SUMMARY
- Liver cancer still remains a highly deadly disease.
- All existing drugs only provide marginal life extension for unresectable liver cancer.
- A personalized cancer vaccine offers the potential for complete remission or cure.
- However, this treatment is customized for each patient.
- The cost of such treatment is also a significant consideration.
WHAT HAPPENED
Geneos Therapeutics is developing therapeutic personalized cancer vaccines.
Their lead experimental oncovaccine, GT-30, is being studied for the immuno-oncology treatment of advanced liver cancer (hepatocellular carcinoma).
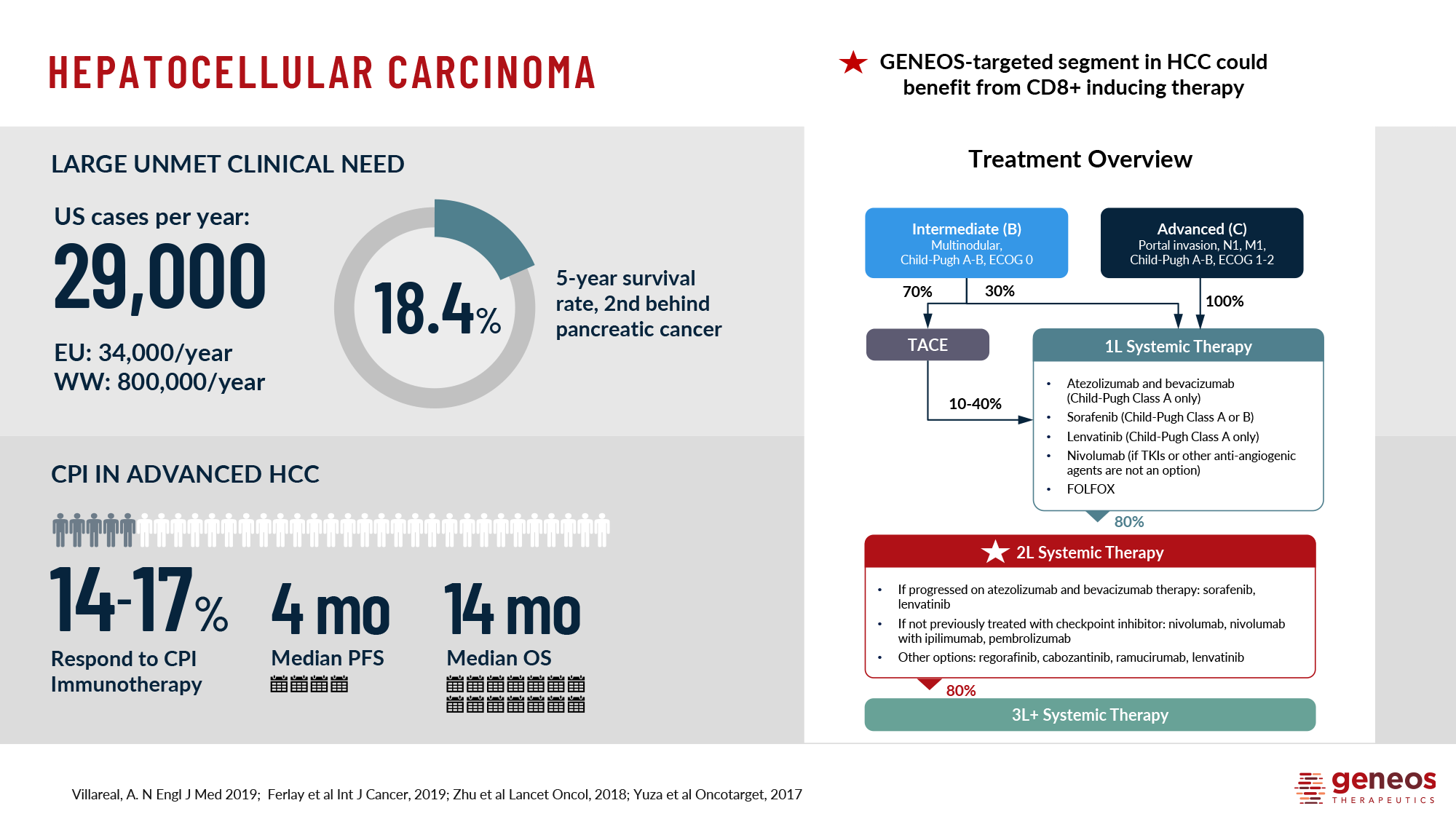
Second-line therapy, which is performed after standard frontline treatments such as Nexavar (sorafenib) or Lenvima (lenvatinib), has brought a significant proportion of patients with unresectable or metastatic liver cancer to a state of remission. This opens the door to potentially curative surgery along with radiation.
From a patient life extension perspective, the clinical efficacy of GT-30 has surpassed all approved pharmacological approaches for the treatment of advanced liver cancer.
Overall, the situation is slowly but surely improving. Four decades ago, the five-year relative survival rate for liver cancer in the U.S. was a tiny 3%. Today, it has increased to 22% [1]. However, this rate is decidedly insufficient and follows a relative survival rate of a paltry 13% for pancreatic cancer [2] [3].
In any case, despite the impressive progress of medical science, it is still very, very early to talk about victory over liver cancer.
WHY IT MATTERS
Hepatocellular carcinoma (HCC) is the most common form of primary liver cancer [1] and is a leading cause of cancer-related deaths worldwide [2]. Each year, over 860,000 diagnoses of liver cancer are made, resulting in more than 760,000 deaths [3] [4]. Liver cancer typically develops in individuals with liver cirrhosis and is often linked to risk factors such as viral hepatitis B or C, excessive alcohol consumption, and non-alcoholic fatty liver disease (NAFLD) associated with metabolic syndrome and diabetes mellitus (DM) [5] [6] [7] [8]. Unfortunately, HCC is often not diagnosed until it has progressed to an advanced stage, making surgical intervention (which in theory can cure it) ineffective for approximately 60% of cases [9] [10] [11] [12]. Current drugs for advanced HCC have very modest therapeutic efficacy, essentially failing to offer patients any appreciable chance of survival [13] [14] [15] [16].
APPROACH
Geneos Therapeutics, as a spin-off biotech startup of Inovio Pharmaceuticals, officially came on investors’ radar in February 2019. To date, Geneos has raised $44.5 million in third-party funding [1] [2].
While parent Inovio is immersed in “popular” diseases like human papillomavirus (HPV)–induced dysplasia, Geneos has bet on pathologies that are very difficult to get close to due to the obvious complexities of treatment. The startup is currently concentrating on treating two types of cancer: advanced hepatocellular carcinoma and newly diagnosed glioblastoma with unmethylated MGMT promoter.
Geneos has licensed Inovio’s proprietary DNA vaccine creation and delivery technologies.
The SynCon process generates DNA sequences that carry selected antigens and are optimized to improve mRNA stability, ribosome loading, and antigenic protein expression. The vaccine consists of plasmids that embed the finalized DNA sequence. The vaccine is injected intradermally or intramuscularly.
To facilitate the entry of plasmids into the cells, a device called Cellectra is used to organize electroporation. This process involves a series of brief electrical impulses that cause the cell membranes to open. After a few hours or days, the cells begin to synthesize antigens. This presentation to the immune system triggers the production of antibodies and killer T cells, “energize” the body with the ability to fight tumor cells.
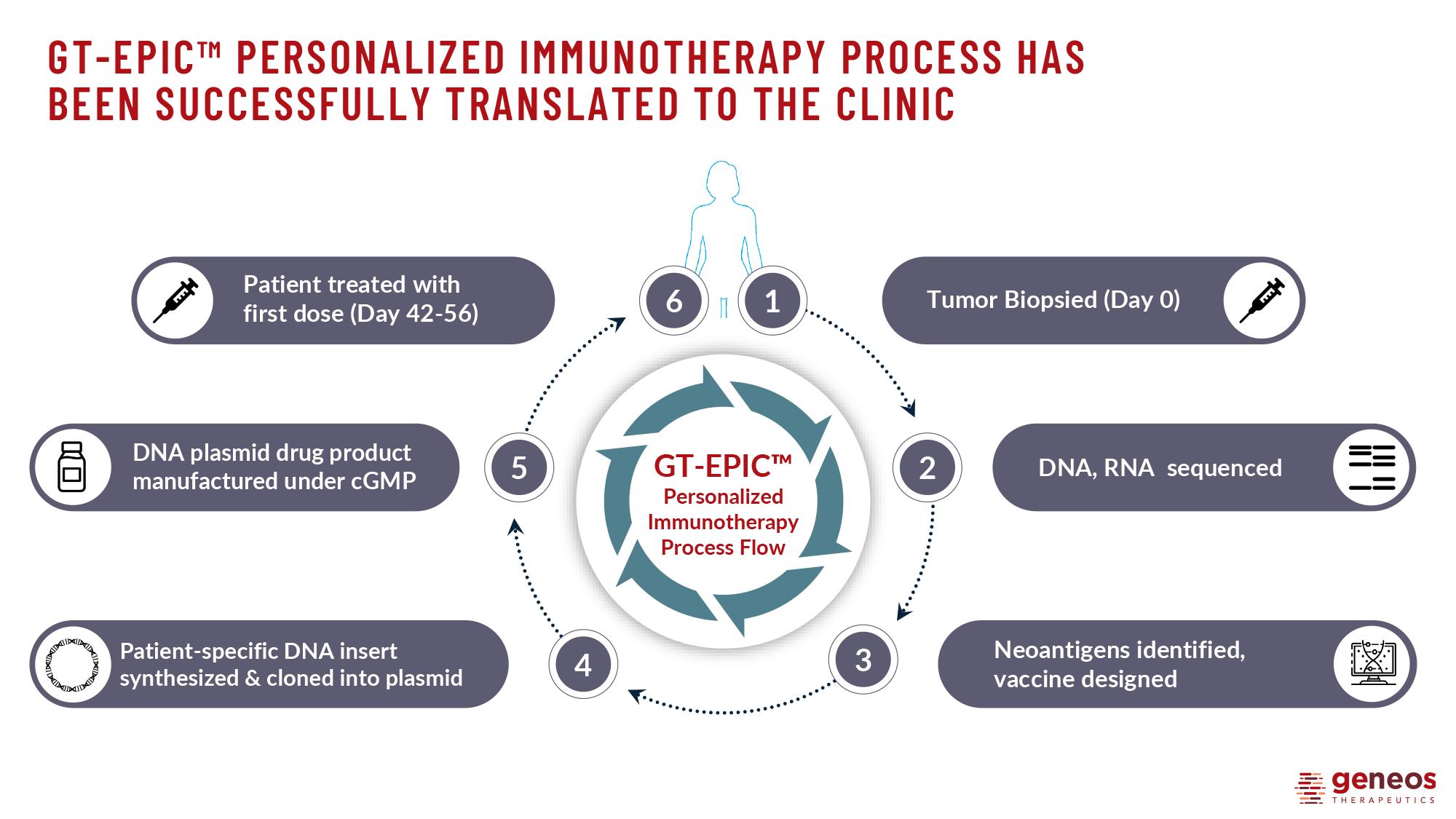
Geneos has developed the GT-EPIC personalized immunotherapy platform by combining these technologies. The platform is used to create a patient-specific vaccine DNA plasmid that encodes neoantigens, which are abnormal mutations or variations in the genome produced by cancer cells, derived from the RNA of tumor biopsies.
The oncovaccine is then combined with another DNA plasmid that encodes the cytokine interleukin 12 (IL-12), which acts as an adjuvant. The combo molecule is administered intradermally using a Cellectra electroporation device. The immuno-oncological therapeutic mixture activates neoantigen-specific CD4+ T helper cells and CD8+ killer T cells, which destroy cancerous cells.
EDGES
Geneos believes that the GT-EPIC platform has several advantages over competitors’ solutions for personalized cancer treatments such as neoantigenic vaccines and cell therapies.
First, plasmids stimulate CD4+ and CD8+ T-cell responses, which is typical for viral vector–based vaccines but more difficult for protein-based or peptide-based vaccines. This is because both plasmids and viral vectors induce antigen expression inside cells. To generate a stable and robust CD8+ T-cell response, antigens must be present on class I molecules of the major histocompatibility complex (MHC-I), i.e. processing and presenting must occur intracellularly.
Second, plasmids have a high payload capacity, enabling them to encode a larger number of different antigens compared to viral vectors. In ongoing clinical trials, Geneos utilizes up to 40 neoantigens per patient. However, preclinical studies suggest that it is possible to encode many more, up to 80, without any issues. The idea is to expose the patient’s immune system to as many target neoantigens as possible, allowing it to determine which ones will best stimulate an immune response and result in optimal clinical efficacy.
The industry is debating whether neoantigens with suboptimal antitumor effects can block more productive neoantigen responses through immunodominance. Geneos, which relies on clinical data, takes the position that patients who have received more neoantigens respond better to treatment than those who have received fewer of them.
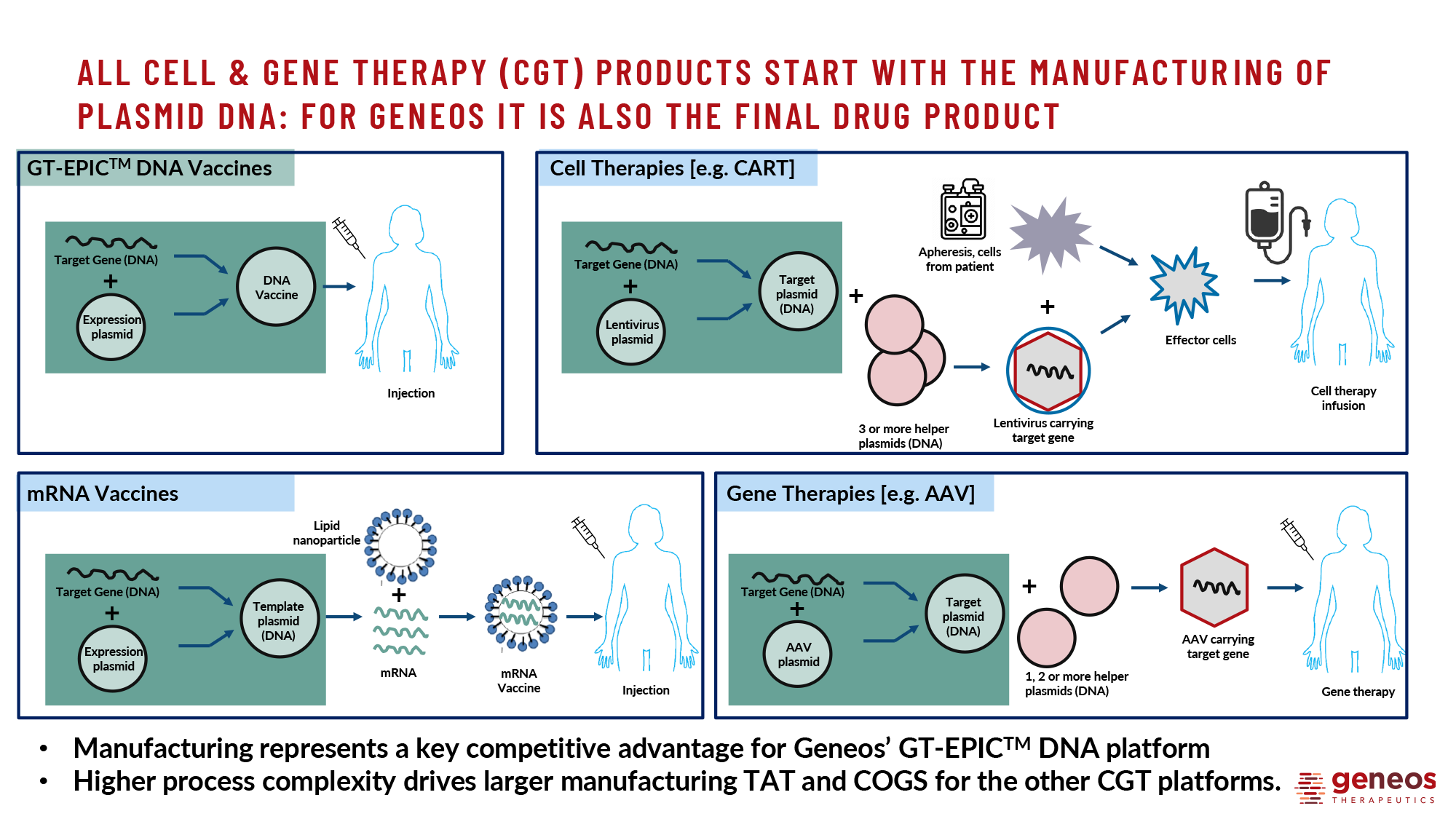
When comparing DNA vaccines to mRNA vaccines, the latter are still more optimal in terms of payload delivery. This is because they only need to cross the plasma membrane to trigger the production of protein antigens. In contrast, DNA vaccines must pass through the nuclear envelope, which reduces their final efficacy. However, DNA vaccines offer the advantage of greater stability, allowing for storage at 2–8 ℃ for years, making them more practical for distribution in developing countries and rural areas without adequate cold storage infrastructure.
Third, the GT-EPIC platform has a relatively low production cost and shorter plasmid manufacturing time compared to vaccines based on adenovirus vectors, mRNA, or CAR T cell therapy. The aspect of pricing will enable a genuine democratization of personalized cancer treatment.
Additionally, the high speed of creating pre-made plasmids within 6–8 weeks (which will later be reduced to 3–4 weeks) is crucial for patients with advanced cancer. These patients cannot afford to wait for 4–6 months for a personalized drug due to the rapid progression of cancer. The speed at which plasmids can be prepared also allows for the treatment of cancer at early stages, without the need for surgery.
BEGINNING
Geneos’ lead experimental cancer vaccine program, GT-30, focuses on treating advanced hepatocellular carcinoma through the above-described immunotherapy combined with Keytruda (pembrolizumab), a PD-1 blocker by Merck & Co.
The program targets liver cancer due to its “cold” tumors lacking tumor infiltrating lymphocytes (TILs), making tumor cells decidedly insufficiently responsive to PD-(L)1 inhibitors alone.
GT-30 can transform “cold” tumors into “hot” immunogenic ones by priming (triggering) a T-cell response in the periphery, away from the tumor. This therapy overcomes certain key resistance mechanisms involved in liver cancer by effectively “driving” T cells into tumor cells.
In November 2022, Geneos demonstrated that administration of GT-30 resulted in a disease control rate (DCR) of 54% (n=13/24) of patients, with 13% (n=3/24) of individuals achieving complete response (CR), that is, going into remission [1].
In comparison, in liver cancer treatment, Keytruda alone does not exceed 4% CR.
An analysis of the T-cell receptor (TCR) repertoire in peripheral blood and tumor tissue was performed before and after immuno-oncology vaccination. The analysis detected new or proliferated T cell clones, predominantly with activated CD8+ phenotype, in all patients. By week 9 of treatment, these clones had infiltrated the tumor microenvironment (TME), which likely contributed to tumor regression.
NOW
The GT-30 (NCT04251117) phase 1b/2a (non-randomized, open-label, multicenter) clinical trial enrolled adult patients (n=36) with hepatocellular carcinoma (HCC) who had previously received prior first-line treatment with tyrosine kinase inhibitors Nexavar (sorafenib) or Lenvima (lenvatinib) and either experienced disease progression or developed intolerance.
Subjects’ unresectable HCC had to be, according to the Barcelona Clinic Liver Cancer (BCLC) staging system, either stage C (advanced stage) or stage B (intermediate stage) not amenable to or refractory to locoregional therapy.
The participants received a combination of immuno-oncology treatments, including a personalized neoantigenic DNA vaccine (GNOS-PV02), an interleukin 12 (IL-12) encoding plasmid (INO-9012), and the PD-1 blocker Keytruda (pembrolizumab).
At the time of data analysis, which took place after a median follow-up of 21.5 months, 34 of 36 patients had undergone at least one repeat scan, allowing for assessment of treatment response according to RECIST 1.1 criteria.
- Two patients discontinued therapy due to treatment-unrelated serious adverse events (AEs) but were still included as non-responders in the full data analysis.
The overall response rate (ORR) was 31% (n=11/36). The complete response (CR), i.e. the remission of HCC, was achieved by 8% (n=3/36) of subjects [1] [2] [3].
Furthermore, a fourth patient, whose disease was initially unresectable, achieved complete remission of all tumor lesions (primary in the liver and metastatic in the lungs) after receiving the fifth dose of a therapeutic personalized cancer vaccine. This allowed the patient to undergo potentially curative surgical resection along with radiation therapy.
Partial response (PR) was achieved in 22%(n=8/36) of patients, disease stabilization (SD) was recorded in 25% (n=9/36) of individuals, and liver cancer progression was encountered in 39% (n=14/36) of participants.
Therefore, the disease control rate (DCR), which is the sum of CR, PR, and SD, was 56% (n=20/36).
The study confirmed the reliability of a third-generation ultrasensitive assay that assesses circulating tumor DNA (ctDNA) levels in determining current disease status, whether it is progression or regression.
- The ctDNA assay has high prognostic value. A decrease in ctDNA levels in liver cancer usually precedes an improvement in MRI findings. This is especially true since foci of HCC, as judged by MRI, often do not resolve completely despite the absence of clinical signs of residual disease.
The median duration of response (DOR) was not reached, the median progression-free survival (PFS) was 4.2 months, and the median overall survival (OS) was 19.9 months.
The experimental treatment demonstrated an acceptable safety profile, which was generally not different from that of pembrolizumab alone. No serious AEs were reported after administration of the cancer vaccine. The most frequent AEs were injection site reactions, which were transient and mild in severity.
ESSENSE
The current scientific progress in the development and clinical use of cancer-fighting mRNA vaccines is characterized by the fact that these agents are primarily used in an adjuvant mode to prevent recurrence after surgical removal of the tumor. It is commonly perceived that therapeutic personalized cancer vaccines are only effective after resection, and not before, meaning they are supposedly ineffective in the treatment of advanced, unresectable, or metastatic tumors. However, the positive outcomes of Geneos’ GT-30 DNA vaccine, which have resulted in complete responses in patients with late-stage advanced liver cancer that had not undergone surgery, suggest that this statement may be incorrect.
TAKEAWAYS
Treatment of advanced hepatocellular carcinoma (HCC) with GT-30, a therapeutic personalized cancer vaccine (PCV), found a response in one-third of patients (ORR 31%), a very respectable rate.
Several clinical trials have evaluated the efficacy of PD-(L)1 blockers, including Keytruda (pembrolizumab), Opdivo (nivolumab), Imfinzi (durvalumab), and Tevimbra (tislelizumab), as monotherapy for the first-line and second-line treatment of advanced HCC. The objective response rates (ORRs) ranged from 12% to 18% [1] [2] [3] [4] [5] [6] [7] [8].
Furthermore, GT-30 resulted in a complete response rate of 8% and a median overall survival of 19.9 months. In contrast, immune checkpoint inhibitors (ICIs) only achieved these rates in the more modest ranges of 2%–4% and 13.2%–16.6 months. However, the oncovaccine did not significantly slow disease progression.
PD-(L)1 blockers used as monotherapy are practically ineffective in producing a complete response in HCC due to immune resistance caused by the specificity of the tumor microenvironment and low tumor mutational burden (TMB) [9].
On the contrary, personalized immunotherapy, due to its ability to induce tumor-specific T-cell responses, sensitizes tumors to the administration of ICIs, which, by “taking the brakes off” the immune system, begin to work properly [10] [11] [12] [13] [14] [15].
In general, Geneos’ approach has been repeatedly validated by developers of other therapeutic PCVs in both preclinical studies [16] [17] [18] [19] and clinical trials in melanoma, glioblastoma, pancreatic cancer, non-small cell lung cancer, and bladder cancer [20] [21] [22] [23] [24] [25] [26]. However, it was Geneos that was one of the first to demonstrate with confidence that the method works effectively in tumor types that are much less immunotherapy-responsive, such as HCC.
Monotherapy with monoclonal antibodies against PD-(L)1 is known to reverse T-cell dysfunction in existing neoantigen-specific T cell clones, but cannot induce new neoantigen-specific T cell clones [27] [28].
According to immunological analysis, the addition of the oncovaccine GT-30 overcame this unfortunate limitation, allowing both the induction of new T cell responses to its encoded neoantigens and the expansion of the T-cell receptor (TCR) repertoire in peripheral blood and tumor. According to single-cell sequencing analysis, the major contribution to the expansion of the T cell pool was made by effector CD8+ memory T cells.
Geneos continues to emphasize the rationale for including as many different target neoantigens as possible in a therapeutic oncovaccine, without neglecting driver and passenger, truncal and branch, shared and private mutations, as well as neoantigenic epitopes with a wider range of predicted binding affinity to human leukocyte antigen (HLA) class I molecules. The maximized repertoire of neoantigens delivered by a cancer vaccine leads to the engagement of a broader set of immune responses, thereby improving the chances of successful treatment.
In addition, it has been hypothesized that associated factors, such as tumor microenvironment and immune adaptation, may play a critical role in the nature of the clinical response [29].
A limitation of the GT-30 oncovaccine is the possible early acquisition of resistance to it due to neoantigen loss and tumor heterogeneity. A solution may be the collection of tumor DNA samples from multiple foci combined with the rapid synthesis of new versions of a personalized vaccine to regain control of therapy-resistant foci.
PERSPECTIVES
Therapies for unresectable liver cancer are evolving rapidly, and it is likely that therapies with better clinical outcomes than the GT-30 oncovaccine will be available in the foreseeable future.
For example, immunotherapeutic combinations of atezolizumab and bevacizumab, durvalumab and tremelimumab, camrelizumab and rivoceranib have already been approved, and patients have responded very well [1] [2] [3].
However, the personalized treatment of hepatocellular carcinoma proposed by Geneos has the undeniable advantage of high safety. Competing therapeutic approaches, on the other hand, are characterized by an increased risk of serious or severe immune-mediated adverse events, i.e. not all patients are suitable for their use. Therefore, the GT-30 oncovaccine will certainly take its rightful place in the armamentarium of liver cancer treatment.
FUTURE
Like any new field of medicine, therapeutic personalized cancer vaccines (PCV) have a long development path with many ups and downs.
The evolution of this field is reminiscent of the history of current cancer immunotherapy, which, despite many experimental failures, eventually gave hope to patients with solid and hematologic tumors. Thus, for almost 20 years, numerous clinical trials of monoclonal antibodies failed to demonstrate reproducible efficacy before rituximab entered the scene in 1997 [1]. For many years, PD-(L)1 blockers showed no significant clinical benefit until the first results with nivolumab were published in 2008 [2]. For many years, CAR T cells failed to become a successful therapeutic modality [3].
Oncovaccines, tailored to the tumor specificity of the individual patient, have demonstrated both their own mechanistic rationale and convincing clinical results. They have reached a stage of maturity where it is safe to say that they will soon join the ranks of standard cancer therapies.
Moderna and BioNTech have been particularly successful, with their mRNA-based therapeutic PCVs having successfully completed clinical validation for the treatment of melanoma and pancreatic cancer, respectively.
The timing of immunotherapeutic vaccination remains a critical topic of debate. Personalized PCVs are often investigated in the later stages of the disease and after the use of immune checkpoint inhibitors (ICIs). However, there is an opinion that administering them earlier in therapy, such as in the neoadjuvant setting (before surgery), could provide greater benefits. This is because the patient has not yet experienced immunoediting phenomenon, T cell exhaustion, or further compromised immune system [4].