Highlights
Voquezna (vonoprazan) is a new drug indicated for the eradication therapy of Helicobacter pylori infection in adults.
Voquezna, which Phathom Pharmaceuticals is behind, is offered in two co-packaged variants: Voquezna Dual Pak and Voquezna Triple Pak combining vonoprazan with amoxicillin (20 mg/500 mg) and vonoprazan with amoxicillin and clarithromycin (20 mg/500 mg/500 mg), respectively.
Voquezna was approved by the U.S. Food and Drug Administration (FDA) in early May 2022.
The Voquezna Dual Pak and Voquezna Triple Pak regimens outperformed standard H. pylori eradication therapy using lansoprazole, a common proton pump inhibitor, equally in the general patient population and among those patients in whom the bacterium was resistant to clarithromycin.
Voquezna Dual Pak will reduce the antibiotic load compared to Voquezna Triple Pak, although the eradication efficacy will be slightly worse.
Voquezna Dual Pak and Voquezna Triple Pak will go on sale in the third quarter of 2022.
Voquezna is preparing to add new indications: for the treatment of erosive esophagitis (severe reflux esophagitis), non-erosive gastroesophageal reflux disease (NERD), and gastroesophageal reflux disease (GERD).
The use of Voquezna improved outcomes in treating erosive esophagitis in terms of complete healing and reduced recurrence of erosions. Using Voquezna will quickly relieve heartburn episodes associated with NERD.
Voquezna: Efficacy and Safety of Vonoprazan for Helicobacter pylori Eradication Therapy
The PHALCON-HP (NCT04167670) phase 3 (randomized, double-blind, active-controlled, multicenter, international) pivotal clinical trial enrolled adult patients (n=992) with Helicobacter pylori infection confirmed by 13C-urease breath test (UBT).
For 14 days, participants were given either twice daily lansoprazole (30 mg) with amoxicillin (1 g) and clarithromycin (500 mg), or twice daily vonoprazan (20 mg) with amoxicillin (1 g) and clarithromycin (500 mg), or twice daily vonoprazan (20 mg) and three times daily amoxicillin (1 g).
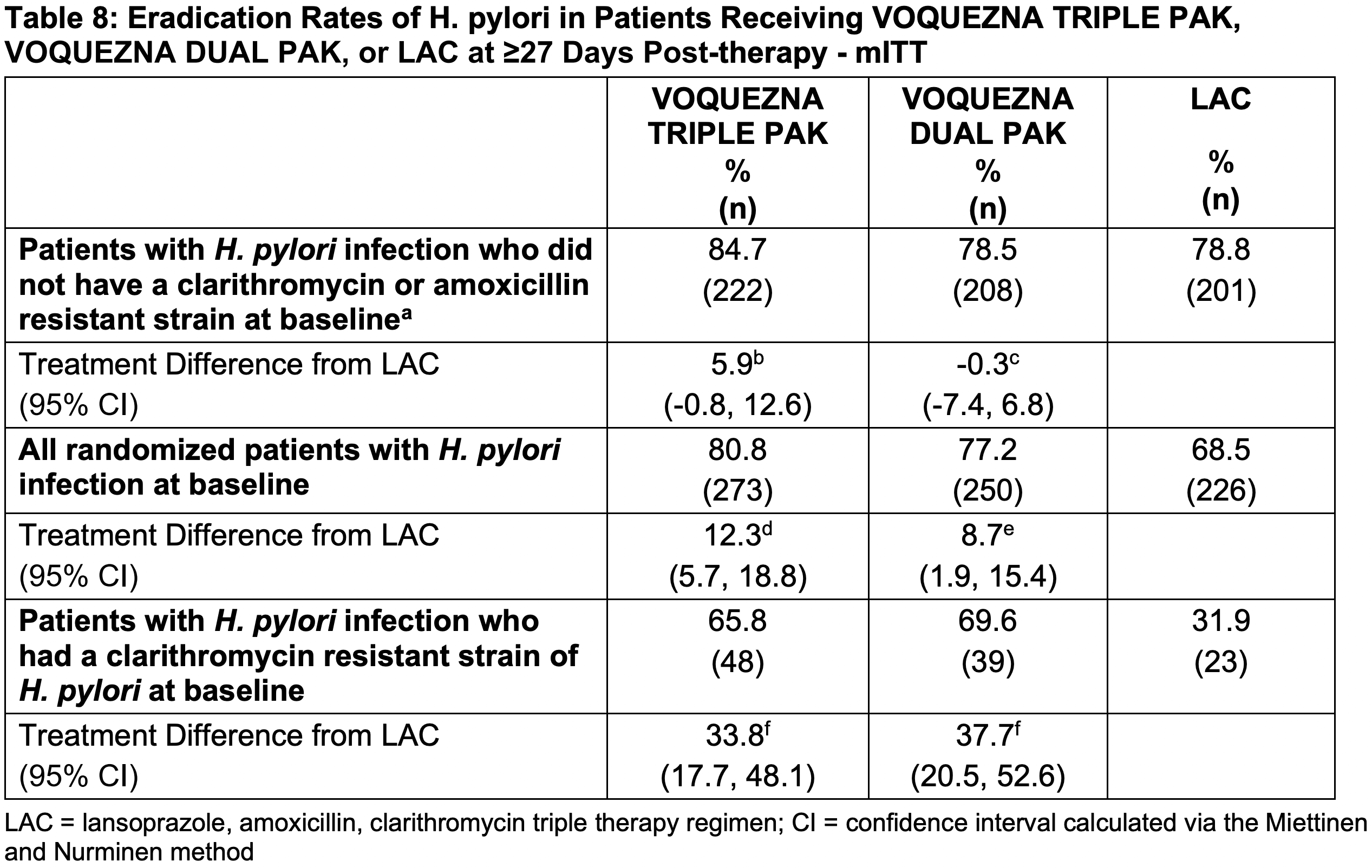
By the primary endpoint, declared successful eradication of H. pylori (confirmed by negative UBT results 4 weeks after completion of treatment), excluding patients with amoxicillin- or clarithromycin-resistant H. pylori strains, came out 84.7% and 78.5% of subjects in the triple and dual therapy groups with vonoprazan respectively — versus 78.8% when lansoprazole was prescribed. Thus, the efficacy of the experimental H. pylori eradication therapy was no worse than the standard treatment (p<0.0001 and p=0.0037).
If patients strictly followed the treatment protocol (carefully adhered to the drug regimen; compliance), the eradication rate of H. pylori was 90.4% and 81.2%, being no worse than the 82.1% in the control group (p<0.0001 and p=0.0077).
Eradication of H. pylori among patients with clarithromycin-resistant strains came out to 65.8% and 69.6% — vs. 31.9% (p<0.0001). At high compliance, the frequencies came out to 67.2% and 79.2% — vs. 29.0% (p<0.0001).
Among all patients with no exceptions, H. pylori eradication rates were 80.8% (85.7% for high compliance) and 77.2% (81.1%) — vs. 68.5% (70.0%) [p<0.0001].
The safety profile of vonoprazan was generally not different from that of lansoprazole.
Voquezna: Efficacy and Safety of Vonoprazan for Erosive Esophagitis Treatment
The PHALCON-EE (NCT04124926) phase 3 ( randomized, double-blind, active-controlled, multicenter, international) clinical trial enrolled adult patients (n=1024) with endoscopically confirmed erosive esophagitis.
The main trial exclusion criteria included: Helicobacter pylori infection; Barrett’s esophagus or other disease affecting the esophagus; and Zollinger–Ellison syndrome or other gastric acid hypersecretion condition.
In the first stage (Healing Phase), participants were given 20 mg of vonoprazan or 30 mg of lansoprazole once daily for a maximum of 8 weeks. Patients who achieved complete healing moved on to the second stage (Maintenance Phase): subjects received 10 mg or 20 mg of vonoprazan or 15 mg of lansoprazole once daily for up to 24 weeks.
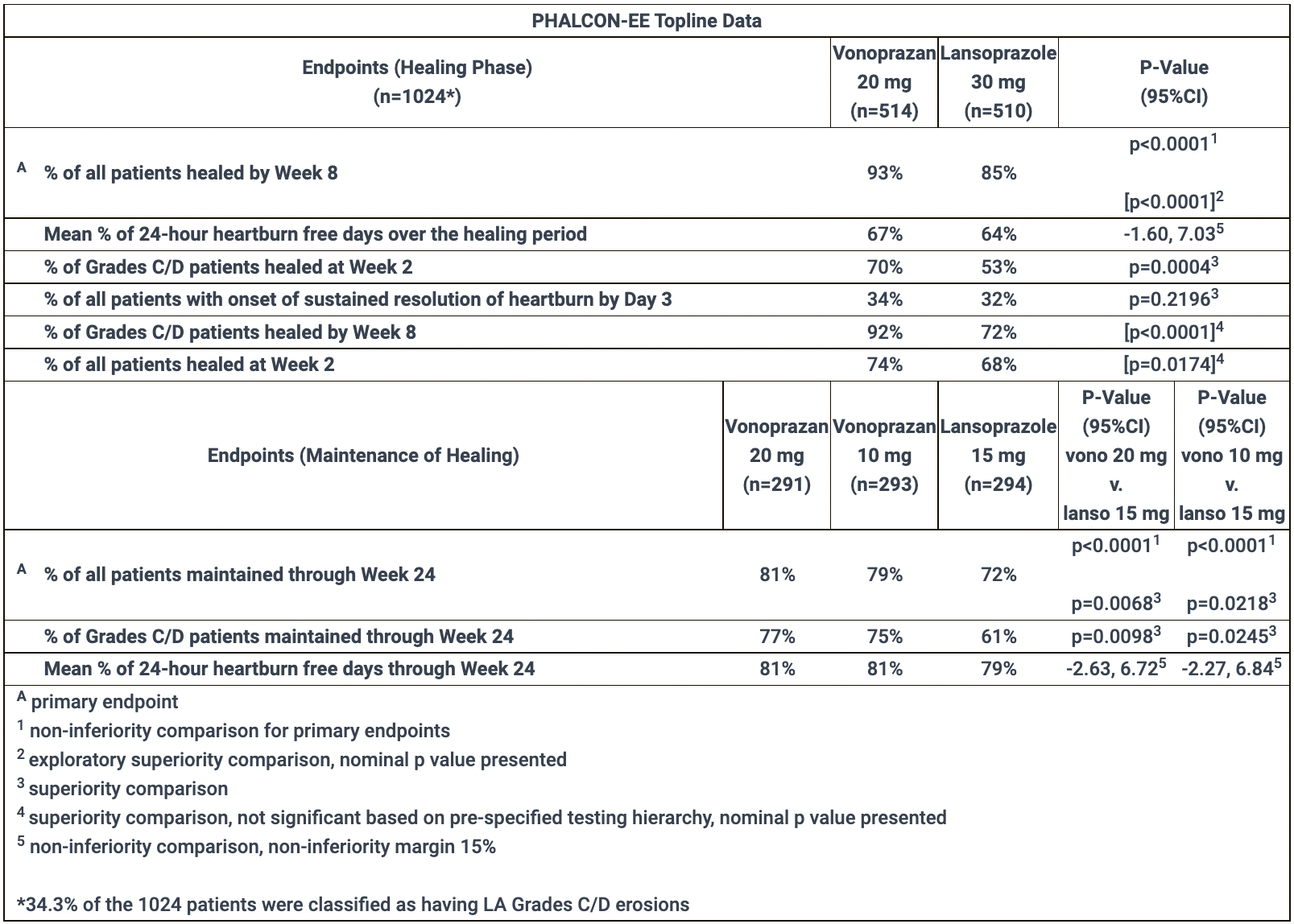
In Healing Phase, the primary efficacy endpoint of therapy, stated by endoscopically confirmed complete healing of erosive esophagitis by week 8, was reached by 93% of patients receiving vonoprazan — versus 85% in the lansoprazole group. Thus, the experimental drug was no worse than the standard drug (p<0.0001).
The use of vonoprazan provided significantly faster healing in patients with moderate-to-severe disease (C/D grade according to the Los Angeles classification; there were 34% of such patients) by week 2: the status was recorded among 70% of subjects — vs. 53% (p=0.0004).
Vonoprazan was no worse than lansoprazole in terms of sustained relief from heartburn by day 3 (34% of patients vs. 32%) and in terms of the mean percentage of complete days without heartburn (67% vs. 64%).
In Maintenance Phase, the primary efficacy endpoint of therapy, stated as maintaining the status of endoscopically confirmed complete healing of erosive esophagitis within 24 weeks, was 79% and 81% of patients treated with 10 mg and 20 mg of vonoprazan, respectively — versus 72% among those treated with lansoprazole. In other words, the use of vonoprazan performed no worse (p<0.0001).
In the case of patients with moderate-to-severe disease, complete healing was maintained for 75% and 77% of participants — vs. 61% (p=0.0245 and p=0.0098).
The mean percentage of complete days without heartburn was 81% and 81% — vs. 79%.
The safety profile of vonoprazan was generally not different from that of lansoprazole.
Voquezna: Efficacy and Safety of Vonoprazan for Non-Erosive Gastroesophageal Reflux Disease (NERD) Treatment
The PHALCON-NERD (NCT04799158) phase 2 ( randomized, double-blind, placebo-controlled, multicenter) clinical trial invited adult patients (n=458) with symptomatic non-erosive gastroesophageal reflux disease (NERD).
During the run-in period, all participants received 20 mg of vonoprazan daily for up to 4 weeks. Patients whose disease stabilized (no heartburn during the last 7 days of the run-in period) were then randomized: as soon as a heartburn episode occurred, subjects took placebo or vonoprazan at a dose of 10 mg, 20 mg, or 40 mg for 6 weeks, with no more than one dose per 24-hour period.
The primary efficacy endpoint of therapy, stated by the percentage of heartburn episodes completely relieved within 3 hours and not followed by new episodes within 24 hours of taking the drug, was 56.0%, 60.6%, and 70.0% among patients who received 10 mg, 20 mg or 40 mg of vonoprazan, respectively — versus 27.3% in the placebo group (p<0.0001).
Voquezna: Mechanism of Action of Vonoprazan
Vonoprazan (TAK-438) is an oral small-molecule potassium-competitive acid blocker (P-CAB).
Vonoprazan inhibits gastric hydrogen potassium adenosine triphosphatase (H+/K+ ATPase) through reversible potassium-competitive ion binding. The enzyme H+/K+-ATPase, which is localized in the parietal cells of the gastric mucosa, is a proton pump. By exchanging potassium from the intestinal lumen for cytoplasmic hydroxonium (a complex ionic compound of a proton with a water molecule; hydronium), it is responsible for acidifying the stomach contents and activating the digestive enzyme pepsin.
Inhibition of H+/K+ ATPase activity leads to suppression of hydrochloric acid secretion in the stomach, which is reflected in beneficial effects during treatment of acid-related gastrointestinal diseases.
Vonoprazan, unlike standard proton pump inhibitors (PPIs) such as omeprazole, lansoprazole, pantoprazole, esomeprazole, etc., has a relatively high value of the acidity constant (pKa) and is stable in an acidic environment, so it accumulates in the acidic compartment of the parietal cells. Vonoprazan, unlike PPIs, does not require acid activation. As a result, vonoprazan is characterized by a stronger and more prolonged suppression of hydrochloric acid secretion.
Sufficient inhibition of hydrochloric acid secretion with vonoprazan can be achieved in all patients because cytochrome P450 (CYP) 2C19, which has a pharmacogenetic polymorphism, is not involved in its metabolism.
Vonoprazan: Market Outlook
Given both the extremely high prevalence of acid-related gastrointestinal diseases and the steadily increasing resistance of Helicobacter pylori to existing treatment regimens, the emergence of new medications will definitely be welcomed.
Vonoprazan, developed by Takeda Pharmaceutical, was approved in Japan in late December 2014. At the end of February 2015, it went on sale. In early June 2016, combination versions of vonoprazan became available, Vonosap (vonoprazan + amoxicillin + clarithromycin) and Vonopion (vonoprazan + amoxicillin + metronidazole).
In Japan, the range of use of vonoprazan for acid-related gastrointestinal diseases is quite wide. Vonoprazan is prescribed in the treatment of peptic ulcer disease (gastric ulcer, duodenal ulcer) and reflux esophagitis (erosive esophagitis), in maintenance therapy of recurrent or recrudescence reflux esophagitis, and for the prevention of gastric or duodenal ulcer during low-dose acetylsalicylic acid or non-steroidal anti-inflammatory drugs (NSAIDs) are used. Vonoprazan is prescribed as an adjunctive drug during H. pylori eradication in the presence of the following conditions: gastric ulcer, duodenal ulcer, gastric mucosa-associated lymphoid tissue (MALT)-lymphoma, idiopathic thrombocytopenic purpura, the stomach after endoscopic resection for early stage gastric cancer, or H. pylori-associated gastritis.
Vonoprazan is approved in China and a number of Asian and Latin American countries, as well as in Russia.
In mid-May 2019, Takeda, with financial support from investment Frazier Healthcare Partners, established Phathom Pharmaceuticals to develop and market vonoprazan in the United States, Canada, and Europe.
The commercial prospect for vonoprazan in the West looks optimistic. First, it will gradually connect new indications beyond H. pylori eradication therapy such as erosive esophagitis (phase 3 clinical trial NCT04124926 successfully completed), non-erosive gastroesophageal reflux disease (NERD) [recruitment into phase 3 clinical trial NCT05195528 is underway after successful NCT04799158 phase 2], and gastroesophageal reflux disease (GERD) [ongoing enrollment in phase 3 clinical trial NCT05343364].
Second, despite the abundance of generic copies of proton pump inhibitors (PPIs), which attract low prices, demand for vonoprazan is still expected to be high. In Japan, for example, where 80% of the PPIs market is represented by generics, sales of vonoprazan reached $850 million in 2021; the drug covered 43% of the local PPIs market. In 2015, Takeda-developed Dexilant (dexlansoprazole), the latest branded PPI to date, managed to earn $530 million in the U.S., although it is essentially no different from other PPIs.
Third, patient and physician interest in vonoprazan is expected to be very decent due to the high prevalence of acid-related gastrointestinal diseases. Thus, for all of 2021, 7.2 billion doses of PPIs were prescribed in the United States and the European Union. There are an estimated 115 million and 145 million H. pylori infected and 65 million and 50 million with GERD in the U.S. and Europe, respectively.
Fourth, with proper marketing initiatives and efforts, vonoprazan is capable of gaining credibility. Is it a given that the entire class of drugs related to PPIs in the U.S. was able to reach peak annual sales of $12.5 billion before their generics and over-the-counter variants emerged.
Fifth, we cannot rule out the appearance of over-the-counter vonoprazan to relieve heartburn symptoms.
Nevertheless, we should not hope for a quick financial return on vonoprazan because of the strong competition from inexpensive generic versions of PPIs. In addition, there is competition from other pharmaceutical manufacturers. For example, in early November 2019, the FDA approved Talicia (omeprazole + amoxicillin + rifabutin, 10 mg/250 mg/12.5 mg) by Israel’s RedHill Biopharma for primary eradication therapy of H. pylori infection in adults. Talicia, which is based on the antibiotic rifabutin, is marked by the highest rate of successful eradication of H. pylori.

Talicia: Highly Effective Eradication Regimen for Helicobacter pylori
Combination drug invented by RedHill Biopharma will get rid of Helicobacter pylori infection in 90% of patients.
In the U.S., Neurogastrx intends to initiate a phase 3 clinical trial of fexuprazan, which, like voxoprazan, belongs to P-CAB. Fexuprazan is licensed from Korea’s Daewoong Pharmaceutical, which secured local regulatory approval for Fexuclu in late December 2021.
Two more P-CABs have entered the South Korean market: Revanex (revaprazan) and K-Cab (tegoprazan), launched by Yuhan Corporation and HK inno.N (previously called CJ Healthcare) in 2007 and 2019, respectively. Tegoprazan, which has already appeared in China as Taixinzan (泰欣赞) and Mongolia, is awaiting approval in several Asian, Central American and South American countries, while in the U.S. and Canada its clinical trials are being conducted by Braintree Laboratories at Sebela Pharmaceuticals.
Other P-CAB class drugs in clinical trials include JP-1366 (phase 3) from Korea’ Onconic Theraupetics as part of Jeil Pharmaceutical and linaprazan (X842; phase 3) from Sweden’s Cinclus Pharma.
Germany’s Katairo has repurposed Remofuscin (soraprazan), an experimental P-CAB, to study in the treatment of Stargardt’s disease and dry age-related macular degeneration (AMD).
In the field of PPIs themselves, the development of new molecules is relatively slow due to the plethora of generics. For example, China’s Sihuan Pharmaceutical is preparing to approve anaprazole, a next-generation proton pump inhibitor and a structural analogue of rabeprazole. [1] [2]
The interesting drug is Redacid (DLBS2411) by Indonesia’s Dexa Medica, which is a standardized bioactive fraction of Cinnamomum burmannii and which suppresses gastric acidity and enhances protection of its mucosa, is being clinically tested. The antisecretory effect of DLBS2411 is realized by inhibiting H+/K+ ATPase and reducing its gene expression, cytoprotective effects are provided by activation of nuclear factor NF-κB, which, first, enhances the synthesis of gastric-epithelial mucous by promoting the expression of cyclooxygenase-2 (COX-2) and prostaglandin E2 (PGE2) and, second, stimulates gastrointestinal submucosal blood-flow by increasing the production of nitric oxide (NO). [3] [4] [5]
Extras
Voquezna Dual Pak and Voquezna Triple Pak. Prescribing information. U.S. [PDF]
Phathom Pharmaceuticals. Corporate overview. March 2022. [PDF]
Phathom Pharmaceuticals. PHALCON-HP pivotal phase 3 results. April 29, 2021. [PDF]
Phathom Pharmaceuticals. PHALCON-EE pivotal phase 3 results. October 18, 2021. [PDF]
Phathom Pharmaceuticals. PHALCON-NERD phase 2 results. February 9, 2022. [PDF]