Highlights
Since its first therapeutic use in 1922 to save a patient with diabetes mellitus, insulin has been an excellent example of scientific innovation. Despite numerous advances that have provided improvements in insulin therapy, pharmacological progress aimed at further perfecting insulin has not been able to definitively solve the problem of treatment optimization.
Over the past 100 years, we have learned that insulin is a complex pharmacological agent with a narrow therapeutic window. Each decade has had its own pioneering milestones, indicative of efforts and advances in various scientific disciplines, basic and applied. A host of insulin dosing issues had to be addressed to accurately match the ever-changing need for insulin throughout the day, with rapid bolus insulin action required during meals and slow and steady basal insulin action required between meals and at night.
For a century, science has been working to create and develop molecular analogues of insulin and its pharmaceutical formulation, chemical engineering production, and delivery biotechnology to mimic as closely as possible the natural patterns of insulin release from pancreatic beta cells and reduce the time spent in a state of hyperglycemia or hypoglycemia.
The latest achievement in insulin therapy is the emergence of long-acting insulin analogues, which have taken patients’ lives to a whole new level. The once-daily basal insulins Lantus (insulin glargine) and Levemir (insulin detemir), first offered by Sanofi and Novo Nordisk in April 2000 and June 2004, followed by Tresiba (insulin degludec) and Toujeo (insulin glargine), prepared by these Danish and French pharmaceutical companies in January 2013 and February 2015, made it possible both to reduce the burden of insulin injections and to achieve more or less acceptable glycemic control.
Still, the overall level of stable glycemic control in type 1 and type 2 diabetes remains far from normalization.
Novo Nordisk will soon launch Awiqli (insulin icodec), an ultra-long-acting basal insulin that is administered subcutaneously once a week.
The U.S. Food and Drug Administration (FDA) is scheduled to make a decision on Awiqli in April 2024. It will also soon be available in Europe, China, and Japan.
Meanwhile, in mid-March 2024, Awiqli was approved in Canada, which became the first country in the world to authorize insulin icodec.
Weekly basal insulin is expected to increase patient adherence to insulin therapy, which in turn will be reflected by improved glycemic control in diabetes. From a practical point of view, everything is transparent: 52 injections per year instead of 365 injections.
Alternative brand names for insulin icodec include Aweeqli, Simwekli, and Wunzeek. Other possible brands include Bemrelfy, Iwelby, and Onwelby.
Awiqli: Why Ultra-Long-Acting Insulin Is Needed
Despite a growing armamentarium of highly effective blood glucose-lowering medications, many patients with type 2 diabetes eventually require insulin therapy [1].
Modern basal insulins have high therapeutic efficacy and a reduced risk of hypoglycemia compared with previous generations of insulins. However, insulin therapy is often delayed even when indicated. This occurs due to clinical inertia and concerns of patients and health care providers [2] [3]. Among the main reasons are fear of hypoglycemia, weight gain, injections, and anticipation of problems associated with strict adherence to treatment and a perceived decrease in quality of life [4] [5] [6] [7] [8] [9] [10] [11].
Even if insulin therapy is eventually initiated, poor adherence (compliance to treatment), where insulin needs to be administered daily, is common and is associated with inadequate glycemic control and high costs to the health care system [12] [13]. In some cases, basal insulin therapy is suboptimally administered (e.g., ineffective dose-finding methods are used), leading to poor clinical outcomes and adherence [14]. Insufficient duration of insulin treatment is another obstacle to achieving glycemic control [15], and the need for frequent insulin injections is a major factor in this problem [16] [17] [18] [19].
If basal insulin could be administered just once a week, this would result in less clinical inertia, greater adherence, and improved patient quality of life, assuming the risk of hypoglycemia remains low. Such optimistic speculation is extrapolated from outcomes comparing weekly and daily administration of glucagon-like peptide-1 receptor (GLP1R) agonists during treatment of type 2 diabetes [20] [21] [22] [23].
Awiqli: Design Features of Insulin Icodec
Long-acting insulin analogues achieve pharmacokinetic profiles suitable for once-daily subcutaneous injection in various ways [1] [2].
Thus, insulin glargine was developed with an elevated isoelectric point (pH shift from 5.4 to 6.7), which leads to the formation of slowly absorbing precipitates of insulin hexamers at physiological pH in vivo, thereby providing a subcutaneous insulin depot. Subsequently, an improved version of insulin glargine was designed in which its higher doses are delivered in a smaller volume, resulting in an even longer and more smooth effect due to the reduced surface area of the more compact injectable depot [3] [4] [5].
Insulin detemir is acylated with 14-carbon fatty acid, which helps to slow down absorption due to dimerization of insulin hexamers and reversible binding to albumin both in the subcutaneous depot and in the circulatory system [6] [7].
Insulin degludec is acylated with a 16-carbon fatty acid. Insulin degludec dihexamers assemble into multihexamers in the subcutaneous depot, with the fatty acid side chains binding the hexamers like “pearls on a string,” thereby prolonging the time they remain in the injectable depot. The fatty acid also promotes the reversible binding of insulin degludec monomers to albumin, which leads to increase its half-life [8].
It should be understood that the development of weekly basal insulin is not solely about prolonging its half-life. In order to reduce the risk of hypoglycemia, the pharmacokinetic (PK) and pharmacodynamic (PD) profiles should be more predictable than those of existing daily insulins, along with less inter-patient and intra-patient variation.
Insulin icodec, as an acylated insulin analogue, is based on a re-engineered version of the experimental oral basal insulin OI338. The addition of a 20-carbon fatty diacid (icosanedioic acid) to the B-chain of the insulin molecule provided strong reversible binding to albumin. Three amino acid substitutions (at positions A14, B16, and B25) increased stability and minimized enzymatic degradation. The above modifications also reduced affinity for insulin receptor and subsequent insulin receptor-mediated clearance, which was reflected by a longer half-life [9] [10] [11].
Insulin icodec is designed to have a prolonged PK profile with a slow and sustained glucose-lowering effect mainly due to reduced binding to insulin receptor and reduced clearance rate rather than prolonged release from the injection site [12]. For example, the affinity of insulin icodec for insulin receptor is only 0.03% of that of native insulin, but the weekly dose of insulin icodec is reduced by one-quarter that of daily insulin glargine [13]. Therefore, the PD profile of insulin icodec is more clinically relevant than its PK profile. Stable state PD simulations have shown that the glucose-lowering effects mediated by insulin icodec are evenly distributed over a one-week dosing period [14].
Awiqli: Clinical Efficacy and Safety of Insulin Icodec
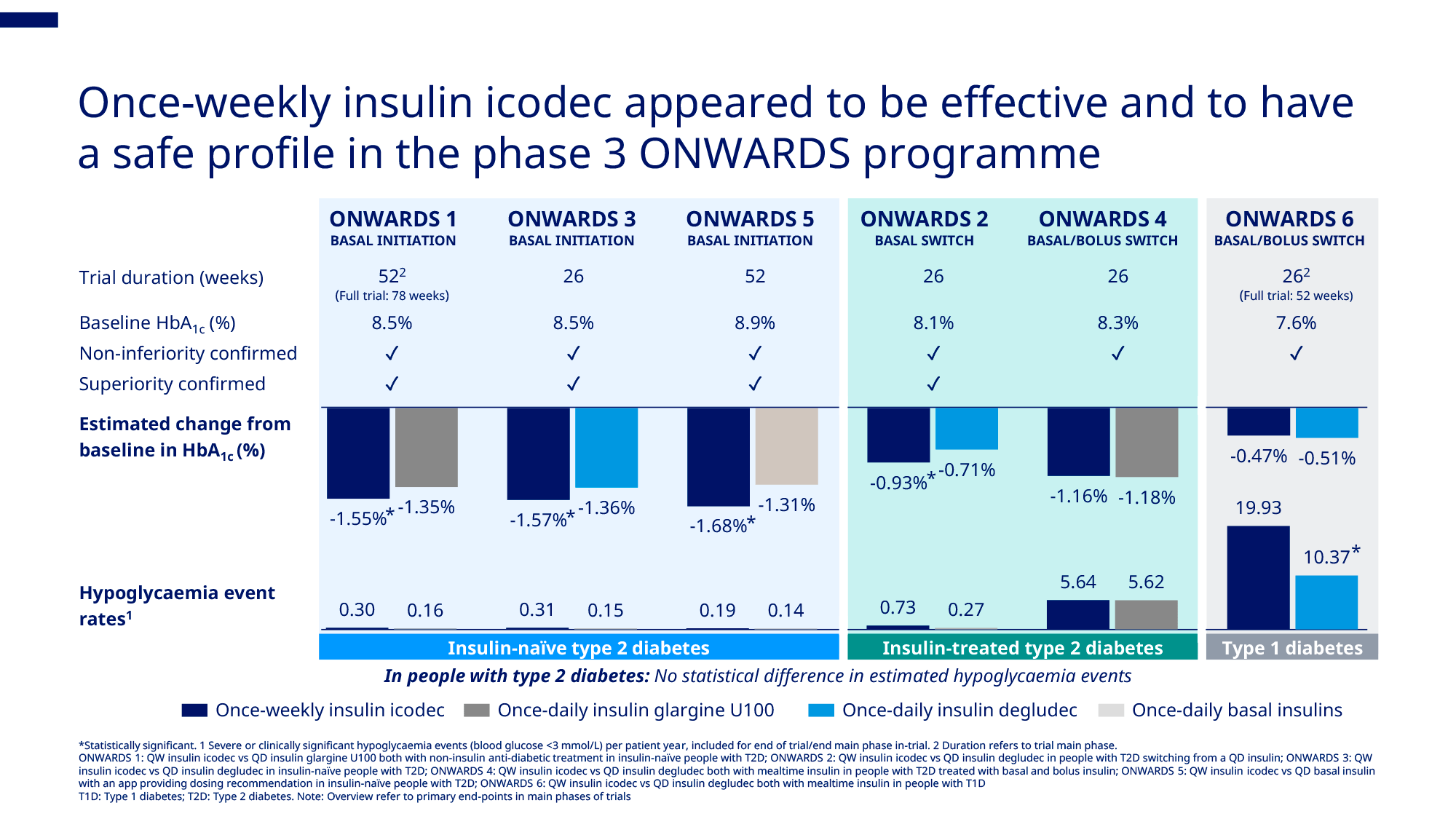
Novo Nordisk has evaluated the efficacy and safety of Awiqli (insulin icodec) in the large-scale ONWARDS phase 3a clinical program enrolling adult patients (n=3765) with type 2 diabetes mellitus.
- ONWARDS 1 (NCT04460885), 78 weeks, 984 patients. Weekly insulin icodec — versus daily insulin glargine. Both insulins are on any non-insulin antidiabetic drugs. In insulin-naïve patients [1].
- ONWARDS 2 (NCT04770532), 26 weeks, 526 patients. Weekly insulin icodec — vs. daily insulin degludec. In patients had previously treated with basal insulin (neutral protamine Hagedorn insulin [insulin isophane], insulin degludec, insulin detemir, or insulin glargine) [2].
- ONWARDS 3 (NCT04795531), 26 weeks, 588 patients. Weekly insulin icodec — vs. daily insulin degludec. In insulin-naïve patients [3].
- ONWARDS 4 (NCT04880850), 26 weeks, 582 patients. Weekly insulin icodec — vs. daily insulin degludec. Both insulins are on bolus insulin aspart 2–4 times a day. In patients had previously treated with basal insulin (neutral protamine Hagedorn insulin [insulin isophane], insulin degludec, insulin detemir, or insulin glargine) and bolus insulin (insulin aspart, insulin lispro, or insulin glulisine) [4].
- ONWARDS 5 (NCT04760626), 52 weeks, 1085 patients. Weekly insulin icodec (with DoseGuide App mobile app recommending dosage) — vs. daily insulin glargine or insulin degludec. In insulin-naïve patients [5].
Awiqli was also evaluated among adult patients (n=582) with type 1 diabetes mellitus who had previously treated with basal and bolus insulin. In the 26-week ONWARDS 6 clinical trial (NCT04848480), participants were administered weekly insulin icodec or daily insulin degludec. Both insulins on a background of bolus insulin aspart 2–4 times daily [6].
Awiqli (Insulin Icodec): Results of ONWARDS Phase 3a Clinical Program
| Study | Patients | Control | HbA1c reduction, % | Achieving HbA1c < 7.0%, % | Hypoglycemia rate, events per patient-year | Body weight change, kg | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Weekly insulin | Daily insulin | Weekly insulin | Daily insulin | Weekly insulin | Daily insulin | Weekly insulin | Daily insulin | |||
| ONWARDS 1 (NCT04460885) | Insulin-naïve, n=984 | Insulin glargine, both groups are on any oral antidiabetics | 1.55* | 1.35 | 58 (53) | 45 (43) | 0.30 | 0.16 | +2.29 | +1.83 |
| ONWARDS 2 (NCT04770532) | Previously received basal insulin, n=526 | Insulin degludec | 0.93* | 0.71 | 40 (37) | 26 (27) | 0.73 | 0.27 | +1.40 | 0.30 |
| ONWARDS 3 (NCT04795531) | Insulin-naïve, n=588 | Insulin degludec | 1.57* | 1.36 | 57 (52) | 42 (40) | 0.31 | 0.15 | +2.8 | +2.3 |
| ONWARDS 4 (NCT04880850) | Previously received basal and bolus insulin, n=582 | Insulin degludec, both groups are on bolus insulin aspart | 1.16** | 1.18 | 41 (26) | 45 (25) | 5.64 | 5.62 | +2.8 | +2.2 |
| ONWARDS 5 (NCT04760626) | Insulin-naïve patients, n=1085 | Insulin glargine or insulin degludec | 1.68* | 1.31 | 47 (41) | 35 (32) | 0.19 | 0.14 | ||
| ONWARDS 6 (NCT04848480) | Previously received basal and bolus insulin, n=582 | Insulin degludec, both groups are on bolus insulin aspart | 0.47** | 0.51 | 40 (10) | 46 (17) | 19.93 | 10.37 | +1.29 | +1.01 |
The proportions of patients who achieved a target HbA1c levels < 7.0% also include those who experienced hypoglycemia (proportions of patients without clinically significant or severe hypoglycemia are shown in parentheses).
Hypoglycemia refers to clinically significant hypoglycemia (blood glucose levels below 54 mg/dL [3 mmol/L]) or severe hypoglycemia (with severe cognitive impairment requiring external assistance for recovery).
* — Weekly insulin icodec was statistically significantly better than daily comparison insulin.
** — Weekly insulin icodec was no worse than daily comparison insulin.
IcoSema = Insulin Icodec + Semaglutide
In parallel, Novo Nordisk has a COMBINE phase 3a clinical program, due to end in 2024, which is studying the treatment of type 2 diabetes with a fixed-dose combination of insulin icodec and semaglutide, a glucagon-like peptide-1 receptor agonist (GLP1RA). The weekly fixed-ratio combination (700 units/mL and 2 mg/mL) is tentatively named IcoSema.
COMBINE 1 (NCT05352815), 52 weeks, 1290 patients. Weekly IcoSema — versus weekly insulin icodec. With or without the addition of daily oral antidiabetic drugs. In patients had previously treated with basal insulin (neutral protamine Hagedorn insulin [insulin isophane], insulin degludec, insulin detemir, or insulin glargine).
COMBINE 2 (NCT05259033), 52 weeks, 680 patients. Weekly IcoSema — vs. weekly semaglutide 1 mg. In insulin-naïve patients but treated with GLP1RA.
COMBINE 3 (NCT05013229), 52 weeks, 680 patients. Weekly IcoSema — vs. daily basal insulin glargine with bolus insulin aspart 2–4 times daily. With or without the addition of daily oral antidiabetic drugs. In patients had previously treated with basal insulin (neutral protamine Hagedorn insulin [insulin isophane], insulin degludec, insulin detemir, or insulin glargine).
COMBINE 4 (NCT06269107), 40 weeks, 474 patients. Weekly IcoSema — vs. daily basal insulin glargine. With or without the addition of daily oral antidiabetic drugs. In insulin-naïve patients.
IcoSema: Results of COMBINE Phase 3a Clinical Program
| Study | Patients | Control | HbA1c reduction, % | Hypoglycemia rate, events per patient-year | Body weight change, kg | |||
|---|---|---|---|---|---|---|---|---|
| Weekly insulin | Daily insulin | Weekly insulin | Daily insulin | Weekly insulin | Daily insulin | |||
| COMBINE 1 (NCT05352815) | Previously treated with basal insulin, n=1290 | Weekly insulin icodec, both groups are on any oral antidiabetics daily or without them | ||||||
| COMBINE 2 (NCT05259033) | Insulin-naïve, n=683 | Weekly semaglutide 1 mg | ||||||
| COMBINE 3 (NCT05013229) | Previously treated with basal insulin, n=679 | Daily insulin glargine with bolus insulin aspart, both groups are on any oral antidiabetics daily or without them | 1.47** | 1.40 | 0.26 | 2.18 | −3.6 | +3.2 |
| COMBINE 4 (NCT06269107) | Insulin-naïve, n=474 | Daily insulin glargine, both groups are on any oral antidiabetics daily or without them | ||||||
Hypoglycemia refers to clinically significant hypoglycemia (blood glucose levels below 54 mg/dL [3 mmol/L]) or severe hypoglycemia (with severe cognitive impairment requiring external assistance for recovery).
* — Weekly IcoSema was statistically significantly better than comparison control.
** — Weekly IcoSema was no worse than comparison control.
Awiqli: Expert Comments
In four of the six ONWARDS phase 3a clinical trials, insulin icodec, Novo Nordisk’s ultra-long-acting basal insulin, statistically significantly outperformed the comparison group in reducing glycated hemoglobin (HbA1c), and did no worse in the remaining two. In other words, the therapeutic efficacy of Awiqli is unequivocally proven.
There was some concern about hypoglycemia. Those receiving weekly insulin experienced hypoglycemia more often than those on daily insulin therapy. However, in most cases the difference in the frequency of clinically significant hypoglycemia (blood glucose levels below 54 mg/dL [3 mmol/L]) was not statistically significant. An exception was observed in ONWARDS 6 clinical trial among patients with type 1 diabetes.
At this point, it remains unclear whether the combination of the slight advantage in glucose control efficacy of Awiqli, complemented by the more than obvious convenience of its use, will outweigh the increased risks of hypoglycemia that it carries, although the incidence in real-life clinical practice is likely to be higher than in clinical trials.
In any case, the emergence of high-quality, once-weekly basal insulin is a significant step forward in easing the injection burden and smoothing out pharmacokinetic and pharmacodynamic fluctuations. However, entirely new practical strategies for Awiqli introduction into clinical routine need to be developed that differ from the current daily insulin treatment of diabetes.
It should be understood that the use of weekly Awiqli will not immediately produce rapid reductions in glucose levels, since it will take approximately three to four weeks to achieve stable steady state insulin concentration. Frequent dose adjustments are not possible, and therefore loading doses may be required initially, even in insulin-independent patients in whom antidiabetic agents do not provide adequate glycemic control. Loading doses may also be helpful in patients transitioning from daily insulin. A temporary adaptation of bolus insulin doses will be needed in type 1 diabetes [1].
As for possible hypoglycemic episodes during the use of weekly Awiqli, they do not seem to last longer than with daily insulin and can be managed with standard approaches. In other words, treatment with weekly insulin should not be accompanied by any concern about worsening the severity of potential hypoglycemia in terms of duration and resistance [2] [3] [4] [5] [6] [7].
According to a systematic review and meta-analysis, weekly insulin icodec compared with daily insulin analogues provided a deeper reduction in HbA1c, allowed a greater proportion of patients to reach target HbA1c levels below 7% (including without hypoglycemia), and prolonged the time to glucose levels in the target range (TIR). Administration of insulin icodec, however, resulted in enhanced weight gain. No statistically significant differences in the frequency of clinically significant and severe hypoglycemic events were found [8].
A more recent systematic review and meta-analysis of phase 3 clinical trials only reached similar conclusions, although it indicated that insulin icodec, on the contrary, leads to weight loss [9].
The increase in body weight, if present, can be explained as follows. The affinity of insulin icodec for albumin is 9.5 times higher than that of long-acting insulins, so it activates insulin receptors much slower and longer [10]. As a result, it triggers a kind of “basal” lipogenesis, adipogenesis, and glycogenesis after reaching steady state. In particular, insulin icodec exerts continuous stimulation of insulin-dependent glucose uptake [10], which enhances lipogenesis in hepatocytes and adipocytes through the regulation of several lipogenic pathways [11]. The continuous insulin-dependent glucose uptake provided by insulin icodec leads to continuous activation of cellular lipogenic and hence anabolic pathways. At the same time, the maintenance effect of insulin icodec provides sustained insulin-mediated suppression of lipolysis, which is a major effect of insulin on fat metabolism [12], which promotes a cellular shift towards an anabolic state leading to weight gain.
Awiqli: Competitive Landscape
Eli Lilly, which directly competes with Novo Nordisk in the diabetes treatment market, is lagging behind in creating weekly insulin. Its insulin efsitora alfa (LY3209590), also known as basal insulin Fc (BIF), an ultra-long-acting basal insulin engineered differently from Awiqli (insulin icodec), will complete a phase 3 QWINT clinical program in spring–summer 2024.
Weekly insulin efsitora alfa is being compared to daily basal insulin glargine (including adjunctive bolus insulin lispro) or insulin degludec among patients with type 2 diabetes who have (or not) previously been treated with insulin therapy. One clinical trial invited patients with type 1 diabetes.
Insulin efsitora alfa is implemented by binding a single-chain insulin analogue (with a number of amino acid substitutions) to the fragment crystallizable (Fc) region of immunoglobulin G (IgG) [1] [2].
Theoretically, this increases the half-life because the fusion protein benefits from the same recycling pathway that provides the relatively long half-life of endogenous IgG [3] [4]. Thus, when IgG enters cells by micropinocytosis, the Fc region binds to the membrane-bound neonatal Fc receptor (FcRn) in acidified endocytic vesicles. Recirculating endosomes return FcRn–IgG complexes to the cell surface, and the physiologic pH of the extracellular medium allows the release of IgG.
The binding affinity of insulin efsitora alfa to the insulin receptor is two orders of magnitude lower than that of the native hormone, but full agonism persists. Insulin efsitora alfa is characterized by low variability and a nearly peakless pharmacokinetic profile at one-week dosing [5] [6] [7] [8].
Phase 2 clinical trials have confirmed the therapeutic validity of insulin efsitora alfa along with the acceptability of its safety.
In the 32-week clinical trial NCT0373636785 among patients with type 2 diabetes already on insulin therapy, weekly insulin efsitora alfa was non-inferior to daily insulin degludec: the reduction in glycated hemoglobin (HbA1c) was 0.6% — versus a 0.7% reduction. Insulin efsitora alfa outperformed insulin degludec in terms of reduced frequency of hypoglycemic episodes and reduced weight gain [9] [10].
In the 26-week clinical trial NCT04450394 among patients with type 2 diabetes who had not previously treated with insulin, weekly insulin efsitora alfa demonstrated non-inferior efficacy to daily insulin degludec: HbA1c decreased by 1.20% — vs. a decrease of 1.26%. The frequencies of hypoglycemia episodes and weight gain magnitudes did not differ statistically significantly [11].
Extras
Awiqli (insulin icodec). Product monograph including patient medication information. Canada. [PDF]