Reyvow (lasmiditan) is a new drug for the acute treatment of migraine with or without aura in adults.
- Reyvow is not indicated for the preventive treatment of migraine.
Reyvow, developed by Eli Lilly, was approved by the U.S. Food and Drug Administration (FDA) in October 2019.
Reyvow has opened a new class of antimigraine drug compounds, ditans.
The list price of Reyvow is $672 for the package of 8 oral tablets available at retail pharmacies, but the amount of actual pay will largely depend on the patient’s insurance plan.
- List price, also referred to as wholesale acquisition cost (WAC), is the price at which pharma companies sell their medicines to wholesalers and may not represent actual transactional prices patients pay at the pharmacy.

Necessity for New Drugs to Treat Migraine
Migraine is the leading cause of disability in people under 50 years of age and the second most common cause of disability worldwide, seriously affecting the daily lives of patients and their families. Antimigraine therapy includes both prophylaxes to reduce the frequency of migraine attacks and their emergency management. Anticonvulsants (topiramate and valproic acid) and beta-blockers (propranolol and metoprolol) help most in the task of prevention; less often antidepressants (amitriptyline and venlafaxine) work. Nonsteroidal anti-inflammatory drugs, ergotamines, and triptans are used to relieve migraine attacks.
Triptans are the most popular class of antimigraine drugs, including seven commercialized medicines: sumatriptan, zolmitriptan, naratriptan, rizatriptan, almotriptan, eletriptan, frovatriptan.
Triptans, as agonists of the serotonin receptor (5-HT) subtypes 5-HT1B and 5-HT1D in blood vessels and nerve endings in the brain, provide cranial vasoconstriction and suppression of the release of vasoactive pro-inflammatory neuropeptides including calcitonin gene-related peptide (CGRP) and substance P. Because triptans activate 5-HT1B, thereby causing vasoconstriction, there is a small risk of serious cardiovascular complications. This is why triptans are contraindicated in patients with vascular disease, hemiplegic migraine, uncontrolled hypertension, and stroke. Due to the fact that cardiovascular disorders are very common in migraines, and 30-40% of patients do not respond to triptans, there is a need for new antimigraine medications.
Reyvow: Mechanism of Action of Lasmiditan
Oral lasmiditan (COL-144, LY573144) is a low-molecular-weight serotonin receptor agonist that binds selectively and with high affinity to its subtype 5-HT1F.
Lasmiditan, by stimulating 5-HT1F receptors expressed on the trigeminal ganglion and secondary trigeminal neurons in the brainstem, inhibits central and peripheral neuronal activity with suppression of CGRP release. Lasmiditan has no activity against 5-HT1B/1D (selectivity to them is 470 times lower than to 5-HT1F) and therefore there is no risk of pathological vasoconstriction, especially since there are no 5-HT1F receptor proteins on endothelial or smooth muscle cells in brain vessels.
Reyvow: Effectiveness of Lasmiditan in Acute Treatment of Migraine
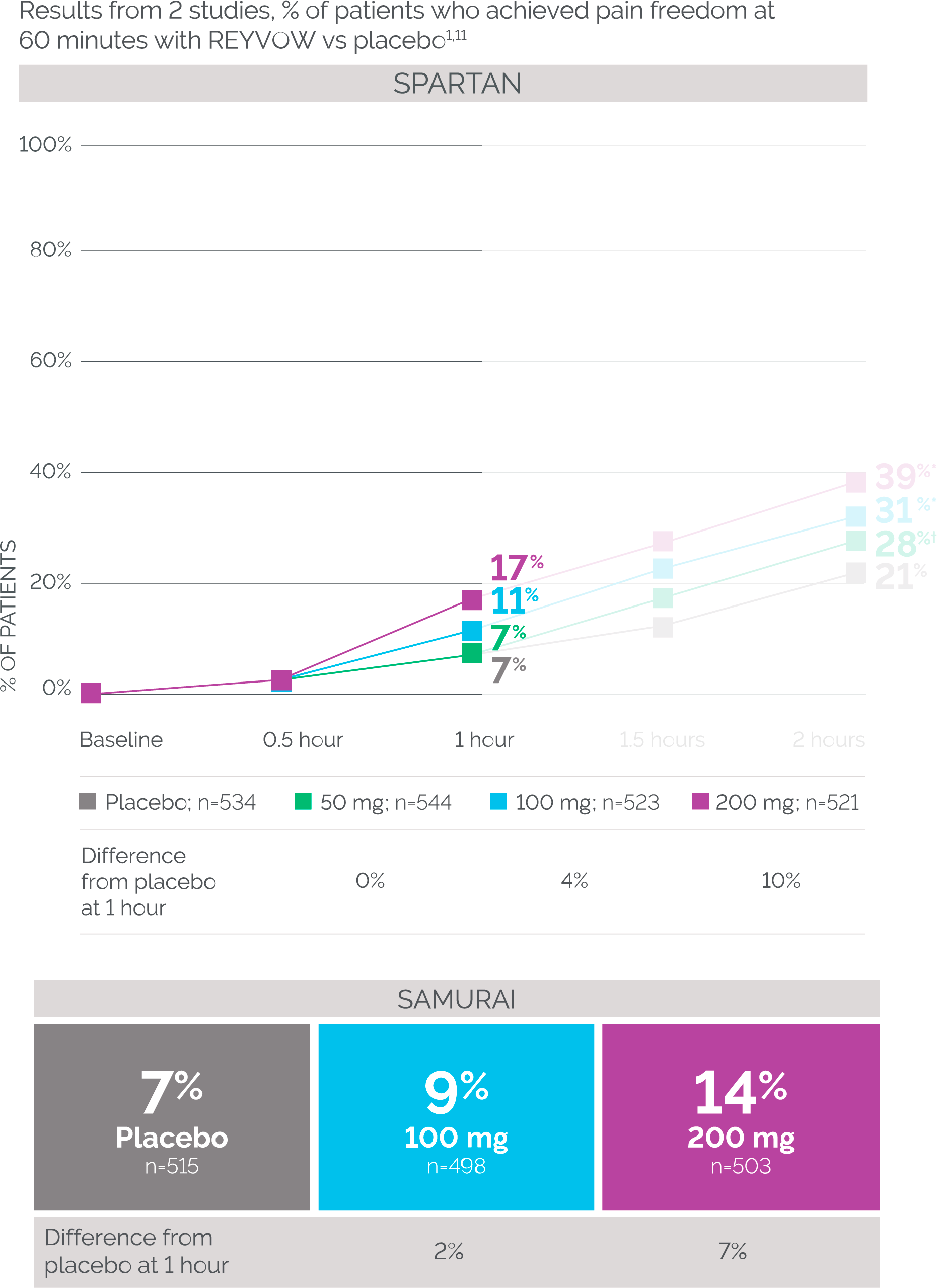
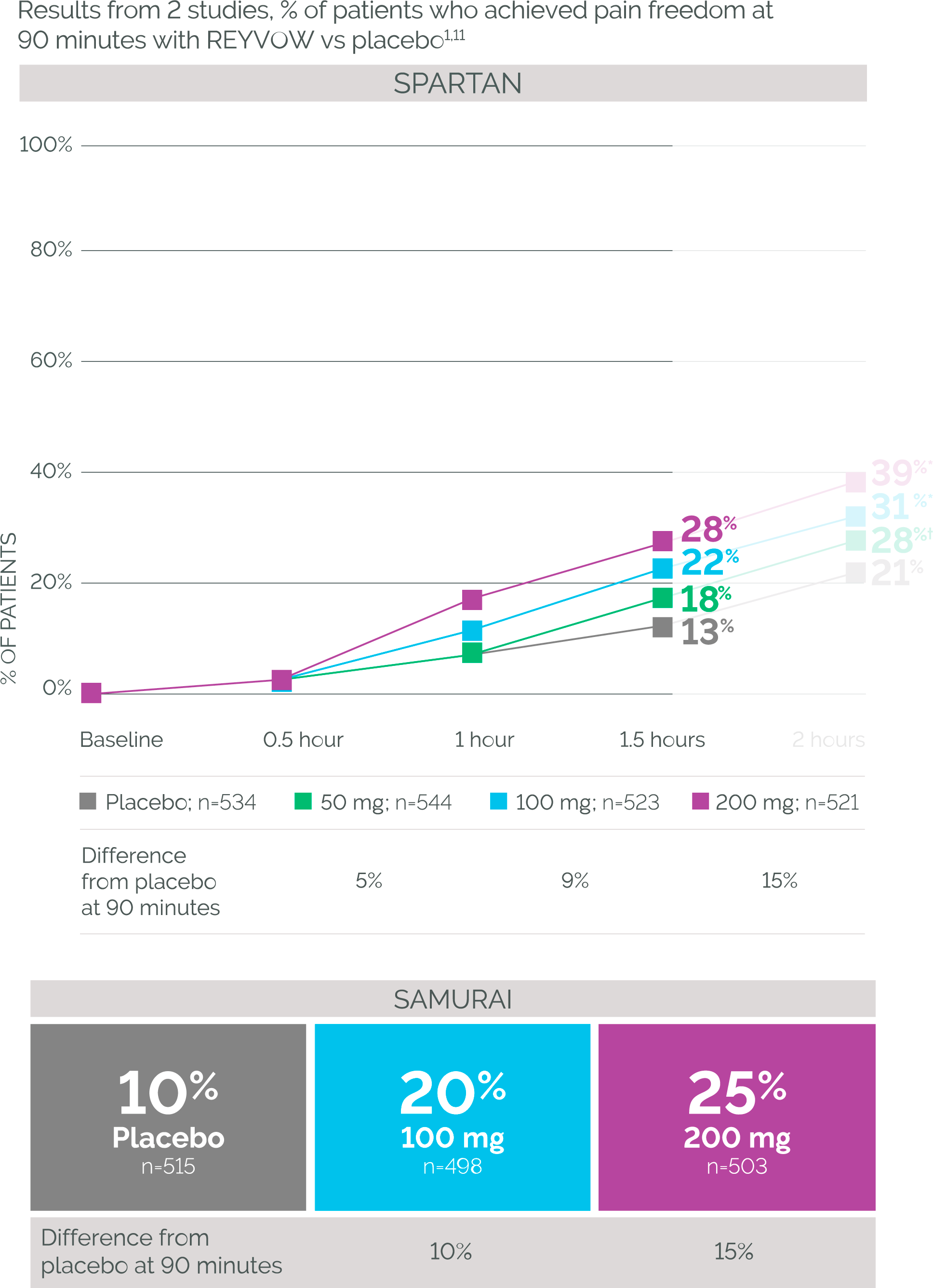
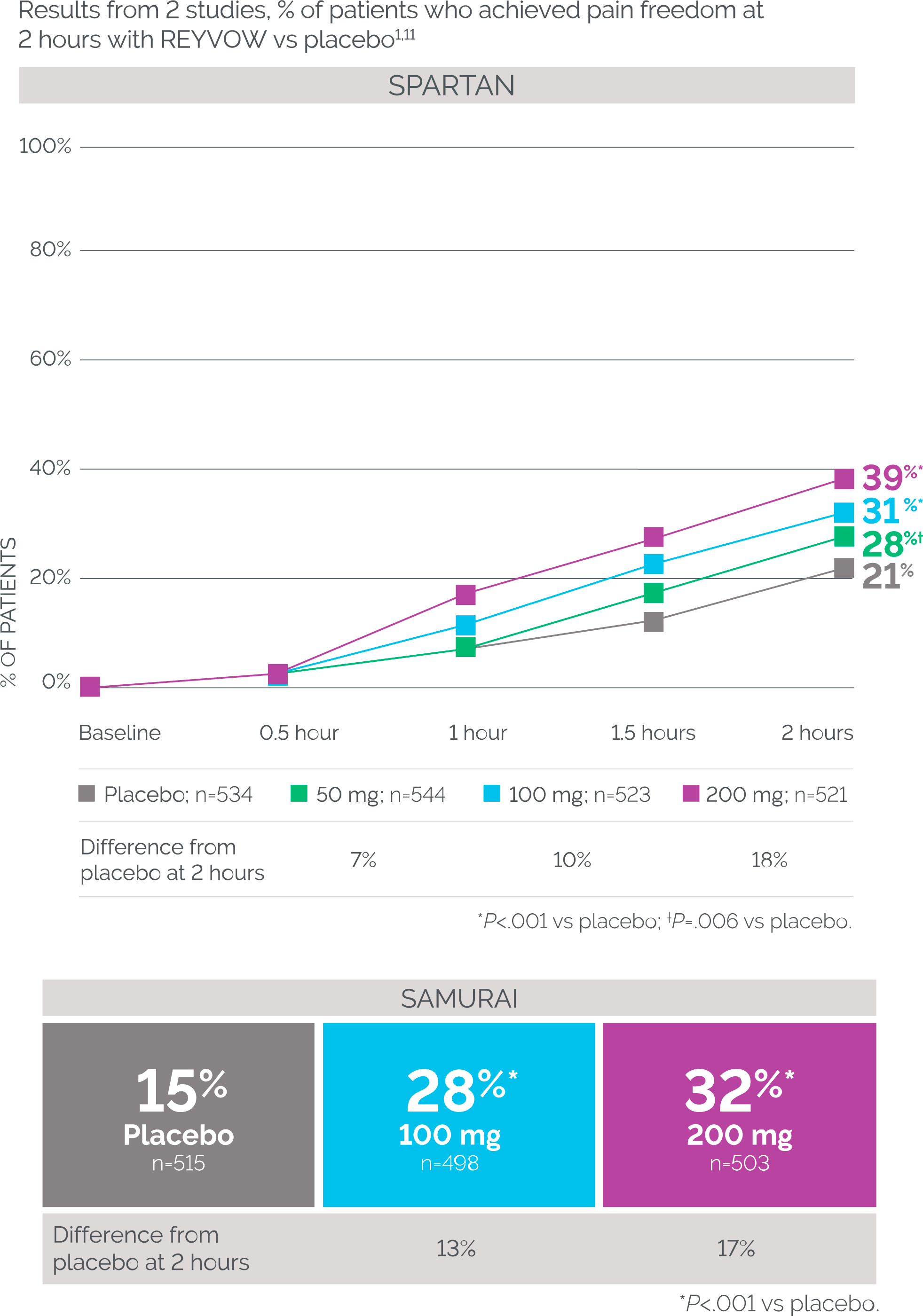
The safety and efficacy of lasmiditan were evaluated in two phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trials SAMURAI (NCT02439320) and SPARTAN (NCT02605174) involving adult patients (n=3177) with at least one year of migraine and experiencing 3–8 migraine attacks per month (less than 15 days with headache per month).
Subjects who were administered lasmiditan (50, 100, or 200 mg) or placebo within four hours of attack onset were allowed to take any additional medication for emergency migraine relief two hours after the experimental treatment, but opioids, barbiturates, triptans, and ergotamines were not permitted within 24 hours of study drug administration.
The primary endpoint was the proportion of patients who got rid of moderate-to-severe headache and the most bothersome symptoms (MBS), such as photophobia, phonophobia, and nausea, after two hours of drug administration.
All doses of lasmiditan showed a significantly higher proportion of patients achieving pain freedom and MBS freedom compared to placebo recipients (p<0.001).

In addition, lasmiditan provided a sustained therapeutic response (within 24 and 48 hours), manifested by freedom from headache, freedom from the most bothersome symptoms, total freedom from migraine, and disability-free outcomes.
In the case of patients taking a second dose of lasmiditan, when it did not work after two hours or when the migraine initially subsided but then returned, its repeat prescription was only effective in relieving an acute migraine attack, not in relapsing headaches.
Additional analysis revealed that the efficacy of lasmiditan is evident regardless of the presence or absence of response to prior triptan therapy, i.e. there is a presumption that lasmiditan can replace the gold standard of migraine management.
Lasmiditan outperformed placebo in a population of patients who turned to concomitant migraine preventive medications in a clinical trial.
The separate CENTURION (NCT03670810) phase 3 clinical trial (randomized, double-blind, placebo-controlled, multicenter, international) attempted to clarify the efficacy of lasmiditan in the task of controlling several consecutive migraine attacks. Reyvow did well with this.
Reyvow: Safety of Acute Treatment of Migraine With Lasmiditan
Prescribing lasmiditan may be associated with dose-dependent adverse events: dizziness (14.7% of patients; the cumulative frequency for all drug doses), paresthesia (5.7%), somnolence (5.5%), fatigue (3.8%), nausea (3.4%), muscular weakness (1.3%), and hypoesthesia (1.2%).

Lasmiditan has been found not to cause cardiovascular complications in patients with at least one cardiovascular risk factor.
Lasmiditan has been tested with the driving performance which has been evaluated using a validated threshold established in a population with blood alcohol concentration of 0.05%. A dose-dependent impairment of computer-based simulated driving performance was seen with all doses of lasmiditan at 90 minutes after administration. However, lasmiditan had no significant effect on driving performance after 8 hours or later after administration of it in doses of 100 or 200 mg. Driving for at least 8 hours after taking Reyvow is not recommended, and there is no objective way for patients to self-report how much the drug may have affected their driving skills.
Reyvow: Outlook on Lasmiditan
The therapeutic efficacy of lasmiditan and triptans is broadly identical: as measured by pain relief as the proportion of patients whose headaches went from moderate-to-severe to mild or disappeared completely within two hours of taking the drug.

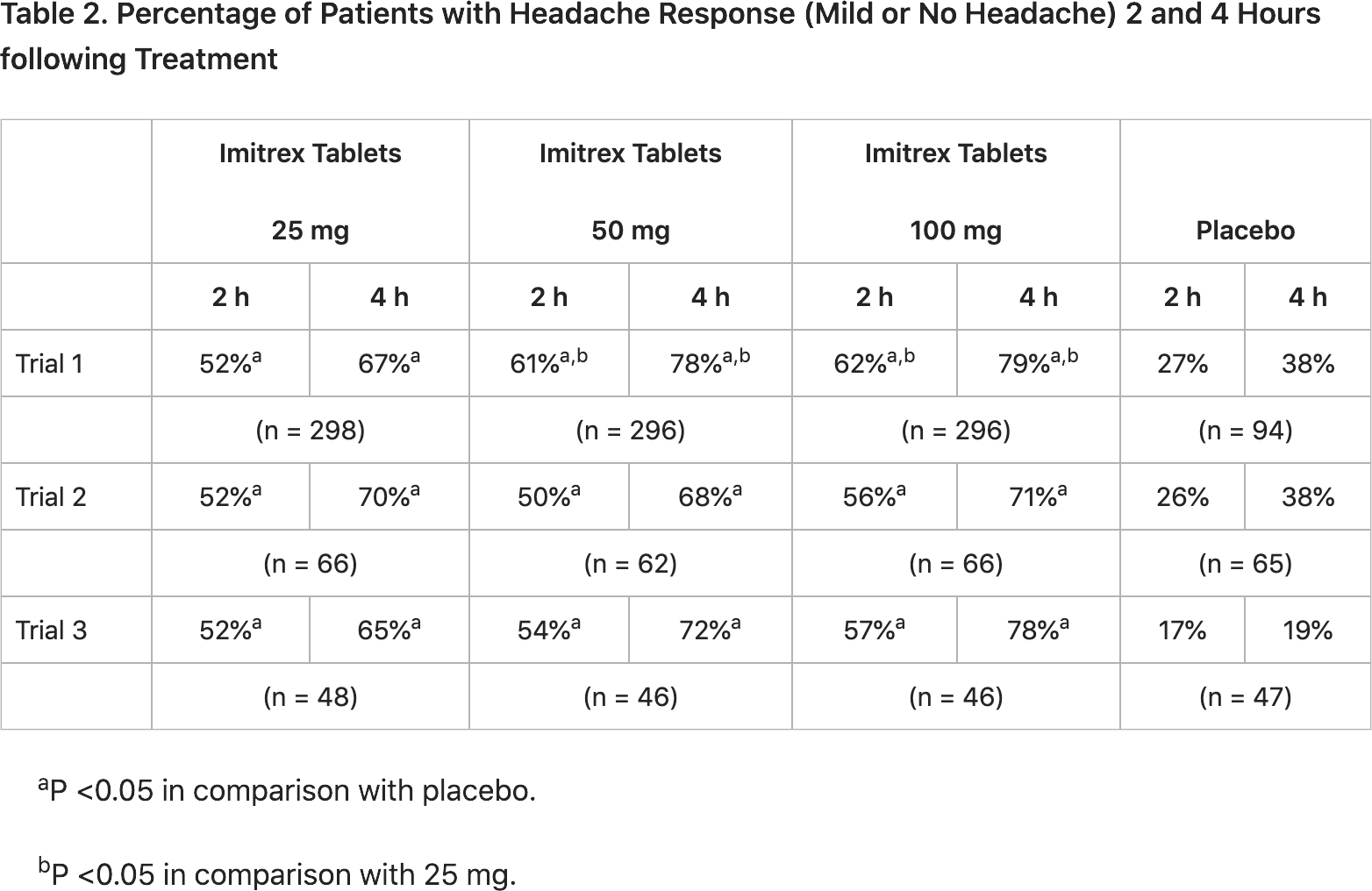
For reference purposes, here are the corresponding results of clinical trials of all seven triptans circulating on the world pharmaceutical market: sumatriptan, zolmitriptan, naratriptan, rizatriptan, almotriptan, eletriptan, frovatriptan.

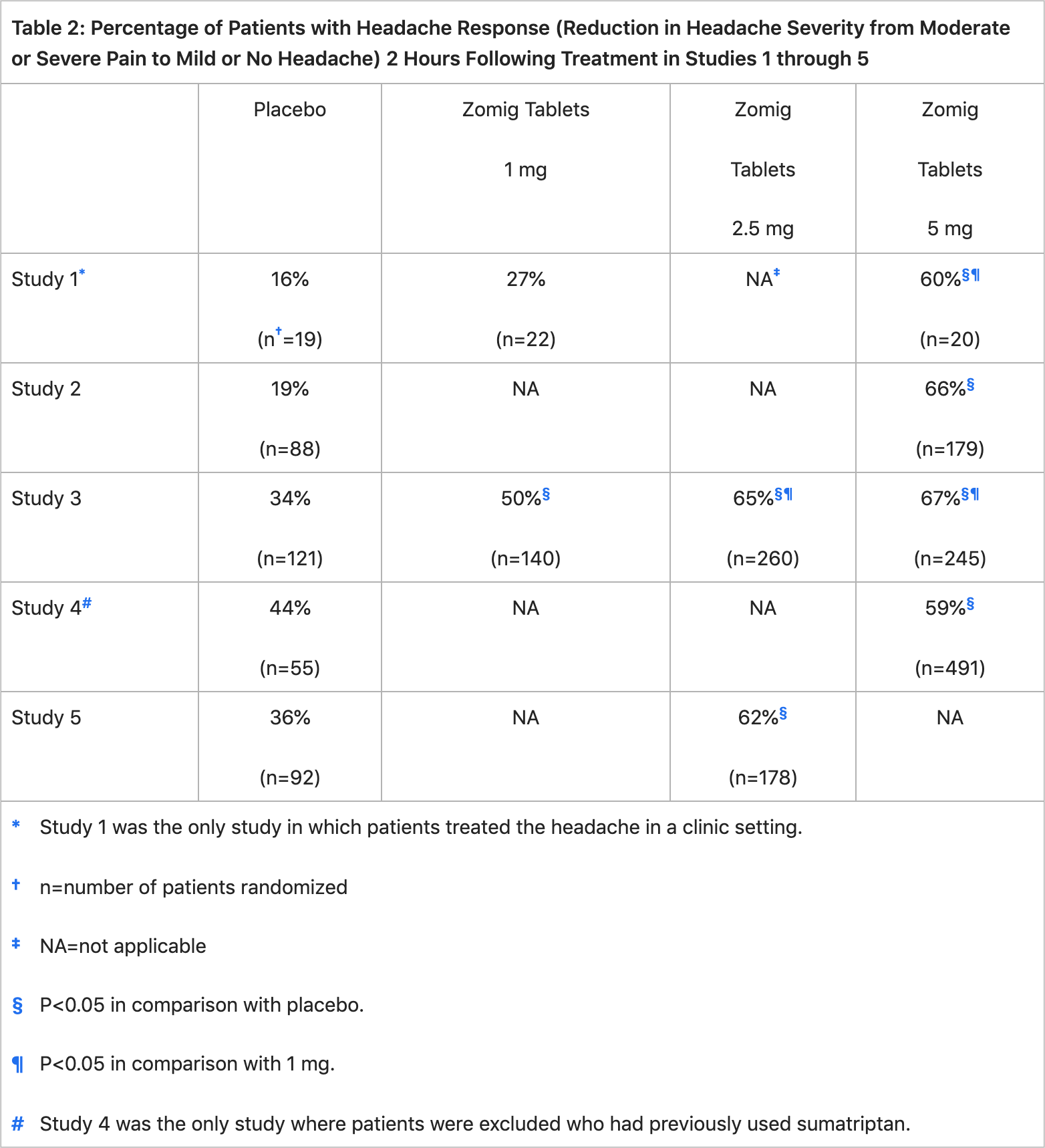
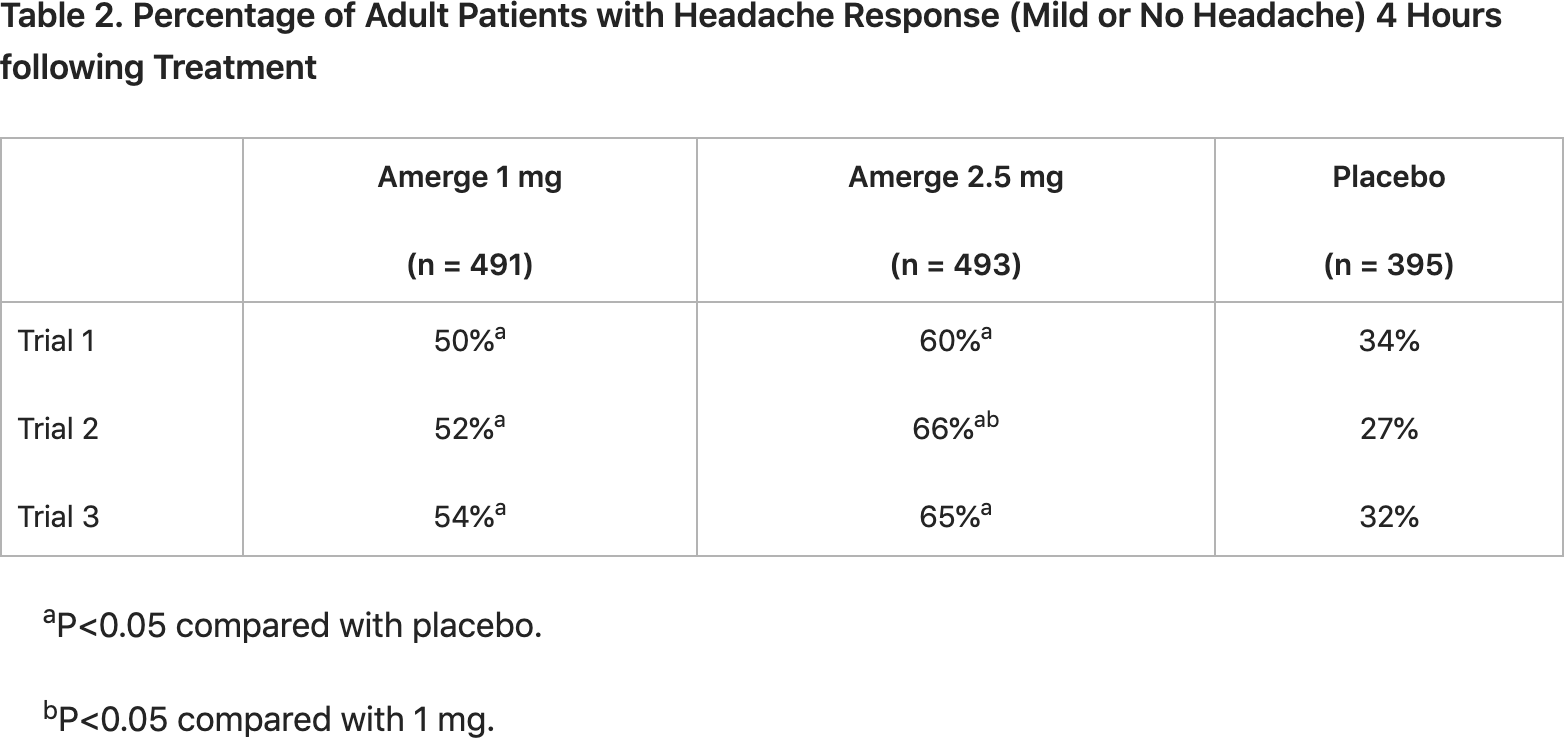
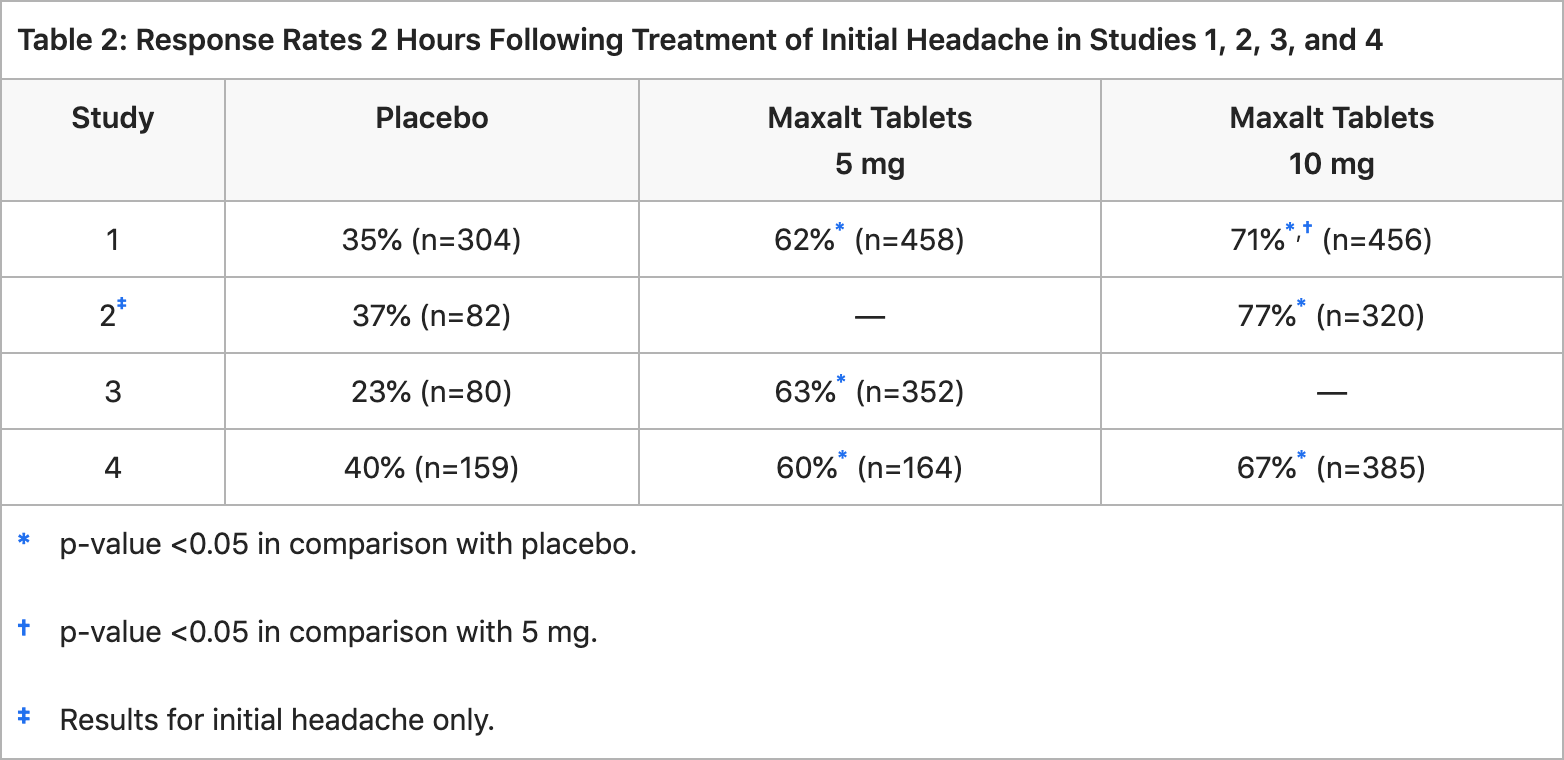
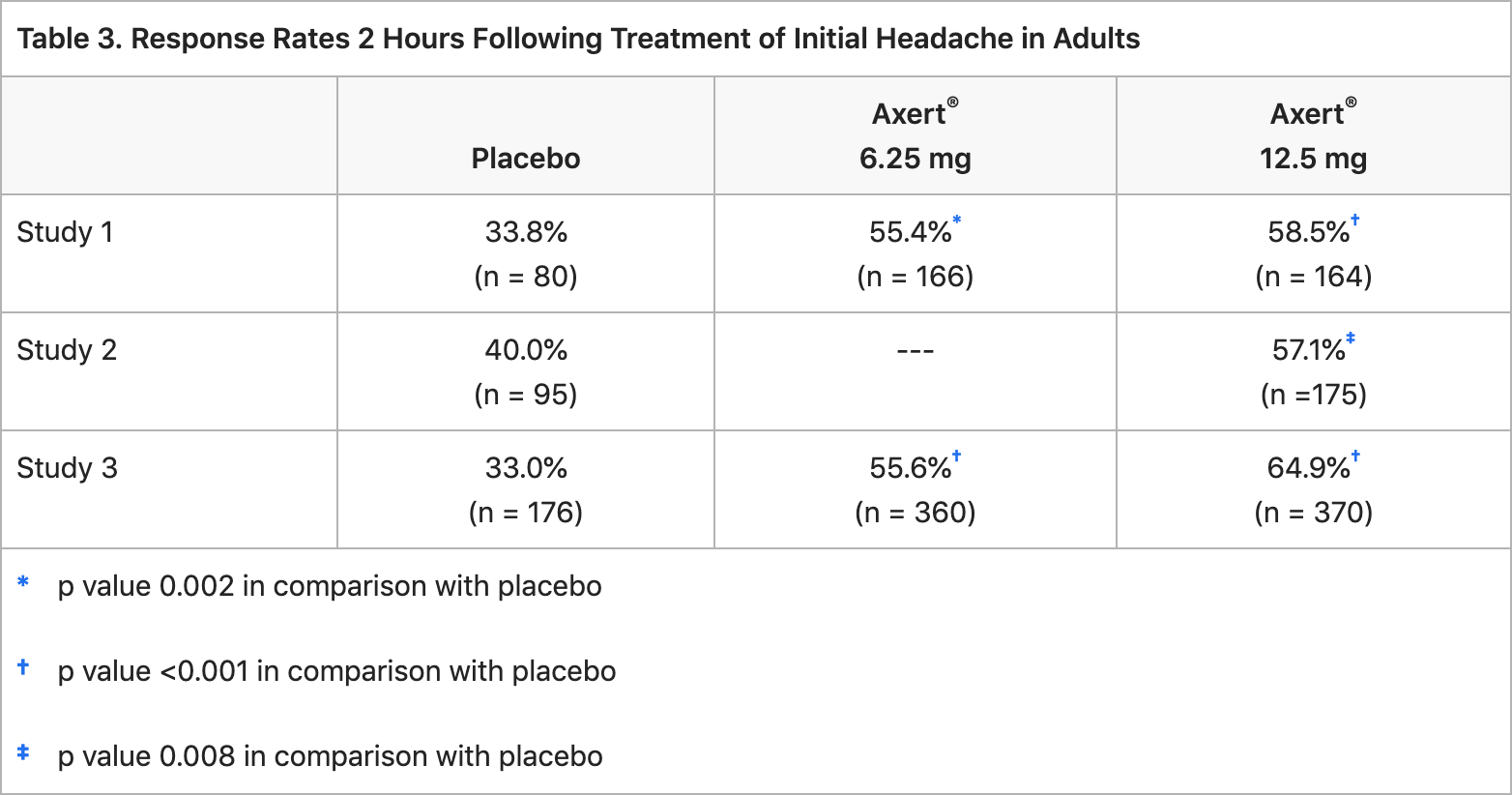
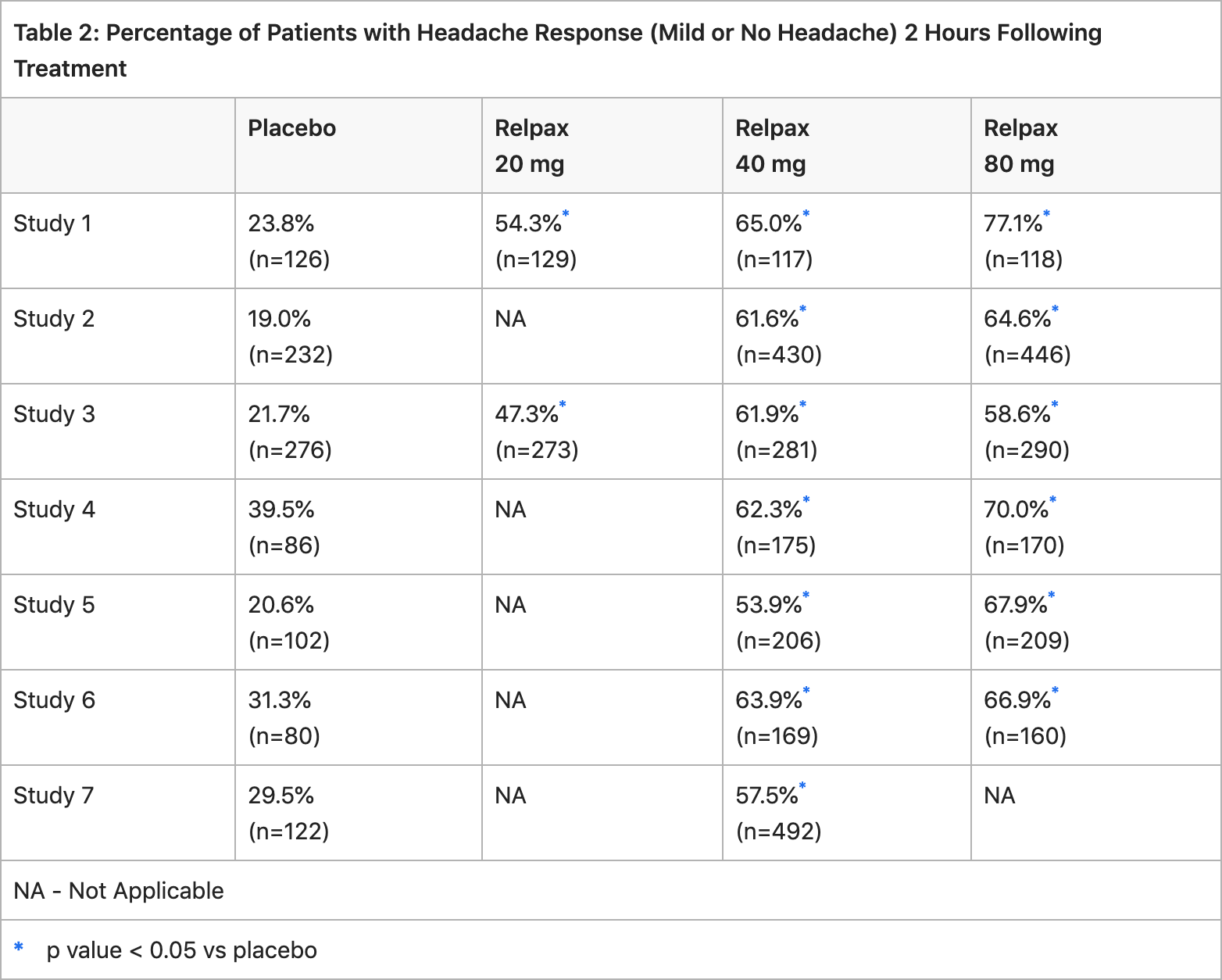
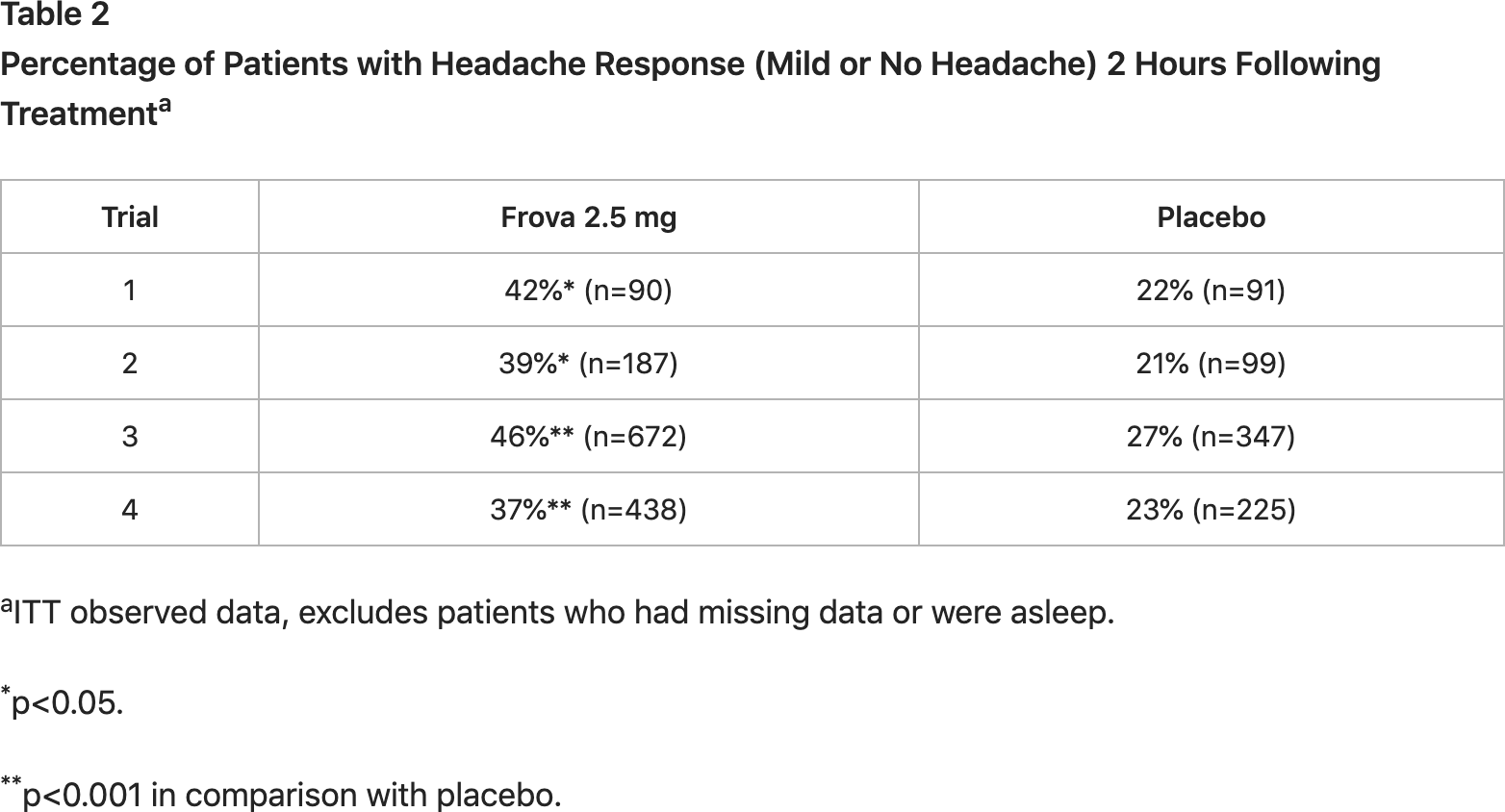
Sumatriptan (Imitrex, Imitrex Statdose, Imitrex Nasal, Tosymra, Onzetra Xsail, Sumavel DosePro, Zembrace SymTouch, Imigran): effectiveness of pain relief in the acute treatment of migraine. Zolmitriptan (Zomig, Zomig-ZMT, Zomig Nasal Spray): effectiveness of pain relief in the acute treatment of migraine. Naratriptan (Amerge, Naramig): effectiveness of pain relief in the acute treatment of migraine. Rizatriptan (Maxalt, Maxalt-MLT): effectiveness of pain relief in the acute treatment of migraine. Almotriptan (Axert): effectiveness of pain relief in the acute treatment of migraine. Eletriptan (Relpax): effectiveness of pain relief in the acute treatment of migraine. Frovatriptan (Frova): effectiveness of pain relief in the acute treatment of migraine.
In January 2017, Eli Lilly shelled out $960 million to acquire CoLucid Pharmaceuticals, the company behind the development of lasmiditan. Curiously, the molecule was discovered by Eli Lilly itself and then sold to CoLucid in 2005. At the time, pain therapy was not the focus of the American pharmaceutical giant, but after the reorganization of research projects, it became highly relevant. Given the safety profile of Reyvow, which has no vasoconstrictor effect, its commercial prospects are ambitious, as migraine suffers more than a billion people on Earth.
Oral Reyvow will organically complement injectable Emgality (galcanezumab), a monoclonal antibody against the calcitonin gene-related peptide (CGRP) used for preventive treatment of migraine in adults.
Emgality, for which Eli Lilly received FDA approval in September 2018, was the third antimigraine drug in the class of injectable CGRP blockers which are used in the task of preventing migraine attacks. First, Aimovig (erenumab) by Amgen and Novartis appeared in May 2018. Then, in September 2018, Ajovy (fremanezumab) by Teva Pharmaceutical Industries saw the light of day. Finally, in February 2020, Vyepti (eptinezumab) by Alder Biopharmaceuticals, which was taken over by Denmark’s Lundbeck for $1.95 billion, was launched.
In June 2019, Emgality expanded its list of indications by adding treatment of episodic cluster headache in adults.
Meanwhile, in December 2019 and February 2020, respectively, Allergan and Biohaven Pharmaceuticals received regulatory approvals for the oral CGRP blockers Ubrelvy (ubrogepant) and Nurtec ODT (rimegepant) for the acute treatment of migraine with or without aura. When comparing the results of late-stage clinical trials, the efficacy of ubrogepant and rimegepant is still inferior to lasmiditan. On the other hand, they, being in the gepant class, are characterized by a lower number of adverse events.
For reference purposes, let us compare the outcomes of clinical trials of lasmiditan, ubrogepant and rimegepant in terms of complete relief from headache after 2 hours of taking the drug. It should be understood that any such comparisons are not methodologically valid because neither different classes of drugs nor different patient populations can be directly compared. Nevertheless, since lasmiditan, ubrogepant and rimegepant are new and oral antimigraine drugs, it is still useful to clarify their effectiveness in a more descriptive tabular view.
Therapeutic efficacy of antimigraine drugs lasmiditan, ubrogepant, and rimegepant in headache getting rid task: cross-trial phase 3 comparison
| % of patients total pain-free after 2 hours, placebo-adjusted | ||||||
|---|---|---|---|---|---|---|
| Eli Lilly | lasmiditan 50 mg | lasmiditan 100 mg | lasmiditan 200 mg | |||
| SAMURAI (NCT02439320) | — | 12.9 (p<0.001) | 16.9 (p<0.001) | |||
| SPARTAN (NCT02605174) | 7.3 (p=0.003) | 10.1 (p<0.001) | 17.5 (p<0.001) | |||
| CENTURION (NCT03670810) | — | 17.4 (p<0.001) | 20.9 (p<0.001) | |||
| Allergan/AbbVie | ubrogepant 25 mg | ubrogepant 50 mg | ubrogepant 100 mg | |||
| ACHIEVE I (NCT02828020) | — | 7.4 (p=0.002) | 9.4 (p<0.001) | |||
| ACHIEVE II (NCT02867709) | 6.4 (p=0.03) | 7.5 (p=0.01) | — | |||
| Biohaven Pharmaceuticals | rimegepant 75 mg | |||||
| BHV-3000-301 (NCT03235479) | 5.0 (p=0.03) | |||||
| BHV-3000-302 (NCT03237845) | 7.6 (p<0.001) | |||||
| BHV-3000-303 (NCT03461757) | 10.3 (p<0.001) | |||||
There is an opinion that gepants will be the drugs of choice for those for whom triptans are contraindicated or they have stopped working, while ditans will be used either when gepants fail or at night, when there is no need to interact with complex technical equipment. Again, a cumulative effect has been noted with gepants; prolonged administration reduces the frequency of subsequent migraine attacks. In addition, preliminary data suggest that co-prescribing oral and injectable CGRP blockers is reasonable.
Biohaven intends to obtain regulatory approval for the use of rimegepant for the preventive treatment of migraine; it has successfully completed the appropriate clinical trial and awaiting FDA’s decision.
AbbVie, which now owns Allergan, has already submitted a New Drug Application (NDA) to FDA for atogepant, an oral CGRP blocker, for the preventive treatment of migraine.
Biohaven is also developing zavegepant (BHV-3500, formerly vazegepant), a CGRP blocker in the form of an intranasal spray, focusing on acute treatment and preventive treatment of migraine. Zavegepant is said to be characterized by the accelerated achievement of targeted therapeutic exposures with significantly earlier time to maximal concentration. In parallel, zavegepant, made in oral formulation, is tested for preventive treatment for migraine.
Extras
Reyvow (lasmiditan). Prescribing information. US. [PDF]