Highlights
Enhertu (trastuzumab deruxtecan) is a new drug indicated to treat unresectable or metastatic HER2-positive breast cancer in adult patients.
Enhertu made its debut in December 2019, when the U.S. Food and Drug Administration (FDA) approved it to treat patients who had already received two or more prior anti-HER2-based regimens in the metastatic setting.
The U.S. regulator granted the drug conditional approval, which means that Enhert had to definitively confirm its effectiveness.
The European Medicines Agency (EMA) approved Enhertu in January 2021, similarly conditionally.
In early May 2022, FDA approval for Enhertu became full-fledged and the drug moved into the earlier therapy category. Enhertu is now used for the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received a prior anti-HER2-based regimen either in the metastatic setting or in the neoadjuvant or adjuvant setting and have developed disease recurrence during or within 6 months of completing therapy.
Enhertu has been offered by AstraZeneca and Daiichi Sankyo.
In March 2019, AstraZeneca agreed with Daiichi Sankyo, which is behind the development of trastuzumab deruxtecan, to work together on the the drug’s evolution. The British pharma company has promised to pay the Japanese drugmaker up to $6.9 billion including an upfront $1.35 billion; the money will be released as certain regulatory and commercial phases of the project are passed.

Enhertu: Trastuzumab Deruxtecan as New Standard of Treatment for HER2-Positive Breast Cancer
Breast cancer is the most common cancer in women and the most frequent cause of death from oncology disease in women. In about 20% of breast cancer diagnoses, tumor cells are characterized by overexpression or amplification of human epidermal growth factor receptor 2 (HER2), which translates into a biologically aggressive disease with a shortened survival period for patients. Although there are many drugs available that target HER2 and improve clinical outcomes, a cure is virtually impossible in locally advanced or metastatic disease — the disease inevitably progresses.
The recommended first-line therapy for previously untreated metastatic HER2-positive breast cancer involves a combination of Herceptin (trastuzumab) and Perjeta (pertuzumab) — the monoclonal antibodies by Roche against HER2 — in combination with the taxane chemotherapy drug docetaxel. The drug cocktail prolongs overall survival (OS) and progression-free survival (PFS) remarkably well, bringing them to a median of 57.1 and 18.7 months, respectively.
Standard second-line therapy for metastatic HER2-positive breast cancer relies on the use of Kadcyla (trastuzumab emtansine) — monoclonal antibody conjugate by the same Roche against HER2 carrying emtansine (DM1), a cytotoxic tubulin polymerization inhibitor. Here we can expect an overall response rate (ORR) of 43.6%, a median OS of 29.9 months and a median PFS of within 9.6 months.
A universal consensus approach to third-line therapy for metastatic HER2-positive breast cancer is currently not proposed: available treatment options are characterized by very modest and even mediocre efficacy, providing an ORR in the range of 9–31% with a median PFS of no more than 3–6 months. Thus, tertiary therapy turns to the notorious trastuzumab in combination with either a chemotherapeutic agent other than docetaxel or the tyrosine kinase inhibitor Tykerb/Tyverb (lapatinib); to lapatinib with capecitabine; to endocrine therapy (for hormone-sensitive disease) combined with either trastuzumab or lapatinib.
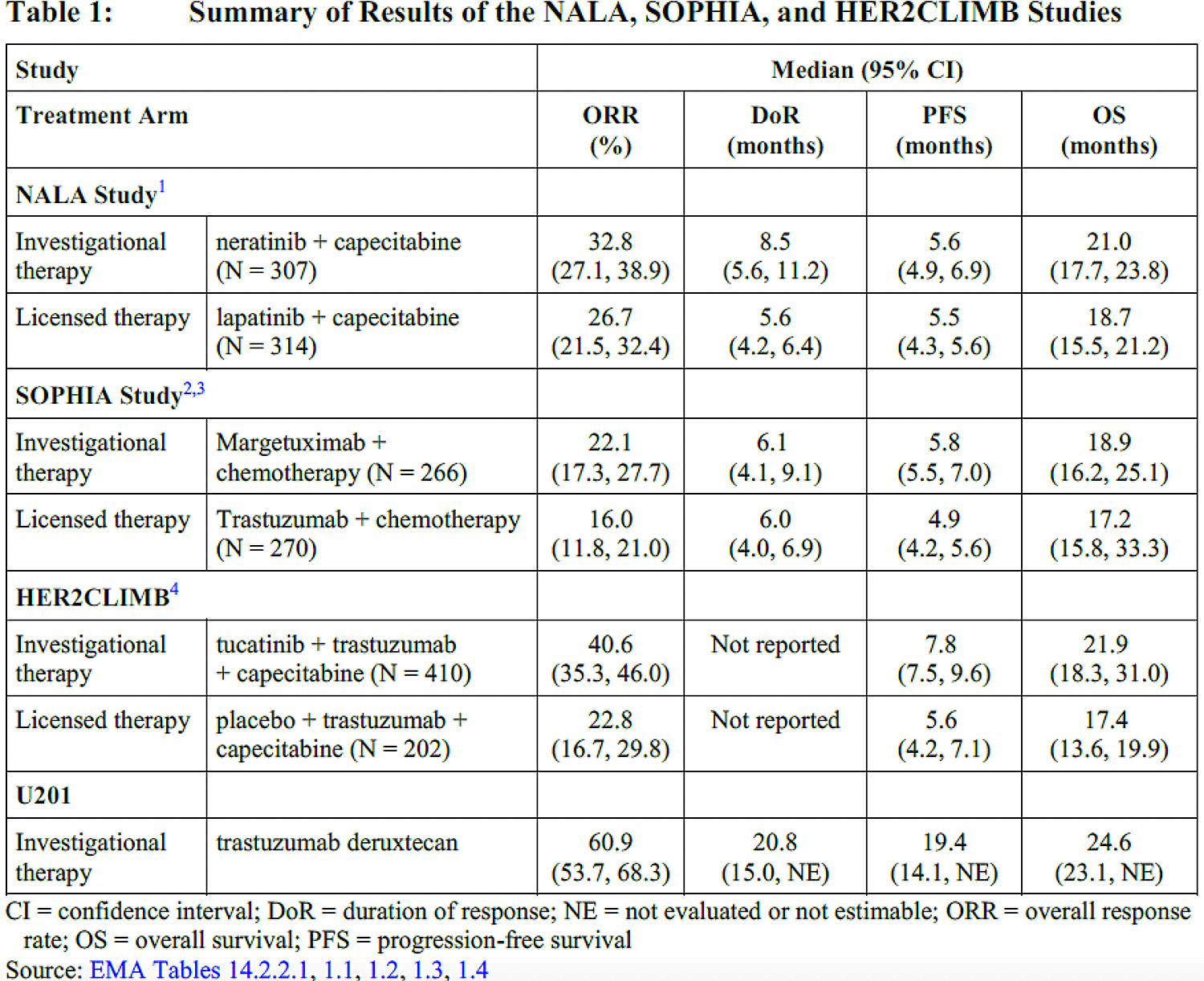
Experimental third-line therapeutic approaches — neratinib + capecitabine, margetuximab + chemo, tucatinib + trastuzumab + capecitabine — show improved clinical outcomes, but the efficacy of treatment with trastuzumab deruxtecan is still better from all points.
Since Enhertu has proven its own unqualified therapeutic efficacy, it is bound to become the new standard of third-line therapy for metastatic HER2-positive breast cancer — after the failure of Herceptin, Perjeta, and Kadcyla. Moreover, if Enhertu continues to show impressive treatment efficacy, it is possible that it will receive the status of the drug of choice for first-line therapy.
Again, even in HER2-negative breast tumors, which account for up to 80% of all breast cancers, there is still some HER2 expression on the surface of the tumor cells. There are currently no approved targeted drugs targeting patients with breast cancer whose cells are characterized by low HER2 expression. Enhertu could be useful here as well: due to the features of its mechanism of action.
Enhertu: Mechanism of Action of Trastuzumab Deruxtecan
Enhertu (trastuzumab deruxtecan, DS-8201) is a humanized monoclonal IgG1 antibody against HER2 (with the same amino acid sequence as trastuzumab) to which deruxtecan (DXd), a derivative of the cytotoxic camptothecin analog exatecan, is linked.
The antibody-drug conjugate (ADC) binds to HER2 expressing tumor cells and releases a cytotoxic drug load. Exatecan, being a DNA topoisomerase 1 (TOP1) inhibitor, suppresses DNA replication, stops the cell cycle and leads to apoptosis of malignant cells. And if each molecule of original Kadcyla (trastuzumab emtansine) carries 3–4 molecules of cytotoxic drug load, in the case of trastuzumab deruxtecan this ratio almost doubled (up to 8 molecules) while maintaining an acceptable pharmacokinetic profile.
Due to the short half-life of exatecan, systemic exposure was minimized.
The proprietary maleimide tetrapeptide linker is stable in plasma; it is cleaved by cathepsins that are abundantly present in tumor cells.
The induction of antibody-dependent cell-mediated cytotoxicity (ADCC) is observed when trastuzumab deruxtecan is administered.
Moreover, deruxtecan easily crosses the cell membrane and therefore has a detrimental effect on neighboring cancer cells, even if they are not characterized by the proper expression of HER2. And this is quite important.
- Deruxtecan is a water-soluble compound. Once the cytotoxic drug load of this monoclonal conjugate is internalized into the tumor cell, it is slowly released into the tumor microenvironment and diffuses back into neighboring tumor cells.
- HER2 expression is not uniform throughout the tumor cell population: some tumor cells express HER2 strongly, while others only express it weakly. Often when patients develop resistance to HER2-targeting therapy, such a drug-resistant cell subclone begins to grow, losing HER2 expression altogether. Trastuzumab deruxtecan can bypass this feature.
Enhertu: Efficacy and Safety of Trastuzumab Deruxtecan in Treatment of Breast Cancer
DESTINY-Breast01
The DESTINY-Breast01 (NCT03248492) phase 2 (nonrandomized, open-label, multicenter, international) pivotal clinical trial tested the administration of trastuzumab deruxtecan among adult women (n=184) with unresectable and/or metastatic HER2-positive breast cancer who did not respond to at least two lines of targeted anti-HER2 therapy.
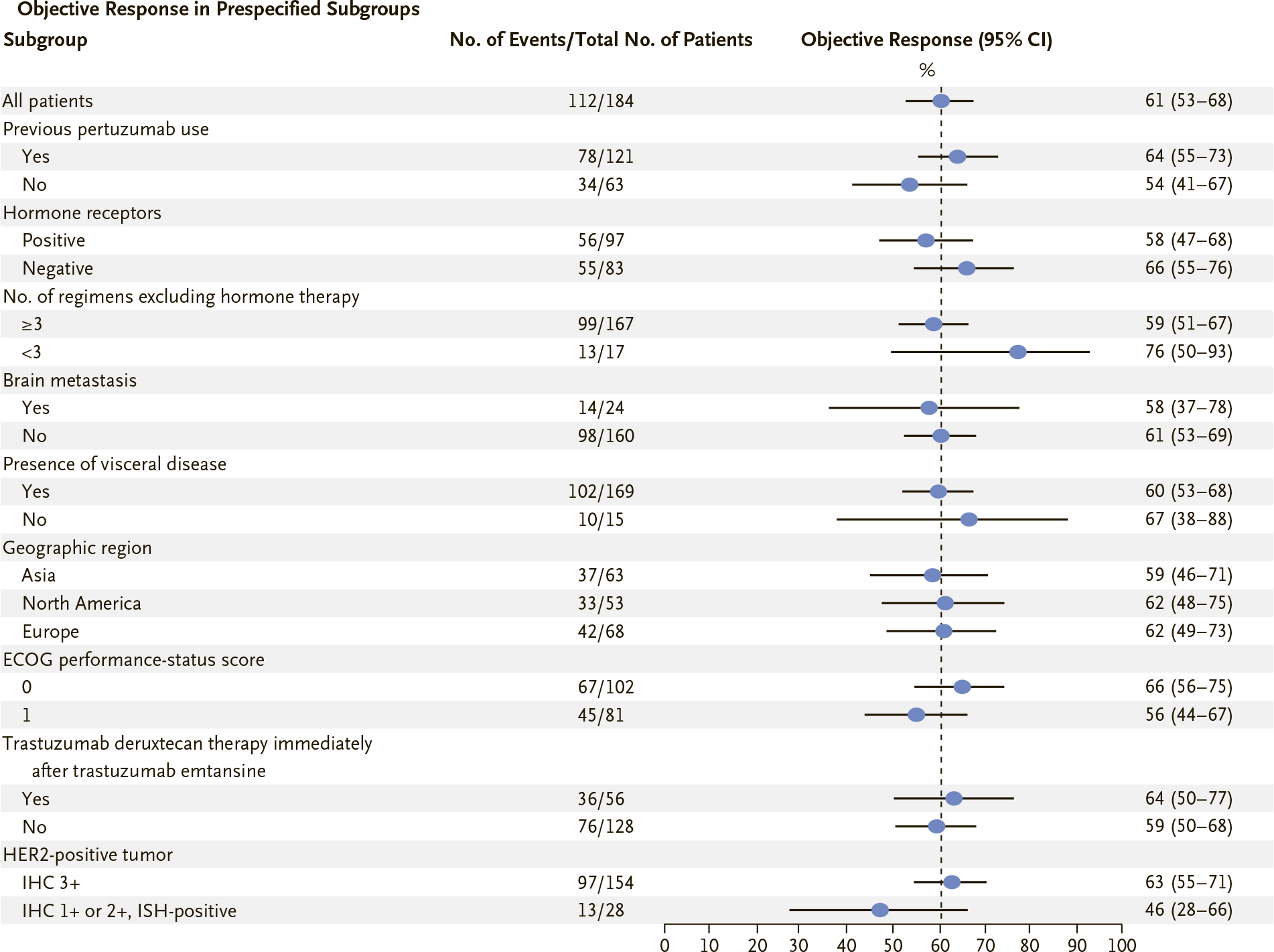
The median age of the subjects was 55 years (28–96), with 76% of the participants being younger than 65 years. 92% of participants had disease characterized by visceral metastases, 29% had bone metastases, and 13% had brain metastases. Breast cancer was hormone-receptor-positive (HR+) in 53% of patients. The median number of prior treatments for locally advanced and/or metastatic settings was 6 (2–27). All patients had already received Herceptin (trastuzumab) and Kadcyla (trastuzumab emtansine), and 66% had also received Perjeta (pertuzumab).
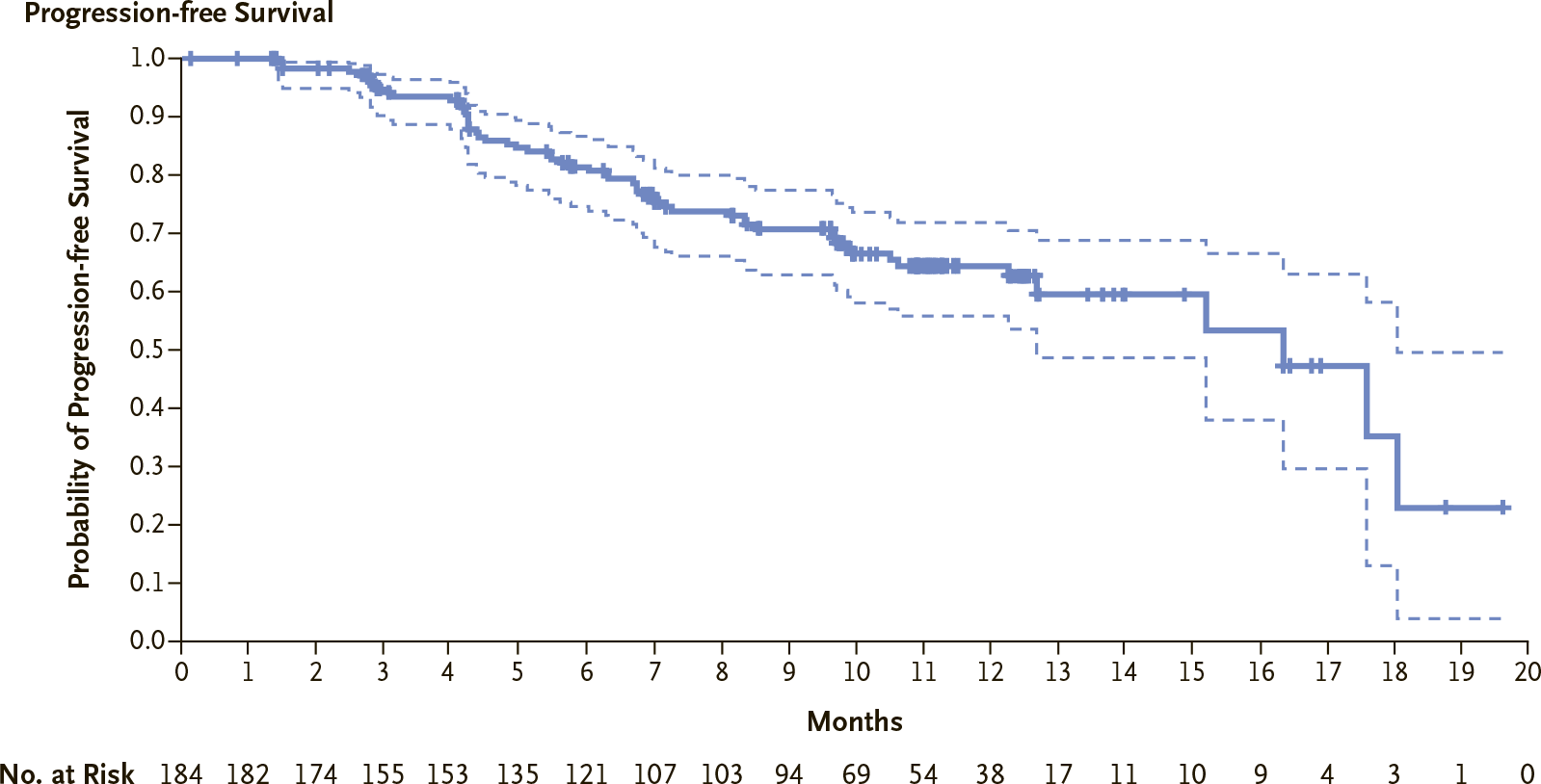
Within a follow-up median of 11.1 months (0.7–19.9), treatment with Enhertu provided the following clinical outcomes:
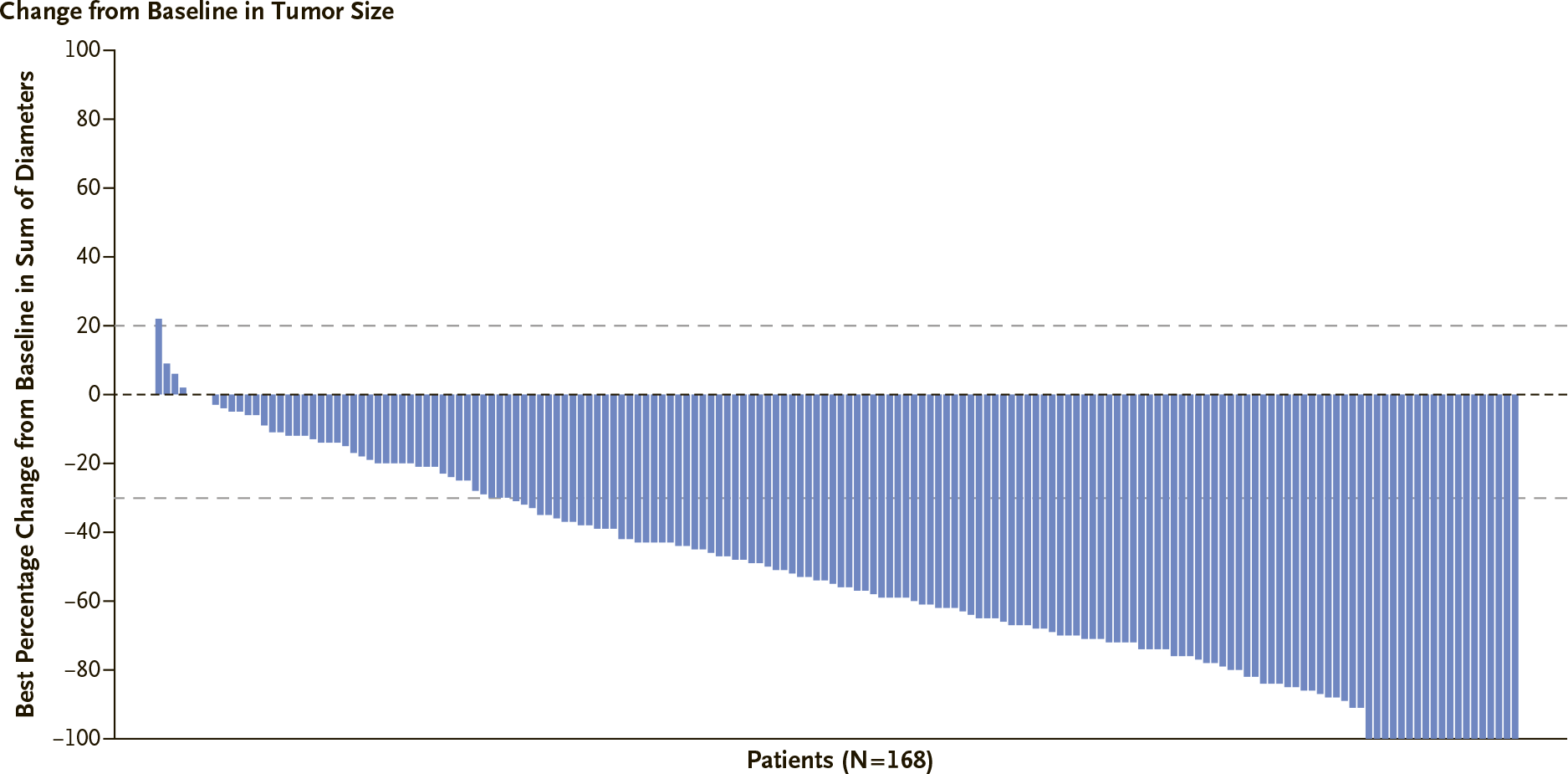
- confirmed overall response rate (ORR) was recorded in 60.9% (95% CI: 53.4 to 68.0) of patients, including complete response (CR) in 6.0% and partial response (PR) in 54.9%
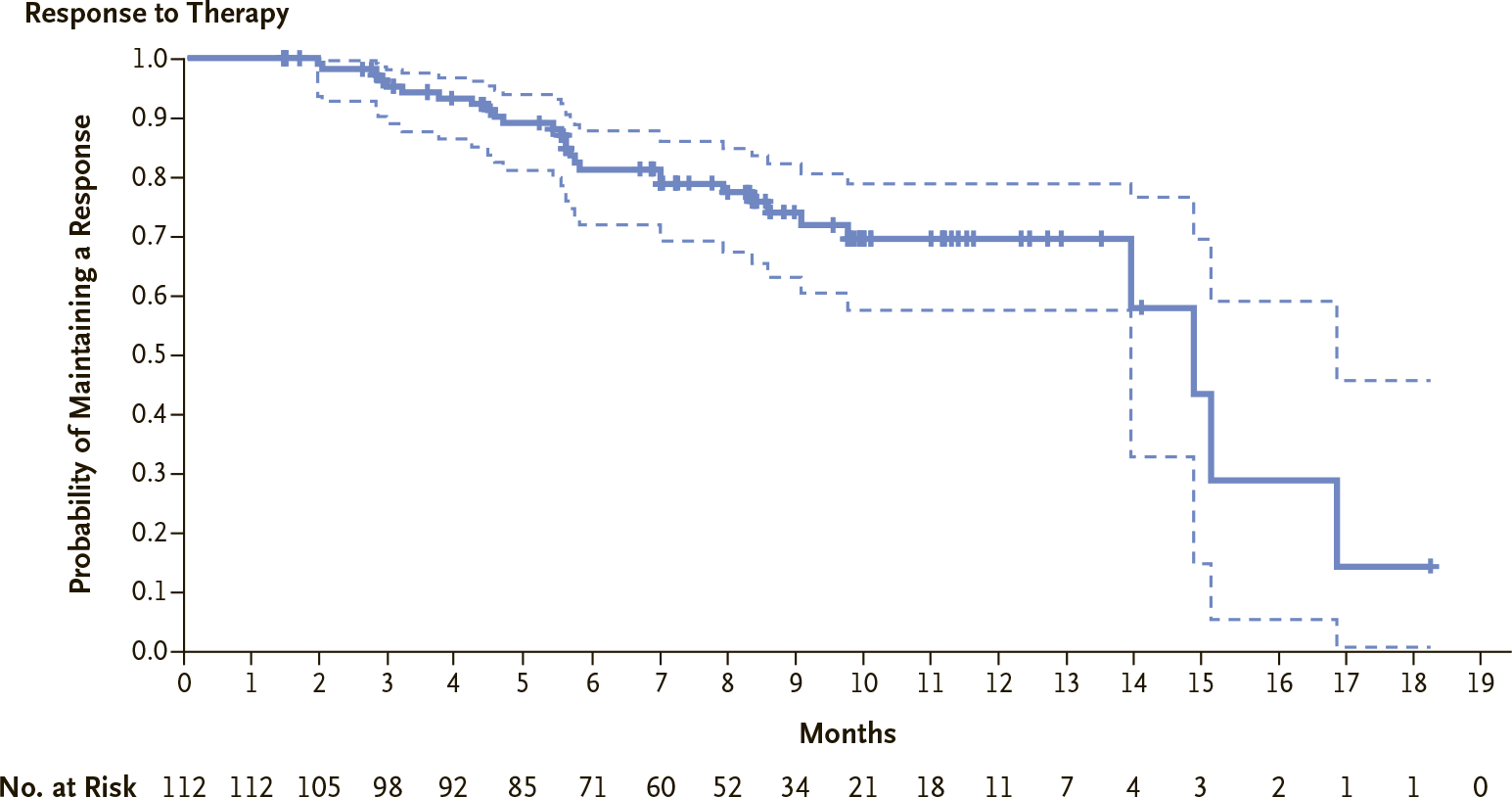
- duration of response (DoR) was a median of 14.8 months (95% CI: 13.8 to 16.9)
- median progression-free survival (PFS) came out to 16.4 months (95% CI: 12.7 to NE)
- median overall survival (OS) was not yet achieved: the estimated probability of OS at 6 months was fair for 93.9% (95% CI: 89.3 to 96.6) of patients, 12 months for 86.2% (95% CI: 79.8 to 90.7).
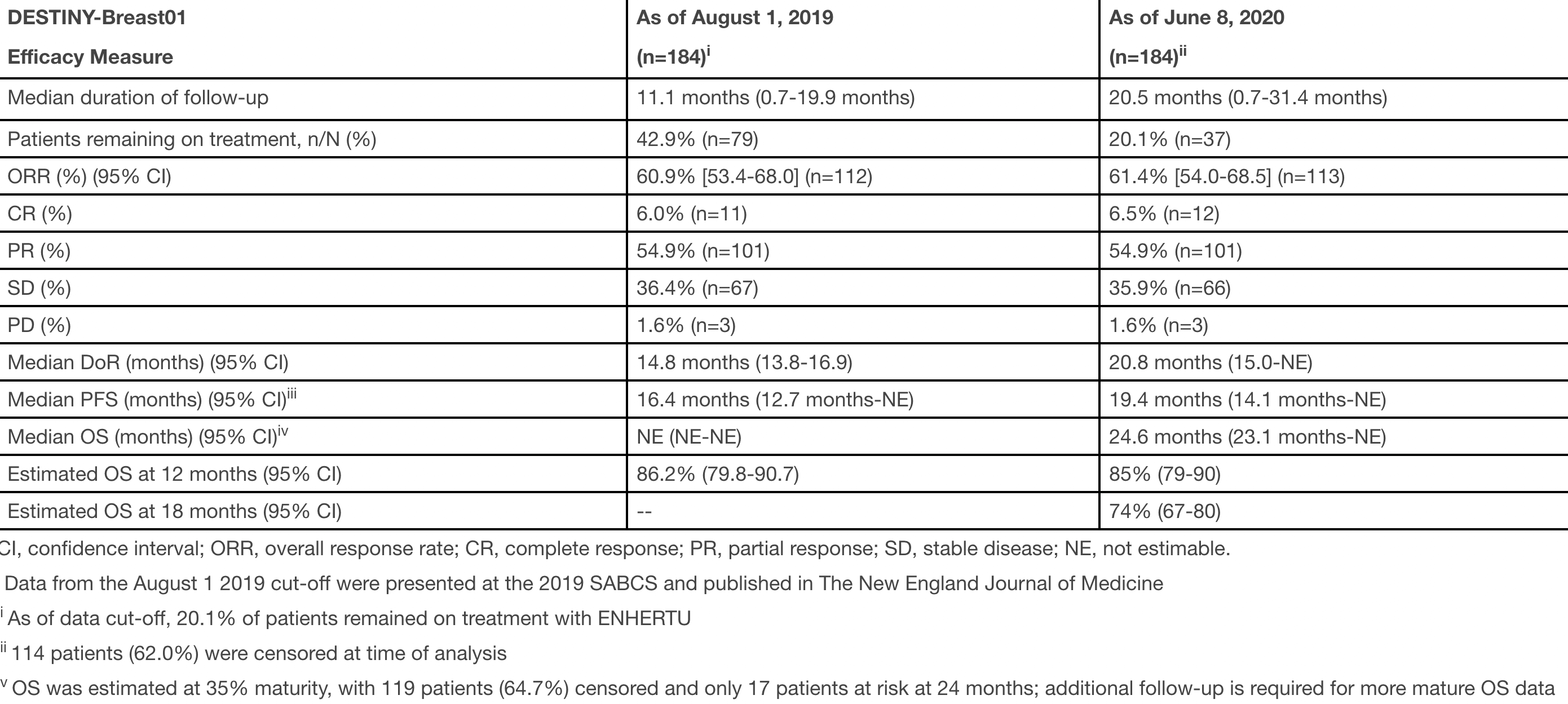
At a median follow-up of 20.5 months (0.7–31.4), prescribing Enhertu for HER2-positive metastatic breast cancer continued to demonstrate the therapeutic efficacy of trastuzumab deruxtecan as follows:
- ORR of 61.4% (95% CI: 54.0 to 68.5), including CR of 6.5% and PR of 54.9%
- median DoR of 20.8 months (95% CI: 20.8 to NE)
- median PFS of 19.4 months (95% CI: 14.1 to NE)
- median OS still had not matured, nearing 24.6 months (23.1–NE), and its estimation for one-third of patients suggested that 85% (95% CI: 79 to 90) of patients would remain alive at least 12 months and 74% (95% CI: 67 to 80) would stay alive at a minimum 18 months.
The median follow-up of 26.5 months recorded the following rates of Enhertu’s therapeutic efficacy:
- ORR of 62,0% (95% CI: 54.4 to 69.0), including CR of 7.1%
- median DoR of 18.2 months (95% CI: 15.0 to NE)
- median PFS of 19.4 months (95% CI: 14.1 to 25.0)
- an exploratory OS analysis with a median follow-up of 31.1 months (95% CI: 30.7 to 32.0), evaluated at a greater maturity (52%) of the accumulated data, found a median OS of 29.1 months (95% CI: 24.6 to 36.1).
DESTINY-Breast03
The DESTINY-Breast03 (NCT03529110) phase 3 (randomized, open-label, active-controlled, multicenter, international) clinical trial invited adult patients (n=524) with HER-positive, unresectable and/or metastatic breast cancer who received prior trastuzumab and taxane therapy for metastatic disease or developed disease recurrence during or within 6 months of completing adjuvant therapy.
The median age of patients was 54 years (20–83), with 80% of participants being younger than 65 years. There were 99.6% women. The disease was characterized by visceral metastases in 73% of the subjects and brain metastases in 16%. Breast cancer was hormone receptor-positive (HR+) in 52% of patients. 48% of patients received one line of systemic therapy for metastatic indications.
Participants were treated with Kadcyla (trastuzumab emtansine) or Enhertu (trastuzumab deruxtecan) until unacceptable toxicity or disease progression.
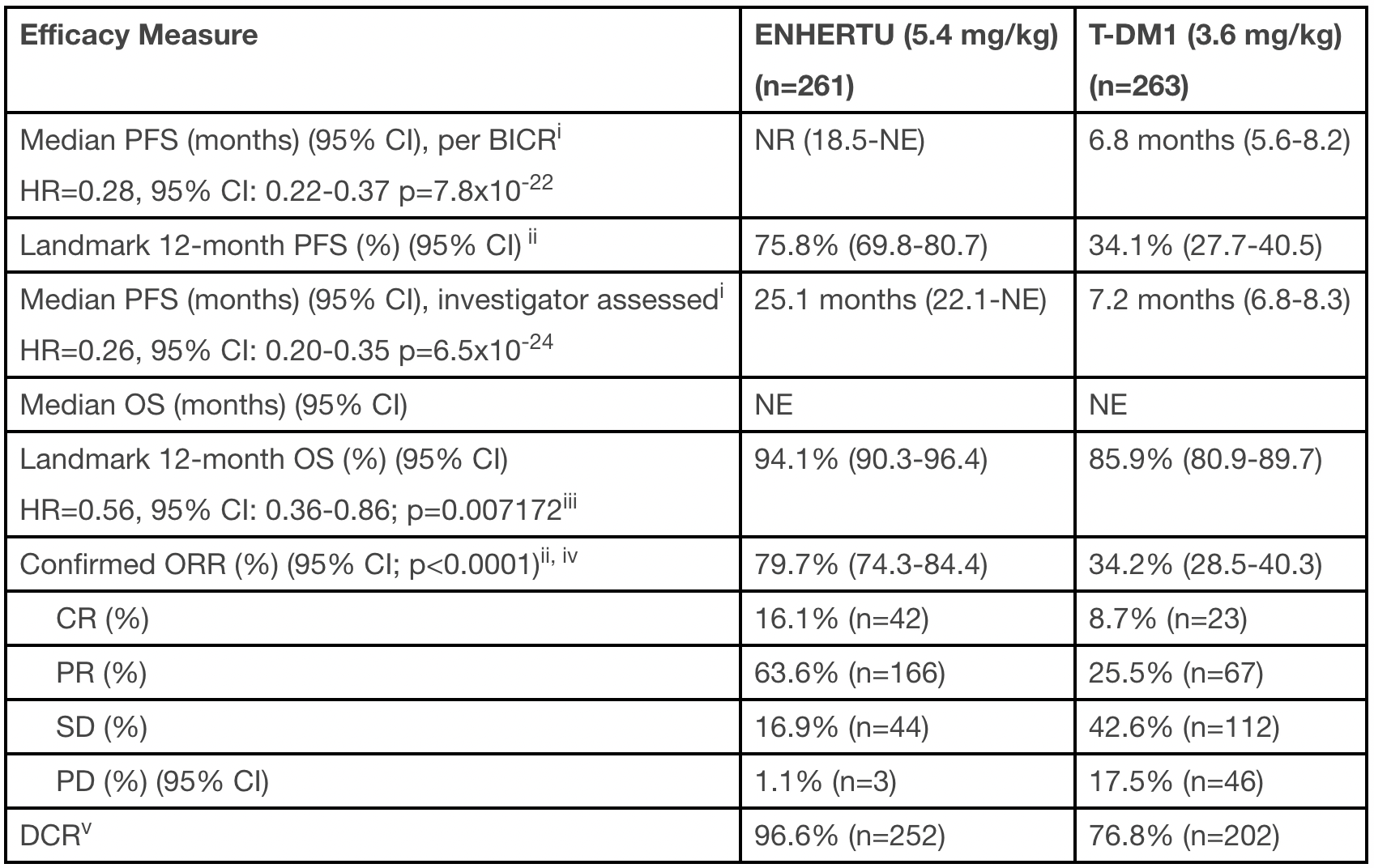
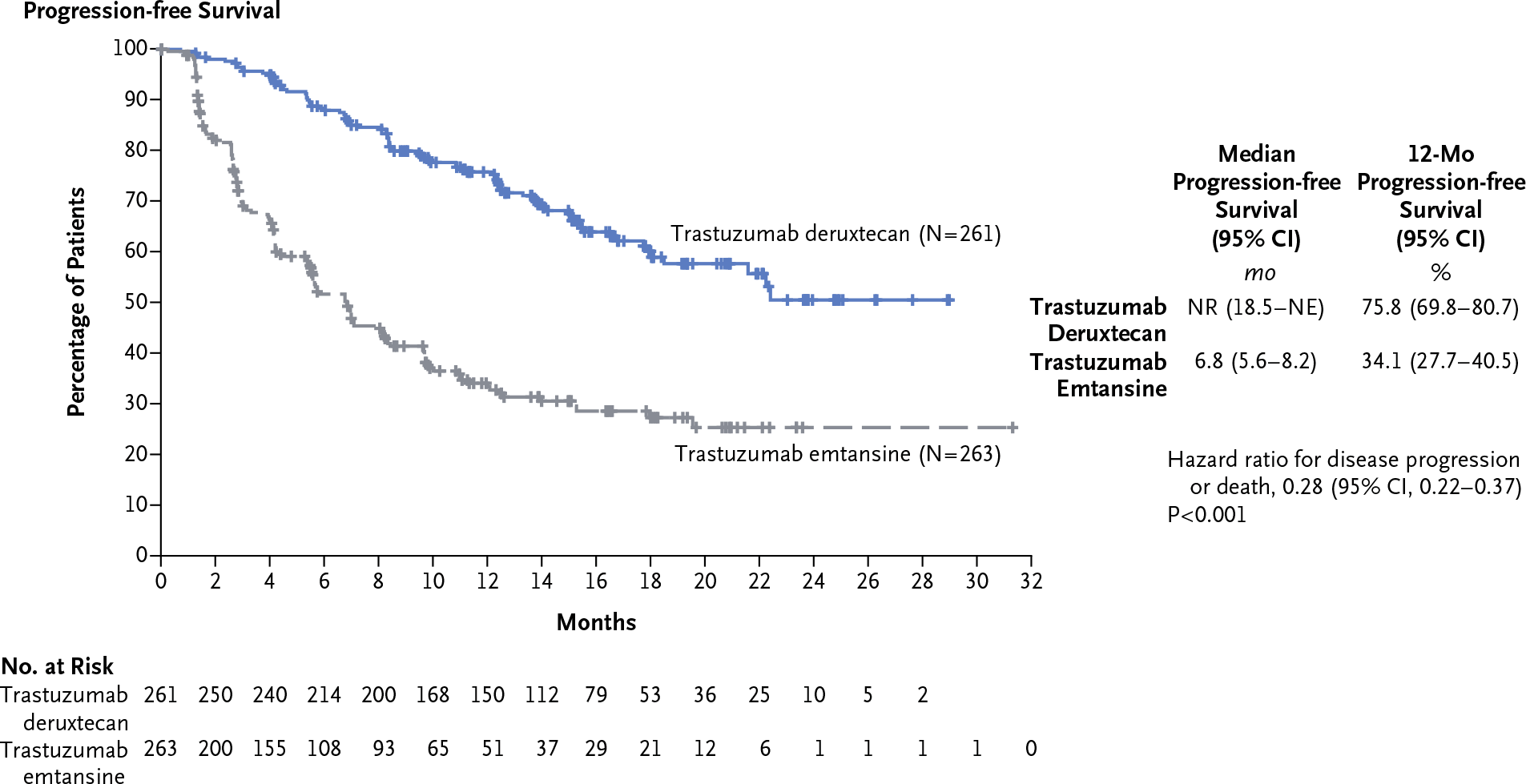
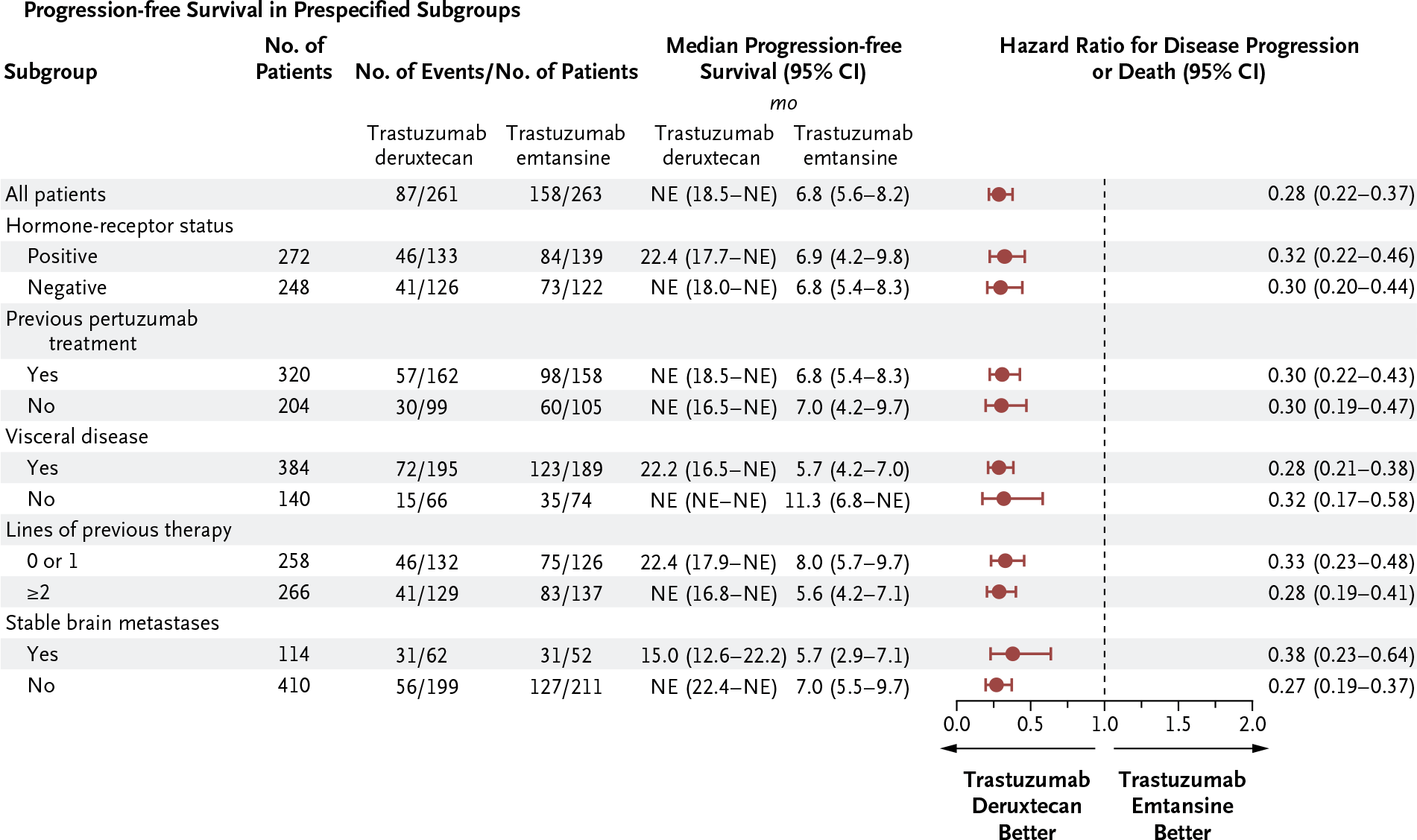
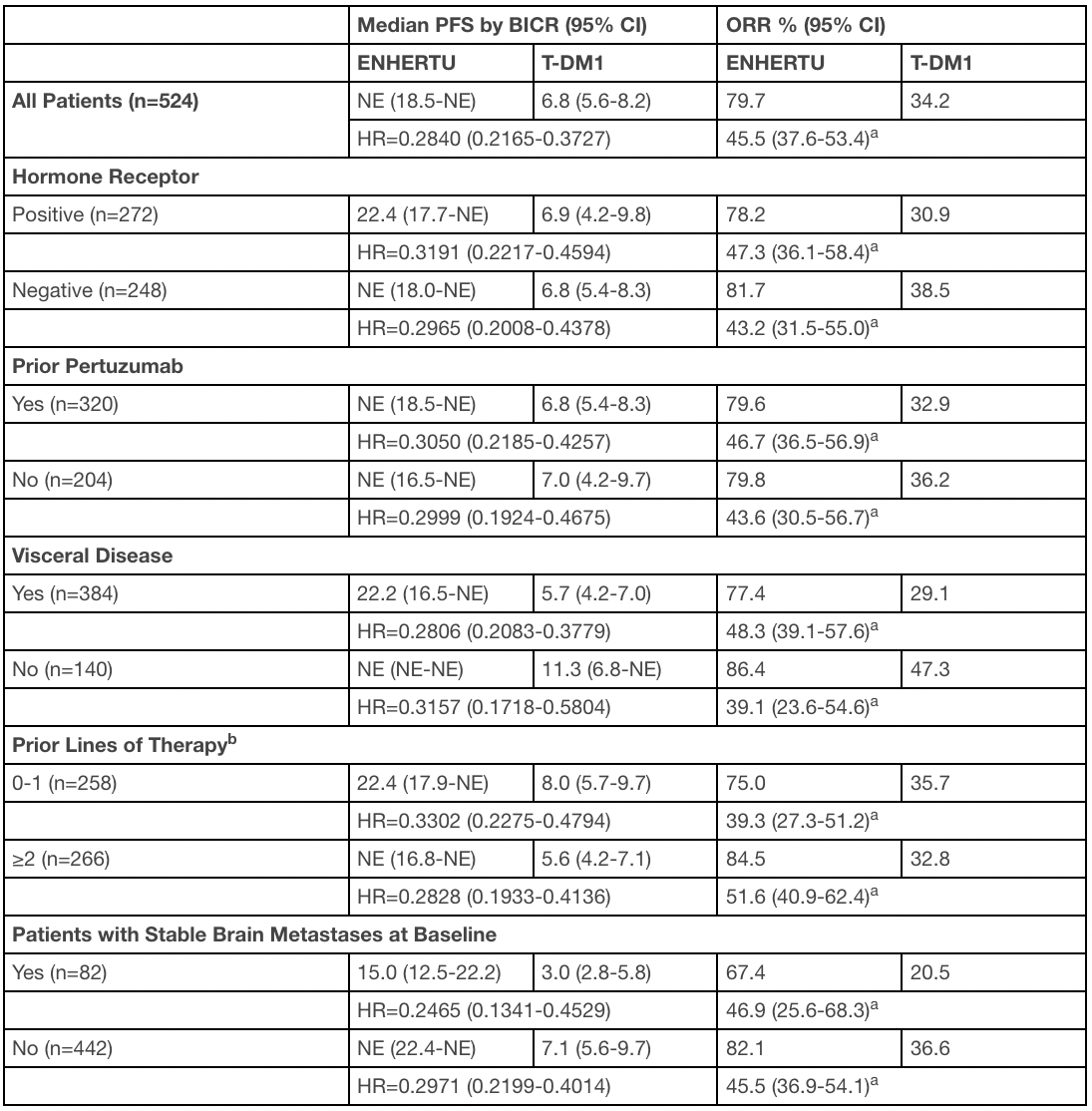
After follow-up for the respective 16.2 and 15.3 month patient groups, the median progression-free survival (PFS) was not reported in the Enhertu group (95% CI: 18.5–NE) — versus 6.8 months (95% CI: 5.6–8.2) in the Kadcyla group, accessed by blinded independent central review (BICR). Administration of Enhertu resulted in a 72% reduction in the risk of disease progression or death relative to use of Kadcyla: hazard ratio (HR) 0.28 (95% CI: 0.22–0.37; p<0.0001).
The investigator assessed that Enhertu therapy more than tripled the duration of PFS compared to standard treatment with Kadcyla: 25.1 months (95% CI: 22.1–NE) — vs. 7.2 months (95% CI: 6.8–8.3). The above relative risk reduction was 74%: HR 0.26 (95% CI: 0.20–0.35; p<0.0001).
Among those receiving trastuzumab deruxtecan, the rate of confirmed overall response (ORR) more than doubled when compared to those treated with trastuzumab emtansine: 82.7% (95% CI: 77.4–87.2), including 15.7% complete response (CR) and 66.9% partial response (PR) — vs. an ORR of 36.1% (95% CI: 30.0–42.5), including CR of 8.3% and PR of 27.8%.
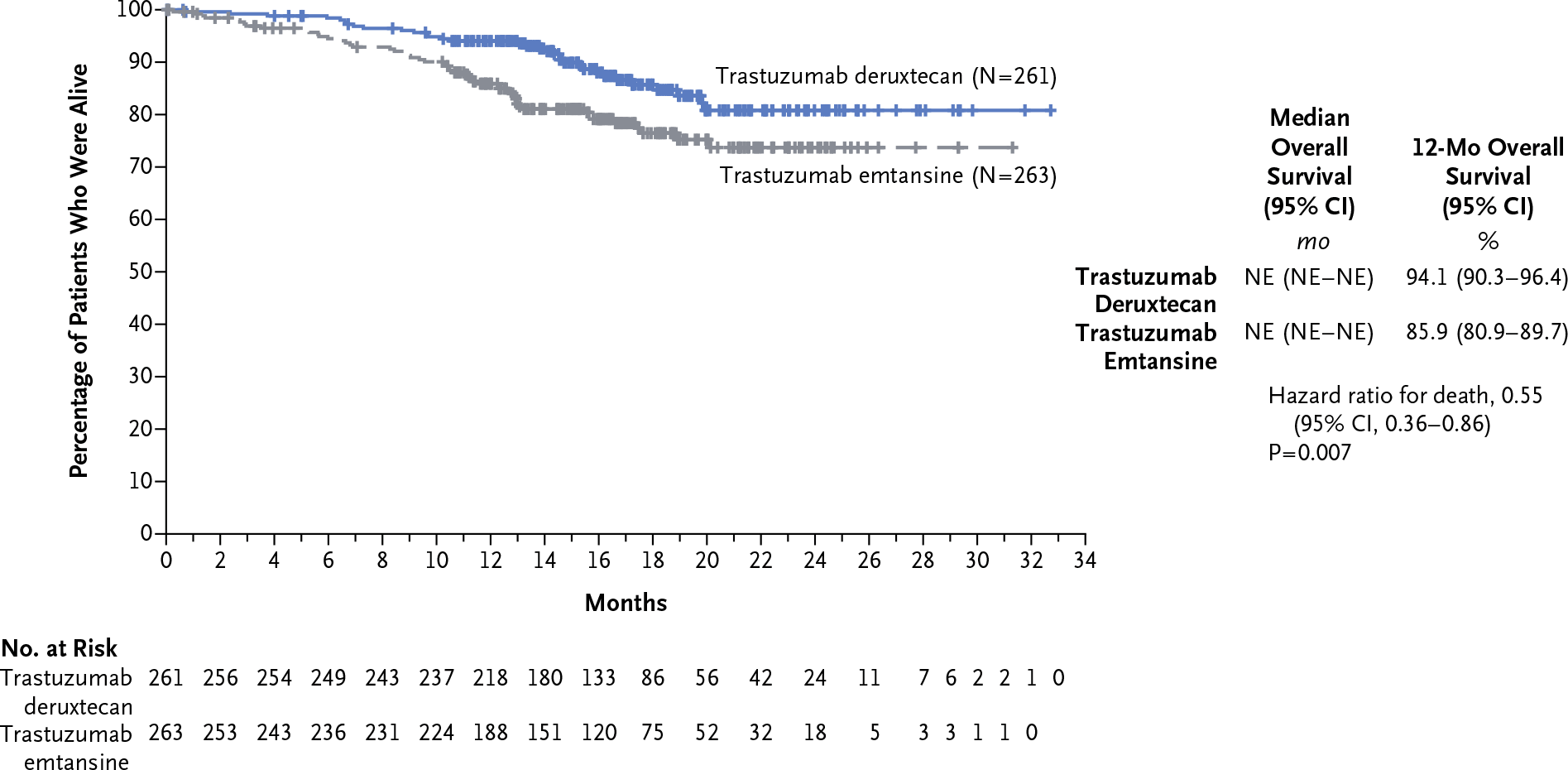
In the Enhertu group, there was a strong trend toward improved overall survival (OS), however, data were not yet mature for analysis: HR 0.55 (95% CI: 0.36–0.86). After one year of treatment, 94.1% (95% CI: 90.3–96.4) of patients in the trastuzumab deruxtecan group remained alive — vs. 85.9% (95% CI: 80.9–89.7) in the trastuzumab emtansine group.
Enhertu consistently and unequivocally outperformed Kadcyla for PFS and ORR in all prespecified patient subgroups defined according to criteria such as hormone receptor status, prior pertuzumab administration, visceral metastasis, number of lines of therapy completed, or stable metastasis to the brain.
Safety
The impressive efficacy of treatment with trastuzumab deruxtecan be paid for by the chance of encountering serious toxicity. The prescribing information of Enhertu carries a black box warning about the risks of severe, life-threatening, or fatal interstitial lung disease (ILD; a group of diseases leading to pulmonary fibrosis), including pneumonitis.
Thus, among patients treated with this drug in the DESTINY-Breast01 (NCT03248492) clinical trial, 9% developed ILD and 2.6% of patients died from it. The median time to manifestation was 4.1 months (1.2–8.3).
Among patients who received Enhertu in the DESTINY-Breast03 (NCT03529110) clinical trial, 10.5% experienced ILD and no fatal outcomes were reported. The median time to manifestation was 5.5 months (1.1–16.7).
Administration of Enhertu during pregnancy may be accompanied by embryofetal toxicity.
The range of common adverse reactions to Enhertu administration is decently wide and includes adverse events (occurred in more than 20% of patients) such as nausea, vomiting, fatigue, alopecia, constipation, anemia, musculoskeletal pain, diarrhea, decreased appetite, anemia, neutropenia, leukopenia, respiratory infections, headache, abdominal pain, thrombocytopenia, cough, stomatitis.
Enhertu: Trastuzumab Deruxtecan Is New Cancer Blockbuster
There is no doubt about Enhertu’s bright future. Patient and physician demand for this drug is so high that it will rapidly earn blockbuster status, easily surpassing the $1 billion annual sales mark.
Industry experts estimate that Enhertu sales will be at least $4 billion in 2026.
If we trust the more optimistic forecasts, which take into account the addition of earlier lines of therapy for breast cancer, the most common cancer in women, as well as other cancers with HER2-positive expression, peak demand for Enhertu is quite capable of getting to $7 billion.

In the context of HER2-positive unresectable and/or metastatic breast cancer, trastuzumab deruxtecan is in the following phase 3 clinical trials:
- DESTINY-Breast02 (NCT03523585). Patients who received anti-HER2 therapy, including Kadcyla. Enhertu versus either Herceptin and capecitabine or lapatinib and capecitabine.
- DESTINY-Breast03 (NCT03529110). Patients previously treated with Herceptin with a taxane. Enhertu versus Kadcyla.
- DESTINY-Breast04 (NCT03734029). Patients with low HER2 expression levels who have not responded to endocrine therapy and have already received 1-2 lines of chemotherapy for metastatic indications. Enhertu versus chemotherapies of choice (capecitabine, eribulin, gemcitabine, paclitaxel, nab-paclitaxel).
- DESTINY-Breast06 (NCT04494425). Patients with low or no HER2 expression levels who have not responded to endocrine therapy and have not previously received chemotherapy for metastatic indications. Enhertu versus chemotherapy of choice (capecitabine, paclitaxel, nab-paclitaxel).
Enhertu is also being rolled out in the DESTINY-Breast05 (NCT04622319) phase 3 clinical trial, which is testing the hypothesis of its applicability in the therapy of HER2-positive breast cancer, that has not fully responded to neoadjuvant treatment (surgical resection with systemic chemotherapy, including taxanes and anti-HER2 drugs) and, being invasive residual, has a high risk of recurrence. A comparison is being made with Kadcyla.
Additionally, Enhertu in combination with AstraZeneca’s PD-L1 blocker Imfinzi (durvalumab) is being tested in the BEGONIA (NCT0374242102) phase 1/2 clinical trial: treatment of locally advanced or metastatic triple-negative breast cancer, previously untreated and characterized by low tumor HER2 expression.
Besides breast cancer, Enhertu is being studied in the treatment of other HER2-positive solid tumors, and phase 2 clinical trials are as follows:
- DESTINY-Gastric01 (NCT03329690). HER2-overexpressing locally advanced or metastatic adenocarcinoma of the stomach or esophageal-gastric junction that had progressed after at least two lines of therapy that included administration of fluoropyrimidine, a platinum-containing drug, trastuzumab. Trastuzumab deruxtecan versus chemotherapeutic irinotecan or paclitaxel.
- DESTINY-Gastric02 (NCT04014075). Unresectable or metastatic HER2-positive adenocarcinoma of the stomach or esophageal-gastric junction that has progressed during or after therapy containing trastuzumab.
- DESTINY-Lung01 (NCT03505710). Unresectable and/or metastatic non-small cell lung cancer (NSCLC) with overexpression and/or activating HER2 mutations, recurrent after or refractory to standard treatment.
- HUDSON (NCT03334617). Locally advanced or metastatic NSCLC that progressed during treatment with a PD-(L)1 blocker and platinum-containing chemotherapy. Trastuzumab deruxtecan in combination with durvalumab.
- DESTINY-CRC01 (NCT03384940). HER2-positive unresectable, recurrent, or metastatic colorectal cancer that has received at least two lines of standard therapy.
- DESTINY-PanTumor02 (NCT04482309). HER2-expressing locally advanced, unresectable, or metastatic solid tumors that have previously been treated, such as bile duct cancer, bladder cancer, cervical cancer, endometrial cancer, epithelial ovarian cancer, pancreatic cancer, and rare tumors.
Extras
Enhertu (trastuzumab deruxtecan). Prescribing information. U.S. [PDF]
Enhertu (trastuzumab deruxtecan). FDA CDER. Multi-disciplinary review and evaluation. [PDF]
Enhertu (trastuzumab deruxtecan). Prescribing information. Europe. [PDF]
Enhertu (trastuzumab deruxtecan). European public assessment report (EPAR). [PDF]
Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020 Feb 13;382(7):610-621. [source]
Trastuzumab deruxtecan (DS-8201a) in patients with advanced HER2-positive breast cancer previously treated with trastuzumab emtansine: a dose-expansion, phase 1 study. Lancet Oncol. 2019 Jun;20(6):816-826. [source]
Profile of trastuzumab deruxtecan in the management of patients with HER2-positive unresectable or metastatic breast cancer: an evidence-based review. Breast Cancer (Dove Med Press). 2021 Feb 25;13:151-159. [source]
A review of fam-trastuzumab deruxtecan-nxki in HER2-positive breast cancer. Ann Pharmacother. 2021 Feb 25;1060028021998320. [source]
Effects of ado-trastuzumab emtansine and fam-trastuzumab deruxtecan on metastatic breast cancer harboring HER2 amplification and the L755S mutation. Oncologist. 2021 Feb 9. [source]