Highlights
China-based Kintor Pharmaceutical is developing an experimental oral proxalutamide to treat ambulatory and hospitalized patients with COVID-19 infection caused by the SARS-CoV-2 coronavirus.
Administration of proxalutamide to outpatients for more than 7 days has been demonstrated to reduce the risk of hospitalization or death by 100%, regardless of patient age or inherent risk factors.
The use of proxalutamide in inpatients has been shown to reduce the risk of death by 80% and to reduce the time of stay in a hospital facility by 4 days.
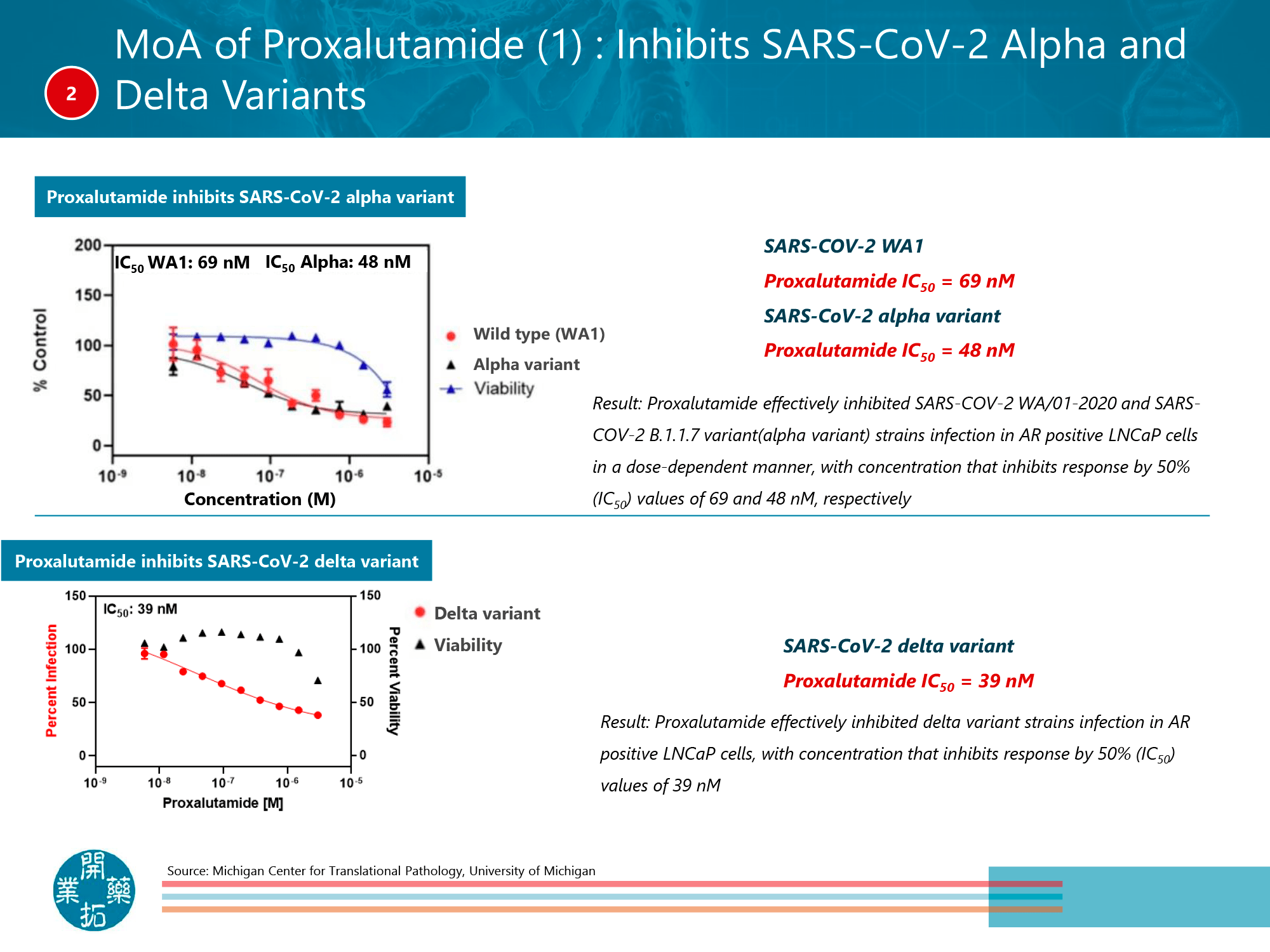
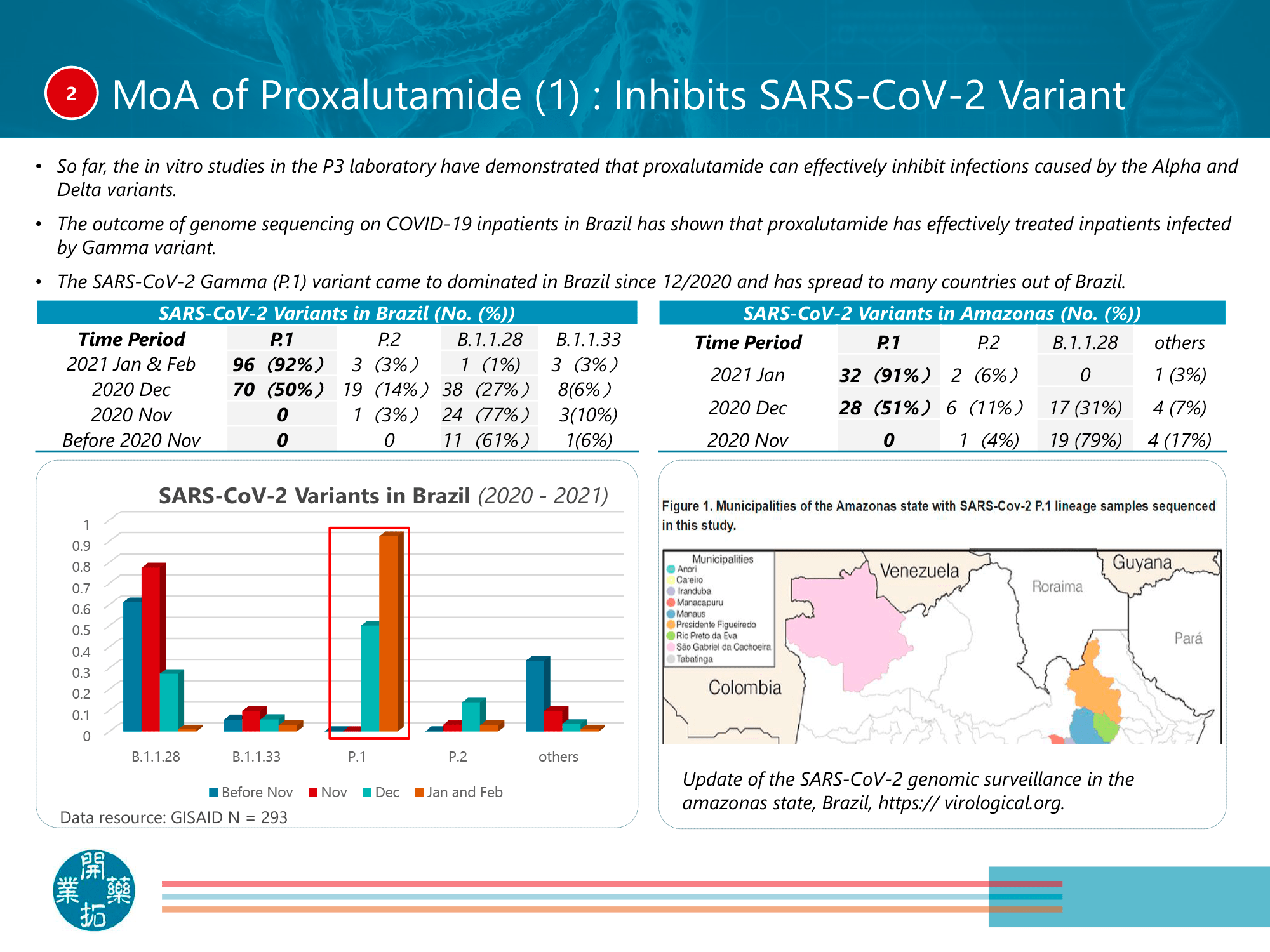
Proxalutamide has been confirmed to effectively reduce the viral load of the original SARS-CoV-2 and its Alpha, Gamma, Delta, and Omicron variants.
Proxalutamide, being an androgen receptor (AR) inhibitor, was originally developed to treat prostate cancer and breast cancer.
The supposed brand name for proxalutamide is Kropsen.
Kintor plans to seek approval of proxalutamide for the treatment of COVID-19 from regulators in China, the US and other countries.
Proxalutamide has already received official approval to treat patients hospitalized with COVID-19: in Paraguay (mid-July 2021), Sarajevo Canton in Bosnia and Herzegovina (January 2022), Ghana (mid-March 2022).
Kintor’s current production capacity allows for up to 1 million packs (28 100-mg pills each) of proxalutamide per month and the Chinese company aims to ramp up production to 50 million packs of proxalutamide per year by the end of 2022.
The cost of a course of COVID-19 treatment with proxalutamide promises to be affordable. The final price has not yet been announced.

Kropsen: Clinical Efficacy and Safety of Proxalutamide in Treating Patients With COVID-19
NCT04870606: Outpatients With Mild-to-Moderate COVID-19
Registration clinical trial NCT04870606 phase 3 (randomized, double-blind, placebo-controlled, multicenter) enrolled non-hospitalized US adult patients (n=733) with mild-to-moderate COVID-19 infection with symptoms manifesting within 5 days before randomization.
Subjects received standard COVID-19 therapy plus 200-mg proxalutamide once daily or placebo for 14 days.
Among the efficacy endpoints of the treatment:
- The proportion of patients who did not require hospitalization for any reason for at least 24 hours after initiation of treatment or who did not need supplemental oxygen (with oxygen saturation [SpO2] ≤ 93%) for at least 24 hours after initiation of treatment.
- Proportion of patients who were alive by day 28 of the study.
- Proportion of patients hospitalized for any reason for 24 hours or more after initiation of treatment who required oxygen therapy or who died by day 28.
- Change in viral load during the 28-day period.
The results of treatment were as follows:
- Proxalutamide reduced the risk of hospitalization or death by 50% if the drug was taken for at least 1 day (n=730): in the placebo group, 8 patients were hospitalized (1 died) — in the proxalutamide group, 4 were hospitalized (no deaths).
- Proxalutamide reduced the risk of hospitalization or death by 71% if the drug was taken for more than 1 day (n=721): in the placebo group, 7 patients were hospitalized (1 died) — in the proxalutamide group, 2 people were hospitalized (no deaths).
- Proxalutamide reduced the risk of hospitalization or death by 100% (p<0.02) if the drug was taken for more than 7 days (n=693): 6 patients were hospitalized in the placebo group (1 died) — no one was hospitalized in the proxalutamide group (no deaths).
- Proxalutamide administered for at least 1 day reduced the risk of hospitalization or death by 100% (p<0.02) among patients aged 50 years or older with or without comorbid risk factors (obesity) and those aged 60 years or older with comorbid risk factors (obesity, diabetes, hypertension, etc.). No hospitalizations or deaths were reported in the proxalutamide group.
- Proxalutamide statistically significantly compared to placebo (p<0.01) provided a continuous reduction in viral load from day 3 to day 28.
- Administration of proxalutamide resulted in improvement of COVID-19-related symptoms such as fever, dyspnea, and cough when compared to placebo at 28 days.
- The safety profile of proxalutamide was characterized by acceptable tolerability. The incidence of treatment-emergent adverse events (TEAEs) was comparable in both groups, with 9.6% of patients treated with proxalutamide and 7.9% with placebo. The most common one related to dizziness: 1.1% of patients in the proxalutamide and placebo groups. No serious adverse reactions were noted.
NCT04446429: Outpatients With Mild COVID-19
The clinical trial NCT04446429 (randomized, double-blind, placebo-controlled) among non-hospitalized adult men (n=268) from Brazil with a COVID-19 infection diagnosed within 7 days before randomization and occurring in mild form.
Participants received standard therapy plus 200-mg proxalutamide once daily or placebo for 7 days.
During the 30-day period following randomization, 3 patients (2.2%) in the proxalutamide group and 35 subjects (26.1%) in the placebo group were admitted to a hospital facility. Thus, proxalutamide administration resulted in a 91% reduction in risk of hospitalization compared with placebo: risk ratio (RR) 0.09 (95% CI: 0.03–0.27).
No deaths were reported among those receiving proxalutamide — 2 people (1.6%) died in the control group.
The most common treatment-emergent adverse events (TEAEs) were as follows: diffuse sweating (in 36% of patients in the proxalutamide group and 4% in the placebo group), diarrhea (21% and 9%), and dyspepsia or heartburn (17% and 5%).
NCT04728802 and NCT05126628: Inpatients With Severe COVID-19
The NCT04728802 and NCT05126628 phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trials conducted in Brazil included adult patients (n=778) hospitalized with COVID-19 infection within 7 days before randomization.
COVID-19 was mainly severe: 64% of subjects required non-invasive ventilation or high-flow oxygenation, and 31% required supplemental oxygen.
Participants underwent standard treatment and received 300-mg proxalutamide once daily or placebo for 14 days.
At the 14-day therapy period, 81.1% of patients in the proxalutamide groups were recovered — versus 36.6% in the placebo groups: risk ratio (RR) 2.21 (95% CI: 1.92–2.56); p<0.0001. Over a period of 28 days, 86.1% of subjects recovered — vs. 47.6%: RR 1.81 (95% CI: 1.61–2.03); p<0.0001.
A fatal outcome from any cause at 14 days was reported for 8.0% of patients in the proxalutamide groups — vs. 39.2% in the placebo groups. Thus, proxalutamide administration provided an 80% reduction in the relative risk of death: RR 0.20 (95% CI: 0.14–0.29); p<0.0001. At 28 days, the all-cause mortality rate was 10.6% — vs. 48.2%, equivalent to a 78% reduction in relative risk of death: RR 0.22 (95% CI: 0.16–0.30); p<0.0001.
Use of proxalutamide reduced hospital stay by a median of 4 days: 8 (interquartile range [IQR] 6–13) days — vs. 12 (IQR 8–18) days (p<0.0001).
The proxalutamide groups demonstrated statistically significant lower use of concomitant antibiotics (cephalosporins, macrolides, vancomycin, meropenem, piperacillin/tazobactam) during the study period, indicating less likelihood of secondary bacterial infection, and colchicine (p<0.0001).
Among the most common treatment-emergent adverse events (TEAEs) were: diarrhea (in 18.2% of patients in the proxalutamide group and 3.4% in the placebo group), irritability (2.1% and 0.0%), and abdominal pain (1.2% and 0.6%).
Kropsen: Mechanism of Action of Proxalutamide
Proxalutamide (GT0918) is a second-generation oral, small-molecule, non-steroidal androgen receptor (AR) inhibitor.
Kintor originally developed proxalutamide to treat AR-associated diseases such as metastatic castration-resistant prostate cancer and metastatic hormone receptor positive (HR+) and androgen receptor positive (AR+) breast cancer. A topical version of proxalutamide is being tested in the treatment of androgenetic alopecia and acne vulgaris.
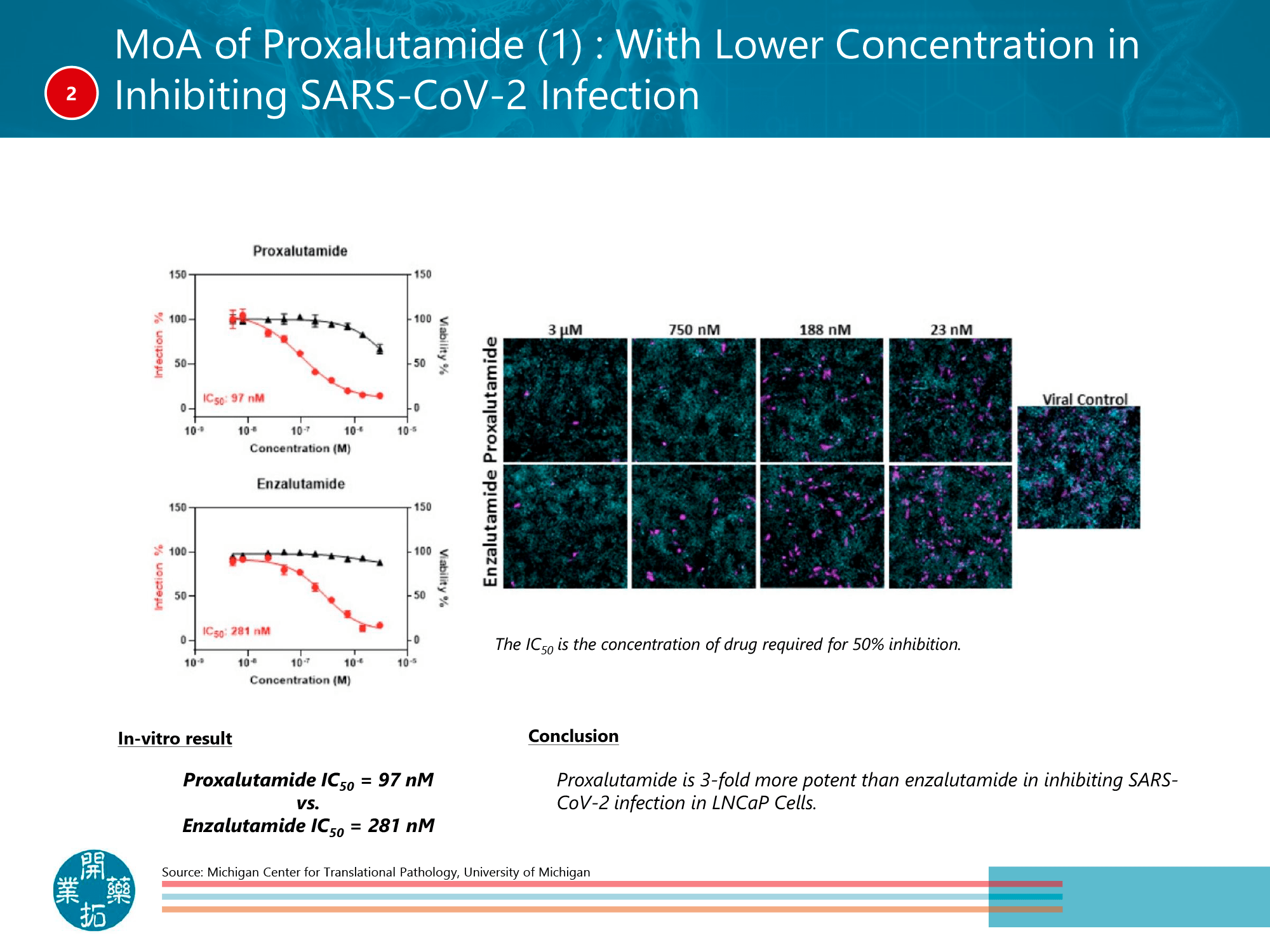
Although the molecule of proxalutamide is very similar to enzalutalumide, a blockbuster by Pfizer and Japanese Astellas Pharma known as Xtandi and successfully used in the treatment of prostate cancer, its chemical structure is modified and optimized by automated design based on the crystal structure of the target protein. The modifications introduced in the proxalutamide improved its molecular solubility and pharmacokinetic properties, thus avoiding excessive accumulation of the drug. This also led to the elimination of clinically manifested negative side effects, including those of the central nervous system. In general, proxalutamide has a higher targeting activity than enzalutalumide and has a dual mechanism of action: proxalutamide both inhibits and downregulates AR and inhibits the expression of target AR genes.
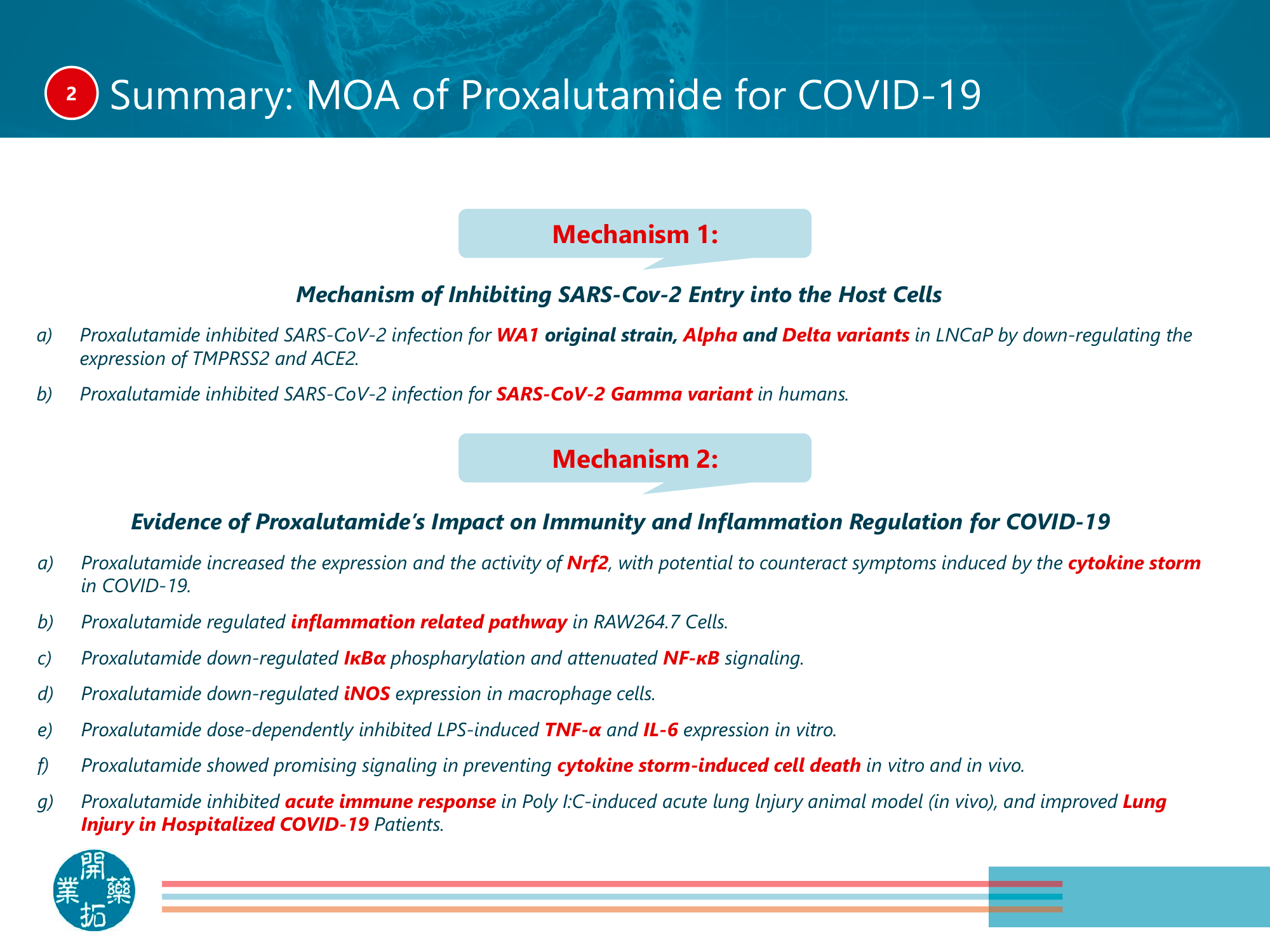
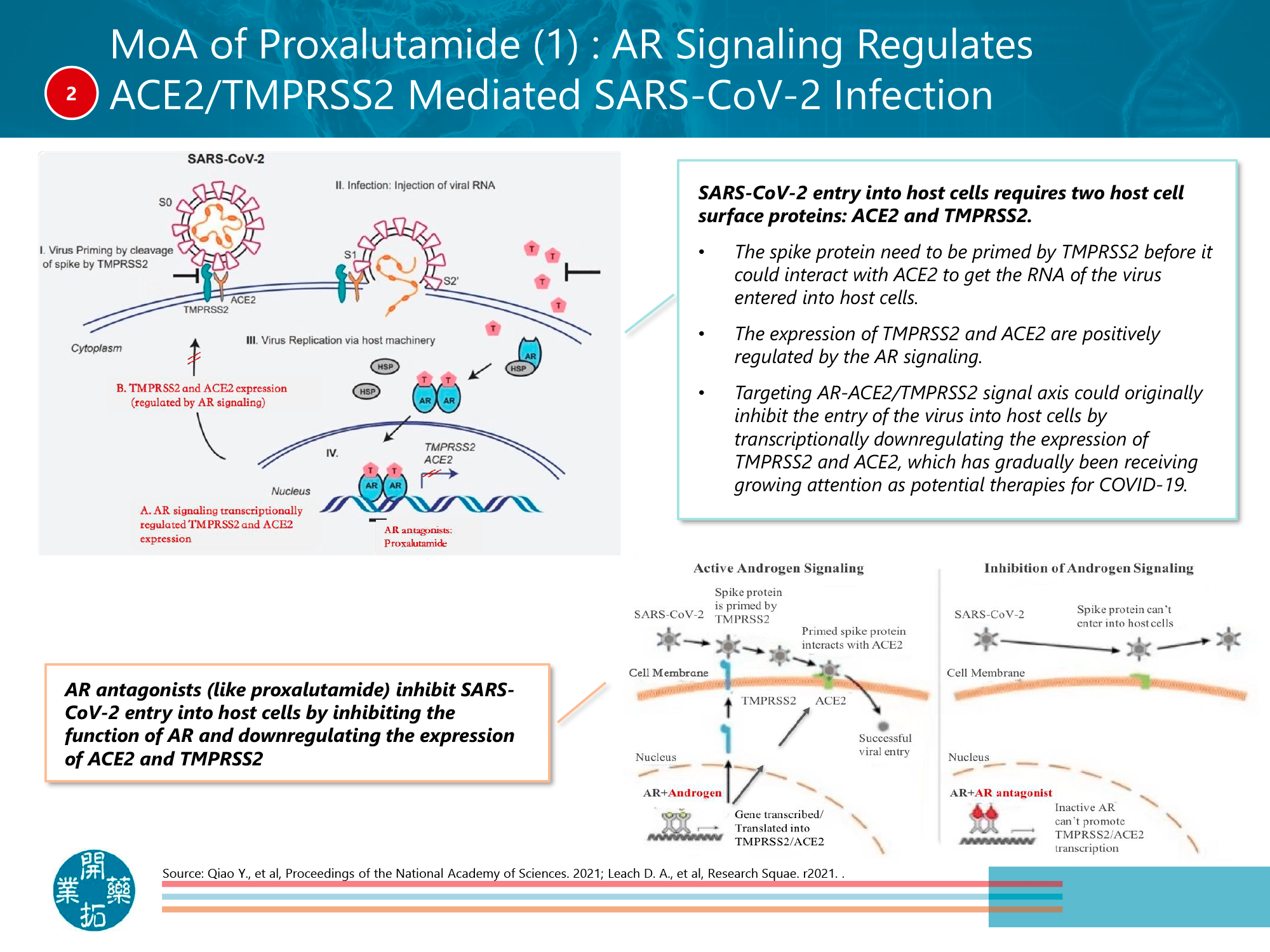
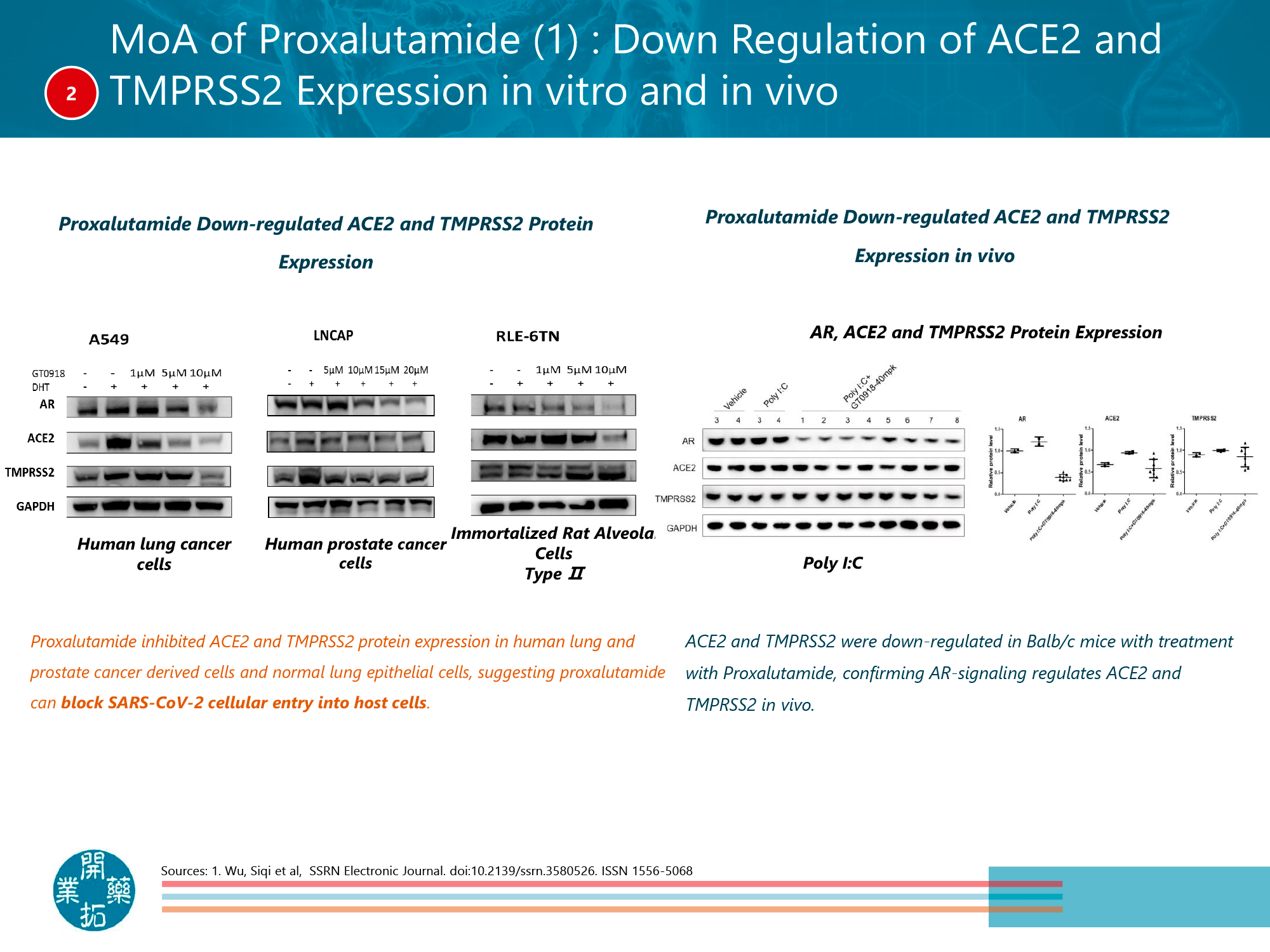
If we talk about the mechanism of action of proxalutamide in the context of COVID-19 infection, the drug works as follows. SARS-CoV-2 coronavirus addresses transmembrane serine protease 2 (TMPRSS2) for proteolytic priming of its S protein for subsequent viral and cell membrane fusion via transmembrane angiotensin-converting enzyme 2 (ACE2) as the main entry point of the virus. The TMPRSS2 gene promoter has an androgen response element (ARE) of 15 base pairs, and the growth of TMPRSS2 protein expression is mediated by a single endogenous regulator, represented by AR. AR activation also induces ACE2 expression. Thus, AR inhibition reduces TMPRSS2 and ACE2 expression, inhibiting SARS-CoV-2 entry into body cells. [1] [2] [3]
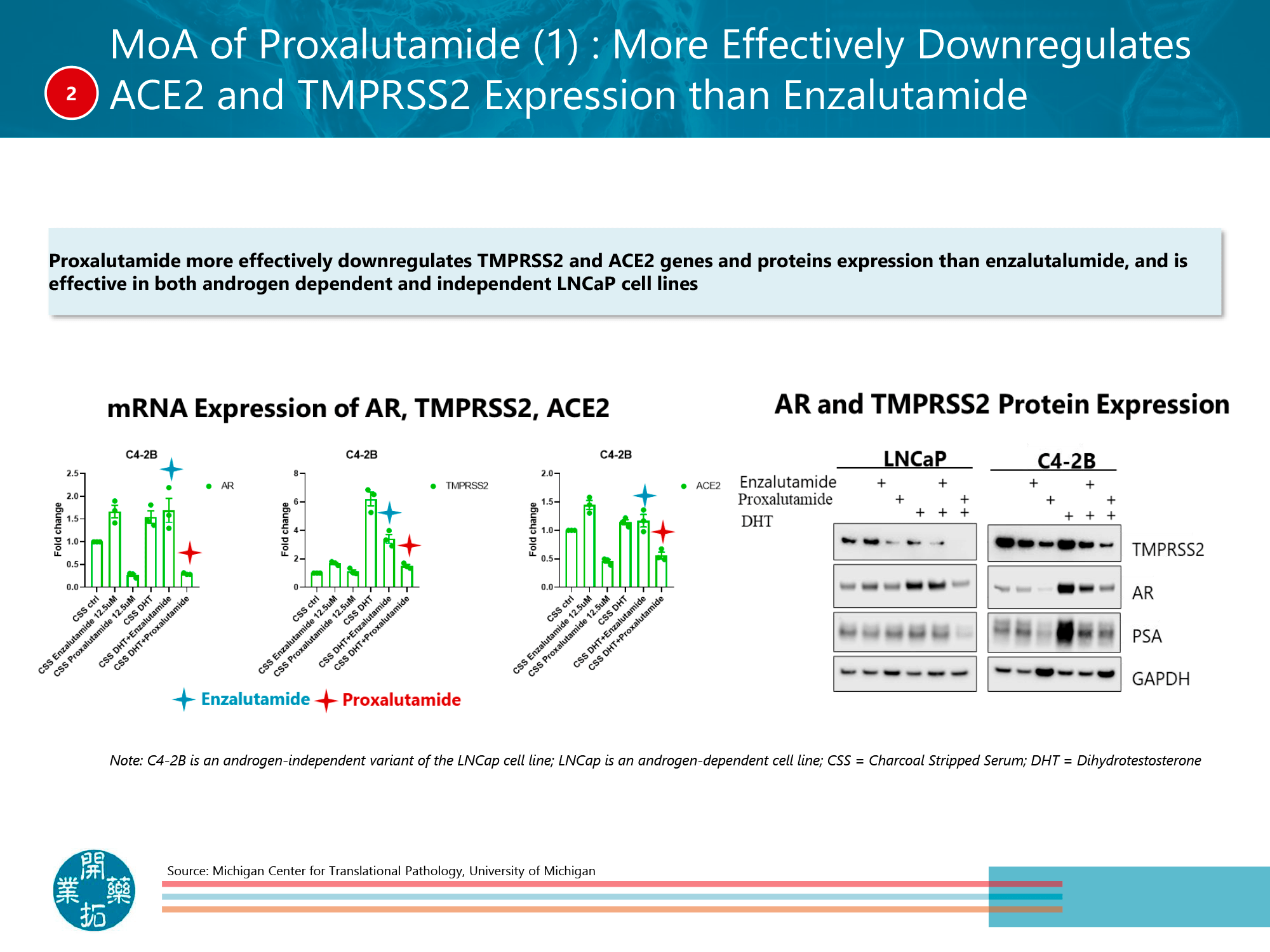
Proxalutamide is more effective than enzalutamide in reducing TMPRSS2 and ACE2 gene and protein expression, and it is effective in both androgen-dependent and independent LNCaP cell lines.
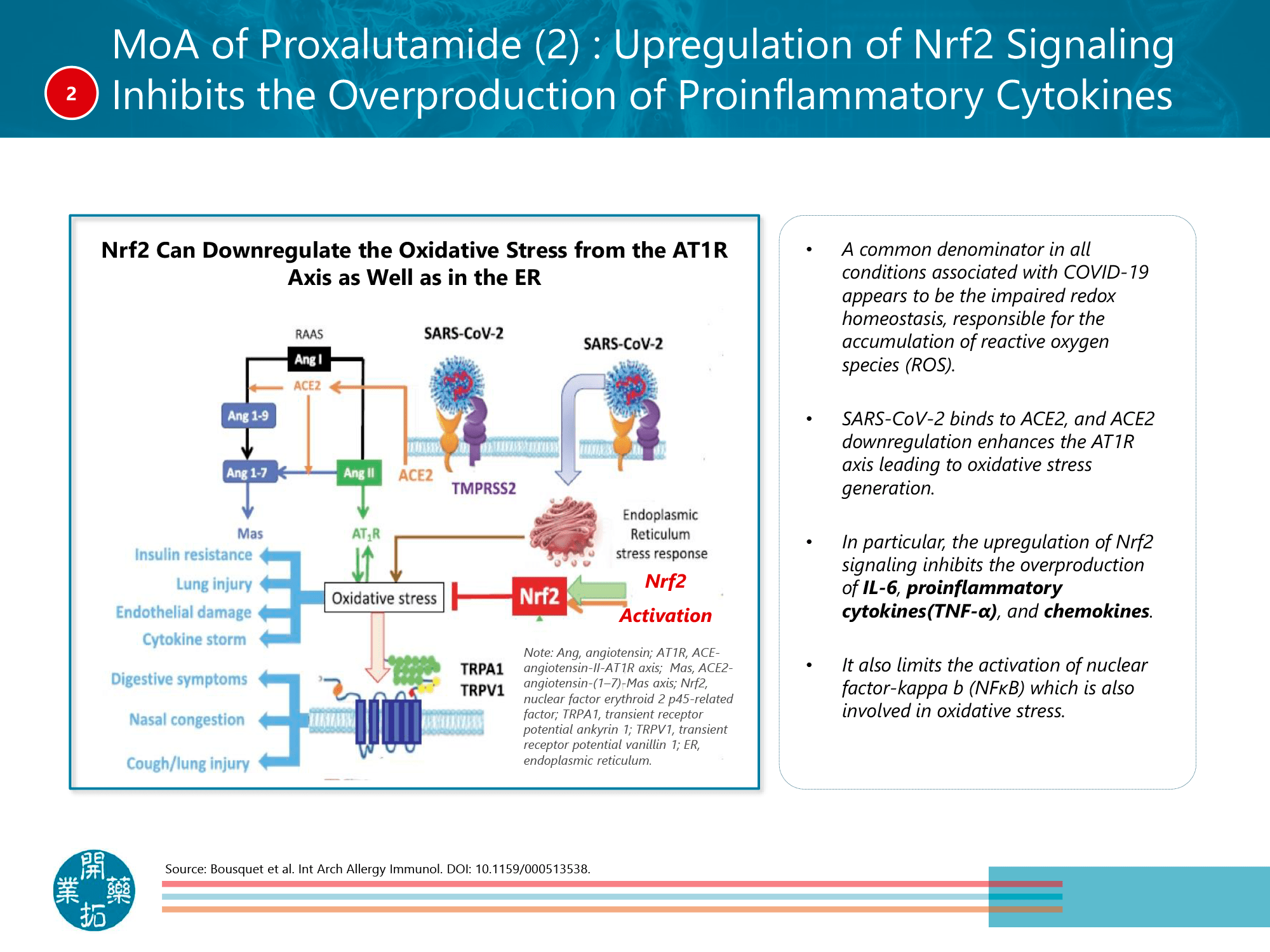
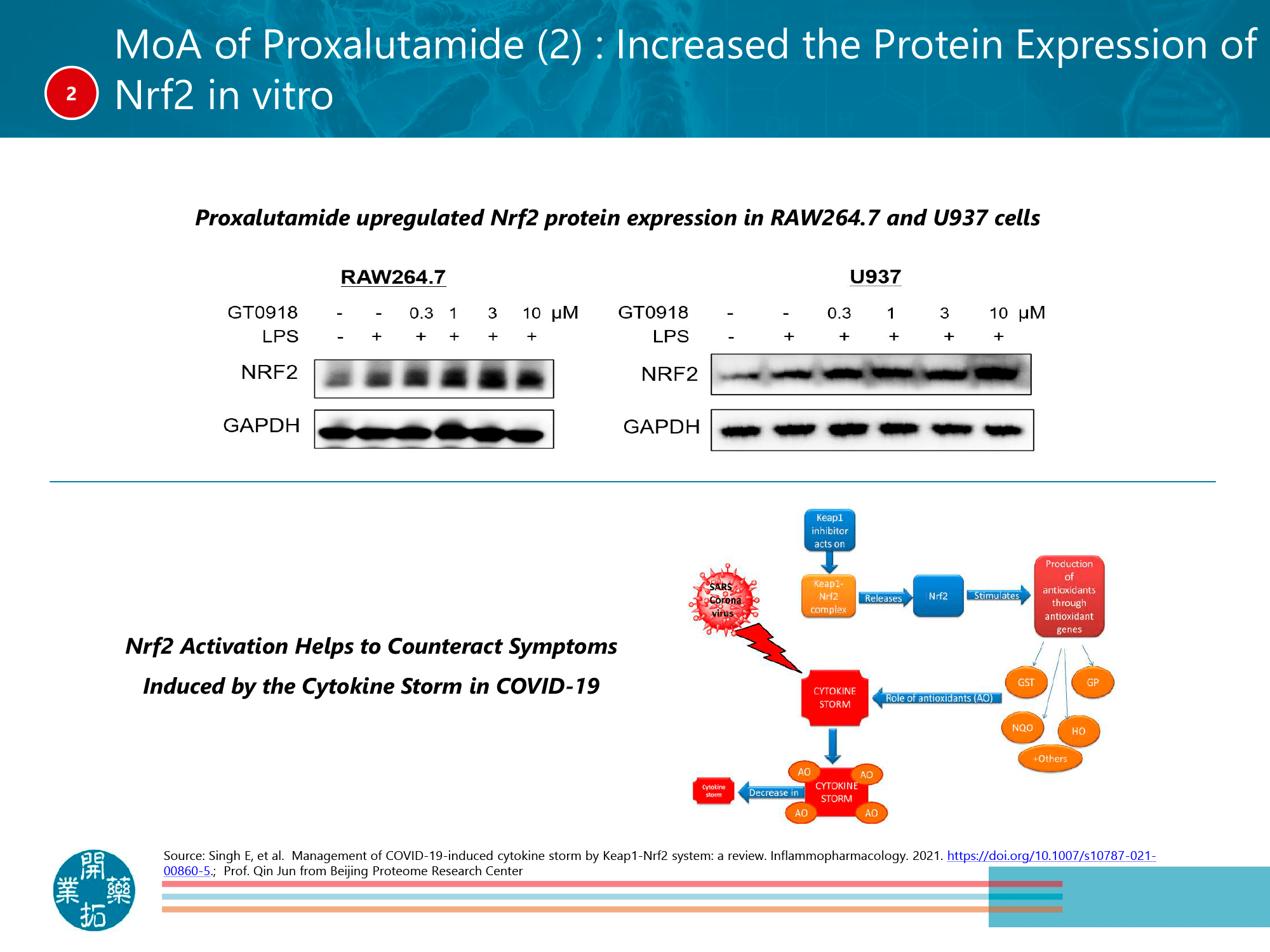
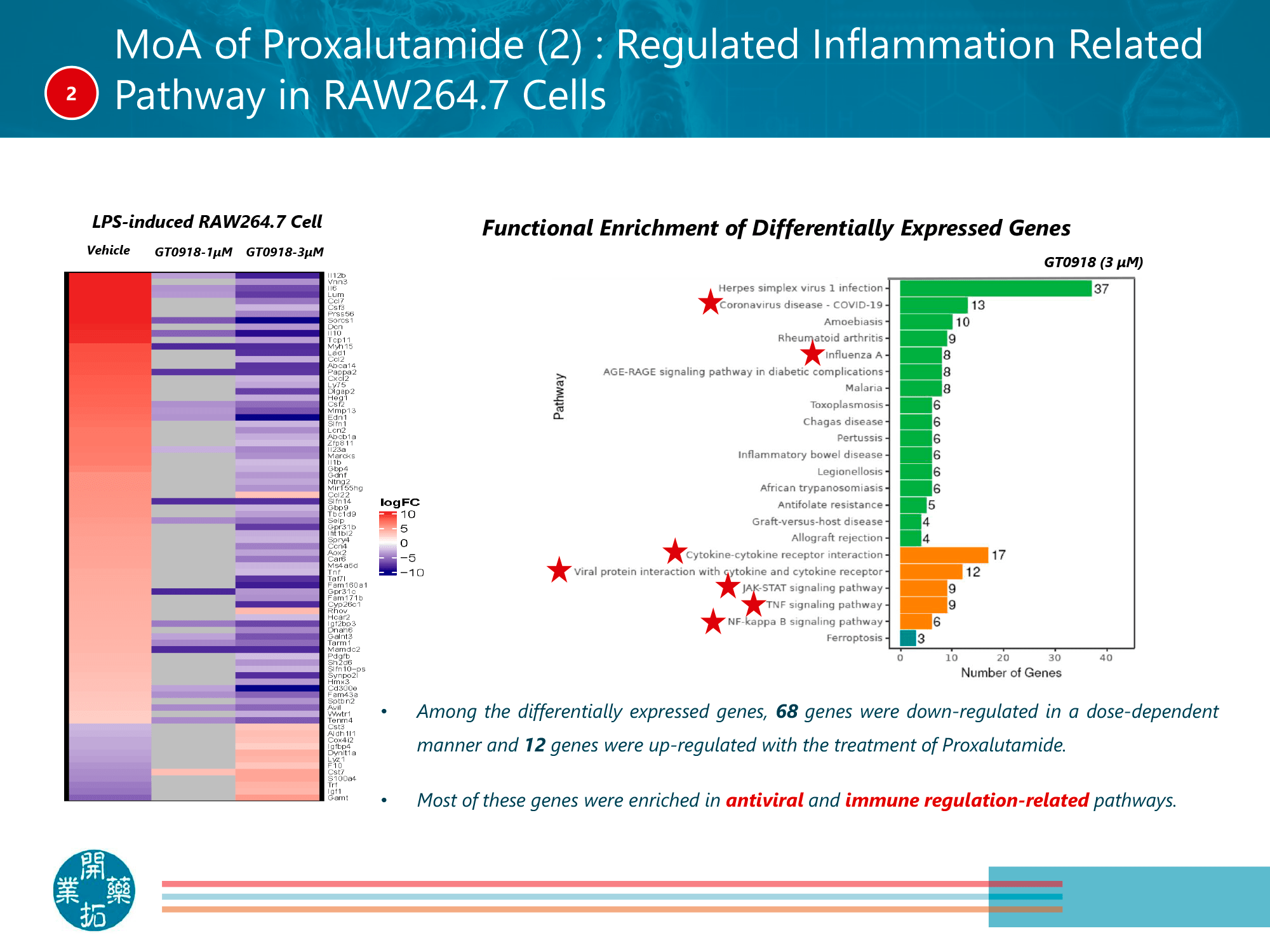
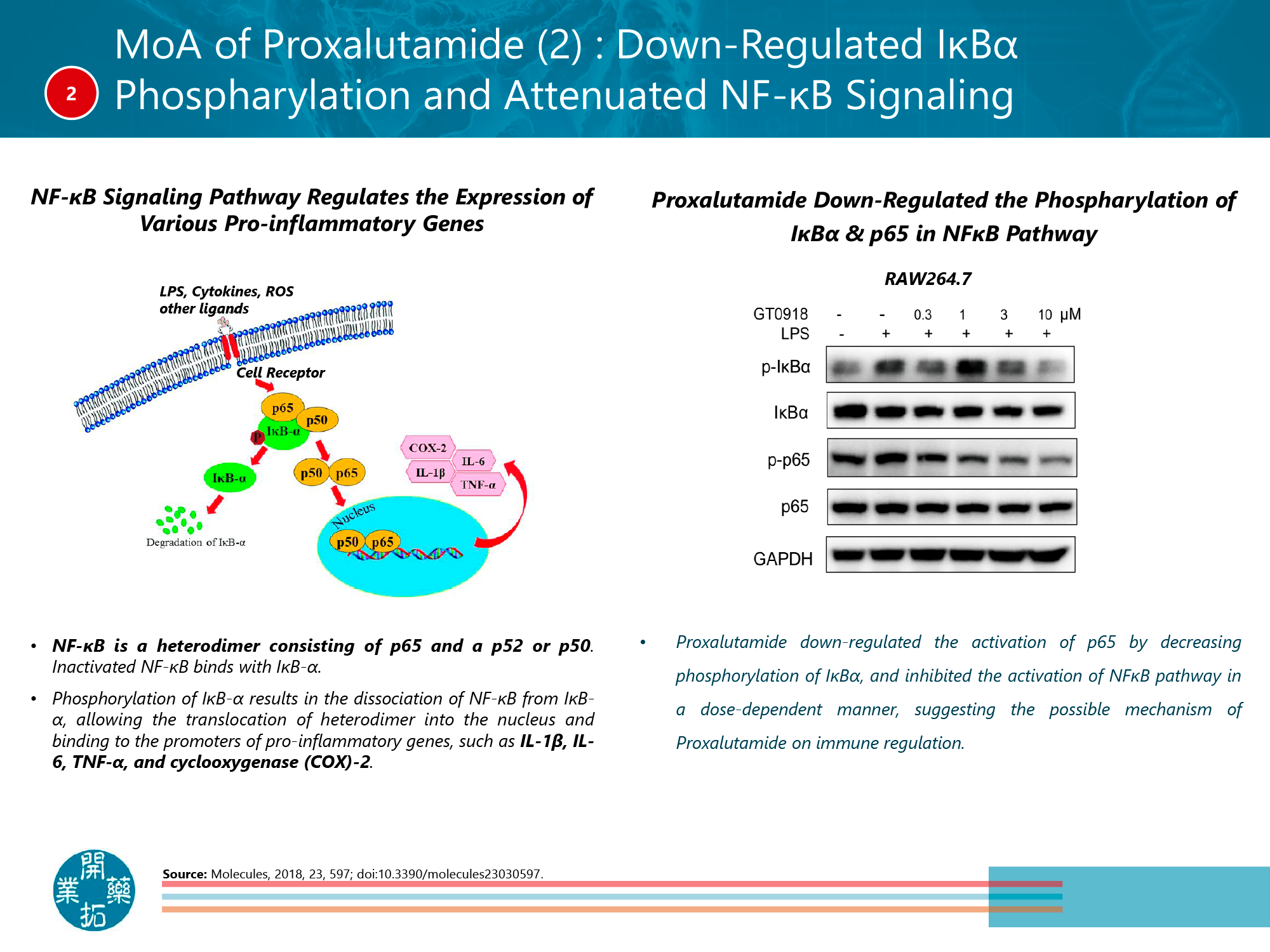
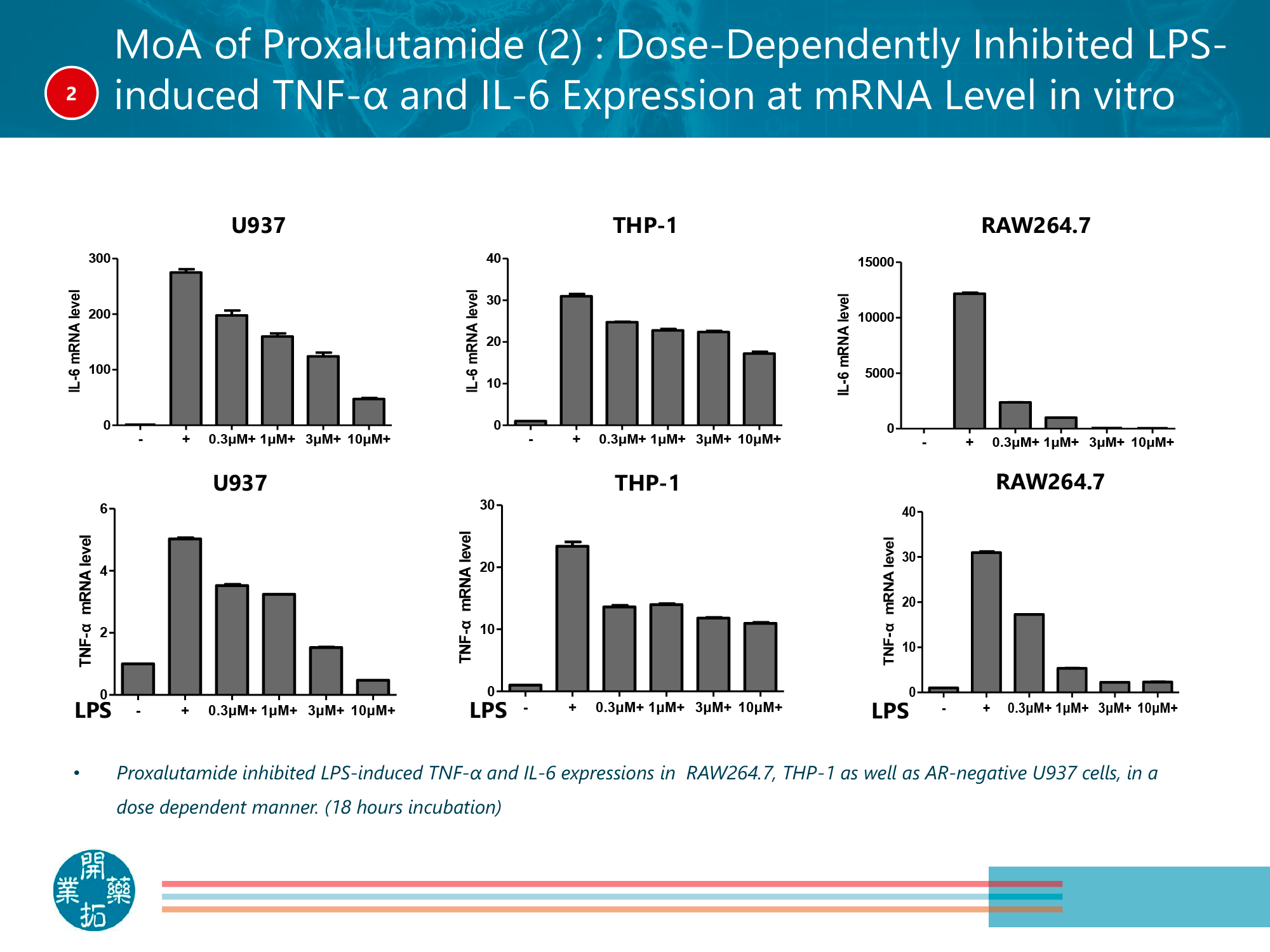
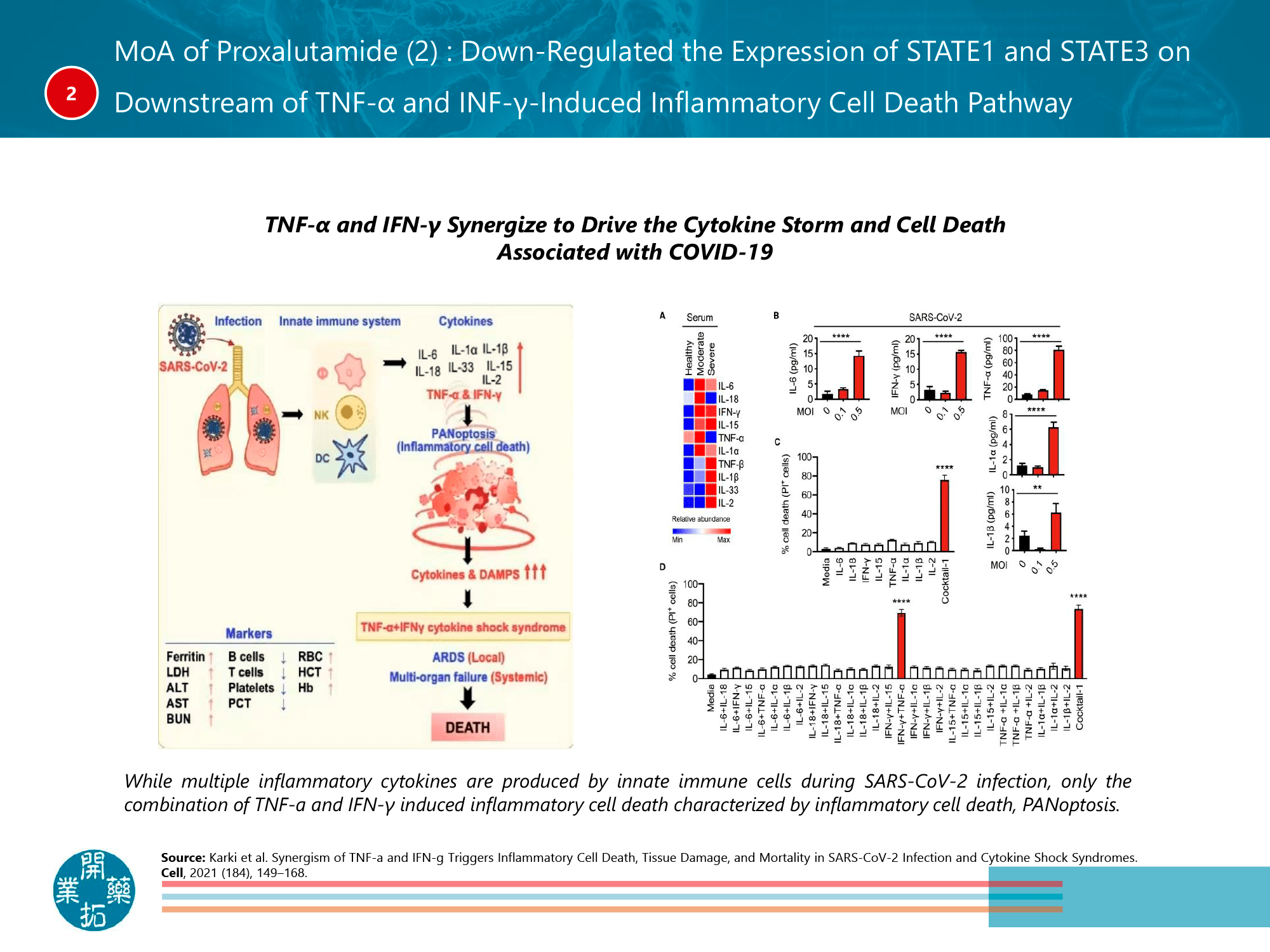
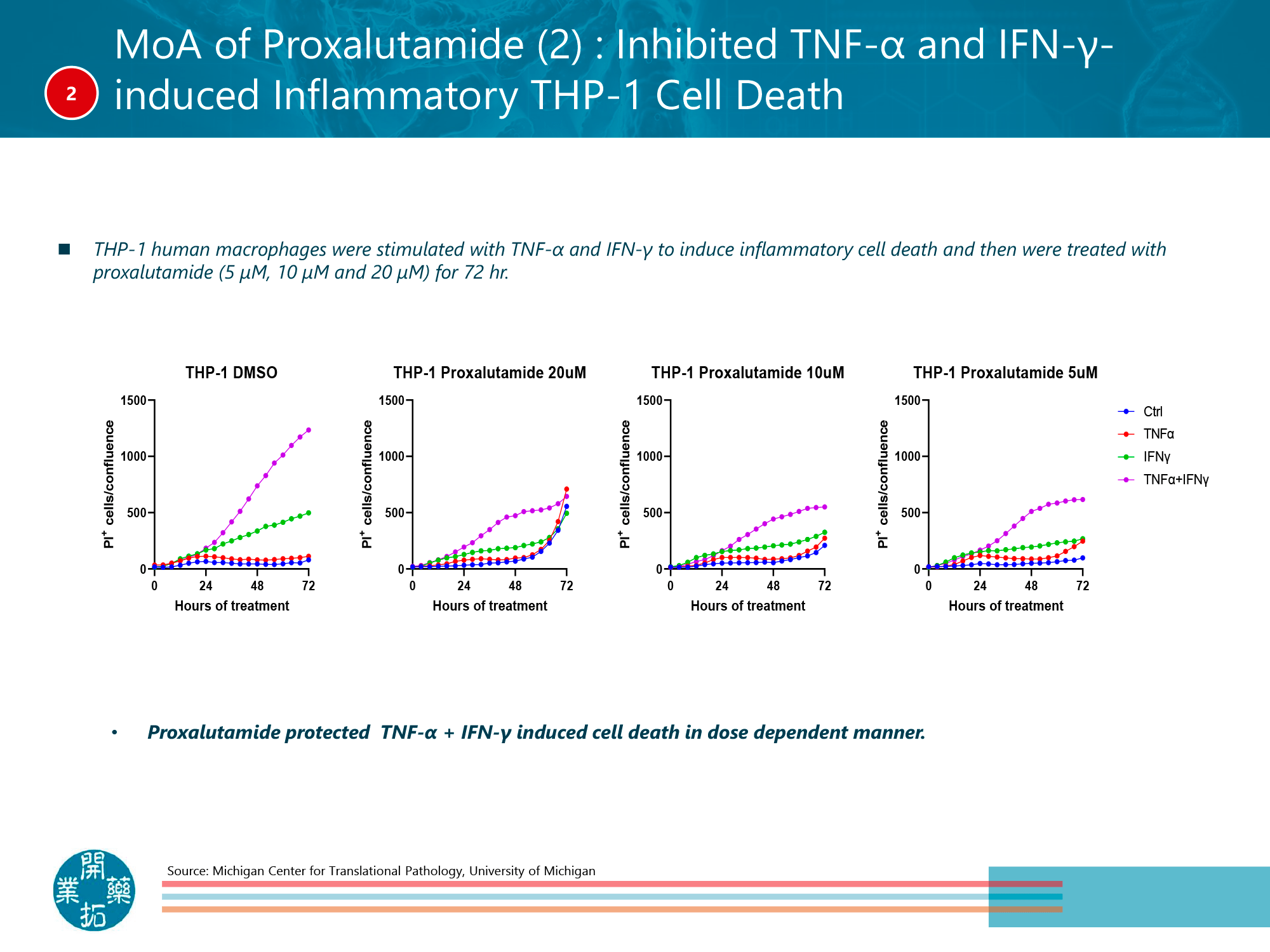
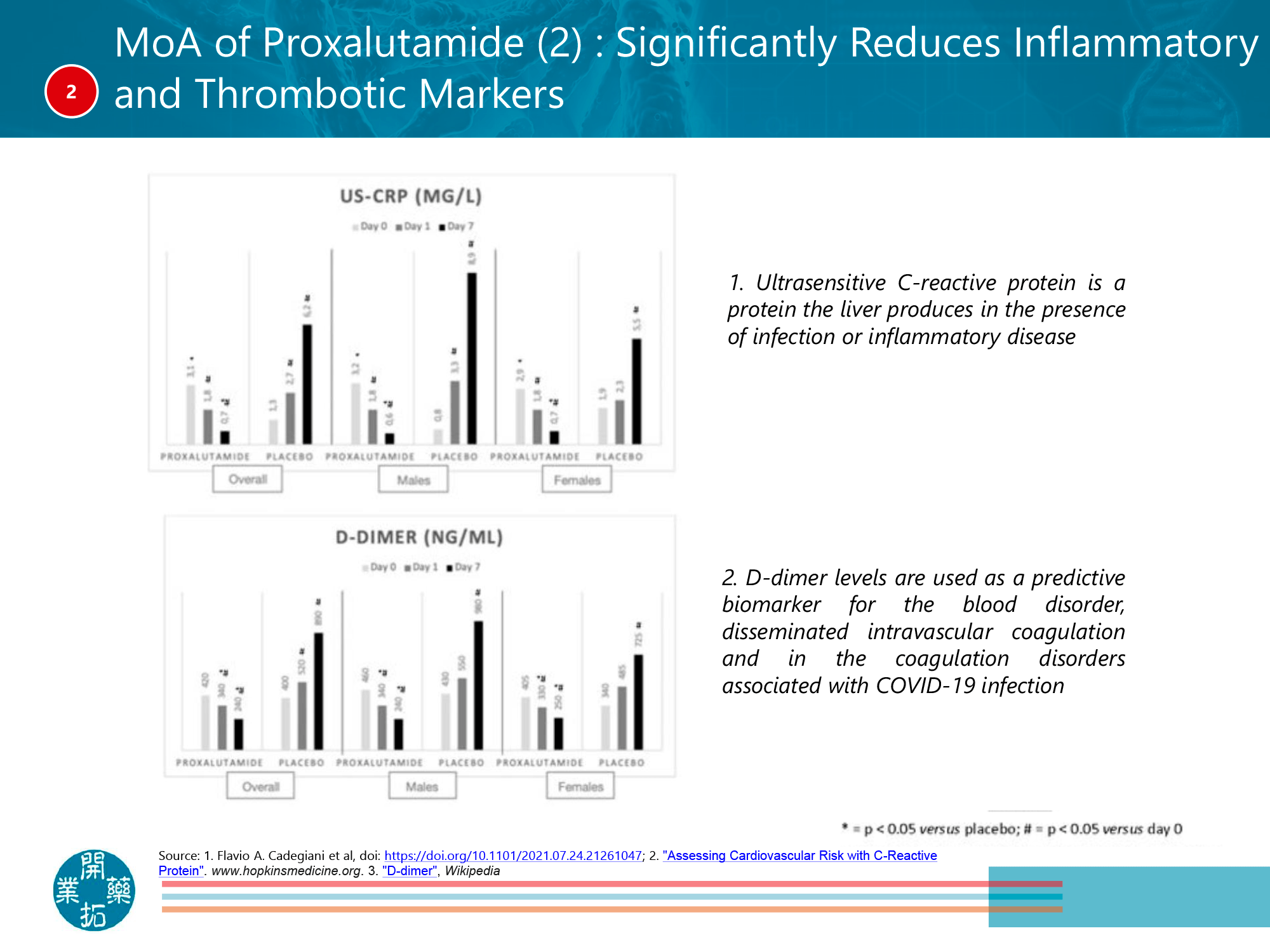
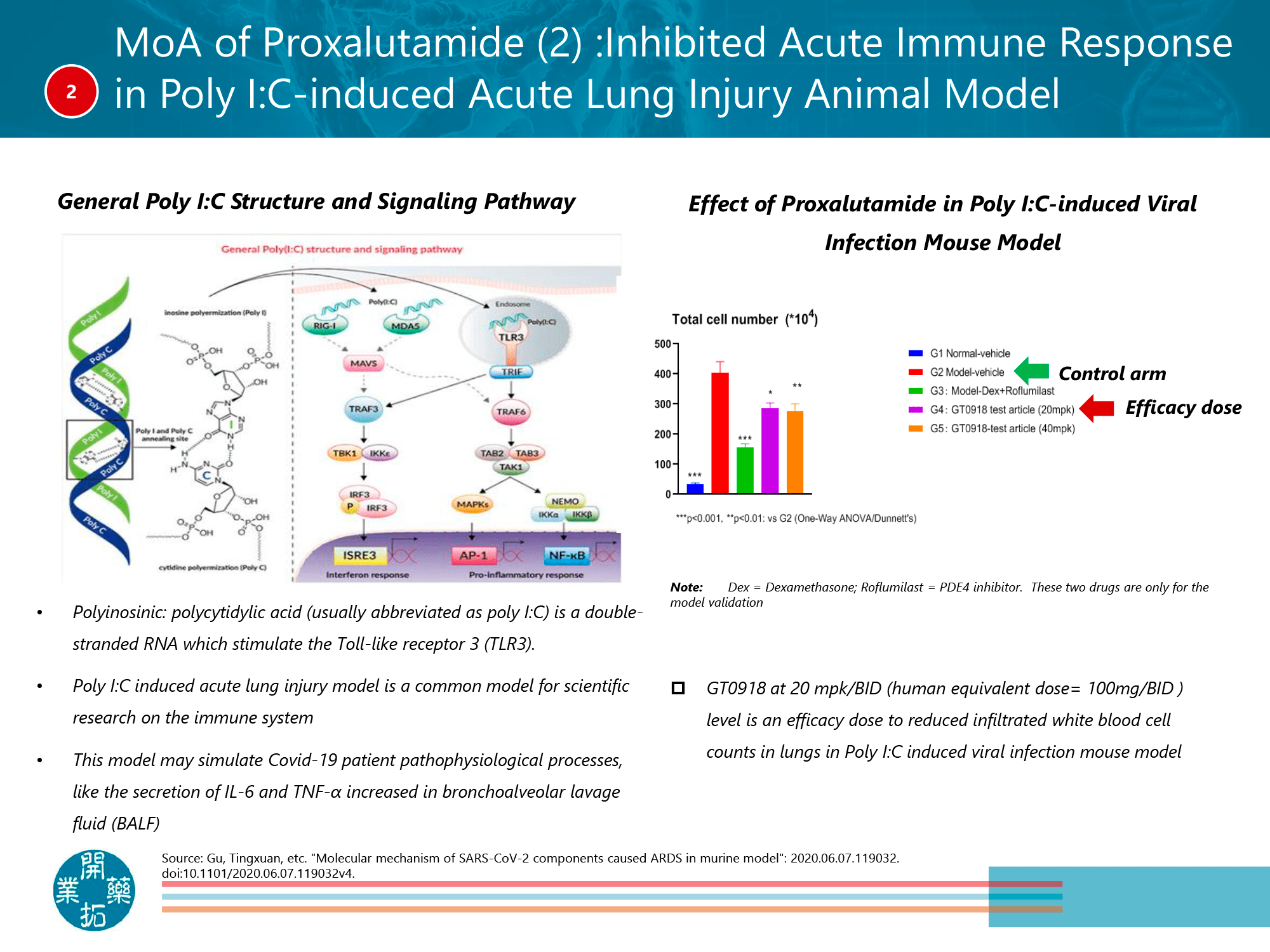
In the more severe COVID-19 proxalutamide promotes pathogen clearance and reduces inflammation by activating the nuclear factor erythroid 2-related factor 2 (Nrf2) pathway in macrophages, which leads to stimulation of the antioxidant-responsive element (ARE), reflected by suppression of the cytokine storm that causes tissue and organ damage. Activation of Nrf2 also induces inhibition of the expression of chemokines and proinflammatory cytokines in macrophages including tumor necrosis factor (TNF) and interleukin 6 (IL-6), and limits the activity of nuclear factor NF-κB, which is involved in oxidative stress leading to the accumulation of reactive oxygen species (ROS) responsible for inflammation. Proxalutamide blocks interferon gamma (IFN-γ) signaling by reducing the expression of signal transducer and activator of transcription 1 (STAT1) in immune cells. Proxalutamide decreases the levels of reactive C-protein and D-dimer and increases the number of lymphocytes, biomarkers of clinical progression of COVID-19. [4] [5] [6] [7] [8] [9]
Proxalutamide: What’s Next
Two clinical trials are ongoing to confirm the therapeutic benefit of proxalutamide in the treatment of COVID-19 infection in outpatients and inpatients:
- NCT04869228 phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial of proxalutamide among outpatients (n=724) aged 45 years and older with mild-to-moderate COVID and risk factors for its complications. Participants from Brazil, China, Malaysia, and the Philippines are being recruited.
- NCT05009732 phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial testing dose-enhanced proxalutamide (300 mg) in the treatment of hospitalized patients with COVID-19 (n=762) from Brazil, China, Philippines, South Africa, and US. Among the main criteria for participation: dyspnea (respiratory rate ≥ 30/min), lung radiological infiltrates with more than 50% progression over 24–48 hours, oxygen saturation (SpO2) ≤ 93%, arterial oxygen partial pressure to fractional inspired oxygen ratio (PaO2/FiO2) ≤ 300 mm Hg.
Extras
Kintor Pharma. Developing novel drugs and commercialization platform. April 8, 2022. [PDF]
Targeting transcriptional regulation of SARS-CoV-2 entry factors ACE2 and TMPRSS2. Proc Natl Acad Sci U S A. 2020 Dec 11;118(1):e2021450118. [source]
The antiandrogen enzalutamide downregulates TMPRSS2 and reduces cellular entry of SARS-CoV-2 in human lung cells. Nat Commun. 2021 Jul 1;12(1):4068. [source]
Final results of a randomized, placebo-controlled, two-arm, parallel clinical trial of proxalutamide for hospitalized COVID-19 patients: A multiregional, joint analysis of the Proxa-Rescue AndroCoV trial. Cureus. 2021 Dec 25;13(12):e20691. [source]
Proxalutamide reduces the rate of hospitalization for COVID-19 male outpatients: A randomized double-blinded placebo-controlled trial. Front Med (Lausanne). 2021; 8: 668698. [source]
Proxalutamide significantly accelerates viral clearance and reduces time to clinical remission in patients with mild to moderate COVID-19: Results from a randomized, double-blinded, placebo-controlled trial. Cureus. 2021 Feb 22;13(2):e13492. [source]