SUMMARY
- Pancreatic cancer is a highly challenging oncologic disease to treat.
- Only 20% of patients are eligible for surgical tumor resection.
- Even if tumors are successfully removed, they almost always recur, leading to rapid death.
- A personalized cancer vaccine has been shown to delay recurrence and death by three years in one-third of patients.
- However, the availability and cost of this breakthrough therapy remain open questions.
WHAT HAPPENED
Germany’s BioNTech is developing a therapeutic personalized cancer vaccine (PCV) for the treatment of oncology diseases.
The mRNA oncovaccine autogene cevumeran has shown success in treating pancreatic cancer that has undergone complete resection.
After three years, approximately one-third of patients remain in complete remission.
This is a notable achievement considering the highly aggressive nature of pancreatic ductal adenocarcinoma (PDAC), which inevitably recurs even after successful surgery.
It is important to avoid making overly optimistic conclusions at this time. However, it is evident that there are conditions for breaking out of the stagnation that has persisted for six decades. The outcomes of pancreatic cancer treatment are generally unfavorable regardless of the method used.
Autogene cevumeran is currently being trialed in the therapy of various cancers, such as melanoma and colorectal cancer, in addition to its current use.
BioNTech’s collaboration with Genentech, a part of Roche, supports these efforts. In September 2016, the partners agreed to jointly develop personalized RNA vaccines against cancer. The Swiss pharmaceutical giant has committed to paying $310 million upfront and subsequent payments as the plan is realized. Costs and revenues are split equally [1].
WHY IT MATTERS
Pancreatic ductal adenocarcinoma (PDAC) accounts for over 95% of pancreatic cancer cases. Upon diagnosis, the majority of patients present with distant metastases or locally advanced unresectable disease, with only 20% of patients having a localized resectable tumor [1].
Pancreatic cancer is the seventh leading cause of cancer-related deaths worldwide [2]. Pancreatic cancer is a disease with a high incidence rate [3] and an almost unchanged survival rate of only 12% over the past 60 years [4]. It is predicted that pancreatic cancer will cause even more deaths by 2025 [3] [5].
Surgery is currently the only cure for pancreatic cancer. However, disease recurrence occurs in approximately 90% of patients within a median of 7–9 months after complete resection, and only 8%–10% of individuals achieve a fair five-year overall survival (OS) [6] [7].
Adjuvant multidrug chemotherapy is the standard of care for postoperative treatment of PDAC. Recurrence is delayed with this treatment, but it still occurs after approximately 14 months [8]. The five-year overall survival rate does not exceed 30% [9]. Radiation, biological, and targeted therapies have been found to be ineffective [8].
HYPOTHESIS
Pancreatic ductal adenocarcinoma (PDAC) has a response rate of less than 5% to immune checkpoint inhibitors such as PD-L(1) blockers [1] [2].
Pancreatic cancer is weakly antigenic due to its low mutation rate, resulting in the production of few neoantigens [2]. Neoantigens are unique protein sequences that arise from the tumor mutation process and mark tumor cells as foreign to T cells. This means that there are few infiltrating T cells that can kill tumor cells.
However, recent studies have shown that neoantigens in PDAC [3] [4] [5] are more abundant than previously believed [6].
Studies of long-term survivors of pancreatic cancer [7] [8] have demonstrated that neoantigens can stimulate T cells in PDAC. Primary tumors with high levels of immunogenic neoantigens had a significantly higher density of activated CD8+ T cells, which was associated with delayed disease recurrence and longer patient survival.
Therefore, as most PDAC tumors contain neoantigens capable of stimulating T cells, it has been hypothesized that delivering neoantigens to induce neoantigen-specific T cells could improve treatment outcomes, including the elimination of micrometastases and containment of recurrence.
A strategy to test this hypothesis is therapeutic mRNA vaccines supported by adjuvants [9].
The mRNA sequence required to encode multiple neoantigens is rapidly manufactured as patient-specific personalized vaccines [10]. These vaccines activate antigen-presenting cells [11] [12] [13] [14]. The efficient delivery of the mRNA vaccine into the body has been fine-tuned during clinical development [15].
EVIDENCE
The NCT04161755 phase 1 (non-randomized, open-label, multicenter) clinical trial invited adult patients (n=16) with pancreatic ductal adenocarcinoma (T1–3, N0–2, M0) who underwent complete surgical resection. Macroscopic completeness (R0 and R1) of the latter was confirmed histologically.
The subjects received the following sequential treatment:
- Tecentriq (atezolizumab). A PD-L1 blocker by Roche, six weeks after resection, with one 1200-mg dose.
- Autogene cevumeran (BNT122, RO7198457). A personalized mRNA oncovaccine was prepared using the proprietary biotechnology platform iNeST (individualized Neoantigen Specific Therapies). The vaccine was encapsulated in lipoplex nanoparticles and contained up to 20 immunodominant neoantigens with high affinity to major histocompatibility complexes class I (MHC-I) and MHC class II (MHC-II) [1] [2]. The vaccine was administered weekly 9 weeks after resection, with 8 priming doses and 1 booster dose, each dose being 25 µg.
- The mFOLFIRINOX chemotherapeutic regimen (folinic acid, fluorouracil, irinotecan, and oxaliplatin), 21 weeks after resection, with 12 cycles.
The aim was, first, to amplify neoantigen-specific T cells that were suppressed by PD-1 signaling, second, prime naïve T cells to vaccine neoantigens, and third, achieve a synergistic effect of systemic chemotherapeutics.
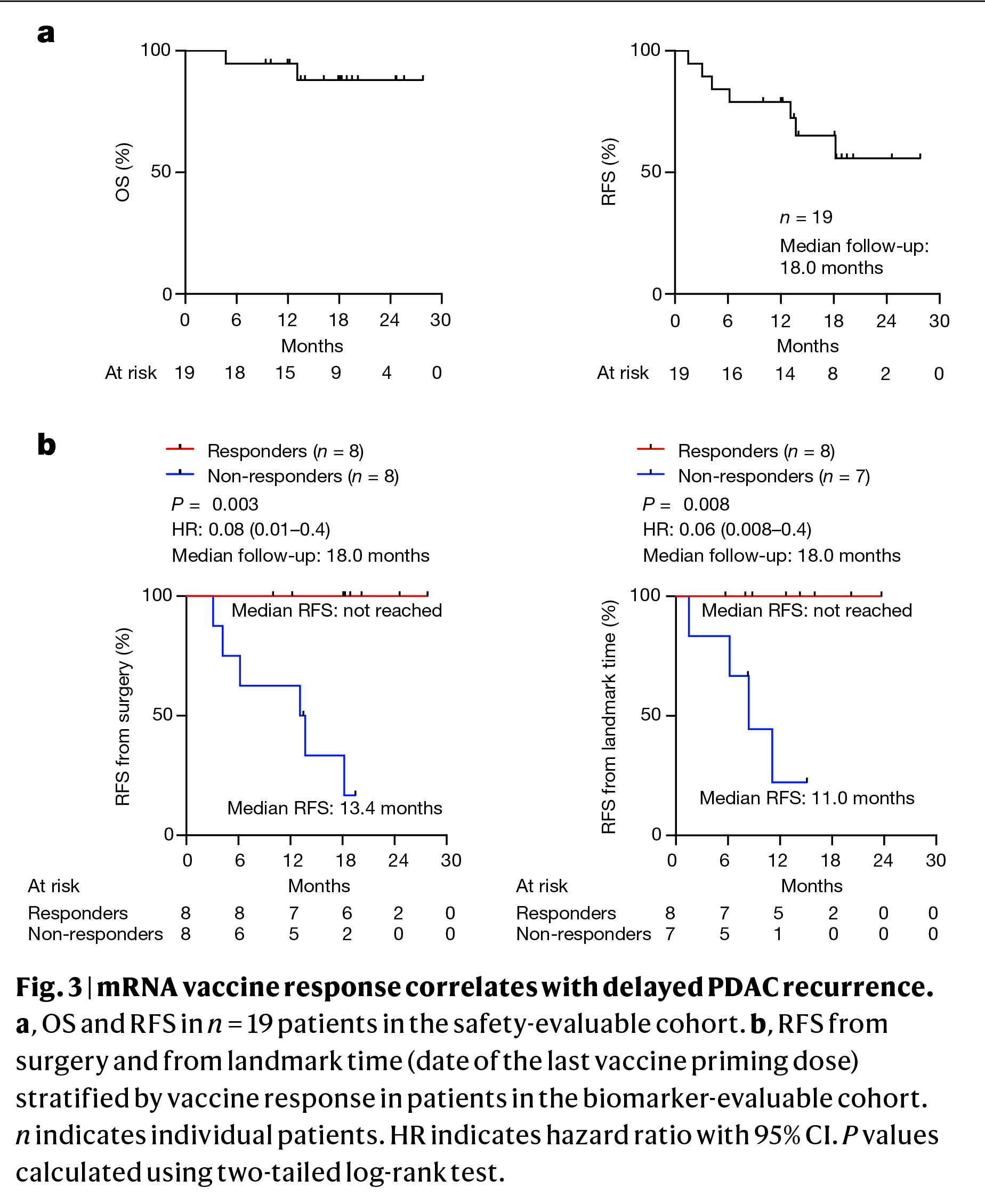
After a median of 18 months of follow-up, the results were as follows [3].
In the cohort of patients (n=19) evaluated for treatment safety, median overall survival (OS) and median recurrence-free survival (RFS) were not achieved.
In the cohort of patients (n=16) evaluated for biomarkers, the median RFS was not reached in the 8 responders to autogene cevumeran therapy, while it was 13.4 months in the 8 non-responders (hazard ratio [HR] 0.08, 95% CI [hereafter]: 0.01–0.40; p=0.003).
This indicates that the administration of a therapeutic personalized cancer vaccine reduced the risk of recurrence or death in pancreatic cancer by 92%.
A landmark analysis was conducted to exclude time-to-response bias and to correlate RFS with response in patients who did not experience a recurrence throughout receiving all 8 doses of autogene cevumeran. The analysis found no median RFS among responders — versus 11.0 months among non-responders (HR 0.06 [0.008–0.4; p=0.008]).
Additionally, responders consistently had lower serum CA19-9 levels, which is the most widely used clinical biomarker of pancreatic cancer [4], when compared to non-responders.
To eliminate the possibility that the respondents were merely patients with a better prognosis, it was verified that the response to atezolizumab, lymph node positivity, margin positivity, primary tumor size, the number of chemotherapy doses, and density of intratumoral CD8+ T cells did not correlate with the response to the mRNA vaccine in any way.
Responders and non-responders had similar immunological fitness, producing equivalent humoral and cellular responses to another mRNA vaccine (against SARS-CoV-2 coronavirus) administered concomitantly with autogene cevumeran.
Both groups had comparable peripheral frequencies of all major innate and adaptive immune cells, as well as similar somatic and germline genetic characteristics.
Thus, the T-cell response enhanced by autogene cevumeran not only correlated with delayed recurrence of pancreatic cancer but was also not associated with differences in patient selection, intratumoral T cell or peripheral T cell frequencies or fitness.
UPDATE
After a median follow-up of 3 years (range 2.3–3.8), responders continued to demonstrate RFS, with median not reached. In contrast, non-responders had a median RFS of 13.4 months (HR 0.14 [0.03–0.60]; p=0.007) [1] [2]. This indicates an 86% reduction in the risk of recurrence or death.
Two respondents experienced recurrence, which was associated with lower aggregate vaccine-induced T cells compared to respondents without recurrence.
After treatment, 75% (n=6/8) of patients remained in remission, while 88% (n=7/8) of non-responders experienced recurrence.
Autogene cevumeran induced 79 different neoantigen-specific CD8+ T cell clones with an estimated median lifespan of 5.5 years (1.3–70.2), according to pre- and post-vaccination T-cell receptor beta chain variable regions (TCRVβ) sequencing. Each patient had a median of 8 (2–28) clones. Since 98% of these clones were not present before vaccination, it is assumed that the therapeutic personalized cancer vaccine induced them de novo.
After 3 years, the majority (85%) of the new T-cell clones continued to persist in responders, which likely contributed to the prolongation of their recurrence-free survival compared to non-responders.
WHAT’S NEXT
BioNTech is exploring ways to increase the breadth and depth of the therapeutic response to its therapeutic personalized cancer vaccine, autogene cevumeran, by improving the vaccine’s efficacy through the identification of more neoantigens. This involves optimizing its potential and expanding the neoantigen identification space to include genetic aberrations beyond single nucleotide polymorphisms (variations, insertions, or deletions) in the mRNA oncovaccine, such as fusions.
The question of whether vaccine-induced clonal T cell diversity contributes to sustained disease control remains unanswered [1] [2]. However, it has been observed that tumors in vaccine responders were more clonal, which may indicate immune-mediated development, as seen in long-term survivors with pancreatic cancer [3].
A more clonal primary tumor is likely to reflect the immune system’s ability to recognize the tumor and respond to the vaccine. Once again, it is supported by evidence that the quality of neoantigens [3] [4] [5], which are markers of tumors with the most immunodominant neoantigens, correlates with immunogenic vaccine neoantigens. This reinforces the concept that optimal neoantigen selection is necessary.
Validation of a therapeutic personalized cancer vaccine, autogene cevumeran, was performed in the adjuvant (post-operative) setting. Historically, vaccines have demonstrated greater efficacy in prophylactic challenges rather than therapeutic ones against infectious pathogens. This is likely due to the fact that vaccine efficacy requires an optimally functioning host immune system.
An active tumor that interferes with the proper functioning of the immune system, along with insufficient knowledge on inter-tumor neoantigen heterogeneity, may hinder responses to cancer vaccination. Therefore, BioNTech is intentionally pursuing a clinical validation approach for autogene cevumeran in patients with minimal residual disease. The goal is to delay recurrence or death to the greatest extent possible.
For patients who have undergone complete resection of pancreatic ductal adenocarcinoma, are currently disease-free, and have not yet received first-line systemic treatment, the IMCODE003 (NCT05968326) phase 2 clinical trial is comparing the triple combination of autogene cevumeran, Tecentriq, and mFOLFIRINOX to the standard of care, mFOLFIRINOX.
In patients with high-risk (stage II–III) colorectal cancer who have undergone complete resection and have detectable circulating tumor DNA (ctDNA), indicating a potential recurrence within two to three years after surgery, a phase 2 clinical trial (NCT04486378) is ongoing. The trial compares the administration of autogene cevumeran with the standard watchful waiting approach.
Of particular note is IMCODE001 (NCT03815058), a phase 2 clinical trial investigating the first-line treatment of metastatic (recurrent or de novo at stage IV) or nonresectable locally advanced (at stage IIIC–D) melanoma with the combination of autogene cevumeran and Keytruda (pembrolizumab), a PD-1 blocker by Merck & Co. The standard treatment for the control group is pembrolizumab alone.