Highlights
Igalmi (dexmedetomidine) is a new drug indicated for the acute treatment of agitation episodes associated with schizophrenia or bipolar I or II disorder in adults.
Igalmi is a long-known dexmedetomidine, implemented in a mouth-dissolving, thin-film sublingual formulation. Igalmi is administered under the tongue or behind the lower lip.
Igalmi, developed by BioXcel Therapeutics, is approved by the U.S. Food and Drug Administration (FDA) in April 2022.
Igalmi will enter the U.S. market in the second quarter of 2022.
The price of Igalmi is not yet known, and that may be a problem given the mass of inexpensive generics used to treat agitation.
According to industry observers, Igalmi could eventually become a blockbuster, crossing the $1 billion-a-year sales mark. This is true if the drug is able to connect with other indications including agitation in dementia.

What Is Agitation
Agitation, defined as a state of excessive psychomotor activity accompanied by increased mental tension and irritability, is a common and difficult to treat symptom associated with a number of psychiatric illnesses, including schizophrenia and bipolar disorder.
According to some estimates, up to a quarter of patients with schizophrenia or bipolar disorder experience agitation. Agitation episodes can occur 10 to 17 times per year.
Agitation can also accompany other pathophysiological conditions such as neurological (e.g., stroke, head injury, dementia), cardiac (acute coronary syndrome, heart failure, arrhythmia), vascular (aortic aneurysm or dissection), pulmonary (pulmonary embolism, pneumonia), gastrointestinal (gastrointestinal bleeding, intraabdominal infection), urogenital (urinary tract infection, kidney stone), toxicological (alcohol intoxication, alcohol withdrawal, drug poisoning, serotonin syndrome), endocrine (diabetic ketoacidosis, thyroid storm), metabolic (electrolyte derangement, renal or liver failure), infectious (sepsis), other (trauma, burns, dehydration, shock, hypo- and hyperthermia).
Early detection and immediate control of agitation allows to avoid symptomatic escalation and appearance of aggression. A noncoercive strategy, implemented by noninvasive therapy that provides rapid resolution of agitation symptoms, is thought to be optimal. Coercive methods, such as physical restraint and isolation, require prolonged hospitalization, often costly and traumatic for the patient.
Verbal techniques to de-escalate agitation are primary. Threats and condescending remarks should be avoided, and external stimuli should be reduced (get rid of loud noises, muffle sound, eliminate the presence of large numbers of medical personnel). If they do not help (the patient is disoriented or in an aggressive, violent state), pharmacotherapeutic approaches are used, including administration of benzodiazepines (lorazepam, midazolam), first-generation (haloperidol, droperidol, fluphenazine, loxapine) or second-generation (aripiprazole, olanzapine, risperidone, ziprasidone) antipsychotics, ketamine.
Treatment of acute agitation with the above drugs is not without problems. For example, benzodiazepines can cause respiratory depression, excessive drowsiness, and paradoxical disinhibition. Neuroleptics have the undesirable effects of prolonging the QTc interval with the potential for cardiac arrhythmias including bidirectional ventricular tachycardia (torsades de pointes), tremor, neutropenia, and extrapyramidal motor disturbances. Since the drugs are usually administered intravenously or intramuscularly, this method of administration may be perceived by the patient as a form of attack. Therefore, oral formulations are preferred and are not available for all of the aforementioned medications.
Igalmi: Mechanism of Action of Dexmedetomidine
Igalmi is dexmedetomidine in a proprietary film sublingual formulation (codename BXCL501).
Film administration of dexmedetomidine, which completely dissolves in the sublingual or buccal area, bypasses first-pass metabolism resulting in more rapid and higher bioavailability than ingested formulations.
Dexmedetomidine, being a highly selective full agonist of all three α2-adrenoreceptor types, provides a sedative effect by reducing the activity of noradrenergic neurons in the brainstem’s locus coeruleus (nucleus with predominance of noradrenergic neurons), thereby increasing the activity of GABAergic inhibitory neurons in the ventrolateral preoptic nucleus. Other sedative drugs like benzodiazepines directly increase the activity of the latter.
Sedation with dexmedetomidine mimics natural sleep and is characterized by reduced amnesia side effects. Dexmedetomidine causes almost no respiratory depression. Because all three types of α2-adrenoreceptor (α2A, α2B, α2C) are associated with stress-related sympathetic and glutamatergic activity, dexmedetomidine is likely superior to other drugs in this class.
Pfizer’s injectable dexmedetomidine made its debut in December 1999, when the FDA approved it under the brand name Precedex for sedation of intubated and ventilated patients. Later, Precedex was approved for sedation of non-intubated patients prior to and/or during surgical and other procedures (e.g., colonoscopy).
Igalmi: Clinical Efficacy of Sublingual Dexmedetomidine in Agitation Management
Igalmi’s filing included results from two SERENITY phase 3 clinical trials (randomized, double-blind, placebo-controlled, multicenter) among adult patients with acute agitation.
A clinical diagnosis of agitation was made when a total score of ≥ 14 on the Positive and Negative Syndrome Scale (PANSS) was obtained by adding the Excited Component (PEC) such as poor impulse control, tension, hostility, uncooperativeness, and excitement, with at least one of these items having a score of ≥ 4.
Subjects were given sublingual dexmedetomidine at a dose of 120 mcg or 180 mcg or placebo.
The primary endpoint was the absolute change in the baseline PEC total score after 2 hours. The secondary endpoint was stated to be the earliest time at which the therapeutic effect of Igalmi on agitation became evident by the change in baseline PEC total score compared to placebo.

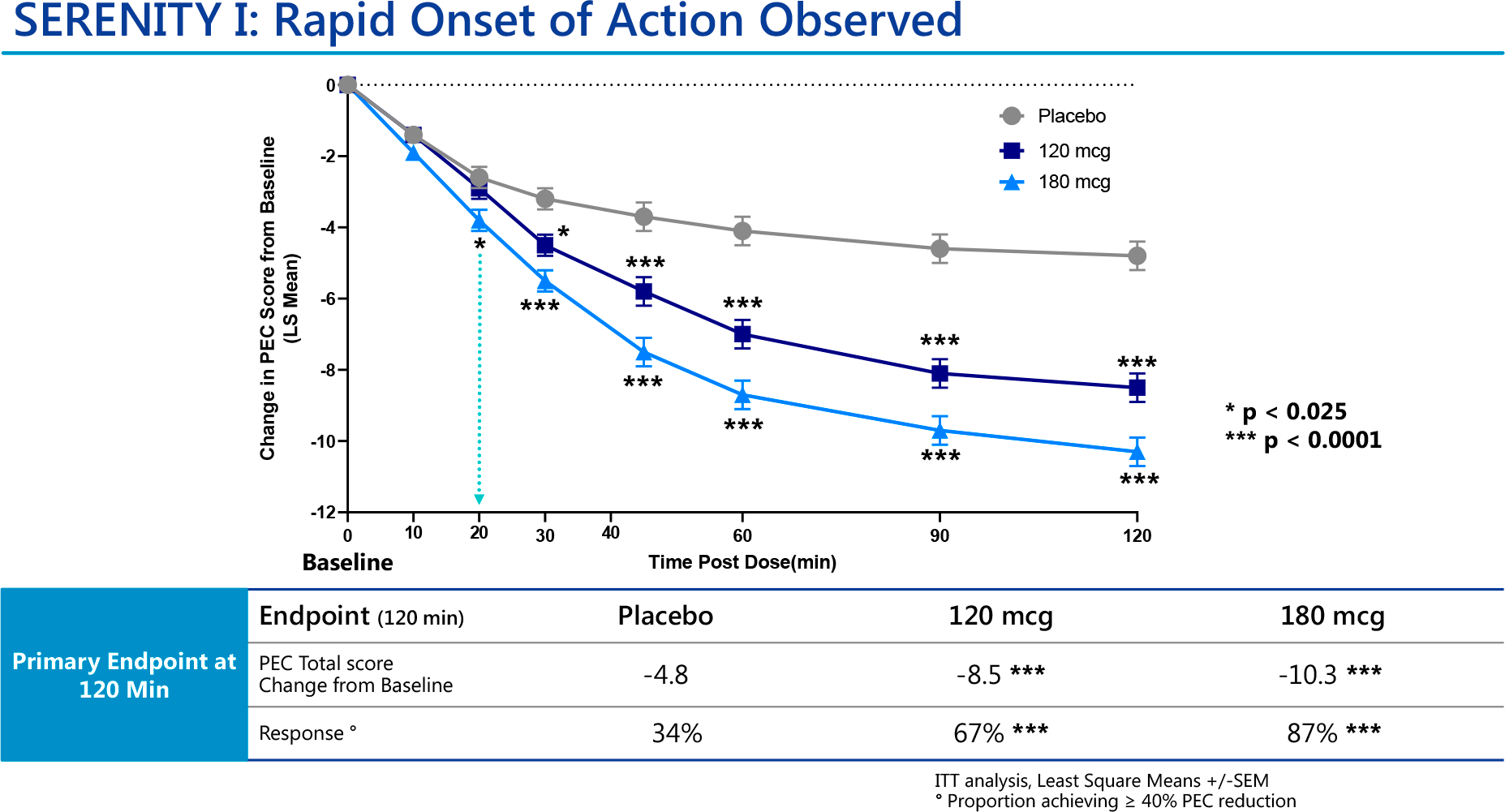
The SERENITY I clinical trial (NCT04268303) involved patients (n=380) with acute agitation due to schizophrenia, schizoaffective disorder, or schizophreniform disorder.
The low-dose and high-dose Igalmi cohort demonstrated statistically significant decreases in PEC total scores of 8.5 and 10.3 points — versus a decrease of 4.8 points in the placebo group (p<0.0001).
To treatment-response status (minimum 40% reduction in PEC total score after 2 hours), went 67% and 87% of participants — vs. 34% in the control group (p<0.0001).
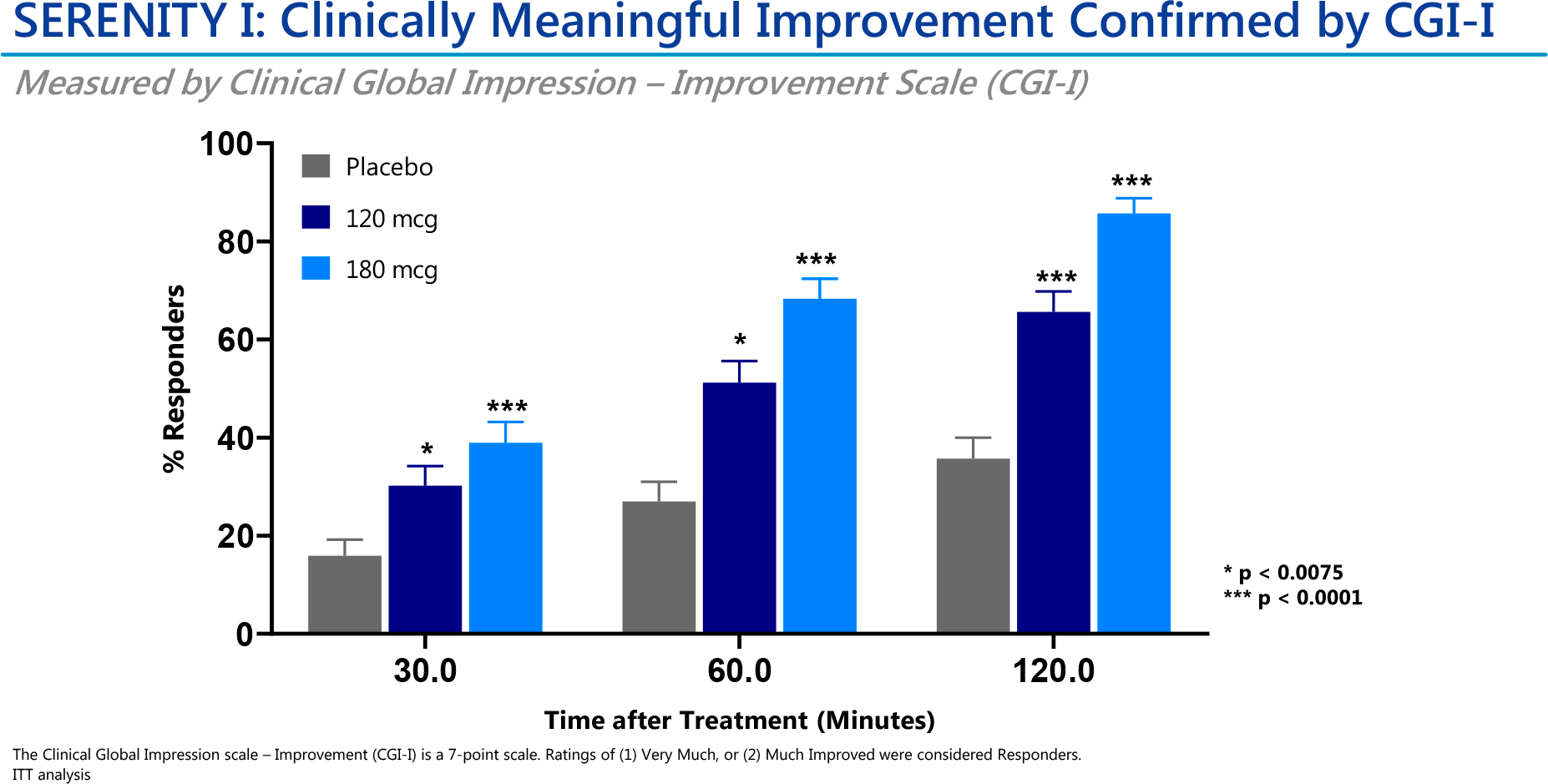
A clear beneficial therapeutic effect of sublingual dexmedetomidine, according to Clinical Global Impression — Improvement scale (CGI-I), was seen after 30 minutes in the low- and high-dose experimental drug cohort (p<0.0075 and p<0.0001).
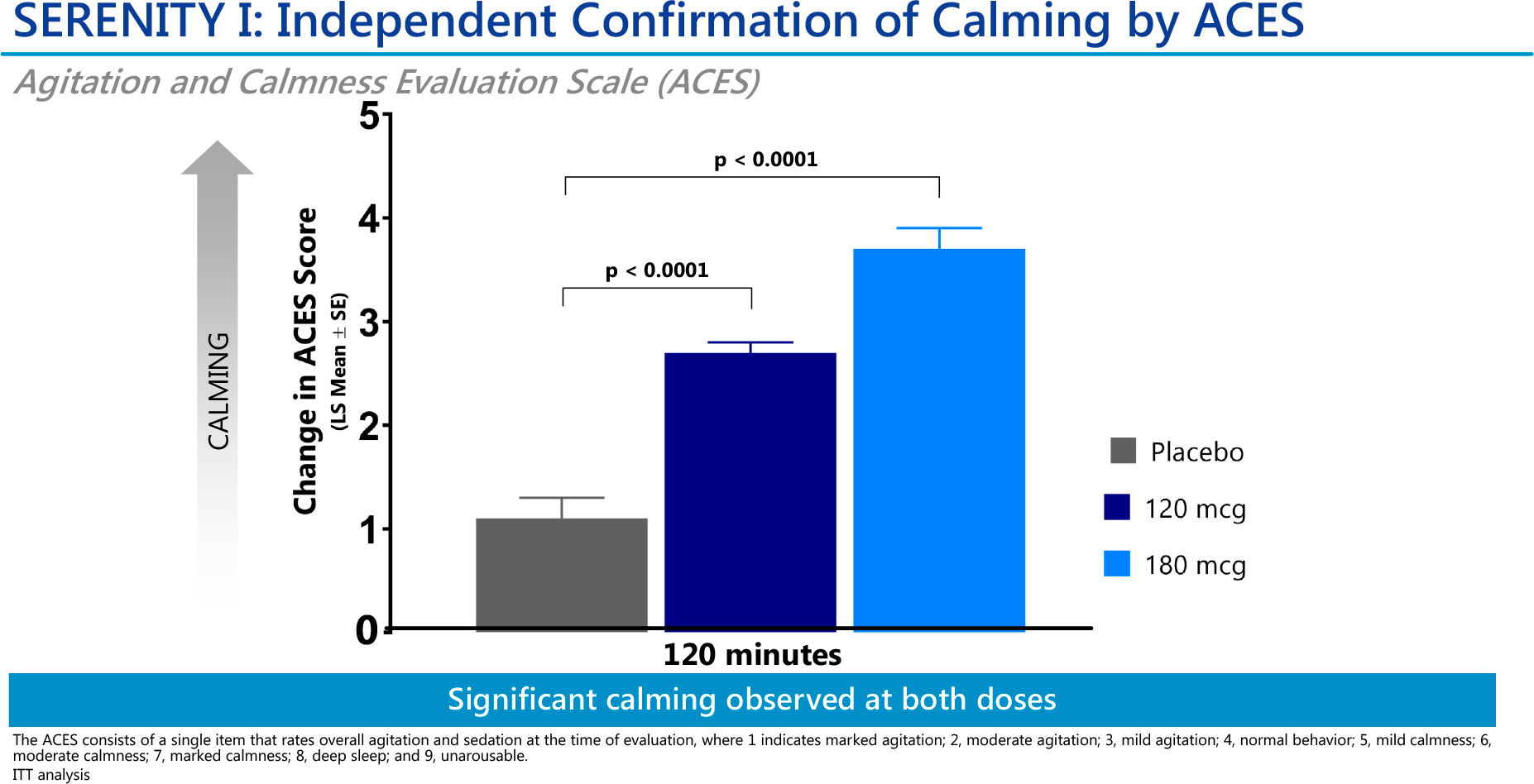
Both doses of Igalmi scored statistically significant changes on the Agitation and Calmness Evaluation Scale (ACES) after 2 hours (p<0.0001).
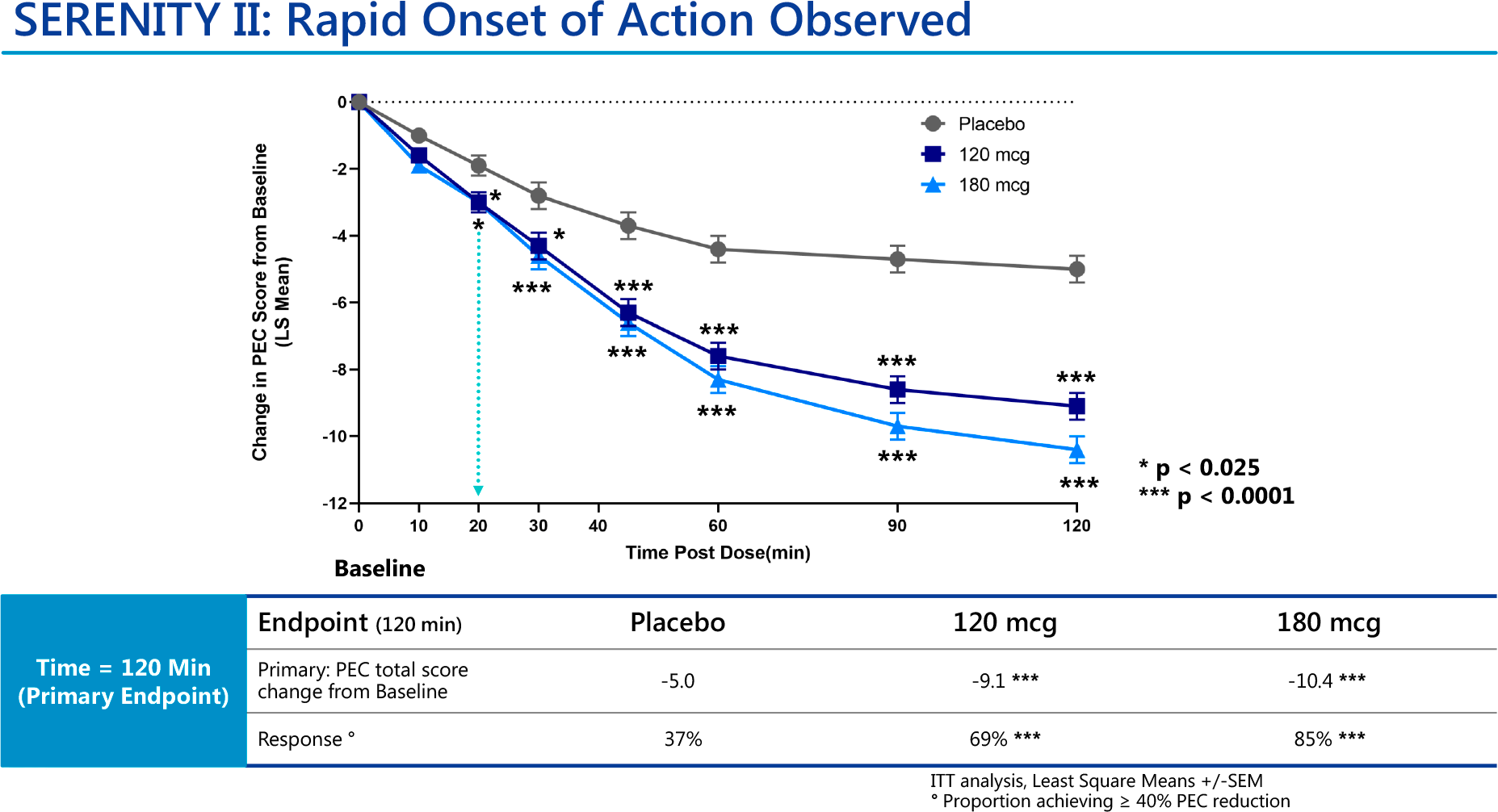
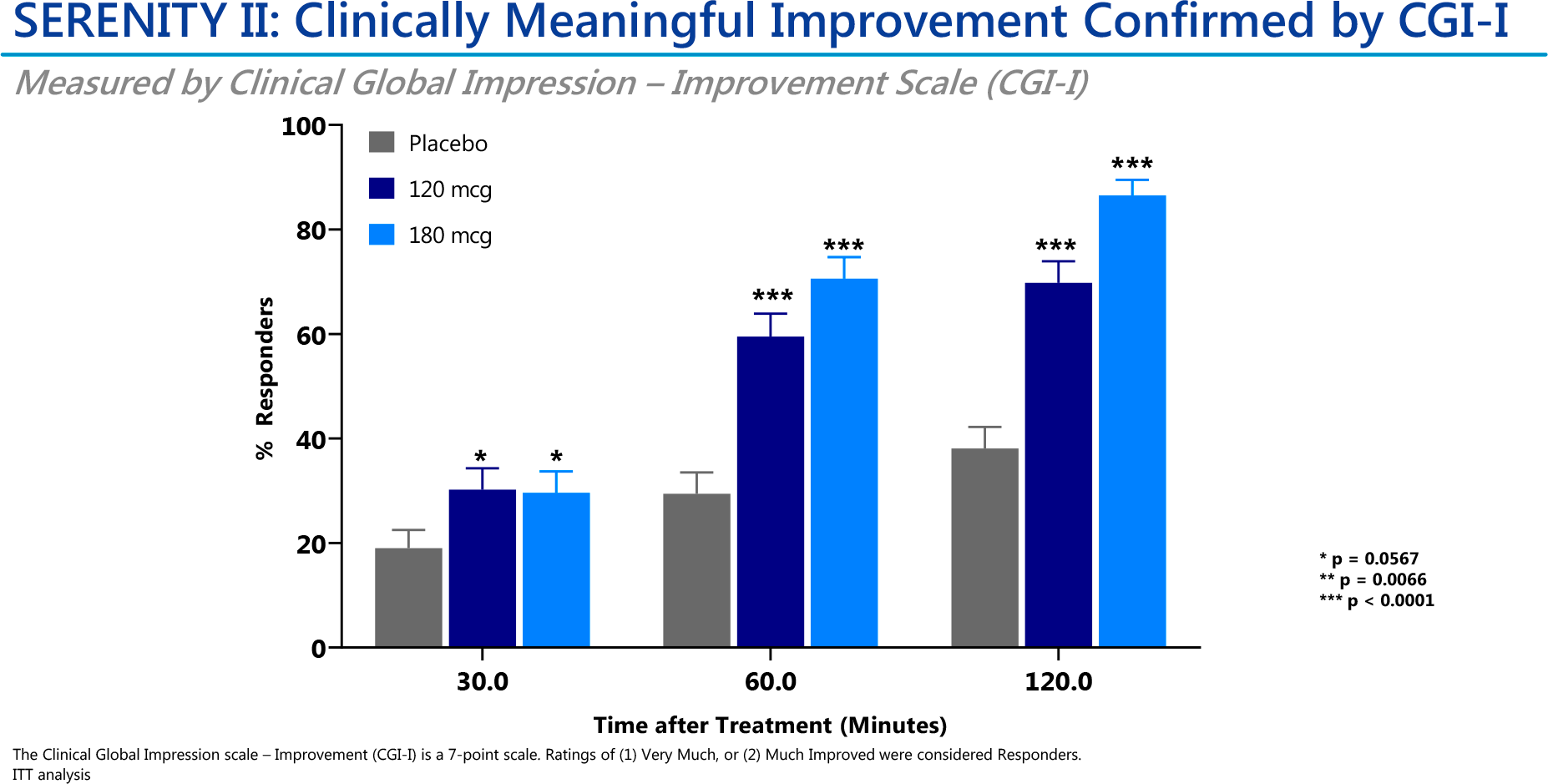
The SERENITY II clinical trial (NCT04276883) included patients (n=378) with acute agitation due to bipolar disorder type I or II (with hypomanic, manic, or mixed episodes).
Administration of Igalmi at low or high dose resulted in statistically significant reductions of 9.1 and 10.4 points in the PEC total score — versus a decrease of 5.0 points in the placebo group (p<0.0001).
Respondent status was recorded for 69% and 85% of subjects — vs. 37% in the control group (p<0.0001).
Positive effects of sublingual dexmedetomidine on the CGI-I scale were demonstrated after 60 minutes after administration — in the two dose cohorts (p<0.0001).
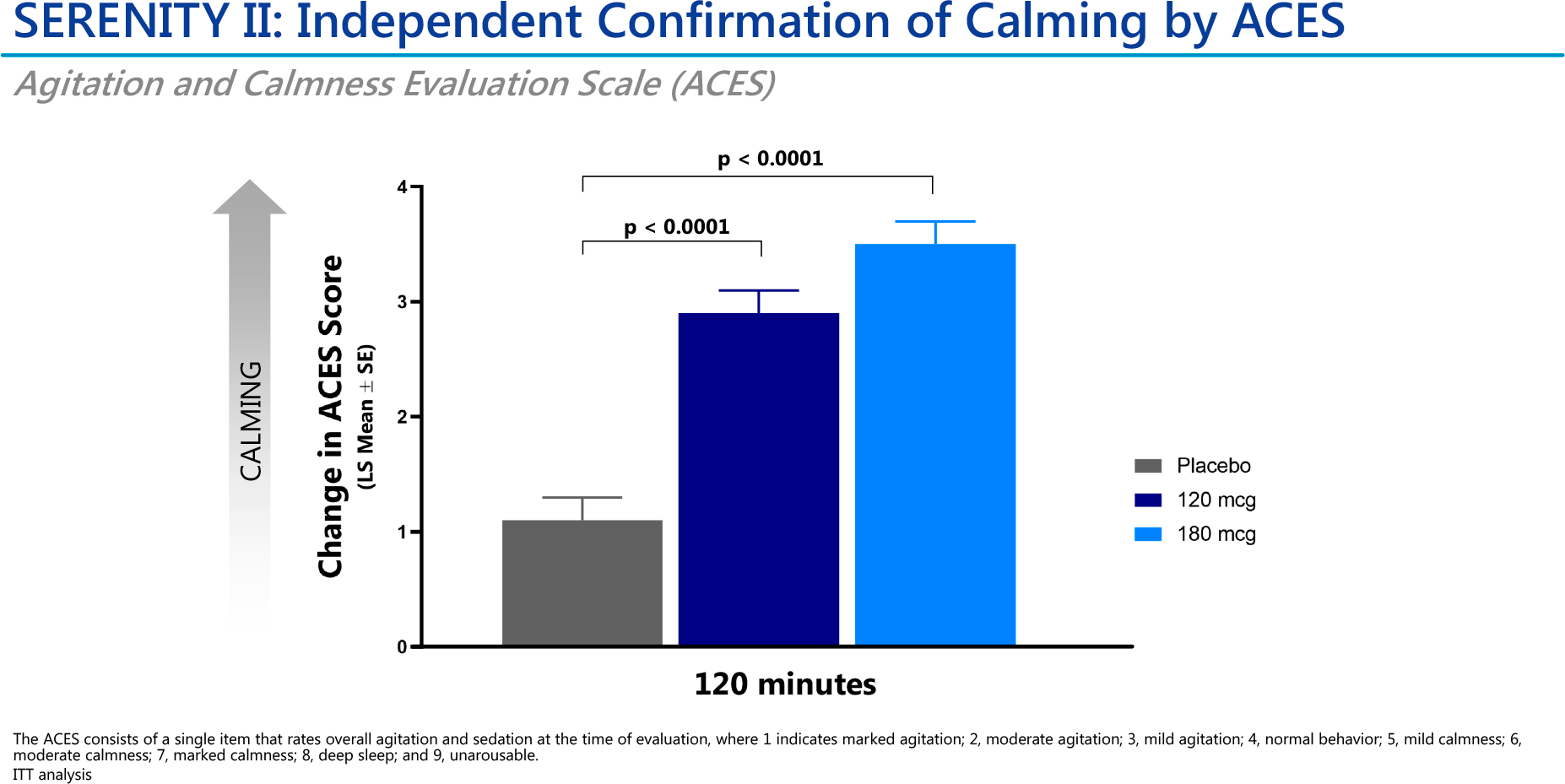
Both Igalmi doses showed statistically significant changes on the ACES scale after 2 hours (p<0.0001).
Igalmi: Safety of Agitation Management With Sublingual Dexmedetomidine
The safety profile of Igalmi was characterized by acceptable tolerance of the drug.
The most common adverse reactions included: somnolence (in 23% and 22% of patients in the high and low dose dexmedetomidine cohorts), oral paresthesia or hypoesthesia (7% and 6%), dizziness (6% and 4%), hypotension (5% and 5%), orthostatic hypotension (5% and 3%), dry mouth (4% and 7%), nausea (3% and 2%), bradycardia (2% and 2%), and abdominal discomfort (2% and 0%). All adverse effects were mild to moderate in severity.
The prescribing information for Igalmi contains warnings about the risks of hypotension, orthostatic hypotension and bradycardia, QT interval prolongation, and somnolence.
Igalmi: What’s Next
Because Igalmi’s mechanism of action is independent of the underlying neuropsychiatric disorder, BioXcel is conducting a parallel clinical testing of a sublingual formulation of dexmedetomidine in the therapy of agitation in Alzheimer’s disease and as a adjunctive treatment for major depressive disorder (clinical depression).
The TRANQUILITY (NCT04251910) phase 1b/2 clinical trial, which evaluated Igalmi in the treatment of agitation in dementia, including Alzheimer’s type, confirmed the therapeutic efficacy of the drug. Two pivotal TRANQUILITY II and TRANQUILITY III phase 3 clinical trials have been initiated.
It is possible that Igalmi will also find use in other conditions with psychiatric hyperactivity such as post-traumatic stress disorder (PTSD), traumatic brain injury (TBI), alcohol withdrawal syndrome (AWS), opioid withdrawal, delirium, and phobias.
Extras
Igalmi (dexmedetomidine). Prescribing information. U.S. [PDF]
Igalmi (dexmedetomidine). Approval presentation. BioXcel Therapeutics, April 6, 2022. [PDF]
Effect of sublingual dexmedetomidine vs placebo on acute agitation associated with bipolar disorder: A randomized clinical trial. JAMA. 2022 Feb 22;327(8):727-736. [source]
Pharmacokinetics of dexmedetomidine after a single sublingual dose of BXCL501 in patients with agitation associated with schizophrenia. 2021 International Society for Bipolar Disorders (ISBD). [PDF]
Effect of BXCL501 for treating acute agitation in patients with bipolar disorder. 2021 International Society for Bipolar Disorders (ISBD). [PDF]
Safety and patient acceptability of BXCL501 for treating acute agitation in patients with bipolar disorder. 2021 International Society for Bipolar Disorders (ISBD). [PDF]
Translational research with dexmedetomidine (dm) for the treatment of agitation from healthy volunteers to two patient groups: those with schizophrenia or with probable senile dementia of the Alzheimer’s type (SDAT). 2019 Annual Meeting of American College of Neuropsychopharmacology (ACNP). [PDF]
Double-blind, placebo-controlled, single ascending dose study to determine the efficacy, safety, and pharmacokinetics of BXCL501 (sublingual dexmedetomidine) in agitation associated with schizophrenia or related disorders. 2019 Annual Meeting of American College of Neuropsychopharmacology (ACNP). [PDF]
Dexmedetomidine — highly favorable pharmacokinetic and pharmacological features for a CNS therapeutic drug. BXCL501: a therapy for improved adaptation to stress. 2019 Annual Meeting of American College of Neuropsychopharmacology (ACNP). [PDF]