Highlights
Xocova (ensitrelvir) is a new drug indicated for the treatment of COVID-19 infection caused by the SARS-CoV-2 coronavirus.
Xocova, which is suitable for the treatment of adults and children (12 years and older), should be prescribed if no more than 72 hours have elapsed since the onset of symptoms. Otherwise, the effectiveness of this antiviral drug will not be as high.
Xocova, developed by Japan’s Shionogi & Co., is approved in Japan in late November 2022.
Xocova works in the same way as the extremely popular antiviral drug Paxlovid (nirmatrelvir + ritonavir) by Pfizer. The mechanism of action of ensitrelvir is similar to that of nirmatrelvir: it inhibits viral replication.
There are two main differences between Xocova and Paxlovid. First, Xocova can be used to treat any patient with mild-to-moderate COVID-19 severity, the use of Paxlovid is limited to those who are at risk of progression to severe infection, followed by hospitalization or death.
Second, both oral medications are prescribed as a 5-day course, but while Paxlovid needs to be taken twice daily (along with the bioavailability enhancer ritonavir), Xocova is only once daily (and without ritonavir). Xocova is used in a loading dose (three 125-mg tablets) on the first day, and one 125-mg tablet on subsequent days.
In addition to the obvious convenience of use, the absence of the need for ritonavir removes a number of issues related to drug interactions, when treatment with Paxlovid obliged to temporarily discontinue a number of other medications. However, some drugs still cannot be taken together with Xocova due to the fact that ensitrelvir has a strong inhibitory effect on cytochromes of the CYP3A family.
It remains to be seen definitively whether the efficacy of Xocova is as good as that of Paxlovid, which reduces the risk of hospitalization or death from COVID-19 by almost 90%.
Xocova, like Paxlovid, is effective against SARS-CoV-2, regardless of its mutations. At any rate, these antivirals are effective in treating COVID-19 caused by the Omicron variant that has spread across the planet, including its BA.4 and BA.5 subvariants, as well as BA.5 subvariants gaining strength, such as BQ.1 (nicknamed Typhon) and BQ.1.1 (nicknamed Cerberus).
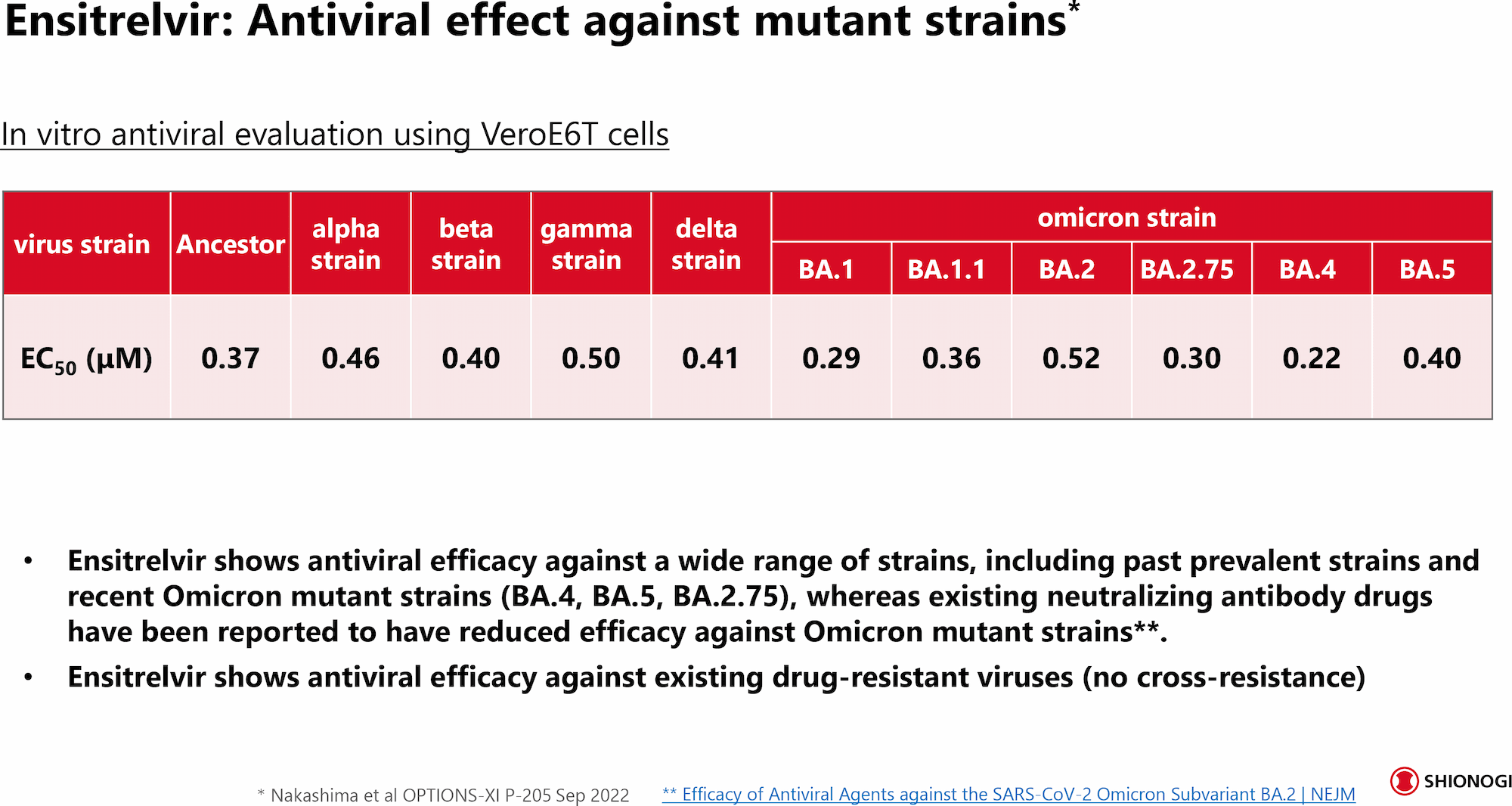
- Ensitrelvir is claimed to successfully counteract Omicron subvariants BA.4/BA.5 and BA.2.75 with the same high antiviral activity as in the case of other coronavirus variants. At any rate, this follows from the in vitro testing.
The need for new medications to control COVID-19 is still high, and there are a number of good reasons for this. First, treating at home reduces the burden on already overheated health care systems.
Second, the oral route of administration is convenient for the patient, and the pills themselves are easier and cheaper to make than injectable medications.
Third, the drugs will help those who oppose vaccination or cannot be vaccinated for medical reasons.
Fourth, the wider the drug arsenal, the lower the risk of virus mutations with subsequent development of resistance to therapy.
Fifth, new antivirals spur price competition and somehow solve the issue of unmet demand for such drugs due to insufficient production.
In addition, we should not forget the serious problem of long COVID (post-COVID-19 syndrome), which is understood to be a state of long-term health problems that persists after a typical period of recovery from COVID-19.
The use of antivirals, in particular Paxlovid, is thought to significantly reduce the risk of developing long COVID, which affects one in four to five people who have had a symptomatic infection, and more often young people.
The price of Xocova has not yet been determined, but Shionogi & Co. suggest that the cost of ensitrelvir for government procurement will be set at world-class levels (read, competitive with other oral COVID-19 drugs). However, for low- and middle-income countries, the price of Xocova will be only slightly higher than for flu medications.
- For reference: Pfizer has set out three levels of cost for a course of COVID-19 treatment with Paxlovid, which depend on the income level of countries — high, middle, or low. For example, the price of Paxlovid for U.S. patients is $530. For low-income countries, Paxlovid is given at cost. Roche together with Shionogi & Co. promotes Xofluza (baloxavir marboxil), which is enough to take in single dose to treat or prevent influenza and which price in the US is $170.

Paxlovid for COVID-19 Treatment. All Details
Treatment efficacy, “Paxlovid mouth,” COVID-19 rebound, management of Omicron variant, treatment resistance, generics, mechanism of action, price.
Long Road
Regulatory approval of ensitrelvir took a long time for Shionogi & Co. The Japanese manufacturer was going to launch the drug on the local market in March. But it didn’t work out: Even with the COVID-19 pandemic, the regulator did not make concessions, not agreeing to approve the drug on the basis of limited clinical data. They had to wait for the accumulation of additional data to confirm the safety and efficacy of Xocova.
In a number of other countries neighboring Japan, Xocova should appear without much delay. For example, in mid-September 2022, Shionogi & Co. agreed with Ildong Pharmaceutical to launch ensitrelvir in South Korea.
The international launch of Xocova will not take place until the second half of 2023.
In early October 2022, Shionogi & Co. signed an agreement with the Medicines Patent Pool (MPP) of Unitaid aimed at increasing access to medicines for poor countries. The parties formalized arrangements for the voluntary licensing of ensitrelvir so that its low-cost generic copies would appear in 117 low- and middle-income countries, and Shionogi & Co will not receive any royalties from sales.
In the meantime, Paxlovid has taken an unqualified lead as an effective COVID-19 control drug. In the first nine months of 2022, Pfizer earned $17.1 billion on it. For all of 2022, Paxlovid should put at least $22 billion into the U.S. pharmaceutical giant’s bank account.
Xocova: Efficacy and Safety of COVID-19 Treatment With Ensitrelvir
The SCORPIO-SR (jRCT2031210350) phase 2/3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial enrolled patients with COVID-19 infection that was mild-to-moderate in severity (symptoms must have manifested no later than 5 days before randomization) or asymptomatic.
Participants were given placebo or ensitrelvir (low- or high-dose) once daily for 5 days.
Phase 2a Results
The results of the the phase 2a study among 47 patients demonstrated that the use of ensitrelvir was statistically significantly superior to placebo (unless otherwise noted) in the following respects:
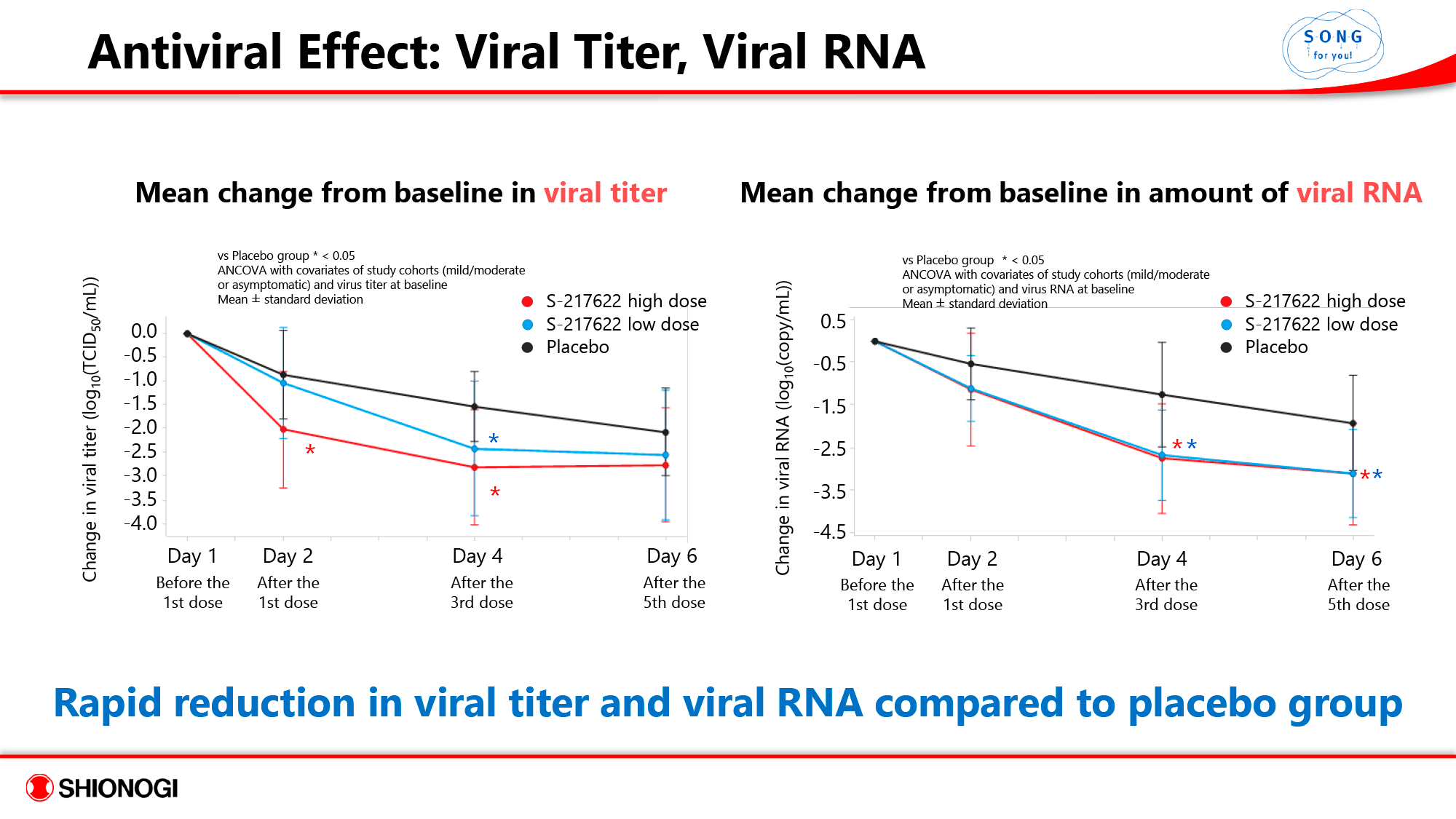
- A more rapid decline in viral titer and viral RNA.
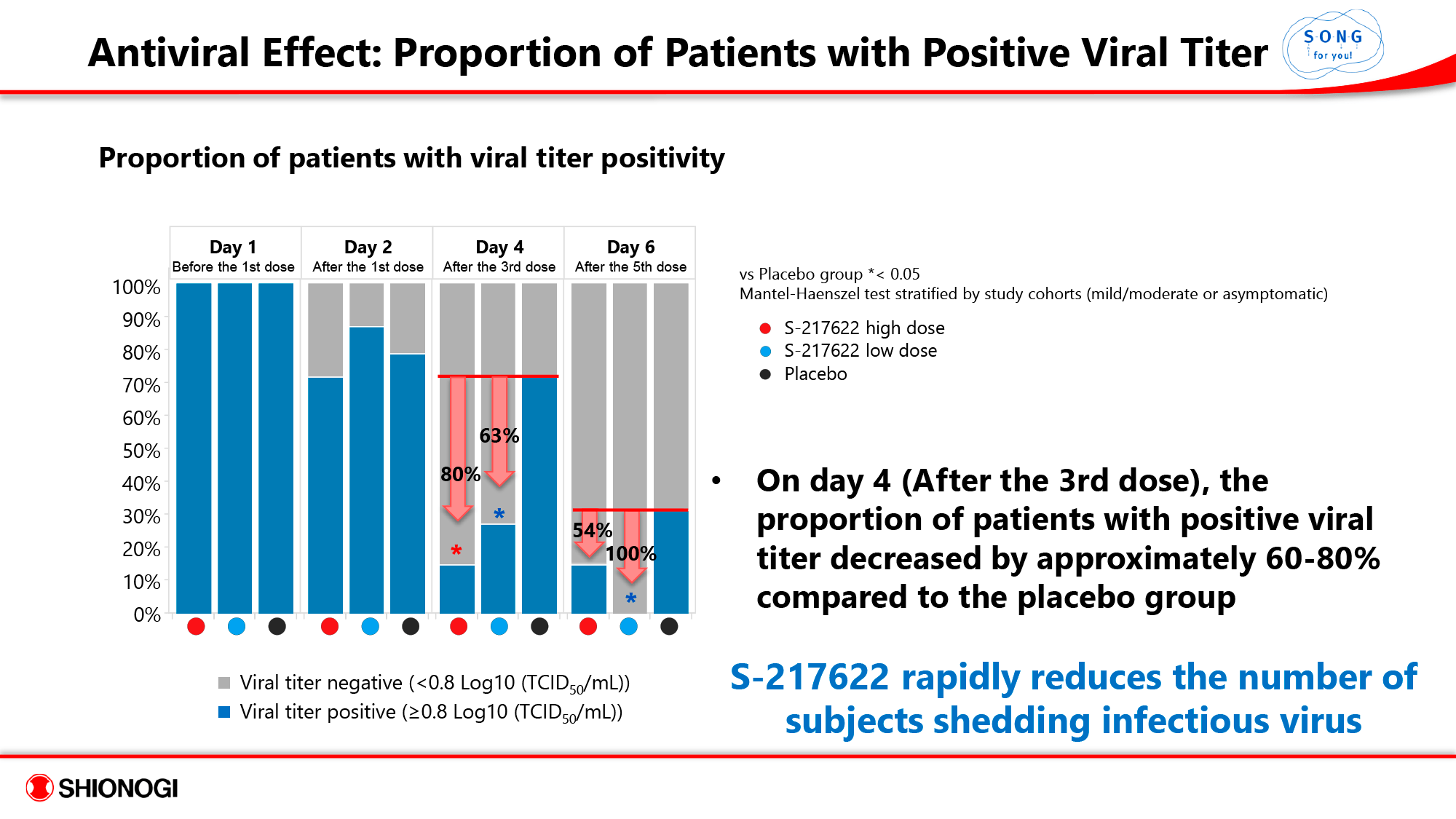
- On day 4 (after the 3rd dose), the proportion of patients with a positive viral titer decreased by 60%–80% compared to the placebo group, meaning Xocova quickly spared patients from the viral shedding status when sick people infect healthy people.
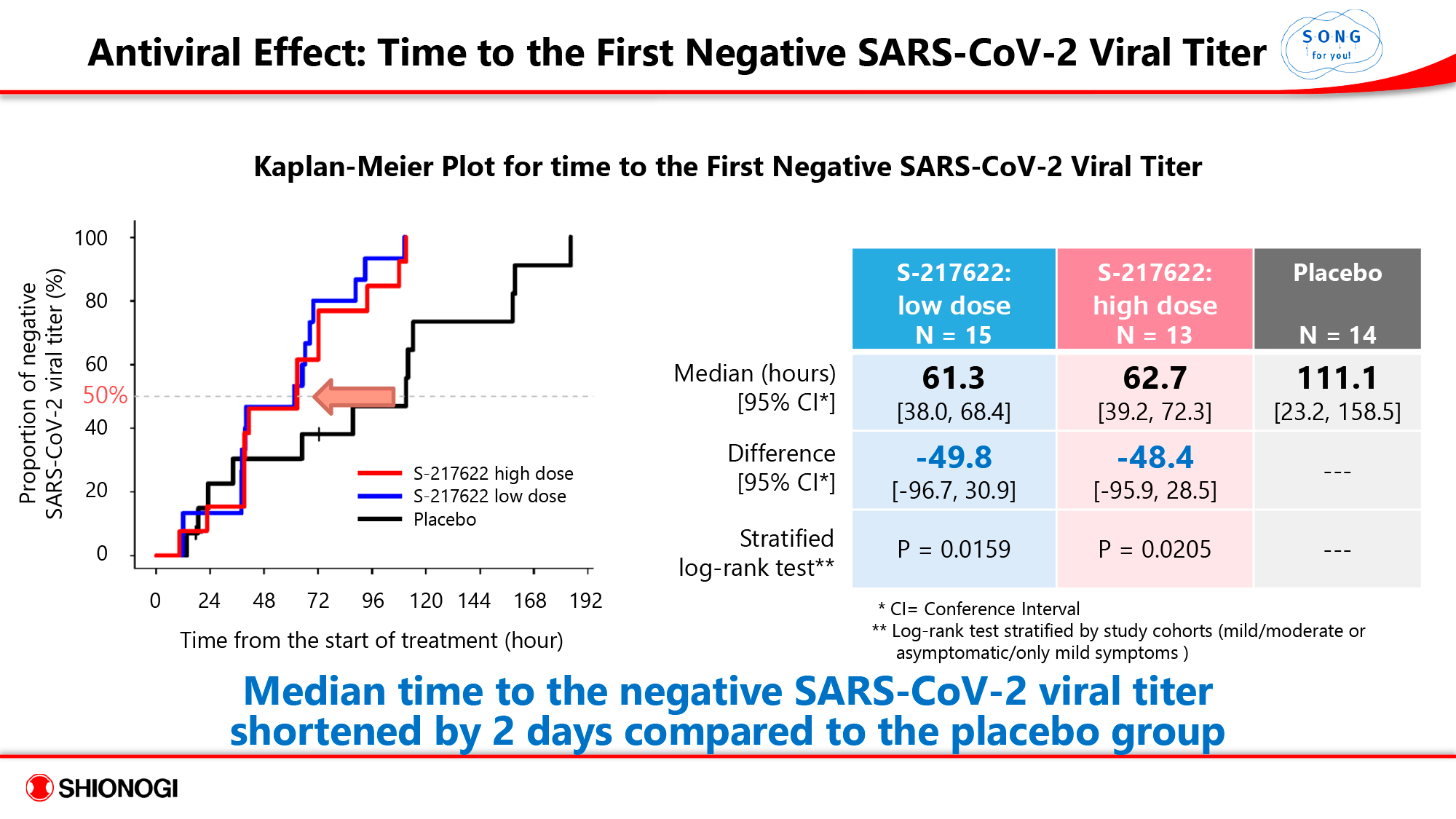
- The median time to negative viral titer was approximately 2.5 days, a reduction of about 2 days compared to the control group.
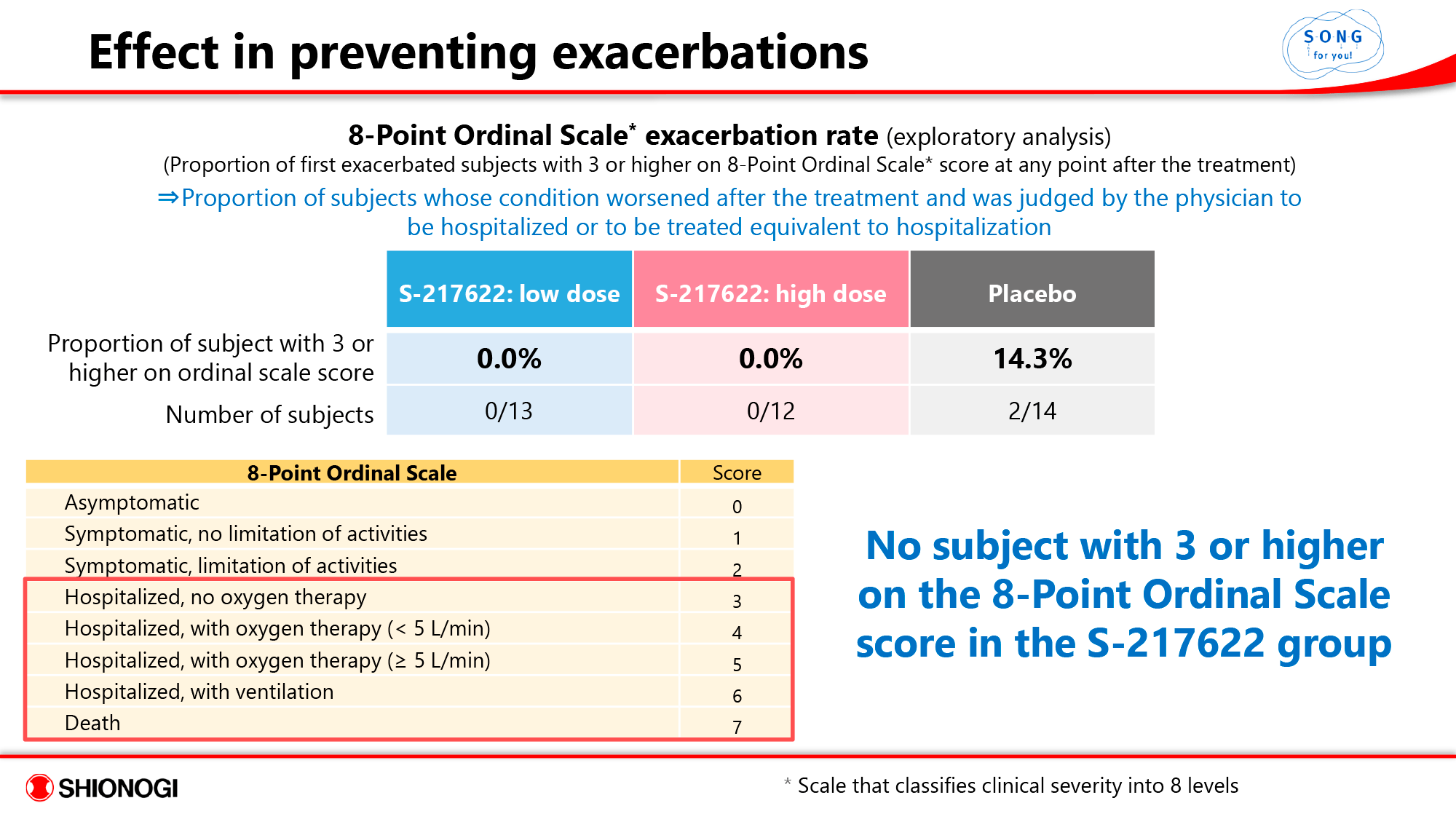
- In the Xocova group, none of the subjects were hospitalized, whereas in the placebo group, 14.3% of patients were hospitalized (or received equivalent treatment).
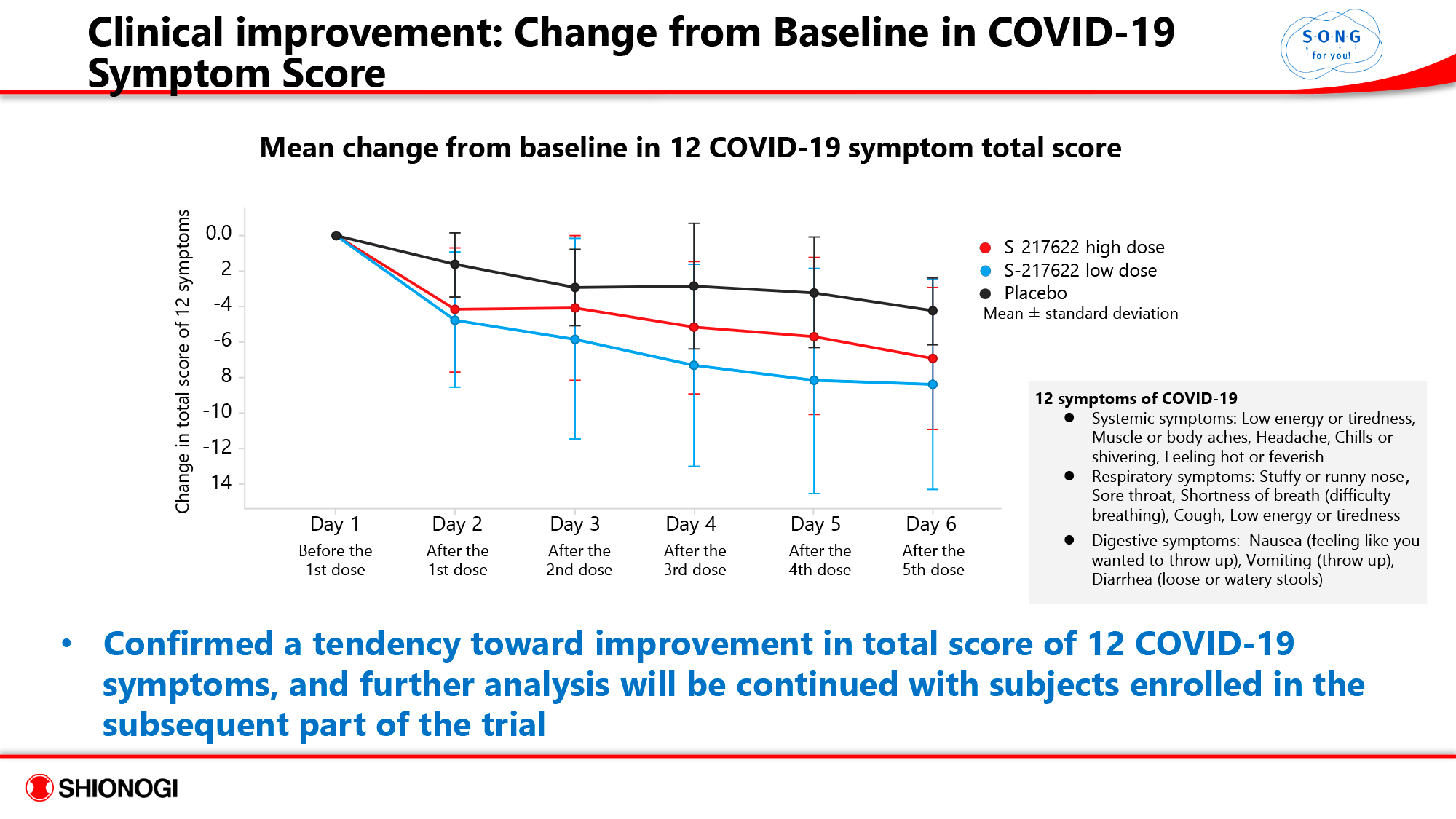
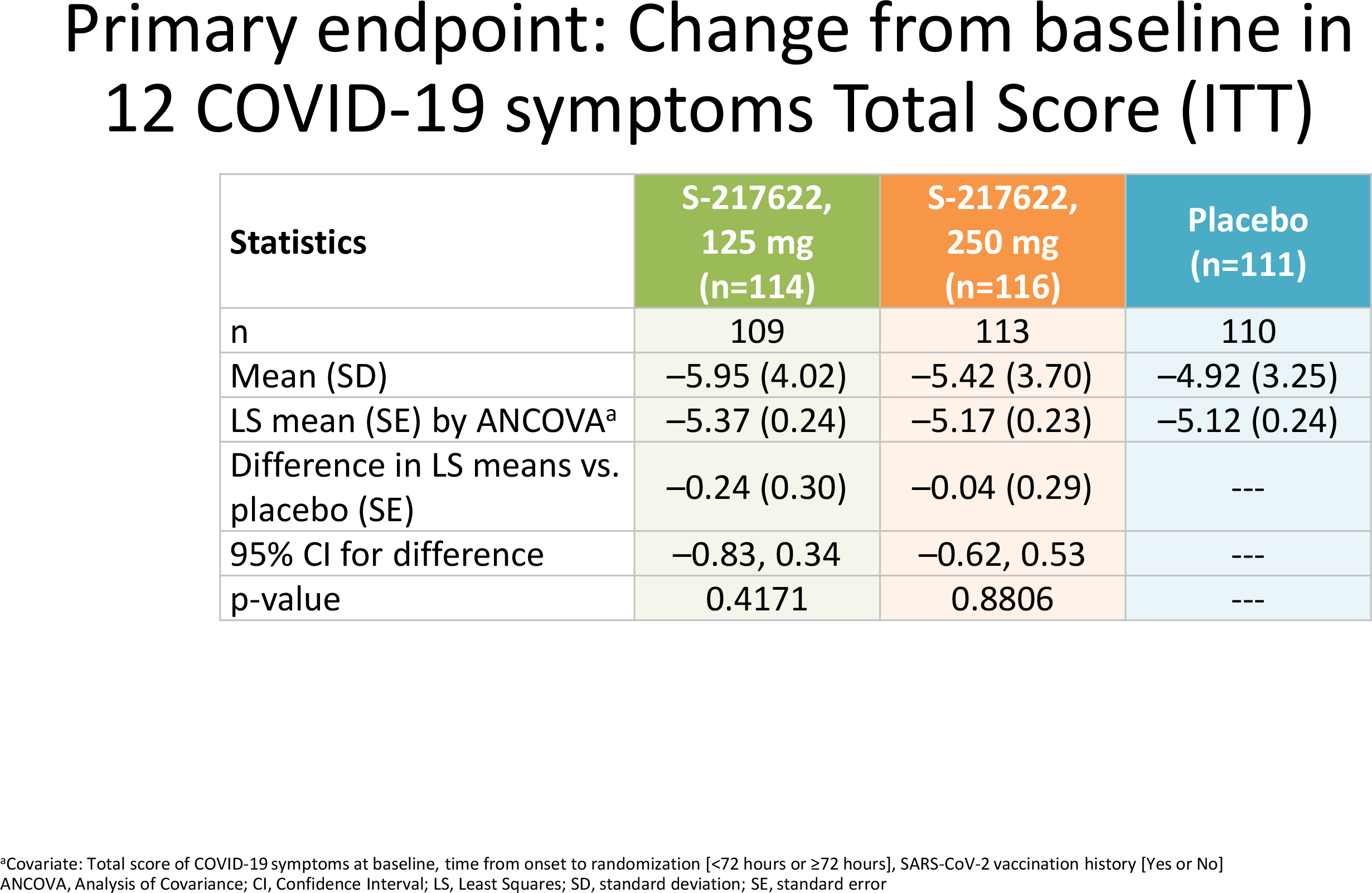
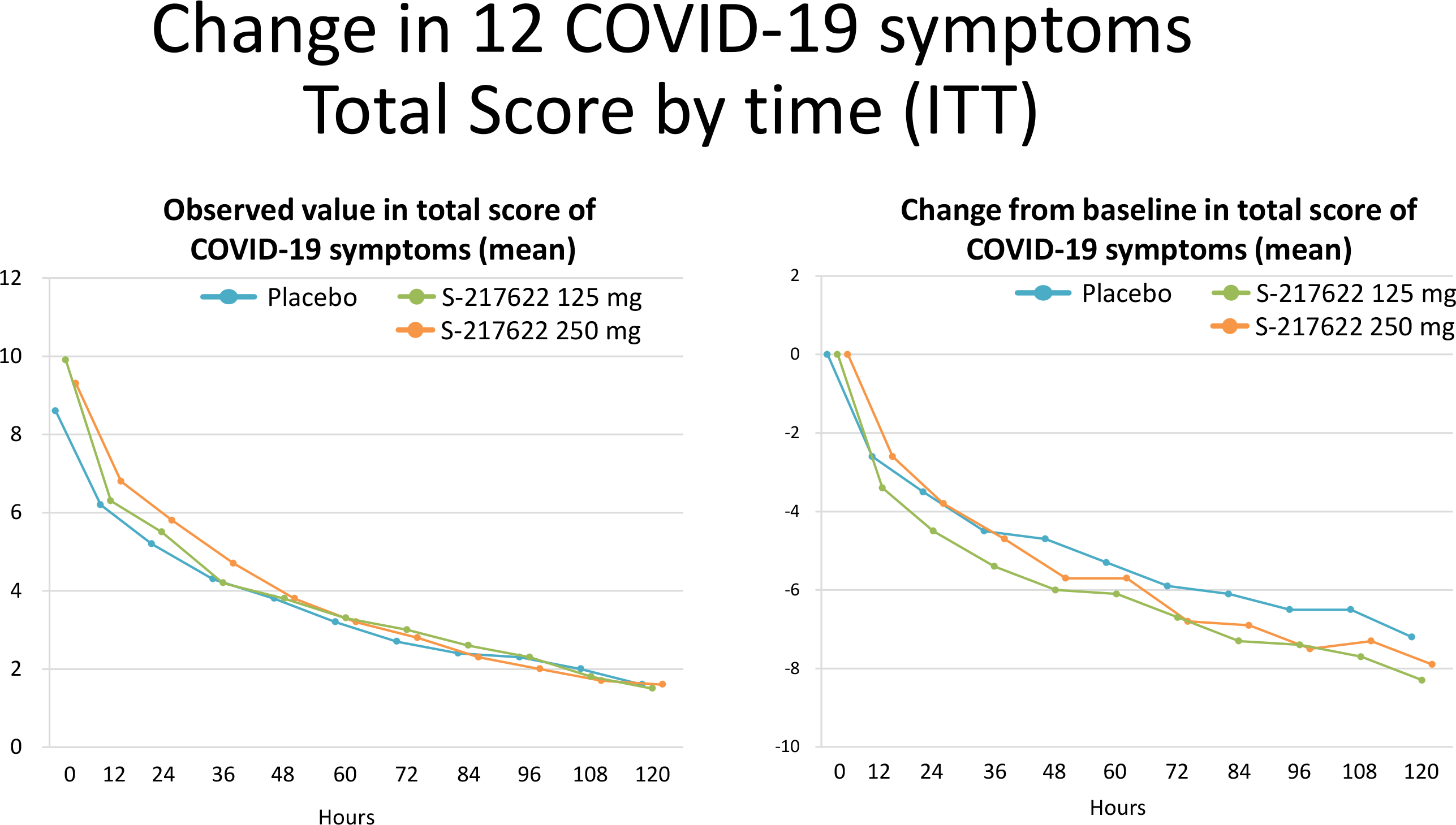
- There was a trend toward an improvement in the overall score on the 12 symptom COVID-19 scale, although no statistically significant difference with placebo was recorded.
The safety profile of ensitrelvir was characterized by acceptable tolerability: none of the patients discontinued treatment.
Among the treatment-emergent adverse events (TEAEs), the most common were the following: nasopharyngitis (in 9.5%, 0%, and 0% of subjects in the high-dose S-217622, low-dose, and placebo group, respectively), headache (4.8%, 13.0%, 0%), rhinalgia (9.5%, 0%, 0%), high-density lipoprotein (HDL) cholesterol decreased (14, 3%, 52.2%, 8.3%), blood triglycerides increased (0%, 13.0%, 0%), aspartate aminotransferase (AST) increased (4.8%, 4.3%, 8.3%), blood bilirubin increased (0%, 8.7%, 0%), alanine aminotransferase (ALT) increased (4.8%, 0%, 8.3%).
Among treatment-related TEAEs, the following were noted: HDL cholesterol decreased (14.3%, 34.8%, 0%), blood triglycerides increased (0%, 8.7%, 0%).
Almost all TEAEs were manifested with a mild degree of severity.
Phase 2b Results
The results of the phase 2b study, which enrolled 428 patients infected primarily with the Omicron variant of the SARS-CoV-2 coronavirus, were generally not different from those collected in the phase 2a study. Ensitrelvir administration resulted in the following beneficial effects:
- A more rapid decline in viral titer and viral RNA.
- On day 4 of treatment, less than 10% of patients had a positive viral titer.
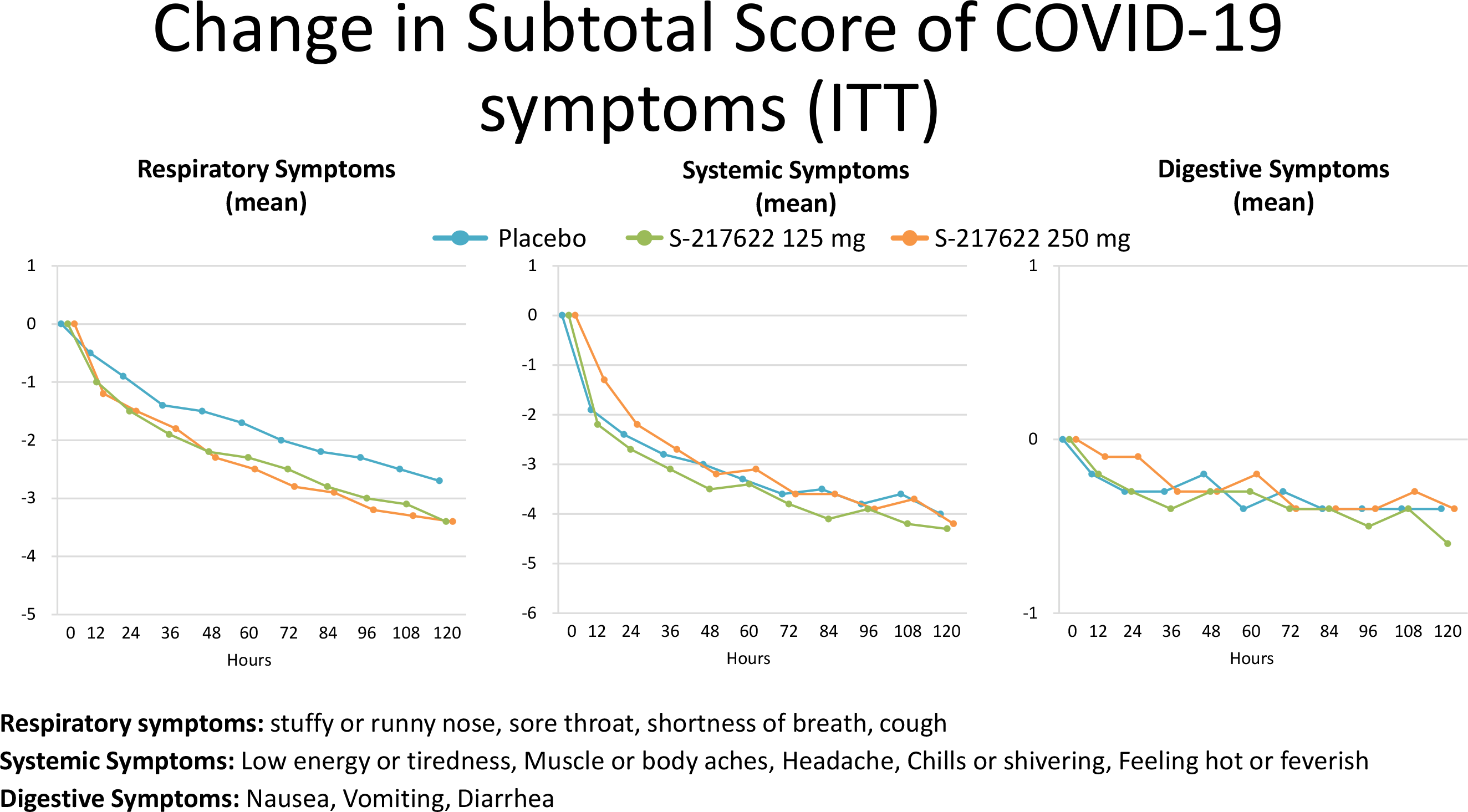
- There was a trend toward improvement in COVID-19 symptoms, according to the time-weighted average change in the total score of 12 COVID-19 symptoms between days 1–6 from the start of treatment, although no statistically significant difference with placebo was noted, but such a difference was registered for respiratory symptoms (stuffy or runny nose, sore throat, cough, shortness of breath).
No new safety concerns have been identified with ensitrelvir.
Update #1
Data from 341 patients treated with either placebo or ensitrelvir at a low dose (375 mg loading dose followed by 125 mg) or high dose (750 mg loading dose followed by 250 mg), have shown the following results from the phase 2b clinical trial
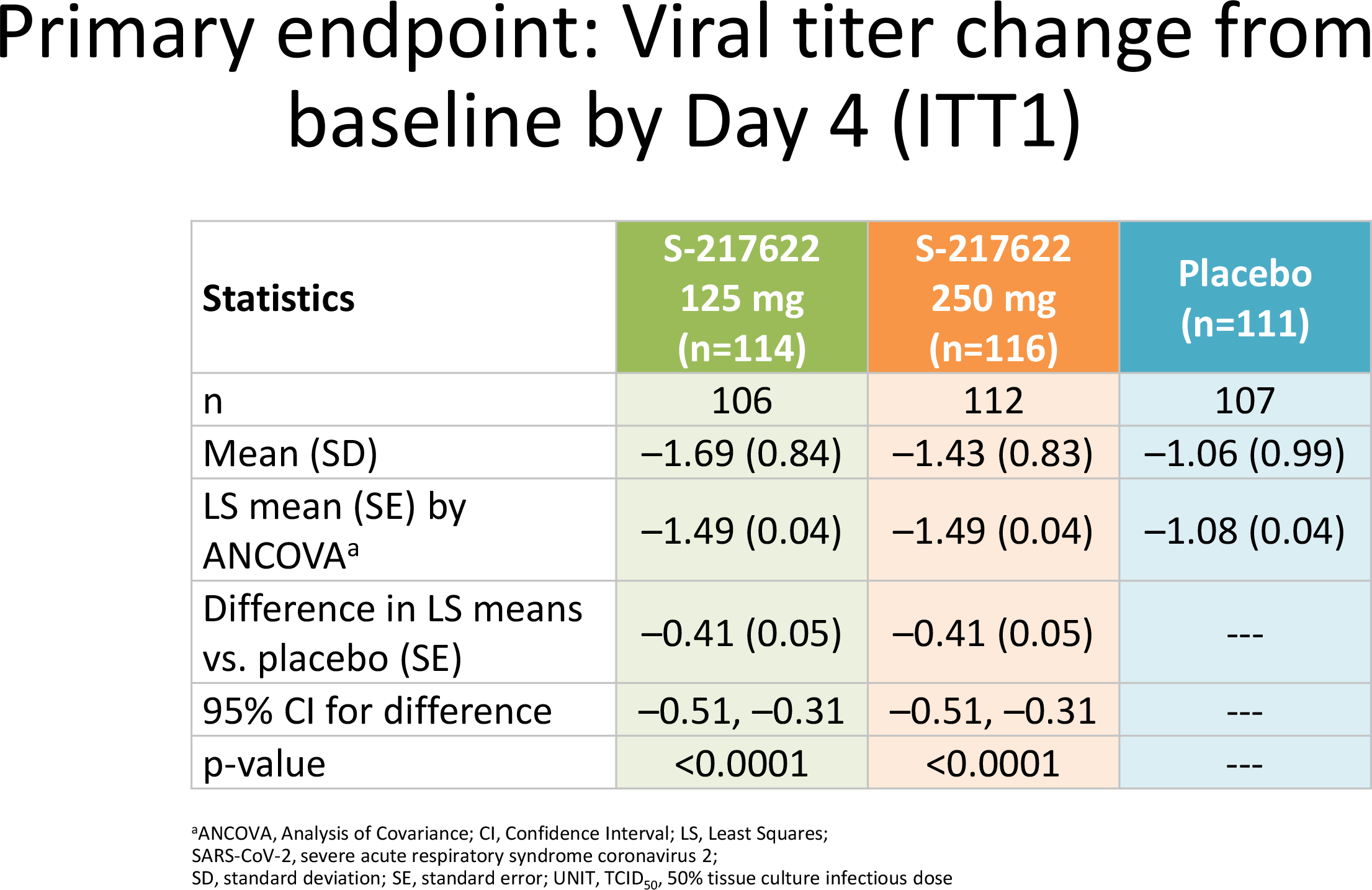
The use of Xocova provided a rapid reduction in viral load. Thus, by day 4 (after the third dose) of therapy the viral titer decreased by a mean of 1.49 log10 TCID50/ml (amount of infectious agent infecting 50% of the cell culture) in the ensitrelvir subgroups — versus a decrease of 1.08 log10 TCID50/ml in the placebo group (p<0.0001). In other words, ensitrelvir compared to placebo accelerated the viral load drop by 2.5 times. Moreover, in the majority of subjects receiving ensitrelvir, the viral titer fell to undetectable values.
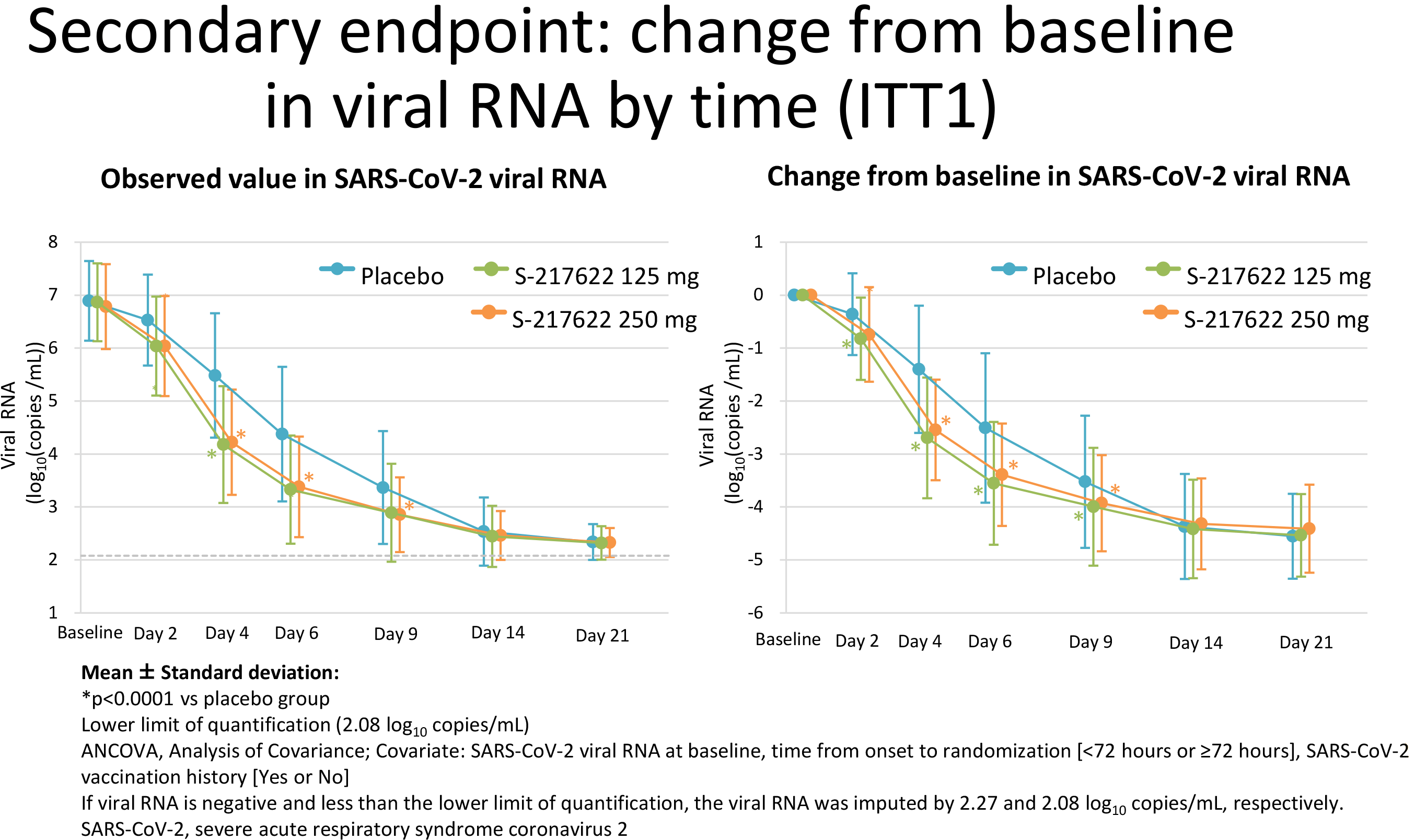
This was also true for the decrease in viral RNA levels (copies/ml): a statistically significant (p<0.0001) difference with the control group was observed by day 4 of treatment.
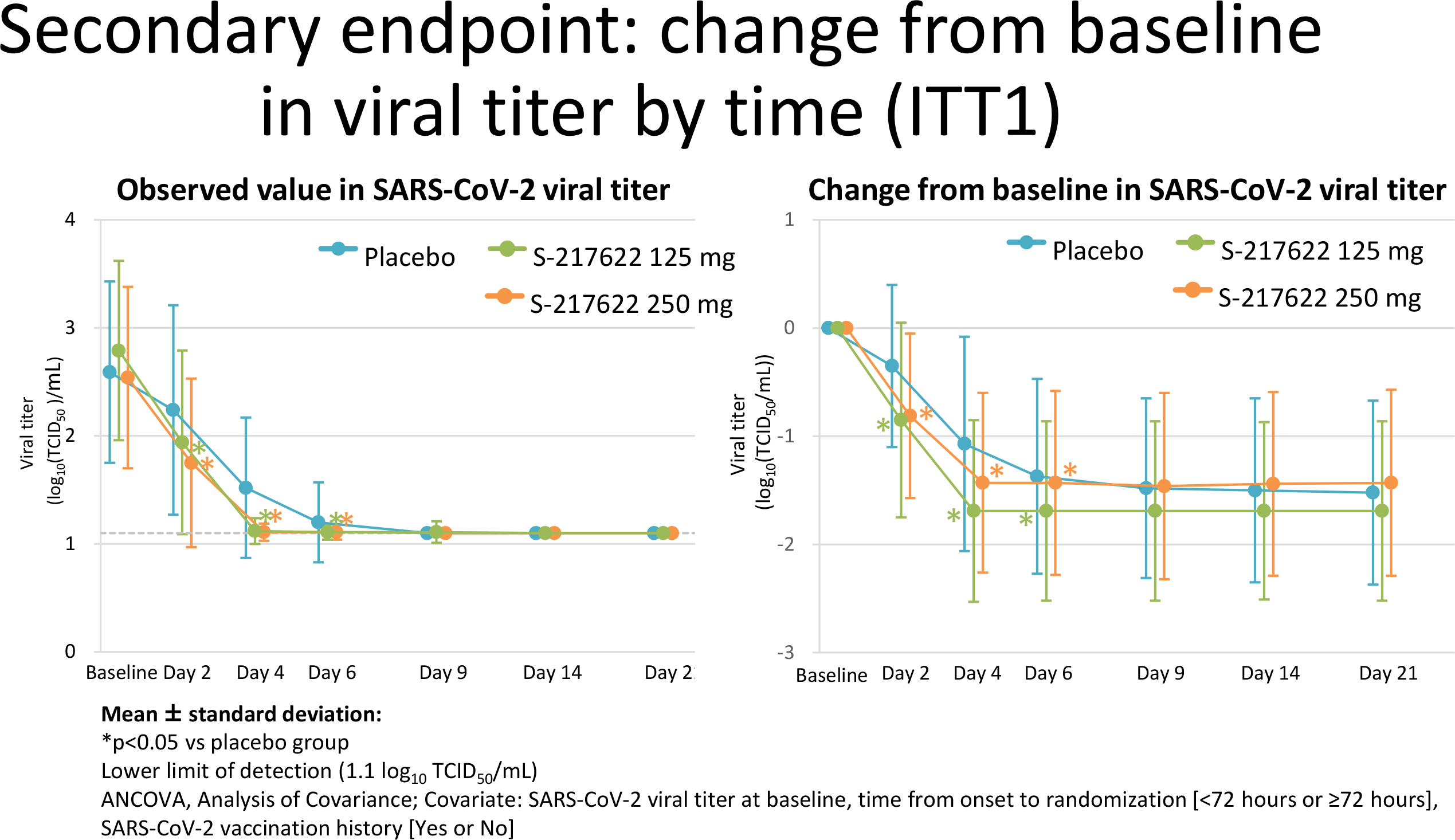
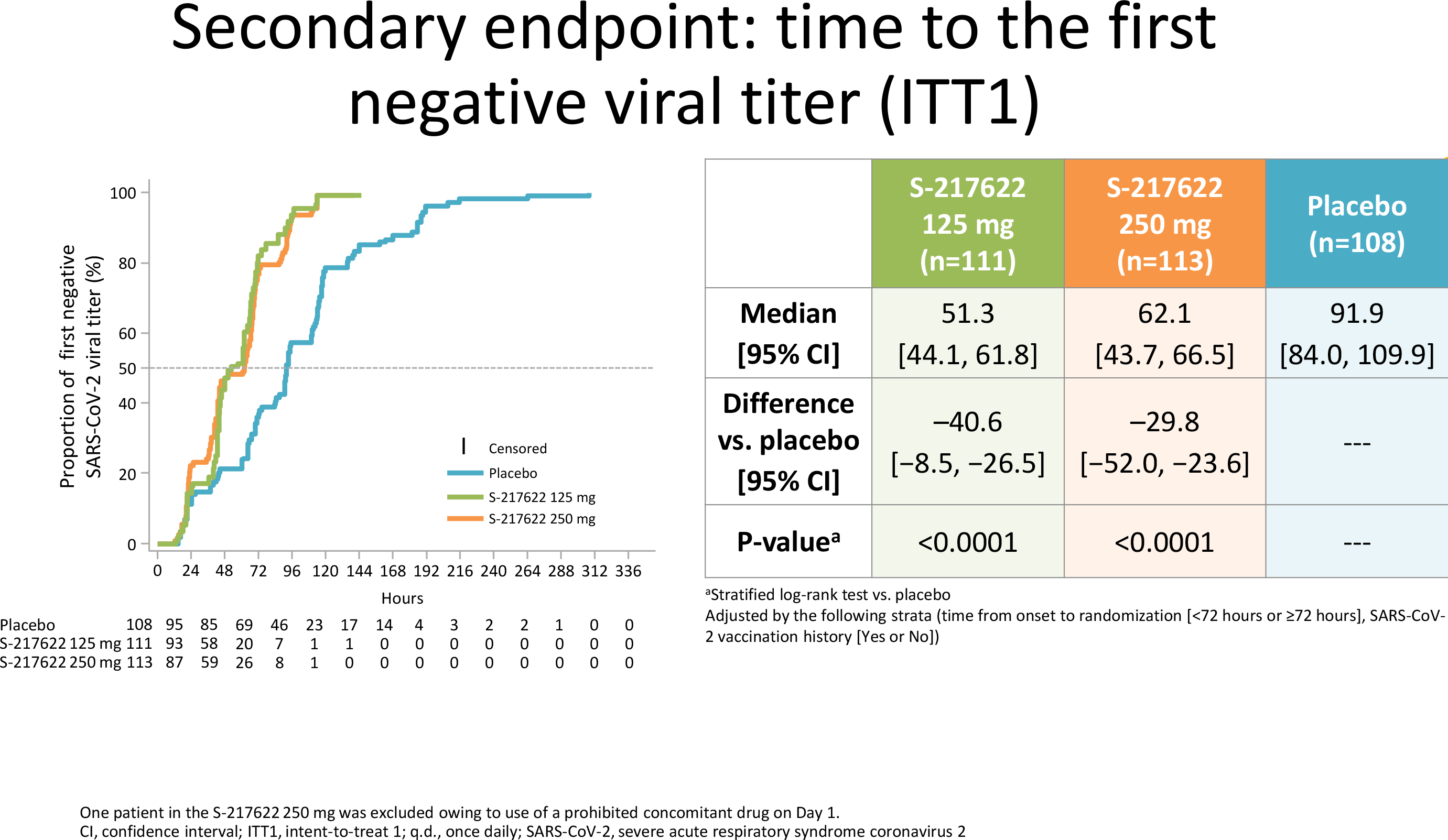
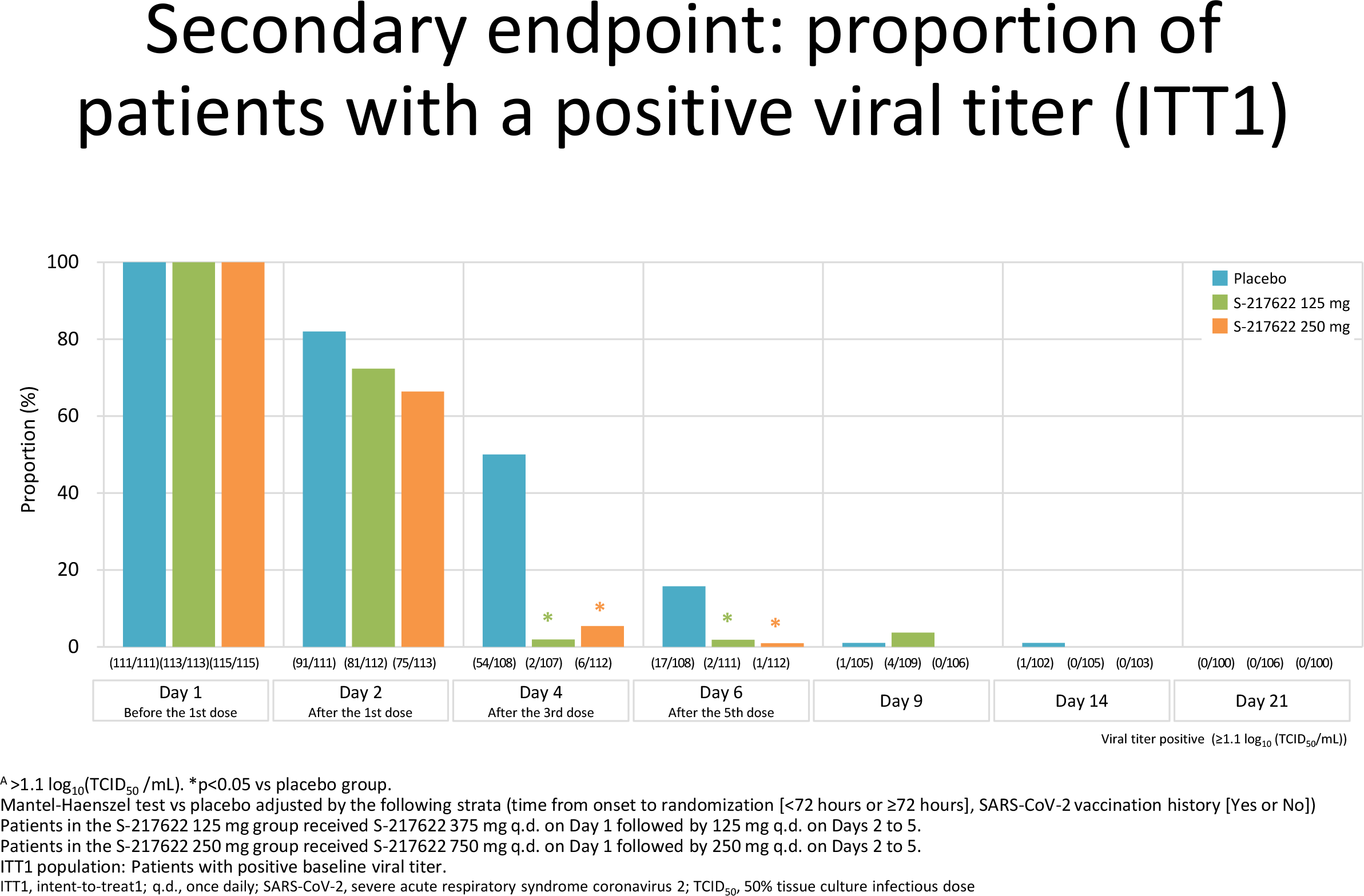
The time to the first negative viral titer test after treatment initiation was a median of 51 hours (95% CI: 44–62) and 62 hours (95% CI: 44–67) in the low- and high-dose ensitrelvir subgroups — versus 92 hours (95% CI: 84-110) in the placebo group (p<0.0001). Thus, administration of Xocova reduced the time of viral shedding when a sick person infected healthy ones by a median of 41 hours and 30 hours, or 1 to 2 days, relative to placebo. By the 4th day of treatment, about 10% remained infectious, compared with about half in the control group.
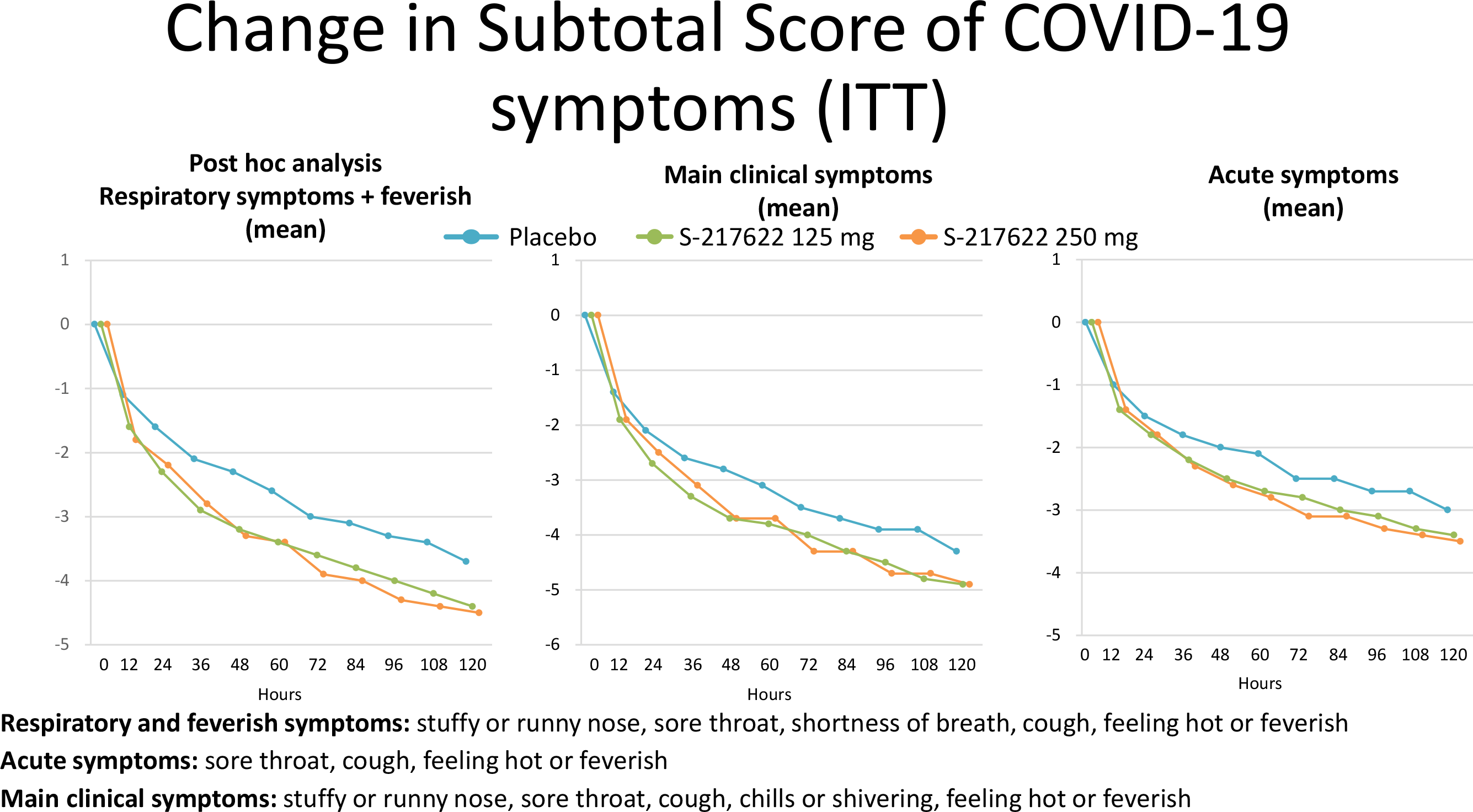
Xocova and placebo showed an identical degree of improvement in COVID-19 symptoms, although when it came to respiratory and feverish symptoms (stuffy or runny nose, sore throat, shortness of breath, cough, feeling hot or feverish), there was some tendency for them to resolve more quickly with ensitrelvir.
The main safety complaint about ensitrelvir was a decrease in high-density lipoprotein (HDL) cholesterol, experienced by 22% and 29% of subjects in the low-dose and high-dose subgroups of the drug.
Phase 3 Results
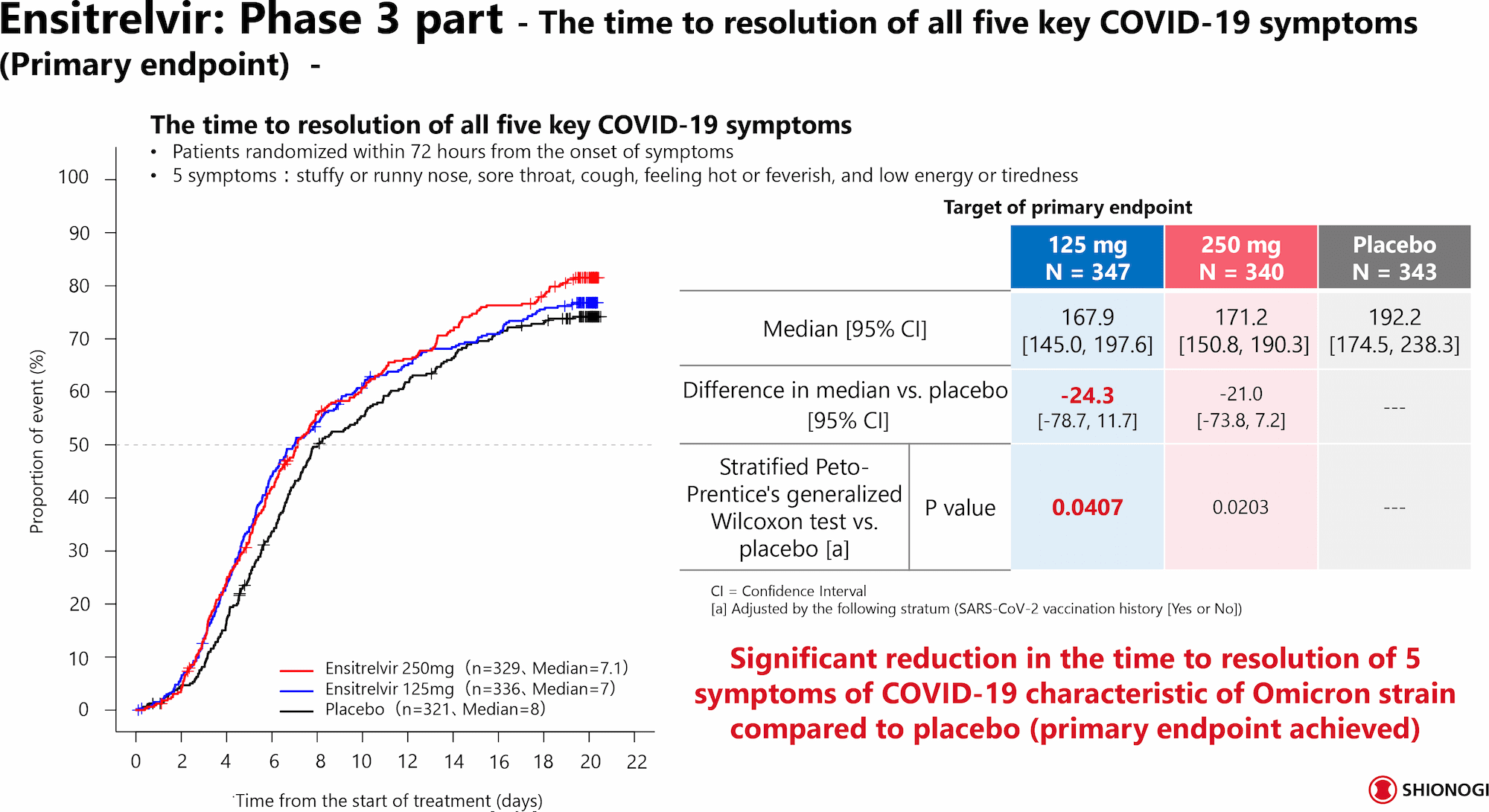
Shionogi & Co. confirmed the efficacy of Xocova in the task of reducing the time required to resolution of five typical symptoms of COVID-19 caused by the Omicron, such as stuffy or runny nose, sore throat, cough, feeling hot or feverish, and low energy or tiredness.
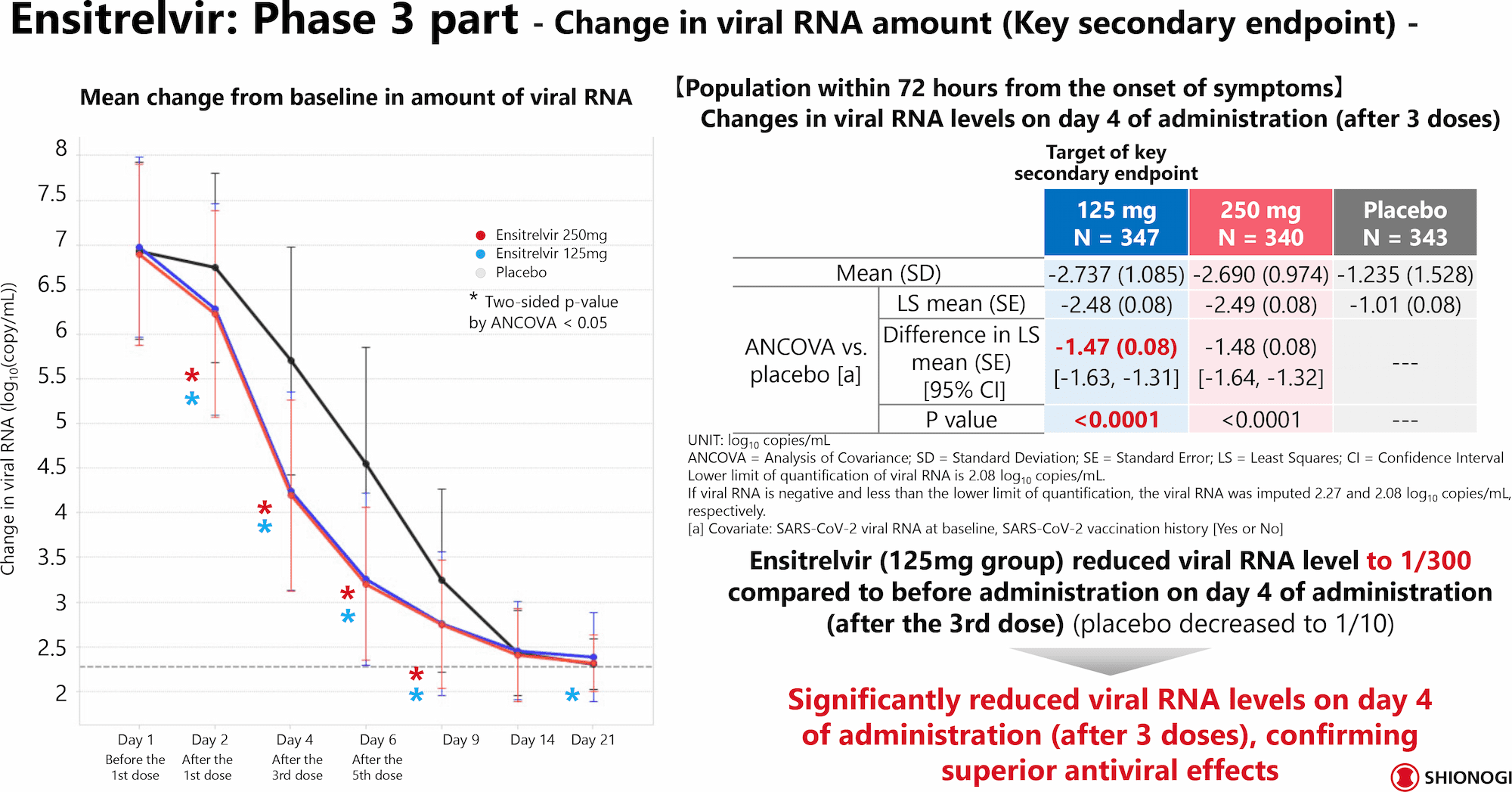
An analysis of data from patients (n=690) who were treated with ensitrelvir (125 mg daily) or placebo no later than 72 hours after manifestation of COVID-19 symptoms found the following outcomes.
Xocova accelerated recovery by approximately one day. While it took a median of 192.2 hours (95% CI: 174.5–238.3) in the placebo group, this time was reduced to 167.9 hours (95% CI: 145.0–197.6) in the ensitrelvir group. The difference was 24.3 hours (95% CI: −78.7 to +11.7; p=0.0407).
It should be understood that the relatively small difference with the placebo group is due to several factors that are responsible for the generally milder course of COVID-19 regardless of whether or not antiviral treatment was used. First, the Omicron variant itself causes a less severe form of infection: The virus proliferates and eliminates faster than when infected with other variant — consequently, remission occurs more quickly. Second, more than 90% of the participants were vaccinated against COVID-19, meaning that their immune system was prepared to repel the viral attack.
On day 4 of treatment (after three doses of the drug), viral RNA load decreased by a mean of 2.74 log10 copies/mL (at a least squares mean of 2.48) in the ensitrelvir group and by 1.24 log10 copies/mL (1.01) in the placebo group (p<0.0001). Or, in simplified terms, Xocova reduced viral RNA load to 1/300 of its initial level, placebo to 1/10.
There was a trend toward shorter time to resolution of other COVID-19 symptoms.
Among patients who started treatment with ensitrelvir within 120 hours after manifestation of the disease, there was a numerical reduction in time to symptom resolution, although without statistical significance.
No serious adverse events have been reported when prescribing Xocova. The most common adverse events in the ensitrelvir group were decreased high-density lipoprotein (HDL) cholesterol and increased triglyceride levels.
Xocova: Ensitrelvir for Prevention of COVID-19
Shionogi & Co. is going to test the feasibility of ensitrelvir in the task of preventing the development of symptomatic COVID-19.
The corresponding SCORPIO-PEP phase 3 clinical trial is scheduled for launch in late 2022. Prophylactic administration of Xocova to healthy individuals (n=2040) who live in the same household as COVID-19–infected individuals will be studied. Results will not be available soon: participant enrollment is due to end in the second quarter of 2023.
Experiments in animal models indicate that Xocova is well suited to protect healthy individuals sharing or in contact with infected individuals from infection with SARS-CoV-2 coronavirus.
Thus, in Syrian hamsters treated with high doses of ensitrelvir, 4 days after inoculation with the highly pathogenic Delta variant, the level of coronavirus RNA in nasal turbinates and lung tissue was dramatically reduced (105-fold), and the viral titer dropped to undetectable. The same was true when infected with Alpha, Gamma, and Omicron variants. After 18 days, neutralizing antibodies against coronavirus were undetectable. In experiments with infection of healthy hamsters with sick ones, prophylactic doses of ensitrelvir resulted in a dramatic reduction of the viral load in the lungs after 6 days of contact between the animals. All this indicates that ensitrelvir administration provides sterile protection against SARS-CoV-2 infection and COVID-19 development.
In comparison, the protective efficacy of molnupiravir in some cases was not different from that of placebo.
It should be understood that in animal experiments, the prophylactic administration of an antiviral drug at the pre-infection or infection stages is a highly sensitive experimental method for detecting protective drug efficacy.
However, clinical validation of Paxlovid for COVID-19 prophylaxis did not justify itself: Preventive administration of the antiviral reduced the risk of COVID-19 development by approximately one third, which was not a statistically significant indicator.
Xocova: Mechanism of Action of Ensitrelvir
Xocova (ensitrelvir) is an oral antiviral drug for the treatment of COVID-19 infection caused by the SARS-CoV-2 coronavirus.
The active ingredient in Xocova is ensitrelvir (S-217622), a small-molecule non-peptidomimetic non-covalent orthosteric selective inhibitor of 3C-like protease (3CLpro), also known as main protease (Mpro), an enzyme necessary for coronavirus replication.
SARS-CoV-2, being an enveloped positive-sense (+) RNA virus, enters host cells by binding its S protein to angiotensin-converting enzyme 2 (ACE2) on the cells and then releasing genomic RNA (gRNA) into the cytoplasm after uncoating. The cell’s ribosomes then translate the gRNA into the two major polyproteins, pp1a and pp1ab. Proteases embedded in viral nonstructural proteins 3 (Nsp3) and 5 (Nsp5), papain-like protease (PLpro) and chymotrypsin-like protease (3CLpro), respectively, cleave pp1a and pp1ab into 16 nonstructural proteins that assemble into replication–transcription complexes (RTCs). The latter produce new gRNAs and a set of subgenomic RNAs (sgRNAs) including open reading frames (ORFs) that encode structural viral proteins such as S protein, membrane (M), envelope (E), and nucleocapsid (N) proteins, as well as a number of accessory proteins. The newly created gRNAs are translated to produce additional nonstructural proteins, serve as a template for further RNA synthesis, or are packaged into new virions.
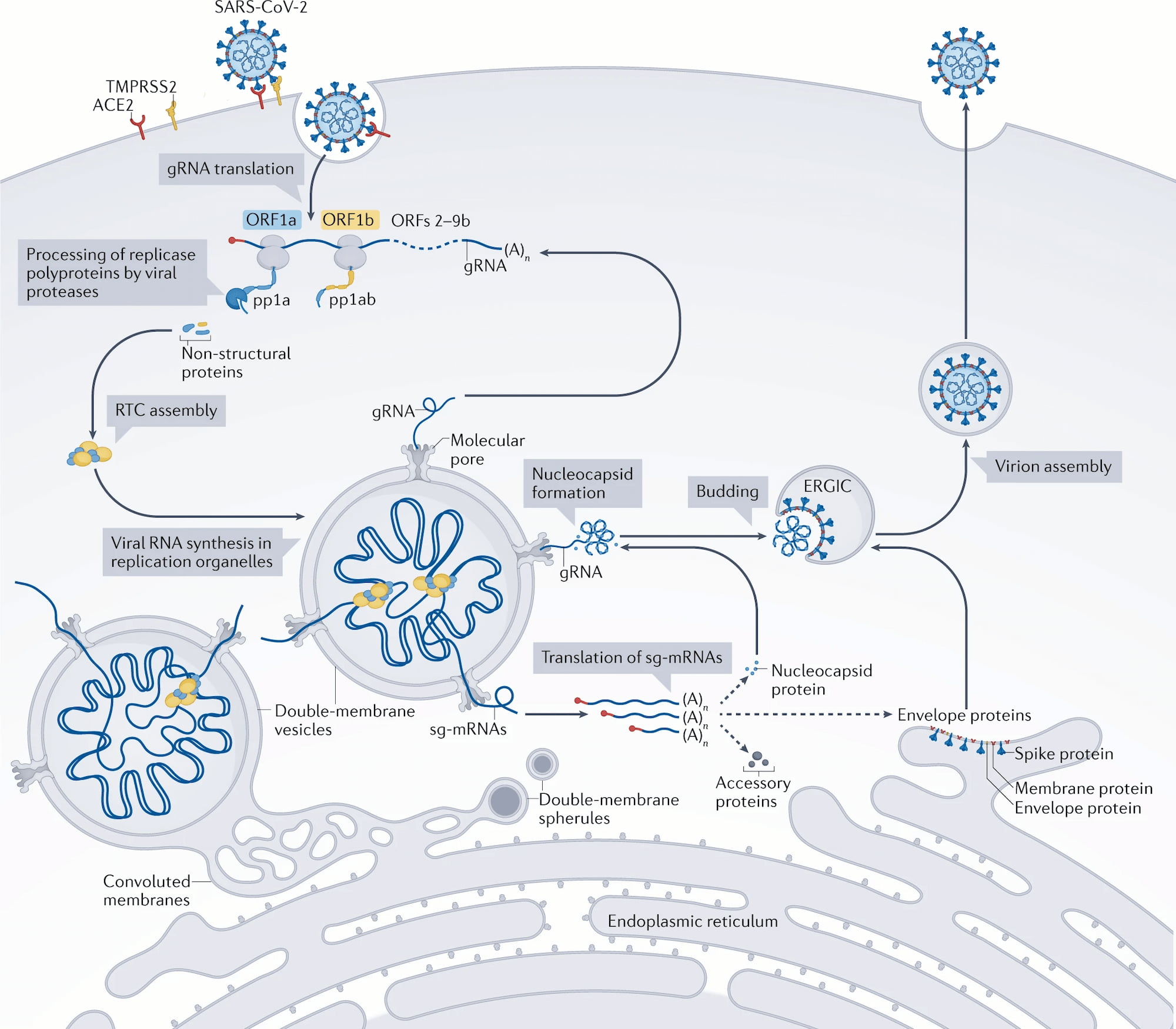
Inhibition of 3CLpro with ensitrelvir interrupts the life cycle of the virus, making it unable to replicate.
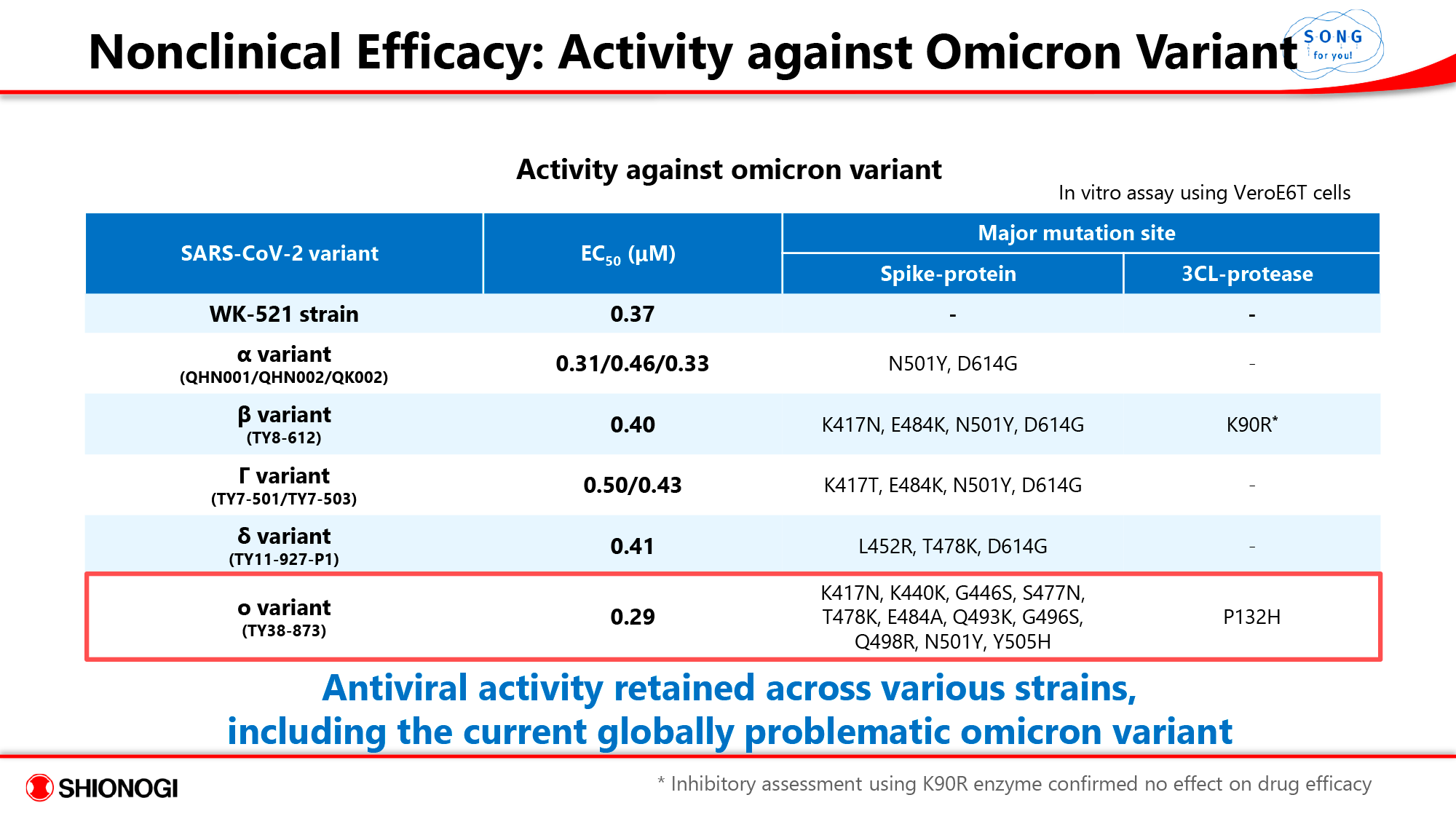
Since no significant mutations near the catalytic center of 3CLpro have been reported so far, it is safe to say that ensitrelvir will retain its high antiviral activity in all SARS-CoV-2 variants, current and future.
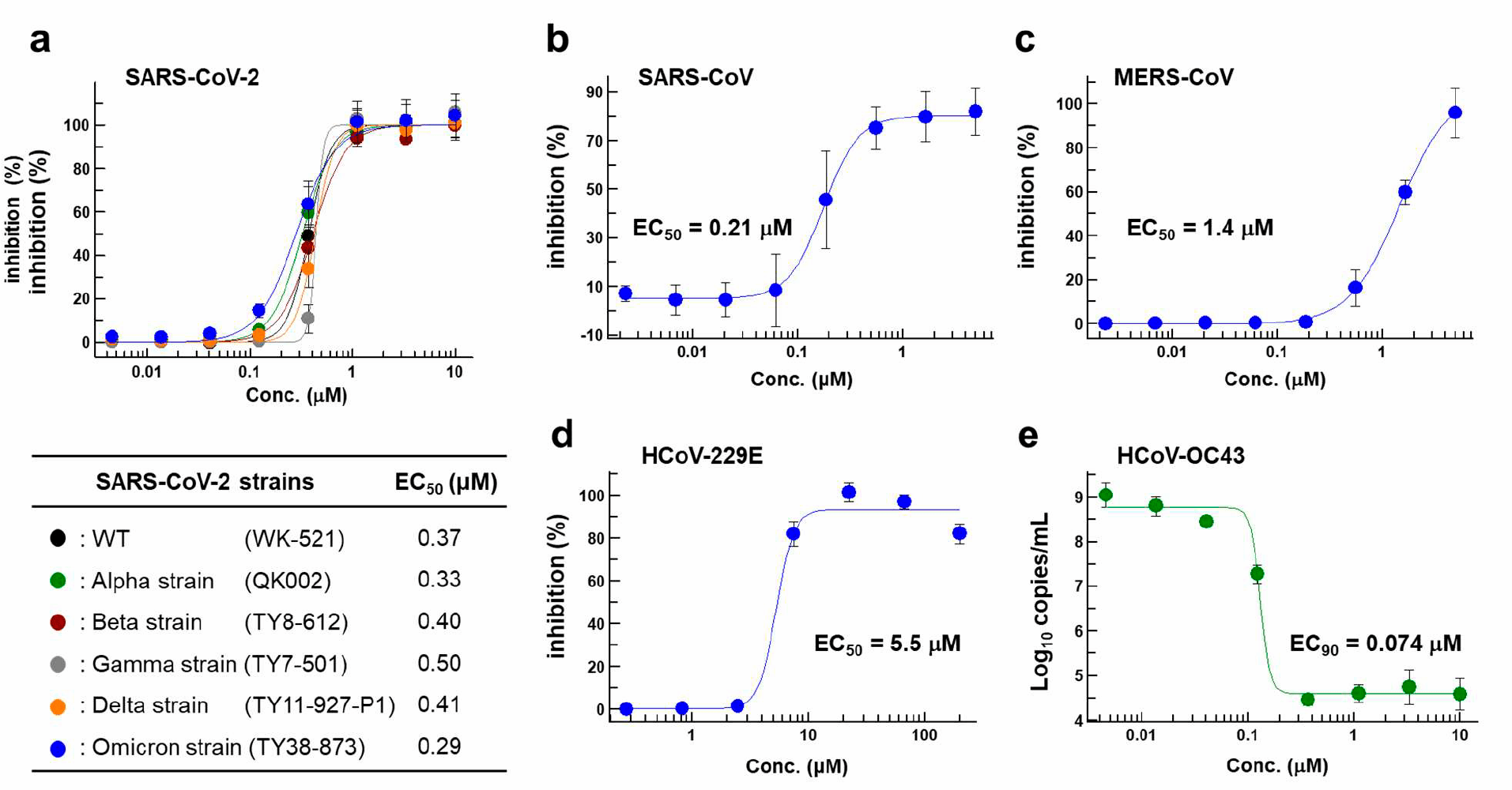
Thus, the in vitro antiviral activity of ensitrelvir assayed on Vero E6/TMPRSS2 cell lines infected with various SARS-CoV-2 variants was independent of mutations. For the original coronavirus and its variants Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Delta (B.1.617.2), and Omicron (B.1.1.529) the EC50 (effective drug concentration required to suppress viral replication by 50%; the lower this value, the more effective, that is, at lower concentrations, the drug compound works) was 0.37 μmol, 0.33 μmol, 0.40 μmol, 0.50 μmol, 0.41 μmol, and 0.29 μmol.
The EC50 value for individual Omicron subvariant (sublineages) BA.1, BA.1.1, BA.2, BA.2.75, BA.4, and BA.5 was 0.29 μmol, 0.36 μmol, 0.52 μmol, 0.30 μmol, 0.22 μmol, and 0.40 μmol.
- For the sake of clarity, it should be understood that in the context of the SARS-CoV-2 coronavirus, mutations leading to new variants are usually understood as spontaneous mutations in the S protein of the virus, which is used for adhesion and cell invasion.
- As a survival strategy, the coronavirus, by mutating the S protein on its surface, tries to increase proliferation, virulence, and infectivity, as well as to find new hosts. This is accomplished through a series of spontaneous mutations, occurring one after another under the pressure of host selection, regardless of the presence of any antiviral drug in the body.
- At the same time, mutations in viral enzymes, which have already evolutionized so that their function is maximized, are not selected for, and therefore do not spread to the entire coronavirus population. If artificial mutational pressure is applied, e.g. in the form of a pharmaceutical enzyme inhibitor, wild variants of the virus die out — new drug-resistant variants emerge. However, such variants are generally less infectious and less capable of spreading.
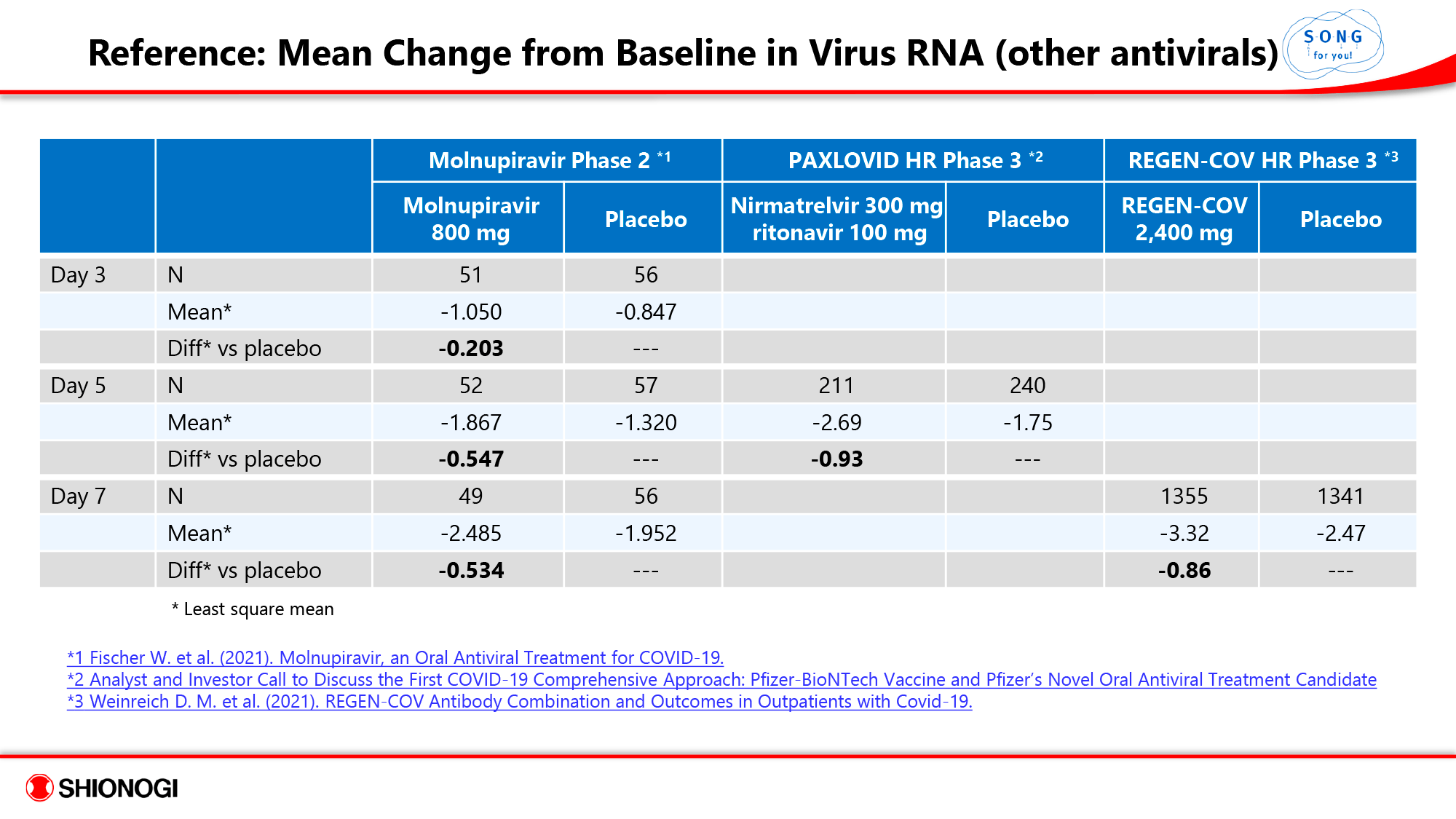
Ensitrelvir reduces viral RNA load at levels comparable to nirmatrelvir, molnipiravir by Merck & Co., and a number of monoclonal antibodies.
The mechanism of action of ensitrelvir is similar to that of nirmatrelvir developed by Pfizer. However, the latter is not as chemically optimal. Nirmatrelvir, first, is a peptidomimetic covalent inhibitor of 3CLpro and, second, requires the concomitant administration of ritonavir as a pharmacokinetic booster. A number of challenges are known to improve the target selectivity and pharmacokinetic profile of peptidomimetic covalent inhibitors because of their inherent natural reactivity properties, low oral bioavailability (due to low cellular permeability), low metabolic stability, and low stability in serum. [1] [2] [3]
Ensitrelvir, unlike Paxlovid, is not characterized by a wide range of drug interactions. Pfizer’s drug includes ritonavir (pharmacokinetic booster of nirmatrelvir), which inhibits cytochrome P450 3A4 (CYP3A4), a hepatic enzyme that metabolizes xenobiotics, i.e. deactivates drug compounds. Adding ritonavir at a low dose increases the bioavailability of nirmatrelvir, helping to slow down the metabolism of this molecule so that it retains its activity in the body for a longer period of time and at higher concentrations. Thus, first, co-administration of Paxlovid with other drugs whose clearance is highly dependent on CYP3A4 activity is contraindicated due to the fact that their concentrations may increase. Second, some drugs that are CYP3A4 inducers may decrease the concentration of ritonavir and nirmatrelvir, resulting in loss of therapeutic efficacy of Paxlovid.
A 5-day course of COVID-19 treatment with Xocova involves taking 7 pills of ensitrelvir. A similarly long course of treatment with Paxlovid requires 20 pills of nirmatrelvir and 10 pills of ritonavir.
Ensitrelvir was developed by Shionogi & Co. in collaboration with Hokkaido University.
Xocova: Expert Comments
The design of the SCORPIO-SR (jRCT2031210350) phase 2/3 clinical trial of ensitrelvir, which resulted in the approval of the drug in Japan, was developed to be as close to a real patient population as possible.
First, the age range of participants was broad (12–70 years). Second, there were no restrictions on vaccination status: both vaccinated and unvaccinated participants were invited. Third, there were no conditions that the patients were characterized by the presence of any risk factors potentially contributing to severe COVID-19 (e.g., diabetes mellitus or a history of cardiovascular disease).
The only requirement was to start COVID-19 treatment no later than 5 days after the onset of its symptoms and signs. And this is obvious, because the mechanism of action of ensitrelvir implies suppression of coronavirus replication, and this is reasonable to do only at the initial stage of disease development, because later on the infection enters a phase where it is not the virus itself but the consequences it causes that play a decisive role.
Remarkably, most of the subjects (80%, 85%, and 93% in phases 2a, 2b, and 3) were vaccinated against SARS-CoV-2. Nevertheless, Shionogi & Co. is confident that the positive treatment effect is due to ensitrelvir and not to the vaccine.
The aim of the clinical trial was to gather evidence that timely administration of ensitrelvir effectively reduces the viral load (this leads to containment of coronavirus spread in the body and suppression of formation of its reservoirs) and quickly stops the symptoms of infection. And it did the job.
Sionogi & Co. has not yet concluded whether ensitrelvir can significantly reduce the risk of worsening the course of COVID-19 with subsequent hospitalization. Apparently, data will be collected in the future. If the outcomes prove themselves, then we can safely talk about strong competition with Paxlovid.
The forthcoming path of ensitrelvir development involves entering the international arena, including the U.S., the most lucrative market for any pharmaceutical business. To this end, an international SCORPIO-HR (NCT05305547) phase 3 clinical trial is underway among outpatients (n=1490) both with and without risk factors for severe COVID-19 (older age and/or a history of certain diseases). Outcomes will be summarized in fall 2023.
The STRIVE (NCT05605093) phase 3 clinical trial, which will test the feasibility of administering ensitrelvir to patients hospitalized with COVID-19, is preparing to launch. On top of standard therapy, participants will be prescribed a 5-day course of Xocova.
Shionogi & Co. has not neglected the pediatric patient population. A clinical trial of ensitrelvir is planned for children ages 6–12.
Overall, Shionogi & Co.’s plans for Xocova extend beyond those of Paxlovid. The Japanese drugmaker intends to prove that ensitrelvir is suitable for treating all patients with COVID-19, including people without risk factors for worsening to severe disease and those with asymptomatic infection. Paxlovid has bypassed these categories of patients.
Extras
Prescribing Information
Xocova (ensitrelvir). Prescribing information. Japan. [PDF]
Shionogi & Co.’s Presentations
Briefing session on COVID-19. Shionogi & Co., November 24, 2022. [PDF]
Shionogi R&D Day 2022. October 12, 2022. [PDF]
Phase 2b part of S-217622, a novel 3C-like protease inhibitor as once daily oral treatment for SARS-CoV-2 infection in Japan and South Korea. ECCMID, April 24, 2022. [PDF]
Results from Ph1 and Ph2a studies of S-217622, a novel 3C-like protease inhibitor as once daily oral treatment for SARS-CoV-2 infection. ECCMID, April 24, 2022. [PDF]
Top-line results of the phase 2a part of the phase 2/3 trial of S-217622, the COVID-19 therapeutic drug. Shionogi & Co., February 7, 2022. [PDF]
Scientific Publications
Ensitrelvir as a potential treatment for COVID-19. Expert Opin Pharmacother. 2022 Nov 10;1-4. [source]
S-217622, a SARS-CoV-2 main protease inhibitor, decreases viral load and ameliorates COVID-19 severity in hamsters. Sci Transl Med. 2022 Nov 3;eabq4064. [source]
SARS-CoV-2 3CLpro mutations selected in a VSV-based system confer resistance to nirmatrelvir, ensitrelvir, and GC376. Sci Transl Med. 2022 Oct 4;eabq7360. [source]
Efficacy and safety of ensitrelvir in patients with mild-to-moderate COVID-19: A protocol for a multicenter, randomized, double-blind, placebo-controlled, phase 3 study (the SCORPIO-SR trial). medRxiv, September 23, 2022. [source]
Oral nonpeptidic, noncovalent triazine coronavirus main protease inhibitors for treating COVID-19. ACS Med Chem Lett. 2022 Aug 19;13(9):1394-1396. [source]
Efficacy and safety of ensitrelvir in patients with mild-to-moderate COVID-19: The phase 2b part of a randomized, placebo-controlled, phase 2/3 study. medRxiv, June 26, 2022. [source]
A pandomized phase 2/3 study of ensitrelvir, a novel oral SARS-CoV-2 3C-like protease inhibitor, in Japanese patients with mild-to-moderate COVID-19 or asymptomatic SARS-CoV-2 infection: Results of the phase 2a part. Antimicrob Agents Chemother. 2022 Oct 18;66(10):e0069722. [source]
Safety, tolerability, and pharmacokinetics of the novel antiviral agent ensitrelvir fumaric acid, a SARS-CoV-2 3CL protease inhibitor, in healthy adults. Antimicrob Agents Chemother. 2022 Oct 18;66(10):e0063222. [source]
Efficacy of ensitrelvir against SARS-CoV-2 in a delayed-treatment mouse model. J Antimicrob Chemother. 2022 Oct 28;77(11):2984-2991. [source]
Discovery of S-217622, a noncovalent oral SARS-CoV-2 3CL protease inhibitor clinical candidate for treating COVID-19. J Med Chem. 2022 May 12;65(9):6499-6512. [source]
Oral administration of S-217622, a SARS-CoV-2 main protease inhibitor, decreases viral load and accelerates recovery from clinical aspects of COVID-19. bioRxiv, February 15, 2022. [source] [PDF]