Highlights
Lyfnua (gefapixant) is the first drug indicated to treat refractory chronic cough (RCC) or unexplained chronic cough (UCC).
Oral Lyfnua, administered twice daily at 45 mg, focuses on the treatment of chronic cough that either persists despite appropriate therapy for the comorbidities that cause it, or when the cause of the cough cannot be identified despite careful examination.
Lyfnua, characterized by a novel mechanism of action and developed by Merck & Co., has received the world’s first regulatory approval, in Japan in January 2022. Kyorin Pharmaceutical is distributing the drug.
The U.S. Food and Drug Administration (FDA) has so far refused to give Lyfnua the green light, citing the need for more data regarding the efficacy of gefapixant. The New Drug Application (NDA) was accepted in early March 2021.
What Is Chronic Cough?
According to epidemiological studies, chronic cough (a cough that lasts more than 8 weeks) occurs in 4%–10% of adults worldwide.
No proven effective treatment for chronic cough has yet been proposed.
Major risk factors for chronic cough in individuals who have never smoked include older age, women, abdominal obesity, occupational exposure to dust or smoke, bronchial asthma, gastrointestinal reflux, upper respiratory cough syndrome, and bronchiectasis. Yet most patients with these conditions do not complain of a chronic cough, that is, there is a distinct pathophysiological process underlying its symptomatic features.
Although sufferers of chronic cough may benefit from treatment of comorbidities, in about half of the cases it finds no relief, acquiring refractory status. Some patients with chronic cough have no underlying disease at all — such a cough, called an unexplained cough, is referred to as a pathology with unclear etiology.
Refractory chronic cough, which does not serve as an airway defense mechanism like a physiological cough, makes you cough 10-100 times an hour for no apparent reason. This severely impairs the quality of life by disrupting patients’ daily and social activities and dramatically affecting its physical (stress urinary incontinence, sleep disturbance, chest pain) and psychological aspects (frustration, anxiety, depression). In many cases, the disease is accompanied by prolonged empirical and usually ineffective treatment, and the time to diagnosis usually exceeds 8 years.
In the treatment of refractory or unexplained chronic cough caused by cough hypersensitivity syndrome that impairs sensory neuronal function, medical interventions aimed at reducing hyperexcited neural pathways, such as morphine, gabapentin, amitriptyline, behavioral therapy may help.

Lyfnua: Efficacy and Safety of Gefapixant in Treatment of Chronic Cough
The COUGH-1 (NCT03449134) and COUGH-2 (NCT03449147) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trials invited adult patients (n=2044) with chronic cough, refractory or unexplained
Among the main inclusion criteria: absence of any lung abnormality contributing to chronic cough; duration of the latter for at least one year.
Among the main characteristics of the subjects: 75% female, mean age 58 years, mean duration of cough of 11 years.
Participants received oral gefapixant twice daily at a dose of 45 mg or 15 mg or placebo.
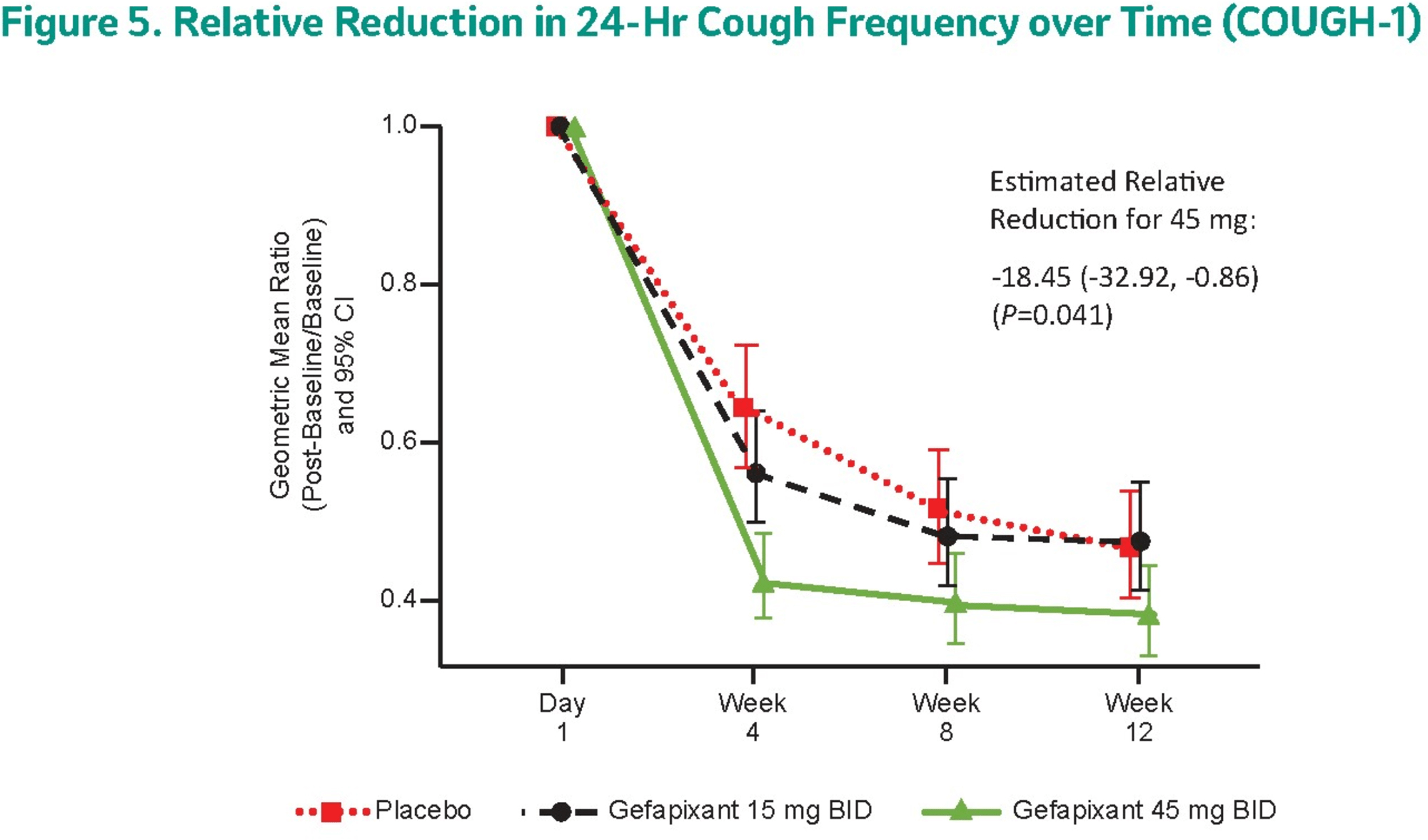
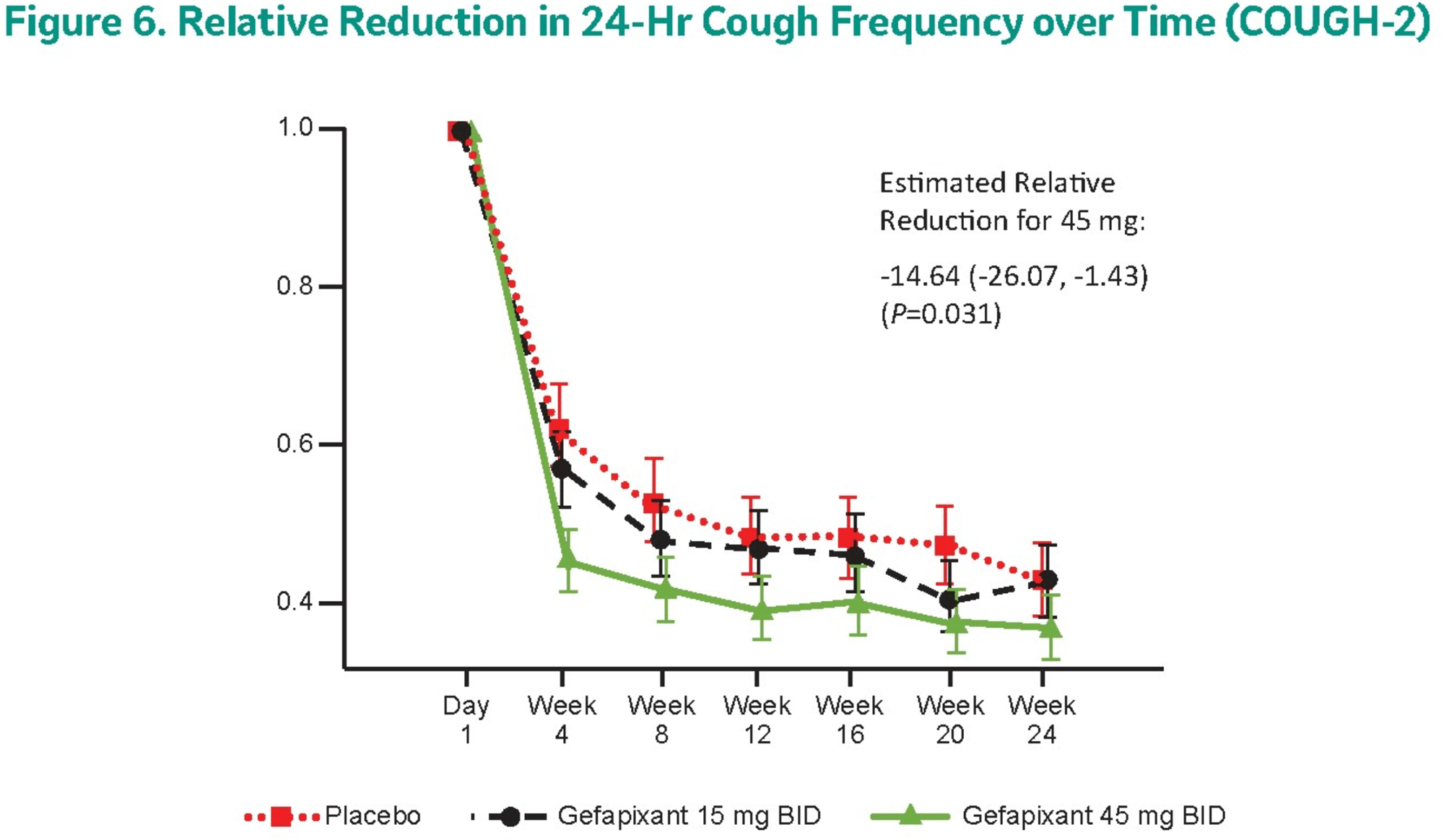
The primary endpoint of treatment efficacy was cough frequency over a 24-hour period (assessed objectively by audio recording the number of coughing events per hour) after 12 and 24 weeks of therapy, respectively, in the first and second trials.
The 45-mg gefapixant groups demonstrated a reduction in the indicated cough frequency, which decreased by a mean of 62% and 63% relative to baseline in COUGH-1 and COUGH-2 trials, respectively. In terms of reductions compared to the placebo groups, cough frequency was reduced by a statistically significant 18.5% (95% CI: −32.9 to −0.9) [p=0.041] and 14.6% (95% CI: −26.1 to −1.4) [p=0.031].
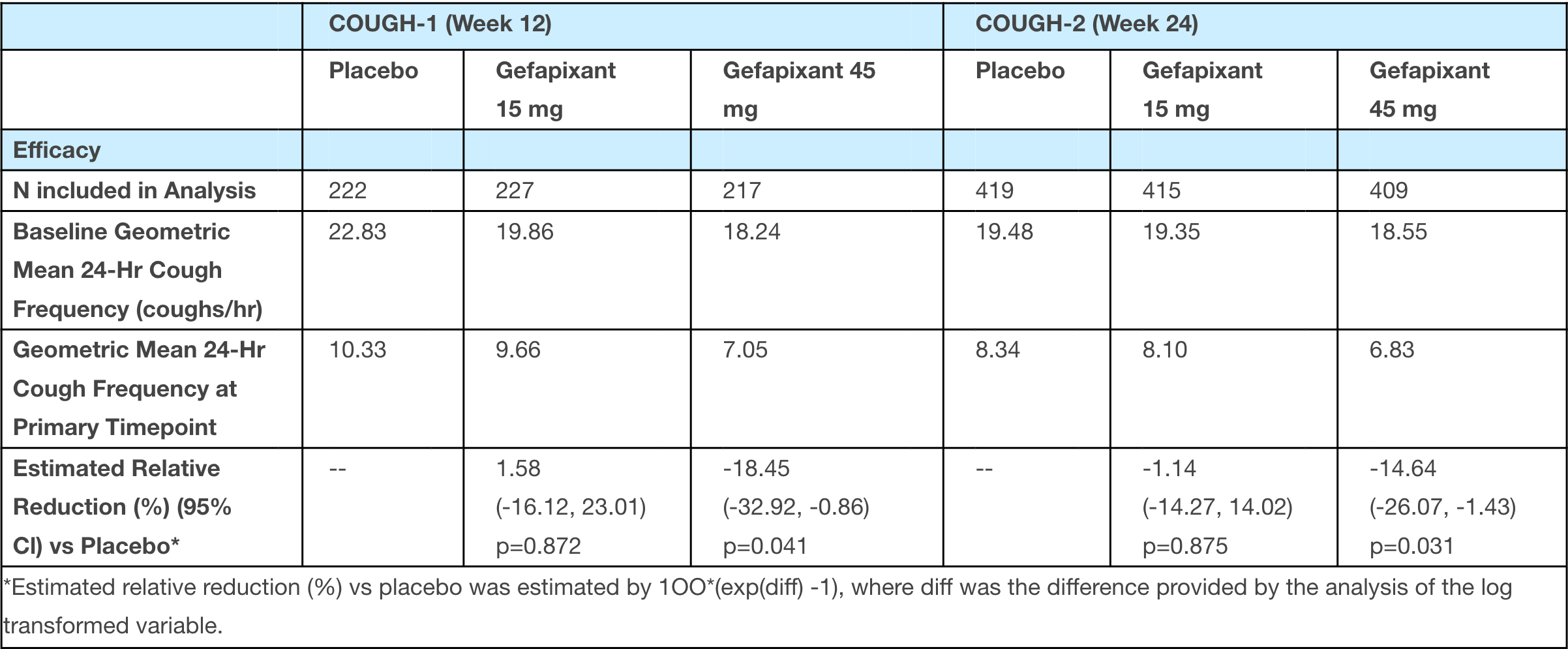
Administration of a 15-mg dose of gefapixant did not result in an exit to the primary endpoint.
Experimental treatment with gefapixant at the 45-mg dose provided a 17.7% (95% CI: −32.6 to −0.5) [p=0.056] and 15.8% (95% CI: −27.3 to −2.5) [p=0.022] reduction in cough frequency immediately after awakening relative to placebo.
After 24-week therapy with the 45-mg gefapixant, significantly more patients than in the placebo group reported a clinically significant improvement in cough-related quality of life: odds ratio 1.4 (p=0.042). According to the Leicester Cough Questionnaire (LCQ), 77% of those receiving gefapixant had an overall score increase of more than 1.3 points from baseline.
The primary adverse reaction to gefapixant administration was a dose-dependent change in taste sensation of mild-to-moderate severity, experienced by 58% and 69% of the COUGH-1 and COUGH-2 patients receiving the 45-mg dose, and 11% and 20% in the 15-mg dose, and 3% and 8% in the placebo groups.
Adverse events resulted in discontinuation of treatment among 15% and 20% of patients who received the 45-mg dose of gefapixant, 3% and 8% in the 15-mg dose, and 3% and 5% in the placebo groups.
Lyfnua: Mechanism of Action of Gefapixant
Small-molecule oral gefapixant (MK-7264, AF-219, RO-4926219) is a nonnarcotic reversible allosteric antagonist of the P2X3 and P2X2/3 receptors.
The purinergic P2X3 receptor is an ATP-dependent ion channel located predominantly on peripheral sensory nerves and expressed on fibers innervating the airway. P2X3 receptors play, it is believed, a key role in sensitization of sensory nerves, especially type C nerves (sympathetic, postganglionic, afferent).
When the airways become inflamed, irritated, mechanically stressed, or damaged, the cells lining them release ATP (and other chemical stimuli) in high concentrations. Binding of extracellular ATP to P2X3 receptors on C fibers triggers signaling indicating possible damage, which creates an action potential manifested by the cough reflex. Gefapixant selectively blocks the binding of extracellular ATP in P2X3 channels, thereby inhibiting coughing.
In vivo, gefapixant has demonstrated efficacy comparable to naproxen in models of inflammatory and osteoarthritic sensitization and gabapentin in models of neuropathic sensitization.
Merck & Co. acquired gefapixant after buying Afferent Pharmaceuticals in 2016. The deal cost an upfront $500 million in cash, plus potentially up to $750 million as certain development and commercialization milestones are reached. Afferent was founded in 2009 after licensing the P2X3 receptor program from Roche, then under study in the chronic pain treatment task.
Gefapixant Against Chronic Cough: Expert Comments
Gefapixant has not shown particularly impressive results. Yes, a percentage reduction in cough frequency might seem acceptable, but based on absolute results, this is not the case.
And so regulators, as with the FDA, are taking a hard look at the entire set of clinical data collected. Again, P2X3 receptor antagonists being developed by other pharma manufacturers are similarly showing modest efficacy. But pharma companies are not giving up, because, first, regulators will hopefully show leniency, as in the case of Japan, due to the lack of approved treatments for chronic cough, and, second, drugs in this class will easily reach blockbuster levels.
It should be understood that the placebo control groups in the COUGH-1 and COUGH-2 clinical trials showed very strong cough relief, so it is possible that either gefapixant really works and therefore managed to overcome the high placebo barrier, or, conversely, the latter was the cause of most of the drug’s positive effects. Indeed, a prior clinical trial NCT02612610 phase 2b showed a decent 38% reduction in cough frequency relative to placebo after 12 weeks of therapy with 50-mg gefapixant twice a day.
The therapeutic effect of gefapixant appears to wane over time; this is suggested by the fact that the results of the 6-month COUGH-2 were worse than those of the 3-month COUGH-1.
The safety profile of gefapixant is not entirely acceptable, although a marked change in taste in exchange for cough relief can be tolerated.
Merck & Co. continues to study gefapixant in the treatment of conditions such as idiopathic pulmonary fibrosis (IPF) with persistent cough, cough-induced stress urinary incontinence (SUI) in women, recent onset chronic cough (lasting no longer than one year).
Gefapixant for Chronic Cough: Competitive Landscape
Bellus Health
BLU-5937, an experimental P2X3 receptor antagonist by Canada’s Bellus Health, has generally failed in the treatment of refractory chronic cough, although the molecule is characterized by 1500-fold selectivity to P2X3 relative to P2X2/3; with gefapixant this figure lies in the 3–7-fold range. The failure of the RELIEF (NCT03979638) phase 2 clinical trial, essentially due to the selection of a poor primary efficacy endpoint, did not prevent Bellus from launching another clinical trial.
In the SOOTHE (NCT04678206) phase 2b clinical trial, administration of BLU-5937 at a dose of 50 or 200 mg twice daily resulted in a 34% reduction in daily cough frequency relative to placebo (p=0.003 and p=0.005) after 4 weeks of treatment. A small proportion of participants experienced a change in taste sensation: 6.5% and 4.8%, respectively.
Bellus intends to set up a phase 3 pivotal clinical trial of BLU-5937 in the second half of 2022.
Bayer
Eliapixant (BAY1817080), Bayer’s experimental P2X3 receptor antagonist, provided a relative 25% reduction in cough frequency — though for the highest 750-mg dose twice daily in a 7-day phase 1/2a clinical trial NCT03310645, modest in patient coverage. That said, the administration of the drug was accompanied by apparent adverse reactions in the form of changes in taste.
In a subsequent PAGANINI (NCT04562155) phase 2b clinical trial, administration of eliapixant at a dose of 75 mg twice daily reduced cough frequency by 27% relative to placebo after 12 weeks of treatment.
In parallel, eliapixant is being studied in the treatment of overactive bladder, neuropathic pain, and endometriosis.
Shionogi & Co.
Sivopixant (S-600918), an experimental P2X3 receptor antagonist from Japan’s Shionogi & Co., administered once daily, did not lead to a statistically significant difference in cough frequency during the day from placebo, although it did so by a relative 32% (p=0.0546) in a narrow 2-week phase 2a clinical trial. However, sivopixant managed to reduce it in a statistically significant way (p=0.0386) by 31% relative to placebo when considering the entire 24-hour interval. Changes in taste sensation were noted for 6.5% of participants.
In a follow-up 4-week NCT04110054 phase 2b clinical trial, sivopixant in a 300-mg dose reduced cough frequency by more than 60% absolute and 12.5% relative over a 24-hour period, but again without statistical significance (p=0.3241). A retrospective analysis found that in the subgroup of patients whose cough frequency was at least 10 times per hour, the relative reduction came out to 22.9%.
As a result, it was decided to launch a phase 3 clinical trial to, first, clarify the optimal dose of sivopixant and, second, to counterbalance the strong results in the placebo group.
Sivopixant is also being tested in the treatment of sleep apnea syndrome, neuropathic pain.
Extras
The discovery and development of gefapixant. Auton Neurosci. 2021 Nov;235:102859. [source]
Treatment of persistent cough in subjects with idiopathic pulmonary fibrosis (IPF) with gefapixant, a P2X3 antagonist, in a randomized, placebo-controlled clinical trial. Pulm Ther. 2021 Dec;7(2):471-486. [source]
Safety and efficacy of gefapixant, a novel drug for the treatment of chronic cough: A systematic review and meta-analysis of randomized controlled trials. Ann Thorac Med. Apr-Jun 2021;16(2):127-140. [source]
Coming soon: the first-ever drug(s) for refractory chronic cough. Lung. 2021 Apr;199(2):83-84. [source]
Characterization of patients with refractory or unexplained chronic cough participating in a phase 2 clinical trial of the P2X3-receptor antagonist gefapixant. Lung. 2021 Apr;199(2):121-129. [source]
Design and rationale of two phase 3 randomised controlled trials (COUGH-1 and COUGH-2) of gefapixant, a P2X3 receptor antagonist, in refractory or unexplained chronic cough. ERJ Open Res. 2020 Nov 2;6(4):00284-2020. [source]
P2X3-receptor antagonists as potential antitussives: Summary of current clinical trials in chronic cough. Lung. 2020 Aug;198(4):609-616. [source]
Gefapixant, a P2X3 receptor antagonist, for the treatment of refractory or unexplained chronic cough: a randomised, double-blind, controlled, parallel-group, phase 2b trial. Lancet Respir Med. 2020 Aug;8(8):775-785. [source]
Gefapixant in two randomised dose-escalation studies in chronic cough. Eur Respir J. 2020 Mar 20;55(3):1901615. [source]
The effect of gefapixant, a P2X3 antagonist, on cough reflex sensitivity: a randomised placebo-controlled study. Eur Respir J. 2019 Jul 4;54(1):1900439. [source]
Action of MK-7264 (gefapixant) at human P2X3 and P2X2/3 receptors and in vivo efficacy in models of sensitisation. Br J Pharmacol. 2019 Jul;176(13):2279-2291. [source]
BLU-5937: A selective P2X3 antagonist with potent anti-tussive effect and no taste alteration. Pulm Pharmacol Ther. 2019 Jun;56:56-62. [source]
Eliapixant (BAY 1817080), a P2X3 receptor antagonist, in refractory chronic cough: a randomised, placebo-controlled, crossover phase 2a study. Eur Respir J. 2021 Nov 18;58(5):2004240. [source]
Randomised trial of the P2X3 receptor antagonist sivopixant for refractory chronic cough. Eur Respir J. 2021 Oct 14;2100725. [source]