SUMMARY
- Personalized cancer vaccines are the future of cancer treatment.
- These vaccines are tailored to the tumor specificity of each patient and can be manufactured quickly.
- The first individualized oncovaccine adhering to the concept of precision medicine will be available in 2025.
- Successful treatment of melanoma and head and neck cancer has already been demonstrated.
- Lung, kidney, bladder and non-melanoma skin cancers are next in line.
WHAT HAPPENED
Moderna, in collaboration with Merck & Co., has developed mRNA-4157 (V940), a personalized cancer vaccine (PCV) that is tailored to each patient with a clear disease-specific focus.
Encouraging clinical outcomes have been observed for the treatment of surgically resected melanoma, surpassing standard therapy.
In addition, remarkable results have been demonstrated in the treatment of unresectable head and neck cancer. Clinical validation of therapies for lung cancer, kidney cancer, bladder cancer, and non-melanoma skin cancer is ongoing.
The mechanistic rationale for personalized cancer vaccines appears reasonable and sound. They trigger an unprecedented powerful antitumor immune response that is highly specific and takes into account the features of oncology disease of each individual patient. However, until the storm of potentially beneficial T-cell reactions turns into a stable and lasting clinical remission, there is simply no future for PCVs. And this is where dozens and hundreds of developers have broken their teeth. But Modern seems to have succeeded.
If everything goes according to plan, the individualized neoantigenic mRNA oncovaccine mRNA-4157 (V940) will receive accelerated regulatory approval in 2025.
The manufacturing and administration processes of mRNA-4157 (V940) are less complex and costly compared to chimeric antigen receptor (CAR) T-cell therapy, which has been a breakthrough in treating advanced hemato-oncological diseases.
Meanwhile, the German company BioNTech has also made significant progress. The personalized cancer mRNA vaccine, autogene cevumeran, is being investigated jointly with Genentech at Roche and has shown promising results in treating pancreatic cancer.

Autogene Cevumeran: Powerful mRNA Vaccine Against Pancreatic Cancer
Personalized immunotherapy prolonged life in one-third of patients with pancreatic ductal adenocarcinoma.
MECHANISM OF ACTION
mRNA-4157 (V940) is a personalized cancer vaccine (PCV) designed to improve the effectiveness of cancer treatment through the concept of precision medicine.
Neoantigens — antigens encoded by mutant genes specific for cancer cells in these neoplasms which are developing and progressing mutate obligatorily — are isolated from tumors and blood samples of the patient. The oncovaccine contains both epitopes of neoantigens, which were discovered during ex vivo experiments on the patient’s immune cells, and epitopes of neoantigens from the whole exome, which, according to predictive bioinformatics algorithm, are immunogenic, i.e. capable of triggering beneficial immunostimulatory reactions in the organism.
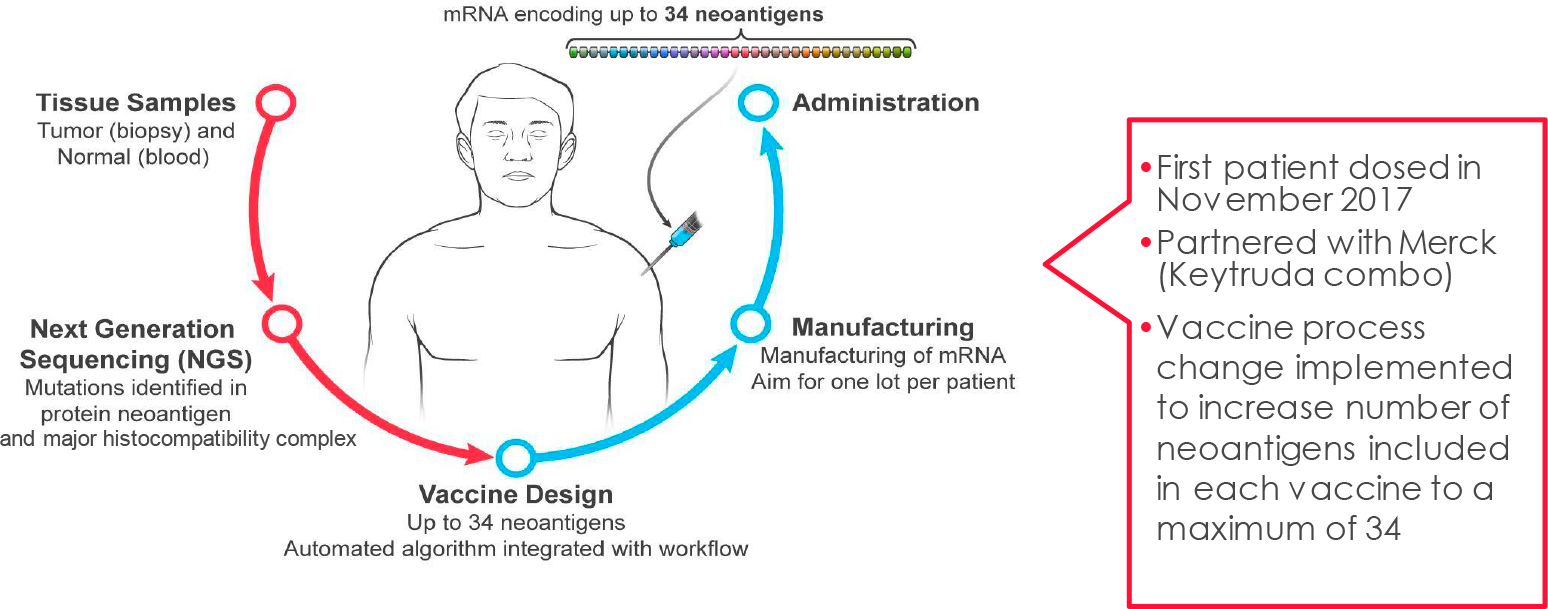
The mRNA sequence is assembled in silico to encode up to 34 epitopes simultaneously, forming a neoantigen concatemer. These mRNA molecules are then encapsulated in proprietary lipid nanoparticles (LNPs). This process confers tolerance, minimizes toxicity during repeated administration, helps the vaccine evade immune system surveillance, and protects it from enzymatic degradation.
Following intramuscular injection of the personalized cancer vaccine, antigen-presenting cells (APCs) capture and translate mRNA instructions, resulting in the expression of corresponding epitopes on their surface. This process induces specific immune responses by CD8+ cytotoxic T cells and CD4+ memory T cells.
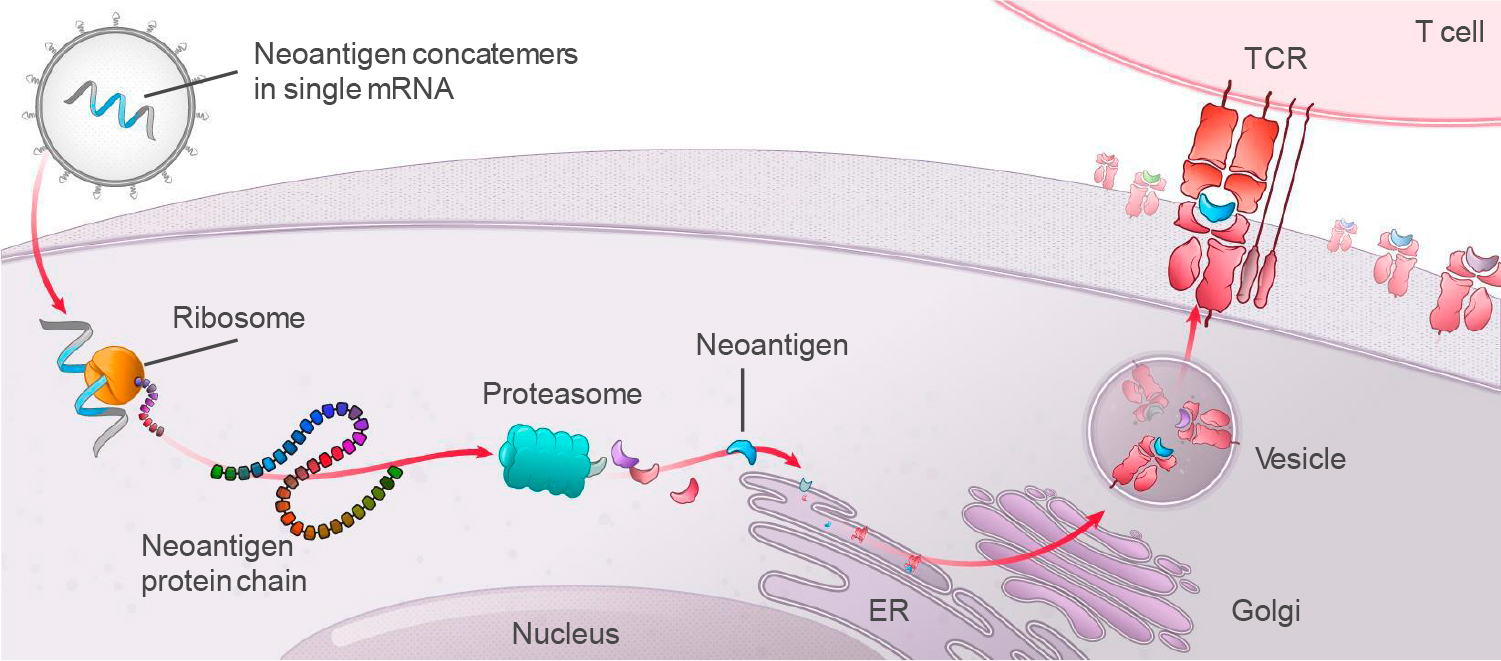
The delivery of multiple tumor-specific antigens (TSAs) into the body simultaneously should significantly increase the likelihood of successful clinical outcomes. This is because the immune system generates a multidirectional T cell response to the neoantigenic peptides presented to it, resulting in an enhanced ability to recognize and kill tumor cells. In other words, the immune system undergoes training.
Moderna’s vaccine mRNA-4157 (V940) is referred to as Individualized Neoantigen Therapy (INT).
The vaccine is being developed in collaboration with Merck & Co., with whom Moderna entered into a strategic agreement in June 2016. Merck & Co. paid Moderna $200 million upfront [1], and the partnership was expanded in May 2018 with an additional $125 million investment [2]. In October 2022, Merck & Co. expressed their confidence in the success of mRNA-4157 (V940) [3], further strengthening the long-term alliance.
CLINICAL VALIDATION
The ongoing KEYNOTE-603 (NCT03313778) phase 1 (non-randomized, open-label, multicenter) clinical trial is fundamental to the further development of a personalized cancer vaccine, mRNA-4157 (V940), as it investigate its potential to treat a wide range of solid tumors with different regimens.
The study covers diagnoses such as non-small cell lung cancer (NSCLC), small cell lung cancer (SCLC), melanoma, urothelial carcinoma (UC), head and neck squamous cell carcinoma (HNSCC) not induced by human papillomavirus (HPV−), pancreatic ductal adenocarcinoma (PDAC), and any malignancy with microsatellite instability-high (MSI-H) or mismatch repair deficiency (dMMR), such as colorectal cancer, gastric and esophageal adenocarcinoma, and endometrial cancer.
A phase 2b (randomized, open-label, multicenter, international) clinical trial, KEYNOTE-942 (NCT03897881), is currently being conducted on patients with high-risk cutaneous melanoma (stage IIIB–D or IV) that has metastasized to a lymph node and has undergone complete surgical resection but still has a high risk of recurrence.
Participants’ disease had to be in remission, without locoregional relapse, distant metastases, or brain metastasis at the time of randomization.
The objective of this study is to determine whether the addition of the personalized oncovaccine mRNA-4157 (V940) to Keytruda (pembrolizumab), Merck & Co.’s PD-1 blocker, is justified by an increase in relapse-free survival (RFS) compared to pembrolizumab alone. The prerequisites for this study are clear: In the adjuvant setting (after resection), there is no tumor, the patient has not yet received too many lines of chemotherapy, and the patient’s immune system is relatively healthy.
Recently launched clinical trials are evaluating the combination of mRNA-4157 (V940) and Keytruda to prolong event-free survival after surgical resection and keep the patient in remission:
- INTerpath-001 (V940-001, NCT05933577) phase 3. Cutaneous melanoma (stage IIB–C, III, or IV) after surgical resection, no evidence of disease, at high risk of recurrence, previously systemic untreated. mRNA-4157 (V940) + pembrolizumab — versus pembrolizumab. Endpoints: RFS, DMFS, OS.
- INTerpath-002 (V940-002, NCT06077760) phase 3. Non-small cell lung cancer (NSCLC) [stage II, IIIA, or IIIB/N2] after surgical resection, no evidence of disease, previously received at least one line of adjuvant platinum doublet chemotherapy. mRNA-4157 (V940) + pembrolizumab — vs. pembrolizumab. Endpoints: DFS, OS, DMFS, LCSS.
- V940-004 (NCT06307431) phase 2. Renal cell carcinoma (RCC, kidney cancer) after surgical resection, no evidence of disease, at intermediate-high or high risk of recurrence, previously untreated. mRNA-4157 (V940) + pembrolizumab —vs. pembrolizumab. Endpoints: DFS, OS, DMFS.
- V940-005 (NCT06305767) phase 2. Muscle-invasive urothelial carcinoma (MIUC, bladder cancer) after surgical resection, at high risk of recurrence, previously systemic untreated. mRNA-4157 (V940) + pembrolizumab — vs. pembrolizumab. Endpoints: DFS, OS, DMFS.
- INTerpath-007 (V940-007, NCT06295809) phase 2/3. Cutaneous squamous cell carcinoma (cSCC) [stage II–IV without distant metastases], locally advanced, resectable, previously untreated. mRNA-4157 (V940) + pembrolizumab before and after surgical resection — vs. surgical resection ± pembrolizumab. Endpoints: EFS, ORR, FFS rate, pCR rate, mPR rate, DFS, DSS, OS.
Abbreviations: DFS, disease-free survival; DMFS, distant metastasis-free survival; DSS, disease-specific survival; EFS, event-free survival; FFS, freedom from surgery; LCSS, lung cancer specific survival; mPR, major pathological response; ORR, overall response rate; OS, overall survival; pCR, pathological complete response; RFS, recurrence-free survival.
MELANOMA TREATMENT
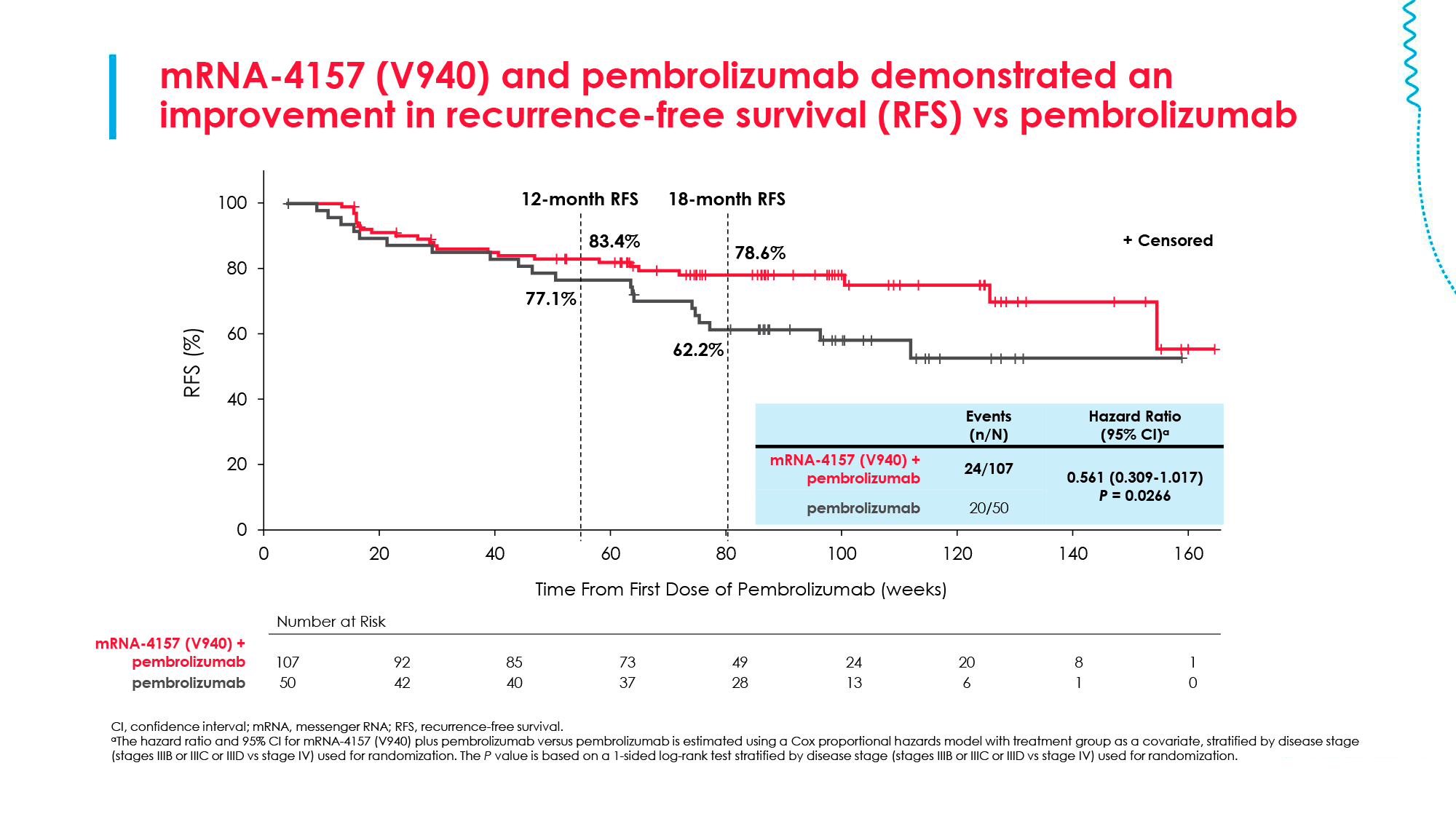
After a median 2-year (23–24 months) follow-up of melanoma patients from the KEYNOTE-942 (NCT03897881) phase 2b trial who received either mRNA-4157 (V940) with Keytruda (pembrolizumab) or pembrolizumab alone, the experimental combination immunotherapy treatment clinically (but not statistically!) improved recurrence-free survival (RFS) by reducing the risk of recurrence or death by 44% compared to pembrolizumab monotherapy: hazard ratio (HR) 0.56 (95% CI [hereafter], 0.31–1.02; two-sided p=0.053) [1] [2] [3].
At 12 months, 83% and 77% of patients, respectively, achieved RFS and at 18 months, 79% and 62% of patients [4].
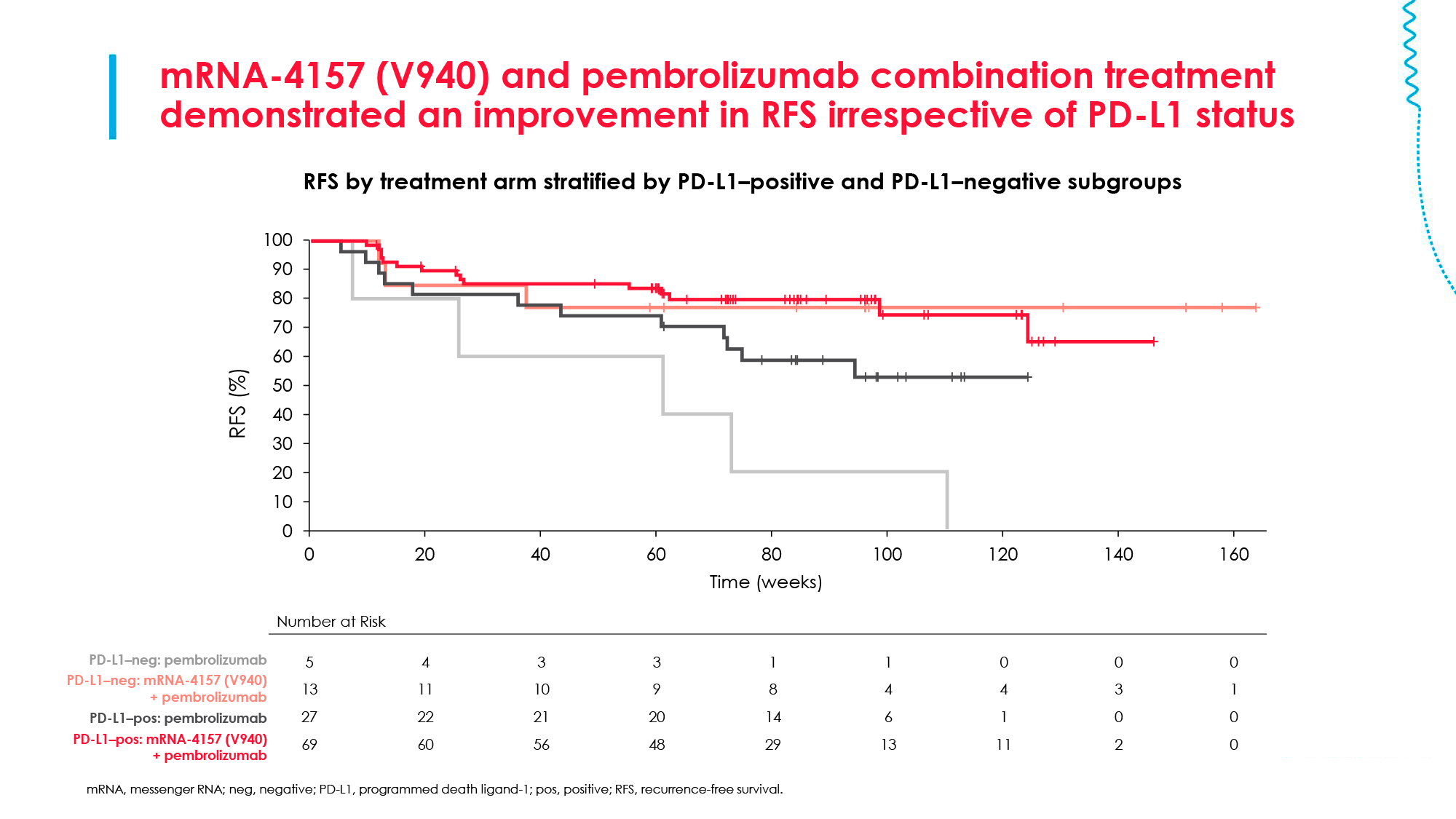
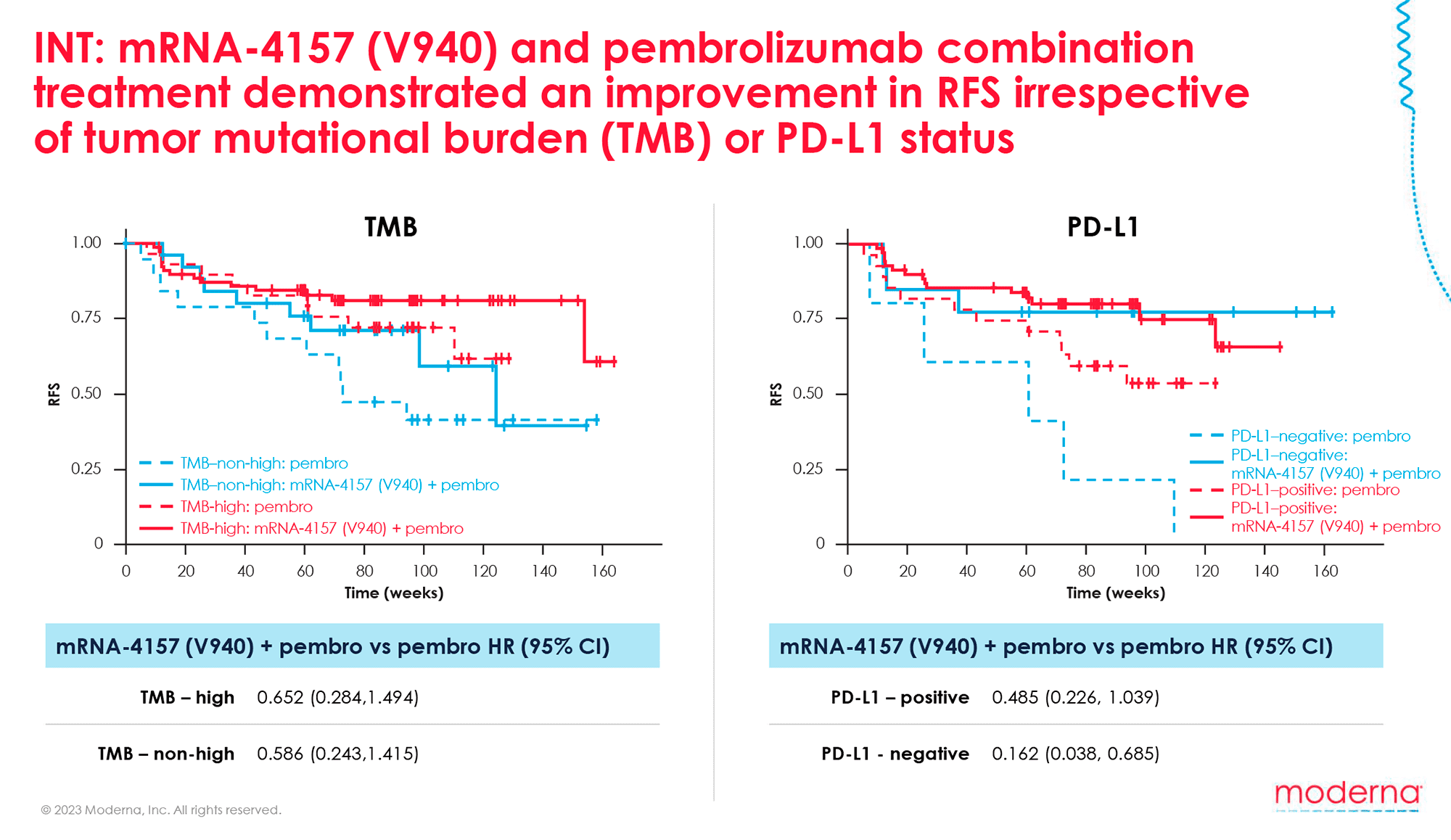
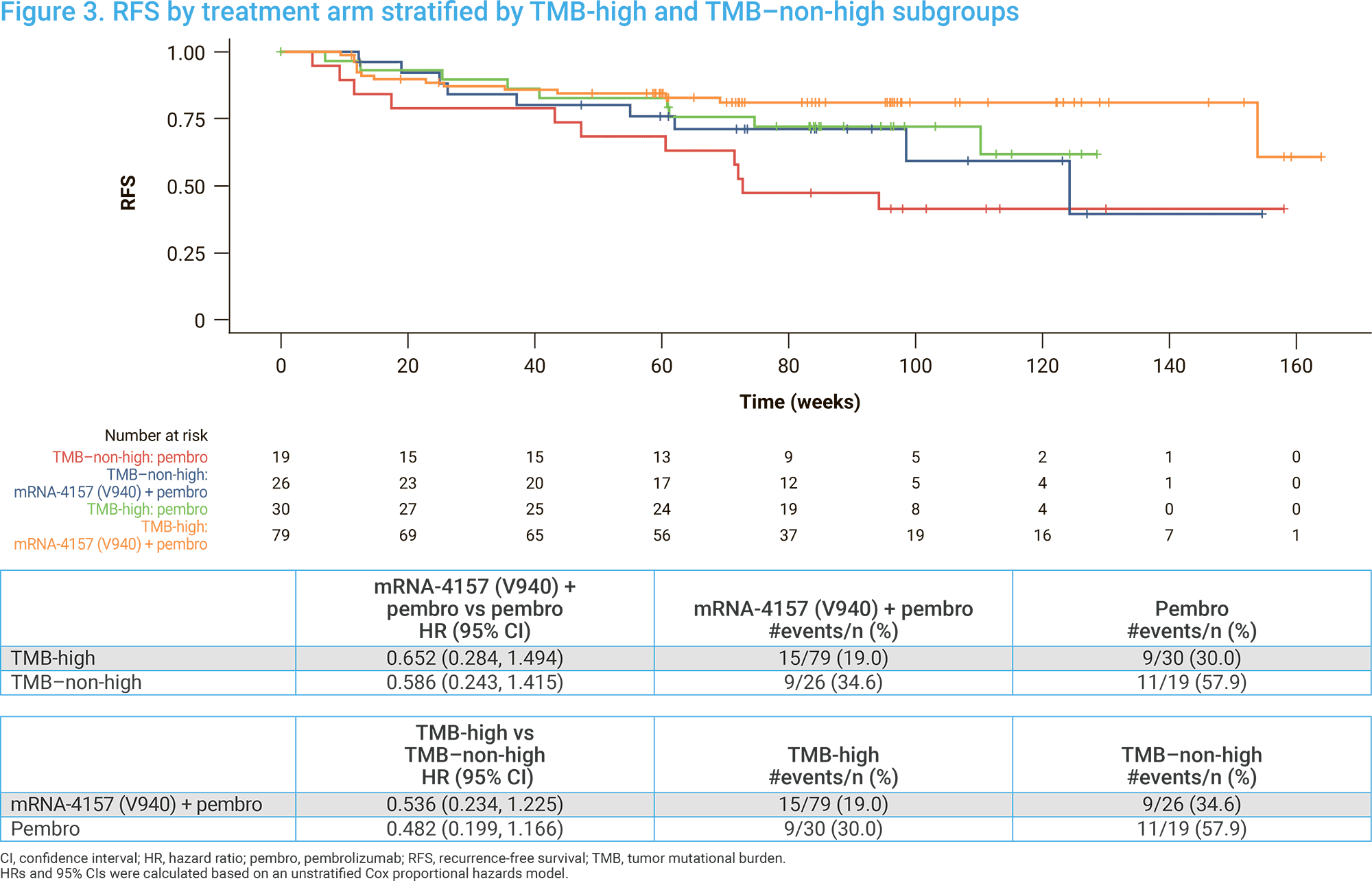
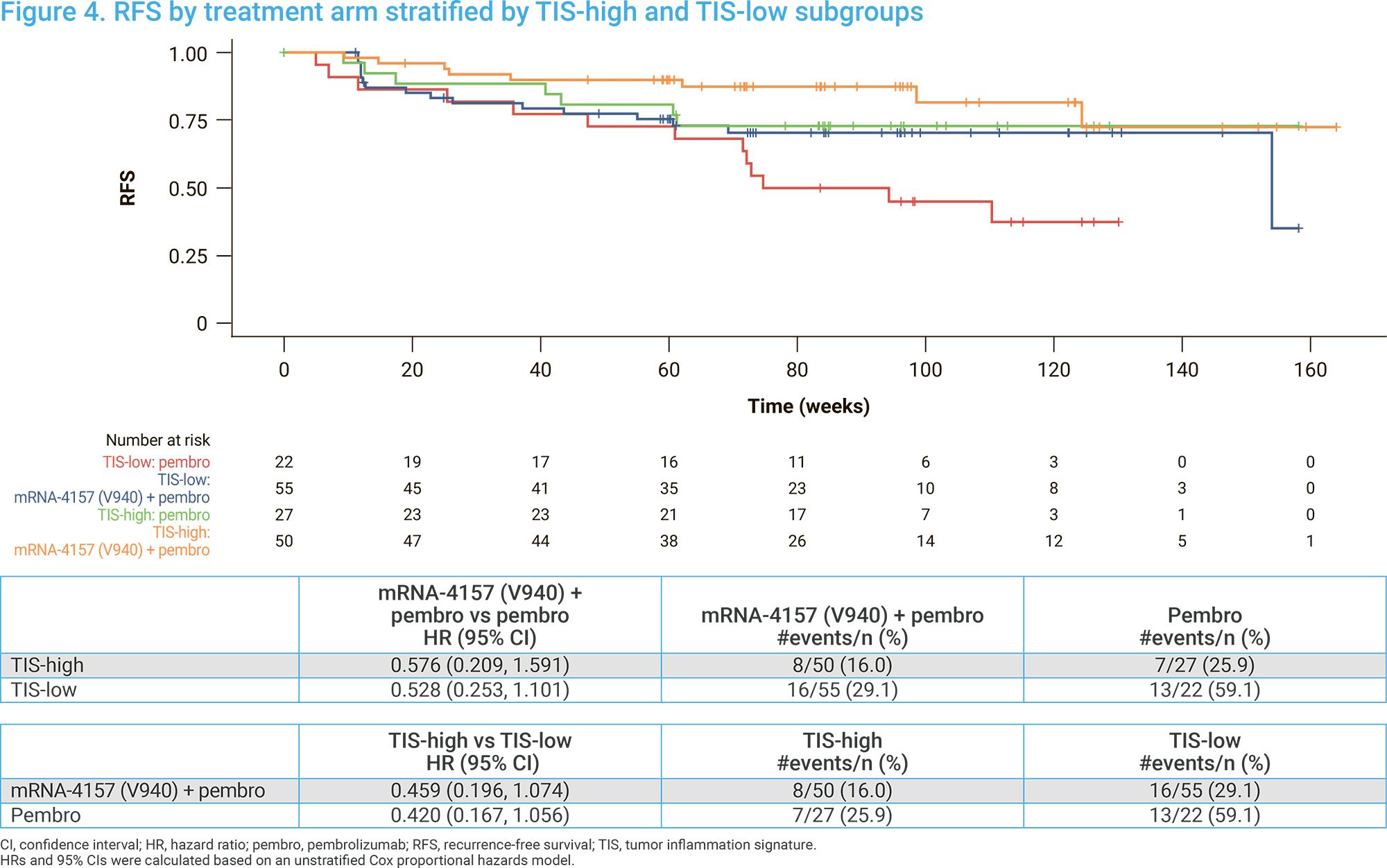
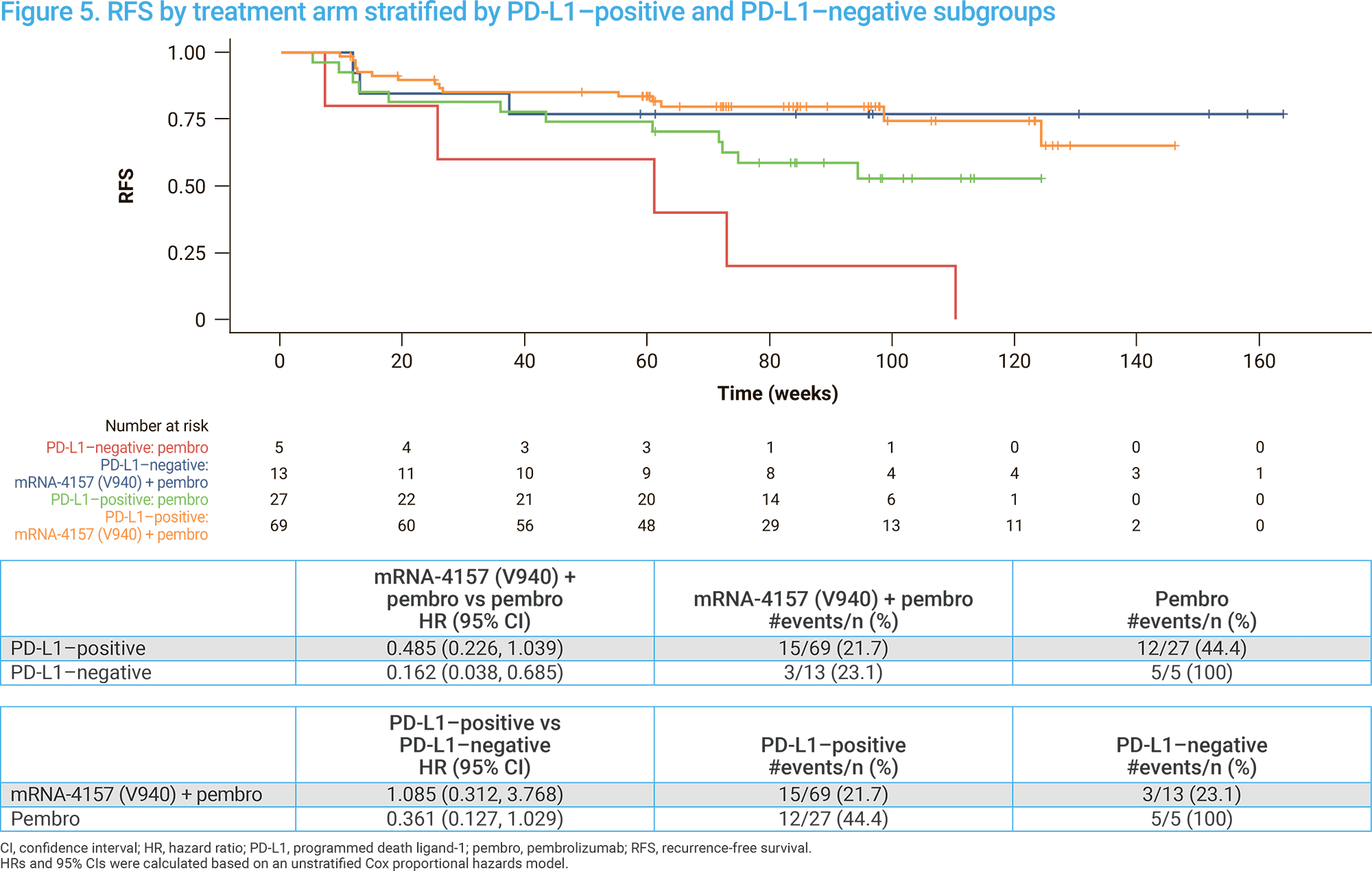
Regardless of tumor mutation burden (TMB), tumor inflammation score (TIS) and PD-L1 status, consistent RFS improvement was observed with personalized mRNA oncovaccine with PD-1 blocker. The corresponding HRs are as follows [5]:
- High TMB (175 mutations per exome or ≥ 10 mutations per megabase) and low TMB: 0.65 (0.28–1.49) and 0.59 (0.24–1.42)
- High TIS and low TIS (cutoff 4.56): 0.58 (0.21–1.59) и 0.53 (0.25–1.10)
- PD-L1 positive (CPS score ≥ 1) and PD-L1 negative tumors: 0.49 (0.23–1.04) and 0.16 (0.04–0.69).
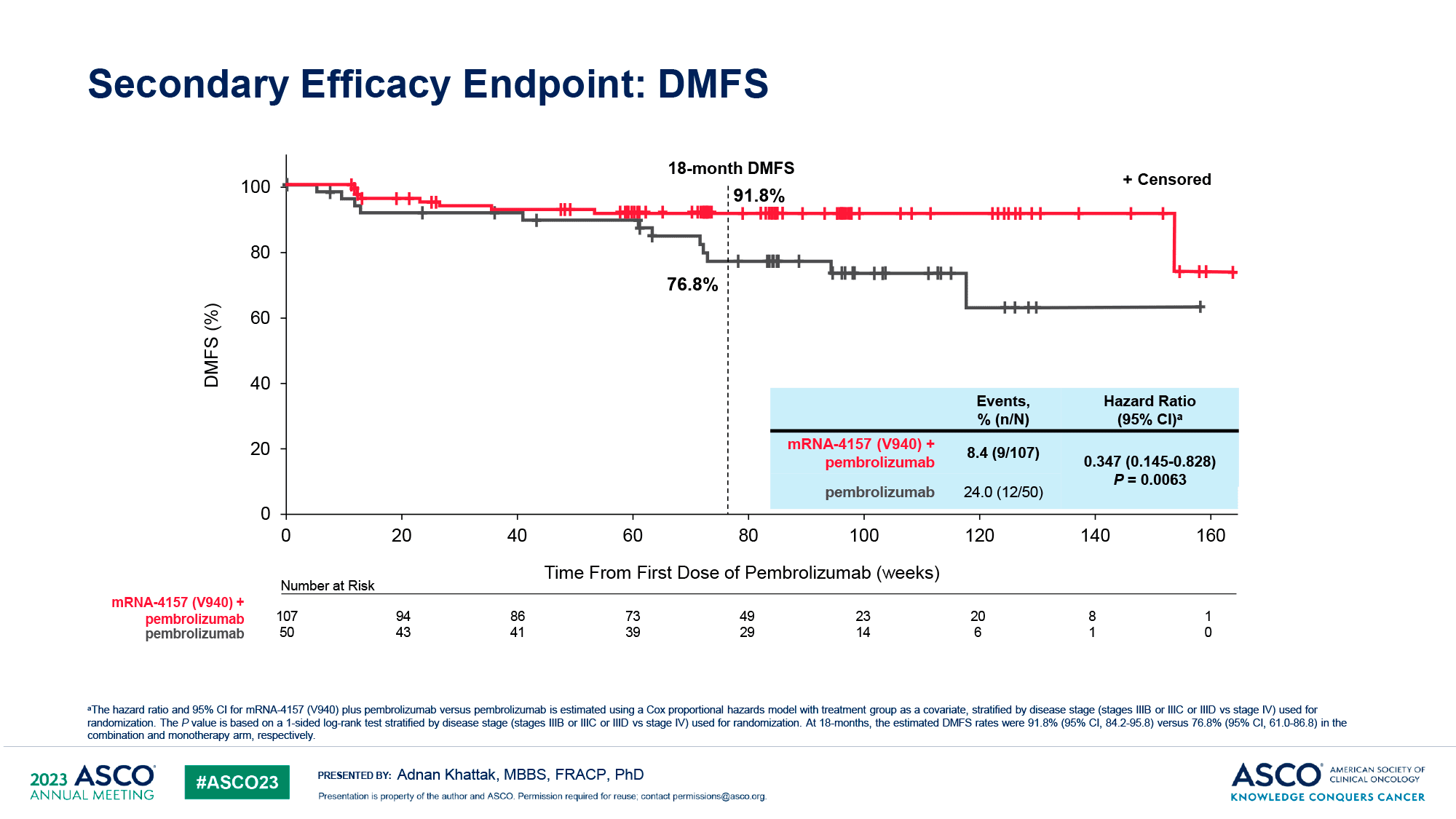
After 18 months of follow-up, 8% of patients in the combination treatment group and 24% of patients in the Keytruda monotherapy group experienced distant melanoma metastasis or death. The rates of distant metastasis-free survival (DMFS) were 93% and 89% at 12 months and 92% and 77% at 18 months [6] [7] [3].
In summary, the addition of the personalized cancer vaccine mRNA-4157 (V940) to the PD-1 blocker pembrolizumab provided a clinically meaningful improvement in DMFS, reducing the risk of distant metastasis or death by 65% compared to treatment with Keytruda alone (HR 0.35 [0.15–0.83]; one-sided p=0.0063).
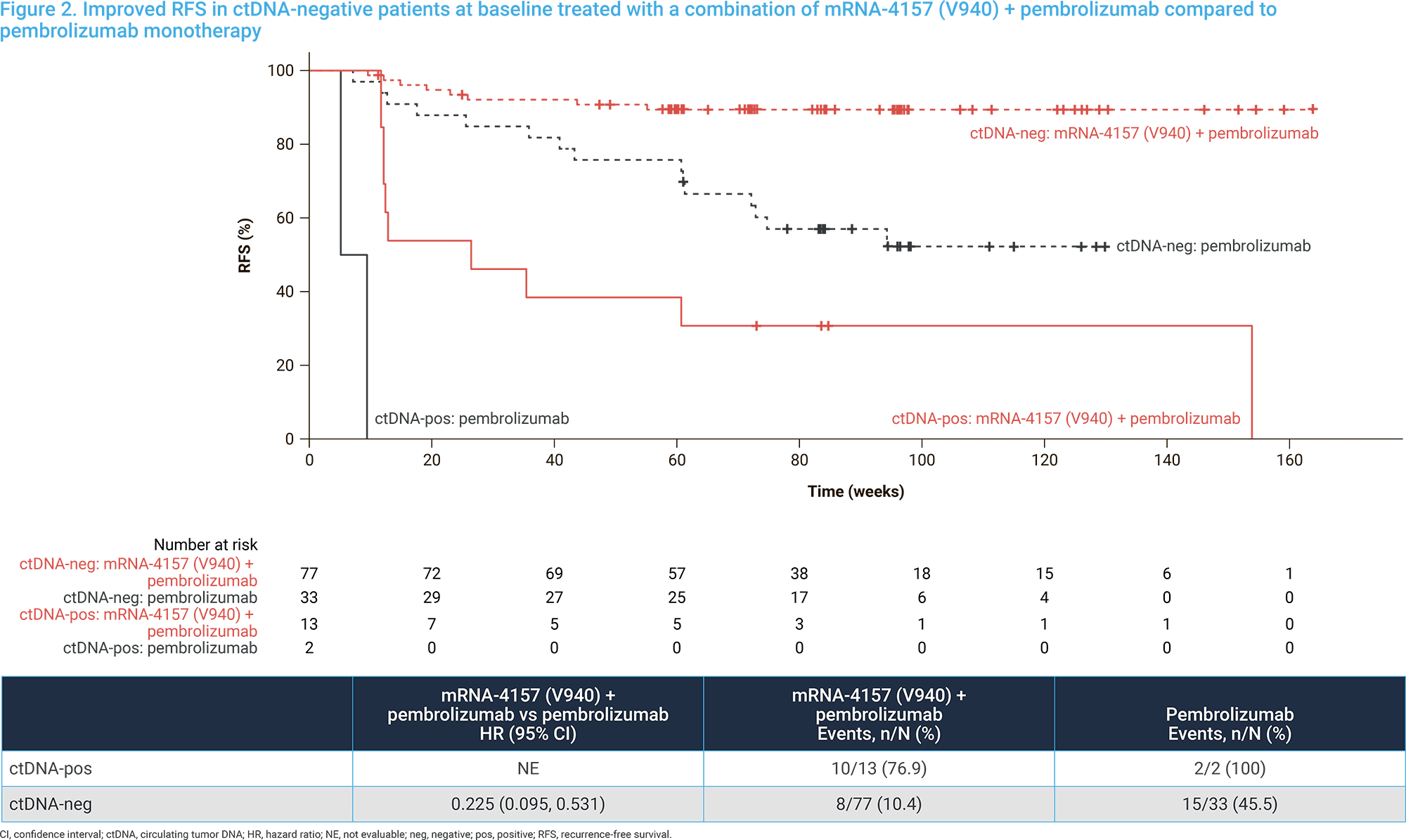
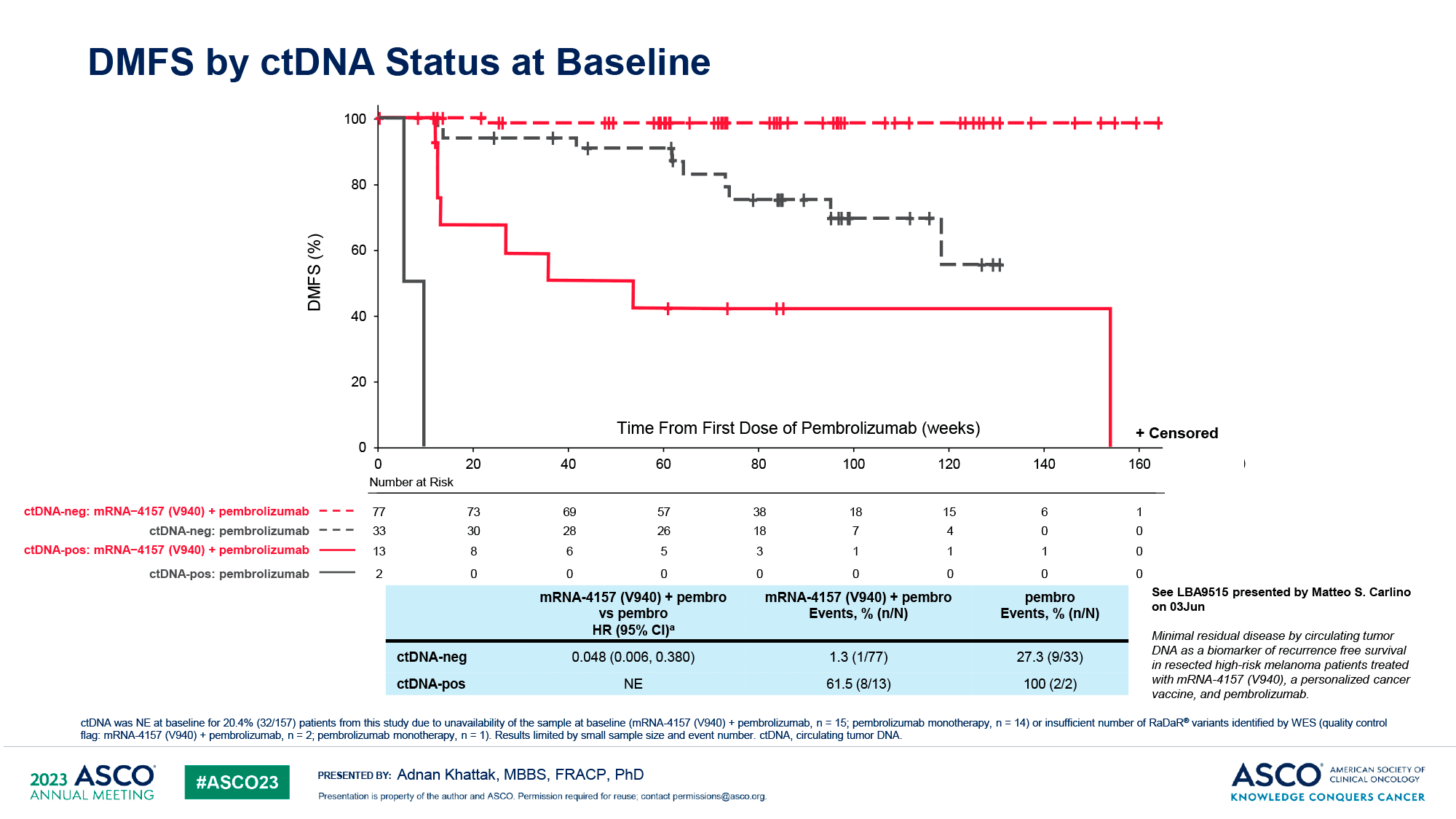
Circulating tumor DNA (ctDNA), which reflects the presence of minimal residual disease (MRD) after tumor resection and is a biomarker of recurrence-free survival (RFS) in high-risk melanoma that has undergone surgery, has been shown to be associated with a better response to therapy when ctDNA is undetectable prior to treatment [8].
Thus, in patients with ctDNA-negative status at baseline, RFS and DMFS rates were better when comparing combination therapy with monotherapy: the risk of recurrence or death and the risk of distant metastasis or death were reduced by 77% (HR 0.23 [0.10–0.53]) and 95% (HR 0.05 [0.01–0.38]), respectively. Trends toward improved RFS and DMFS with co-treatment were also observed in ctDNA-positive patients. However, the small number of patients did not allow definitive conclusions to be drawn that the efficacy of the therapeutic personalized cancer vaccine mRNA-4157 (V940) is generally independent of initial ctDNA status.
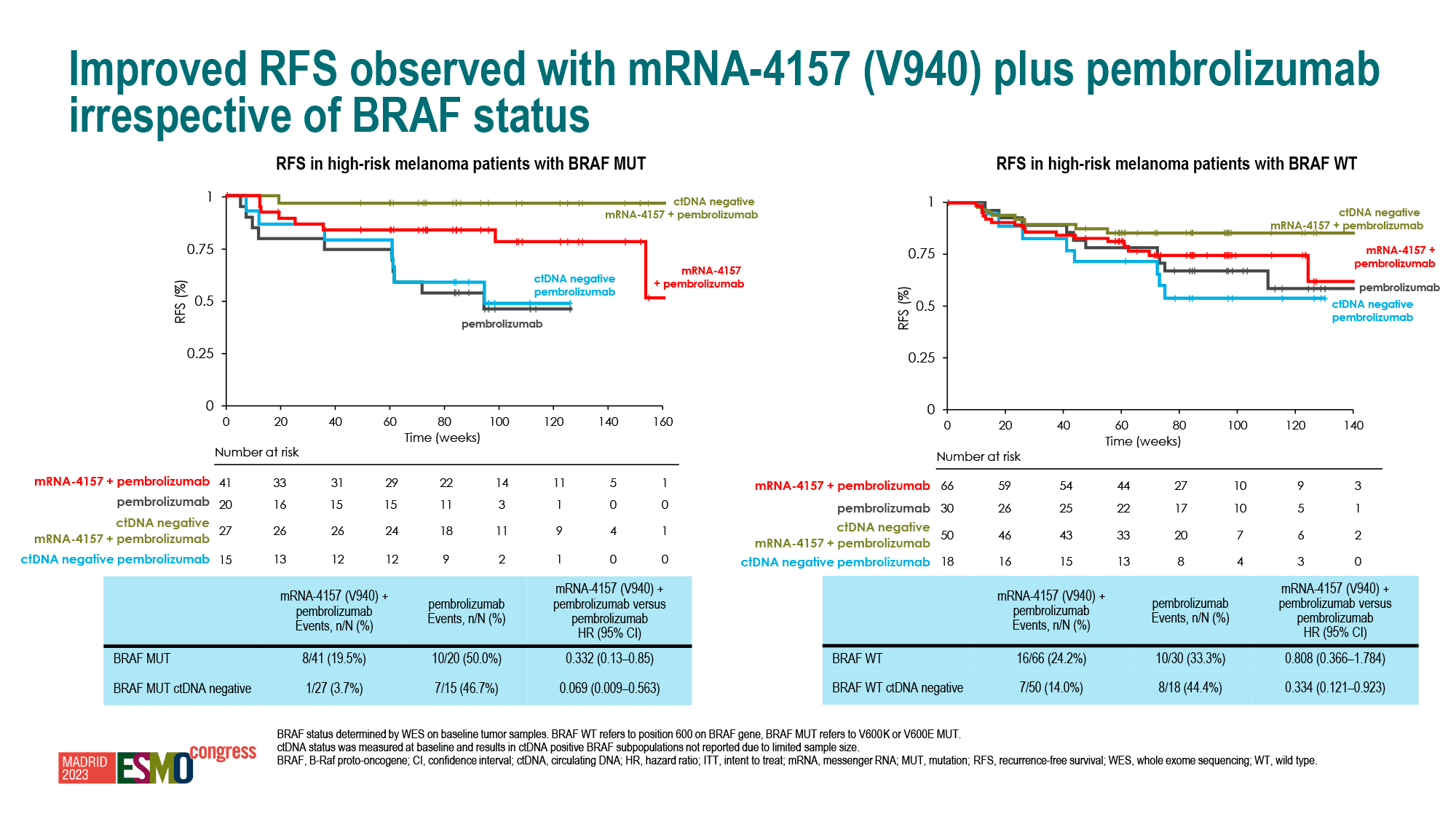
Individualized neoantigen therapy with mRNA-4157 (V940) outperformed standard therapy regardless of BRAF status, mutant or wild-type.
After a median of 3 years of follow-up, the combination treatment of melanoma with mRNA-4157 (V940) and pembrolizumab resulted in a significant improvement in RFS and DMFS, reducing the risk of recurrence or death by 49% (HR 0. 51 [0.29–0.91]; one-sided nominal p=0.0095) and reducing the risk of distant metastases or death by 62% (HR 0.38 [0.17–0.86]; one-sided nominal p=0.0077) compared to treatment with pembrolizumab alone [9].
ESSENCE
Long-term anti-PD-1 monotherapy is a standard and effective clinical practice for adjuvant treatment of resected high-risk melanoma to prevent recurrence [1] [2] [3]. However, it is associated with a high risk of chronic toxicity [4]. The therapeutic personalized cancer vaccine mRNA-4157 (V940) seems ready to refresh this paradigm.
Nevertheless, there is robust evidence of improvement in RFS and DMFS compared to current therapeutic approaches.
Thus, a 3.5-year follow-up of patients treated with a one-year course of pembrolizumab revealed that 60% and 65% of individuals remained in RFS and DMFS and 55% and 61% after 5 years of follow-up [5] [6]. After one year of therapy with nivolumab, 52% and 59% of patients achieved 4-year RFS and DMFS [7].
That is, in the long term, approximately half of patients experience melanoma recurrence (or death), necessitating a move to the next lines of therapy. Therefore, mRNA-4157 (V940) was tested to reduce the risk of recurrence (RFS), which can be worsened by metastasis (DMFS), for the longest possible duration. The mRNA oncovaccine achieved this preventive effect, although without a confirmed statistically significant difference compared to pembrolizumab monotherapy. This may be due to the small sample size of the participants.
Meanwhile, pembrolizumab has been shown to be suitable for concurrent use in both the neoadjuvant and adjuvant settings, before and after resection [8]. Under certain conditions, the combination of ipilimumab with nivolumab has also shown promise in the neoadjuvant setting [9] [10]. The hypothesis is that a tumor that has not yet been resected has enough mass to activate and expand the systemic antitumor T-cell response to a similar strength as in the case of immunotherapy for recurrent melanoma [11].
The issue of improving overall survival (OS) remains unresolved and significant. Currently, there is no reliable data on whether PD-1 blockers extend OS. Additionally, the RFS and DMFS endpoints are only surrogates for OS, and it is a stretch to draw any definitive conclusions based on them [12].
Anyway, it is important for Moderna to invest more effort in the development of mRNA-4157 (V940). In the post–COVID-19 era, there are no longer super profits from selling SARS-CoV-2 vaccines.
From a business perspective, Moderna was extremely smart to spend a long time conducting a phase 2b clinical trial before launching the pivotal phase 3 at the end of July 2023 [13]. This approach was taken due to the high number of failed clinical trials of cancer vaccines. While not everyone may agree with this interim approach to development, a conservative strategy is reasonable.
HEAD AND NECK CANCER TREATMENT
An interim analysis was conducted on the clinical outcomes of KEYNOTE-603 (NCT03313778) phase 1 in a treatment cohort of unresectable head and neck squamous cell carcinoma (HNSCC) [with tumors in the oral cavity, oropharynx, laryngopharynx, or larynx] that was not induced by human papillomavirus (HPV−). The patients had not been previously treated with any immune checkpoint inhibitors (ICIs). The analysis revealed the following results [1].
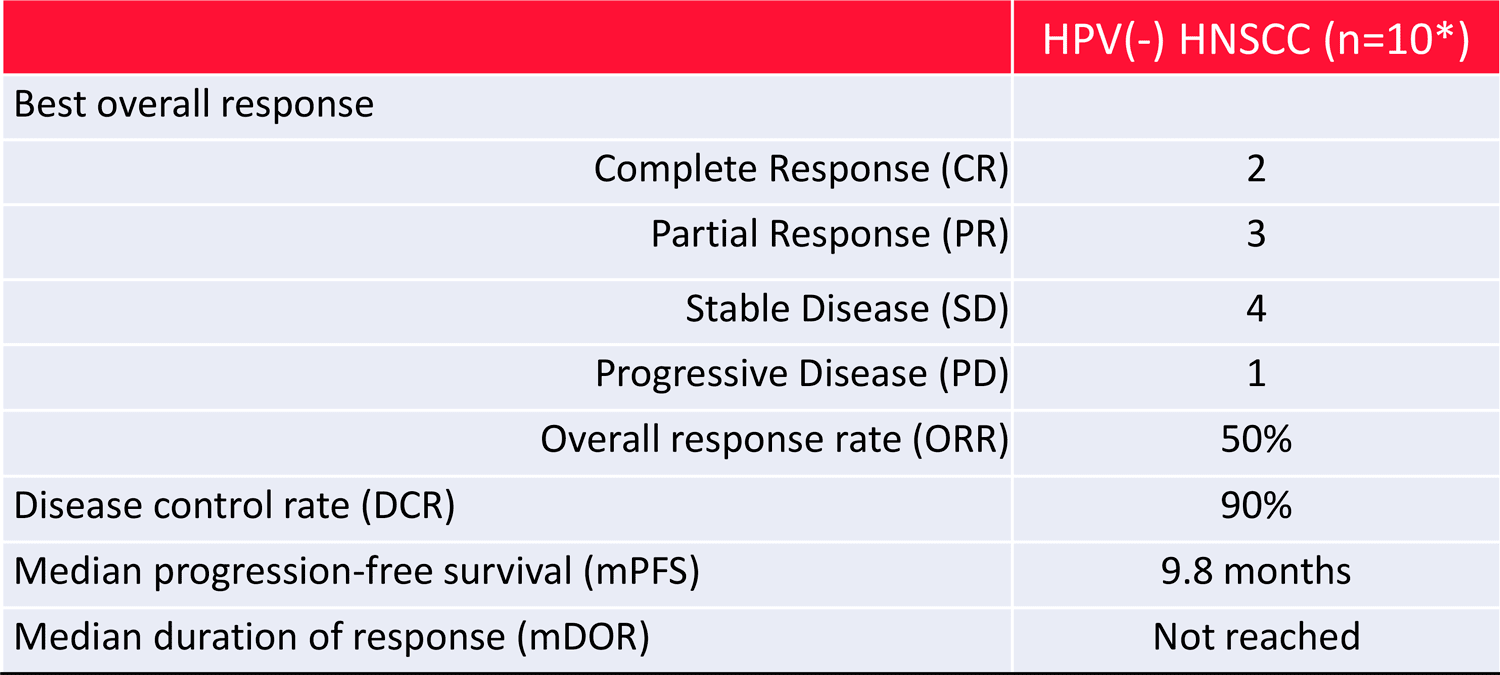
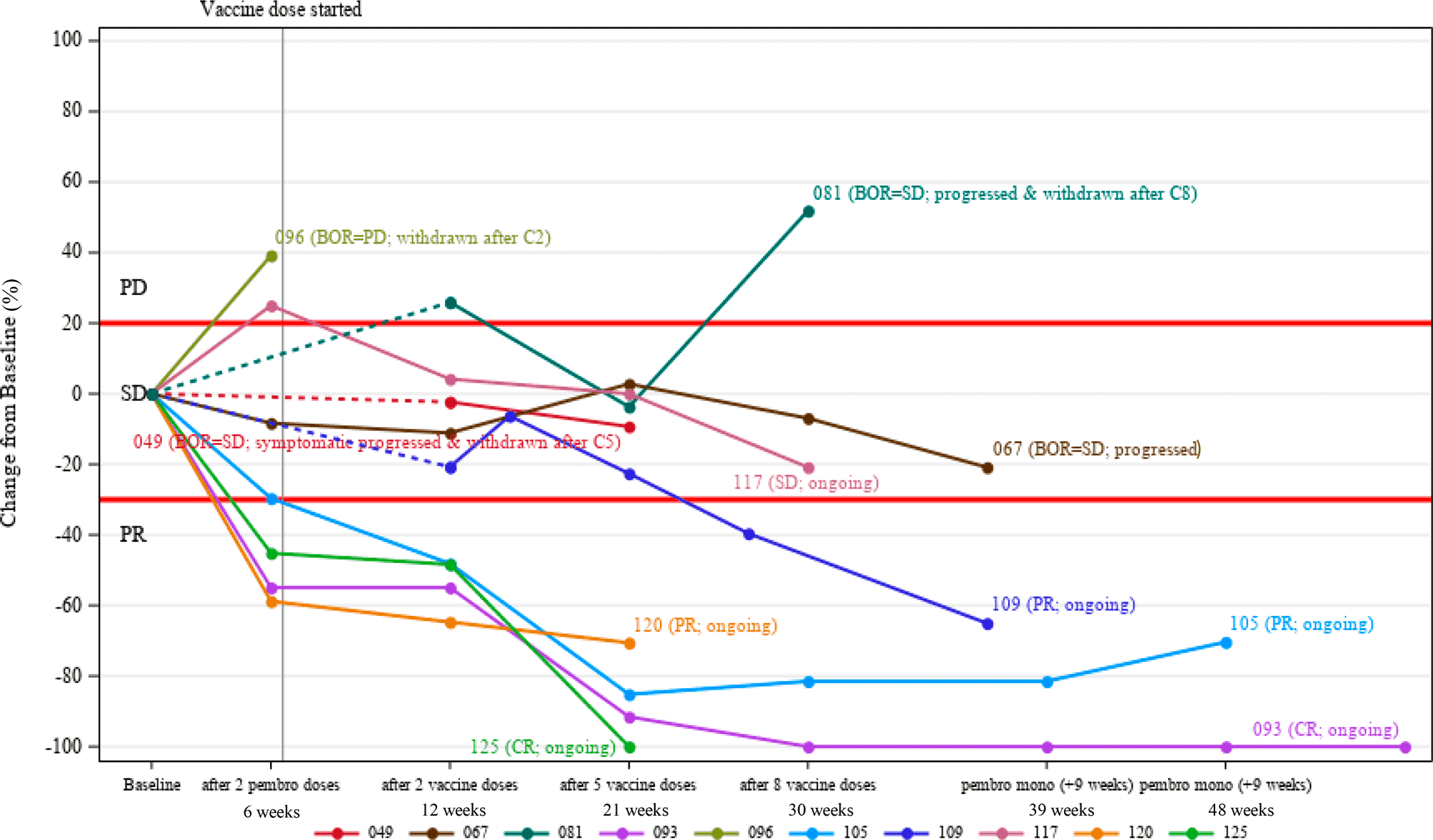
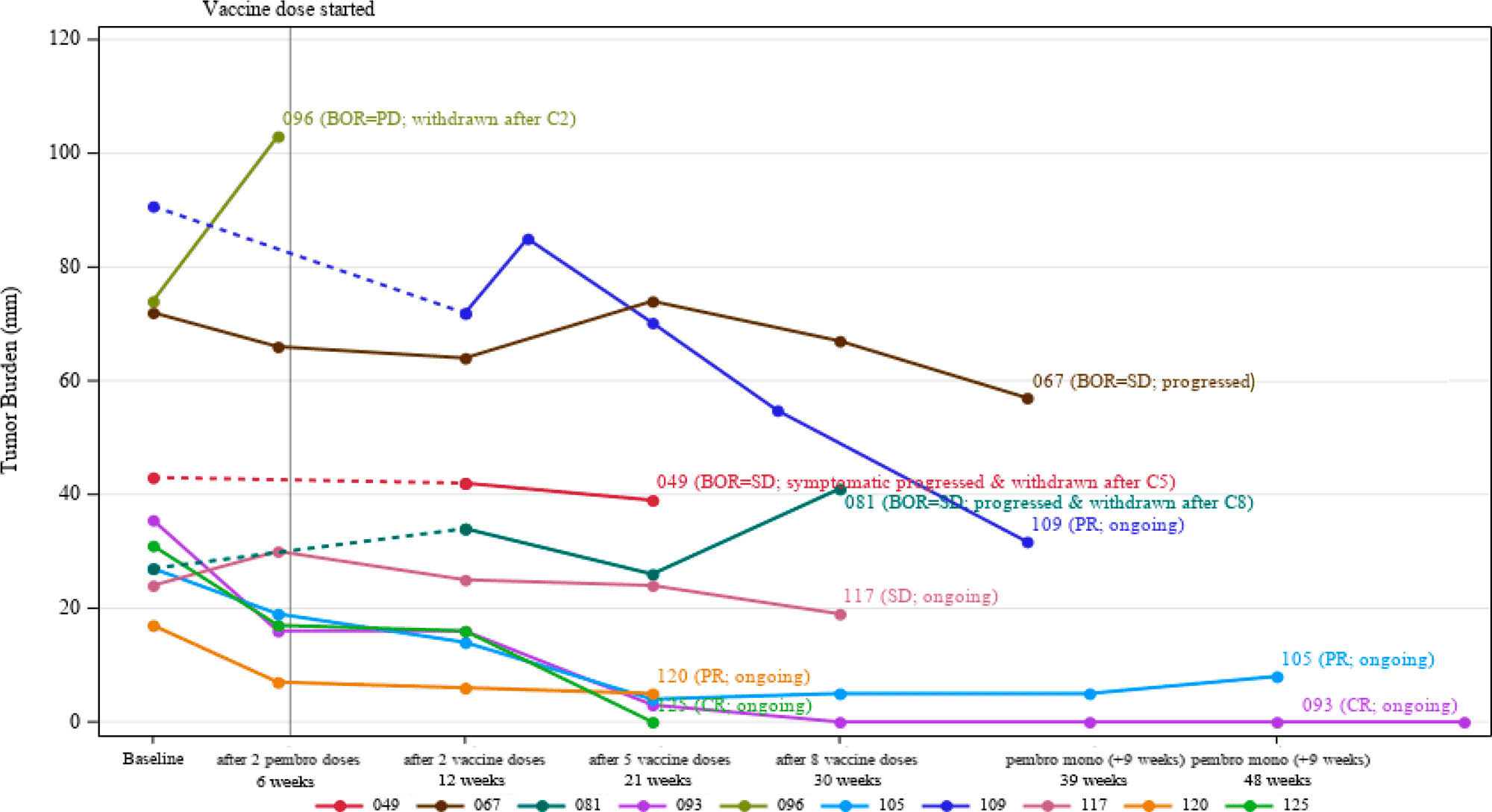
As of early October 2020, the combination of the individualized mRNA oncovaccine mRNA-4157 (V940) and the PD-1 blocker Keytruda (pembrolizumab) by Merck & Co. resulted in an overall response rate (ORR) of 50% (n=5/10). Of the patients, 20% (n=2/10) achieved a complete response (CR) and 30% (n=3/10) achieved a partial response (PR). Stable disease (SD) was observed in 40% (n=4/10) of subjects, while only one individual experienced progressive disease (PD). Therefore, the disease control rate (DCR), which is the sum of CR, PR, and SD, was 90% (n=9/10).
The duration of response (DoR) median has not yet matured. The median progression-free survival (PFS) was 9.8 months.
Notably, 4 out of 5 responders showed positive response to treatment after only two doses of pembrolizumab, even before mRNA-4157 (V940) was administered. Once they received the vaccine, the responses deepened. For instance, two patients in PR went into CR. A patient in PD on Keytruda finally achieved a PR after receiving the vaccine infusion.
In comparison, pembrolizumab monotherapy for recurrent or metastatic HNSCC resulted in an ORR of 14.6% and a median PFS of 2.0 months. The experimental cancer vaccine treatment outperformed the standard first-line therapy, which involves administration of Keytruda together with chemotherapy, with an ORR of 36% and a median PFS of 4.9 months [2] [3] [4].
The analysis of predictive biomarkers led to interesting conclusions. Patients with tumors characterized by increased levels of inflammation, as evidenced by GEP and CYT scores, showed a trend towards a favorable clinical response. However, no correlation was found with tumor mutational burden (TMB).
- The GEP score reflects RNA expression of 18 inflammatory genes related to antigen presentation, chemokine expression, cytolytic activity, and adaptive immune resistance, including PD-L1. Additionally, it indicates the level of T cell inflammation in the tumor microenvironment (TME). The CYT score is based on transcript levels of two key cytolytic effectors, granzyme A and perforin.
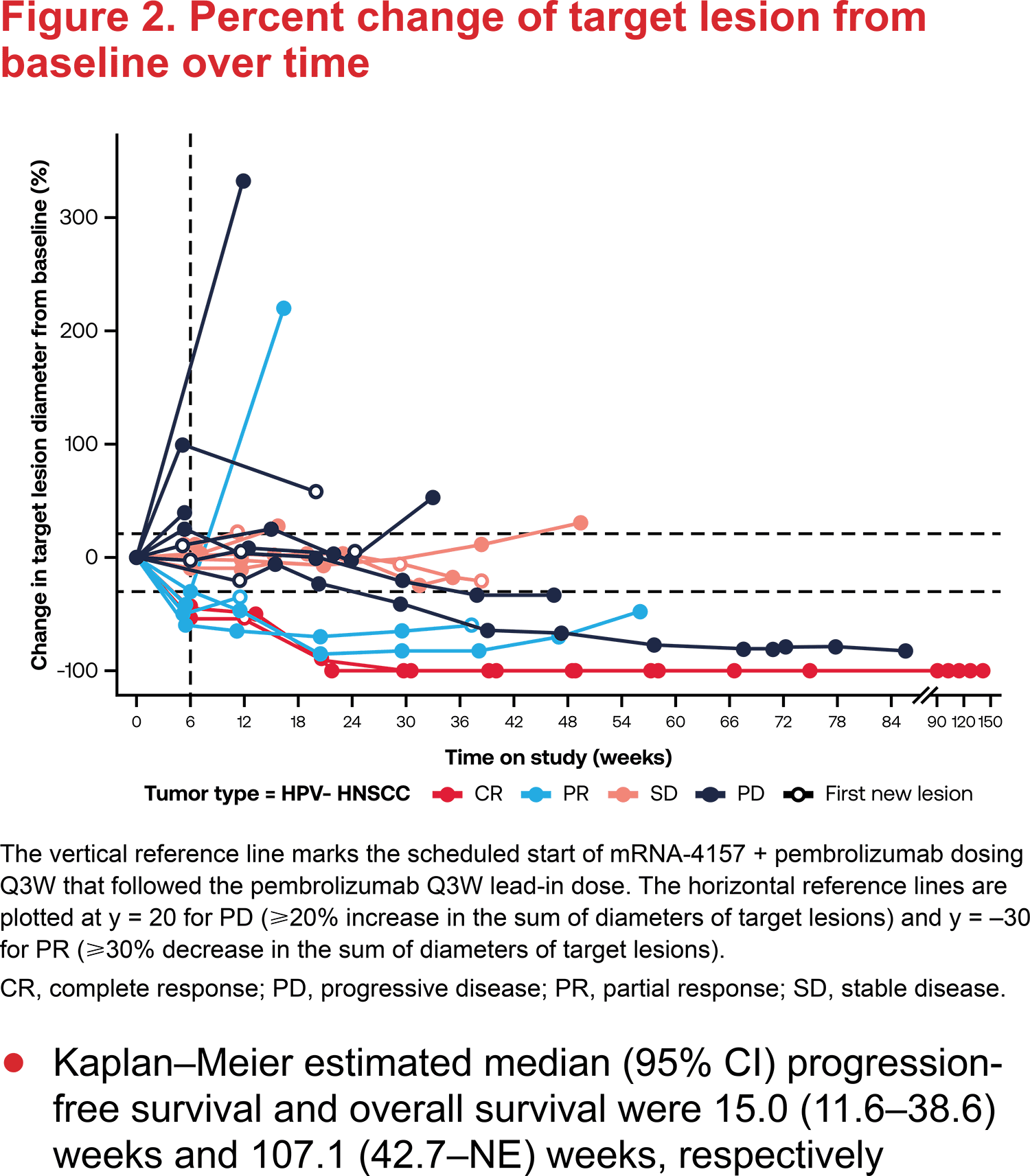
As of early May 2023, further analysis was conducted with a median follow-up of 9.0 (2.7–45.5) months and enrolling more patients. The results showed an ORR of 27% (11–50), including a CR of 9% and a PR of 18%, and a DCR of 64% (41–83). The estimated medians of PFS and overall survival (OS) were 3.5 (2.7–9.0) months and 25.0 (9.0–NE) months, respectively [5].
ESSENCE
Patients diagnosed with head and neck squamous cell carcinoma (HNSCC) that are negative for human papillomavirus (HPV−) have a poor prognosis, with a five-year survival rate of no more than 50% [1].
The limited increase in durable clinical responses to PD-(L)1 therapeutic blockade is believed to be due to reduced effector cytolytic activity and clonal diversity [2] [3] [4] [5].
Given that the individualized oncovaccine mRNA-4157 (V940), which encodes up to 34 tumor-associated neoantigens, induces specific activation of antitumor T cells, which was confirmed by successful treatment of melanoma, it was logical to trial its administration in tandem with the PD-1 inhibitor pembrolizumab.
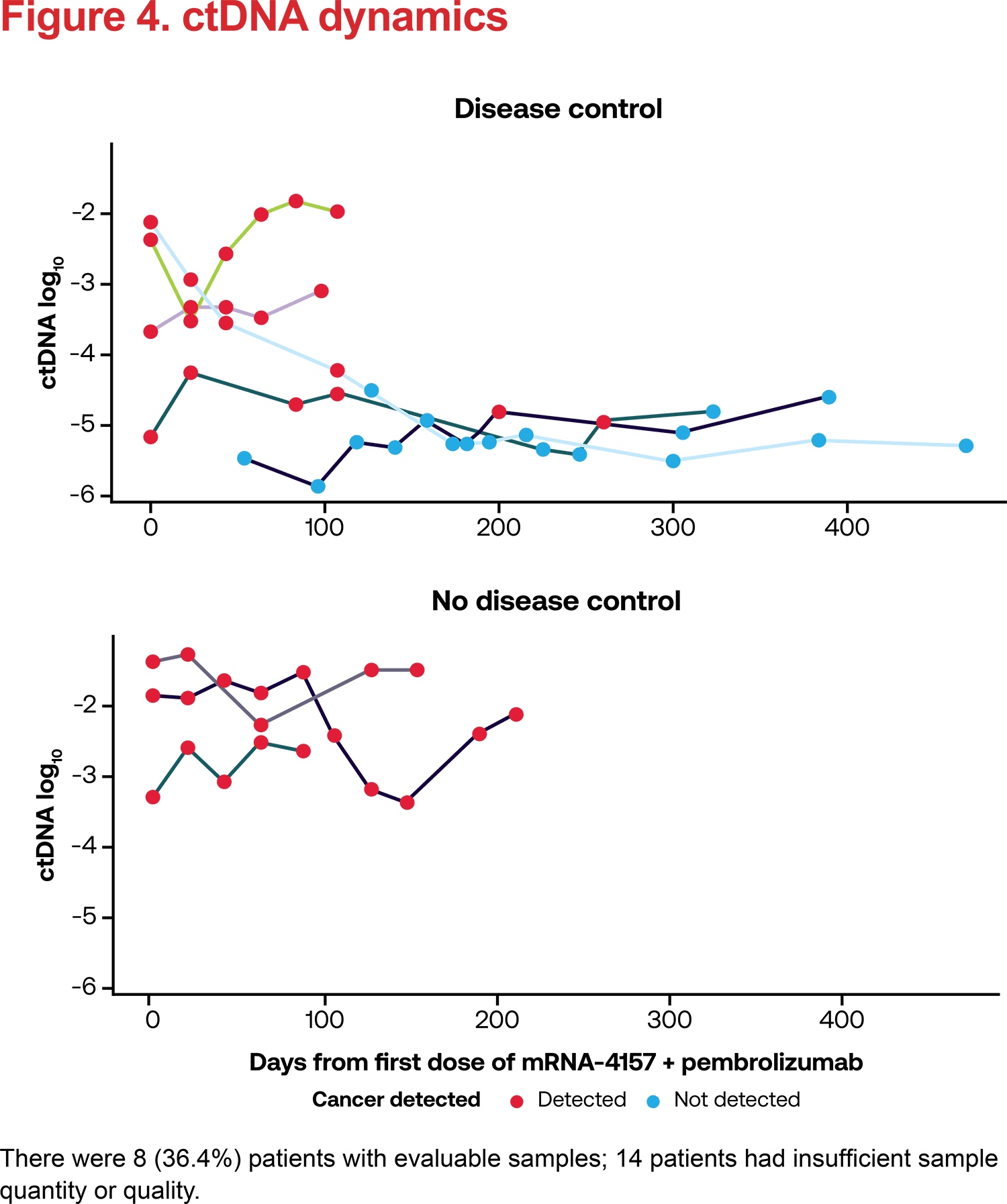
The immuno-oncology cocktail demonstrated activation of immune responses in those who responded to treatment, as evidenced by a decrease in circulating tumor DNA (ctDNA) levels. “Warmer” tumor such as HNSCC (HPV−) have a more favorable tumor microenvironment (TME) for the generation of T-cell responses induced by the combination of mRNA-4157 (V940) with pembrolizumab. Furthermore, the addition of neoantigens through a personalized cancer vaccine reduces the threshold for the level of tumor mutational burden (TMB) required to achieve a therapeutic response to pembrolizumab.
Preliminary findings show that in HNSCC (HPV−) treatment, the addition of the mRNA vaccine to standard pembrolizumab can extend overall survival by at least 50% compared to the latter alone.
CANCER VACCINES: GOOD BUT NOT GOOD ENOUGH
Although cancer vaccines have promising potential, the development of this area of biotechnology is progressing slowly. There are several obstacles to overcome including the heterogeneity of tumor antigens and their mutational variation, the absence of a unified signaling pathway for antigen recognition and immune response activation, multiple mechanisms for cancer cells to evade immunological surveillance, the selection of the appropriate immunostimulatory adjuvant, and the optimal route of vaccine delivery.
Nevertheless, there are several interesting cancer vaccines in the clinical pipeline, including personalized ones.
So far, only two personalized cancer vaccines have been approved worldwide: Oncophage (vitespen) and Provenge (sipuleucel-T).
There are three additional cancer drugs based on oncolytic viruses: Oncorine, Imlygic (talimogene laherparepvec), and Delytact (teserpaturev). They are used to treat head and neck carcinoma, melanoma, and malignant glioma, respectively. Although they are not classified as cancer vaccines, they share similarities with oncovaccines due to their mechanisms of action. The immune system is presented with tumor antigens that accumulate due to the targeted destruction of cancer cells induced by oncolytic viruses.
The tuberculosis vaccine BCG (Bacillus Calmette –Guérin), which has been used with great success in immunotherapy of non-muscle invasive bladder cancer (NMBIC) for almost half a century, stands out.
PERSONALIZED CANCER VACCINES: INDIVIDUALIZED ONCOLOGY TREATMENT
ONCOPHAGE
Oncophage (vitespen) is a personalized cancer vaccine indicated to adjuvant treatment for post-nephrectomy localized renal cell carcinoma (kidney cancer) with an intermediate risk of recurrence.
Oncophage, formerly known as Prophage, is a complex of heat shock protein (HSP) gp96 and peptide fragments derived from the patient’s tumor tissue. The autologous antigenic complex, vitespen (HSPPC-96), stimulates resident dendritic cells. These cells activate cytotoxic T lymphocytes (CTL) and T helper cells, which are key components of the antitumor immune response cascade [1].

Oncophage, developed by Antigenics (now Agenus as of January 2011 [2]), received regulatory approval only in Russia, where it was authorized in April 2008 [3] [4].
In November 2009, Antigenix withdrew its application for marketing authorization of Oncophage in the European Union. This decision came after an expert committee at the European Medicines Agency (EMA) concluded that the oncovaccine could not significantly prolong relapse-free survival. The manufacturer did not provide complete information regarding the composition of Oncophage and its manufacturing process, as well as the mechanism of action in renal cell carcinoma and the appropriate dose [5].
According to studies, Oncophage administration reduces the risk of disease progression or death (PFS) by 41% (HR 0.59 [0.37–0.94]; p=0.026) and the risk of death (OS) by 46% (HR 0.54 [0.30–0.97]; p=0.036) [6] [7].
PROVENGE
Provenge (sipuleucel-T) is a personalized cancer vaccine indicated for the treatment of asymptomatic or minimally symptomatic metastatic castration-resistant prostate cancer.
Provenge is manufactured from a patient’s own peripheral blood mononuclear cells (PBMC), including antigen-presenting cells (APCs), T- and B-lymphocytes, and natural killer (NK) cells, which are then activated ex vivo by recombinant human PAP-GM-CSF protein. This protein is a combination of prostatic acid phosphatase (PAP), an antigen highly expressed in tumor tissues in prostate cancer, and granulocyte-macrophage colony-stimulating factor (GM-CSF), an immune cell activator. After intravenous infusion of sipuleucel-T (APC-8015), humoral and T-cell immune antitumor responses are elicited [1] [2].

Provenge developed by Dendreon, which was acquired by Canadian Valeant Pharmaceuticals International for $495 million in February 2015, and subsequently sold to Chinese conglomerate Sanpower Group for $820 million in July 2017 [3] [4] [5] [6]. A year later, Sanpower resold Dendrion to China’s Nanjing Cenbest, a large retailer that sought to enter the biotechnology industry, for $868 million. However, this transaction is essentially nominal, as Sanpower remains the largest shareholder of Nanjing Cenbest [7].
In April 2010, Provenge was approved by the US Food and Drug Administration (FDA) [8].
In September 2013, Provenge received marketing authorization from the European Medicines Agency (EMA), but in May 2015, it was terminated at the request of Dendrion due to commercial considerations [9].
The therapeutic efficacy of Provenge is modest. The personalized cancer vaccine reduces the risk of death by 22% (HR 0.78 [0.61–0.98]; p=0.032) and prolongs life by a median of 4.1 months relative to placebo [10]. However, a course of treatment consisting of three doses costs almost $200,000 without health insurance coverage [11].