What Is Monkeypox
General Information
Monkeypox is a zoonotic (animal-transmitted) viral infection that is clinically difficult to distinguish from smallpox, but is less contagious, milder in its course, and less fatal.
Monkeypox is caused by the monkeypox virus, a relative of the smallpox, cowpox, and vaccinia viruses.
The monkeypox virus is transmitted to humans by contact with infected animals or humans and by contaminated items and objects. Monkeys and humans are accidental carriers of the virus; the reservoir remains unknown, but most likely rodents.
The incubation period from infection with monkeypox virus to clinical manifestations of the disease is less than 2 weeks.
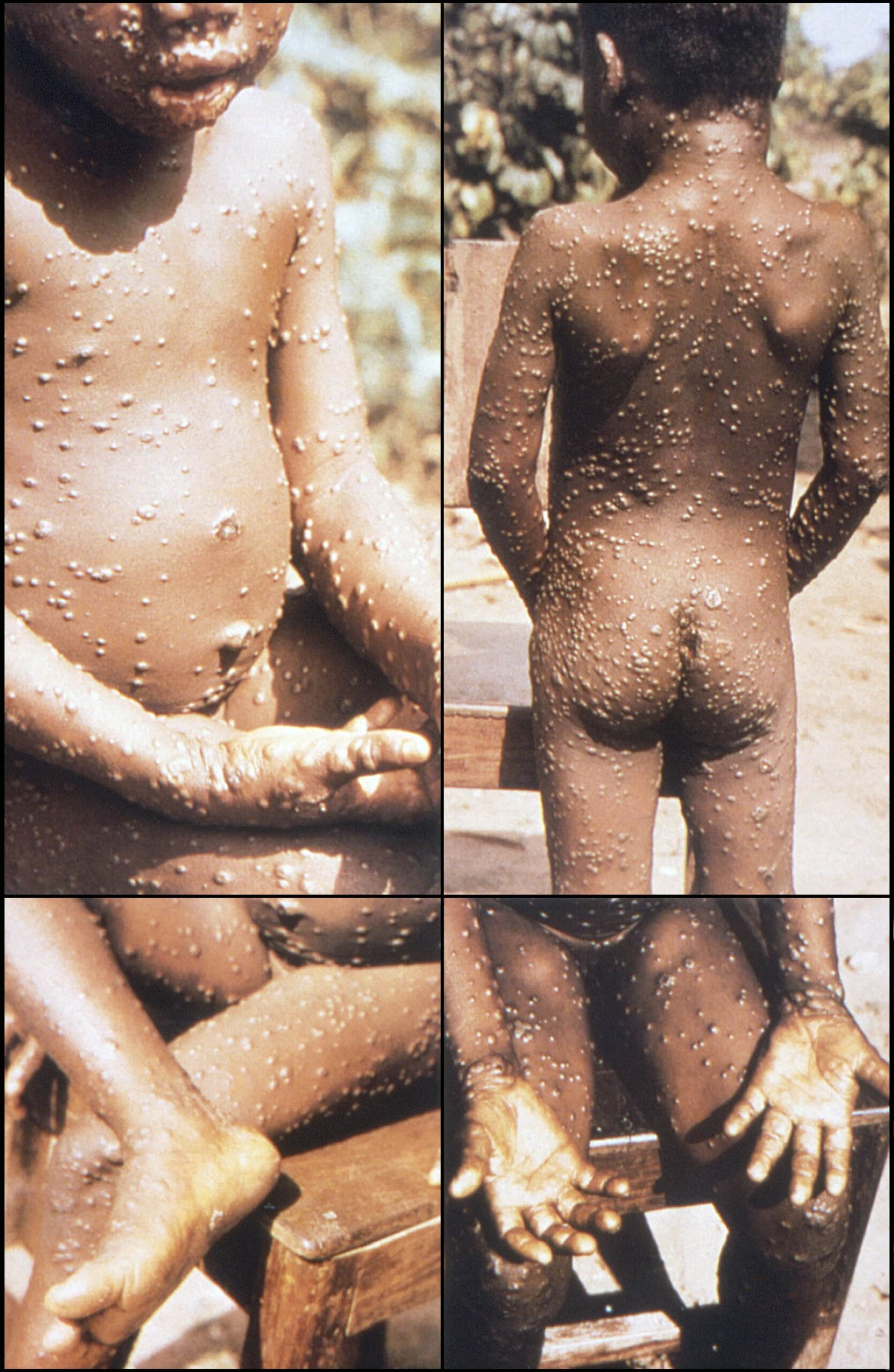
The main symptoms of monkeypox are flu-like symptoms (fever, chills, muscle pain), followed by enlarged lymph nodes and a characteristic rash. Most patients with monkeypox have a mild form of the disease.
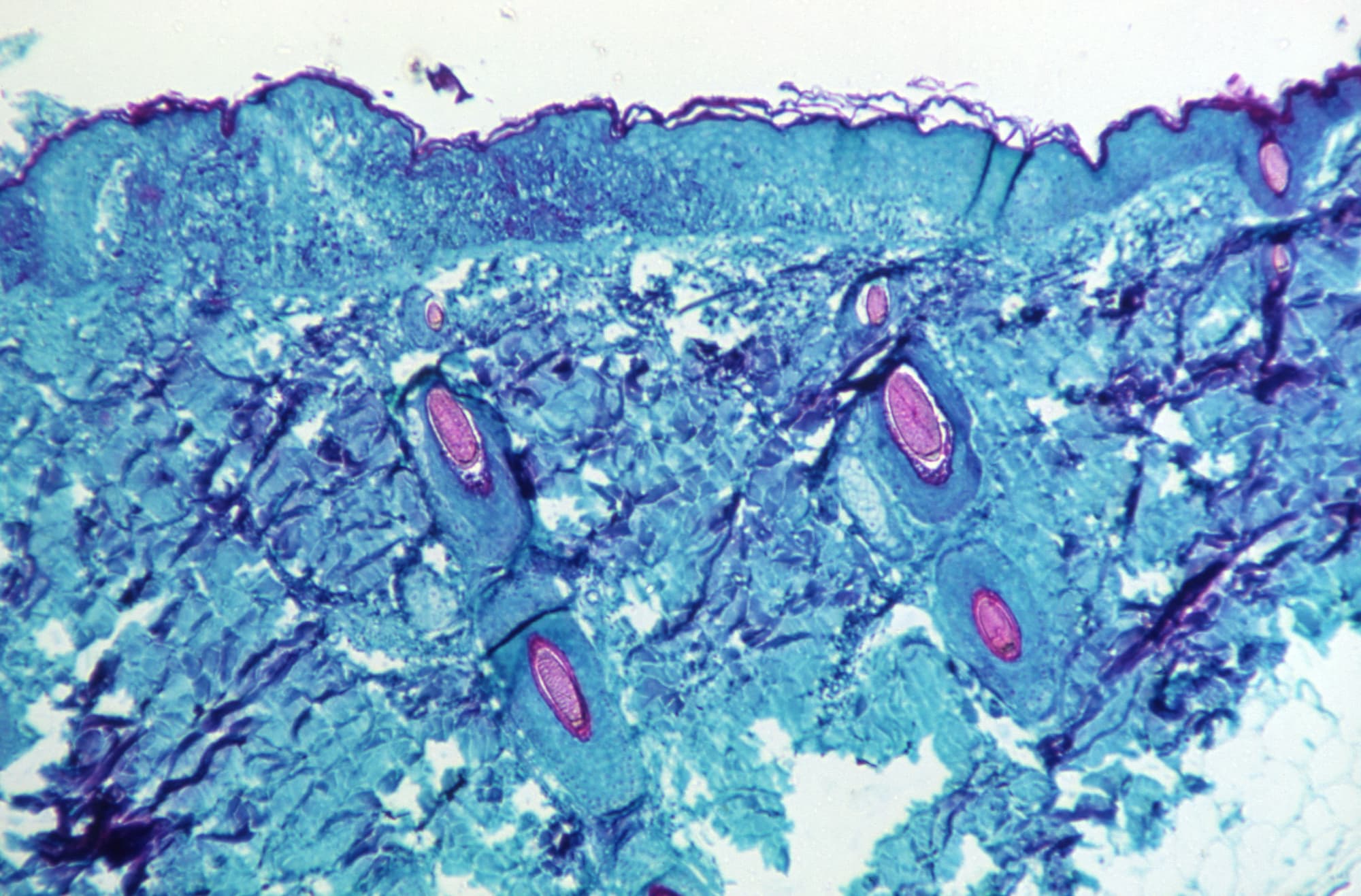
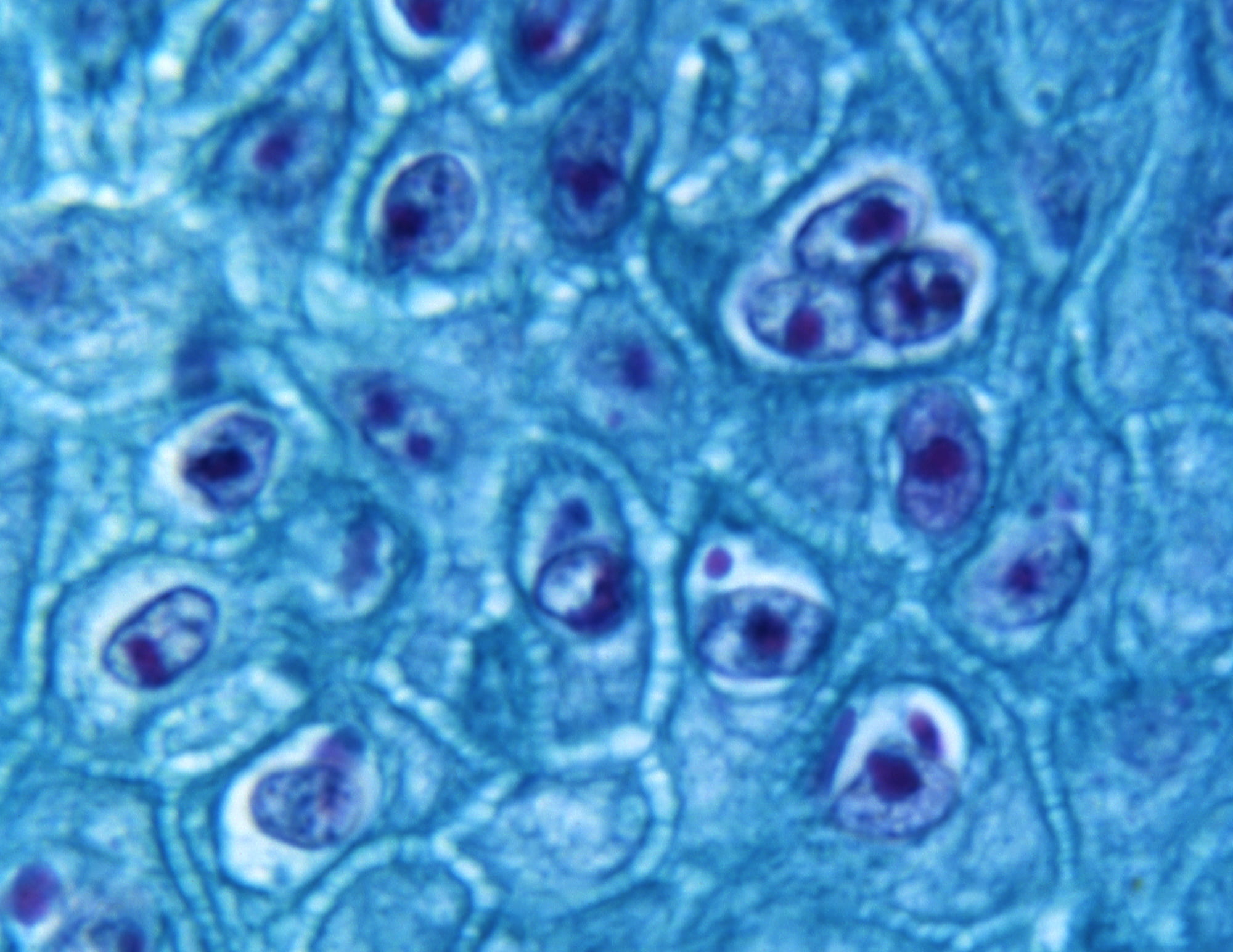
Although clinical signs of infection are helpful in making the diagnosis, laboratory confirmation is needed to differentiate monkeypox from diseases caused by other viruses, including related ones.
Most patients with monkeypox recover independently without any medical intervention. For critically ill patients, supportive care is necessary. There are a number of antiviral drugs that are approved to treat smallpox that are probably effective against monkeypox.
Smallpox vaccines reliably protect against monkeypox.
Monkeypox Pathogen
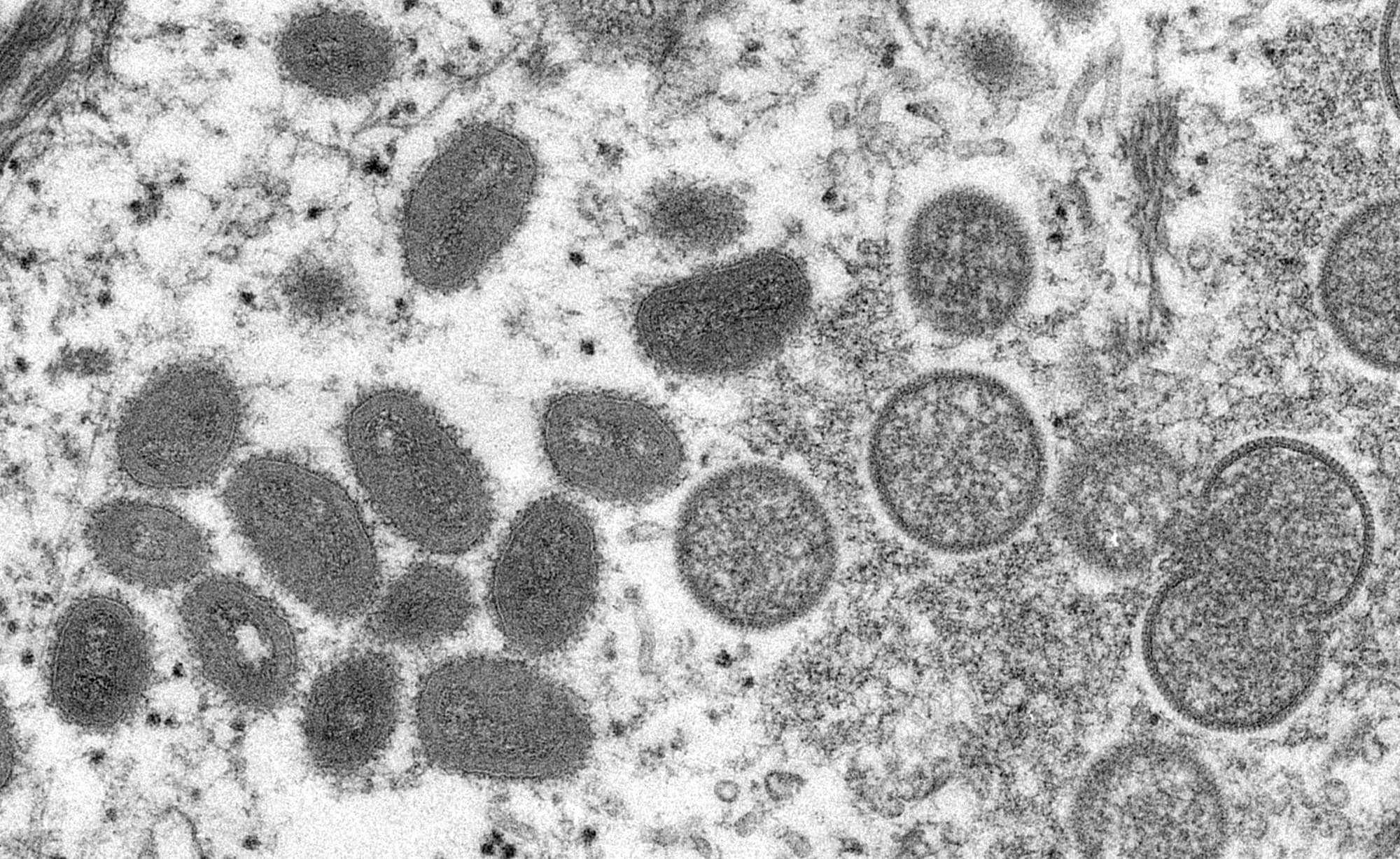
Monkeypox, which occurs in humans and animals, is caused by Monkeypox virus (MPV, MPXV), a enveloped double-stranded DNA virus with a genomic size of 190,000 base pairs that belongs to the genus Orthopoxvirus of the family Poxviridae.
Monkeypox virus got its name when it was first isolated in Copenhagen in 1958 from cynomolgus macaques (Macaca fascicularis) imported from Singapore to Denmark and used as laboratory animals for polio vaccine–related vaccine research after an outbreak of smallpox-like vesicular disease occurred in their colonies. [1]
- The term “monkeypox” is essentially inappropriate because the largest animal reservoirs of the virus have been found in rodents. [2]
Genomic sequencing has revealed two phylogenetically distinct clades (genetic groups) of Monkeypox virus: the West African clade, found from western Cameroon to Sierra Leone, and the Congo Basin clade (Central African clade), found from central and southern Cameroon to the Democratic Republic of Congo (DRC). The Congo Basin clade is considered more dangerous. [2] [3] [4]
Monkeypox virus is included in the genus Orthopoxviruses, which includes 12 viruses, such as Variola virus (VARV), Vaccinia virus (VACV), Cowpox virus (CPX, CPXV), Camelpox virus (CMPV), Raccoonpox virus (RCN), etc. Monkeypox virus is neither a direct ancestor nor a direct descendant of Variola virus, which causes smallpox.
Monkeypox Epidemiology
The monkeypox virus is thought to have infected humans for thousands of years in areas of sub-Saharan Africa. [1]
In terms of epidemic risks, monkeypox is the most important orthopoxvirus infection in humans since the eradication of smallpox. [2]
Monkeypox as a cause of disease in humans was first identified in 1970 in the Democratic Republic of Congo (DRC; formerly the Republic of Zaire) in a 9-month-old child after appropriate tests at the WHO Collaborating Centre in Moscow. Monkeypox could have been detected much earlier, but until then smallpox was rampant in the DRC, and the clinical pictures of the two diseases are very similar. [3] [4] [5]
After recognition of the infection as pathogenic to humans, 404 cases of monkeypox were reported between 1970 and 1986, mainly in children under 16 years of age and usually after contact with small forest animals (rodents, monkeys). All cases occurred in seven West and Central African countries: DRC, Côte d’Ivoire, Sierra Leone, Cameroon, Central African Republic (CAR), Liberia, and Nigeria. Of these, 338 cases were detected during intensified WHO surveillance in the DRC from 1981 to 1986, with 13% of those ill having been vaccinated against smallpox (most more than 10 years ago). The overall case fatality rate (CFR) was 10%. [1] [6] [7] [8] [9] [10]
In 1986, intensified WHO surveillance was discontinued, and only 12 cases of monkeypox were reported between 1987 and 1992. In other words, without adequate surveillance, the disclosed incidence may be significantly underestimated. [9]
After the complete eradication of smallpox from the earth and the subsequent discontinuation of mandatory vaccination against this terrible infection, the World Health Organization monitored the activity of monkeypox in humans. The planet’s chief medical regulator was concerned that the elimination of smallpox vaccination, which also protected against other orthopoxviruses, including Monkeypox virus, would increase the susceptibility and incidence of related viral infections.
And so it was when 885 cases of fever-associated rash were reported in the DRC between 1996 and 1998. The unequivocal diagnosis of monkeypox was complicated by simultaneously circulating chickenpox (varicella). Nevertheless, in most cases, it was later determined that it was Monkeypox virus that caused the disease. At first, it was thought to have mutated, and therefore the infection became more like smallpox. Subsequent analysis of the genetic sequence of the virus revealed no significant changes. The overall low CFR (1% compared to 9.8% in 1981–1986) during this outbreak was further evidence that Monkeypox virus had not evolved into a more lethal pathogen for humans. [6] [9] [11] [12]




A population study conducted between 2005 and 2007 in the DRC found a 20-fold increase in the incidence of monkeypox compared to the 1981–1986 period. There were 760 laboratory-confirmed cases of infection. WHO’s fears were justified: As the population immunologically naïve to orthopoxviruses increased significantly with the cessation of smallpox vaccination campaigns en masse, this caused an increased risk of monkeypox infection. Thus, individuals previously immunized against smallpox had a 5.2-fold lower risk of monkeypox infection than unvaccinated individuals. Other factors of increased risk of infection included living in forested areas, male gender, and age under 15 years old. [13]
The first outbreak of monkeypox outside the Central and West African belt began in the United States in May 2003, when a child developed a fever and rash. A little later, another 70 similar cases were reported, of which 35 were laboratory-confirmed; no fatalities were reported. The source of infection was prairie dogs. These rodents of the squirrel family were infected with Monkeypox virus as a result of cross-infection in a pet store from unquarantined other rodent species imported from Ghana. People have been infected in a variety of ways: by touching or being bitten or scratched by an animal, by cleaning the cage or touching the bedding, by just being in the same room with them. In other words, monkeypox was transmitted by percutaneous, mucocutaneous, and inhalation exposure. [14] [15] [16] [17] [18] [19] [20] [21] [22]
Since 2017, cases of monkeypox, which had been absent in this West African country for 39 years, have increased in Nigeria. Thus, between September 2017 and January 2019, 311 cases (132 laboratory-confirmed) were reported, and 7 people died. In 2021, 98 cases were reported (34 confirmed). The total number of monkeypox infections from the outbreak through the end of April 2022 was 558 (241 confirmed cases), 8 people died (CFR 1.4%). The actual incidence may well be an underestimate, as Nigerians avoid visiting medical facilities for fear of contracting COVID-19. [23] [24] [25] [26]




From early January 2020 to early May 2022, there were 10,545 cases (39 lab-confirmed) and 362 deaths (CFR 3.4%) in the DRC, where monkeypox still rages. [27]
Now monkeypox is gaining strength in other African countries as well. Thus, in mid-December 2021, the disease arrived in Cameroon, where by mid-May 2022 it had affected 24 people (3 laboratory-confirmed cases), 9 of whom died (CFR 37.5%). In early March 2022, the Central African Republic (CAR) reported cases of monkeypox, with the virus infecting 17 people (8 confirmed) by mid-May, 2 of whom died (CFR 11.8%). [27]
Occasional single cases of monkeypox associated with travel to Nigeria have been reported in countries outside Africa: three cases in the United Kingdom in September 2018, [28] [29] [30] one in Israel in October 2018, [31] one in Singapore in May 2019, [32] one in the United Kingdom in December 2019, [33] three in the United Kingdom in May–June 2021, [34] one in the United States in July 2021, [35] [36] one in the United States in November 2021. [37]
In May 2022, a major outbreak of monkeypox began in Western countries. It was the first to strike a dozen and a half countries in Europe almost simultaneously, and also affected the United States and Canada.
Monkeypox Transmission
The monkeypox virus is transmitted to humans through contact with infected animals or humans, as well as contaminated material, objects, or items.
The monkeypox virus enters the body through damaged skin (even if the injuries are not visible), respiratory tract, and mucous membranes (eyes, nose, and mouth).
In endemic areas the monkeypox virus is transmitted to humans from an infected live or dead animal through bite, scratch or direct contact with blood, meat, body fluids, skin-mucosal lesions, direct contact with contaminated objects (e.g. through hair), indirect contact with contaminated objects (e.g. through bedding). Thus, transmission can occur by cutting or cooking meat of eaten infected animals, contact with them during housekeeping or play. [1] [2] [3] [4]
The transmissibility of monkeypox virus from human to human is very low: Close and prolonged contact is required for the transmission of virus particles. Nevertheless, cases of serial transmission have been reported. Transmission can occur via large droplets from the respiratory tract. Because such droplets cannot travel long distances, prolonged face-to-face contact is required for transmission: for example, within a 2-meter radius for 3 hours or more in the absence of personal protective equipment. Human-to-human transmission of monkeypox virus can occur through direct contact with the bodily fluids of the infected person, by contact of mucous membranes or skin with open lesions of rash or fomites (contaminated objects such as clothing, bedding, towels, etc.). [1] [3] [5] [6] [7] [8] [9] [10] [11]
Cases of transmission of the monkeypox virus through substances of human origin (blood, organs, tissues, cell cultures) have not been recorded. Nevertheless, there are reports of cases of mother-to-child transmission during pregnancy [12], and studies have shown the presence of the virus in the blood, tissues and organs of infected animals. [13] [14] The existence of viremia (i.e. blood specimens positive for viral DNA) has been demonstrated. The duration of viremia is unclear [15], and there are no data on viremia in asymptomatic patients, including during the incubation period.
Cases of nosocomial transmission have been documented. [6]
During an outbreak of monkeypox in the United States in May 2003, none of the 57 health care workers in contact with patients reported signs or symptoms of the disease. [16] In contrast, in smallpox, the incidence of secondary attack rate, as a measure of contagiousness, is as high as 20%. [17] [18]
The route of infection and degree of exposure have also been found to influence the severity of clinical manifestations of monkeypox. With complex exposure (e.g., a bite wound), signs of systemic disease develop more frequently than with noninvasive exposure (e.g., touching an infected animal or cleaning its cage). [19]
Monkeys and humans are occasional carriers of the virus; the reservoir host (main disease carrier) remains unknown, but it is most likely African rodents. In endemic areas, the virus is maintained in nature by circulation among a number of mammals, including mice, rats, squirrels, Gambian rats, elephant shrews, and primates. [4] [20]
Monkeypox virus has been isolated in wild animals in the nature only twice. The first time the virus was isolated in 1985 from an apparently sick Thomas’s rope squirrel (Funisciurus anerythrus) in the Democratic Republic of Congo (DRC), the second time in 2012 from a dead calf of the smoky mongoose (Cercocebus atys) in Côte d’Ivoire. [21] [22]