Highlights
Voxzogo (vosoritide) is a new drug indicated to increase linear growth in pediatric patients with achondroplasia who are 5 years of age and older with open epiphyses, i.e. whose bones are still growing.
Voxzogo, developed by BioMarin Pharmaceutical, was approved in November 2021 by the U.S. Food and Drug Administration (FDA). The regulatory decision has been issued under accelerated review: vosoritide has yet to definitively confirm its own therapeutic efficacy.
Voxzogo received marketing approval from the European Medicines Agency (EMA) in August 2021: vosoritide is indicated for the treatment of genetically confirmed achondroplasia in patients 2 years of age and older whose epiphyses are not closed.
In 2022, Voxzogo is expected to be available in other countries, including Australia, Brazil, Japan.
The cost of Voxzogo for U.S. patients is approximately $320,000 per year, excluding discounts and rebates. A one-year course of Voxzogo in Europe would cost $300,000. According to industry projections, vosoritide is on track to reach $1 billion in annual sales.
What Is Achondroplasia
Achondroplasia is an autosomal dominant genetic disorder that is a primary skeletal dysplasia whose main feature is dwarfism: disproportionately short arms and legs with a normally normal trunk length. The average height of an adult with achondroplasia is 131 cm in men and 123 cm in women. Other characteristic features of achondroplasia include macrocephaly (large head), specific facial features (prominent frontal tubercles and underdevelopment of the middle third of the face), excessive lumbar lordosis, varus knee deformity, and trident hands.
Complications of achondroplasia include spinal cord compression (spinal stenosis), hydrocephalus, restrictive lung disease, sleep apnea, middle ear dysfunction, orthopedic complications, obesity, and gastroesophageal reflux. Intelligence is not affected.
Achondroplasia is caused by heterozygous gain-of-function mutations affecting the gene that codes for fibroblast growth factor receptor 3 (FGFR3), which is involved in the regulation of bone growth. The mutant FGFR3 gene, being constitutively (permanently) active, initiates an excessive inhibitory signal that inhibits chondrocyte proliferation and differentiation, resulting in slower bone growth due to impaired endochondral ossification (formation of long bones and other bones).
In approximately 80% of patients with achondroplasia, the parents have normal growth, that is, FGFR3 mutations occur de novo, while the pathogenic variant is de novo inherited exclusively from the father. There is thought to be an association with advanced paternal age at the time of conception (due to intractable DNA replication defects during spermatogenesis): the incidence of achondroplasia in children whose fathers are over 50 is 1 case per 1875 live births — versus 1 per 15 000 in the general population.
Achondroplasia, which affects approximately 250 000 people worldwide, is the most common form of bone dysplasia (1 case per 20 000 live births) and the most common cause of dwarfism.
Prior to the advent of vosoritide, there were no approved treatments for achondroplasia that specifically targeted the pathophysiological processes underlying the disease.
Voxzogo: Mechanism of Action of Vosoritide for Treatment of Achondroplasia
C-type natriuretic peptide (CNP), encoded by the NPPC gene, and its cognate receptor, natriuretic receptor 2 (NPR2, NPR-B), are potent stimulators of endochondral ossification. In mice, decreased NPPC expression or NPR2 expression (or lack thereof) leads to severe dwarfism. In contrast, overexpression of NPPC in mice and NPPC in human disease models is characterized by increased production of endogenous C-type natriuretic peptide, which is mirrored by sustained excessive skeletal growth. Continuous intravenous infusion of exogenous C-type natriuretic peptide restores impaired bone growth in mice with achondroplasia and increases long bone growth in nonmutant monkeys by inhibiting the FGFR3-mediated MAPK signaling pathway.
Vosoritide (BMN 111) is a recombinant analog of C-type natriuretic peptide with an extended (due to implemented resistance to neutral-endopeptidase) elimination half-life. Daily subcutaneous injections of vosoritide promoted sustained long bone growth in juvenile mice and monkeys with a normal skeleton and resulted in correction of the dwarfism phenotype in mice with achondroplasia.
In patients with achondroplasia, endochondral bone growth is negatively regulated due to a gain-of-function mutation in FGFR3. The binding of vosoritide to NPR-B antagonizes FGFR3 downstream signaling by inhibiting extracellular signal-regulated kinases 1 and 3 (ERK1/2) in the mitogen-activated protein kinase (MAPK) pathway at the level of serine-threonine protein kinase RAF-1. As a result, vosoritide, like CNP, acts as a positive regulator of endochondral bone growth as it promotes chondrocyte proliferation and differentiation.
Voxzogo: Vosoritide for Effective and Safe Treatment of Dwarfism
The NCT03197766 phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial invited patients (n=121) aged 5–18 years with genetically confirmed achondroplasia. Participants received daily subcutaneous injections of placebo or vosoritide at a dose of 15 mcg/kg — for 52 weeks. The primary endpoint was established by a change in mean annualized growth velocity (AGV).
Baseline characteristics of subjects (placebo and vosoritide groups, respectively): mean age 9.06 and 8.35 years, male 54% and 52%, mean annualized growth velocity 4.06 and 4.26 cm per year, mean height 102.9 and 100.2 cm.
Dwarfism therapy with vosoritide provided an increase in AGV at the least-squares mean (LSM) of 1.71 cm/year (95% CI: 1.40–2.01), compared with baseline. In the placebo group, this change was 0.13 cm/year (95% CI: −0.18 to 0.45). The resulting difference of 1.57 cm/year added (95% CI: 1.22–1.93) was statistically significant (p<0.0001).

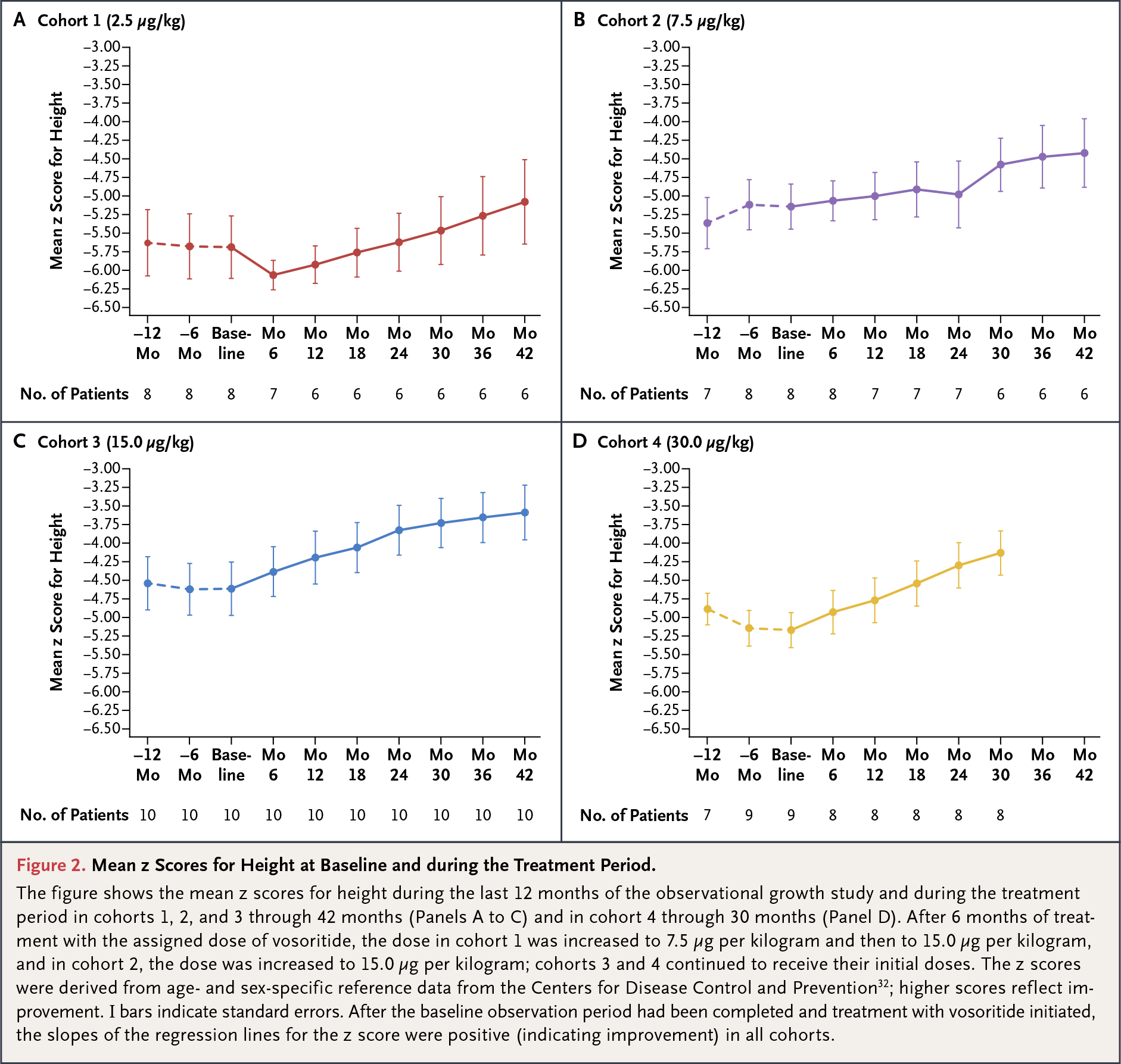
The use of Voxzogo improved the Z score, which estimates a patient’s anthropometric status (in this case, body length to age) from the median of the standard population. In the vosoritide group, the LSM-increasing height Z score was 0.27 (95% CI: 0.18–0.36) — versus a decrease of 0.01 (95% CI: −0.10 to 0.09) in the placebo group (p<0.0001). For understanding: positive values of the Z score indicate an increase in the anthropometric index compared to the standard, and negative values indicate a decrease.
However, there was no statistically significant difference (p=0.51) between the vosoritide and placebo groups in changes in the ratio between upper and lower body segments, which was calculated as the ratio between sitting and standing height, followed by subtracting standing height: −0.03 (95% CI: −0.06 to 0.00) — vs. −0.02 (95% CI: −0.05 to 0.01).
The safety profile of vosoritide was characterized by tolerability: no serious adverse reactions to the drug administration were observed. Except for some adverse events at the site of vosoritide injection, which were non-serious and transient.
Given the structural similarity between C-type natriuretic peptide, of which vosoritide is a biological analog, and endogenous atrial natriuretic peptide (ANP), periodic monitoring of pulse rate and blood pressure was performed. The vascular side effects of vosoritide were found to be mild, transient, and clinically insignificant in the form of self-limiting changes in blood pressure.
According to the reviewers of the clinical study, long-term use of vosoritide on a continuous basis can lead to a sustained and beneficial effect in the form of proportional skeletal development. As a result, a person suffering from achondroplasia who adheres to Voxzogo treatment will achieve a significant increase in his or her own growth.
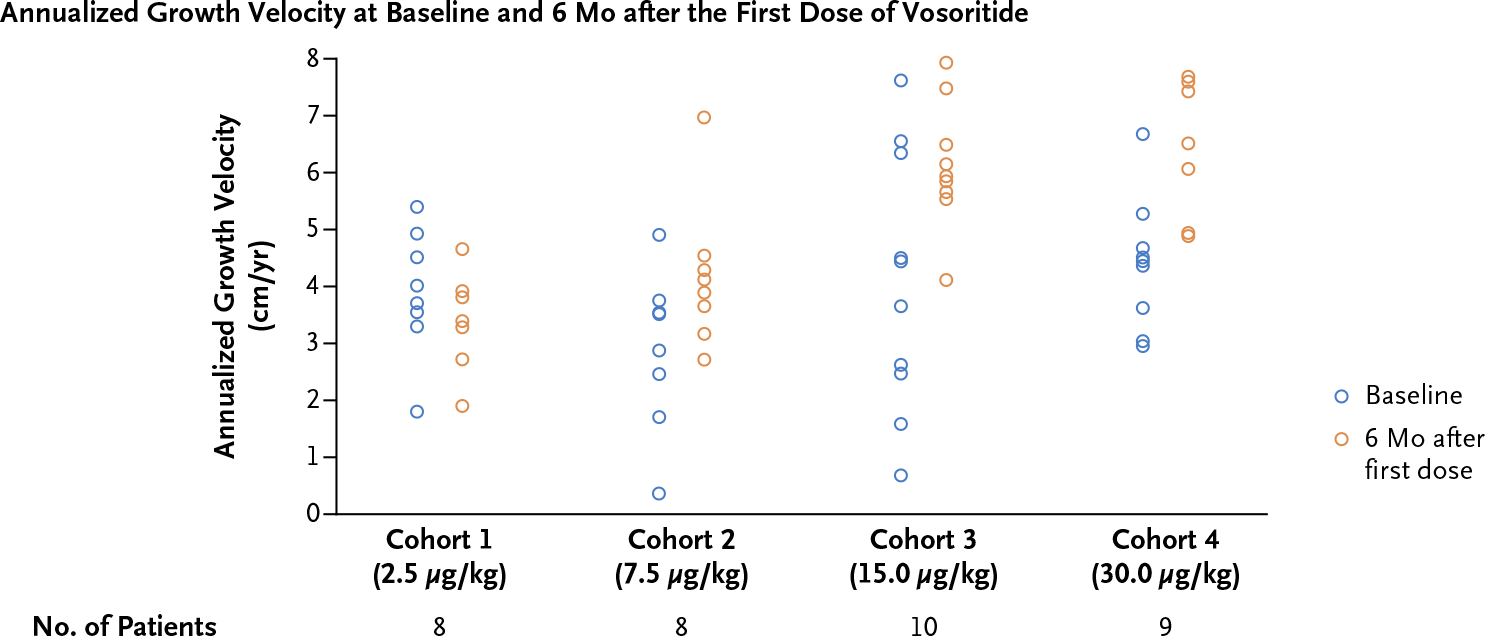
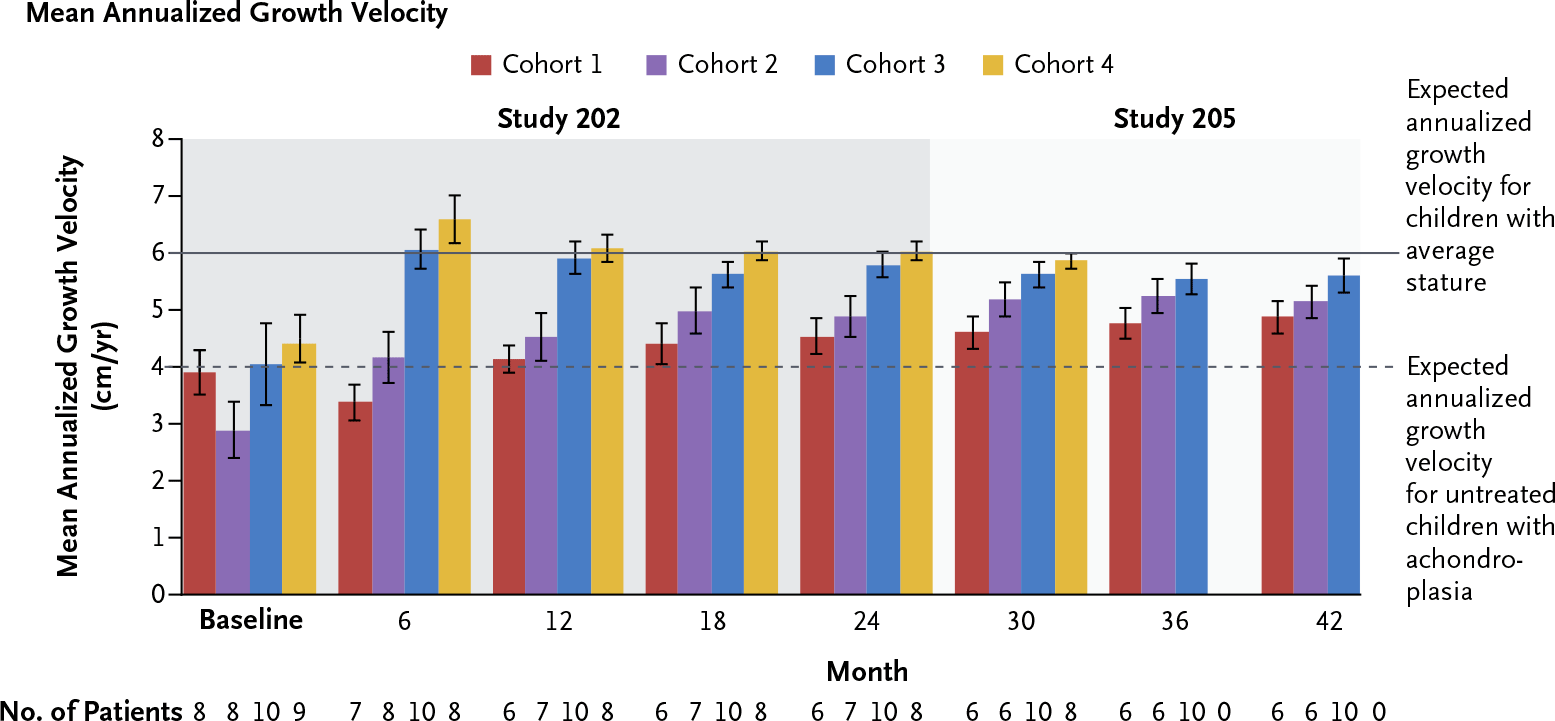
BioMarin also reported results from the NCT02055157 phase 2 (nonrandomized, open-label, multicenter, international) clinical trial that enrolled patients (n=35) aged 5–14 years with genetically confirmed achondroplasia and then from the NCT02724228 phase 2 follow-up that continued the subjects.
During follow-up up to 3.5 years, it was found that administration of Voxzogo resulted in sustained annualized growth velocity of 1.10–2.34 cm/year — in various dose cohorts. Vosoritide helped increase growth by a maximum of 9.0 cm.
Vosoritide and Treatment of Achondroplasia: What’s Next
BioMarin understands that vosoritide has left many questions unanswered and unresolved, organized the NCT03424018 phase 3 (non-randomized, open-label, multicenter, international) clinical trial, in which it invited participants who underwent NCT03197766. This long-term trial, which will continue until patients with achondroplasia reach their final adult height, will definitively establish the balance between the benefits and harms of vosoritide. In addition, it will be determined exactly how vosoritide affects quality of life, daily activity, and changes in the frequency and type of medical and surgical interventions. It will also be answered whether vosoritide provides a growth spurt during puberty that is absent in achondroplasia.
In parallel, the NCT03583697 phase 2 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial in which vosoritide is being tested in the treatment of patients (n=70) of infant and pediatric age (maximum 5 years) diagnosed with achondroplasia. It is necessary to understand whether such early pharmacotherapy of dwarfism is justified and whether its significant medical complications, such as foramen magnum stenosis with brainstem compression, can be addressed.
Vosoritide and Treatment of Dwarfism: Competitive Environment
BioMarin is not alone, other players in the pharmaceutical industry are trying to meet the challenge of treating achondroplasia. Thus, Denmark’s Ascendis Pharma is developing TransCon CNP (ACP-015), another analog of C-type natriuretic peptide, which, unlike vosoritide, is characterized by a much longer elimination half-life.

In the ACcomplisH (NCT04085523) phase 2 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial, subcutaneous injections of 6 mg/kg TransCon CNP are given once weekly to prepubertal children (n=60) aged 2–10 years with a genetically confirmed diagnosis of achondroplasia.
TransCon CNP refers to the proprietary TransCon (transient conjugation) technology developed by Ascendis to release the drug at a predetermined rate regulated by physiological conditions, which provides optimal therapeutic effect against the background of convenient dosing. TransCon molecules include three components: an unmodified drug, an inert carrier that protects the latter from clearance, and a linker that temporarily binds them. After subcutaneous injection into the human body and when specific pH and temperature parameters are met, the linker breaks down, releasing the drug.
Pfizer, through its July 2019 acquisition of Switzerland’s Therachon, is working on recifercept (PF-07256472, TA-46), a recombinant protein that is a soluble form of fibroblast growth factor receptor 3 (FGFR3) and acts as a decoy receptor to prevent fibroblast growth factor (FGF) from binding to mutant FGFR3.
Resifercept, administered weekly subcutaneously in three different doses, is in the NCT04638153 phase 2 (randomized, open-label, multicenter, international) clinical trial among patients (n=63) aged 3 months to 10 years with a genetically confirmed diagnosis of achondroplasia.
QED Therapeutics, a division of BridgeBio Pharma, is involved in oral small-molecule infigratinib (BGJ398), an ATP-competitive tyrosine kinase receptor inhibitor of fibroblast growth factor receptors 1, 2, and 3 (FGFR1, FGFR2, FGFR3).
Preclinical data suggest that low-dose infibratinib has a potentially better efficacy profile demonstrated in a mouse model of achondroplasia — compared to other anti-dwarfism drugs such as vosoritide, TransCon CNP, and resifercept.

Infibratinib is being tested in the PROPEL 2 (NCT04265651) phase 2 (nonrandomized, open-label, multicenter, international) clinical trial among children (n=60) aged 3–11 years with a genetically confirmed diagnosis of achondroplasia, participants are given the drug daily (four dose cohorts).
Japan’s Ribomic has relied on aptamers, short, single-stranded nucleic acid molecules that are matched in vitro to a given target based on high and specific affinity. Oligonucleotides are modified to resist ribonucleases and have the ability to fold to form a three-dimensional structure that binds to the target.
PEGylated RNA aptamer RBM-007 (APT-F2P) being highly specific to fibroblast growth factor 2 (FGF2), one of the signaling molecules activating FGFR3, blocks FGF2 binding to its four cell receptors thus inhibiting FGF2-induced signaling and cell proliferation, and restoring osteoblast differentiation blocked by FGF2.
RBM-007, administered subcutaneously in various doses, has been successfully tested in healthy volunteers in the JapicCTI-205345 phase 1 clinical trial.
Vosoritide and Combined Treatment of Dwarfism
It is possible that in the foreseeable future, achondroplasia will be treated with a combination of several drugs from those being developed. And the point here is the following.
Vosoritide, being an analog of natural C-type natriuretic peptide, binds to NPR2, which induces synthesis of cyclic guanosine monophosphate (cGMP), which in turn inhibits MAPK signaling pathway (due to inhibition of certain enzymes). Inhibition of MAPK leads to increased production of extracellular matrix (ECM), which, along with chondrocytes, serves as a template for bone during the process of endochondral ossification.
Although vosoritide affects MAPK, it has no effect on other signaling pathways that are thought to contribute to the pathophysiology of achondroplasia, such as STAT1, Wnt/β-catenin, PI3K/AKT, PLCγ. And therefore, there is some possibility that certain patients with dwarfism will not respond adequately to vosoritide because of their resistance to C-type natriuretic peptide.

The problem can be solved by turning to synergism: the same infibratinib and resifercept affect, in addition to MAPK, STAT1 signaling pathway, and therefore it may be reasonable to add them to vosoritide. In other words, the former will ensure the proper proliferation of chondrocytes, the latter will ensure their differentiation.
Vosoritide: Rage and Discord of Dwarfs
After Little People of America (LPA) — a nonprofit patient organization founded in 1957 that provides support, resources, and information to dwarfism sufferers and their families — became aware of the development of vosoritide, it unleashed a streamlinedly angry statement. In brief, the gist of the message, which could be considered a reflection of either profound ignorance, medieval delusion, and misplaced religious humility, or a truly acute social problem, is as follows.
Little People of America is deeply committed to the notion of the value of the diversity of the human race. Dwarfism is one such value, contributing to the biological, social, and cultural diversity of humanity. We have never actively promoted medical research aimed at treating dwarfs. Nevertheless, we do not oppose them, especially when it comes to improving the quality of life of people with short stature. We urge all dwarfs and their families to thoroughly investigate pharmacological treatment options for dwarfism and make an informed decision. Informed choices are important, given that it is not known how safe the long-term effects of biotechnology on the body are. In any case, we emphasize: New treatments are not necessary for dwarfs to continue an engaging, healthy and productive life.
According to Mark Povinelli, LPA president, vosoritide is one of the most divisive things the organization has had to deal with in its six decades of existence. “We want to show that you can have a completely fulfilling life without having to worry about growth velocity,” said Mr. Povinelli, calling fixations on height a societal issue.
LPA has accomplished much in the task of changing the way the world perceives stunted people. Advocating for universal justice, it has succeeded in shattering stereotypes and has struggled to reclaim “dwarf pride” — being a little person is a unique trait to be celebrated, not a problem in need of a cure, and “dwarf pride” means thriving because of your body, not in spite of it.
The debut of the vosoritide in 2012 sharpened the ideological controversy by bringing uncomfortable social issues into the light. A parallel can be drawn here with the decades-long debate among deaf people over cochlear implants that “fix” hearing loss.
The successes of BioMarin and vosoritide are perceived by the dwarfs as an attempt to eliminate their community. “We are offered a cure, but in essence we are not sick.” Again, 80% of babies with achondroplasia are born to parents of normal height, meaning that the decision whether to give the child vosoritide will be made by people who have nothing to do with little people culture and who know nothing about “dwarf pride.”
If we look at the problem objectively, vosoritide is quite capable of becoming an alternative to limb lengthening surgery — a long and difficult procedure, which in most cases is accompanied by serious complications: fractures, muscle contractures, nerve and vessel damage, valgus deformity of the ankle, osteoarthritis with late-onset, etc.
Many dwarfs are infuriated by the LPA’s statement because it’s not so much about growth as it is about the potential improvement in quality of life that vosoritide can provide. Yes, its long-term safety is questionable, but pharmacotherapy for dwarfism is far less dangerous and painful than surgery. In addition to the fact that getting rid of achondroplasia involves eliminating common complications (spinal stenosis, brainstem compression, sleep apnea), adding a few inches solves many problems, from the nuances of feminine hygiene to pushing the button in the elevator and withdrawing money from the ATM.
What genocide of dwarfs can we even talk about if we are dealing with a common genetic disease, a serious and disabling one. Dwarfs are not a race, an ethnic group, or a separate subspecies of human beings, but only sick people.
Other people with low stature have not been affected by the disunity in the dwarf community that started because of the vosoritide. They are not going to change themselves or their dwarf children, saying that we are “not broken” to be “repaired.”
Be that as it may, no consensus has yet been formed around the vosoritide. Some dwarfs complain that the drug is insulting to them as individuals, others grieve that vosoritide did not exist when they were children. Some parents of little children see vosoritide as a source of hope for a healthy and fulfilling life for their offspring, while others see it as a threat to their sense of dignity.
BioMarin itself responds to “dwarf pride” as follows: “We cannot make a drug that enhances skeletal growth but does not make you taller.”
Extras
Voxzogo (vosoritide). Prescribing information. US. [PDF]
Voxzogo (vosoritide). Prescribing information. Europe. [PDF]
BioMarin Pharmaceutical. U.S. FDA approval for Voxzogo (vosoritide). Conference call. November 19, 2021. [PDF]
BioMarin Pharmaceutical. Virtual R&D Day 2021. November 30, 2021. [PDF]
Once-daily, subcutaneous vosoritide therapy in children with achondroplasia: a randomised, double-blind, phase 3, placebo-controlled, multicentre trial. Lancet. 2020 Sep 5;396(10252):684-692. [source]
C-type natriuretic peptide analogue therapy in children with achondroplasia. N Engl J Med. 2019 Jul 4;381(1):25-35. [source]
BridgeBio Pharma. Corporate presentation. December 2021. [PDF]