Highlights
Twymeeg (imeglimin) is a new drug indicated for the treatment of adult patients with type 2 diabetes mellitus. Twymeeg is indicated for use with diet and exercise.
Imeglimin is the first member of a completely new class of hypoglycemic drugs, characterized by the advantages of currently available anti-diabetic drugs. At the same time, imeglimin is free of serious negative adverse effects, which all the current medications for the treatment of type 2 diabetes without exception come with.
Twymeeg, developed by France’s Poxel, was approved in Japan at the end of June 2021. Sumitomo Dainippon Pharma is commercializing it in this country, as well as in several Southeast Asian territories including China, South Korea, Taiwan, Indonesia, Vietnam, Thailand, Malaysia, Philippines, Singapore, Myanmar, Cambodia, and Laos.
- In mid-September 2021, Twymeeg launches in Japan.
The corresponding agreement between Poxel and Sumitomo Dainippon, entered into in late October 2017, called for the latter to pay the former $42 million upfront plus a potential $257 million as the project develops and sales of the finished drug, as well as a royalty on its sales (in the first year 8% of net sales, in subsequent years 8%–18% depending on the volume of the drug net sales).
In February 2018, Roivant Sciences licensed the imeglimin to market it in the U.S., Europe, and other countries outside the Sumitomo Dainippon deal. For this, Poxel received a $50 million upfront payment and promises of future payments of up to $600 million plus royalties on sales. In November 2020, Metavant Sciences, which Roivant specifically created to develop imeglimin, returned the rights to the drug to Poxel due to a change in development strategy. Thus, the arrival of imeglimin in the West is still questionable: Poxel definitely needs partners to conduct proper pivotal clinical trials.
- As of January 2022, Poxel continues to explore options to take Twymeeg through a phase 3 clinical trial to bring the drug to the U.S. and European markets. Twymeeg is focused on the treatment of type 2 diabetes mellitus with chronic kidney disease (CKD) at stage 3b/4. Obviously, a partner with money is needed.
- As of February 2022, Poxel believes that in the near future there is no hope of concluding the large-scale partnership agreements needed to bring Twymeeg to the U.S. and European markets. However, the growing interest in Twymeeg suggests that the drug will still appear in some specific sales territories outside of Southeast Asia.
According to industry forecasts, imeglimin is capable of reaching sales of over $3 billion per year, $600 million of which will be earned in Japan.

Why We Need New Drugs for Treatment of Type 2 Diabetes Mellitus
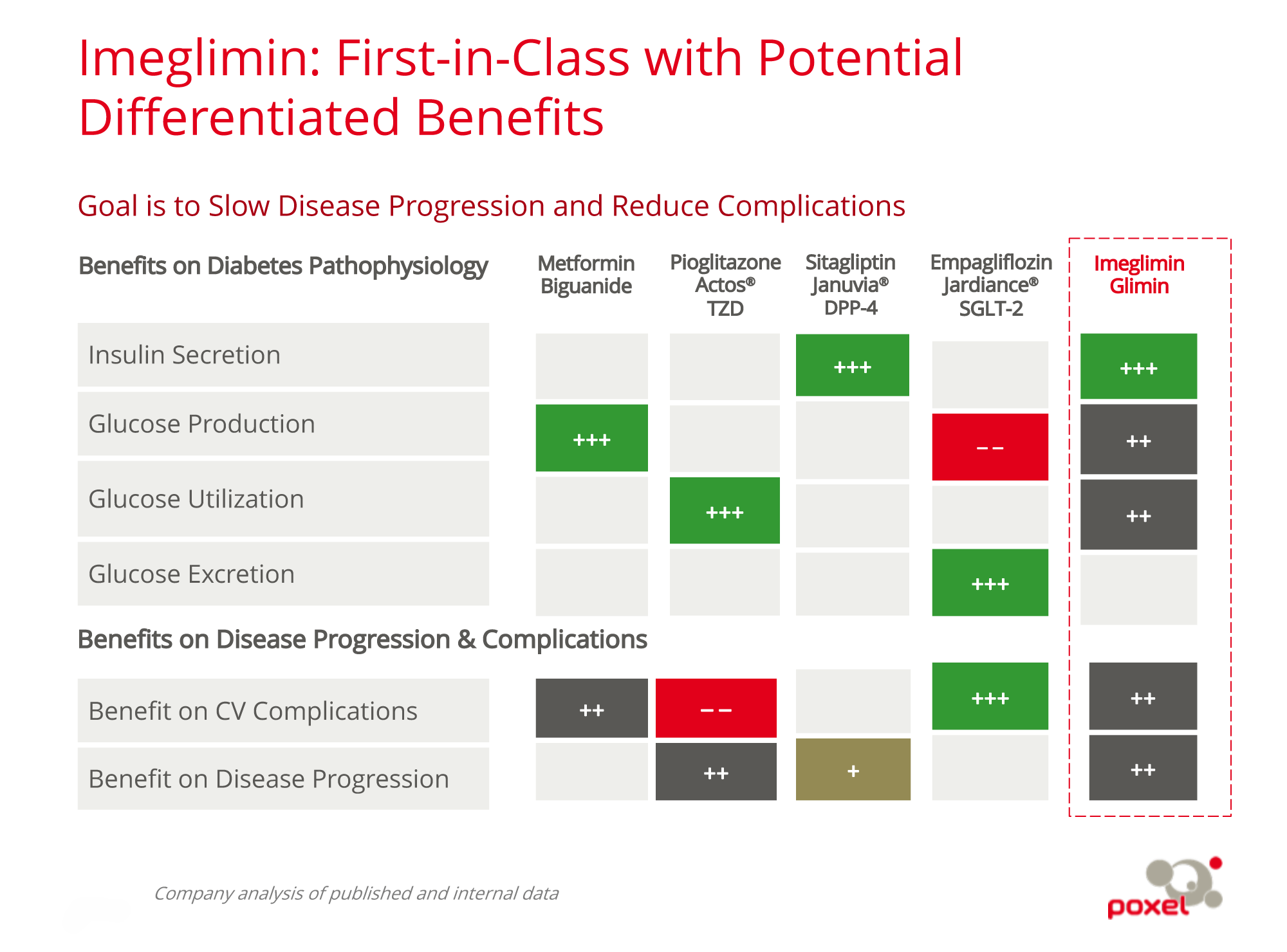
At first glance, there seem to be enough classes of therapeutic compounds proposed for the treatment of type 2 diabetes mellitus: each has a unique mechanism of action, safety profile, therapeutic efficacy, and route of administration. However, there are extremely few drugs that target all pathological pathways associated with the disease. This is why, in order to achieve proper glycemic control, a comprehensive approach, involving the prescription of several anti-diabetic drugs at once, is usually required.
For example, metformin, which belongs to the class of biguanides and inhibits glucose formation in the liver (gluconeogenesis), is widely used as first-line therapy. It is effective and does not lead to weight gain or risk of hypoglycemia. Meanwhile, some patients do not tolerate the gastrointestinal side effects of metformin, manifested by diarrhea, nausea, and vomiting.
Insulin production stimulants, such as sulfonylurea derivatives and meglitinides (glinides), are also often prescribed first. The clinical efficacy of insulin secretagogues is not long-term, and concomitant hypoglycemia and weight gain limit their use.
- Acetohexamide, carbutamide, chlorpropamide, glibenclamide (glyburide), glibornuride, gliclazide, glimepiride, glipizide, gliquidone, glisoxepide, glyclopyramide, glycyclamide (tolcyclamide), metahexamide, tolazamide, tolbutamide
- Enyglid/GlucoNorm/NovoNorm/Prandin/Surepost (repaglinide)
- Glufast (mitiglinide)
- Starlix (nateglinide)
Thiazolidinediones (glitazones), which increase peripheral tissue sensitivity to insulin and increase insulin-dependent glucose consumption, are characterized by long-lasting effects and rare cases of hypoglycemia, but possible edema, weight gain, risks of heart failure, and bone fractures negate the benefits.
- Actos/Glidipion/Glizone/Glustin/Pioglit/Pioz/Pyoglar/Zactos (pioglitazone)
- Avandia (rosiglitazone)
- Duvie (lobeglitazone)
Alpha-glucosidase inhibitors, which act as competitive reversible inhibitors of enzymes necessary to break down complex carbohydrates, slow their absorption in the small intestine. The resulting sugar-lowering effect is relatively weak and short-term. Adverse events include flatulence, diarrhea, intestinal pneumatosis, and hypoglycemia.
- Glucobay/Prandase/Precose (acarbose)
- Glyset/Diastabol (miglitol)
- Voglib (voglibose)
Relatively new classes of anti-diabetic drugs are targeting incretins — metabolic hormones that stimulate a decrease in blood glucose levels. For example, glucagon-like peptide-1 receptor (GLP-1R) agonists are rarely associated with hypoglycemia, stimulate beta-cell growth, inhibit glucagon, induce confident weight loss, suppress appetite, and slow gastric emptying. Most patients experience gastrointestinal adverse reactions: nausea, vomiting, diarrhea, abdominal pain, constipation.
- Adlyxin/Lyxumia (lixisenatide)
- Bydureon/Byetta Long (exenatide)
- Byetta (exenatide)
- Ozempic (semaglutide)
- Rybelsus (semaglutide)
- Tanzeum/Eperzan (albiglutide)
- Trulicity (dulaglutide)
- Victoza (liraglutide)
Parallel to GLP-1R agonists are dipeptidyl peptidase-4 (DPP4) inhibitors, or gliptins, which inhibit the activity of the incretin-degrading enzyme of the same name. Drugs in this class are not characterized by serious side effects, but are not very good at reducing glucose levels.
- Galvus/Xiliarx/Jalra (vildagliptin)
- Januvia/Tesavel/Xelevia (sitagliptin)
- Marizev (omarigliptin)
- Nesina/Vipidia (alogliptin)
- Onglyza (saxagliptin)
- Saterex (gozogliptin)
- Suganon/Evodine (evogliptin)
- Suiny (anagliptin)
- Tenelia (teneligliptin)
- Tradjenta/Trajenta (linagliptin)
- Zafatek/Wedica (trelagliptin)
- Zemiglo (gemigliptin)
The newest drugs to treat type 2 diabetes include sodium-glucose co-transporter type 2 (SGLT2) inhibitors, or gliflozins, which block glucose reuptake in the kidney tubules, promoting glucose loss in the urine. They are very effective at both lowering blood sugar levels and preventing cardiovascular complications and limiting the progression of renal failure, but can lead to ketoacidosis, urogenital tract infections, and candidiasis vulvovaginitis.
- Apleway/Deberza (tofogliflozin)
- Farxiga/Forxiga (dapagliflozin)
- Invokana (canagliflozin)
- Jardiance (empagliflozin)
- Lusefi (luseogliflozin)
- Remo/Remozen (remogliflozin)
- Steglatro (ertugliflozin)
- Suglat (ipragliflozin)
- Zynquista (sotagliflozin)
Finally, insulin therapy itself, the most potent way to control glucose levels, is characterized by significant risks of hypoglycemia and weight gain.
Twymeeg: Imeglimin’s Mechanism of Action
Type 2 diabetes mellitus is a widespread disease affecting over 500 million people worldwide. The disease is characterized by dysfunction of beta cells of the pancreatic islets and peripheral insulin resistance, leading to hyperglycemia. In addition to the need for profound lifestyle changes involving a low-calorie diet with increased physical activity, pharmacological treatment is usually required to maintain effective glycemic control. The latter, represented by an extensive armamentarium of medications, is usually accompanied by a number of negative side effects, especially pronounced in the elderly. This is why the medical need for new anti-diabetic drugs that are safe and effective remains unmet.
Imeglimin (EMD-387008, PXL-008, RVT-1501) is the first representative of completely new drug compounds containing tetrahydrotriazine, called glimins.
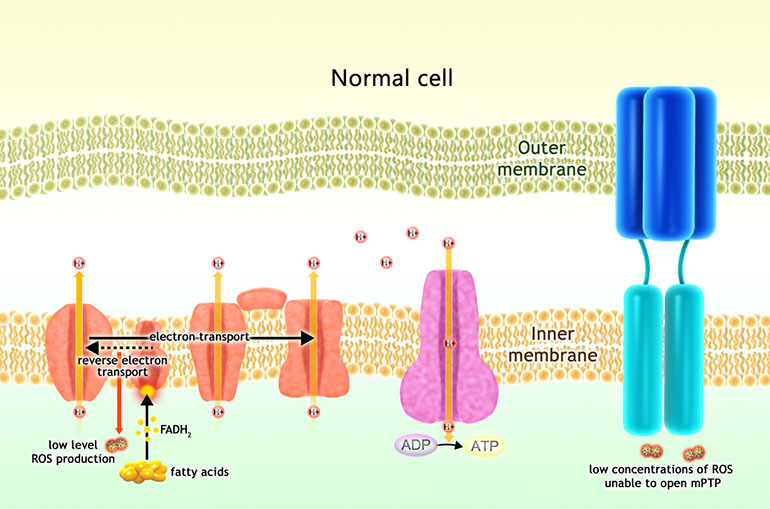
The mechanism of action of imeglimin differs from the existing hypoglycemic drugs and is aimed at the bioenergetics of mitochondria and the improvement of their functions. Imeglimin is an oral small-molecule blocker of oxidative phosphorylation, which modulates the activity of the mitochondrial respiratory chain complex and reduces the formation of reactive oxygen species.
Imeglimin has a beneficial effect on three main pathophysiological components of type 2 diabetes, which are manifested by insulin secretion deficiency with increased apoptosis of pancreatic beta cells, excessive gluconeogenesis by hepatocytes, impaired glucose uptake by peripheral insulin-sensitive tissues (skeletal musculature).
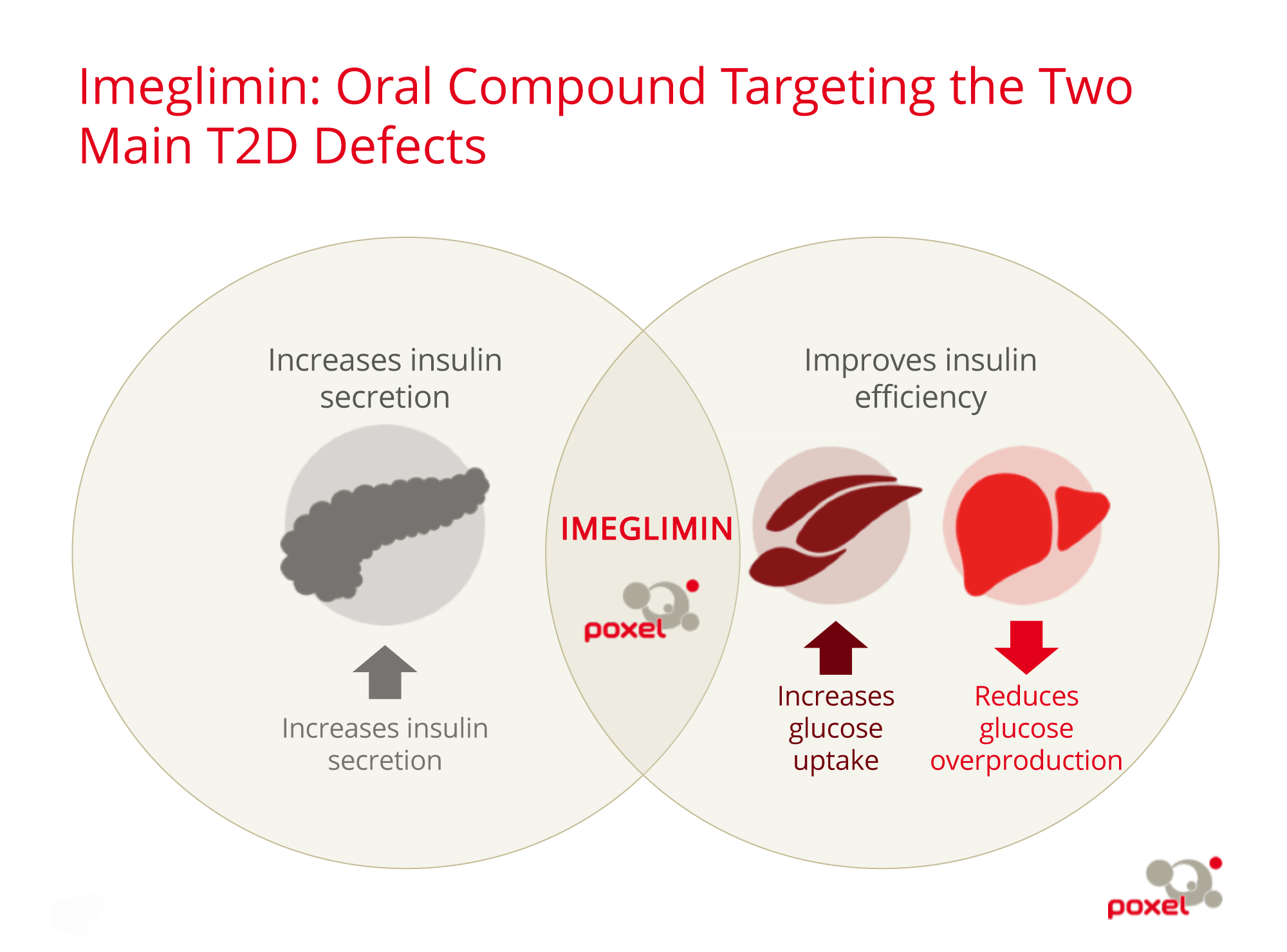
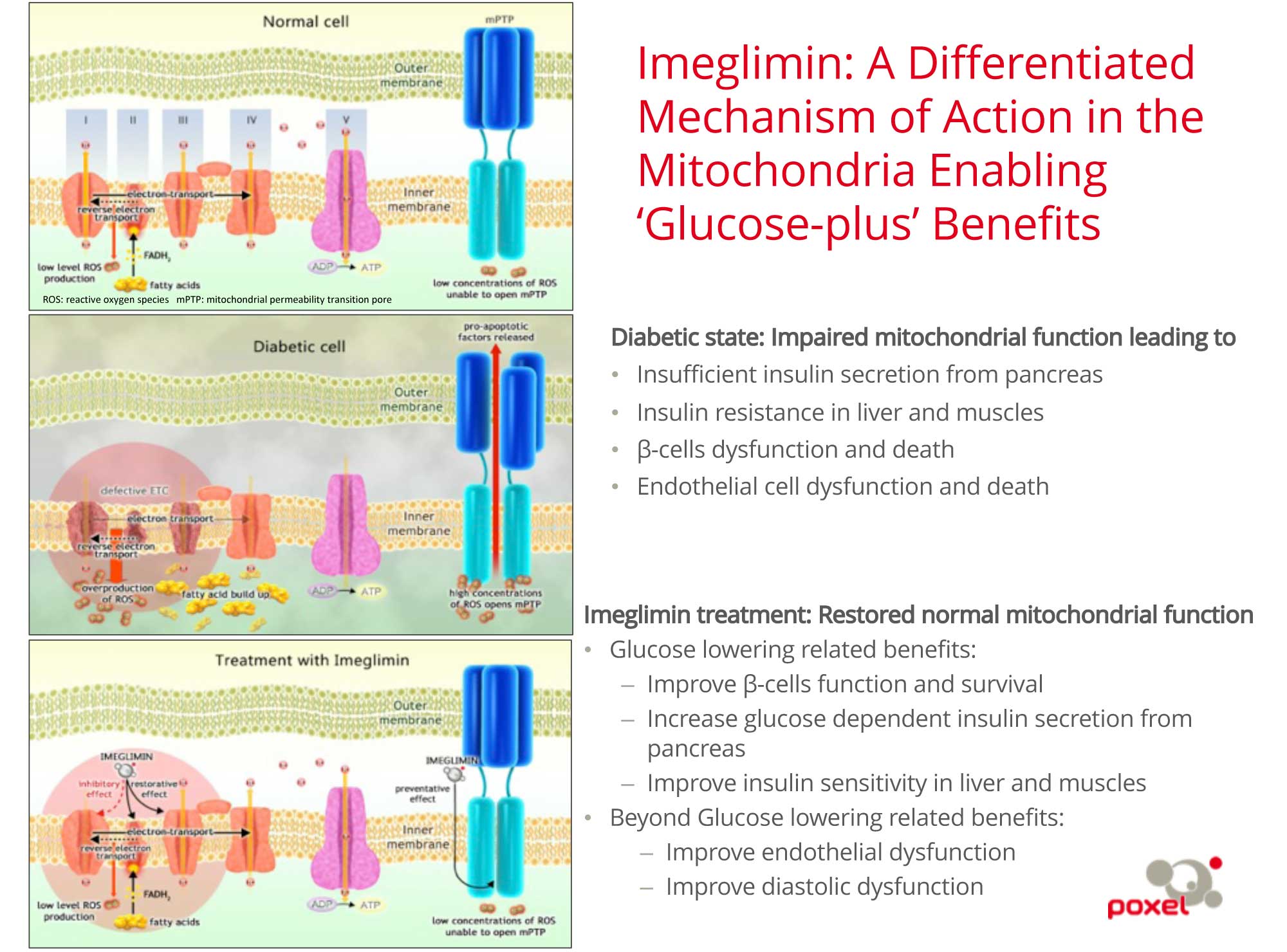
The mechanism of action of imeglimin is represented by a double effect: first, an amplification of glucose-stimulated insulin secretion and preservation of beta-cell mass; second, an enhancement of insulin action, including the potential to inhibit hepatic glucose production and improvement in insulin signaling in the liver and skeletal muscle.
At the cellular and molecular level, the mechanism of action of imeglimin is realized through the correction of mitochondrial dysfunction, a common underlying element in the pathogenesis of type 2 diabetes.

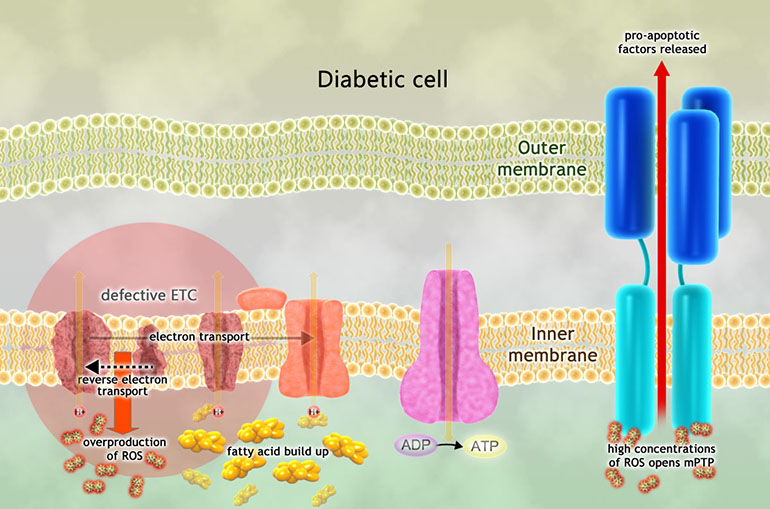
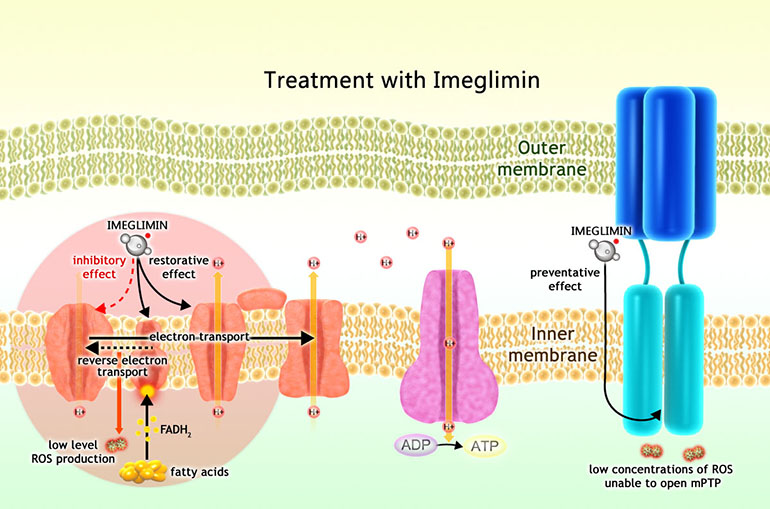
Thus, there is a rebalance of the respiratory chain activity (partial inhibition of complex I and correction of the insufficient activity of complex III), which leads to a decrease in the formation of reactive oxygen species (reduction of oxidative stress) and prevention of opening of the mitochondrial permeability transition pore (mPTP) [implicated in preventing endothelial cell death].
Imeglimin enhances glucose-stimulated ATP production and induces nicotinamide adenine dinucleotide (NAD+) synthesis via the “salvage pathway”. In addition to its key role as a mitochondrial cofactor, NAD+ metabolites contribute to increased glucose-stimulated insulin secretion (via enhanced Ca2+ mobilization).
Imeglimin prevents the loss of functional mass of beta cells: by moderately increasing the proliferation of beta cells and inhibiting their apoptotic death.
In general, imeglimin targets the key root cause of type 2 diabetes: defects in cellular energy metabolism.
The development of imeglimin began in 2009, when Poxel separated from Merck KGaA, becoming a biotech startup in its own right. Nevertheless, Poxel will still share the money from Twymeeg sales with Merck KGaA.

Twymeeg: Efficacy and Safety of Imeglimin for Diabetes Treatment
To evaluate the efficacy and safety of imeglimin in the treatment of type 2 diabetes mellitus, the TIMES clinical program of three phase 3 pivotal studies involving over one thousand Japanese patients was conducted:
- TIMES 1 (JapicCTI-173769): a 24-week clinical trial (randomized, double-blind, placebo-controlled, multicenter) that tested the mono-use of imeglimin.
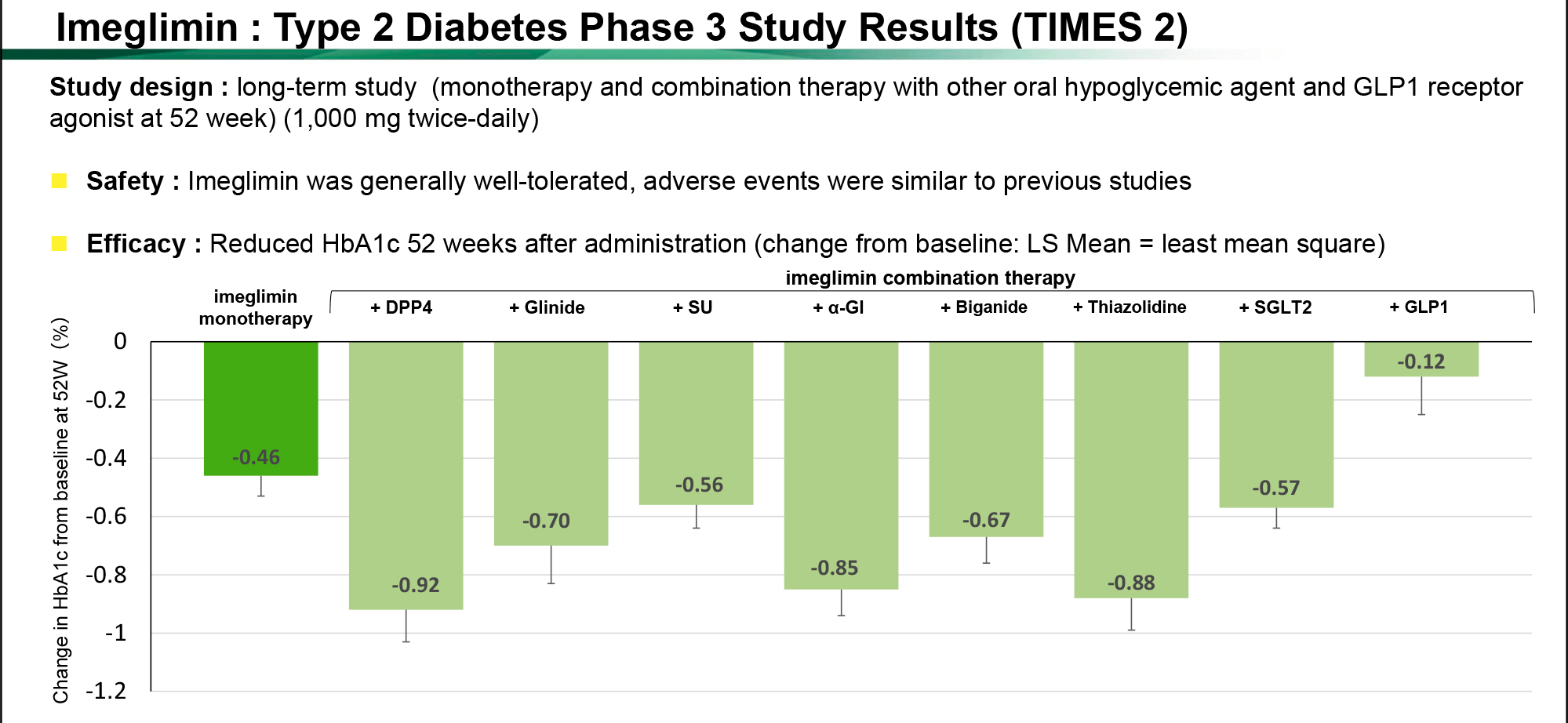
- TIMES 2 (JapicCTI-173782): a 52-week clinical trial (randomized, open-label, placebo-controlled, multicenter) examining the monodosing of imeglimin or its use with other anti-diabetic drugs such as sulfonylureas, glinides, metformin, alpha-glucosidase inhibitors, glitazones, DPP4 inhibitors, GLP-1R agonists, and SGLT2 inhibitors.
- TIMES 3 (JapicCTI-183846): a 16-week clinical trial (randomized, double-blind, placebo-controlled, multicenter) followed by a 36-week open-label period testing the addition of imeglimin to insulin therapy.
TIMES 1
The TIMES 1 clinical trial enrolled patients (n=212) aged 20 years or older with type 2 diabetes mellitus on a diet and exercise regimen. Baseline glycated hemoglobin (HbA1c) levels ranged from 7.0% to 10.0%.
Participants were given 1000 mg of imeglimin twice daily or placebo.
After 24 weeks of treatment, HbA1c levels decreased by a mean of 0.72% (95% CI: −0.86 to −0.58) in the imeglimin group versus an increase of 0.15% (95% CI: 0.01 to 0.29) in the placebo group: a difference of −0.87% (95% CI: −1.04 to −0.69; p<0.0001).

35.8% of patients who received imeglimin reached their target HbA1c level below 7%, compared with 7.5% in the control group (p<0.0001).
Among patients not previously treated for diabetes, HbA1c levels fell by a mean of 0.81% (95% CI: −0.96 to −0.67) — vs. an increase of 0.06% (95% CI: −0.08 to 0.20): the difference was −0.87% (95% CI: −1.07 to −0.67; p<0.0001).
Among patients who were previously treated for diabetes, HbA1c levels decreased by a mean of 0.51% (95% CI: −0.73 to −0.29) — vs. an increase of 0.33% (95% CI: 0.09 to 0.56): the difference was −0.84% (95% CI: −1.16 to −0.52; p<0.0001).
Other clinical outcomes are as follows:
- Fasting plasma glucose (FPG): change of −0.31 mmol/L in the imeglimin group — versus +0.71 mmol/L in the placebo group (p<0.0001).
- Fasting proinsulin-to-insulin ratio: change of −0.0138 — vs. +0.0036 (p=0.0579). The increase in this ratio reflects beta-cell dysfunction associated with the onset and progression of type 2 diabetes.
- Fasting proinsulin-to-C-peptide ratio: change of −0.0003 — vs. +0.0002 (p=0.0012). The increase in this ratio is considered a better indicator of impaired beta cells, since C-peptide does not undergo hepatic clearance, meaning its concentration is less dependent on insulin resistance.
- Quantitative Insulin Sensitivity Check Index (QUICKI): change of +0.0017 — vs. −0.0076 (p=0.0050). The lower this index, defined by the inverse of the sum of the logarithms of fasting insulin and fasting glucose, the greater the insulin resistance.
- Beta-cell function index according to Homeostatic Model Assessment (HOMA-β): change of +3.5276 — vs. −2.7121 (p=0.0002).
- Insulin resistance index according to Homeostatic Model Assessment (HOMA-IR): change of +0.1961 — vs. +0.1321 (p=0.7325).
- Homeostatic Model Assessment (HOMA) is a method to quantify pancreatic beta-cell function and insulin resistance as a percentage of the normal control population. The method is based on computer modeling and is based on fasting glucose, insulin, or C-peptide levels. HOMA2 is an advanced computer model that takes into account factors of hepatic and peripheral insulin resistance, a physiological measure of glucose homeostasis.
- Total cholesterol levels increased by 3.3% in the imeglimin group compared with the placebo group (p=0.0439); low-density lipoprotein (LDL) cholesterol levels increased by 7.2% (p=0.0051). The differences were not clinically significant.

The safety profile of imeglimin was favorable. The proportions of subjects who experienced adverse events were similar in the drug and placebo groups. No serious adverse reactions associated with the treatment were noted. The tolerability of imeglimin was positive: very rare gastrointestinal complaints were mild. Administration of imeglimin did not result in an increase in hypoglycemia: although imeglimin potentiates beta-cell function and insulin secretion, this compound induces insulin secretion only in response to glucose.
TIMES 2
The TIMES 2 clinical trial invited patients (n=714) aged 20 years or older with type 2 diabetes mellitus. Baseline HbA1c levels ranged from 7.0%–10.0% or 7.5%–10.5% for monotherapy or combination treatment, respectively.
Participants were given 1000 mg of imeglimin twice daily or the same amount with other anti-diabetic drugs.
After 52 weeks of treatment, the results were as follows:
- imeglimin monotherapy reduced HbA1c levels by 0.46% (95% CI: −0.59 to −0.33)
- combination of imeglimin with DPP4 inhibitors: −0.92% (95% CI: −1.14 to −0.71)
- combination of imeglimin with glitazones: −0.88% (95% CI: −1.10 to −0.67)
- combination of imeglimin with alpha-glucosidase inhibitors: −0.85% (95% CI: −1.03 to −0.67)
- combination of imeglimin with glinides: −0.70% (95% CI: −0.95 to −0.45)
- combination of imeglimin with metformin: −0.67% (95% CI: −0.86 to −0.48)
- combination of imeglimin with SGLT2 inhibitors: −0.57% (95% CI: −0.71 to −0.43)
- combination of imeglimin with sulfonylureas: −0.56% (95% CI: −0.71 to −0.40)
- combination of imeglimin with GLP-1R agonists: −0.12% (95% CI: −0.39 to −0.15)
TIMES 3
The TIMES 3 clinical trial enrolled patients (n=208) aged 20 years or older with type 2 diabetes mellitus who were on insulin therapy but without adequate glycemic control. Baseline HbA1c levels ranged from 7.5% to 11.0%.
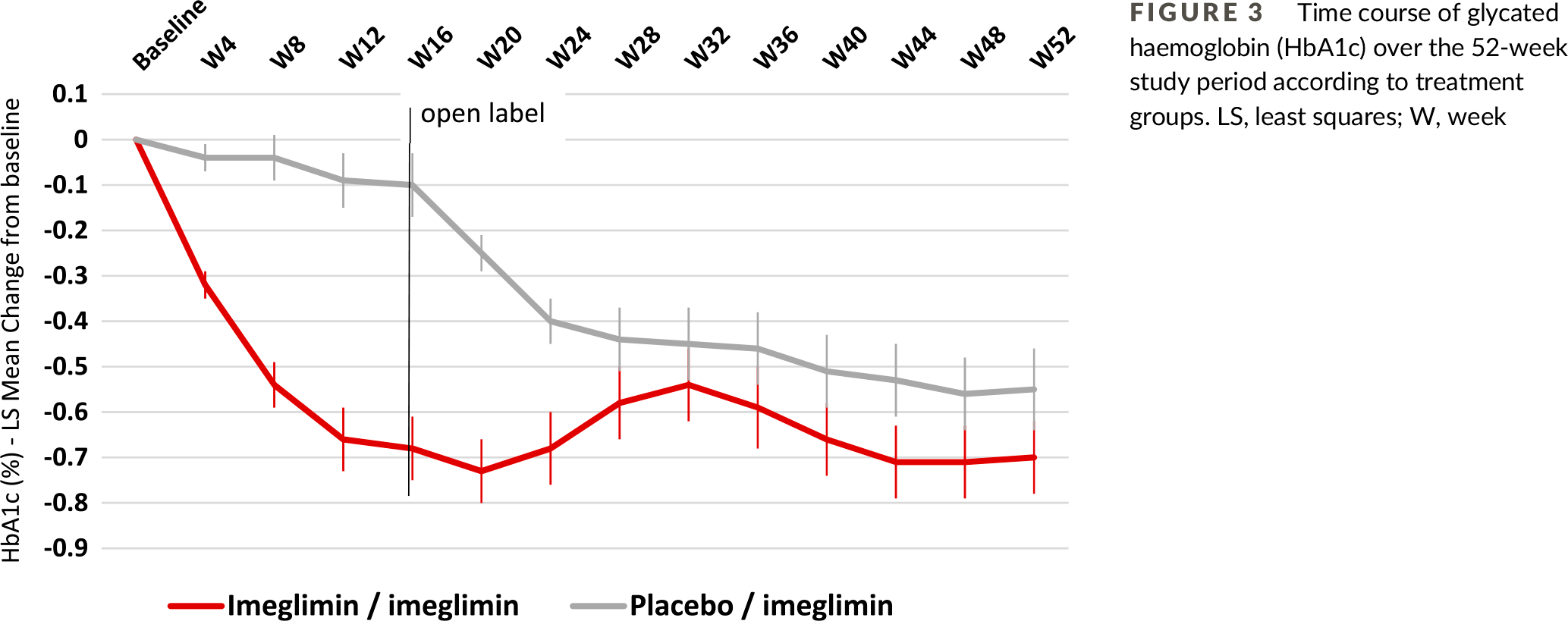
In a double-blind, 16-week treatment period, participants received 1000 mg of imeglimin twice daily or placebo on their usual insulin therapy. The drug group showed a mean of 0.60% (95% CI: −0.80 to −0.40) decrease in HbA1c levels relative to the control group (p<0.0001).
In the open 36-week treatment period that followed, all subjects received the above-mentioned dose of imeglimin. Those patients who initially followed a course of imeglimin showed a decrease in HbA1c levels by a mean of 0.64% (95% CI: −0.82 to −0.46) relative to baseline. Patients who received imeglimin after placebo showed a mean HbA1c drop of 0.54% (95% CI: −0.71 to −0.38) relative to baseline.
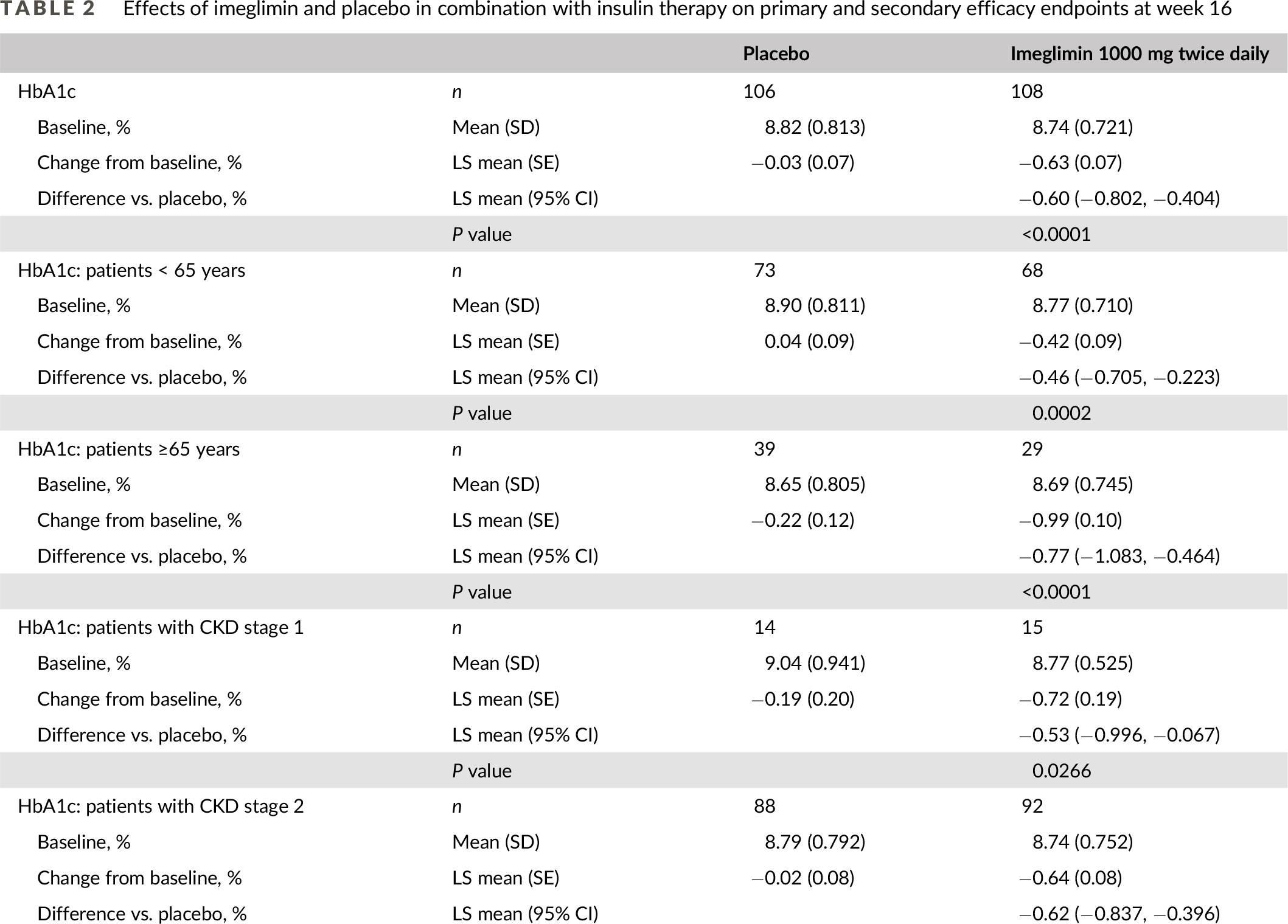
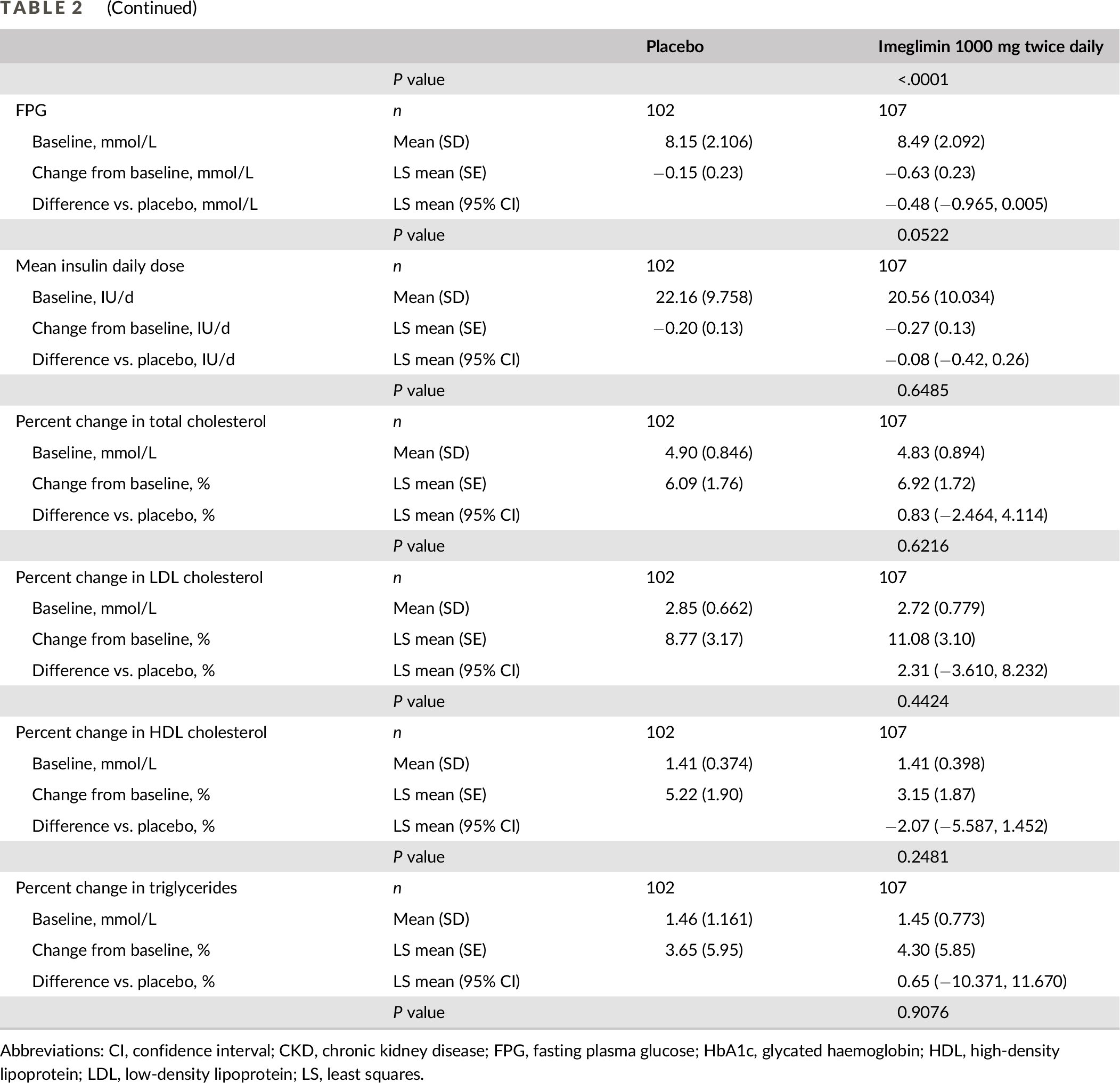
The safety profile of imeglimin was characterized by acceptable tolerability, and no serious treatment-related adverse reactions were reported. The frequencies of hypoglycemic events were similar in the two groups, none of which led to treatment discontinuation. No clinically significant changes in laboratory assessments, physical examinations (body weight), and cardiovascular evaluations (blood pressure) were recorded.
Imeglimin: Expert Comments
Sumitomo Dainippon believes that the initial introduction of imeglimin into clinical practice in Japan will be in the form of its combination with other anti-diabetic drugs. And there are reasons for this. First, imeglimin has shown itself particularly well in combination with DPP4 inhibitors. Second, DPP4 inhibitors (not metformin) are more than popular in Japan: almost half of all previously untreated patients with type 2 diabetes are using them.
If we talk about prescribing imeglimin as a first-line drug, there is a good chance for this, as Japanese people are increasingly faced with insufficient insulin secretion and insulin resistance due to the continued penetration of food commonly eaten in the West into their diets (westernization).
The main marketing focus will be on elderly patients with type 2 diabetes because of the acceptable safety profile of imeglimin, which does not cause any serious adverse events critical in this population of aged individuals.
Twymeeg is not recommended in moderate-to-severe renal impairment (estimated glomerular filtration rate [eGFR] < 45 mL/min/1.73 m2) due to a possible significant increase in blood concentrations of the drug. However, a pharmacokinetic study has found that reducing the dose of imeglimin to 500 mg twice daily is well suited to treat patients with eGFR in the 15–45 mL/min/1.73 m2 range. For patients with eGFR < 15 mL/min/1.73 m2, a dose of 500 mg of imeglimin every other day is appropriate.
The TIMES 1 clinical trial found that the therapeutic efficacy of imeglimin relative to placebo was generally independent of whether patients were previously treated for diabetes or not. Although the absolute level of glucose reduction was more significant among previously untreated patients, this may be due, first, to a less advanced form of diabetes in these patients and, second, to an insufficient 12-week washout period among previously treated patients.
Because of the slight increase in gastrointestinal adverse reactions in response to the administration of imeglimin at a dose of 1500 mg twice daily, it was decided to further reduce it to 1000 mg twice daily.
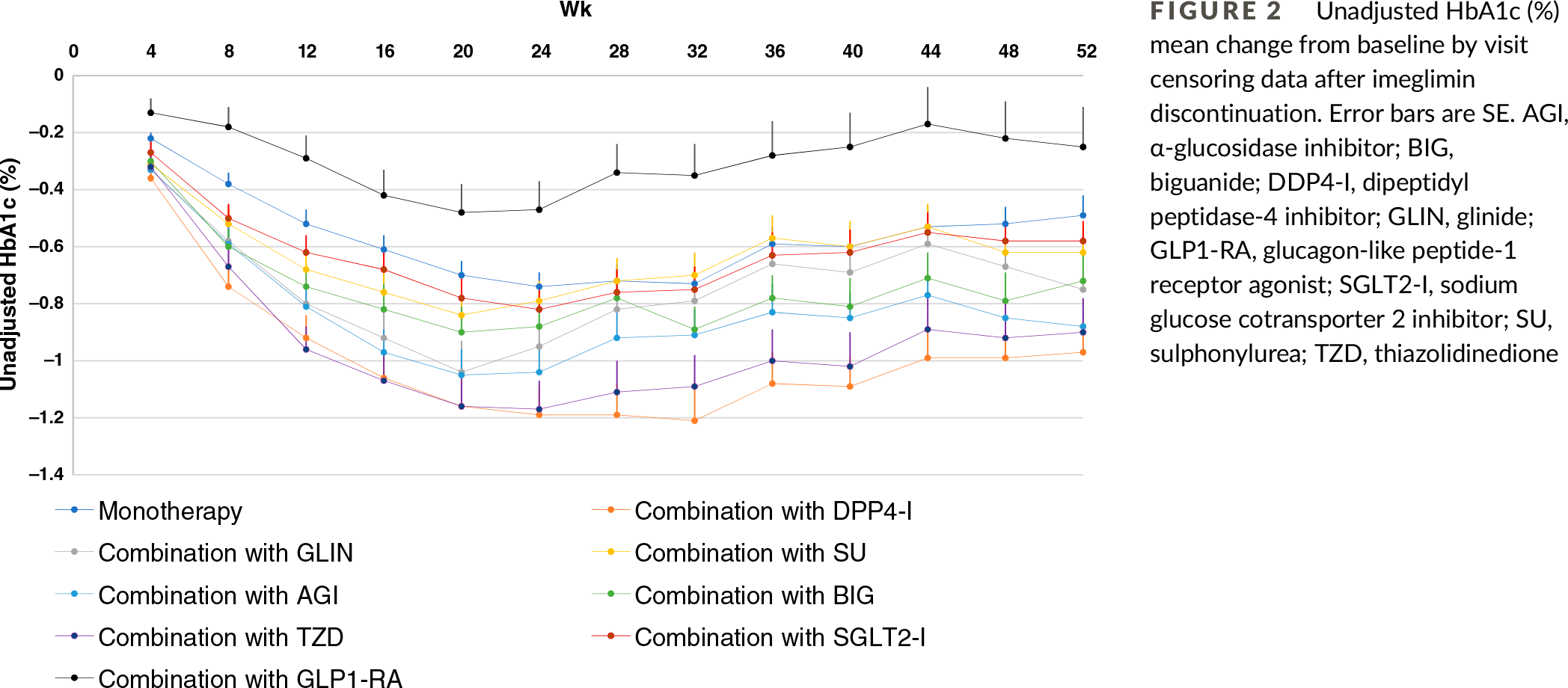
The TIMES 2 clinical trial showed that imeglimin has a clinically significant effect in lowering blood glucose levels regardless of the class of drugs with which it is combined. Although the addition of GLP-1R agonists was an exception: very modest additive efficacy was noted. This is explained by several factors.
First, the cohort of patients receiving GLP-1R agonists was characterized by greater disease severity, and therefore beta cell mass was obviously reduced. Second, the signaling pathways mediated by imeglimin and GLP-1R agonists ultimately converge, reflected by the impaired ability of imeglimin to stimulate insulin release in response to glucose intake.
In contrast, the addition of DPP4 inhibitors to imeglimin had the most significant glucose-lowering effect. This was apparently the result of a therapeutically successful combination of different mechanisms of action that complement each other without blocking or overlapping.
The TIMES 3 clinical trial confirmed the rationale for adding imeglimin to insulin therapy. Because type 2 diabetes is a progressive disease characterized by increasing deterioration of pancreatic beta-cell function, it is believed that the patients included in the trial retained a residual beta-cell mass (although their diabetes lasted an average of 13.3 years), and this entailed the benefit of increased glucose-stimulated insulin secretion.
Remarkably, the addition of imeglimin improved glycemic control without the need to intensify insulin therapy: either by increasing the basal insulin dose or by adding prandial doses of rapid insulin.
Due to the absence of any serious adverse events, the addition of imeglimin to insulin therapy may benefit elderly patients, since aged people often have functional limitations (e.g., difficulty with precise insulin administration), comorbidities, and insufficient social support.
It should be understood that the results of TIMES 3 cannot be extended unequivocally to the global population of diabetics. East Asian patients differ from other patients with type 2 diabetes: they are characterized by marked beta cell dysfunction, reduced adiposity, and reduced insulin resistance. Drugs that stimulate beta-cell function, such as DPP4 inhibitors and GLP-1R agonists, have been demonstrated to have a greater glucose-lowering effect.
Extras
Twymeeg (imeglimin). Prescribing information. Japan. [PDF]
Poxel. Corporate presentation. January 2022. [PDF]
Efficacy and safety of imeglimin monotherapy versus placebo in Japanese patients with type 2 diabetes (TIMES 1): A double-blind, randomized, placebo-controlled, parallel-group, multicenter phase 3 trial. Diabetes Care. 2021 Apr;44(4):952-959. [source]
Long-term safety and efficacy of imeglimin as monotherapy or in combination with existing antidiabetic agents in Japanese patients with type 2 diabetes (TIMES 2): A 52-week, open-label, multicentre phase 3 trial. Diabetes Obes Metab. 2021 Dec 6. [source]
Efficacy and safety of imeglimin add-on to insulin monotherapy in Japanese patients with type 2 diabetes (TIMES 3): A randomized, double-blind, placebo-controlled phase 3 trial with a 36-week open-label extension period. Diabetes Obes Metab. 2022 Jan 4. [source]
Mechanism of action of imeglimin: A novel therapeutic agent for type 2 diabetes. Diabetes Obes Metab. 2021 Mar;23(3):664-673. [source]
Imeglimin population pharmacokinetics and dose adjustment predictions for renal impairment in Japanese and Western patients with type 2 diabetes. Clin Transl Sci. 2021 Dec 27. [source]