Leqvio (inclisiran), offered by Novartis, is a new drug indicated for add-on therapy to diet in adult patients with primary hypercholesterolemia (heterozygous familial and non-familial) or mixed dyslipidemia.
Leqvio may be used as follows:
- in combination with either statins or with statins and other lipid-lowering therapies if you cannot get to proper low-density lipoprotein (LDL) cholesterol levels even taking the maximum tolerated dose of statin
- alone or in combination with other lipid-lowering therapies if you cannot tolerate statins or they are contraindicated.
In December 2020, the European Medicines Agency (EMA) granted marketing authorization to Leqvio.
At the same time, the U.S. Food and Drug Administration (FDA) has issued a complete response letter (CRL) regarding the new drug application (NDA) for inclisiran. According to the regulator, there are unresolved facility inspection-related conditions that preclude approval of inclisiran. Due to the COVID-19 pandemic, the FDA was unable to inspect the European third-party manufacturer producing the drug. Novartis estimates that inclisiran will not be available in the U.S. until 2022.
In December 2022, the FDA approved Leqvio for use as an adjunct to diet and maximally tolerated statin therapy for the treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease (ASCVD), who require additional lowering of low-density lipoprotein cholesterol (LDL-C).
Novartis priced Leqvio at $3,250 per dose, meaning the first year of treatment will cost $9,750 and subsequent years $6,500.

What Is Unique Feature of Leqvio
The subcutaneously administered Leqvio is characterized by a unique dosing regimen. After the prescription of two loading doses of inclisiran with an interval of 3 months between them, the subsequent administration of the drug is conducted only once every 6 months. In other words, a maintenance dose of Leqvio only once every six months is enough for a therapeutically effective and sustained reduction of LDL cholesterol.
Why It Matters
Cardiovascular diseases (CVDs) are a vast group of pathologies involving the heart and blood vessels. CVDs are the number one cause of death worldwide.
↓
As a diagnostic category, CVDs include four main areas, according to which arteries are affected:
- coronary artery disease (CAD) [also called coronary heart disease (CHD), ischemic heart disease (IHD), or simply heart disease]: manifested by myocardial infarction, angina pectoris, heart failure, coronary death
- cerebrovascular disease (impaired cerebral circulation): manifested by stroke, transient ischemic attack
- peripheral artery disease (PAD): manifested by intermittent claudication
- aortic atherosclerosis, thoracic or abdominal aortic aneurysm.
↓
Coronary artery disease accounts for one-third to half of all CVDs diagnoses and is the most common cause of death.
↓
Atherosclerosis is to blame for the development and progression of coronary artery disease in almost all cases.
↓
Atherosclerosis is a condition in which the inner lumen of arteries narrows due to the subendothelial formation of atheromatous plaques consisting of lipids, cell fragments, smooth muscle cells, collagen, and calcium. The exact cause of the development of atherosclerosis, which can affect any artery in the body, is still unknown. Atherosclerosis begins in adolescence, progressing over time: by the age of 65, it is found to some degree in almost all people.
↓
Among the many risk factors for atherosclerosis, hypercholesterolemia — elevated levels of low-density lipoprotein (LDL) cholesterol — holds a special place. It has been proven that its reduction many times decreases the risk of developing and worsening atherosclerosis, both in primary prevention and secondary prevention.
↓
Statins are the standard hypolipidemic drugs but their effectiveness varies enormously among individual patients with nearly 80% of people failing to reduce LDL cholesterol to acceptable levels. Again, some patients are intolerant to statins: usually because of adverse reactions in the form of myalgia and general weakness, two-thirds stop taking statins after a year of use. This is why there is a high unmet medical need for new effective and safe pharmacological ways to control LDL cholesterol.
Leqvio: Mechanism of Action of Inclisiran
The low-density lipoprotein receptor (LDL-R) is a mosaic protein that mediates endocytosis of cholesterol-rich LDL. LDL receptors are the primary receptors for the transport of LDL from the systemic bloodstream into cells; each carries 3,000–6,000 molecules of fat (including cholesterol).
In other words, LDL-Rs maintain plasma LDL levels. At the same time, the liver is responsible for eliminating approximately 70% of circulating LDL. The more extensive the available pool of LDL-Rs, the more efficient is the transport of cholesterol and the lower is its concentration in plasma.
Proprotein convertase subtilisin/kexin type 9 (PCSK9) is one of the most important regulators of LDL cholesterol metabolism. This enzyme binds to LDL-Rs on the surface of hepatocytes. As a result, instead of following their physiological pathway of recycling back to the hepatocyte membrane, they are redirected to lysomal destruction in the liver. As the pool of free LDL-Rs is reduced, plasma levels of LDL cholesterol increase. PCSK9 also inhibits intracellular degradation of apolipoprotein A (ApoB), a protein that is part of LDL particles and very-low-density lipoproteins (VLDL).
Inclisiran disrupts PCSK9 synthesis which leads to a corresponding increase in the number of LDL-Rs that contribute to the clearance of LDL cholesterol from the plasma.

The mechanism of action of inclisiran is based on the principles of RNA interference (RNAi), a natural cellular process of silencing (suppression of expression) of genes. Inclisiran is implemented by small interfering RNAi (siRNA) molecules that mediate RNAi. Inclisiran is conjugated to N-acetylgalactosamine (GalNAc), an amino sugar derivative of galactose, which stabilizes, enhances and prolongs the therapeutic chemistry of siRNA. Since GalNAc binds to asialoglycoprotein receptors that are abundantly expressed in the liver, inclisiran enters mainly the hepatocytes where it interferes with PCSK9 synthesis. This is accomplished by binding siRNA molecules to the RNA-induced silencing complex (RISC) with further cleavage of the matrix RNA (mRNA) encoding PCSK9.
Leqvio: Efficacy and Safety of Inclisiran
Regulatory approval was granted to Leqvio based on the results of three Phase 3 (randomized, double-blind, placebo-controlled, multicenter) pivotal clinical trials that examined the efficacy and safety of inclisiran. Patients were mostly on statin therapy (and at the maximum tolerated dose) with some also receiving ezetimibe. Overall, the administration of Lequio resulted in a 51% reduction in LDL cholesterol levels over a 17-month course of treatment.

The summary results are as follows:
- ORION-9 (NCT03397121). Treatment of patients (n=482) with heterozygous familial hypercholesterolemia (HeFH). After 17 months of therapy, the inclisiran group showed a 40% decrease in LDL cholesterol levels — versus an 8% increase in the placebo group; the difference was −48% (p<0.0001).
- ORION-10 (NCT03399370). Treatment of patients (n=1561) [US only] with atherosclerotic cardiovascular disease (ASCVD). After 17 months of therapy, the inclisiran group showed a 51% decrease in LDL cholesterol levels, whereas the placebo group, by contrast, showed a 1% rise; the difference was −52% (p<0.00001).
- ORION-11 (NCT03400800). Treatment of adult patients (n=1617) [outside the United States] with ASCVD (coronary artery disease, cardiovascular disease, or peripheral artery disease) or increased risk of ASCVD developing (type 2 diabetes, familial hypercholesterolemia, or greater than 20% chance of a cardiovascular event in the next 10 years on the Framingham Risk Score). After 17 months of therapy, the inclisiran group showed a 46% drop in LDL cholesterol — vs. a 4% increase in the placebo group; the difference was −50% (p<0.00001).
To date, inclisiran has collected data in three pivotal phase 3 clinical trials (randomized, double-blind, placebo-controlled, multicenter).
Participants’ baseline laboratory values: serum LDL cholesterol ≥1.8 mmol/L (≥70 mg/dL) [for HeFH, ≥2.6 mmol/L (≥100 mg/dL)] and fasting triglycerides <4.52 mmol/L (<400 mg/dL).
Patients had to adhere to statin therapy at the maximum tolerated dose. Those who were not taking statins had to have documented evidence of intolerance to any dose of at least two drugs in this class. Ezetimibe was allowed to be used.
Subjects were given subcutaneously 300 mg of inclisiran or placebo on the first day and after three months, and then every six months thereafter.
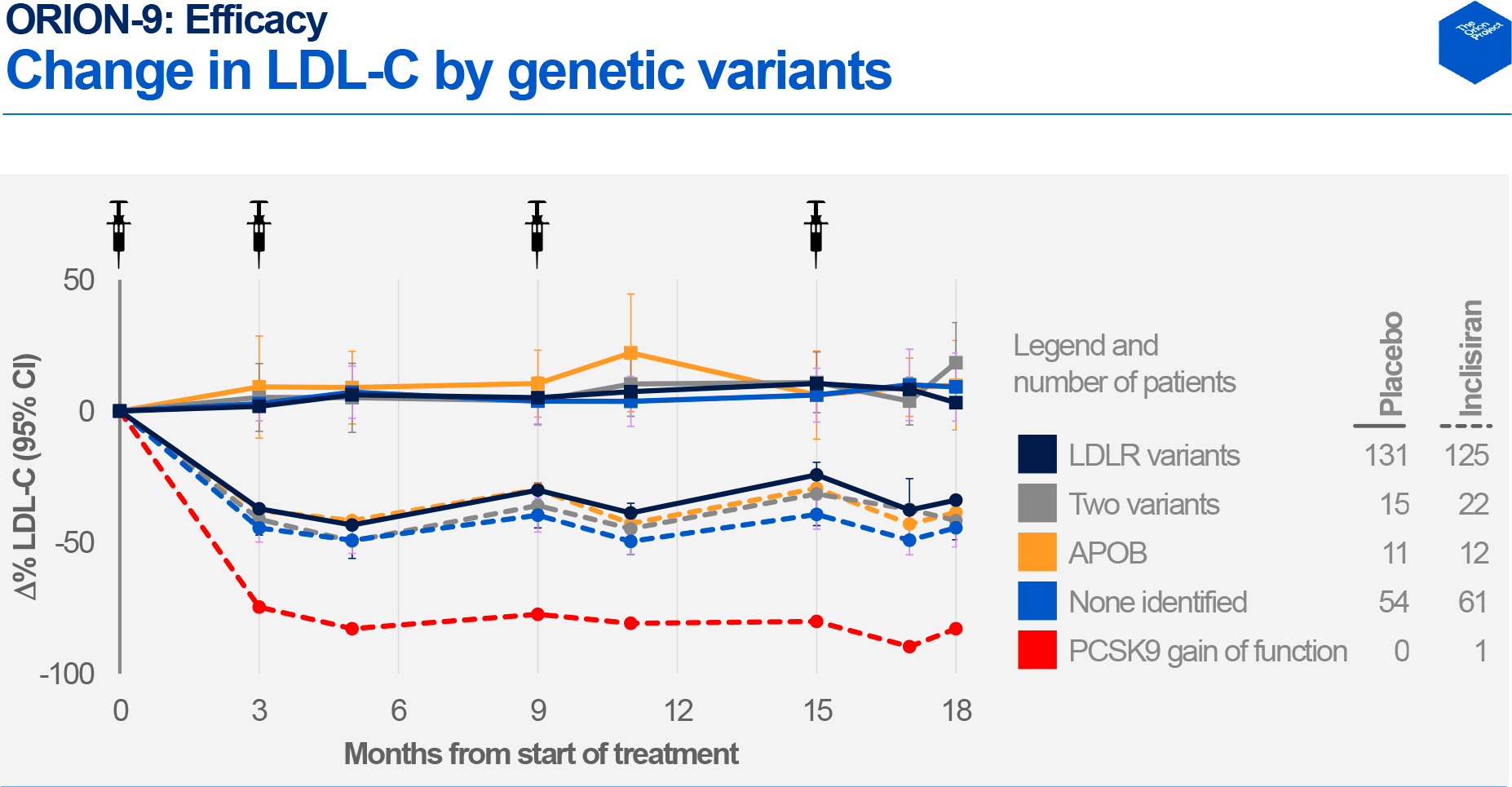
The ORION-9 (NCT03397121) clinical trial involved adult patients (n=482) with heterozygous familial hypercholesterolemia (HeFH) confirmed clinically or genetically.
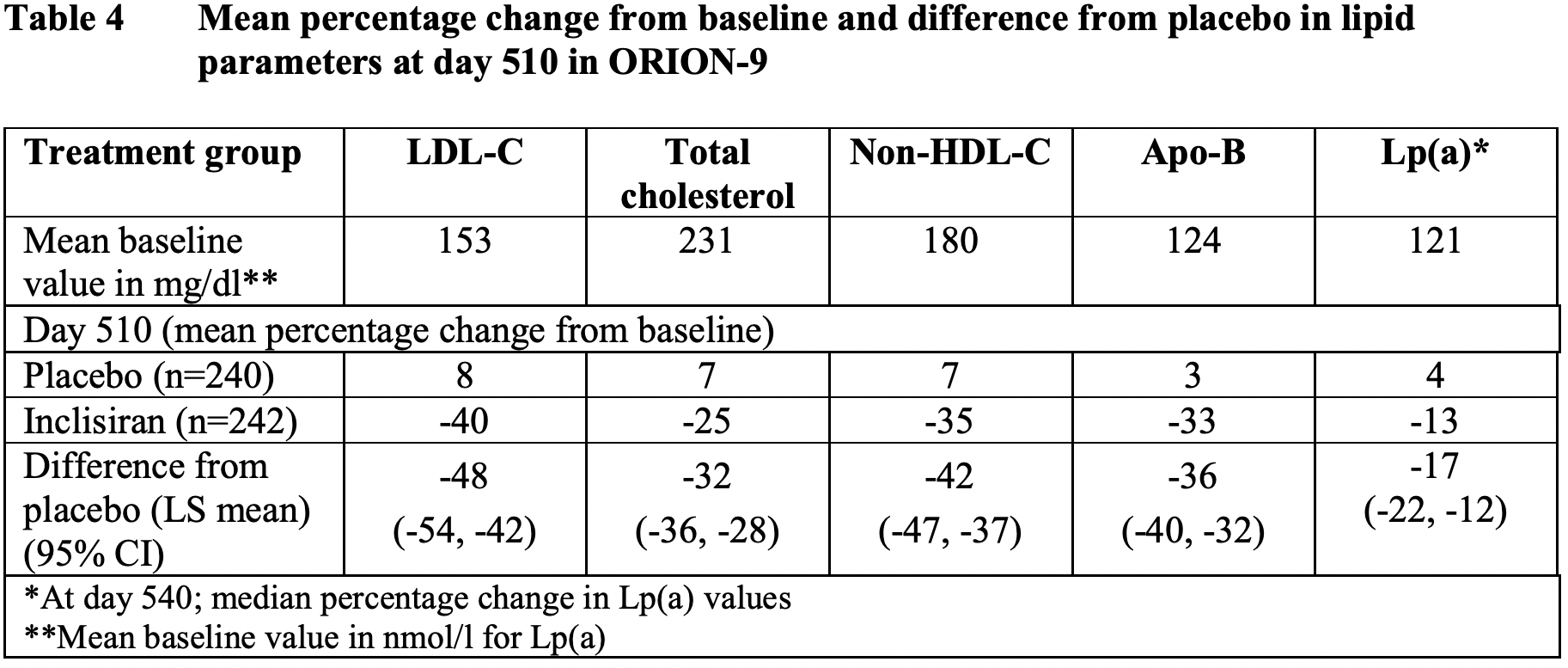
After 17 months, there was a change in the levels of the following lipid parameters in the inclisiran group compared to the placebo group:
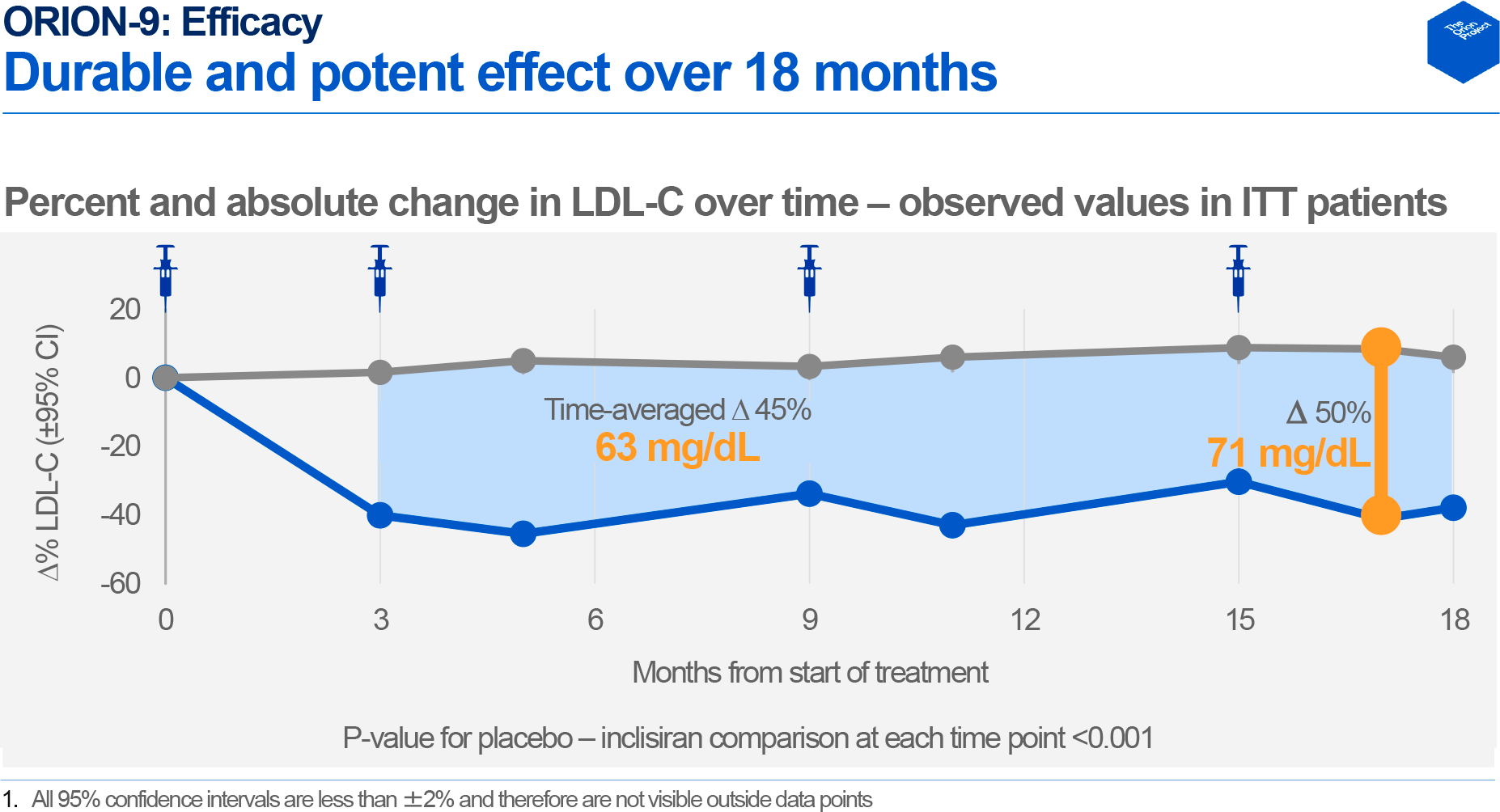
- LDL cholesterol (LDL-C): −40% — vs +8%; the difference was −48% (95% CI: −54 — −42)
- total cholesterol (TC): −25% — vs. +7%; −32% (95% CI: −36 — −28)
- non-high-density lipoprotein cholesterol (non-HDL-C): −35% — vs. +7%; −42% (95% CI: −47 — −37)
- apolipoprotein B (ApoB): −33% — vs. +3%; −36% (95% CI: −40 — −32)
- lipoprotein(a) [Lp(a)]: −13% — vs. +4%; −17% (95% CI: −22 — −12).
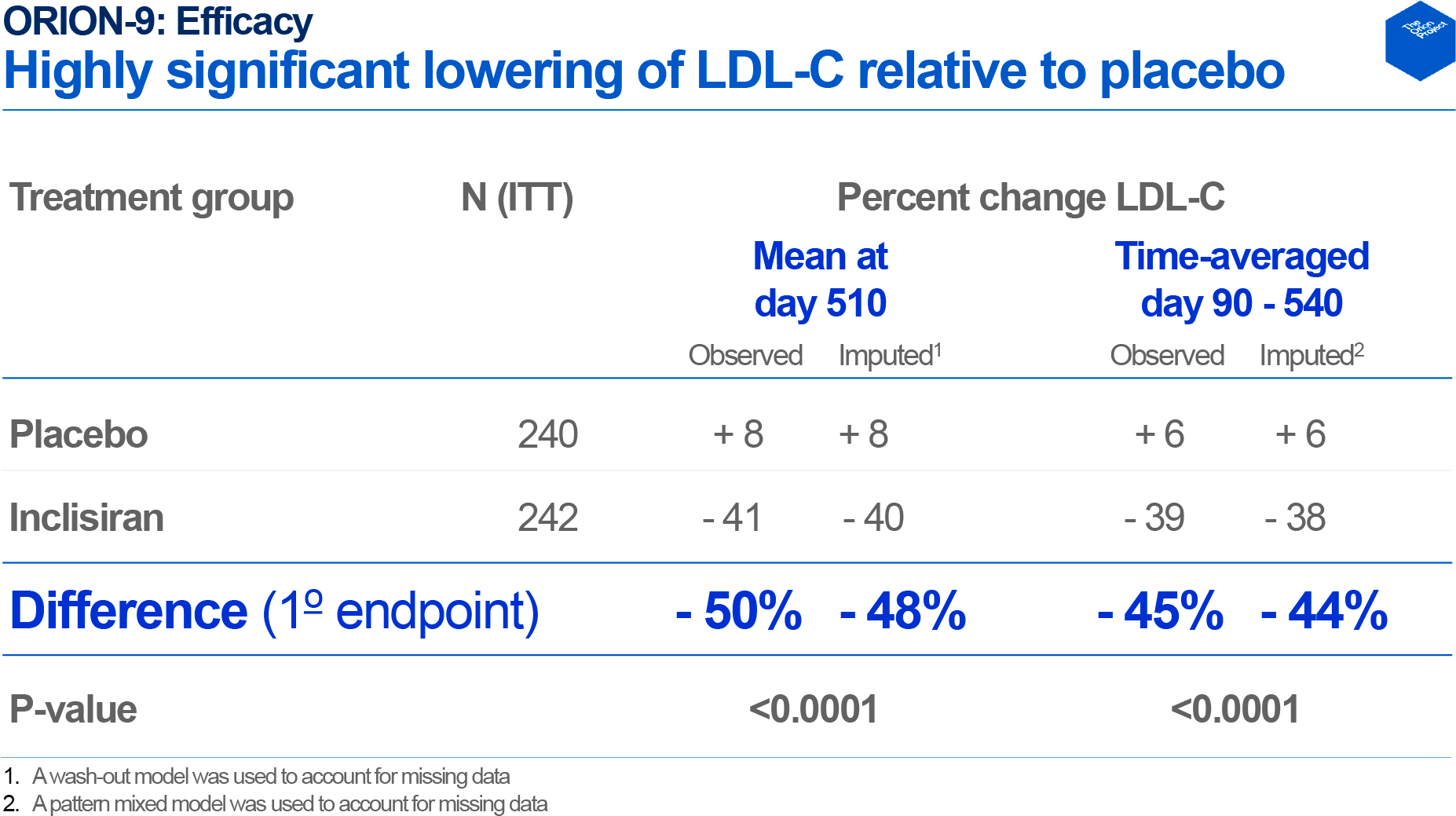
Between 3–18 months, the average difference in LDL-C with the control group came out to −45%: −39% vs +6%.
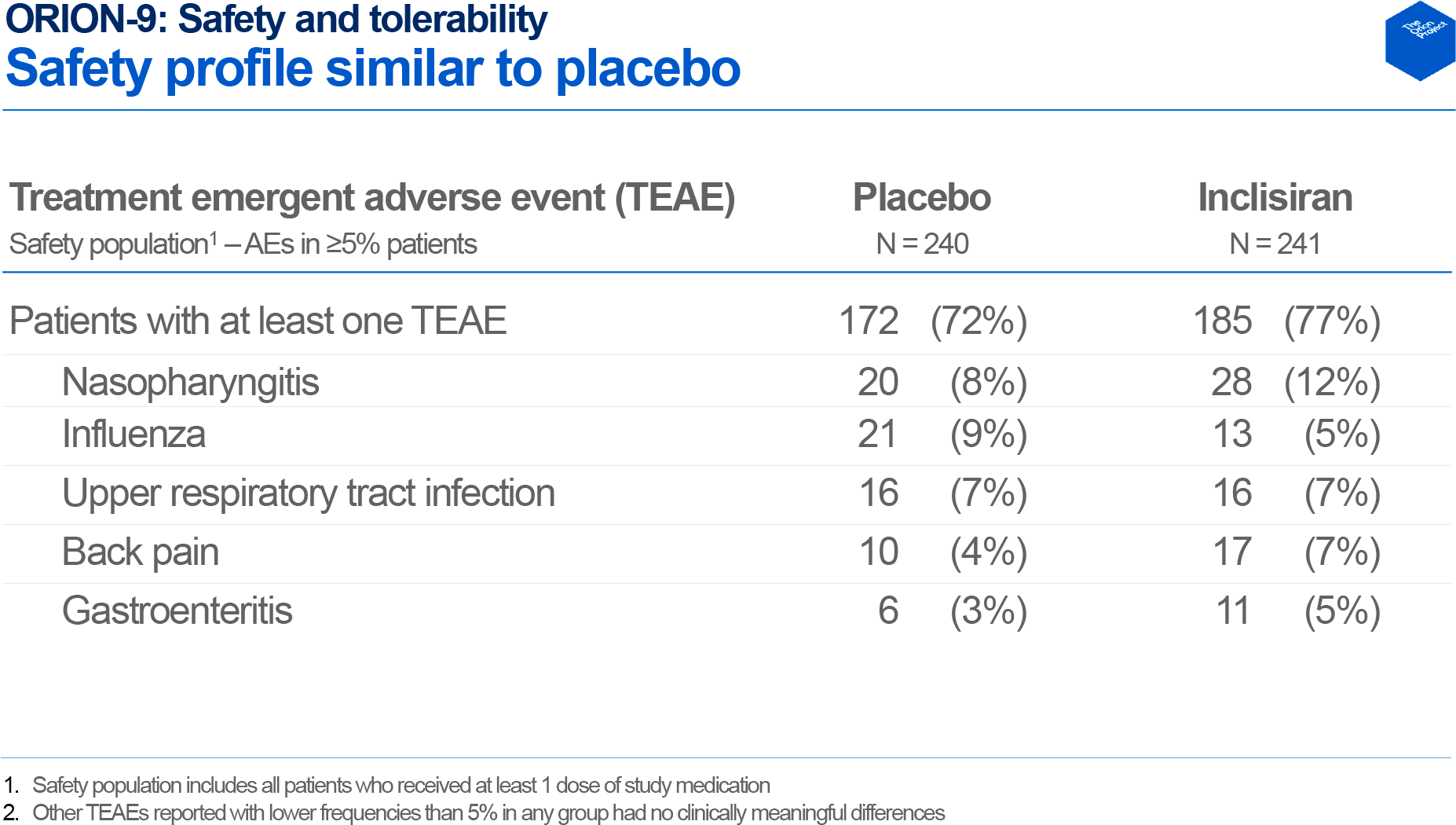
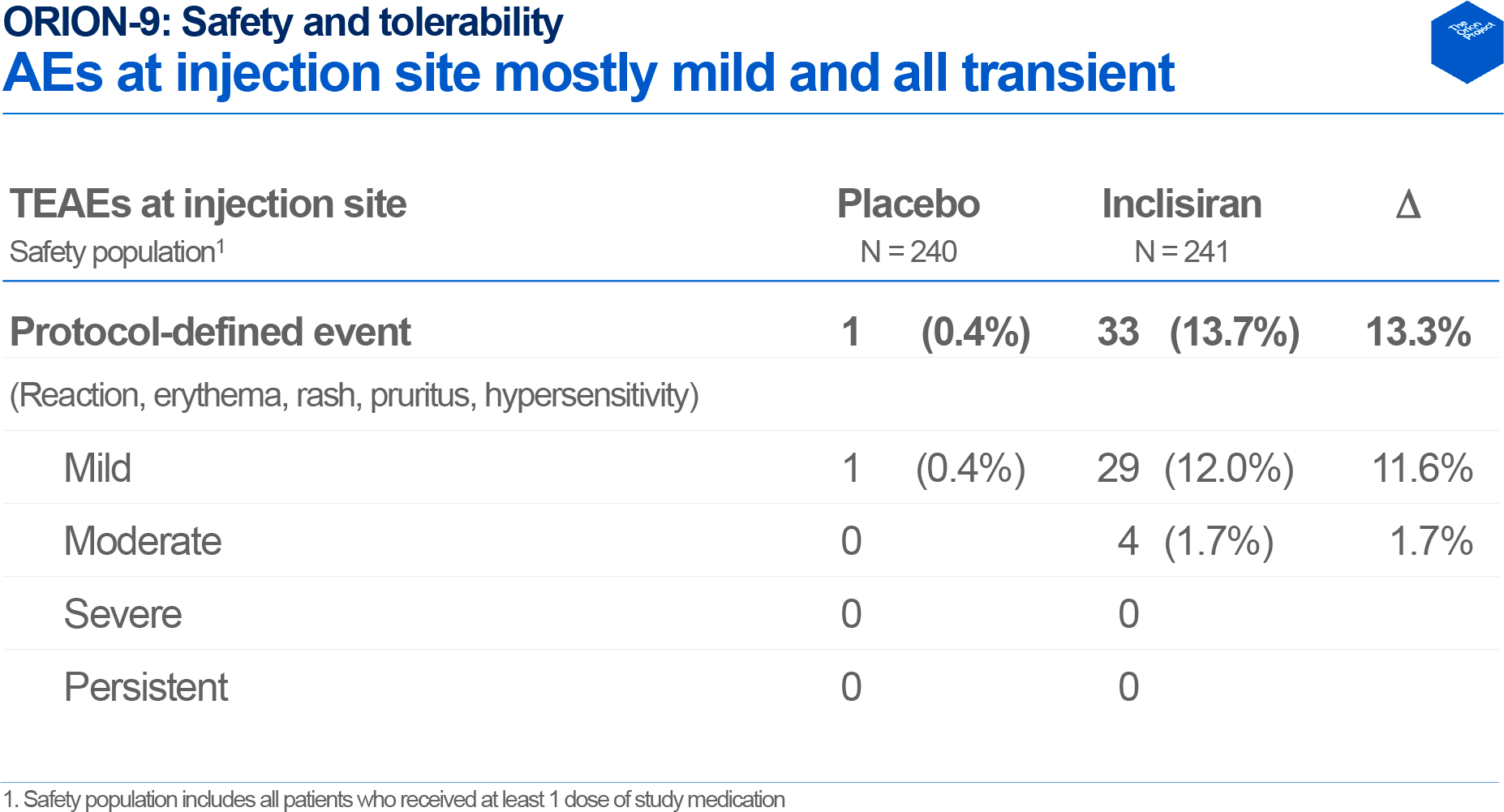
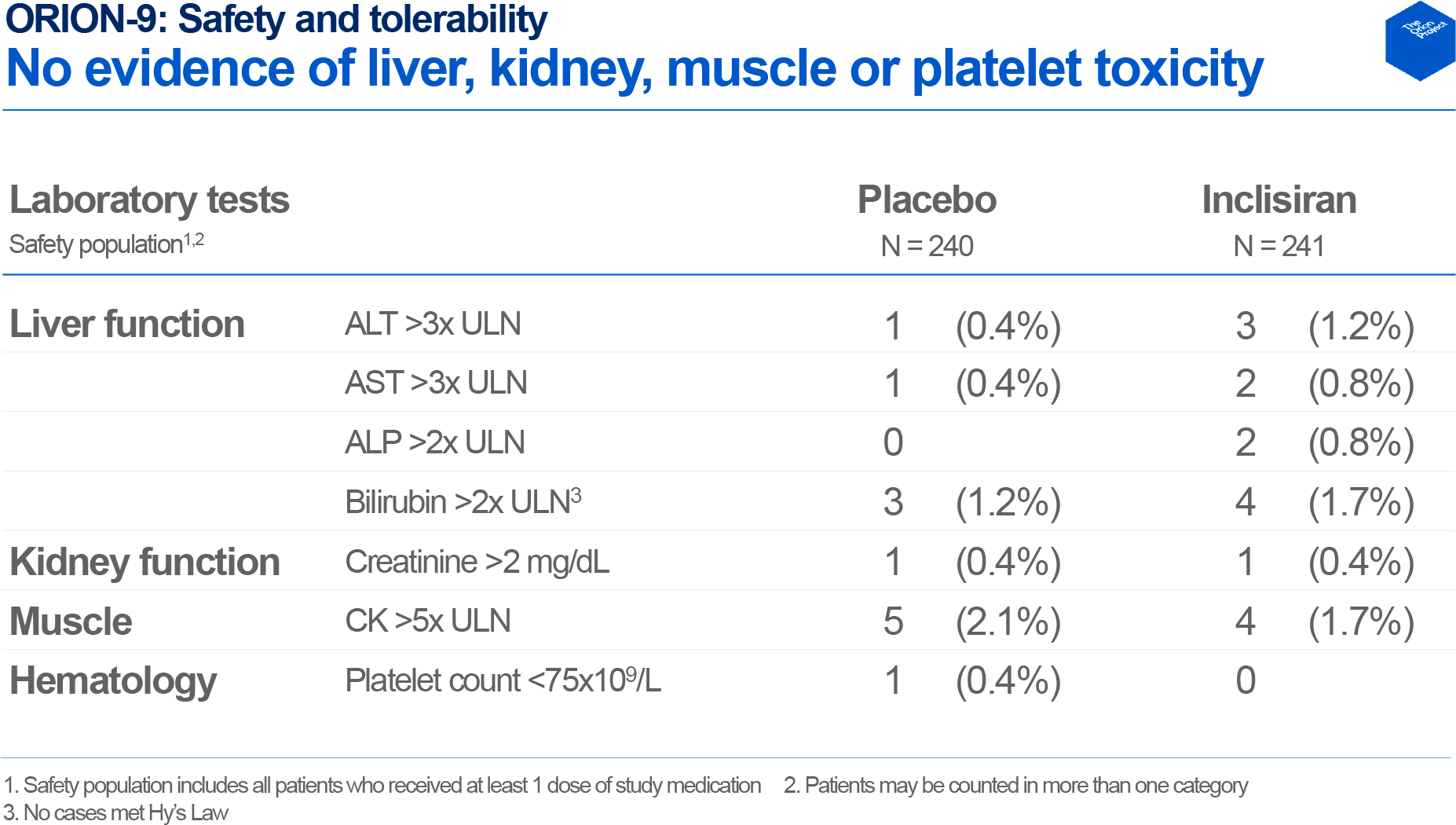
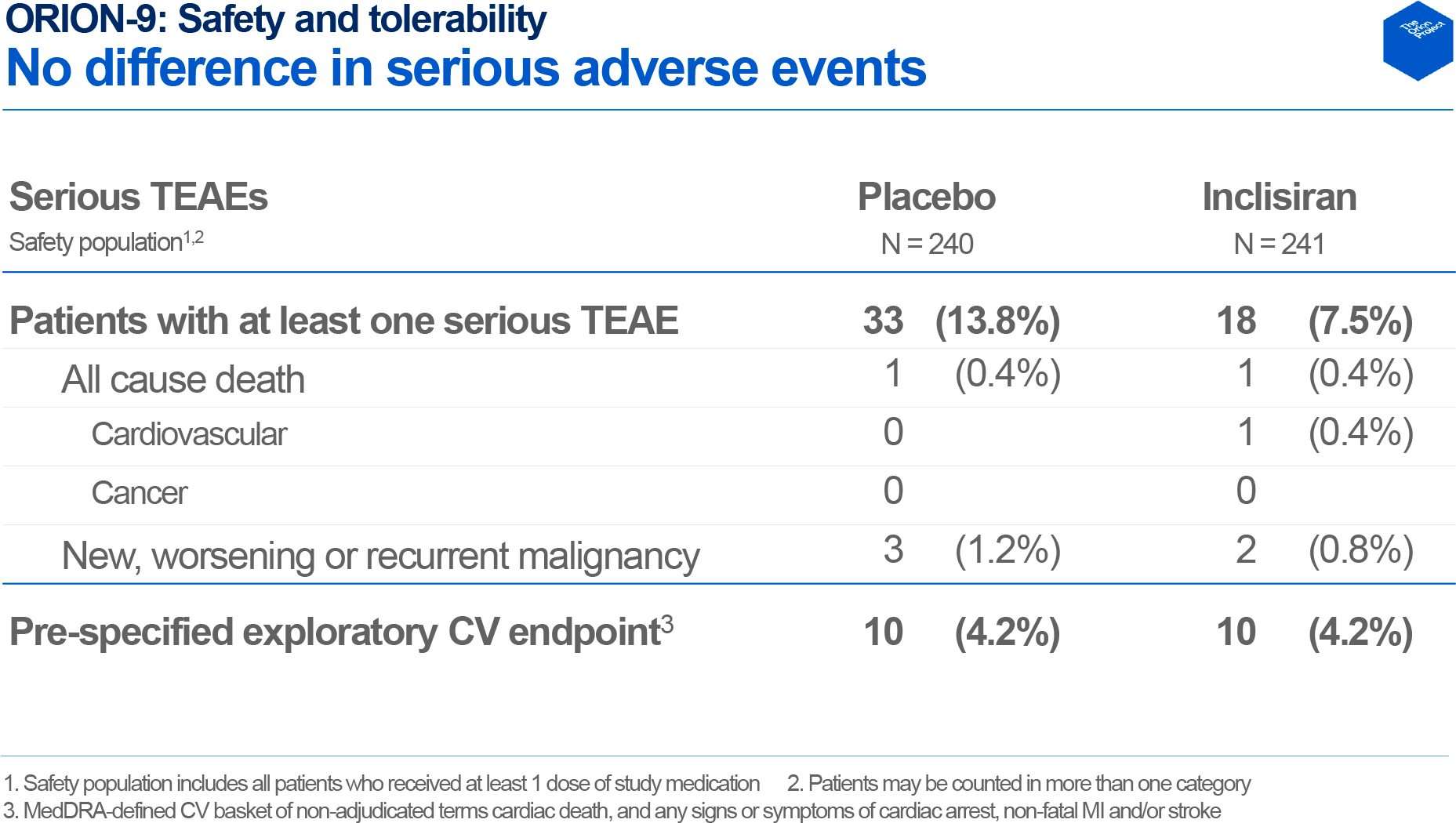
The adverse reaction profiles of the inclisiran and placebo groups were generally similar, with 7.5% of subjects (n=18/241) in the Leqvio group and 13.8% (n=33/240) in the control group experiencing severe adverse events. The prevalence of fatalities and malignancies was comparable: 0.4% vs. 0.4% and 0.8% vs. 1.3%, respectively. There were low rates of clinically significant increases in liver transaminases: ALT 1.2% vs. 0.4%, AST 0.8% vs. 0.4%, while none of these events was associated with inclisiran therapy. Leqvio administration was associated with injection site reactions which, however, were mild and transient: 13.7% (n=33/241) vs. 0.4% (n=1/240).
The ORION-10 (NCT03399370) clinical trial invited US adult patients (n=1561) with atherosclerotic cardiovascular disease (ASCVD).
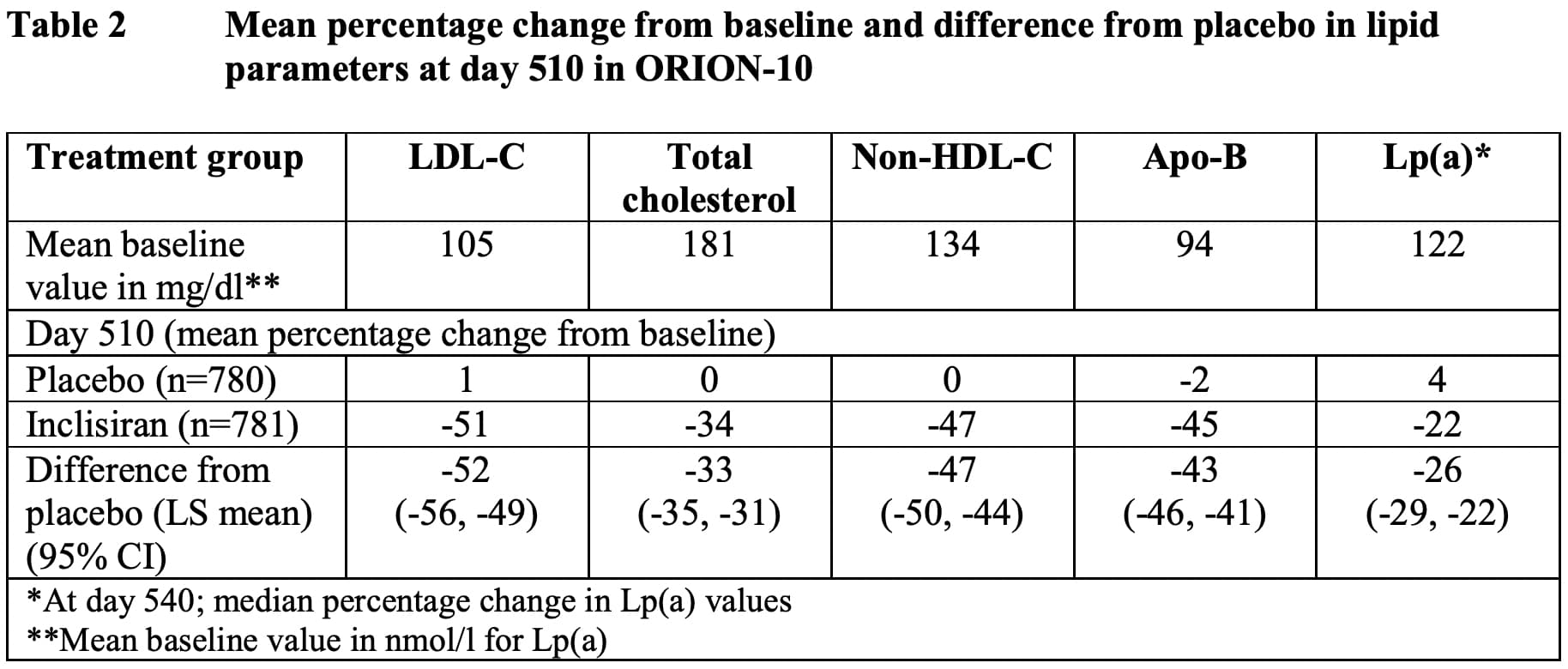
After 17 months, there was a change in the levels of the following lipid parameters in the inclisiran group compared to the placebo group:
- LDL-C: −51% — vs +1%; the difference was −52% (95% CI: −56 — −49)
- TC: −34% — vs. +0%; −33% (95% CI: −35 — −31)
- non-HDL-C: −47% — vs. 0%; −47% (95% CI: −50 — −44)
- ApoB: −45% — vs. −2%; −43% (95% CI: −46 — −41)
- Lp(a): −22% — vs. +4%; −26% (95% CI: −29 — −22).
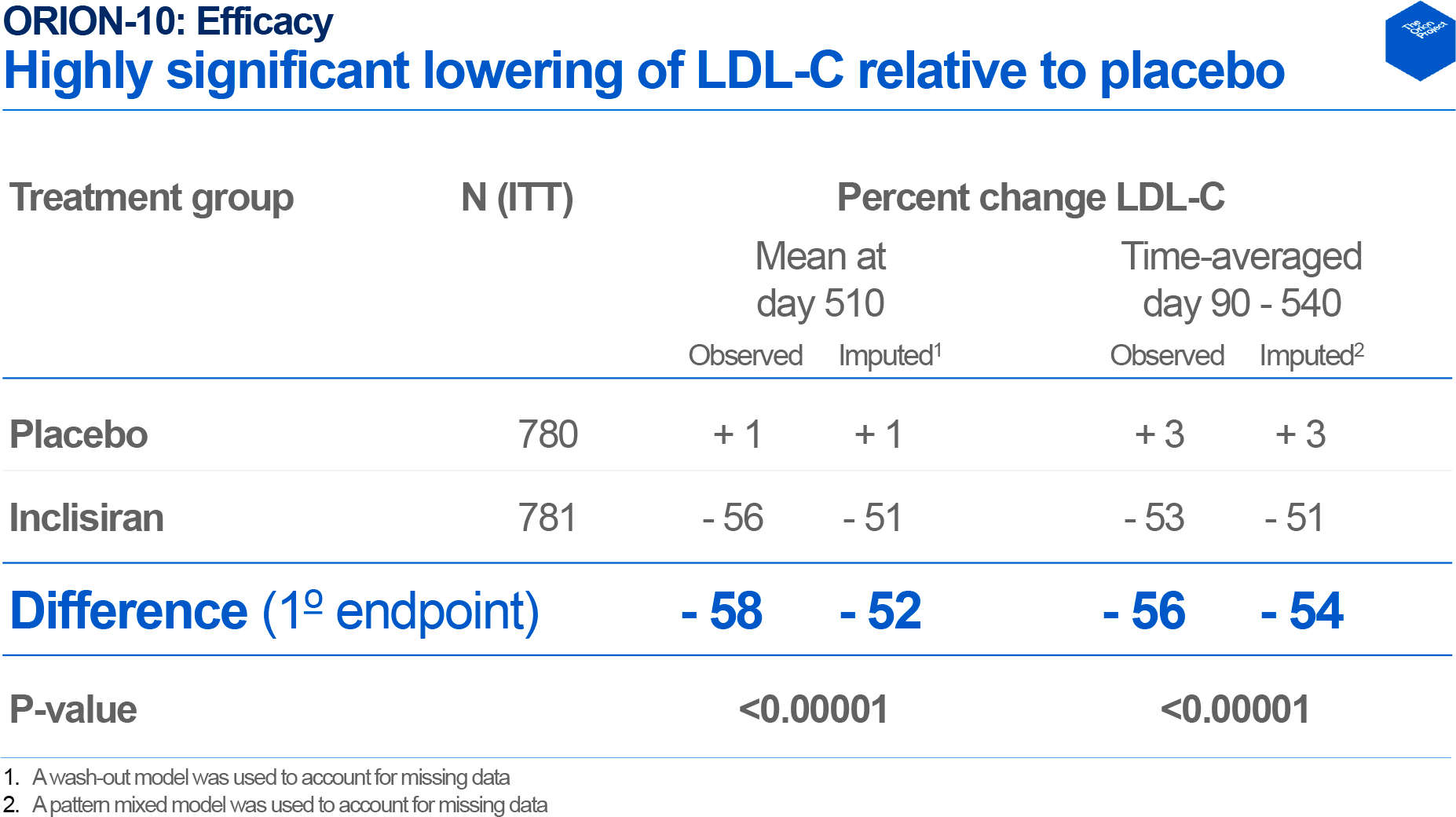
Inclisiran administration fixed an average drop in LDL cholesterol of 53% between 3–18 months, while the control group added 3%; the resulting difference was −56%.

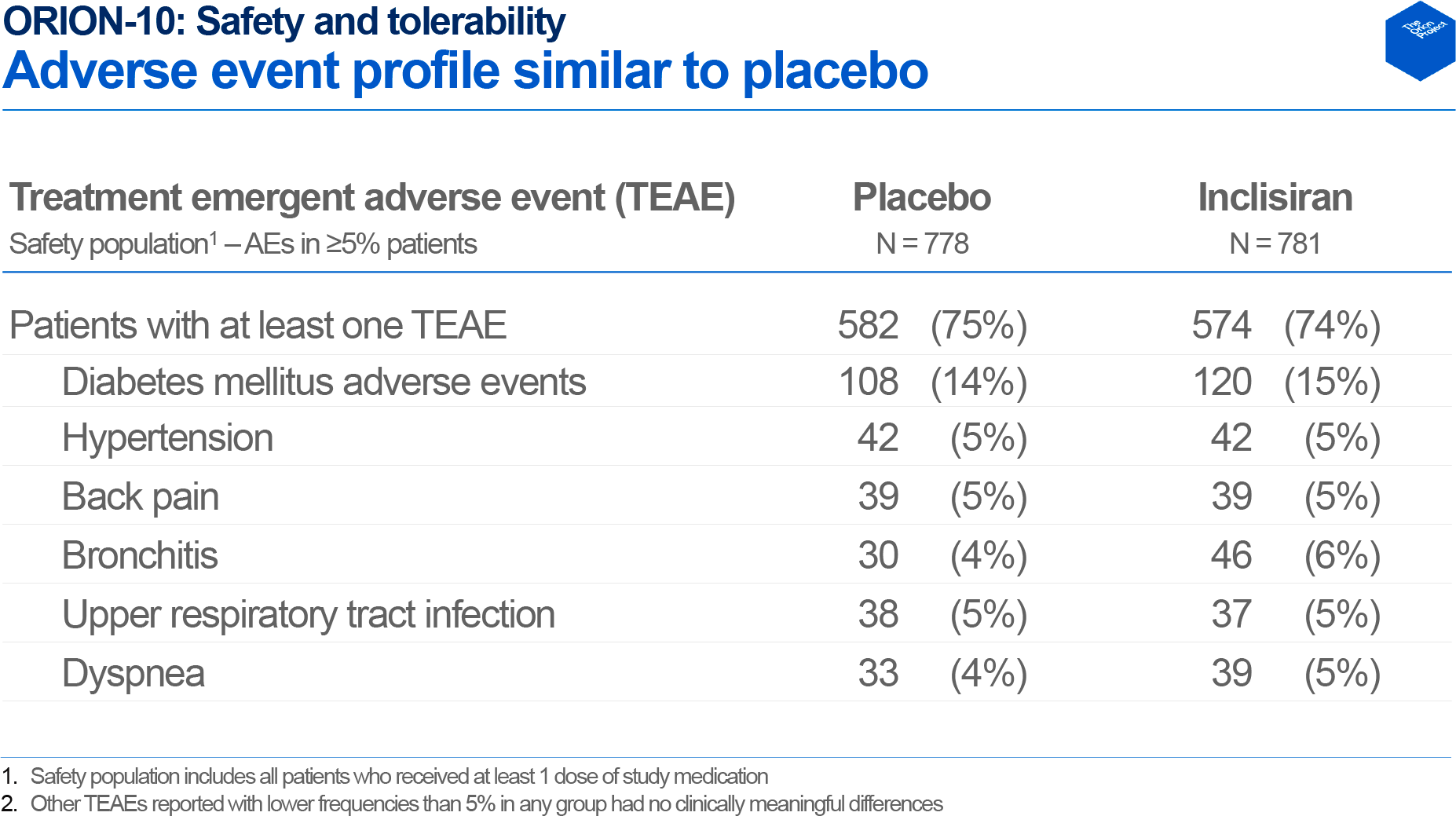
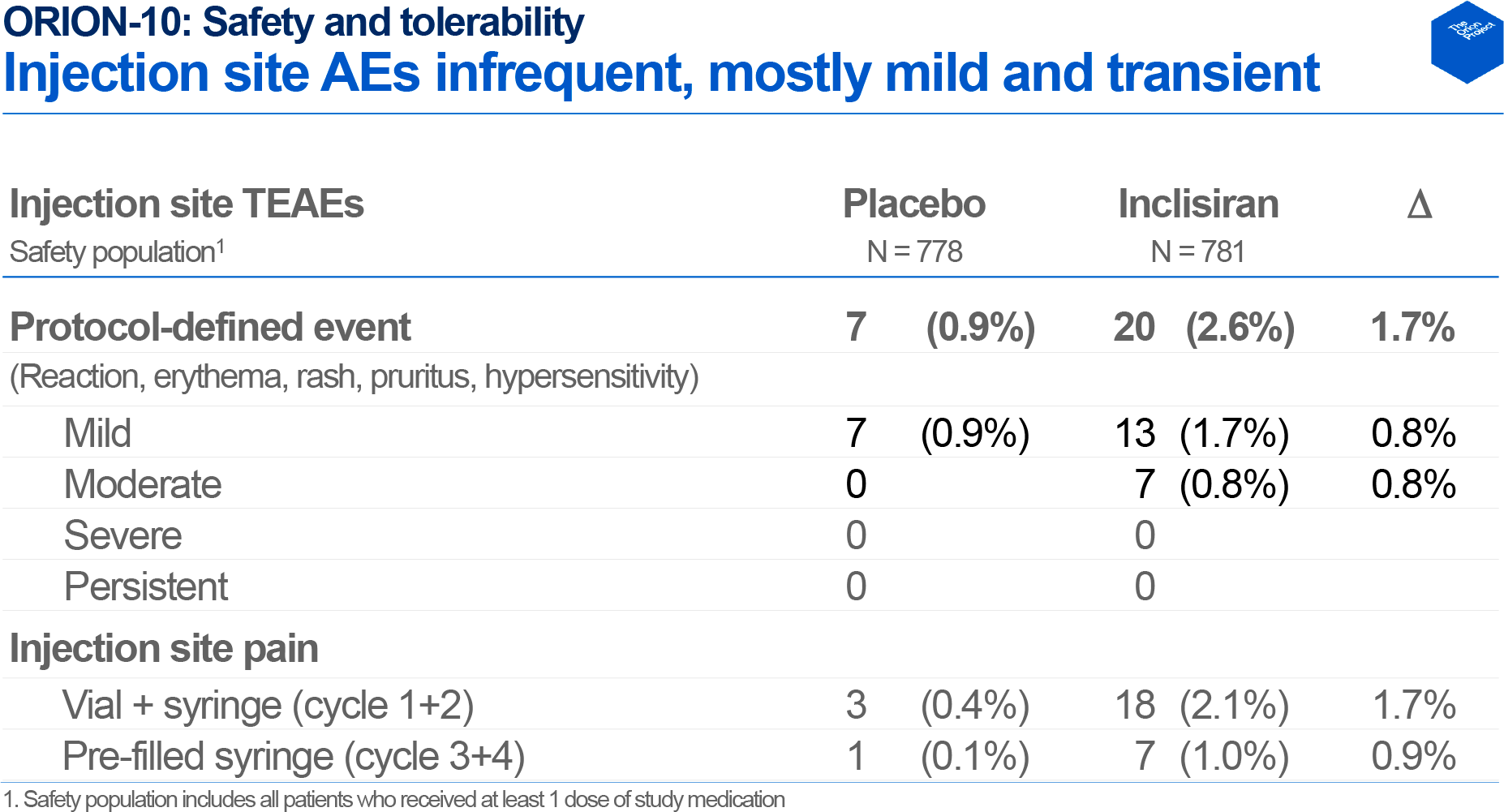
In terms of safety, the use of inclisiran was characterized by a similar spectrum of adverse reactions and their frequency compared to placebo. Inclisiran injections were associated with mild to moderate injection site reactions: 2.6% of patients (n=20/781) versus 0.9% (n=7/778).
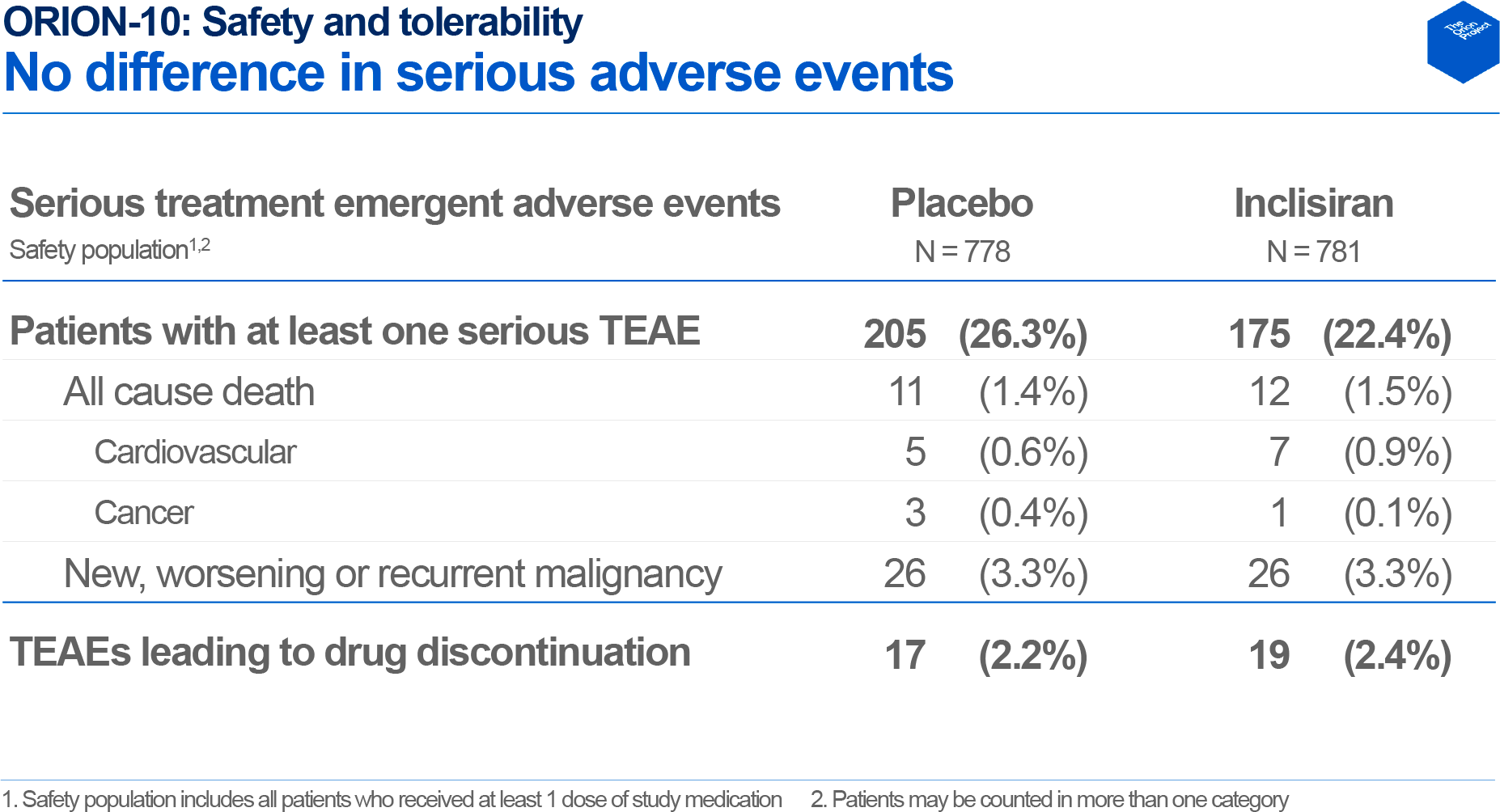
In terms of adverse cardiovascular outcomes, which were collectively defined as cardiac death or any signs or symptoms of cardiac arrest, non-fatal myocardial infarction and/or stroke, 7.4% of patients (n=58/781) in the inclisiran group experienced this — vs. 10.2% (n=79/778) in the control group. Meanwhile, cardiovascular death was reported for 0.9% of subjects (n=7/781) vs. 0.6% (n=5/778), and fatal or non-fatal myocardial infarction or stroke for 4.1% (n=32/781) vs. 3.3% (n=26/778).

The ORION-11 (NCT03400800) clinical trial enrolled adult patients (n=1617) with ASCVD or increased risk of developing it.
After 17 months, there was a change in the levels of the following lipid parameters in the inclisiran group compared to the placebo group:
- LDL-C: −46% — vs +4%; difference was −50% (95% CI: −53 — −47)
- TC: −28% — vs. +2%; −30% (95% CI: −32 — −28)
- non-HDL-C: −41% — vs. +2%; −43% (95% CI: −46 — −41)
- ApoB: −38% — vs. +1%; −39% (95% CI: −41 — −37)
- Lp(a): −19% — vs. 0%; −26% (95% CI: −21 — −16).

Between 3–18 months, the average decrease in LDL cholesterol was 48% versus an increase of 3%; the difference was −50%.

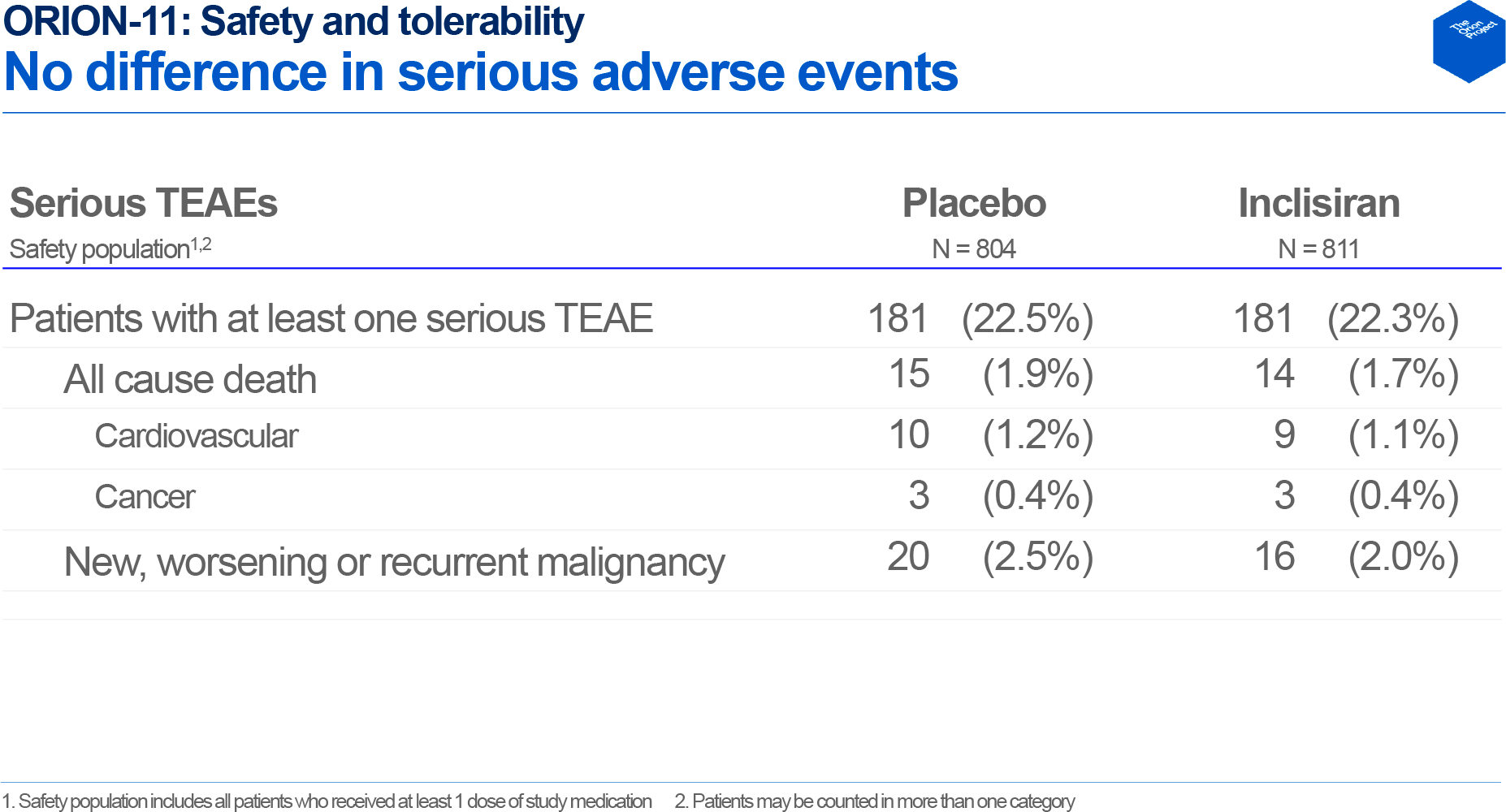
There were fewer cardiovascular complications in the inclisiran group: cardiovascular death 1.1% (n=9/811) vs. 1.2% (n=10/804), fatal and non-fatal myocardial infarction 1.2% (n=10/811) vs. 2.7% (n=22/804), fatal and non-fatal stroke 0.2% (n=2/811) vs. 1.0% (n=8/804).

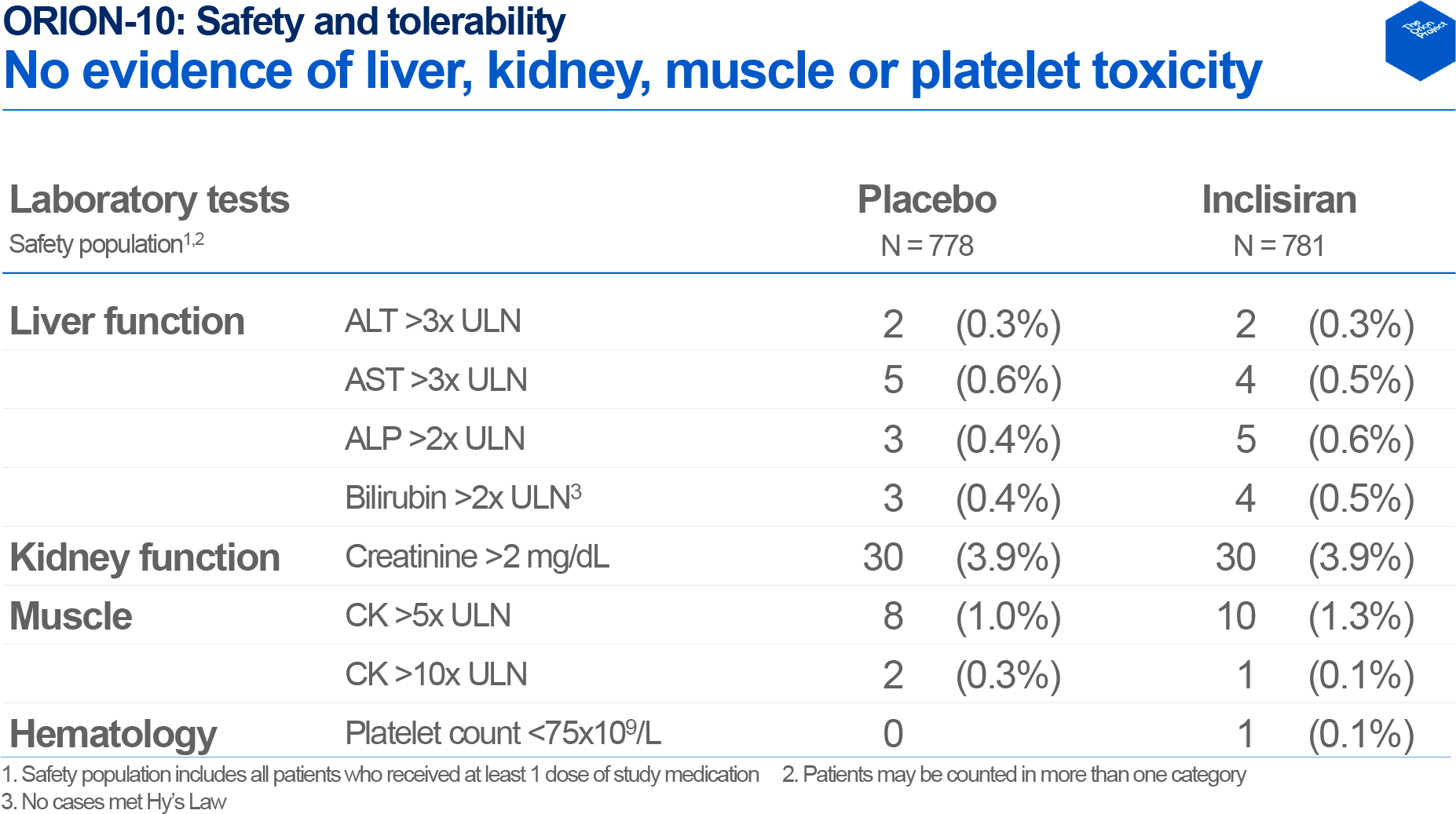
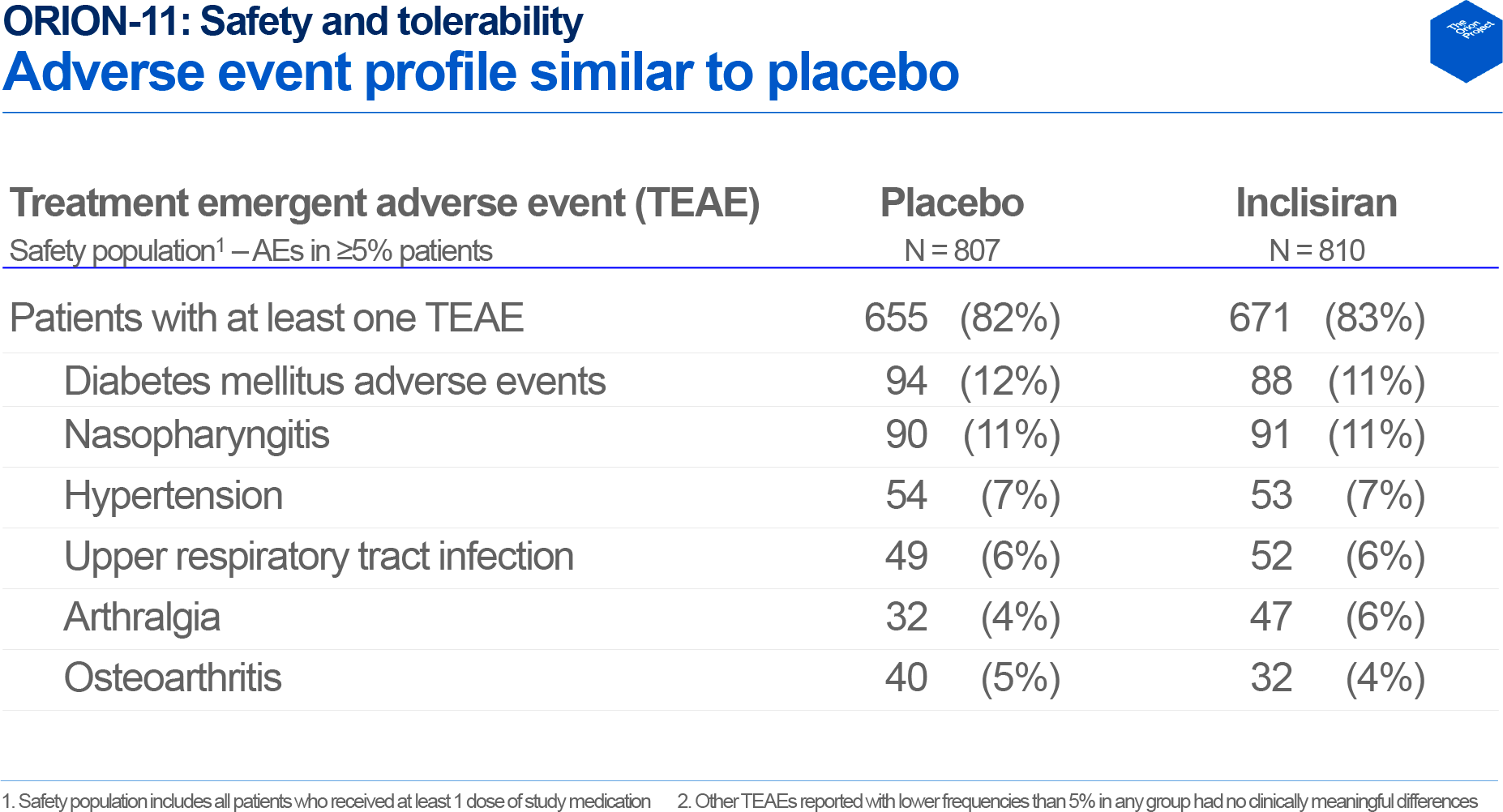
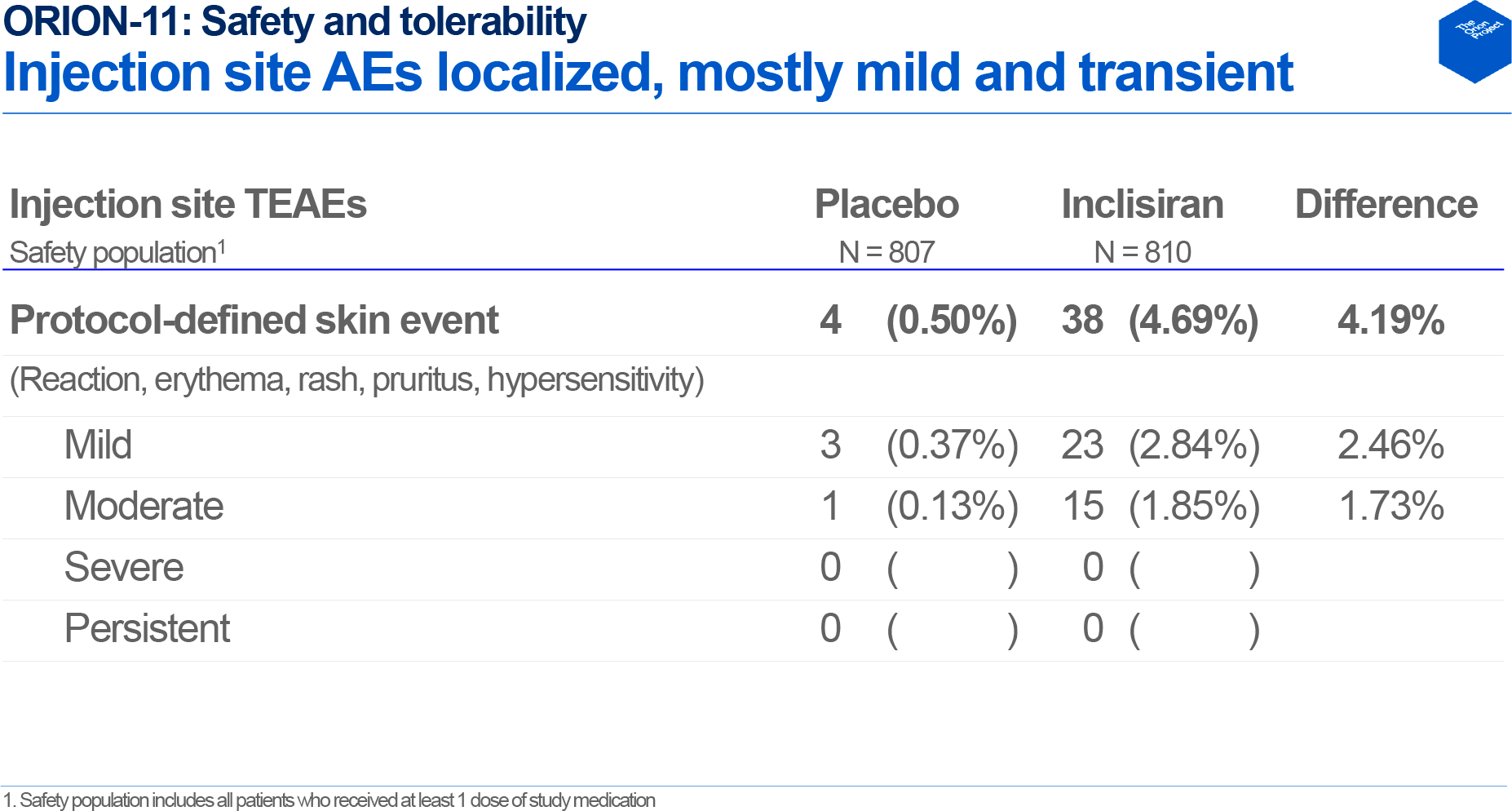
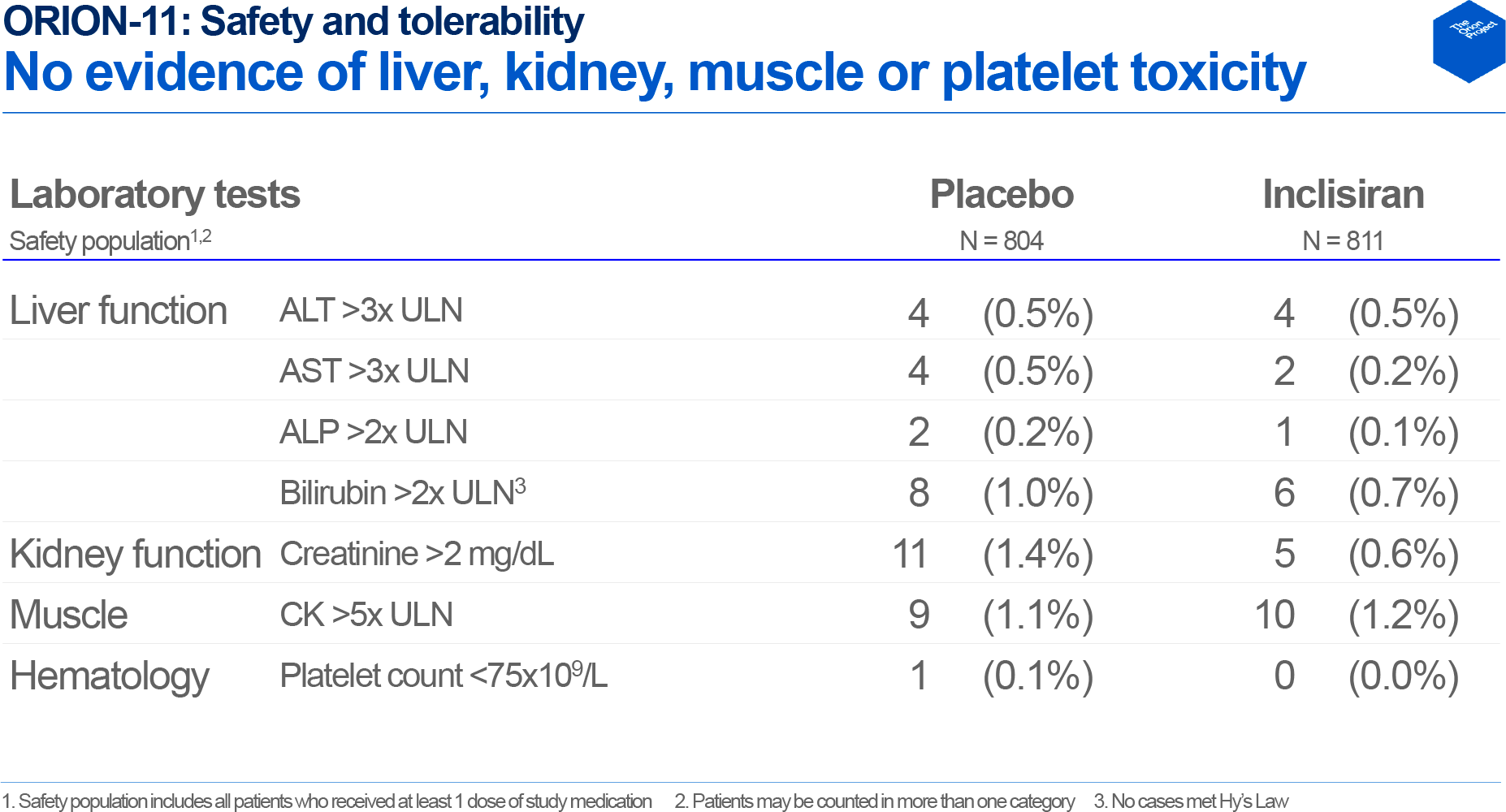
No differences in the frequency of adverse reactions such as diabetic events, nasopharyngitis, hypertension, upper respiratory tract infections, arthralgia, and osteoarthritis were reported between the inclisiran and placebo groups. No adverse effects of the experimental drug on the liver, kidneys, muscles, or platelets were observed, as confirmed by the corresponding laboratory measures. Only 4.7% (n=38/810) of those receiving inclisiran experienced mild to moderate adverse skin reactions at the injection site, such as redness, itching, rashes, and hypersensitivity.
Something Curious
Novartis took over inclisiran after it bought The Medicines Company in November 2019 shelling out $9.7 billion in cash. The latter acquired the worldwide rights to inclisiran from its developer, Alnylam Pharmaceuticals, in February 2013 for an upfront $25 million and a potential $180 million as certain development milestones passed plus double-digit royalties from sales of the ready-to-use drug.
The impressive amount that Novartis paid must be recouped by sales of Leqvio by either high demand for the drug or a high price for it. There’s no hurry, though, in charging a hell of a price tag since inclisiran’s patent protection doesn’t expire until 2035.
Leqvio, it is believed, needs to reach peak annual sales of $2.2 billion to at least get back the money spent by Novartis on its takeover of The Medicine Company.
By the way, Novartis has not been particularly forward-thinking. Yes, the Basel-based pharmaceutical company signed a five-year agreement with Alnylam back in 2005 paying $10 million upfront and acquiring its 19.9% stake. However, in 2010, the Swiss pharmaceutical giant refused to exercise its right to purchase for $100 million the non-exclusive rights to integrate Alnylam’s RNAi platform and intellectual property into its projects under development. In 2015, Novartis sold all RNAi-related assets to Arrowhead Pharmaceuticals, including reassigning the license to use Alnylam’s platform against three dozen therapeutic targets.
Praluent and Repatha: Sad Lessons From Competitors
A pair of PCSK9 inhibitors, Praluent (alirocumab) and Repatha (evolocumab), are already on the market to reduce risks of cardiovascular complications and lower LDL cholesterol levels in primary hyperlipidemia, including familial hypercholesterolemia.
These monoclonal antibodies by Sanofi/Regeneron Pharmaceuticals and Amgen, which debuted in the summer of 2015, are administered over statins (by subcutaneous injection) every two weeks or month and are quite decent at controlling bad cholesterol. And while inclisiran directly blocks PCSK9 synthesis, alirocumab and evolocumab block circulating PCSK9.
These drugs are not very popular. The cost of Praluent and Repatha is too high to divert the attention of patients, doctors, and insurance companies from penny statins, which are overwhelmingly represented by cheap generic copies. The manufacturers even had to do something unprecedented for the U.S. by impressively reducing prices (from $14,000 to $5,850 a year) but that didn’t help either.
Novartis’ marketing strategy for Leqvio in the United States is still unclear. But it is already obvious that greed will have a negative impact on the fate of the novelty. By the way, the production cost of inclisiran is comparable to that of traditional low-molecular-weight compounds, and the drug itself can be stored under normal conditions without requiring an expensive cold chain.
The U.S. Institute for Clinical and Economic Review (ICER) estimates that the cost of an annual course of Leqvio for American citizens should not exceed $5,644 for patients with atherosclerosis.
EvaluatePharma predicts that by 2024 inclisiran will be almost a blockbuster reaching $930 million in sales. And in 2026, demand for it will equal that of Repatha exceeding $2 billion.
Leqvio: Way Forward for Inclisiran
The main goal for inclisiran is to gather evidence that it can significantly reduce the risk of major adverse cardiovascular events (MACE) such as death due to cardiovascular complications, non-fatal myocardial infarction, non-fatal stroke, and urgent coronary revascularization procedure.
Yes, a powerful LDL cholesterol-lowering is great but patient outcomes related to prolongation of life and improvement of its quality are much more important.
According to the pooled data of ORION-9, ORION-10, and ORION-11, inclisiran reduced the risk of MACE by 24% statistically significant relative to placebo: 7.1% of patients experienced adverse cardiovascular events — against 9.4% in the placebo groups (p<0.05). The main beneficial contribution of inclisiran came from the side of reducing the risk of nonfatal myocardial infarction (5.2% vs. 7.8%).
One could be indignant that the absolute difference of 2.3% is too negligible to claim an impressive relative 24%. But let’s not forget that the lauded and ubiquitous statins, which are touted as highly effective preventive drugs, in fact, provide an even smaller difference of 1.1% which, however, turns into as much as 36% relative risk reduction.
The five-year ORION-4 (NCT03705234) phase 3 clinical trial of 15,000 patients with atherosclerosis (in the US and UK) is ongoing and should definitively establish by 2024 whether inclisiran is really suitable for the secondary prevention of cardiovascular complications. Presumably, ORION-4 will show a 30% reduction in the relative risk of MACE.
The long-term safety of inclisiran remains an open question since its mechanism of action involves interference with the genetic apparatus. That’s why a three-year clinical trial ORION-8 (NCT03814187) has been launched. It is open to patients from all other trials, including ORION-5 (NCT03851705) that covering patients diagnosed with homozygous familial hypercholesterolemia.
At this stage of research, there were no claims about the safety of inclisiran. By the way, existing hypocholesterolemic drugs are accompanied by risks of myalgia, general fatigue, diabetes mellitus, hepatotoxicity, hemorrhagic stroke, and formation of anti-drug antibodies that reduce the beneficial effect of LDL cholesterol reduction. Inclisiran’s safety evidence is unequivocally critical. Yes, Onpattro (patisiran), which was the world’s first RNA interference drug, has not uncovered any serious problems with adverse side effects, but it is used in rare disease — hereditary transthyretin amyloidosis (hATTR) with polyneuropathy (hATTR-PN) also known as familial amyloid polyneuropathy (FAP) — and therefore cannot provide reliable evidence for the safety of RNA interference due to too limited a patient base.
Extras
Leqvio (inclisiran). Prescribing information. U.S. [PDF]
Leqvio (inclisiran). Prescribing information. Europe. [PDF]
Leqvio (inclisiran). European public assessment report (EPAR). [PDF]
Inclisiran for the treatment of heterozygous familial hypercholesterolemia. N Engl J Med. 2020 Apr 16;382(16):1520-1530. [source]
Two phase 3 trials of inclisiran in patients with elevated LDL cholesterol. N Engl J Med. 2020 Apr 16;382(16):1507-1519. [source]
ORION-9 & ORION-10. Investor conference call. American Heart Association. 18 November, 2019. [PDF]
ORION-11. Investor conference call. European Society of Cardiology (ESC) Congress. September 2, 2019. [PDF]
ICER. Bempedoic acid and inclisiran for patients with heterozygous familial hypercholesterolemia and for secondary prevention of ASCVD: effectiveness and value. Final report. March 2, 2021. [PDF]
Novartis enters into agreement to acquire The Medicines Company. Investor presentation. November 25, 2019. [PDF]