Zynrelef (bupivacaine + meloxicam) is a new medication designed to relieve postoperative pain in adult patients who have undergone surgery such as a bunionectomy, open inguinal herniorrhaphy, or total knee arthroplasty.
Zynrelef, which can provide analgesic effects for up to 72 hours, is used in the form of instillations in the soft and periarticular tissues. The drug, realized in the form of a viscous solution, is used in the area of surgical intervention after final irrigation and suction (but before wound closure) and before suturing each layer if several tissue layers are involved.
The safety and efficacy of Zynrelef have not been studied in surgical procedures involving multiple vessels such as intrathoracic, large multilevel spinal, and head and neck surgeries.
Zynrelef, developed by Heron Therapeutics, is approved by the U.S. Food and Drug Administration (FDA) in mid-May 2021.
In late September 2020, Zynrelef received marketing approval in the European Union when the European Medicines Agency (EMA) approved the new drug for the management of somatic postoperative pain from small- to medium-sized surgical wounds in adults. Zynrelef is not intended for use in major surgeries including abdominal, vascular, and thoracic surgeries.

Zynrelef for Postoperative Pain: Clinical Efficacy
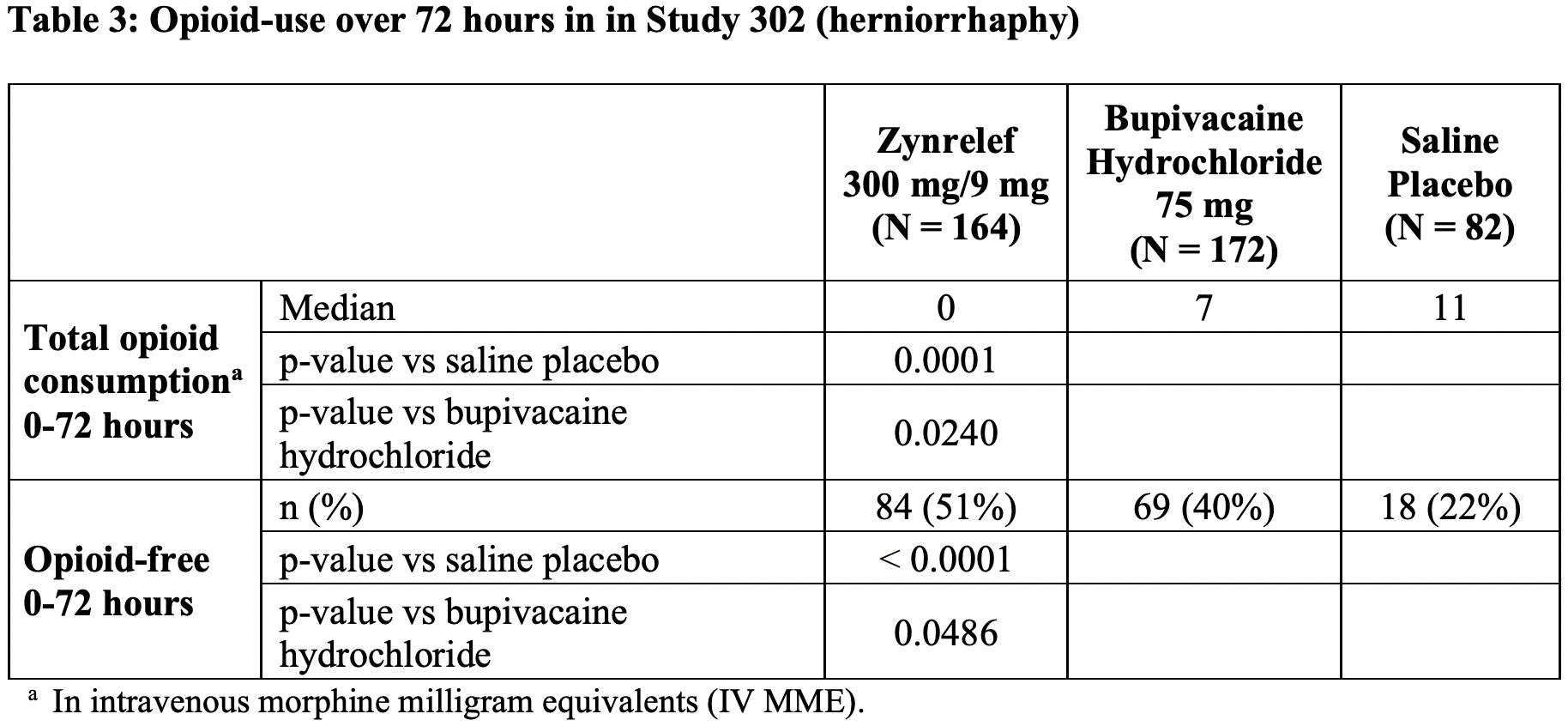
Zynrelef has been evaluated in three pivotal clinical trials: EPOCH 1 (NCT03295721) and EPOCH 2 (NCT03237481) phase 3 and NCT03015532 phase 2b. The trials, conducted according to randomized, double-blind, placebo-controlled and with the active drug comparison group, multicenter protocols, invited patients who respectively underwent unilateral simple bunionectomy (repair of valgus deformity of the big toe) with regional lidocaine Mayo block, unilateral open inguinal herniorrhaphy (hernia repair) with mesh under general anesthesia, primary unilateral total knee arthroplasty (knee replacement) under general anesthesia.
The subjects were randomized into groups that received Zynrelef, bupivacaine, or placebo.
There was no scheduled pain medication regimen after surgery but patients were allowed to use rescue analgesics as needed such as oral oxycodone 10 mg every 4 hours, intravenous morphine 10 mg every 2 hours, and/or oral paracetamol 1000 mg every 6 hours.
In all trials, the Zynrelef group outperformed the control groups with respect to the exit to the primary endpoint as stated by the mean area under the curve (AUC) of pain intensity on a numerical rating scale (NRS) recorded over a 72-hour period.
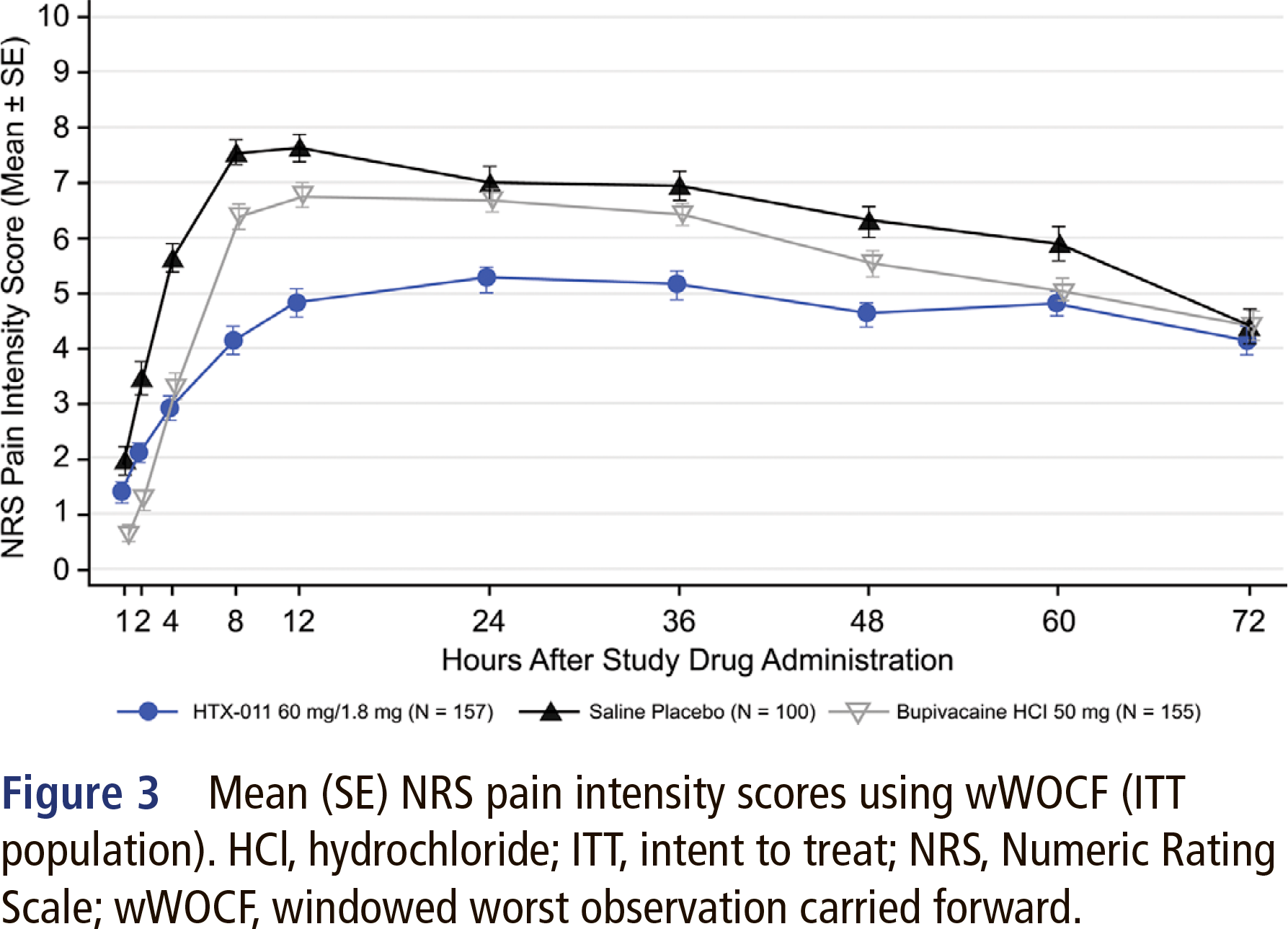
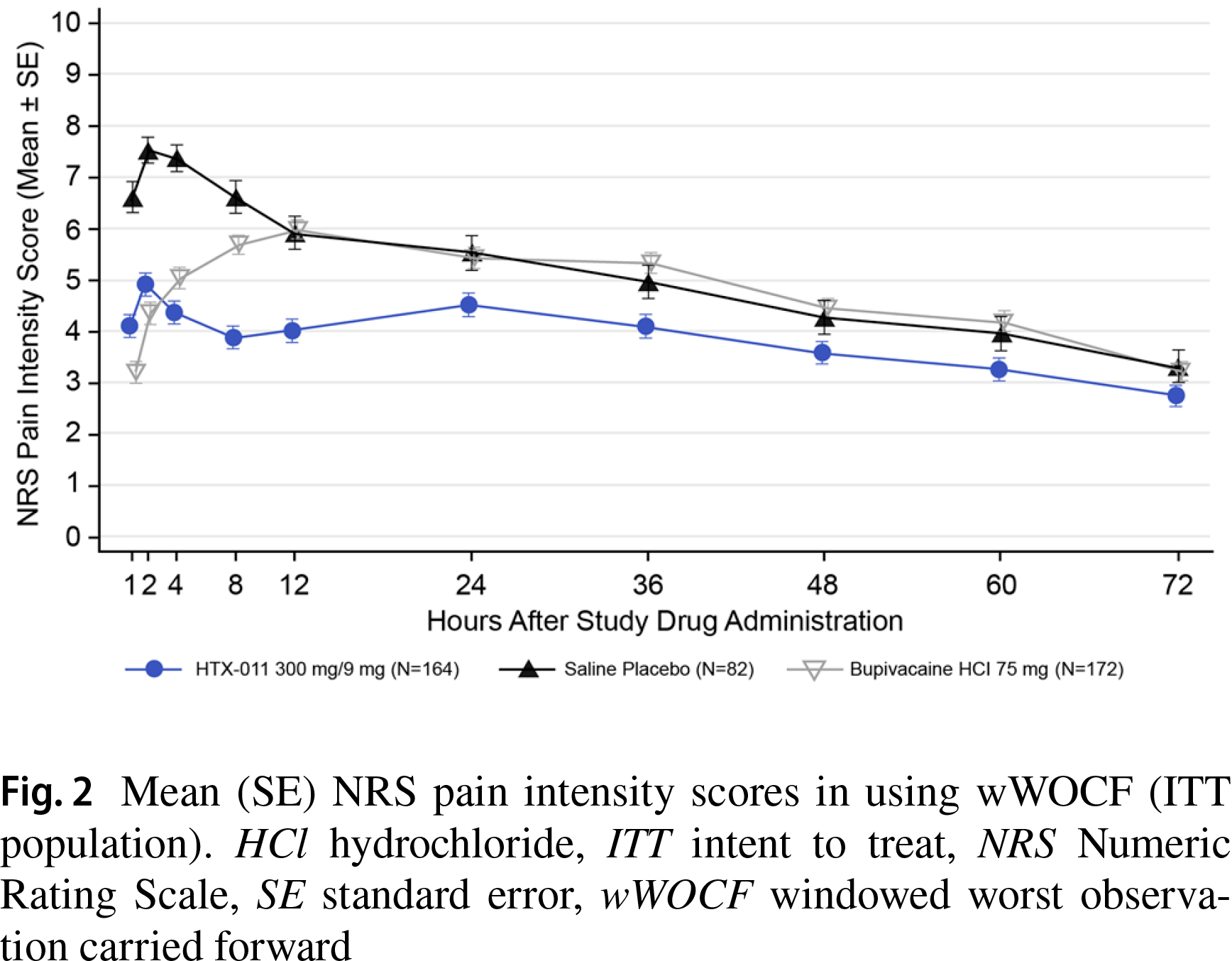
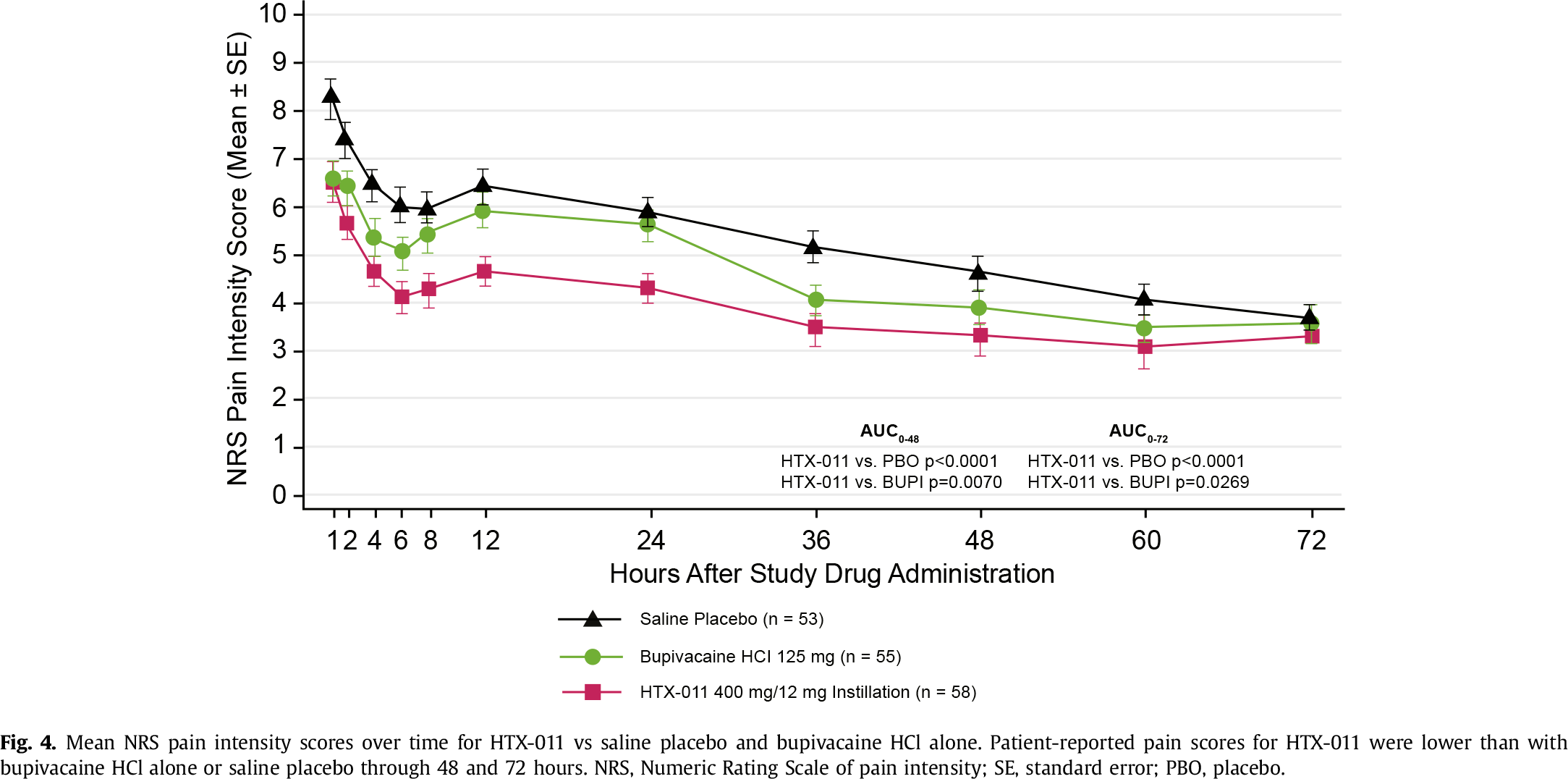
Administration of Zynrelef resulted in an increase in the proportion of patients who did not require opioids or had their dose reduced.
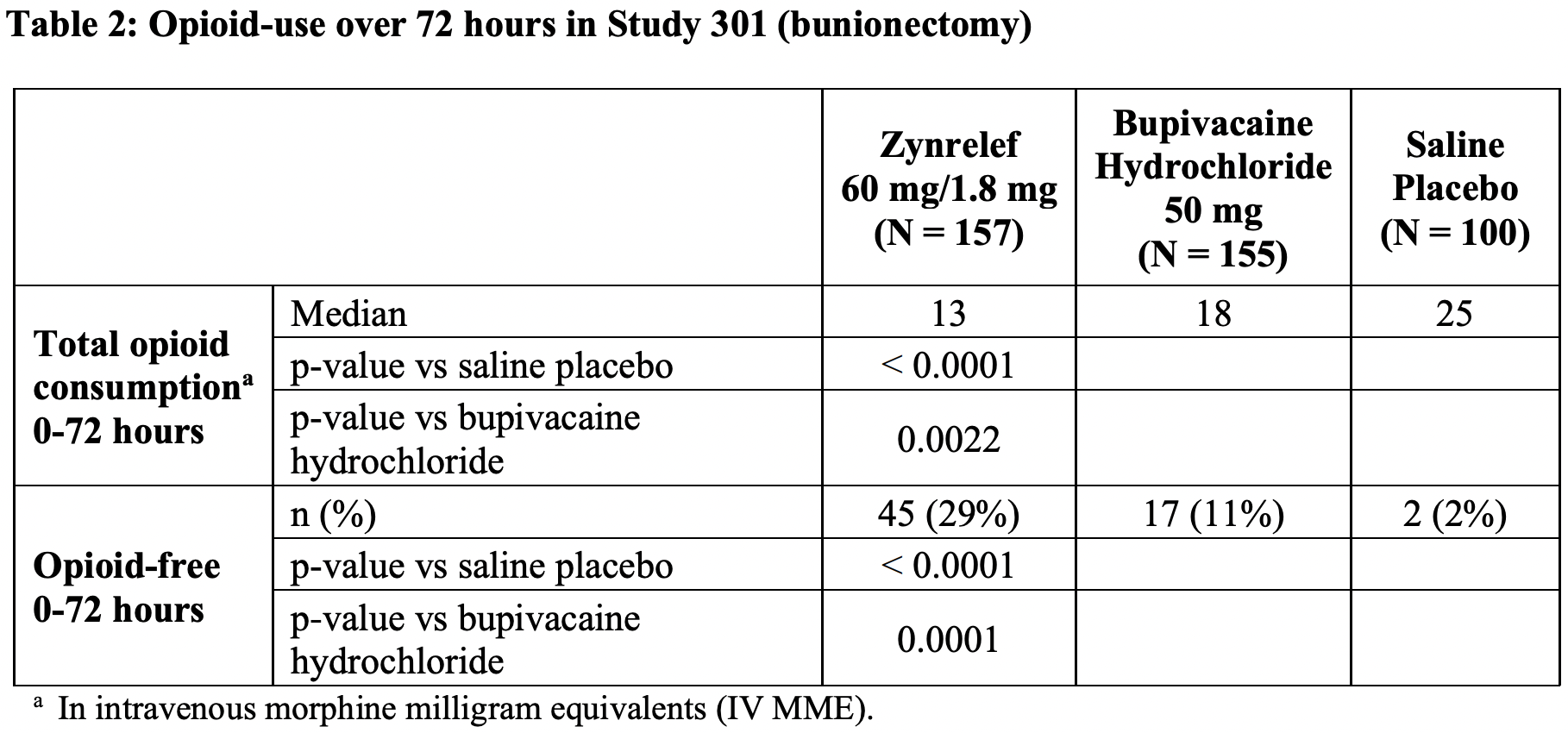
According to a meta-analysis of 7 prospective randomized clinical trials of Zynrelef, this medication when compared to bupivacaine or placebo cumulatively reduced pain intensity in the first 24 hours after surgery by 1.8 points (95% CI: 1.42–2.2) and contributed to a 7.96-fold (95% CI: 5.13–12.36) increase in the probability that no opioid was required. At 72 hours, there was a 3.25-fold (95% CI: 2.3–4.58) increase in the specified probability. At 72 hours, opioid use equivalent to intravenous morphine decreased by 10.61 mg (95% CI: 8.13–13.09).
The prescribing information for Zynrelef has a black-box warning for risks associated with the administration of NSAIDs such as serious cardiovascular thrombosis (myocardial infarction and stroke) and gastrointestinal tract events (bleeding, ulceration, perforation). Zynrelef is contraindicated in obstetrical paracervical block anesthesia and coronary artery bypass graft (CABG) surgery as well as in patients with allergic reactions to NSAIDs.
How Zynrelef Works
Zynrelef (HTX-011) is a combination drug that contains bupivacaine and meloxicam in a sustained-release formulation based on Biochronomer proprietary polymer technology for stable controlled drug delivery.
Meloxicam is a non-steroidal anti-inflammatory drug (NSAID) with anti-inflammatory, analgesic, and antipyretic properties. The exact mechanism of action of meloxicam, like any other NSAID, has not been fully understood, but it is known that the molecule inhibits cyclooxygenase 1 and 2 (COX-1 and COX-2). These enzymes are responsible for converting arachidonic acid into prostaglandin H2, the first step in the synthesis of prostaglandins which are mediators of inflammation. Prostaglandins sensitize afferent nerves and potentiate the action of bradykinin in induced pain. Meloxicam controls tissue inflammation thereby normalizing pH allowing substantially more bupivacaine to penetrate the cell membrane.
Bupivacaine is an amide-type local anesthetic with both anesthetic and analgesic effects. In high doses, bupivacaine causes surgical anesthesia, and in lower doses — sensory blockade (analgesia) with the less pronounced motor blockade. Local anesthetics block the generation and the conduction of nerve impulses presumably by increasing the threshold for electrical excitation in the nerve, by slowing the propagation of the nerve impulse, and by reducing the rate of rise of the action potential. In general, the progression of anesthesia is related to the diameter, myelination, and conduction velocity of affected nerve fibers. Clinically, the loss of nerve function occurs in the following order: pain, temperature, touch, proprioception, skeletal muscle tone.
Regarding Treatment of Postoperative Pain
Pain is one of the most common conditions affecting patients’ health and quality of life. As one of the most severe forms of acute pain, postoperative pain remains an area that suffers from a high unmet medical need.
The World Health Organization (WHO) estimates that more than 234 million major surgical operations are performed worldwide each year, the equivalent of one surgical operation per year for every 25 people.
Postoperative pain is often the predominant symptom experienced by surgical patients. Despite notable advances in pain understanding, less than half of patients who undergo surgery experience adequate postoperative pain relief. Thus, 65% of people experience moderate to severe pain, with 46% of patients still suffering from pain even after discharge. Remarkably, even minimally traumatic surgical interventions can cause pain. Still, it is orthopedic surgery that is the leading cause of postoperative pain.
Acute postoperative pain has clear pathophysiology related to peripheral and central sensitization as well as humoral factors contributing to pain at rest and during movement. Surgical tissue trauma leads to activation and sensitization of nociceptors. As a result, a person experiences constant pain at rest and increased pain on stimuli at the site of injury. Different surgical procedures affect different organs and specific tissues in and near them, creating different patterns of nociceptor sensitization and differences in the quality, location, and intensity of postoperative pain.
Prostaglandins, interleukins, cytokines, and neurotrophins are the mediators released locally and systemically during and after surgery and contribute to nociceptor sensitization. Decreased tissue pH and oxygen tension levels and increased lactate concentrations persist at the surgical site for several days. Such body reactions contribute to peripheral sensitization and spontaneous pain behavior. Nerves damaged by surgery can spontaneously discharge, and such action potentials manifest themselves as neuropathic pain, which sometimes develops into a chronic form. Painful stimuli during and after surgery increase the response of nociceptive neurons in the central nervous system, thereby amplifying the intensity of pain.
Postoperative pain can originate from the skin or deeper somatic and visceral structures. It can be classified into nociceptive somatic (from the skin, muscles, bones), nociceptive visceral (from thoracic and abdominal organs), and neuropathic (caused by damage to neural structures). It is usually a combination of several types of pain.
The aim of analgesic protocols is not only to reduce the intensity of pain but also to reduce the frequency of negative side effects and improve patient comfort. Although opioids remain an important component of the treatment of severe postoperative pain, their use as the sole therapeutic agent leads to significant problems such as impaired ventilation, sedation, nausea, vomiting, and delayed recovery of bowel function. And that is why a multimodal and balanced approach is suggested when opioids are complemented by several antinociceptive drugs (two or more) with different mechanisms of action.
Pain is optimally managed by combining regional anesthesia and analgesia techniques with systemically administered medications. Among the latter: acetaminophen, non-selective nonsteroidal anti-inflammatory drugs (NSAIDs), selective cyclooxygenase-2 (COX-2) inhibitors, N-methyl-D-aspartate antagonists (ketamine), α2-adrenoreceptor agonists (clonidine, dexmedetomidine), α2δ-receptor modulators (gabapentin, pregabalin), systemic local anesthetics, corticosteroids. Nefopam is known to reduce the need for opioids when combined with patient-controlled morphine analgesia.
The most severe postoperative pain occurs in the first 72 hours after surgery and even taking opioids does not always stop it, not to mention that prescribing them is high-risk due to possible addiction. Again, the addition of acetaminophen or systemic NSAIDs, often in high daily doses, is associated with an increased risk of hepatic, renal, gastrointestinal, and cardiovascular toxicity. All of this is translated into patient discomfort and overall dissatisfaction, delayed postoperative recovery, increased length of hospital stay, and increased medical costs.
Management of postoperative pain with locoregional anesthesia is a highly effective solution. And there are two approaches: infiltration blockade or field blockade (several injections of a local anesthetic around the wound, surgical site, or tissue area) and nerve blockade (target nerves whose location is determined by ultrasound, their stimulation, or anatomically).
Bupivacaine administered perioperatively (before the closure of the surgical wound) is the current ubiquitous standard for postoperative anesthesia. The short duration of anesthetic effect of bupivacaine (6–12 hours) has led to the appearance in 2011 of its liposomal version with delayed-release — Exparel by Pacira BioSciences, but its analgesic effect rarely lasts over 24 hours. One explanation is related to local tissue acidosis as a result of surgical trauma, which reduces the ability of local anesthetics to penetrate the membrane of nerve cells thereby resulting in a time-limited analgesic effect.
This is why there is still an unmet need for new analgesic medications capable of providing continuous pain relief for at least the first 72 hours after surgery.
Zynrelef: Facts and Forecasts
Heron was able to secure regulatory approval for Zynrelef only the third time. Thus, in May 2019, the FDA rejected New Drug Application (NDA) due to manufacturing issues, and in June 2020, it refused to do so, citing a number of preclinical issues.
Yes, Zynrelef’s efficacy is superior to that of Exparel and its safety profile is just as good. However, Heron needs to stick to the right pricing strategy otherwise it won’t be able to grab more or less decent market share. In other words, Zynrelef should be sold at a substantial discount relative to Exparel.
And so it did. Heron put a price tag on Zynrelef as follows: for a vial with 200 mg bupivacaine and 6 mg meloxicam, the wholesale acquisition cost (WAC) is $135.5; for a vial with 400 mg bupivacaine and 12 mg meloxicam, it is $267.5. These prices are 22% and 28% lower compared to Exparel’s WAC. In addition, hospitals qualifying under the 340B Drug Pricing Program have an even greater discount of 41% and 46% relative to Exparel price.
According to Evaluate Pharma’s consensus forecasts, Zynrelef’s commercial prospects are more optimistic than those of Exparel. The latter, which debuted back in 2011 and earned $418 million in 2020, will improve slowly and cross the half-billion-dollar annual sales threshold sometime in 2026. Zynrelef should get to comparable sales volumes by then.
Heron expects to further expand Zynrelef’s list of indications to include its use in cesarean section and pediatric (ages 3–17) herniorrhaphy. Moreover, there are prerequisites for off-label use once surgeons understand the full potential of the drug.
In parallel, Heron is developing HTX-034, a combination of bupivacaine and meloxicam to which a third component is added in the form of aprepitant, a selective high-affinity neurokinin 1 (NK1) antagonist used to prevent nausea and vomiting induced by chemotherapy or surgery. It is thought that aprepitant should enhance the analgesic activity of bupivacaine. At least in preclinical models, it lasted 7 days.
In February 2021, Posimir, Durect’s version of bupivacaine in a delayed-release formulation based on the proprietary SABER (sucrose acetate isobutyrate extended release) technology, appeared.
Allay Therapeutics is working on ATX-101, an ultra-slow-release bupivacaine formulation where postoperative pain relief lasts an incredible two weeks straight after a single dose.
Extras
Zynrelef (bupivacaine + meloxicam). Prescribing information. U.S. [PDF]
Zynrelef (bupivacaine + meloxicam). Prescribing information. Europe. [PDF]
Zynrelef (bupivacaine + meloxicam). European Public Assessment Report (EPAR). [PDF]
Zynrelef (bupivacaine + meloxicam). FDA approval. Heron Therapeutics. May 13, 2021. [PDF]
HTX-011 reduced pain intensity and opioid consumption versus bupivacaine HCl in bunionectomy: phase III results from the randomized EPOCH 1 study. Reg Anesth Pain Med. 2019 May 21;rapm-2019-100531. [source]
HTX-011 reduced pain intensity and opioid consumption versus bupivacaine HCl in herniorrhaphy: results from the phase 3 EPOCH 2 study. Hernia. 2019; 23(6): 1071–1080. [source]
HTX-011 reduced pain and opioid use after primary total knee arthroplasty: results of a randomized phase 2b trial. J Arthroplasty. 2020 Oct;35(10):2843-2851. [source]
HTX-011: another game changer multimodal analgesic or an ephemeral, experimental drug! Saudi J Anaesth. Jul-Sep 2020;14(3):419-420. [source]
Efficacy of new long-acting bupivacaine HTX-011 in providing pain relief for patients undergoing elective surgery — a meta-analysis of prospective randomized controlled trials. Anesth Essays Res. Apr-Jun 2020;14(2):288-294. [source]