Monkeypox Treatment
General Information
Most patients with monkeypox have a mild form of the disease and recover on their own without any medical intervention. [1] [2] [3]
Treatment is mainly symptomatic and supportive (reduction of fever, decrease of itching, prevention of dehydration), including prevention and treatment of secondary bacterial infections.
In case of risk factors for dehydration (nausea, vomiting, dysphagia), a short hospital stay for intravenous hydration may be necessary.
Severely ill patients require supportive care until the patient has recovered from the infection. Antiviral medications may be needed for these patients.
Persons at increased risk of severe monkeypox may require hospitalization and/or antiviral medications. High-risk categories include infants and young children, pregnant women, the elderly, and severely immunocompromised individuals.
Monkeypox Drugs
There are several antiviral drugs for the treatment of monkeypox. It should be understood that clinical data on the efficacy of these drugs when used in humans is lacking. This is due, first, to the impossibility of conducting adequate and controlled trials due to lack of access to the right patient pool and, second, to the unethical nature of infecting volunteers with monkeypox to study the efficacy of any drugs. Nevertheless, the drugs have been successfully tested in animal models including mice, rabbits, and primates infected with orthopoxviruses, which include smallpox and monkeypox viruses.
- Despite periodic outbreaks of monkeypox in African countries, pharmaceutical companies have never bothered to test their drugs on infected people.
Cidofovir has a pronounced nephrotoxicity profile and is therefore unsuitable as the first choice drug.
Because of the possible development of drug resistance in poxviruses in response to tecovirimat, the possibility of coadministration with brincidofovir should be investigated.
Cidofovir
Intravenous cidofovir, approved in late June 1996 in the United States and in early May 1997 in Europe under the brand name Vistide, is used to treat cytomegalovirus retinitis in AIDS patients. Topical formulations of cidofovir are used in the off-label treatment of warts and molluscum contagiosum.
Cidofovir was developed by the Institute of Organic Chemistry and Biochemistry (IOCB) at the Academy of Sciences of the Czech Republic and the Belgium’s Rega Institute for Medical Research. Gilead Sciences later joined the project and promotes the drug in the United States. Outside of them, Pfizer markets Vistide. Due to the age of patents on the invention and intellectual property of cidofovir, generic copies have been offered.
Cidofovir diphosphate, the active intracellular metabolite of cidofovir (CDV, GS504, HPMPC), an acyclic nucleoside analogue of deoxycytidine monophosphate (dCMP), inhibits viral replication by selectively inhibiting viral DNA polymerase. It also inhibits human cellular DNA polymerases, but this effect is significantly weaker than the effect on viral ones. In addition, cidofovir is incorporated into the growing chain of viral DNA, which leads to a decrease in the rate of synthesis of the latter. [1] [2] [3]
The antiviral activity of cidofovir has been tested on various viruses, proving successful in a number of cases. In the case of monkeypox virus in animal models, cidofovir was shown to be effective against it, reducing the likelihood of lethal outcome. [4] [5] [6]
Clinical data on the efficacy of cidofovir against monkeypox in humans are lacking, and its administration may be associated with serious adverse events including nephrotoxicity. Animal studies have shown that cidofovir is carcinogenic, teratogenic, and causes hypospermia.
The prescribing information for Vistide contain a corresponding black box warning regarding the risk of acute renal failure, which can lead to dialysis and/or death. This can happen after literally one or two doses of cidofovir. To reduce the risk of nephrotoxicity, it is recommended that intravenous prehydration with normal saline and probenecid, which inhibits transport of organic anions in the renal proximal tubule epithelial cells, be given with each infusion of Vistide. [7]
- Vistide (cidofovir). Prescribing information. U.S. [PDF]
- Vistide (cidofovir). Prescribing information. Europe [PDF]
Tecovirimat
In mid-July 2018, the U.S. Food and Drug Administration (FDA) approved Tpoxx (tecovirimat), the world’s first smallpox drug.

Oral Tpoxx, indicated for the treatment of smallpox in adults and children (weighing at least 13 kg), is administered twice daily for 14 days.
In early December 2021, Health Canada approved Tpoxx for the treatment of smallpox in adults and children (weighing at least 13 kg).
In early January 2022, the European Medicines Agency (EMA) granted marketing authorization for the drug. The drug, called Tecovirimat SIGA, is indicated in adults and children (weighing at least 13 kg) to treat smallpox, monkeypox, and cowpox, and to treat complications caused by vaccinia virus replication after vaccination against smallpox.
In mid-May 2022, the FDA approved Tpoxx in an intravenous formulation.
Tecovirimat (VP-14637), discovered by ViroPharma, was sold in August 2004 for $1 million in cash and $1 million in stock to Siga Technologies, which brought it to life as Tpoxx.
- In November 2009, VP-14637, originally being developed by ViroPharma to treat respiratory syncytial virus (RSV) infection, [1] [2] was purchased by MicroDose Therapeutx and reformulated into an inhaled dry powder (MDT-637). In April 2011, Gilead Sciences joined the project. In June 2013, Teva Pharmaceutical Industries acquired MicroDose.
Tecovirimat (ST-246) is an inhibitor of the activity of the envelope protein VP37, which, being encoded by a highly conserved gene, is present in all orthopoxviruses and has no homologues in mammals. Tecovirimat blocks the interaction of VP37 with cellular GTPase Rab9 and TIP47 protein (Rab9-specific effector protein), thus preventing the formation of egress competent enveloped virions necessary for cell-to-cell and long-range dissemination of virus in the host. [3] [4] [5]
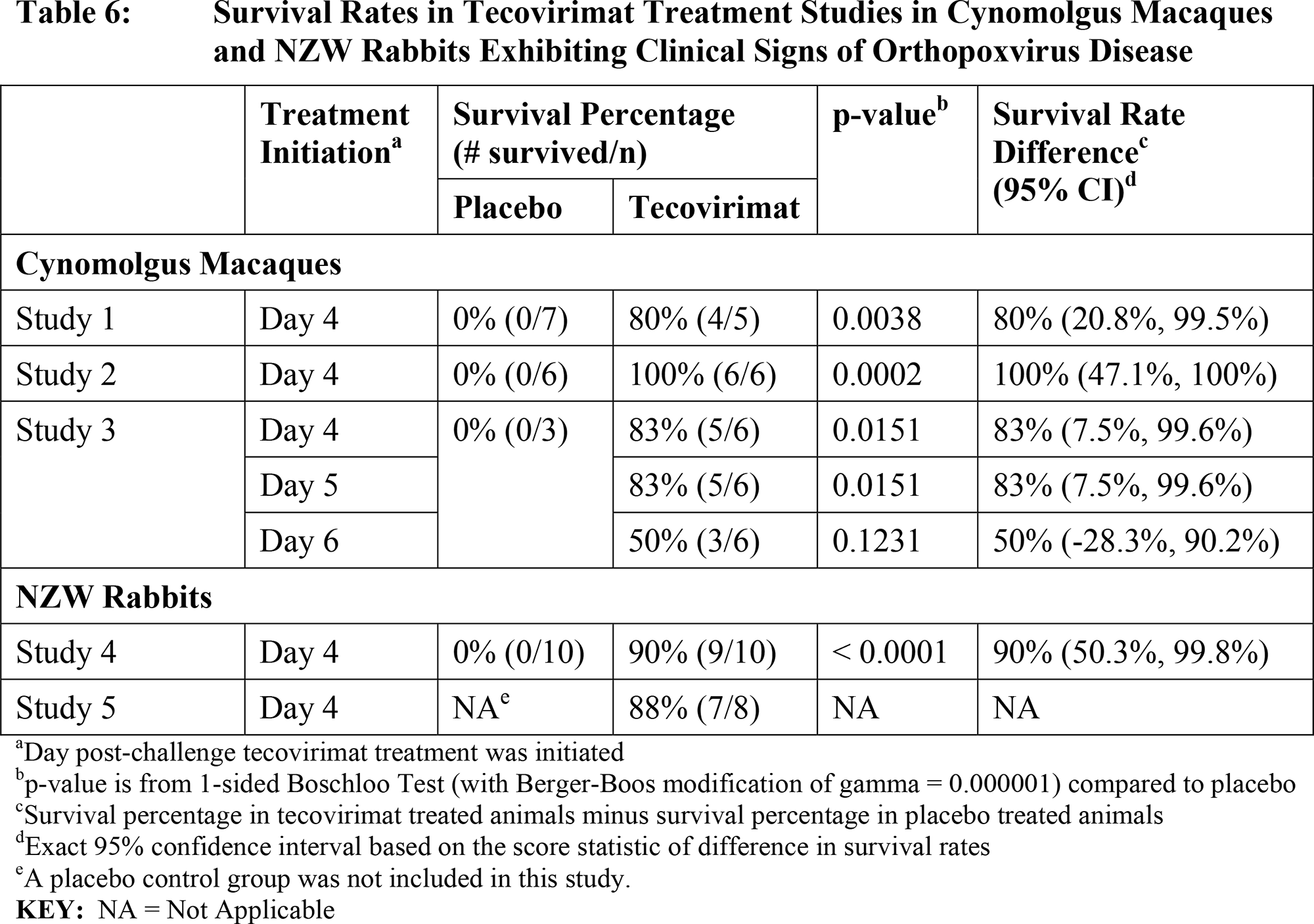
The efficacy of Tpoxx was tested in animal models of non-human primates and rabbits infected with species-specific orthopoxoviruses other than smallpox virus, Monkeypox virus (MPXV) and Rabbitpox virus (RPV), respectively. The collected animal survival rates allowed to safely assume that tecovirimat would have a similar therapeutic effect on humans infected with orthopoxoviruses including smallpox and monkeypox viruses.
Animals were given a lethal dose of the virus, then treated with tecovirimat a few days after infection to evaluate the efficacy of the drug after the development of clinical signs of disease, such as dermal pox lesions and fever. It was found that the earlier treatment was started, the more effective it was. For example, survival rates in cynomolgus macaques (Macaca fascicularis) ranged from 83% to 100% if tecovirimat was administered on day 4 after infection and were 83% and 50% if treatment was initiated on days 5 and 6 after infection, respectively. For rabbits, survival rates were 90% and 88% when treatment was initiated on days 4 and 5 after infection. [6]
Although the efficacy of Tpoxx was only evaluated on animals, it was still given to volunteers (n=359). The safety profile of tecovirimat is quite acceptable, not actually different from that of placebo.
There have been documented cases of Tpoxx administered as an emergency investigational drug to patients facing complications from smallpox vaccination, including a critically ill child with eczema vaccinatum and a military recruit with progressive vaccinia. Tecovirimat was administered along with intravenous vaccinia immune globulin (VIG), and both patients survived. [7] [8] [9]
Tecovirimat’s patent protection expires in 2024.
A number of clinical trials of tecovirimat are ongoing:
- ISRCTN43307947. Among hospitalized residents of the Central African Republic (CAR) diagnosed with monkeypox.
- NCT04971109. Treatment of orthopoxvirus infections or serious complications after smallpox vaccination among U.S. Department of Defense personnel and affiliated individuals.
- NCT05380752. Intravenous tecovirimat for the treatment of orthopoxvirus infections or serious complications following smallpox vaccination among U.S. military personnel.
- NCT04957485. Study of the interaction of tecovirimat with Jynneos/Imvanex/Imvamune smallpox vaccine in terms of changes in its immunogenicity.
Back in May 2011, Siga agreed with the Biomedical Advanced Research and Development Authority (BARDA), part of the Office of the Assistant Secretary for Preparedness and Response (ASPR) at the U.S. Department of Health and Human Services (HSS), to supply tecovirimat for the Strategic National Stockpile (STS) to address the smallpox threat. The $460 million contract involved delivery of 2 million courses of the drug, then called Arestvyr. In September 2018, the agreement with BARDA was updated to maintain a stockpile of oral tecovirimat (1,488,000 courses) and intravenous tecovirimat (212,000 courses), and the contract value exceeded $600 million.
In mid-January 2021, Canada formalized a $33 million contract to supply shipments of oral Tpoxx over 5 years.
- Tpoxx (tecovirimat). Prescribing information. U.S. [PDF]
- Tpoxx (tecovirimat). Prescribing information. Canada. [PDF]
- Tecovirimat SIGA. Prescribing information. Europe. [PDF]
- Siga Technologies. Management Presentation. May 2022. [PDF]
- Siga Technologies. Corporate Brochure. 2022. [PDF]
Brincidofovir
In early June 2021, the FDA approved Tembexa (brincidofovir) indicated to treat smallpox in adults and children, including neonates.
Tembexa in tablets or oral suspension is prescribed in short regimen on days 1 and 8 of treatment.
Oral brincidofovir (BCV, CMX001, HDP-CDV), developed by Chimerix, is a prodrug of cidofovir. In brincidofovir, cidofovir is conjugated to a lipid to mimic the natural lipid lysophosphatidylcholine to utilize the endogenous lipid uptake pathway. This led to an increase in the intracellular concentration of cidofovir with a concomitant decrease in plasma concentration, thereby significantly enhancing the antiviral activity of cidofovir. Inside cells, the lipid ester linkage of brincidofovir is cleaved, releasing cidofovir, which is phosphorylated to its active metabolite, cidofovir diphosphate. [1]
The mechanism of action of brincidofovir is similar to that of cidofovir. The molecule has an antiviral effect on orthopoxviruses, acting as a competitive substrate inhibitor of viral DNA synthesis mediated by viral DNA polymerase. The incorporation of cidofovir into the growing chain of viral DNA leads to a decrease in the rate of it synthesis. In vitro brincidofovir is about 25–150 times stronger than cidofovir and has a wider spectrum of activity. [2]
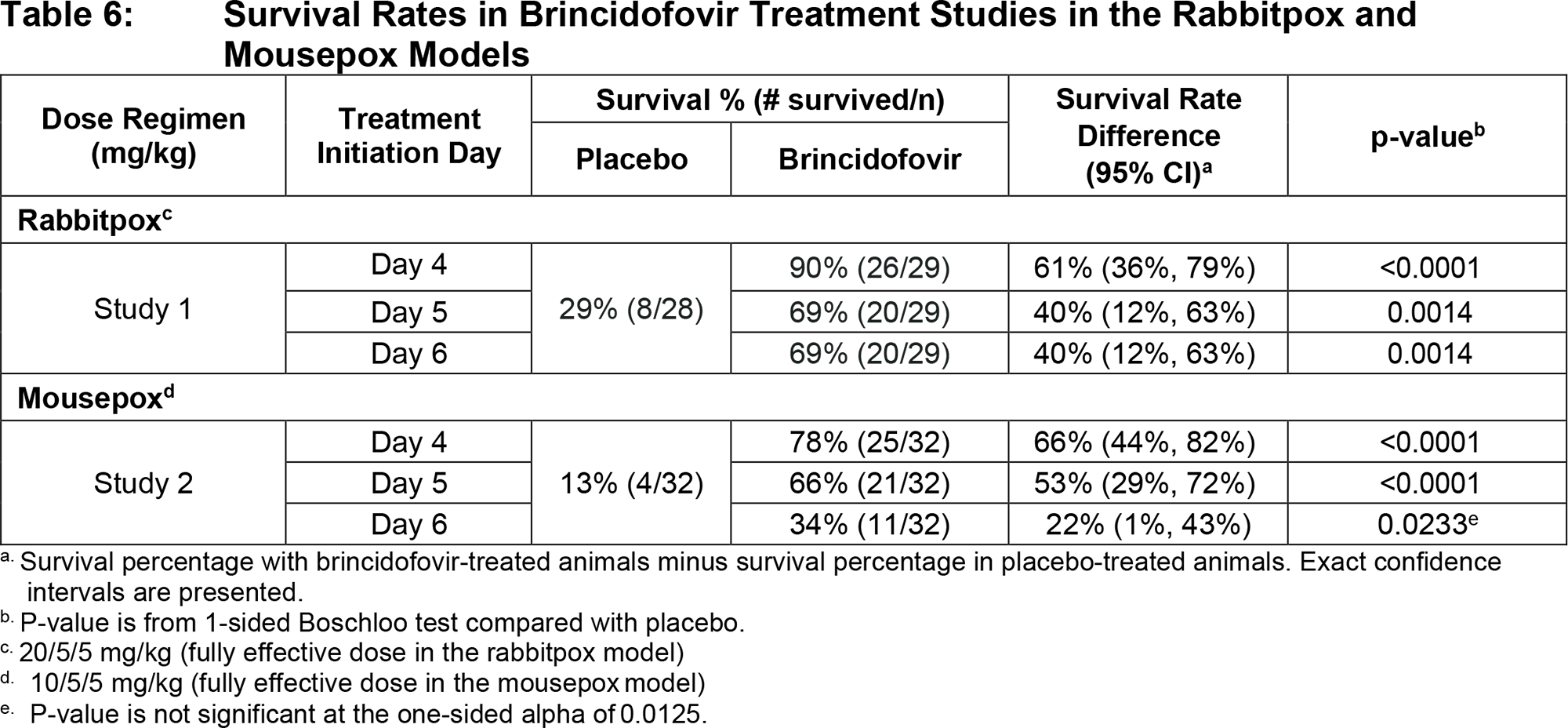
The efficacy of Tembexa was tested in animal models of rabbits and mice infected with species-specific orthopoxoviruses other than smallpox virus, Rabbitpox virus (RPV) and Ectromelia virus (ECTV), respectively. The collected animal survival rates allowed to safely assume that brincidofovir would have a similar therapeutic effect in humans infected with orthopoxviruses including smallpox and monkeypox viruses.
Animals received a lethal dose of the virus, then started treatment with brincidofovir several days after infection in order to evaluate the efficacy of the drug after clinical signs of disease, particularly fever, had developed. It was found that the earlier treatment was started, the more effective it was. Thus, survival rates in rabbits were 90%, 69%, and 69% if brincidofovir was administered on days 4, 5, and 6 after infection, respectively. For mice, the indicated survival rates were 78%, 66%, and 34%. [3]
The prescribing information for Tembexa come with a black box warning regarding increased mortality in patients who have received the drug for a prolonged period of time. In the phase 3 clinical study NCT01769170, which checked brincidofovir in the task of preventing cytomegalovirus (CMV) infection in patients who underwent allogeneic stem cell transplantation, administration of Tembexa for 14 weeks had no proper effect, and mortality in the brincidofovir group was 15.5% versus 10.1% in the placebo group. [4]
Tembexa has seven years of orphan exclusivity in the U.S. market, and its patent protection is expected to be extended through 2034.
In late December 2021, BARDA signed a contract with Chimerix to supply up to 1.7 million doses of Tembexa, worth $500 million to $600 million, to build Strategic National Stockpile (SNS) to counter the smallpox threat.
In mid-May 2022, Chimerix sold all rights to Tembexa for $225 million in advance to Emergent BioSolutions. Up to $100 million more will be received as the contract with BARDA is implemented, which is also transferred to Emergent, which specializes in serious diseases such as cholera, typhoid, anthrax, and botulism. In addition, Chimerix will receive a double-digit royalty on sales of Tembexa.
- Meanwhile, Japan’s SymBio Pharmaceuticals, which licensed brincidofovir from Chimerix in late September 2019, is developing its intravenous formulation (SyB V-1901), targeting the drug for the treatment of adenovirus infection that has developed with immune deficiencies (e.g., after allogeneic stem cell transplantation) and BK virus infection after kidney transplantation (BK virus–associated nephropathy, BKVAN).
- Tembexa (brincidofovir). Prescribing information. U.S. [PDF]
- Chimerix. Corporate presentation. January 2022. [PDF]
Experimental Drugs
The need for new antiviral drugs is understandable. Not only is the threat of outbreaks of orthopoxvirus infections constantly on the rise, but their pathogens can mutate to become drug resistant. [1] [2]
NIOCH-14
The Novosibirsk Institute of Organic Chemistry (NIOC) in collaboration with the State Research Center of Virology and Biotechnology VECTOR has developed an oral antiviral drug NIOCH-14, a tricyclodicarboxylic acid derivative that is not inferior to tecovirimat in its antiviral activity against orthopoxviruses. The mechanism of action of NIOCH-14 does not differ from that of Tpoxx (tecovirimat) because the molecule, being a prodrug, is metabolized in the body to tecovirimat. [1] [2] [3] [4] [5] [6]
Sarracenia Purpurea
A tincture made from the root of the carnivorous purple pitcher plant (Sarracenia purpurea) has been used successfully by Native American tribes to treat smallpox. [1] [2] According to a 2012 study, the botanical preparation of S. purpurea is an in vitro effective inhibitor of replication of vaccinia, monkeypox, and smallpox viruses at the level of early transcription. [3]