Highlights
Vivjoa (oteseconazole) is a new drug indicated for the treatment of recurrent vulvovaginal candidiasis in order to reduce its recurrence rate.
Vivjoa is indicated for treating women who are incapable of childbearing. This category includes individuals who are postmenopausal or permanently infertile biological women. The reproductive limitations of Vivjoa are due to the fact that the drug is characterized by embryofetal toxicity.
Vivjoa, developed by Mycovia Pharmaceuticals, is approved by the U.S. Food and Drug Administration (FDA) in late April 2022.
Vivjoa is the first drug approved specifically to treat recurrent vaginal yeast infection.
What Is Vulvovaginal Candidiasis
Vulvovaginal candidiasis, also known as vaginal yeast infection, is a common cause of vulvovaginitis due to the growth of Candida albicans and other Candida fungi.
Vulvovaginal candidiasis can be idiopathic or secondary to other risk factors, including antibiotic use, sexual intercourse, pregnancy, oral contraceptives, and diabetes mellitus.
Typical symptoms of vaginal yeast infection include thick white vaginal discharge, often accompanied by vulval itching and irritation, external dysuria, and/or dyspareunia.
C. albicans accounts for 85%–95% of vaginal yeast strains.
Recurrent vulvovaginal candidiasis is defined as more than 3–4 documented symptomatic separate episodes within 1 year. Recurrent disease is encountered in up to 9% of patients./

Biotechnology for Menopause and Infertility
Is it possible to prolong a women’s health and ability to get pregnant?
Uncomplicated vulvovaginal candidiasis is treated with antifungal drugs: either azole antimycotics (oral fluconazole or intravaginal clotrimazole, miconazole, tioconazole, butoconazole, or terconazole) or the polyene antimycotic nystatin intravaginally.
Treatment of complicated vulvovaginal candidiasis (severe or recurrent disease; infection caused by Candida species other than C. albicans; infection in pathological conditions) involves identifying the relevant pathogen and determining its sensitivity to pharmacotherapy. The latter, being prolonged in treatment time, may include oral fluconazole, intravaginal boric acid, nystatin or flucytosine (together with amphotericin B), as well as itraconazole, posaconazole, voriconazole, anidulafungin, caspofungin, micafungin.
Almost 75% of women have had vaginal yeast infection at least once in their lifetime, and about half of them experience repeat infections. Up to 9% of women suffer from recurrent vulvovaginal candidiasis.
Brexafemme (ibrexafungerp), a new drug for the treatment of uncomplicated vulvovaginal candidiasis, appeared in early June 2021. Ibrexafungerp, developed by Scynexis, is the first representative of a new class of antifungal drugs in more than 20 years.

Brexafemme: New Drug for Vaginal Yeast Infection
Scynexis offered ibrexafungerp, a new antifungal medication for vulvovaginal candidiasis treatment.
Vivjoa: Efficacy and Safety of Oteseconazole
The efficacy and safety of Vivjoa have been studied in three phase 3 clinical trials: the first two, identical in design, compared oteseconazole with placebo and the third with fluconazole.
Subjects aged 12 years or older had to have had three or more episodes of acute vulvovaginal candidiasis in the past 12 months.
Among the mandatory inclusion criteria were a positive test for Candida spp.; a score of clinical signs (erythema, edema, excoriations) and symptoms (itching, burning, irritation) of vulvovaginal candidiasis ≥ 3 during screening and < 3 before initiation of the treatment.
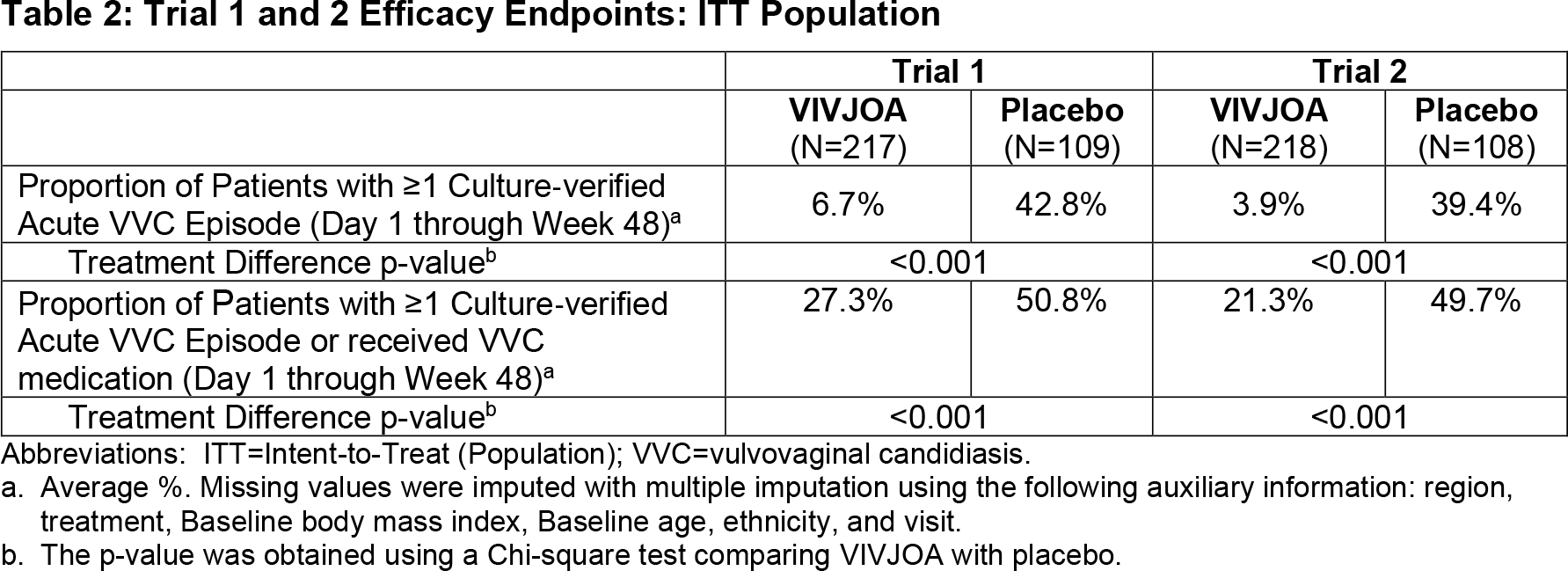
The NCT03562156 and NCT03561701 phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trials enrolled 652 women.
Initially, all participants received induction therapy: patients were given three doses of fluconazole (150 mg every 72 hours) for one week. If acute vulvovaginal candidiasis resolved after 14 days after the first dose of fluconazole, subjects were randomized: patients were given placebo or oteseconazole 150 mg once daily for 7 days and then once weekly for 11 weeks.
The primary efficacy endpoint of treatment was the proportion of patients experiencing one or more episodes of acute vulvovaginal candidiasis, confirmed to be caused by Candida spp. and with a clinical signs and symptoms score ≥ 3, within 48 weeks of randomization.
At follow-up, recurrence of vulvovaginal candidiasis was seen in 6.7% and 3.9% of patients treated with oteseconazole — versus 42.8% and 39.4% in the placebo groups (p<0.001).
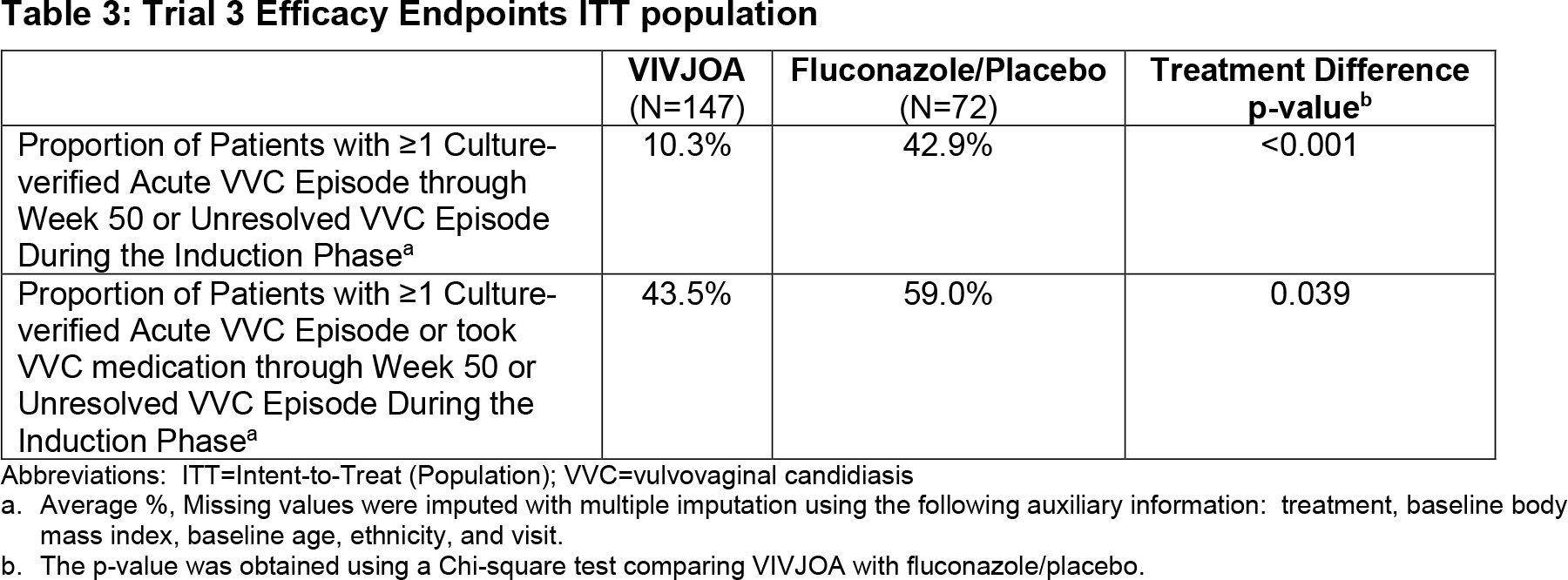
The NCT03840616 phase 3 (randomized, double-blind, placebo-controlled, multicenter) clinical trial recruited 219 women.
At the beginning, all participants received induction therapy: patients were given either two doses of oteseconazole (650 mg on day 1 and 450 mg on day 2) or three doses of fluconazole for one week (150 mg every 72 hours). If acute vulvovaginal candidiasis resolved after 14 days after the first dose of induction therapy, subjects were randomized: patients were given placebo or oteseconazole 150 mg once weekly for 11 weeks.
The primary efficacy endpoint was the proportion of patients who either experienced one or more episodes of acute vulvovaginal candidiasis, confirmed to be caused by Candida spp. and with a clinical signs and symptoms score ≥ 3, or who failed to clear their infection during the induction phase of therapy at 50 weeks post-randomization.
At follow-up, recurrence of vulvovaginal candidiasis was reported among 10.3% patients receiving oteseconazole — versus 42.9% in the placebo group (p<0.001).
Among the most common adverse reactions to Vivjoa administration were headache (in 7.4% of patients) and nausea (3.6%).
Vivjoa: Mechanism of Action of Oteseconazole
Oteseconazole (VT-1161, SHR8008) is an oral small-molecule azole metalloenzyme inhibitor that targets 14α-demethylase (CYP51), a fungal enzyme that catalyzes an early step in the ergosterol biosynthetic pathway necessary to form and maintain the integrity of fungal cell membranes. Inhibition of CYP51 results in the accumulation of 14-methylated sterols, which leads to disruption of the function of certain membrane-bound enzymes and disruption of the tight packing of phospholipid acyl chains. This is reflected by suppression of fungal growth.
Unlike previous azole inhibitors containing an imidazole or triazole motif that binds to human cytochrome P450 (CYP), oteseconazole has a tetrazole motif (a five-membered ring of four nitrogen atoms and one carbon atom) and therefore has both improved target selectivity and almost no binding to human CYP51.
For example, oteseconazole binds to fungal CYP51 about 2200 times stronger than human CYP51, while itraconazole and voriconazole bind 2 and 92 times stronger for fungal CYP51 compared to human one.
In vitro oteseconazole exhibits antifungal activity against most isolates of the following microorganisms associated with recurrent vulvovaginal candidiasis: andida albicans, Candida glabrata, Candida krusei, Candida parapsilosis, Candida tropicalis, Candida lusitaniae, Candida dubliniensis.
Oteseconazole was developed by Viamet Pharmaceuticals, which was bought in January 2018 by investment NovaQuest Capital Management. In September, the latter’s money was used to establish Mycovia.
Oteseconazole: Market Outlook
Oteseconazole became the first drug approved specifically for treating recurrent vaginal yeast infection. But Mycovia’s monopoly will soon disappear, as Scynexis prepares to expand the range of indications of Brexafemme, which has successfully passed the CANDLE (NCT04029116) phase 3 clinical trial in the task of preventing recurrences. In doing so, ibrexafungerp is not subject to any reproductive restrictions, as in the case of oteseconazole.
Oteseconazole has successfully completed a phase 2 clinical trial NCT01891331 in the treatment of acute vulvovaginal candidiasis.
Mycovia is also studying oteseconazole in the treatment of onychomycosis and invasive fungal infections.
China’s Jiangsu Hengrui Pharmaceuticals, Mycovia’s oteseconazole partner, is conducting NCT04956419 and NCT05074602 phase 3 clinical trials of this drug in treating acute and recurrent vulvovaginal candidiasis.
In October 2019, Hungary’s Gedeon Richter obtained the rights to commercialize and manufacture oteseconazole in Europe, Latin America, Australia, Russia and other CIS countries.
Extras
Vivjoa (oteseconazole). Prescribing information. US. [PDF]
Oteseconazole: an advance in treatment of recurrent vulvovaginal candidiasis. Future Microbiol. 2021 Dec;16:1453-1461. [source]
A randomized phase 2 study of VT-1161 for the treatment of acute vulvovaginal candidiasis. Clin Infect Dis. 2021 Oct 5;73(7):e1518-e1524. [source]