk of contracting monkeypox than unvaccinated individuals. A comparison of active surveillance data in the 1980s with data from 2006–2007 found a 20-fold increase in the incidence of monkeypox due to the cessation of the mass smallpox vaccination campaign. [5]
During the 2003 monkeypox outbreak in the United States, eight cases of people previously vaccinated with smallpox 13–38 years ago were found to be infected, and three were asymptomatic. Despite the modest sample size, it can be assumed that smallpox vaccination, even given in the distant past, ensures that about half of those vaccinated develop very long-lasting cross-immunity against monkeypox. [6]
Individuals who have been exposed to monkeypox virus and have not received smallpox vaccine within the past 3 years should explore vaccination. [7]
Monkeypox Post-exposure Prophylaxis
Post-exposure prophylaxis with a third-generation (live attenuated) smallpox vaccine should be considered for some individuals after exposure to monkeypox in addition to surveillance and isolation. [1]
- Post-exposure prophylaxis of monkeypox refers to the organization of protective measures after the suspected fact of possible infection: for example, direct contact with a diseased person or contaminated objects in the same room as the diseased person.
The antibody response after primary smallpox vaccination usually occurs 4–8 days earlier than after smallpox infection. [2] Thus, primary vaccination given even after infection can alter the course of the disease or interrupt it. There is a possibility of strong protection against the development of smallpox when vaccinated 3–4 days after infection and at least partial protection against death when vaccinated 4–5 days after infection. [3] [4] [5] [6] [7]
In view of the above, post-exposure prophylaxis of monkeypox should be given as early as possible. If smallpox vaccination is given within 4 days of exposure, there is hope of preventing the development of the disease. If it is done between 4 and 14 days, it should be expected to reduce the severity of the course of the disease, but not to prevent it. [8]
During the 2013 monkeypox outbreak in the United States, smallpox vaccination was provided to a limited number of individuals exposed to the virus and recommendations were made for pre-exposure vaccination of those involved in the outbreak investigation and medical personnel who came in contact with the ill. To this end, 7 individuals received the smallpox vaccine pre-exposure and 23 individuals post-exposure, with one case developing laboratory-confirmed monkeypox. [9]
The role of post-exposure prophylaxis of monkeypox with vaccinia immune globulin (VIG) remains unclear. VIG is a hyperimmune product derived from the pooled plasma of smallpox vaccinees with a high antibody titer against Vaccinia virus. However, such prophylaxis may be considered for use in persons with severe immunodeficiency of T-cell function, since smallpox vaccination is contraindicated for them. [10]
Smallpox Vaccines
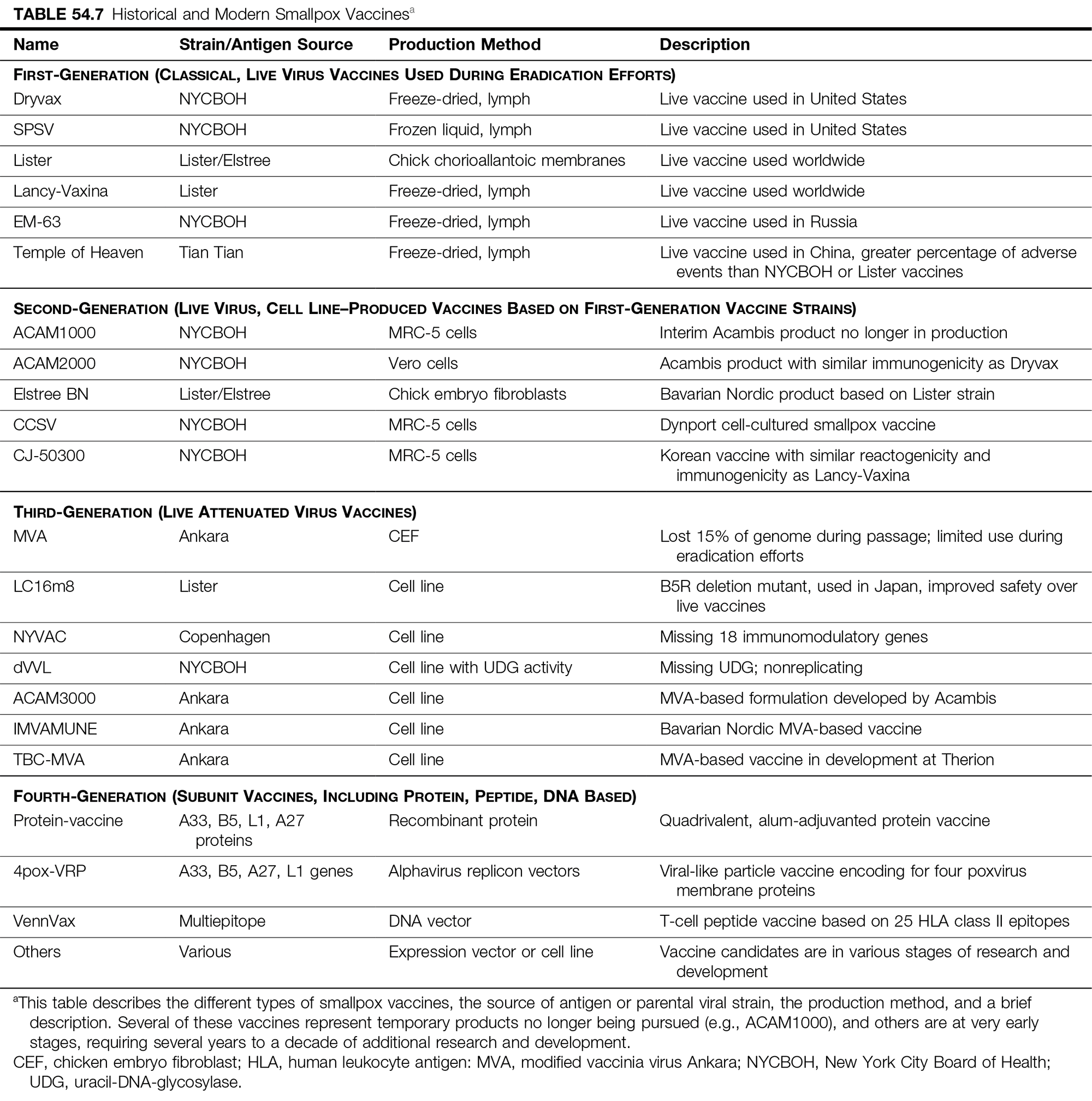
There are four generations of smallpox vaccines. [1]
The first generation, represented by the classical vaccines based on the live Vaccinia virus (VACV), was used during the effort to eradicate smallpox from the planet. Such vaccines included Dryvax, SPSV, Lister/Elstree, Lancy-Vaxina, EM-63, and Temple of Heaven.
The second generation of smallpox vaccines, building on and completely replacing the first generation, is turning to the production of live Vaccinia virus on cell lines. These include ACAM1000, ACAM2000, Elstree BN, CCSV, and CJ-50300.
The third generation of smallpox vaccines have relied on live attenuated (weakened) Vaccinia virus. They are particularly suitable for immunocompromised individuals and therefore at increased risk of progressive vaccinia, as well as those with severe eczema or exfoliative skin disease. The representatives are as follows: MVA, LC16m8, NYVAC, dVVL, ACAM3000, Jynneos/Imvanex/Imvamune, and TBC-MVA.
The fourth generation of smallpox vaccines currently in development offers hope for modern vaccines (mainly subunit vaccines) that are as safe and effective as possible.
Even after smallpox has been completely eradicated from the planet, states still accumulate smallpox vaccines in their strategic stockpiles. They are needed to combat possible outbreaks of infections caused by orthopoxiruses, including the monkeypox virus. [2]
According to a 2013 report, the World Health Organization (WHO) headquarter in Switzerland holds 2.7 million doses of smallpox vaccines (2.4 million doses of vaccines used in the smallpox eradication campaign and 300,000 doses of ACAM2000). There are also commitments from donor countries for an additional 32 million doses of vaccines (ACAM2000, LC16m8, Jynneos/Imvanex/Imvamune). Other countries have their own stockpiles, which could range from 570 million to 720 million doses worldwide. Vaccine manufacturers have a production capacity of 255 million doses per year, although some production lines would need to be reactivated to do so. [3]
How much and what kind of smallpox vaccines are available in Europe remains unknown. It is claimed that 1.4 million doses of Jynneos/Imvanex/Imvamune have been collected in the Danish storage facility.
The U.S. has a stockpile of more than 100 million doses of ACAM2000, a live replication-competent vaccine based on the NYCBOH strain of Vaccinia virus, and continues to stockpile Jynneos/Imvanex/Imvamune vaccine, with over 1000 doses already accumulated.
Smallpox vaccine ACAM2000, which was developed by UK-based Acambis and which replaced the Dryvax in February 2008, is an improved version of the latter, which is no longer in production. ACAM2000 is produced by cloning Dryvax using the plaque purification (sequential passage of the virus to a single genetic clone), is grown not on calf lymph but in African green monkey kidney cells (Vero), and is tested to be free of foreign agents. [4] ACAM2000 was produced by Sanofi until it was sold to Emergent BioSolutions in early October 2017 for $125 million.
- ACAM2000. Prescribing information. U.S. [PDF]
Russia has three vaccines against smallpox: Microgen produces the live smallpox vaccine and the inactivated smallpox vaccine OspaVir, both based on the Lister/Elstree strain, and the 48th Central Research Institute of the Ministry of Defense has developed TEOVak, an oral, tablet-based live smallpox vaccine based on the B-51 strain.
An in-depth understanding of poxviruses immunology, identification of T- and B-cell epitopes, and advances in reverse immunology have provided the global pharma industry with an opportunity to develop a number of effective smallpox vaccines based on alternative biotechnological approaches. These fourth-generation vaccines, being mainly subunit (containing individual antigenic parts of the virus), are characterized by a number of notable advantages, such as clearly defined composition, absence of viral and/or bacterial contaminants, easy adaptation to multivalent implementation, fast and economically justified production, increased efficacy, improved safety profile.
A promising direction in improving the effectiveness of smallpox vaccination, along with proper safety, is the strategy of heterologous prime-boost immunization, where a subunit vaccine (fourth generation) is used for initial stimulation of the immune system, and a vaccine based on the attenuated Vaccinia virus (third generation) is used to consolidate the development of immunity. [5]
Identification of target antigens for a subunit smallpox vaccine is complicated by the fact that poxviruses encode hundreds of proteins, and their complex life cycle is represented by two infectious forms, intracellular mature virion (IMV) and extracellular enveloped virion (EEV). A quadrivalent vaccine containing recombinant ectodomains of Vaccinia virus membrane proteins (L1R and A27L proteins from MV and A33R and B5R proteins from EV) and backed with adjuvant aluminum hydroxide and cytosine–phosphoguanine (CpG) was developed. [6]
Experiments with 4pox DNA vaccines encoding the genes of the above-mentioned Vaccinia virus proteins, as well as DNA vaccines carrying individual genes, have been successfully carried out. In addition to smallpox, they also protect against monkeypox. [7] [8] [9]
A low-cost subunit smallpox vaccine with only the B5R protein produced by the plants Australian tobacco (Nicotiana benthamiana) and Swiss chard (Beta vulgaris var. cicla) has been demonstrated. [10]
VennVax, invented by EpiVax, delivers a DNA plasmid encoding genes for multiple highly conserved and immunogenic T-cell epitopes of Variola major and Vaccinia virus to the body in order to build robust T cell–mediated immunity. Notably, the vaccine does not induce the production of neutralizing antibodies. Given that 48 of the 50 epitopes in VennVax are more than 90% identical to those in Monkeypox virus, and 68% of the epitopes are completely identical, the vaccine is also suitable for the prevention of monkeypox. [11]
An intranasal mucosal vaccine containing Vaccinia virus killed by an antimicrobial nanoemulsion of soybean oil and detergent is of interest. [12]
In Russia, the State Research Center of Virology and Biotechnology VECTOR has developed two fourth-generation smallpox vaccines: a pentavalent DNA vaccine based on recombinant plasmids containing the genes of five virion proteins of Variola major (A30L, F8L, and M1R from IMV, A36R and B7R from EEV), and a live highly attenuated VACdelta6 (VACΔ6) based on the Lister/Elstree strain of Vaccinia virus with targeted knockdown of six of its genes (C3L, N1L, J2R, A35R, A56R, and B8R) to reduce reactogenicity and neurovirulence and increase immunogenicity. [13] [14] [15] [16] [17] [18]
- On May 18, 2022, VECTOR submitted an application to the Russian Ministry of Health for authorization of the VACdelta6 vaccine, brand-named OrtopoxVac.
Smallpox Vaccines Safety
Prior to the Smallpox Eradication Program (SEP), which involved mandatory vaccination of everyone in the world, several strains of Vaccinia virus were in use. In 1967, the WHO Smallpox Eradication Unit, which surveyed 59 laboratories producing smallpox vaccine, found impressive heterogeneity in their production. Thus, 39 laboratories had grown the virus on calf skin, 12 on sheep skin, 6 on buffalo skin, 3 on chorioallantoic membrane of the chicken embryo, and 2 in tissue culture of bovine embryonic fibroblasts. [1]
Among the vaccinia strains were used Lister/Elstree strain (in 39% of laboratories), New York City Board of Health (NYCBOH) strain (12%), Paris strain (12%), the remaining laboratories (37%) exploited various other strains, including those poorly characterized or representing a mixture of Vaccinia virus and Cowpox virus. The biological properties of a particular strain depended on the method of passage, and yet the vast majority of these heterogeneous vaccines had adequate clinical efficacy against smallpox, particularly Variola major.
Nevertheless, quality control, safety, and supply control were long overdue, since the vaccines distributed did not always meet requirements for efficacy, microbial contamination, and stability. Some of the strains used were characterized by an increased incidence of postvaccinal encephalitis. Therefore, in 1963 WHO established criteria and regulations for the production of smallpox vaccines, reducing the number of Vaccinia virus derivatives used to three strains: Lister/Elstree, EM-63 (Moscow Research Institute of Viral Preparations, Russia), and NYCBOH. [2]
The three specified vaccinia strains are considered equivalent in the task of protection against smallpox during outbreaks and provide some level of post-exposure protection when administered within three to four days of infection. [3] Although immunizing agents are highly effective, each of these vaccines can cause serious adverse events. [4] [5] [6] [7] [8]
The smallpox vaccines currently held in the global stockpile are derived from these historical vaccinia strains. In animal models, the strains differ in their pathogenicity, [9] [10] and although a statistical correlation with adverse events has never been proven, differences in incidence have still been observed in humans with different strains. [11] [12] Differences in the safety profiles of different smallpox vaccines have been reflected in vaccination policies. In the late 1950s, early infant vaccination was replaced by vaccination after one year of age, which significantly reduced the number of serious adverse complications.
The most common adverse events after a smallpox vaccine are similar to those occurring with other vaccines: pain at the vaccination site, muscle soreness, fatigue, slight fever, and headache. A specific reaction is lymphadenopathy (enlarged lymph nodes).
Serious and/or severe adverse events associated with smallpox vaccines are as follows: myocarditis and/or pericarditis, encephalitis, encephalomyelitis, encephalopathy, progressive vaccinia (vaccinia necrosum), generalized vaccinia, severe vaccinial skin infections, erythema multiforme major (including Stevens–Johnson syndrome), eczema vaccinatum, blindness, and fetal death in pregnant women.
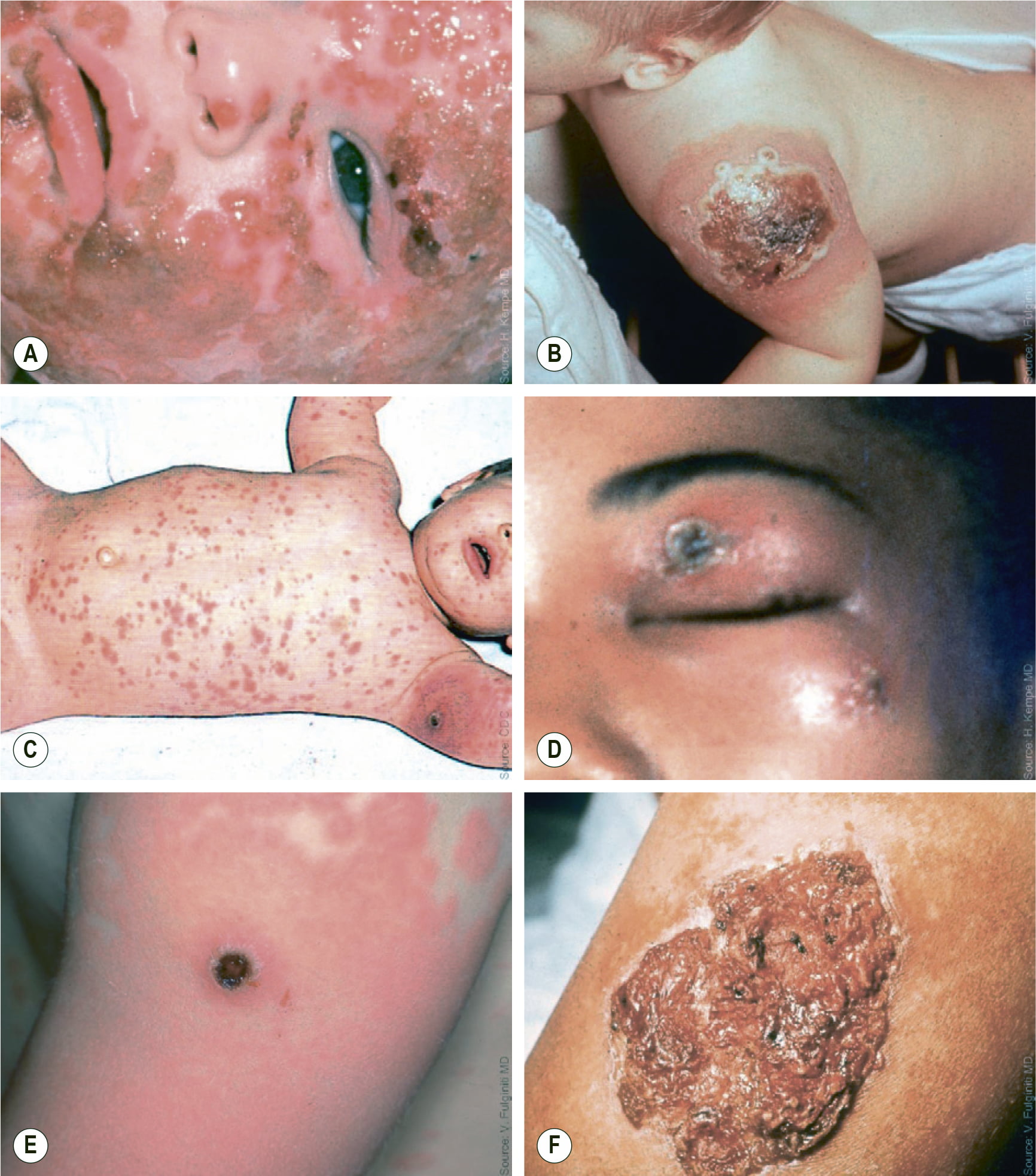
Historically, for every 1 million people who received the primary smallpox vaccination, there were somewhere between 5 and 10 people with adverse events serious enough to require hospitalization and one or two deaths. Absent the threat of contracting smallpox (or other orthopoxvirus), these risks are unnecessary. But they pale in comparison to those encountered during the smallpox epidemic. Its outbreak, with 1 million cases in the unvaccinated population, resulted in hundreds of thousands of deaths and long-term consequences (blindness, limb deformities, facial scarring, skin depigmentation) in most survivors.
In general, the exact safety profile of any smallpox vaccine remains uncertain because of a number of population issues, such as the prevalence of risk-predisposing diseases (atopic dermatitis, immunosuppression), the vaccinia strain, the method used for vaccination, environmental risk factors, and the general health of those who are currently immunologically naïve to smallpox vaccine.
These problems can change the frequency of adverse events predicted from historical data. [12] [13] [14] [15] For example, experience with the December 2002 smallpox vaccination campaign introduced in the United States military showed that the frequency of most adverse events was lower than expected. [14] [16]
However, myopericarditis occurred more frequently than suggested by historical data associated with age. [14] [15] [16] [17] [18] It could not be clarified whether age differences play a role in the risk of myopericarditis: The first smallpox vaccination was usually given to children (under 5 years of age), in the above campaign adults (over 18 years) were vaccinated. [15] [17] [19] [20] [21] Clinical trials of ACAM2000 vaccine have not definitively concluded whether this serious adverse event is more troublesome with its use.
Vaccinia strains derived from NYCBOH, when compared with other replicating strains, have historically been associated with less pathogenicity, and their safety profile is characterized by fewer adverse events, such as death from postvaccinal encephalitis (PVE) or permanent neurological disability caused by it. [22] Because PVE is a complication not related to excessive viral replication, it can result from immunization with the Jynneos/Imvanex/Imvamune vaccine. A review of experience with several different vaccinia strains showed that moderate-to-high pathogenic strains (Lister/Elstree and Ikeda) caused more adverse neurological events than low pathogenic strains (LC16m8, CV-I, and EM-63), despite equivalent skin-take rates and seroconversion. [22] [23]
Although this secondary level of evidence suggests that the less pathogenic strains of Vaccinia virus are characterized by increased safety without reduced efficacy, the incidence of serious adverse events (especially PVE) was too low to prove statistically significant differences between strains. Unequivocal statements would require clinical trials of different smallpox vaccines on millions of recipients.
Attenuated smallpox vaccines, which are safer, appeared at least in 1931, when a researcher at the Rockefeller Institute (New York, USA) described a serial passaging of the NYCBOH strain in chicken embryo cells. [24] Subsequently, two strains, CVI-78 and CV-II, the latter of which underwent a total of 235 passages on chicken embryo explants, demonstrated their effectiveness in intradermal inoculation with fewer adverse events. [25]
The attenuated CV-II–based smallpox vaccine was then tested on 60,000 Netherlands Army recruits. Although it had lower local and systemic reactogenicity compared with other replicating vaccines, the resulting neutralizing antibody titer was lower compared with the group inoculated with the Lister/Elstree calf lymph–based smallpox vaccine. [26]
In the early 1970s, the U.S. National Institute of Allergy and Infectious Diseases (NIAID) “resurrected” attenuated CVI-78 by comparing four smallpox vaccines: NYCBOH from calf lymph, NYCBOH from chicken embryos, Lister/Elstree from sheep skin, and CVI-78 from chicken embryos. As a result, induction of neutralizing antibody titers to CVI-78 was significantly lower, and, upon standard challenge vaccination (revaccination), the CVI-78 recipients had more frequent primary skin reactions, which is an indication of a lack of protective immunity. [27] [28] [29]
Testing in humans of other attenuated strains, including temperature-sensitive (LC16m8) derivatives of Darian and G-9, an attenuated variant of the highly pathogenic Temple of Heaven strain, showed an improved immune response compared to CVI-I. Detailed results, however, have not been published.
Monkeypox Vaccines
Currently, the only officially approved preventive protection against monkeypox in adults is a vaccine developed by Denmark’s Bavarian Nordic.
The vaccine, called Jynneos, was approved by the U.S. Food and Drug Administration (FDA) in late September 2019. Jynneos is also approved for smallpox vaccination.
Prior to that, in late July 2013 and late November 2013, Bavarian Nordic brought its vaccine to markets in Europe and Canada, where it was approved only against adult smallpox infection and was named Imvanex and Imvamune, respectively.
- However, Imvanex has been successfully used off-label to protect against monkeypox: In 2018, more than 200 people in the U.K. were vaccinated after imported infection was detected.
- In mid-November 2020, Imvanex expanded its range of indications to include prevention of monkeypox and other related orthopoxviruses.
Jynneos/Imvanex/Imvamune, which is an attenuated live non-replicating MVA-BN virus–based vaccine that is administered subcutaneously twice at 4-week intervals, induces strong humoral and cellular immune responses to orthopoxviruses. A booster dose of the vaccine every 2 years is thought to provide sufficient neutralizing antibodies.
- Modified vaccinia Ankara (MVA) virus is a highly attenuated strain of Vaccinia virus developed in Germany (between 1953 and 1968) by 570 serial passages in primary chicken embryo fibroblasts (CEF) of the Chorioallantois vaccinia virus Ankara (CVA) strain derived from from pox skin lesions after intradermal inoculation of calves and donkeys and maintained by the Turkish Vaccine Institute in Ankara. MVA has been used to protect livestock against orthopoxviruses. Since MVA lost approximately 10% of the CVA genome, it lost its ability to replicate effectively in primate cells, thereby negating the risks of serious and severe side effects. Bavarian Nordic performed additional attenuation, obtaining an even more attenuated MVA-BM virus while maintaining the proper level of immunogenicity. [1] [2] [3] [4] [5] [6] [7]
The efficacy of Jynneos/Imvanex/Imvamune against smallpox was predicted by comparing its immunogenicity with that of the smallpox vaccine ACAM2000 by Emergent BioSolutions.
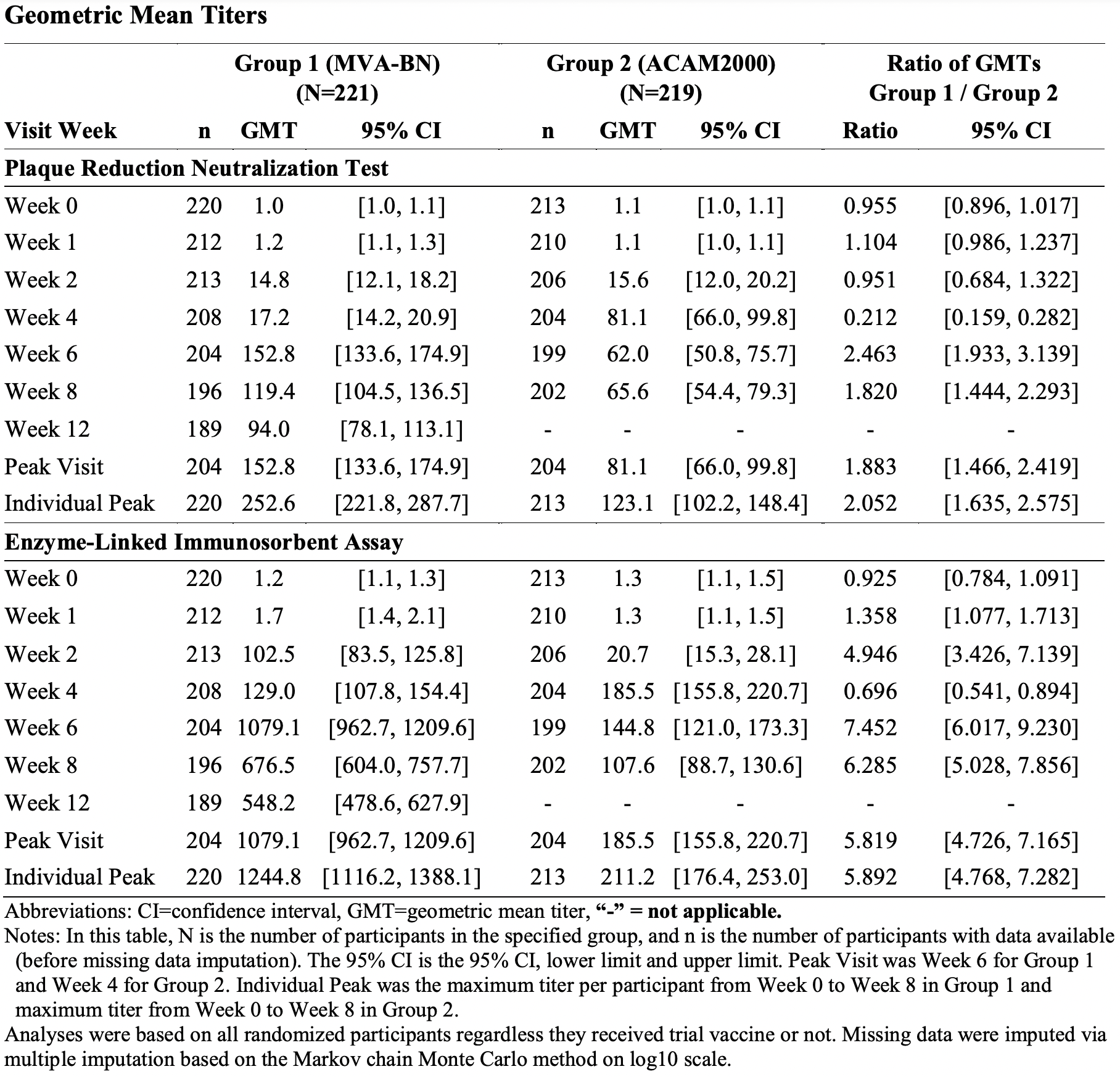
A clinical trial NCT01913353 phase 3 (randomized, open-label) among previously unvaccinated U.S. military adults (n=433) who received either two subcutaneous doses of Jynneos/Imvanex/Imvamune 28 days apart and then one percutaneous dose of ACAM2000, or the latter alone, found that the immune response in the first group of subjects was noninferior than in the second group when comparing the geometric mean titer of neutralizing antibodies assessed by the plaque reduction neutralization test (PRNT) after 2 and 4 weeks for the compared vaccines, respectively. [8]
The efficacy of Jynneos/Imvanex/Imvamune against monkeypox was predicted based on its immunogenicity in the above clinical trial and based on several animal studies. The vaccine allowed 80%–100% of cynomolgus macaques (Macaca fascicularis) not to die — versus 0%–40% in the placebo group.
Jynneos/Imvanex/Imvamune is characterized by acceptable tolerability. Overall, the safety profile of the vaccine is significantly better than that of ACAM2000. The most common adverse events were headache (in 16% of subjects), myalgia (14%), and lymphadenopathy (9%), whereas participants in the ACAM2000 group experienced lymphadenopathy (51%), headache (38%), myalgia (36%), and contact dermatitis (23%). Severe adverse events were reported in 4% and 30% of subjects, respectively.
Since MVA-BN does not replicate in human cells, no lifelong mark remains on the skin at the Jynneos/Imvanex/Imvamune injection site, characteristic of all smallpox vaccines.
- Jynneos. Prescribing information. U.S. [PDF]
- Imvanex. Prescribing information. Europe. [PDF]
- Imvamune. Prescribing information. Canada. [PDF]
Vaccinia Immune Globulin (VIG)
In 1960, vaccinia immune globulin (VIG), a hyperimmune product derived from the pooled plasma of smallpox vaccinees with a high antibody titer against Vaccinia virus, was proposed for the treatment of severe infections caused by the smallpox vaccination. [1] [2]
There have been no rigorously controlled trials of VIG to treat smallpox or vaccinia (complications of smallpox vaccination). Nevertheless, a reduction in the incidence of smallpox among close contacts of patients by about a quarter compared to a control group has been reported. [3] [4] [5] [6]
With the advent of more effective antiviral drugs, there appears to be no place for VIG in either the prevention or treatment of smallpox. That said, VIG continues to be used to treat adverse events after smallpox vaccination: Efficacy is claimed for eczema vaccinatum and some forms of progressive vaccinia, but not for accidental smallpox vaccine implantation or benign maculopapular rashes.
Thus, before the introduction of VIG into clinical practice, progressive vaccinia was always fatal, [1] afterwards, the case fatality rate (CFR) dropped to 25%–50%, although the data may be distorted because other measures, such as antiviral agents, blood transfusions from recently vaccinated donors, surgical debridement, were often taken simultaneously. [7]
The CFR in severe eczema vaccinatum was 8%–30% before the introduction of VIG, [1] [8] afterwards it dropped to less than 1%. [9]
VIG is contraindicated in patients in whom ocular vaccinia is complicated by keratitis. In rabbits, such therapy caused corneal scarring, presumably due to precipitation of antigen–antibody complexes. [10]