Highlights
Welireg (belzutifan) is a new drug indicated for the treatment of adult patients with Von Hippel–Lindau disease (VHL) who require therapy for associated renal cell carcinoma (RCC), central nervous system hemangioblastomas, or pancreatic neuroendocrine tumors (pNET), not requiring immediate surgery.
Welireg developed by Merck & Co. is approved by the U.S. Food and Drug Administration (FDA) in mid-August 2021.
Belzutifan has added to the still scarce and nonspecific pharmacological armamentarium for fighting tumors associated with Von Hippel–Lindau disease.
What Is Von Hippel–Lindau Disease
Von Hippel–Lindau disease (VHL) is a neoplastic disease characterized by visceral cysts and benign tumors that affect the central nervous system (CNS), kidneys, adrenal glands, pancreas, and reproductive organs and that can transform into malignancy.
Von Hippel–Lindau disease, also known as Von Hippel–Lindau syndrome, is a rare (1 in 36,000) genetic disorder and a type of phakomatosis that results from a mutation in the Von Hippel–Lindau tumor suppressor gene (VHL).
Von Hippel–Lindau disease is classified into two general types based on the risk of developing renal cell carcinoma and pheochromocytoma.
Fatal outcome is usually due to complications of renal cell carcinoma and/or CNS tumors.
Treatment of Von Hippel–Lindau disease involves early detection and removal of tumors to prevent or minimize impairments such as loss of hearing or vision, neurological symptoms, and the need for renal replacement therapy, as well as to prevent tumor metastasis.
Drugs are prescribed in the following cases: retinal hemangioblastoma — vascular endothelial growth factor (VEGF) inhibitors; pheochromocytoma or clear cell renal cell carcinoma (ccRCC) — tyrosine kinase inhibitors. Radiation therapy is indicated for CNS tumors, retinal hemangioblastoma, endolymphatic sac tumors.
Welireg: Mechanism of Action of Belzutifan
Small-molecule oral belzutifan (MK-6482, PT2977) is an inhibitor of hypoxia-inducible factor 2-alpha (HIF-2α), a transcription factor involved in oxygen sensitivity processes by regulating genes that promote adaptation to hypoxia.
Under normal physiological conditions, when oxygen is sufficient (normoxia), HIF-2α is inactive and is degraded by prolyl hydroxylases (PHD) and the ubiquitin-proteasome system. In case of hypoxia, HIF-2α is not degraded, which is manifested by its enhanced transcriptional function leading to the expression of hundreds of different genes responsible for anaerobic metabolism, angiogenesis, cell proliferation and survival, evasion of immunological surveillance, remodeling of extracellular matrix, pH homeostasis, amino acid and nucleotide metabolism, and genomic stability among other things.
In certain pathologies (even under conditions of normal oxygenation), the transcriptional mechanisms of HIF-2α are disrupted, determining enhanced blood vessel growth and cell proliferation. For example, in more than 90% of cases of clear cell renal cell carcinoma (the most common type of kidney cancer), inactivation of in the Von Hippel–Lindau tumor suppressor (VHL) as a component of the ubiquitin-proteasome system is observed, resulting in stabilization and accumulation of HIF-2α, which, by translocating into the nucleus and heterodimerizing with the hypoxia-inducible factor 1-beta (HIF-1β), activates the transcription of genes related to tumor progression (angiogenesis, cell proliferation, tumor growth) such as VEGFA, CCND1, CXCR4, TGFA. Activation of HIF-2α also stimulates immunosuppressive mechanisms in the tumor microenvironment by polarizing components of the innate immune system from myeloid progenitor cells — to a prooncogenic phenotype.
Belzutifan binds to HIF-2α to block the interaction between HIF-2α and HIF-1β under conditions of hypoxia or when the VHL protein is disrupted. This is reflected by decreased transcription and expression of HIF-2α target genes. In vivo belzutifan demonstrated antitumor activity in murine renal cell carcinoma xenografts.
Welireg: Efficacy and Safety of Belzutifan
The NCT03401788 phase 2 (nonrandomized, open-label, multicenter, international) clinical trial enrolled adult patients (n=61) with Von Hippel–Lindau disease and at least one tumor related to renal cell carcinoma. Subjects could also have tumors associated with Von Hippel–Lindau disease localized outside the kidneys, including central nervous system (CNS) hemangioblastomas and pancreatic neuroendocrine tumors.
Among the exclusion criteria: prior antitumor systemic therapy, metastatic disease.
The main patient characteristics were as follows: median age 41 years (19–66), 53% male, median diameter of renal cell lesions 2.2 cm (1.0–6.1), median time from cancer diagnosis to treatment initiation 17.9 months (2.8–96.7), 77% had previously undergone renal cell carcinoma surgery.
Participants were prescribed belzutifan daily until disease progression or unacceptable toxicity.
After a median of 21.8 months (20.2–30.1) of treatment, 88.5% of patients continued on belzutifan therapy.
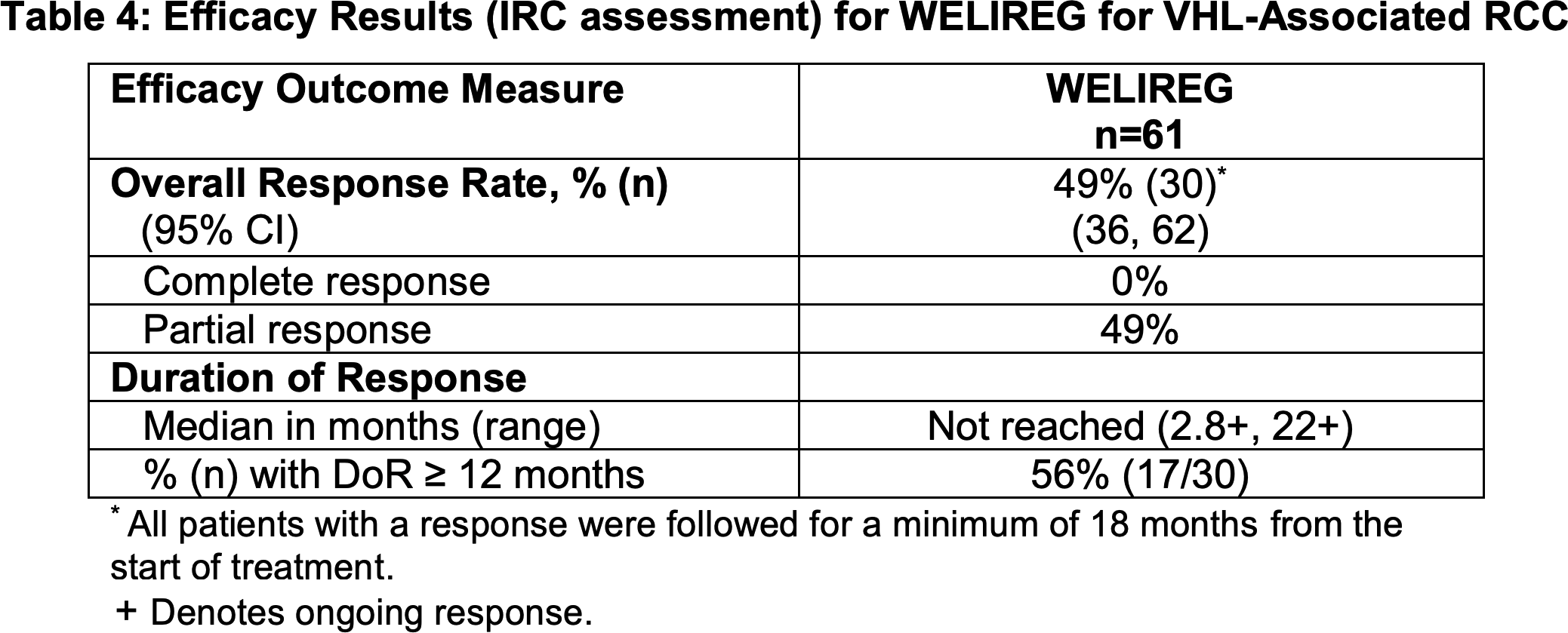
In renal cell carcinoma due to Von Hippel–Lindau disease, administration of Welireg brought the overall response rate (ORR) to 49% (95% CI: 36–62); all responses were partial (PR). Disease stabilization (SD) was recorded in 49% of patients.
Duration of response (DoR) to therapy was not achieved: NR (2.8+ to 22.3+), with 56% having a response lasting 12 months or longer.
Time to response (TTR) was 8.2 months (2.7–19.1).
Tumor size reduction was demonstrated in 92% of patients (n=56/61).
No median progression-free survival (PFS) was achieved, with a 12-month PFS rate of 98.3% and a 24-month rate of 96.5%.
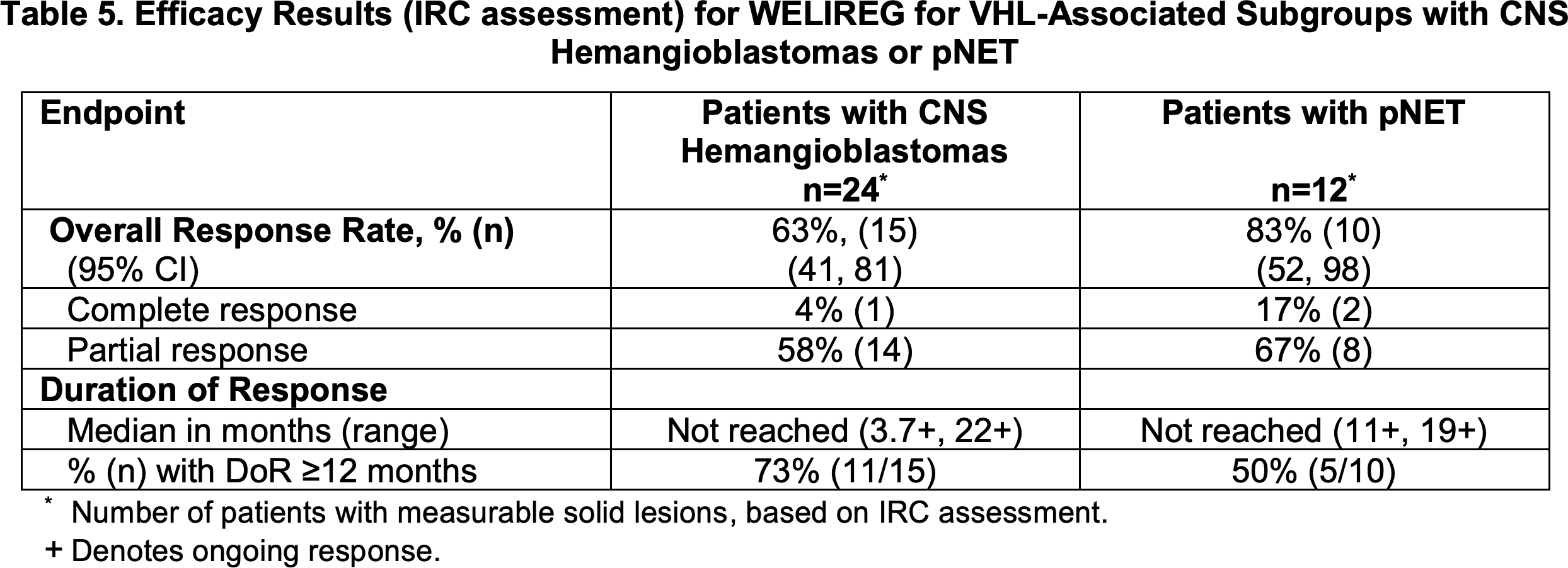
Subjects with CNS hemangioblastomas (n=24) or pancreatic neuroendocrine tumors (n=12) gave the following efficacy rates for treatment with belzutifan, respectively:
- ORR: 63% (95% CI: 41–81) [4% CR, 58% PR] and 83% (95% CI: 52–98) [17% CR, 67% PR];
- DoR: NR (3,7+ to 22+) and NR (11+ to 19+);
- DoR at 12 months or longer: in 73% and 50% of patients;
- TTR: 3.1 months (2.5–11) and 8.1 months (2.7–11).
Prescribing information for Welireg has a black box warning about the risks of fetal toxicity, and therefore the drug should not be prescribed to pregnant women. During treatment, non-hormonal contraception should be used; some hormonal contraceptives lose their effectiveness with belzutifan.
Among the most common adverse reactions to Welireg: decreased hemoglobin (93% of patients), anemia (90%), fatigue (64%), increased creatinine (64%), headache (39%), dizziness (38%), increased glucose (34%), and nausea (31%).
Anemia and hypoxia may be severe, and therefore, if clinically justified, transfusions are recommended. The use of erythropoiesis-stimulating agents (ESAs) is not recommended.
Because of adverse reactions, 3.3% of patients discontinued treatment, 39% temporarily interrupted it, and 13% reduced the dose of the drug.
Belzutifan: Market Outlook
Merck & Co. received belzutifan in its May 2019 acquisition of Peloton Therapeutics, for which it paid $1.05 billion upfront with a promise of another $1.15 billion as regulatory and commercial development milestones for experimental drug programs are reached.
According to industry forecasts, demand for belzutifan will reach $386 million per year by 2026.
Interest in belzutifan will surge if it succeeds in expanding its range of indications.
Belzutifan is undergoing extensive clinical review in the treatment of clear cell renal cell carcinoma (ccRCC), monotherapeutically and in combination with other drugs including the tyrosine kinase inhibitors Cabometyx (cabozantinib) and Lenvima (lenvatinib) and the PD-1 blocker Keytruda (pembrolizumab).
Belzutifan is also being studied in the treatment of pheochromocytoma and paraganglioma (PPGL), pancreatic neuroendocrine tumor (pNET), glioblastoma multiforme (GBM), hepatocellular carcinoma (HCC), colorectal cancer (CRC), pancreatic ductal adenocarcinoma (PDAC), and biliary tract cancer (BTC).
Extras
Welireg (belzutifan). Prescribing information. U.S. [PDF]