Highlights
Favipiravir is an oral drug used in the treatment of COVID-19 infection caused by the SARS-CoV-2 coronavirus.
Favipiravir is included in the official clinical guidelines of several countries, including Egypt, Hungary, Malaysia, Romania, Russia, Thailand, Turkey, UAE, Venezuela, and Vietnam. It is indicated for the treatment of mild-to-moderate COVID-19, with equal use in both outpatient and inpatient settings. Nevertheless, the vast majority of the world does not use favipiravir as a pharmacological weapon against the pandemic.
Rather than summarize the relevance and validity of favipiravir in the context of COVID-19 treatment, we suggest reviewing the results of systematic reviews and meta-analyses, which, based on the outcomes of multiple clinical trials, have attempted to objectively evaluate the therapeutic efficacy of favipiravir. In any case, making informed medical decisions is still relevant because of the ongoing SARS-CoV-2 pandemic.
It should also be recalled that recently, highly effective antiviral medications have emerged that are doing very well in treating COVID-19 in outpatients. Such oral drugs include the following: Paxlovid (nirmatrelvir + ritonavir), Lagevrio (molnupiravir), and Xocova (ensitrelvir). All of them have shown decent effectiveness in counteracting the coronavirus, keeping complications of the infection from developing, preventing hospitalization, and reducing the risk of death.

Paxlovid: New Cure for Coronavirus
Pfizer’s oral antiviral drug reduced the risk of hospitalization or death from COVID-19 by 89%.
What Is Favipiravir?
The history of favipiravir (T-705) began in late March 2014, when Avigan (favipiravir), developed by Toyama Chemical as part of Fujifilm, appeared in Japan to treat influenza.
The drug, however, is in reserve and not available to the general public: favipiravir is indicated for the treatment only of new or returning (but not seasonal) serotypes of influenza A, B, and C virus that can lead to pandemics, cause severe disease, or against which existing influenza medications are ineffective. This restriction was made, among other reasons, because favipiravir is teratogenic: in the early stages of pregnancy, it leads to fetal development defects and is, therefore, contraindicated in pregnant women and in men and women during pregnancy planning.
In the context of influenza, favipiravir works as follows. Influenza viruses replicate and transcribe their genome in the nuclei of infected cells via a heteromeric RNA polymerase complex. The latter consists of three protein subunits — polymerase acidic protein (PA), polymerase basic protein 1 (PB1), and polymerase basic protein 2 (PB2) — that are highly conserved, closely interacting, and critical for efficient viral replication and associated virulence.
The PB2 subunit binds the 5′-cap pre-mRNAs of the host cell and positions them for cleavage by a cap-dependent endonuclease located in the N-terminal domain of the PA subunit. this “cap-snatching” process provides RNA primers for the transcription of viral mRNA performed by RNA-dependent RNA polymerase (RdRp), whose function is provided by the PB1 subunit. The transcriptase activity of PB1 is responsible for the synthesis of messenger, complementary, and virion RNAs.
Because favipiravir, as a modified pyrazinecarboxamide analog, targets the PB1 subunit by actually inhibiting RdRp, it thereby suppresses influenza virus replication.
In parallel, it was found that favipiravir is able to suppress the replication of other RNA viruses, including coronaviruses, and does so in a different way than in the case of influenza.
Favipiravir, being a prodrug, undergoes intracellular ribosylation and phosphorylation, turning into the therapeutically active form — favipiravir ribofuranosyl-5′-triphosphate (favipiravir-RTP), which is engaged in RdRp inhibition. Favipiravir-RTP, acting as an analog of the purine nucleotide, exhibits antiviral effects of chain termination, inhibition of RNA synthesis, and lethal mutagenesis.

Molnupiravir: New Effective Pill for Coronavirus. All That We Know
Molnupiravir pills by Merck & Co. can help COVID-19 patients avoid going to the hospital or dying.
Favipiravir in Countries Around World
The largest introduction of favipiravir in the context of COVID-19 treatment took place in Russia. Favipiravir is approved by the Russian Ministry of Health to treat COVID-19 infections of mild-to-moderate severity, and favipiravir can be used in both outpatient and inpatient settings.
In Russia, favipiravir found a wide response among manufacturers and is sold under such brand names as Avifavir, Areplivir, Covidolek, Coronavir, Favibirin.
Favipiravir is approved for use and included in the clinical treatment protocols of COVID-19 in several other countries including Egypt, Hungary, Malaysia, Romania, Thailand, Turkey, UAE, Venezuela, and Vietnam. At the same time, India, which had previously been very active in promoting favipiravir in the fight against COVID-19, abandoned it in the end. Saudi Arabia did the same.
Regulators in the United States, the European Union, and Japan — the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), and the Pharmaceuticals and Medical Devices Agency (PMDA) — have not approved favipiravir for use against COVID-19. Nor has the World Health Organization (WHO) approved it.

Yeliva: New Drug for COVID-19
Oral opaganib will reduce the likelihood of death and accelerate recovery in hospitalized patients with COVID-19.
Outside Russia, favipiravir is known under many of the following brand names: Abigan, Avigan, Avipiravir, Balflu, Baxtovir, Ciplenza, Cobiflu, Codifab, Covipos, Daxyflu, FabiFlu, Fabifort, Fabimed, Fabistin, Fabiwar, Fabrion, Fapivir, Fapvir, Favchem-Flu, Favicare, Favicim, Favicovid, Favicovir, Faviford, Favijaj, Favikast, Favikav, Favilab, Favimax, Favimits, Favinil, Favipil, Favipira, Favira, Favirek, Faviscan, Favisern, Favisun, Faviton, Favitron, Favivent, Favivir, Favizac, Favizen, Favtris, Feblus, Fenzavir, Ferasun, Feravir, Fevisafe, Feviwill, Fluguard, Fluvicut, Fluvigan, Infavir, Infravir, Metflu, Mysfevir, Pancovir, Piramvir, Qifenda, Reeqonus, Syvir, Veffavir, Viraflu.
If we talk about the cost of favipiravir in Russia, as a country with the maximum implementation of it in clinical practice and the strongest support from the government, there are set maximum sale prices for this drug. The limit is 5,000 rubles ($65; here and below at the exchange rate as of mid-February 2022) for a pack of 50 favipiravir 200-mg tablets. Two packs of favipiravir, which would cost 10,000 rubles ($130), are needed for a 10-day course of treatment for a patient.
By comparison, India’s Sun Pharmaceutical Industries offers favipiravir at a price of 35 rupees per 200-mg tablet, that is 1,750 rupees ($23) for 50 pills. Moreover, India’s Nilrise Pharmaceuticals is willing to give favipiravir at 15 rupees (20 cents) for a 400-mg tablet. Thus, there is a multiple cost discrepancy with Russian variants of favipiravir, which cannot but raise questions about certain corruption elements.
According to expert estimates, the minimum estimated cost of producing a 10-day course of favipiravir for COVID-19 treatment under the Russian scheme is approximately $22, and that includes adjustments for losses, formulation, packaging, and profit margins. Since the estimate was made in the spring of 2020, now that there is no shortage of the active pharmaceutical ingredient (API) of favipiravir, the cost may be even lower.
Xocova: Powerful New Japanese Pill for Coronavirus Treatment
Ensitrelvir by Shionogi & Co. is a highly effective antiviral drug that works just as well as Pfizer’s Paxlovid.
Favipiravir for Treatment of COVID-19: Systematic Reviews and Meta-Analyses
A systematic review is a scientific study whose objective is to review published work on a specific issue, followed by critical analysis, evaluation, and synthesis of the data collected.
Meta-analysis means combining the results of several studies using statistical methods to test one or more interrelated scientific hypotheses.
Systematic review and meta-analysis, whose function is to minimize bias in the interpretation of data, are the main tools of evidence-based medicine. The results of a systematic review, when of high methodological quality, are the most reliable sources of information needed to make informed decisions about health care.
The following studies have comprehensively compared the clinical outcomes of adding favipiravir to standard antiviral therapy (other antivirals, respiratory support, antibiotics, immunomodulators, herbal medicines, etc.) versus prescribing the latter alone.

MesenCure: Israeli Miracle Drug Saves From Death by COVID-19
A cell therapy developed by Bonus BioGroup is amazingly able to fight coronavirus and its most severe complications.
Meta-Analysis #1
The systematic review by Nepalese experts examined the results of 4 clinical trials (3 randomized, 1 non-randomized) of favipiravir: 3 were conducted in China (ChiCTR2000029544, ChiCTR2000029600, ChiCTR2000030254) and 1 in Russia (NCT04434248) — data from which were available as of late August 2020.
Conclusions
- Pros. Favipiravir provided statistically significant clinical or radiological improvements during treatment of COVID-19 infection.
- Cons. Favipiravir did not statistically significantly lead to faster elimination of the SARS-CoV-2 coronavirus from the body and did not reduce the likelihood of needing additional oxygen support.
- Comments. Because of the small sample size of the systematic review, the power of the study may have been reduced. The lack of blinding in the original clinical trials increased the risks of bias and systematic error. Despite the good therapeutic potential of favipiravir, additional large-scale prospective randomized double-blind controlled clinical trials are needed to provide an unequivocal opinion on the appropriateness of this drug.
- Bottom line. At this stage, it is reasonable to take a position on the rational use of favipiravir in clinical practice.
Details
Viral Clearance
The meta-analysis found no statistically significant benefit from adding favipiravir to standard COVID-19 therapy in the task of accelerating the body’s clearance of the SARS-CoV-2 coronavirus. Thus, on day 7 of treatment, the risk ratio (RR) was 1.13 (95% CI: 0.55 to 2.33; p=0.73) [I2=84%; P=0.002]; on day 14, RR was 1.06 (95% CI: 0.84 to 1.33; p=0.65) [I2=67%; P=0.05].
Similarly, no statistically significant advantage was found in the risk difference (RD) criterion: on day 7 of therapy, RD was 0.06 (95% CI: −0.34 to 0.45; p=0.77) [I2=84%; P=0.002]; on day 14, RD was 0.03 (95% CI: −0.17 to 0.24; p=0.74) [I2=73%; P=0.02].

Clinical or Radiological Improvement
The meta-analysis showed that the addition of favipiravir to standard treatment for COVID-19 infection resulted in a statistically significant difference in terms of clinical or radiological improvements. Thus, on treatment day 7, RR and RD were 1.25 (95% CI: 1.01 to 1.53; p=0.04) [I2=0%; P=0.68] and 0.11 (95% CI: 0.01 to 0.22; p=0.04) [I2=0%; P=0.88], on day 14 they were 1.29, (95% CI: 1.08 to 1.54; p=0.005) [I2=16%; P=0.30] and 0.19 (95% CI: 0.07 to 0.32; p=0.002) [I2=20%; P=0.28].

Clinical or Radiological Worsening
According to the meta-analysis, clinical or radiological worsening at the end of COVID-19 treatment was less likely in the favipiravir group compared with other antivirals, although without a statistically significant difference: odds ratio (OR) was 0.59 (95% CI: 0.30 to 1.14; p=0.12) [I2=39%; P=0.19].

Need for Oxygen Support or Noninvasive Ventilation
The meta-analysis demonstrated that adding favipiravir to standard COVID-19 therapy reduced the likelihood of needing oxygen support or noninvasive mechanical ventilation, but without statistical significance: OR 0.76 (95% CI: 0.42 to 1.39; p=0.37) [I2=0%; P=0.99].

Duration of Conversion to Negative RT-PCR
According to the meta-analysis, conversion to negative reverse transcription polymerase chain reaction (RT-PCR) for the SARS-CoV-2 coronavirus RNA occurred approximately 5 days earlier among those receiving favipiravir: mean difference (MD) was −5.16 (95% CI: −6.95 to −3.37; p<0.00001) [I2=45%; P=0.18].

Meta-Analysis #2
The systematic review by Indian experts looked at the results of 4 clinical trials (3 randomized, 1 non-randomized) of favipiravir: 4 trials were conducted in China (ChiCTR2000029544, ChiCTR2000029600, ChiCTR2000030254) and 1 in Russia (NCT04434248) — data from which were available as of early October 2020.
In fact, we are talking about other experts’ interpretations of the results of the same clinical trials that were considered in meta-analysis #1.
Conclusions
- Pros. Favipiravir provided statistically significant clinical or radiologic improvements after 7–10 days of treatment for COVID-19 infection.
- Cons. Favipiravir did not result in statistically significant acceleration of elimination of the SARS-CoV-2 coronavirus from the body and did not reduce the likelihood that noninvasive mechanical ventilation was needed.
- Comments. The small number of clinical trials included in the systematic review does not allow a definitive conclusion regarding the therapeutic validity of favipiravir in COVID-19 infection. More data need to be collected in additional high-quality randomized or non-randomized trials or observational studies.
- Bottom line. Opinion on favipiravir is that it does have therapeutic benefit but its scope is limited.
Details
Viral Clearance
The meta-analysis found that adding favipiravir to standard COVID-19 therapy accelerated the elimination of the SARS-CoV-2 coronavirus but without statistically significant benefit. Thus, at day 10–14 of treatment, the odds ratio (OR) was 1.91 (95% CI: 0.91 to 4.01; p=0.09) [I2=30%; P=0.23].

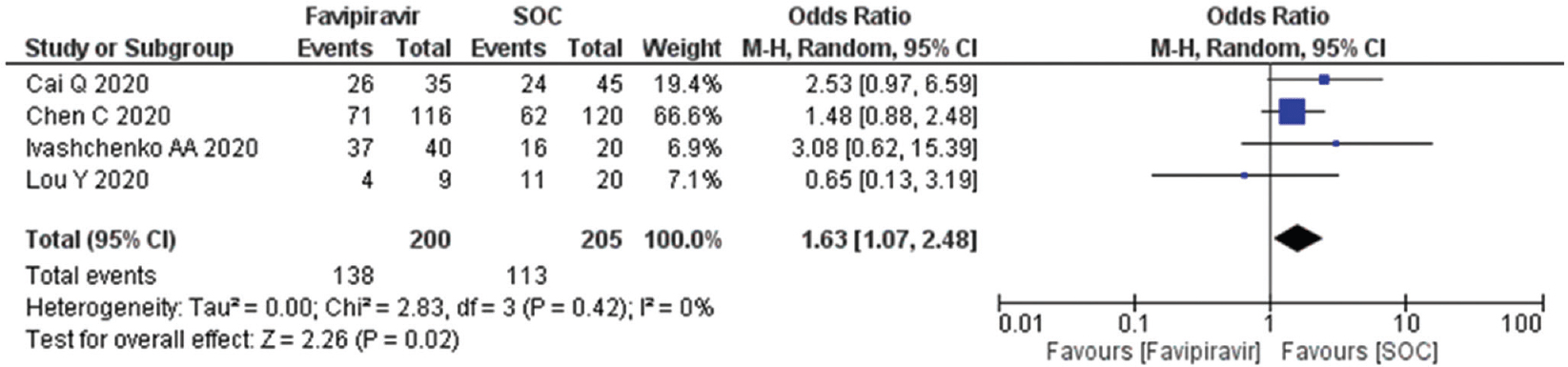
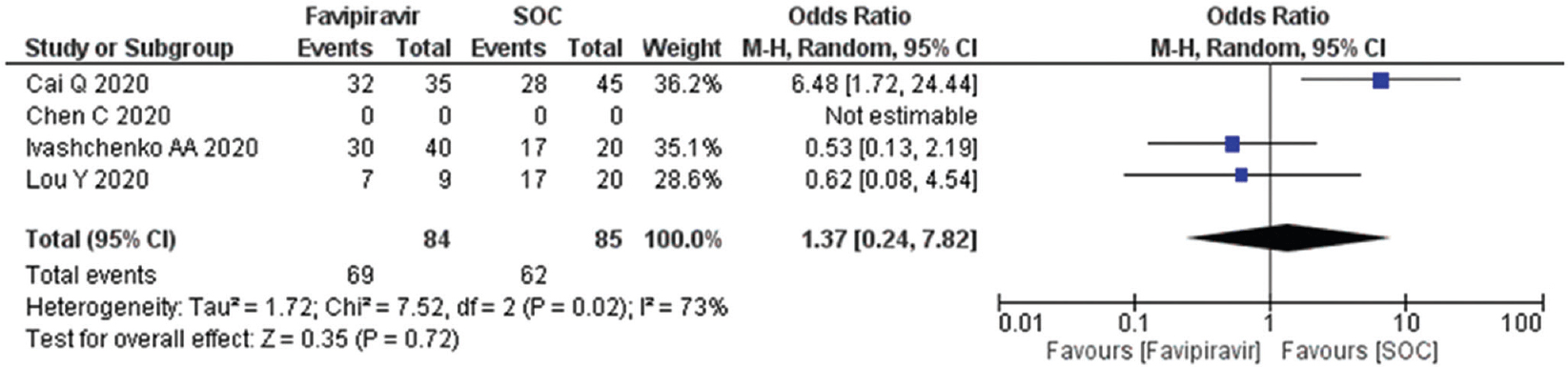
Clinical or Radiological Improvement
The meta-analysis demonstrated that the addition of favipiravir to standard treatment for COVID-19 infection was associated with higher odds of clinical or radiological improvement. Thus, after 7–10 days of treatment, the OR came out to 1.63 (95% CI: 1.07 to 2.48) [I2=0%; P=0.42]; after 10–14 days, the OR was 1.37 (95% CI: 0.24 to 7.82) [I2=73%; P=0.02]. However, statistical significance was demonstrated only in the first case but not in the second: p=0.02 and p=0.72, respectively.
Need for Noninvasive Ventilation
According to the meta-analysis, the addition of favipiravir to standard COVID-19 therapy resulted in a reduced likelihood of needing noninvasive mechanical ventilation but without statistical significance: OR 0.80 (95% CI: 0.43 to 1.47; p=0.47) [I2=0%; P=0.73].

Meta-Analysis #3
The systematic review by Japanese experts reviewed the results of 5 clinical trials (4 randomized, 1 non-randomized) of favipiravir: 3 were conducted in China (ChiCTR2000029544, ChiCTR2000029600, ChiCTR2000030254) and 1 each in Russia (NCT04434248) and Japan (jRCTs041190120) — data from which were available as of mid-September 2020.
Conclusions
- Pros. Favipiravir provided statistically significant clinical or radiological improvement during 7 and 4 days of therapy for COVID-19 infection and accelerated elimination of the SARS-CoV-2 coronavirus from the body during 7 days of treatment.
- Cons. Favipiravir provided no statistically significant benefit in accelerating viral clearance during the 14-day therapy period.
- Comments. The systematic review demonstrated high promise of favipiravir in the treatment of COVID-19 infection. However, the study was accompanied by several limitations. First, the doses and durations of favipiravir were different in the clinical trials included in the meta-analysis. Second, not all trials took outcomes strictly after 7 and 14 days of therapy. Third, definitions of what should be understood by clinical improvement differed. The results of the meta-analysis should be supported by additional clinical trials, particularly those evaluating different doses of favipiravir and duration of administration among patients with varying degrees of severity of COVID-19.
- Bottom line. Favipiravir has been shown to have great potential for the treatment of COVID-19, particularly among patients with asymptomatic or mild-to-moderate disease.
Details
Viral Clearance
The meta-analysis found that the addition of favipiravir to standard COVID-19 therapy accelerated clearance of the SARS-CoV-2 coronavirus. Thus, a statistically significant odds ratio (OR) of 0.40 (95% CI: 0.19 to 0.84; p=0.02) [I2=39%; P=0.18] was recorded on treatment day 7. However, no statistical significance was detected on treatment day 14: OR 0.46 (95% CI: 0.14 to 1.45; p=0.18) [I2=52%; P=0.10].

Nevertheless, after 7 and 14 days of therapy, 65.4% and 88.9% of patients in the favipiravir groups reached viral clearance status — versus 43.4% and 78.8% in the control groups, which was a statistically significant difference (p<0.00001) [I2=25%; P=0.26 and I2=0%; P=0.68].

Clinical or Radiological Improvement
The meta-analysis showed that the addition of favipiravir to standard treatment for COVID-19 infection resulted in a statistically significant difference in terms of clinical or radiographic improvement: at day 7 and 14 of treatment, the OR was 1.60 (95% CI: 1.03 to 2.49; p=0.04) [I2=0%; P=0.83] and 3.32 (95% CI: 1.44 to 7.65; p=0.005) [I2=15%; P=0.31], respectively.

The proportions of patients who reported clinical improvement on days 7 and 14 of therapy were 54.3% and 84.6% in the favipiravir groups — vs. 34.4% and 65.8% in the control groups, which was a statistically significant difference (p<0.00001) [I2=73%; P=0.01 and I2=67%; P=0.05].

Meta-Analysis #4
The systematic review by Iranian experts evaluated the results of 9 clinical trials (8 randomized, 1 non-randomized) of favipiravir: 4 were conducted in China (ChiCTR2000029544, ChiCTR2000029600, ChiCTR2000030254, ChiCTR2000030894) and 1 each in Russia (NCT04434248), Japan (jRCTs041190120), India (CTRI/2020/05/025114), Egypt (NCT04349241), and Oman (study) — data from which were available as of late December 2020.
Conclusions
- Pros. Favipiravir provided statistically significant clinical and radiological improvements within 7 days of treatment of COVID-19 infection.
- Cons. Favipiravir did not statistically significantly lead to faster elimination of the SARS-CoV-2 coronavirus from the body, did not reduce the likelihood of needing additional oxygen support, did not reduce the chances of transfer to the intensive care unit (ICU), and could not affect fatal outcomes.
- Comments. The systematic review could not unequivocally answer the question of the reasonableness of the use of favipiravir in clinical practice, and the causes are as follows. First, the small sample size in each clinical trial. Second, because of the multi-drug pharmacotherapy in most of the included trials, there is a risk of affecting the efficacy of favipiravir. Third, the dose and duration of administration of favipiravir varied widely. Fourth, it is difficult to determine clinical improvement among patients in the various clinical trials because they were characterized by different disease severity, age, and health status. Overall, favipiravir had no significant positive effect on reducing the likelihood of death in the overall group of patients with mild-to-moderate COVID-19. It is possible that the initiation of therapy with favipiravir was too late after the onset of disease symptoms, which explains its low efficacy in the clinical setting. Additional clinical trials with a larger sample size are needed to accurately assess the therapeutic efficacy of favipiravir.
- Bottom line. Due to the limited evidence available, caution should be exercised in the widespread use of favipiravir in clinical practice, both by prescribing it only to patients who really need it and by starting therapy as early as possible in the course of COVID-19 infection.
Details
Viral Clearance
The meta-analysis found no statistically significant benefit from adding favipiravir to standard COVID-19 therapy in the task of accelerating the body’s clearance of the SARS-CoV-2 coronavirus. Thus, on day 7 of treatment, the risk ratio (RR) was 1.08 (95% CI: 0.83 to 1.39; p=0.580) [I2=62%; P=0.02], on day 10, RR was 1.02 (95% CI: 0.92 to 1.14; p=0.648) [I2=0%; P=0.85], and on day 14, RR was 1.11 (95% CI: 0.98 to 1.26; p=0.094) [I2=43%; P=0.11].

Clinical or Radiological Improvement
The meta-analysis showed that the addition of favipiravir to standard treatment for COVID-19 infection resulted in a statistically significant difference in terms of clinical or radiological improvement at day 7 of treatment: RR 1.24 (95% CI: 1.09 to 1.41; p=0.001) [I2=0%; P=0.94].
On the other hand, at treatment day 14, favipiravir did not provide a statistically significant difference: RR 1.11 (95% CI: 0.98 to 1.26; p=0.108) [I2=35%; P=0.18].

Need for Oxygen Support
The meta-analysis demonstrated that adding favipiravir to standard COVID-19 therapy reduced the likelihood of needing oxygen support but without statistical significance: RR 0.93 (95% CI: 0.67 to 1.29; p=0.664) [I2=0%; P=0.95].

Transfer to ICU
According to the meta-analysis, favipiravir failed to statistically significantly reduce the likelihood of patients being transferred to the intensive care unit (ICU): RR 1.14 (95% CI: 0.50 to 2.59; p=0.759) [I2=0%; P=0.53].

Mortality
According to the meta-analysis, the mortality rate among those receiving favipiravir was approximately 30% lower although without a statistically significant difference: RR 0.71 (95% CI: 0.26 to 1.92; p=0.499) [I2=0%; P=0.95].

Update #1
Due to the subsequent withdrawal of the journal publication on the favipiravir clinical trial in Egypt (because both the original data underlying the study and the randomization procedure were questionable), experts re-analyzed the rates of acceleration of viral clearance and mortality reduction. The results for favipiravir were generally unchanged: its efficacy on these indicators did not statistically significantly differ from the control group.
Meta-Analysis #5
The systematic review by Swiss and Italian experts examined the results of 6 randomized clinical trials of favipiravir: 3 were conducted in Russia (NCT04434248, NCT04501783, NCT04542694), 1 each in China (ChiCTR2000029544), Egypt (NCT04349241), and India (CTRI/2020/05/025114) — data from which were available as of early May 2021.
Conclusions
- Pros. Favipiravir shortened the time required for elimination of the SARS-CoV-2 coronavirus from the body and increased the chances of clinical or radiological improvement during the 7-day treatment period for COVID-19 infection.
- Cons. Among those who received favipiravir was more likely to be admitted to the intensive care unit (ICU), given the baseline severity of the patients’ condition.
- Comments. Administration of favipiravir early in COVID-19 development resulted in a beneficial effect, reflected by accelerated viral clearance with concomitant clinical improvement, resulting in a shorter hospital stay. Despite a reduction in the likelihood of mortality, the use of favipiravir did not provide a clear reduction in the number of deaths in absolute terms.
- Bottom line. The current evidence base, characterized by low or very low credibility of the evidence, is insufficient to reliably justify the use of favipiravir as monotherapy or combination therapy for COVID-19 infection.
Details
Viral Clearance
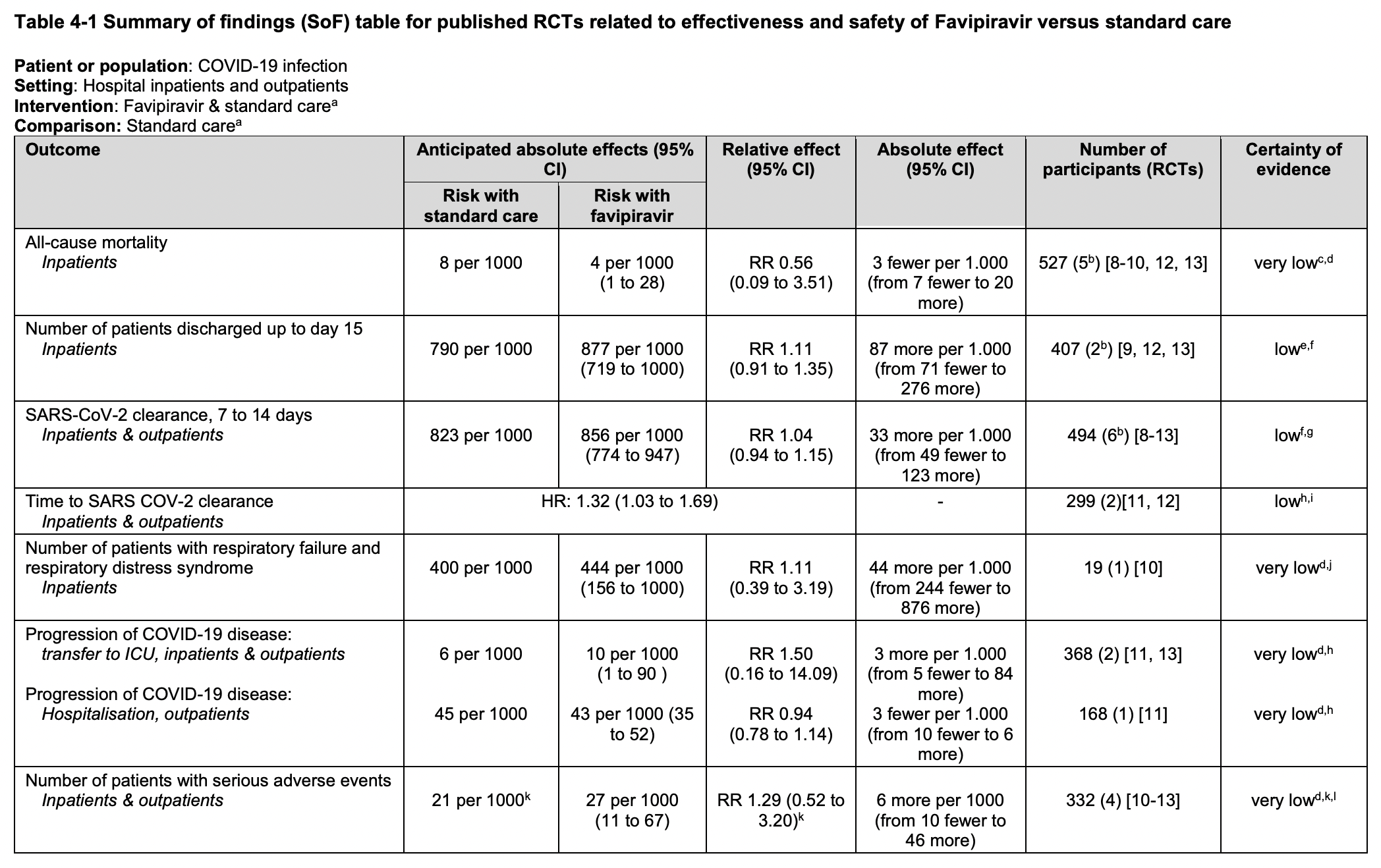
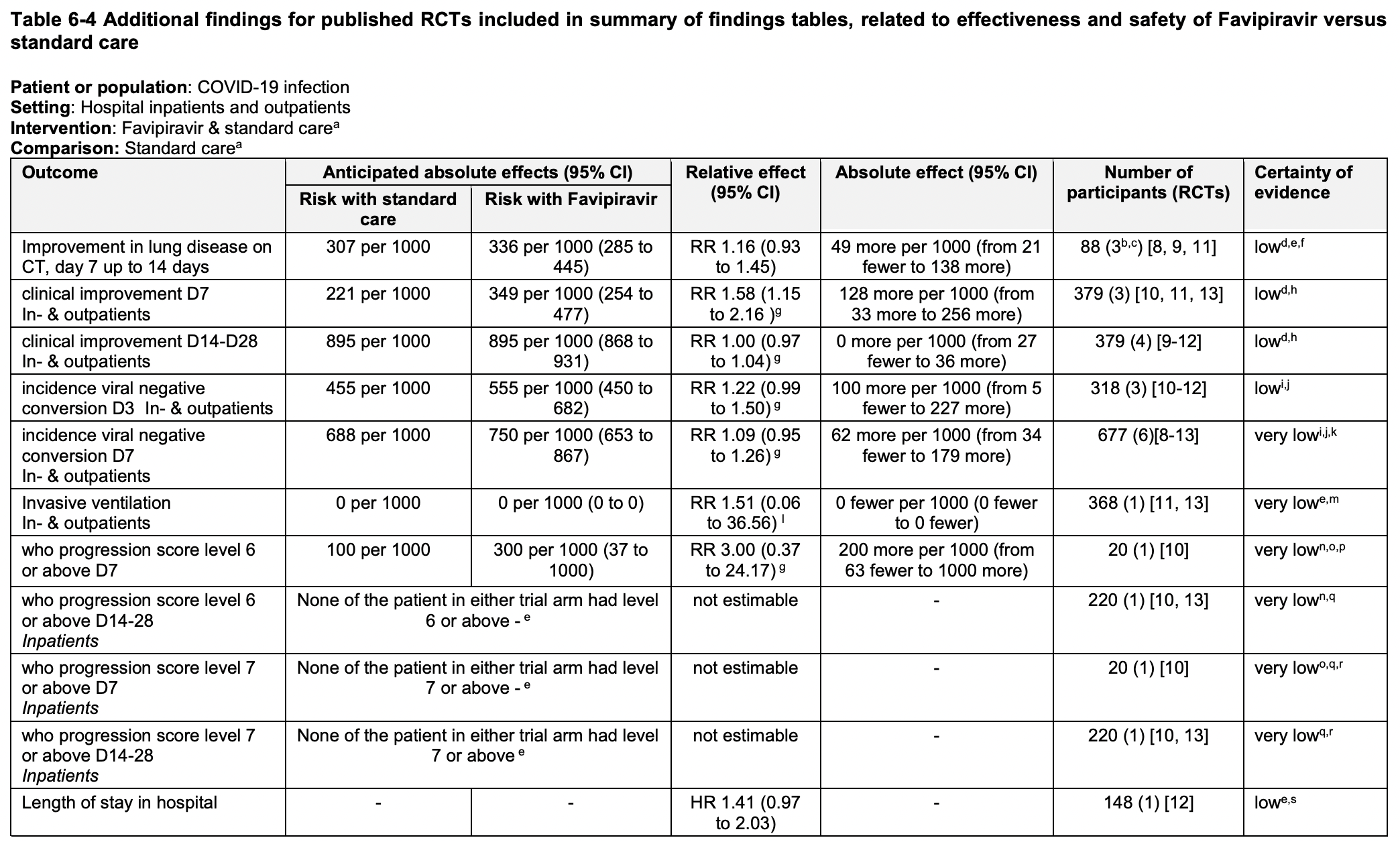
According to the meta-analysis, the addition of favipiravir to standard COVID-19 therapy accelerated clearance of the SARS-CoV-2 coronavirus. Thus, on day 3 of treatment the relative risk (RR) was 1.22 (95% CI: 0.99 to 1.50), on day 7, RR was 1.09 (95% CI: 0.95 to 1.26), on day 14, RR was 1.04 (95% CI: 0.94 to 1.15).
Meanwhile, the time required for viral clearance was reduced by approximately one-third: hazard ratio (HR) 1.32 (95% CI: 1.03 to 1.69).
Clinical or Radiological Improvement
The meta-analysis showed that adding favipiravir to standard treatment for COVID-19 infection approximately doubled the odds of clinical or radiological improvement by day 7 of treatment: RR 1.58 (95% CI: 1.15 to 2.16).
On the other hand, between days 7–14 and 14–28 of treatment, favipiravir did not provide anything similar: RR 1.16 (95% CI: 0.93 to 1.45) and RR 1.00 (95% CI: 0.97 to 1.04), respectively.
Transfer to ICU
The meta-analysis demonstrated that those receiving favipiravir were more likely to be transferred to the intensive care unit (ICU): RR 1.50 (95% CI: 0.16 to 14.09). At the same time, there was a slightly increased risk of respiratory failure or acute respiratory distress syndrome (ARDS): RR 1.11 (95% CI: 0.39 to 3.19).
Mortality
According to the meta-analysis, the mortality rate among hospitalized patients who received favipiravir was approximately half that of patients who received standard care: RR 0.56 (95% CI: 0.09 to 3.51). In absolute terms, this translates into a reduction of 3 deaths per 1,000 patients (95% CI: 7 to 20).
Meta-Analysis #6
The systematic review implemented by Turkish experts examined the results of 12 clinical trials (9 randomized, 3 non-randomized) of favipiravir: 3 studies each were conducted in China (ChiCTR2000029544, ChiCTR2000029600, ChiCTR2000030254) and Russia (NCT04434248, NCT04542694, NCT04542694), 2 in Egypt (NCT04351295, NCT04349241), 1 each in India (CTRI/2020/05/025114), Oman (study), Hungary (study), and Saudi Arabia (study) — data from which were available as of early June 2021.
Conclusions
- Pros. No real clinical benefit from favipiravir has been found.
- Cons. Favipiravir did not statistically significantly reduce the likelihood of the need for noninvasive mechanical ventilation and failed to affect mortality in COVID-19 infection.
- Comments. The systematic review was characterized by several limitations. For instance, the sample size for the meta-analysis had to be narrowed due to the lack of strictly controlled clinical trials, while all included were open-label. In the COVID-19 pandemic, it was difficult to conduct a large-scale trial due to the lack of patients without prior treatment. There was a problem with unified determination of patient severity. Additional randomized clinical trials or qualitative observational studies with adequate sample size are needed to accurately establish the efficacy of favipiravir in COVID-19.
- Bottom line. Favipiravir has not demonstrated statistically significant benefit with respect to the most important measures of clinical success in treating COVID-19 infection — reducing the likelihood of needing mechanical ventilation or reducing the chance of mortality — and is unlikely to be recommended for the treatment of patients with moderate disease, whereas it is appropriate for COVID-19 therapy in the asymptomatic or mild form.
Details
Viral Clearance
The meta-analysis did not investigate how favipiravir administration affects the rate at which the SARS-CoV-2 coronavirus is eliminated from the body. And there’s a reason for that.
Although early in the pandemic it was thought that assessing changes in viral load and viral clearance rate was appropriate for tracking disease progression in patients with COVID-19, further study of SARS-CoV-2 features showed that viral load as a clinical outcome was not a good choice for assessing treatment effectiveness. Thus, many patients continued to test positive for the presence of coronavirus RNA even after they had unambiguously recovered.
Clinical or Radiological Improvement
The meta-analysis also declined to clarify whether the use of favipiravir affects clinical improvement, including radiological improvement, because the specifics in interpreting this outcome varied widely among clinical trials, thereby endowing it with a fair amount of subjectivity.
Need for Noninvasive Ventilation
According to the meta-analysis, the addition of favipiravir to standard COVID-19 therapy reduced the likelihood of needing noninvasive mechanical ventilation by half but without statistical significance: odds ratio (OR) 0.50 (95% CI: 0.13 to 1.95) [I2=75%; P<0.01].

Mortality
According to the meta-analysis, favipiravir had no beneficial effect on reducing the odds of mortality in coronavirus: OR 1.11 (95% CI: 0.64 to 1.94) [I2=0%; P=0.69].

Meta-Analysis #7
The systematic review by Japanese, British, Vietnamese, Iraqi, and Egyptian experts examined the results of 14 clinical trials (13 randomized, 1 non-randomized) of favipiravir: 4 trials each in China (ChiCTR2000029544, ChiCTR2000029600, ChiCTR2000030254, ChiCTR2000030894) and Russia (NCT04434248, NCT04501783, NCT04542694, NCT04542694), 2 in Egypt (NCT04349241, NCT04351295), and 1 each in India (CTRI/2020/05/025114), Japan (jRCTs041190120), Oman (study), and Iran (study) — data from which were available as of early February 2021.
Conclusions
- Pros. In addition to speeding up ridding the body of SARS-CoV-2 coronavirus, favipiravir increased the chances of relief of fever, improvement in the radiological picture of lungs affected by COVID-19 infection, and discharge from the hospital.
- Cons. Favipiravir did not reduce the length of hospital stay or reduce the risk of death.
- Comments. Favipiravir accelerated elimination of coronavirus from the body although it only shortened the time required by less than one day. There is some evidence that favipiravir reduces the risk of lung fibrosis in the long term. Because of the high heterogeneity of studies, it is not possible to state unequivocally that favipiravir treatment results in overall clinical improvement. Favipiravir may contribute to clinical improvement in patients with COVID-19 but more reliable data are needed. It is possible that higher doses of favipiravir will lead to a significant increase in treatment efficacy but they may also be reflected by an increased incidence of adverse reactions.
- Bottom line. Favipiravir exhibits some clinical benefit but its magnitude is by no means significant enough to suggest beyond a reasonable doubt that widespread use of this drug, regardless of COVID-19 severity, is justified.
Details
Viral Clearance
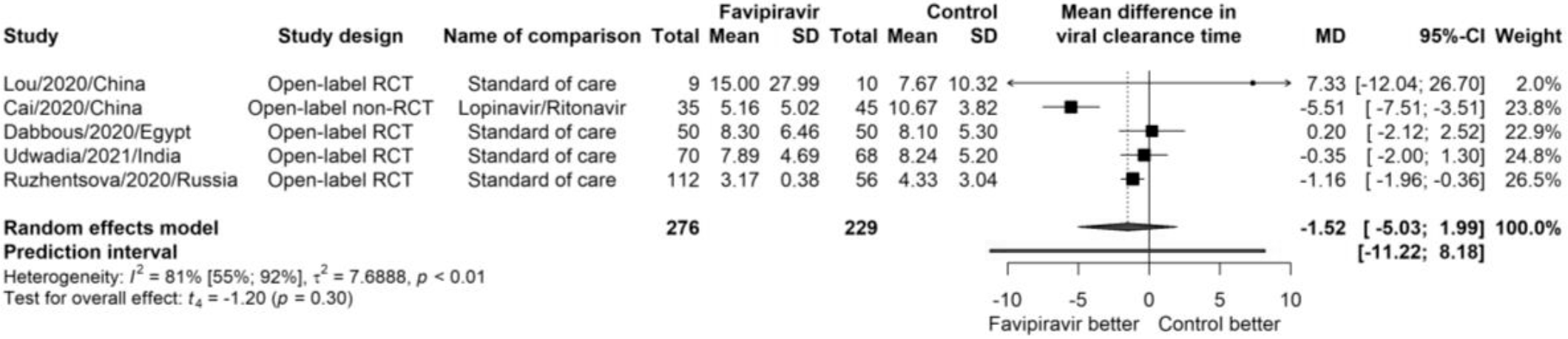
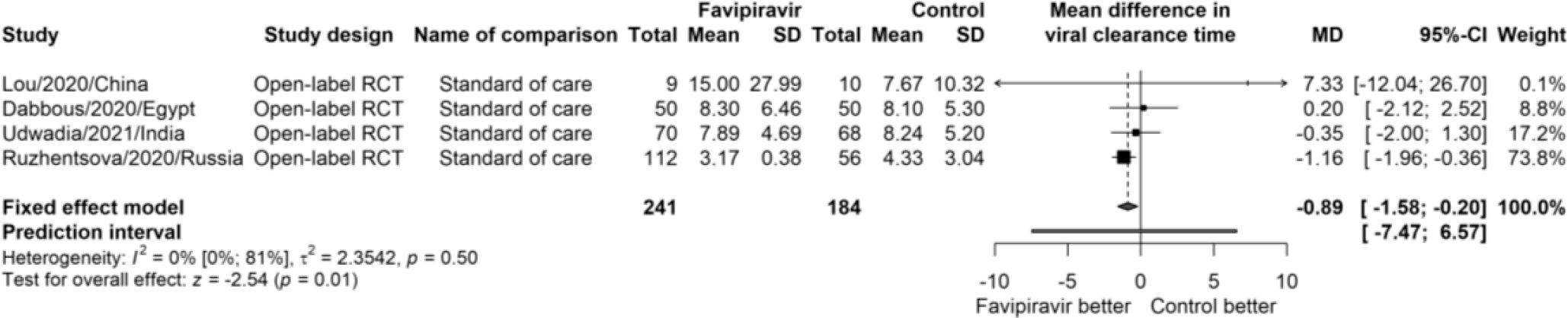
The meta-analysis found that although there was no statistically significant difference with the control group, favipiravir still accelerated elimination of SARS-CoV-2 coronavirus by reducing the time required for viral clearance by approximately 1.5 days: mean difference (MD) −1.52 (95% CI: −5.03 to 1.99; p=0.3) [I2=81%; P<0.01]. However, in sensitivity analyses (studies directly comparing favipiravir with other antivirals were excluded), heterogeneity decreased dramatically (I2=0%; P=0.50), making the difference statistically significant: MD −0.89 (95% CI: −1.58 to 0.20; p=0.01).
Clinical or Radiological Improvement
The meta-analysis found that adding favipiravir to standard treatment for COVID-19 infection did not result in a statistically significant rate of clinical improvement at day 10 because of high heterogeneity (I2=77%; P<0.01): risk ratio (RR) 1.54 (95% CI: 0.80 to 2.98); p=0.14.

However, a clinical improvement on day 3 still had a statistically significant difference, with favipiravir being almost twice as likely to provide relief of fever: RR 1.91 (95% CI: 1.5 to 2.34); p<0.01 [I2=0%; P=0.41].

The favipiravir group also showed an increased frequency of improvement in chest CT scan results on day 14–15: RR 1.40 (95% CI: 1.18 to 1.66); p<0.01 [I2=4%; p=0.37).

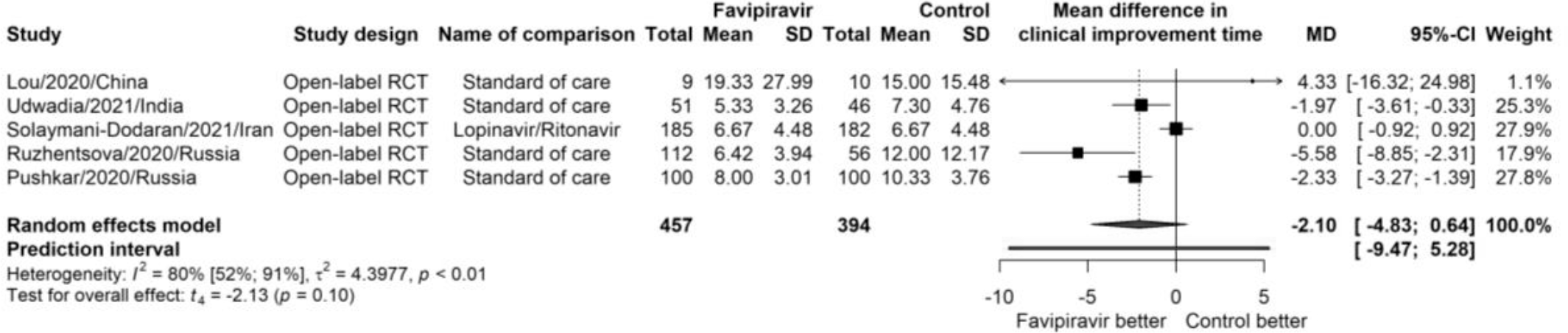
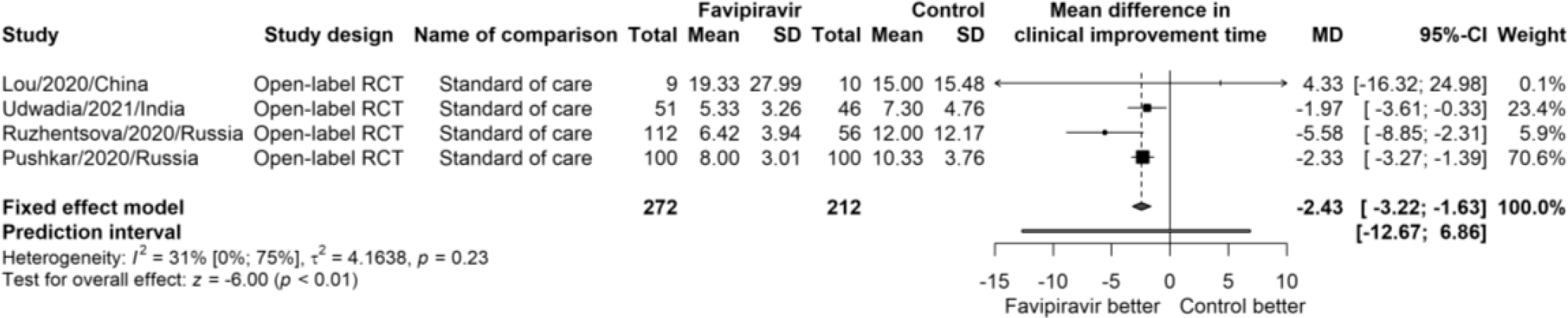
Despite the modest results, favipiravir marked a reduction in time to clinical improvement by an average of 2 days: MD −2.10 (95% CI: −4.83 to 0.64); p=0.10 [I2=80%; P<0.01]. Sensitivity analysis confirmed this: MD −2.43 (95% CI: −3.22 to −1.63); p<0.10 [I2=31%; P=0.23].
Discharge Rate and Length of Hospitalization
Favipiravir had a statistically significant effect on the rate of hospital discharge on day 10–11: RR 1.31 (95% CI: 1.13 to 1.51); p<0.01 [I2=0%; P=0.55). But did not on day 14–15: RR 1.00 (95% CI: 0.85 to 1.17); p=0.99 [I2=0%; P=0.58).


Favipiravir did not shorten hospital stay: MD −0.40 (95% CI: −1.09 to 0.29); p=0.26 [I2=27%; P=0.24).

Mortality
Favipiravir failed to outperform standard COVID-19 treatment when it comes to reducing the risk of mortality: RR 1.05 (95% CI: 0.67 to 1.63); p=0.84 [I2=0%; P=0.99].

Extras
Favipiravir versus other antiviral or standard of care for COVID-19 treatment: a rapid systematic review and meta-analysis. Virol J. 2020; 17: 141. [source]
Systematic review and meta-analysis of effectiveness and safety of favipiravir in the management of novel coronavirus (COVID-19) patients. Indian J Pharmacol. 2020 Sep-Oct; 52(5): 414–421. [source]
Favipiravir for the treatment of patients with COVID-19: a systematic review and meta-analysis. BMC Infect Dis. 2021; 21: 489. [source]
The efficacy and safety of favipiravir in treatment of COVID-19: a systematic review and meta-analysis of clinical trials. Sci Rep. 2021; 11: 11022. [source]
Favipiravir for the treatment of COVID-19. EUnetHTA Joint Action 3 WP4. Version 10.0, May 2021. [source] [PDF]
Effectiveness of favipiravir in COVID-19: a live systematic review. Eur J Clin Microbiol Infect Dis. 2021 Aug 4 : 1–9. [source]
The efficacy and adverse effects of favipiravir on COVID-19 patients: a systematic review and meta-analysis of published clinical trials and observational studies. Lancet Preprint. 2021 Jul 20. [source]