Highlights
Eli Lilly continues clinical testing of the experimental drug tirzepatide in the task of reducing excess weight in obesity or overweight.
The clinical program of tirzepatide is large-scale: The goal is to prove that tirzepatide is suitable for the widest possible population of overweight patients, including those with type 2 diabetes or with any cardiovascular disease.
Data from one completed late-stage clinical trial of tirzepatide have now been collected. It has been demonstrated that weekly use of the drug by subcutaneous injection resulted in two-thirds of patients losing at least 20% of their excess weight. It took 72 weeks, that is, almost a year and a half.
The maximum dose of tirzepatide “burned off” an average of 22.5% fat, reducing the weight by 24 kg. This was true for those who strictly followed the treatment protocol without skipping any doses of the drug.
In mid-May 2022, the U.S. Food and Drug Administration (FDA) approved Mounjaro (tirzepatide) for the treatment of type 2 diabetes. Mounjaro’s impressive therapeutic efficacy outperformed all existing antidiabetic drugs.

Mounjaro: New Dual-Action Drug for Type 2 Diabetes Mellitus
Tirzepatide by Eli Lilly is a powerful new antidiabetic drug.
Tirzepatide is also being studied in the treatment of nonalcoholic steatohepatitis (NASH) and heart failure with preserved ejection fraction (HFpEF).
The emergence of tirzepatide will not only shake up the extremely saturated diabetes market, it will also make other players in the obesity treatment sector nervous, especially Novo Nordisk and its Wegovy (semaglutide). Eli Lilly will make many billions of dollars on each of the tirzepatide’s indications.
Tirzepatide Against Overweight: Efficacy and Safety
The SURMOUNT-1 (NCT04184622) phase 3 (randomized, double-blind, placebo-controlled, multicenter, international) clinical trial invited adult patients (n=2539) without type 2 diabetes, who were either obese (body mass index [BMI] ≥ 30 kg/m2) or overweight (BMI ≥ 27 kg/m2) with a history of weight-related comorbidities (hypertension, dyslipidemia, obstructive sleep apnea, cardiovascular disease).
Participants had to have experienced at least one previous unsuccessful attempt at weight loss through dieting.
Subjects were given weekly subcutaneous injections of placebo or tirzepatide at a dose of 5 mg, 10 mg, or 15 mg for 72 weeks. In the tirzepatide subgroups, the dose was gradually increased to the target maintenance dose.
Patients were instructed to follow a lifestyle change program, which involved reducing caloric intake (by 500 kcal/day) and increased physical activity (at least 150 min/week).
Two primary efficacy endpoints were established: the percentage change in body weight from baseline and the proportion of patients who showed at least 5% weight loss.
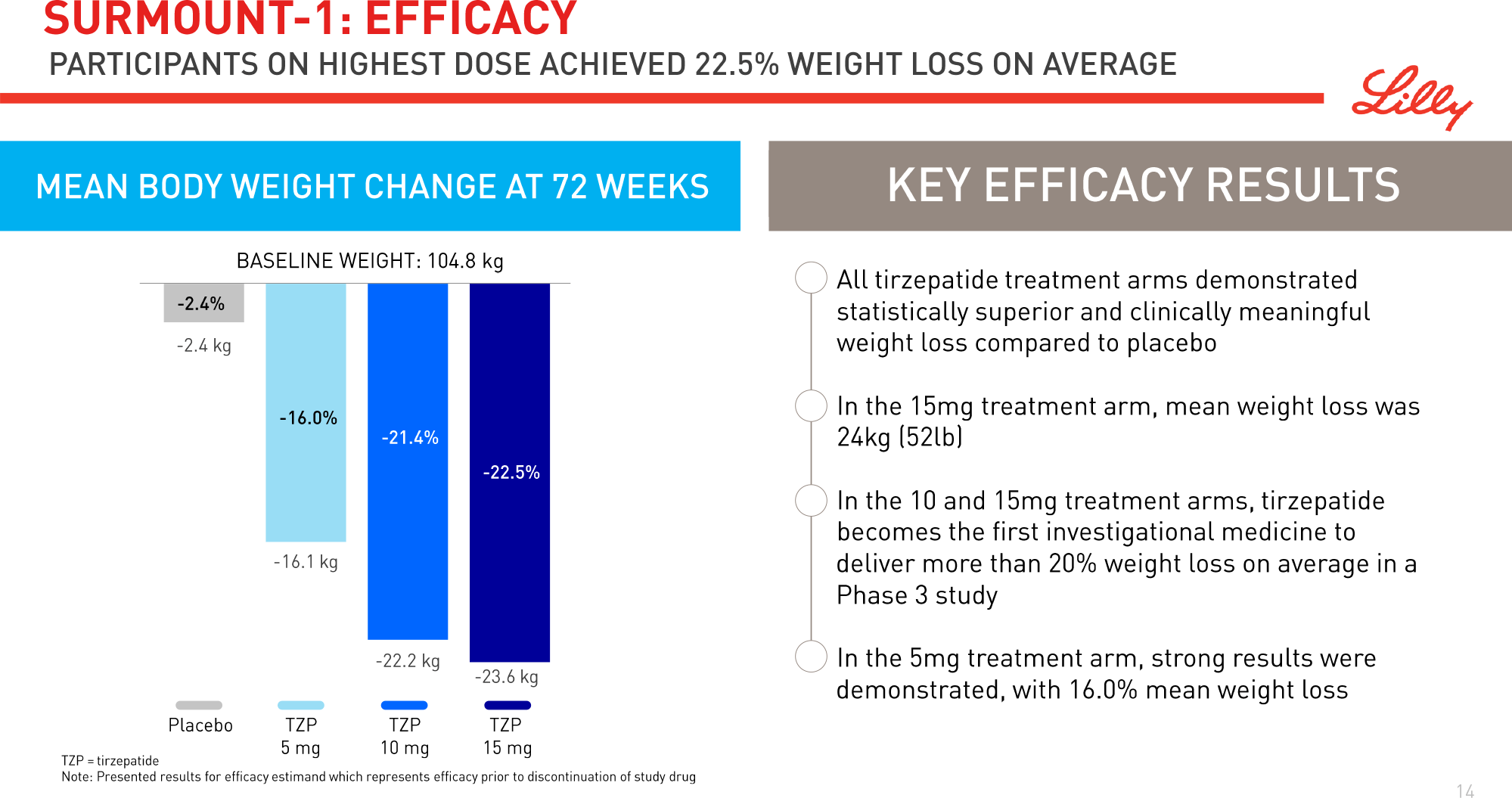
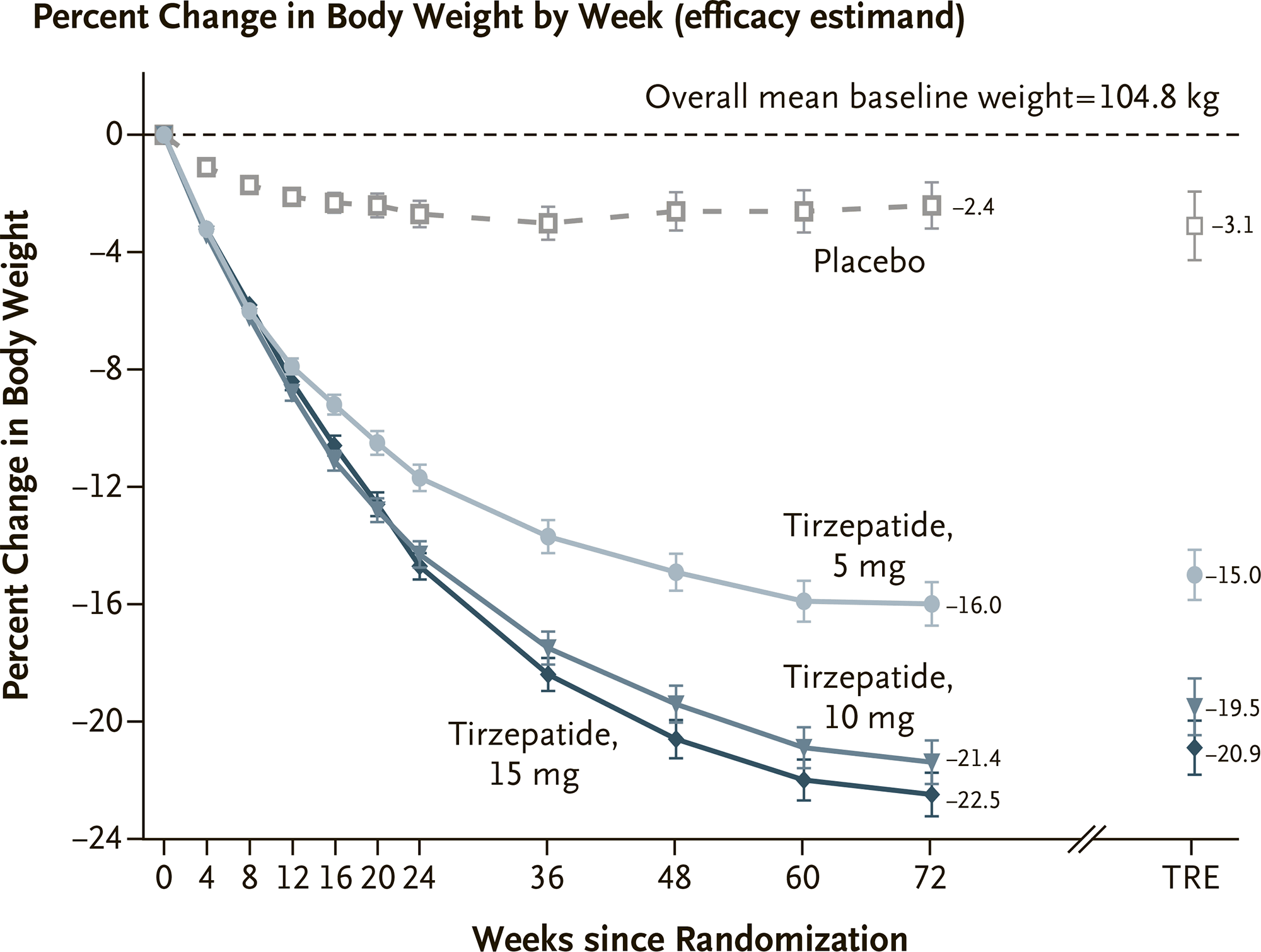
Patients’ baseline weight was an average of 104.8±22.12 kg.
Efficacy of Tirzepatide
The results of the experimental therapy were evaluated in two ways. The first methodology was based on the assumption that patients strictly followed the treatment protocol, did not miss a single dose of the drug and completed the entire course of therapy — the so-called ideal patients. The second methodology assumed an assessment regardless of the degree of adherence to the treatment protocol — a population of patients as close to real patients as possible.
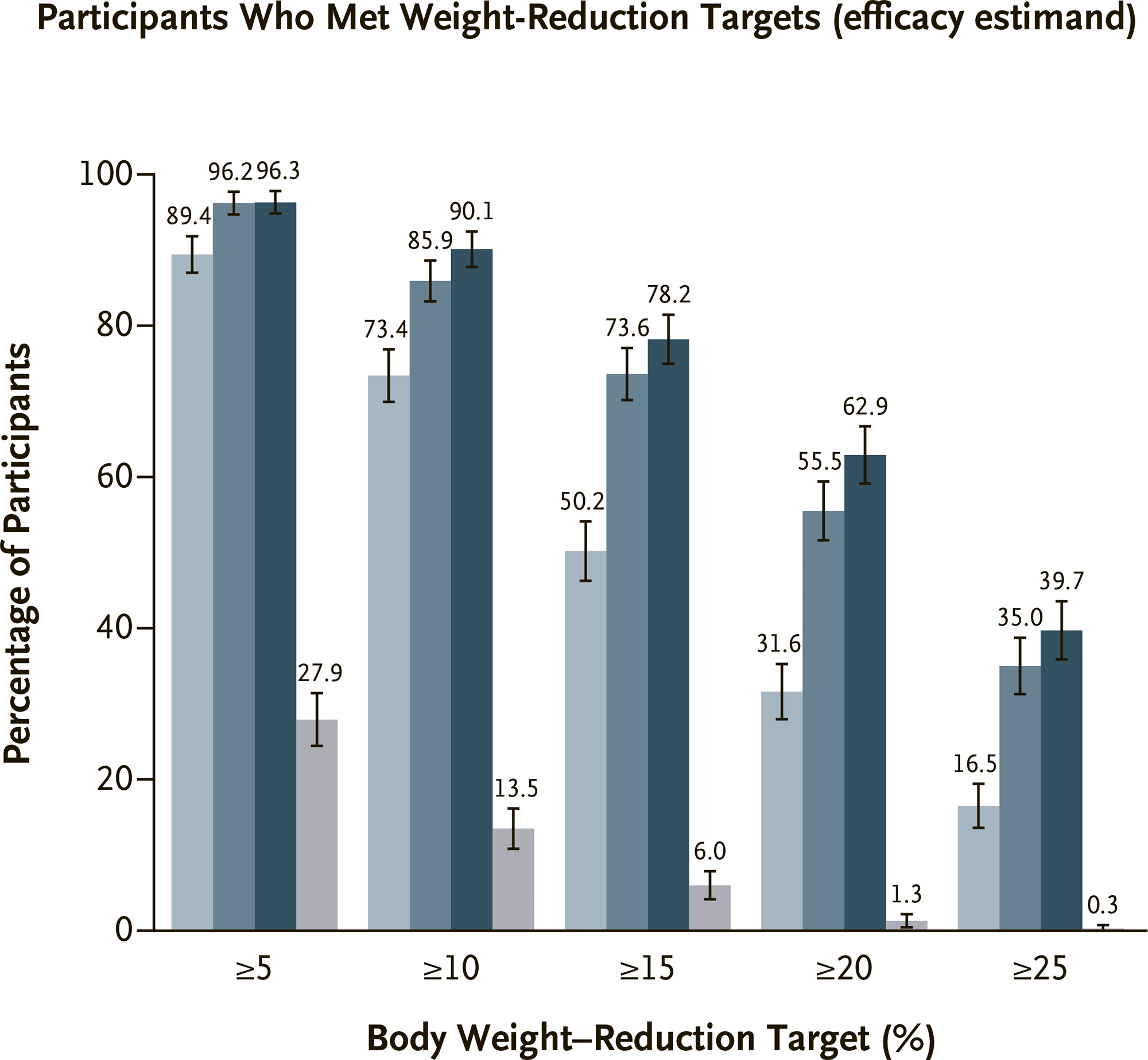
Assessment #1
The mean weight loss in the tirzepatide subgroups (5 mg, 10 mg, and 15 mg) was 16.0% (95% CI: 15.2 to 16.8), 21.4% (95% CI: 20.6 to 22.2), and 22.5% (95% CI: 21.7 to 23.3) — versus 2.4% (95% CI: 1.6 to 3.2) in the placebo group. This was equivalent to a loss of 16.1 kg, 22.2 kg, and 23.6 kg — vs. 2.4 kg.
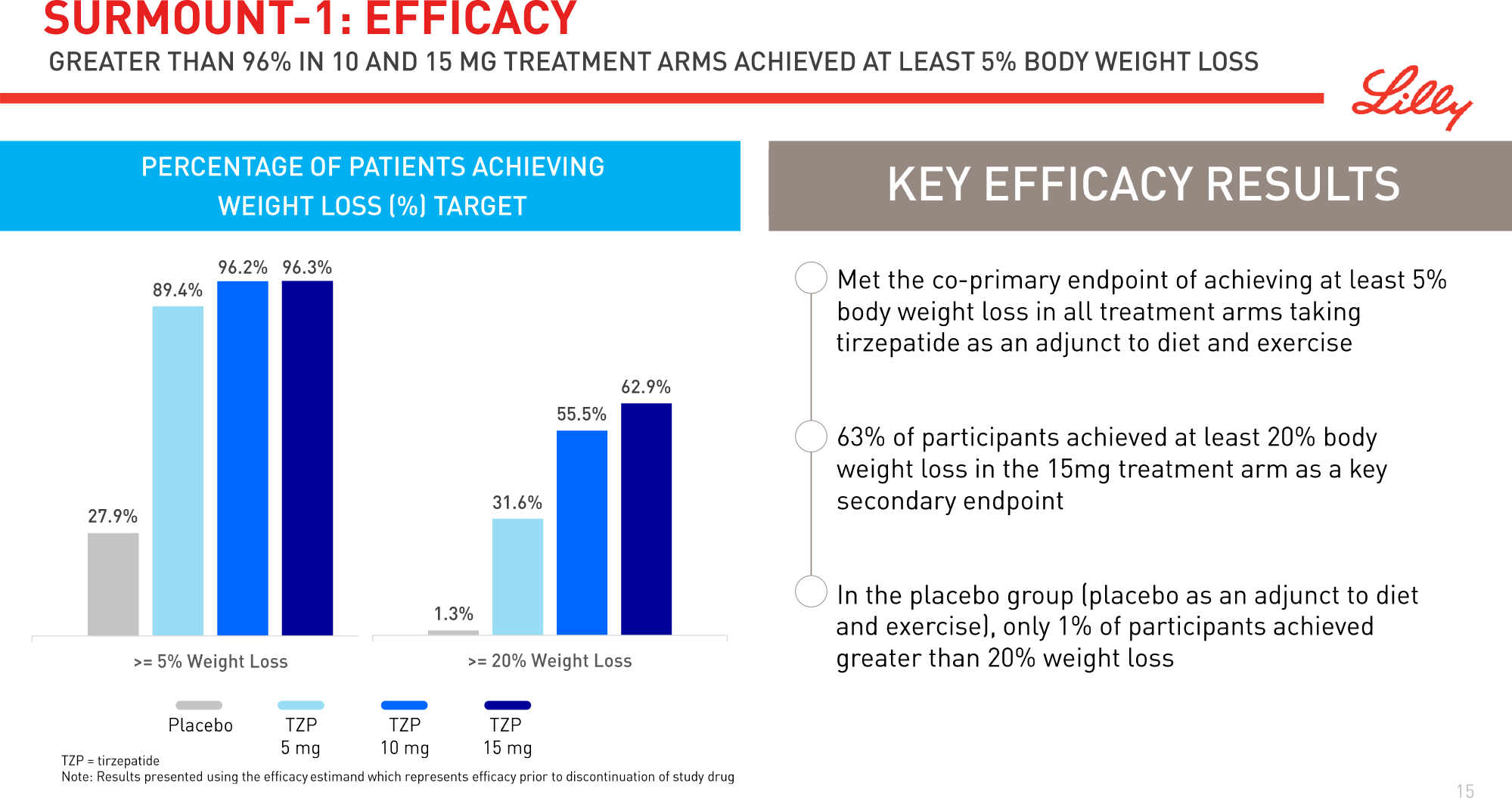
Reductions in excess body weight of at least 5% were reported for 89% (95% CI: 87 to 92), 96% (95% CI: 95 to 98), and 96% (95% CI: 95 to 98) of patients in the above tirzepatide subgroups — vs. 28% (95% CI: 24 to 31) in the control group.
Weight reductions of at least 20% were recorded for 32%, 56%, and 63% of patients receiving tirzepatide at doses of 5 mg, 10 mg, and 15 mg, respectively — vs. 1.3% in the placebo group.
The mean reduction in total fat mass was 33.9% — vs. 8.2%, and the ratio of total fat mass to total lean mass (fat-free) decreased from a baseline of 0.93 to 0.70 — vs. a decrease from a baseline of 0.95 to 0.88.
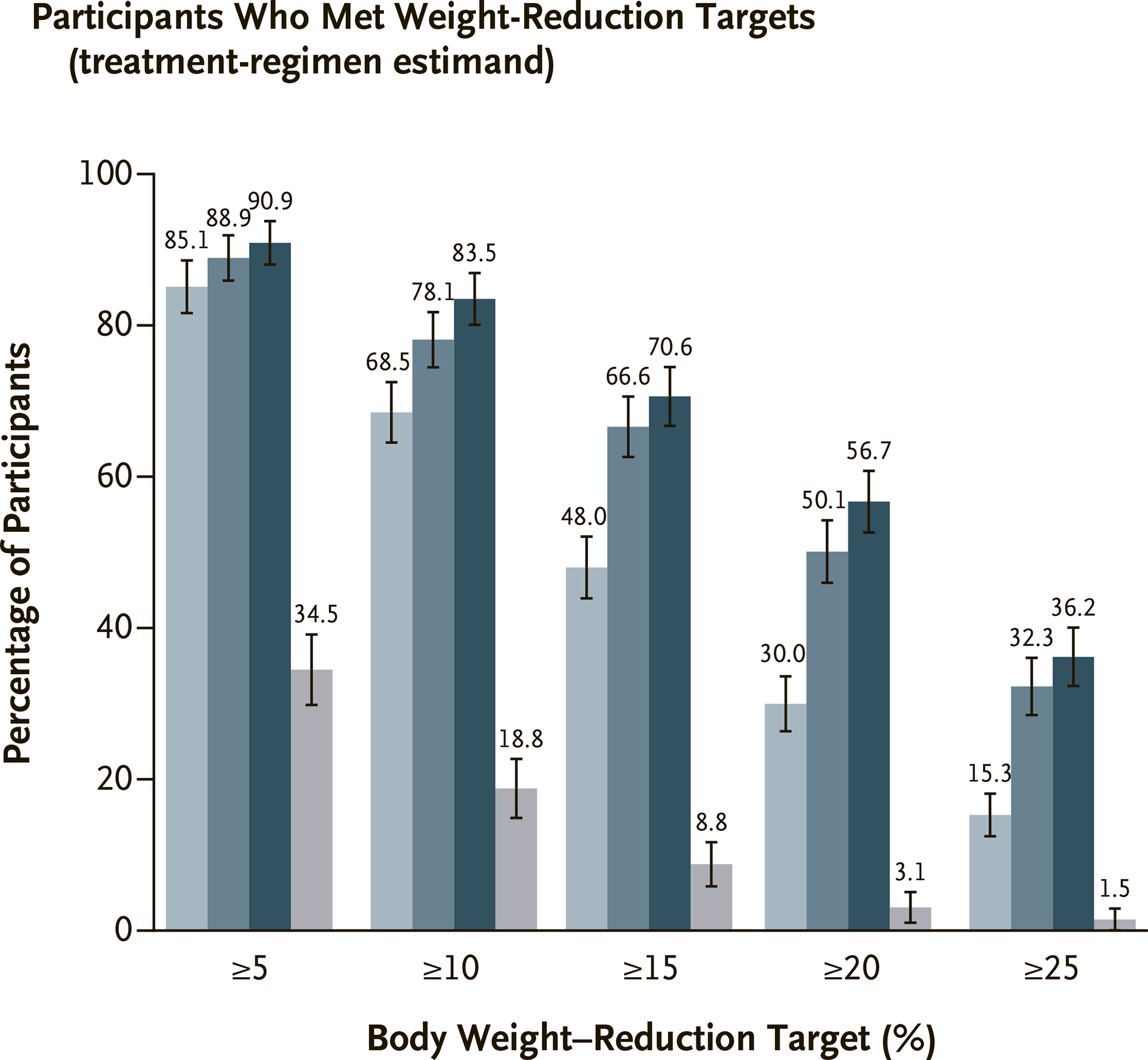
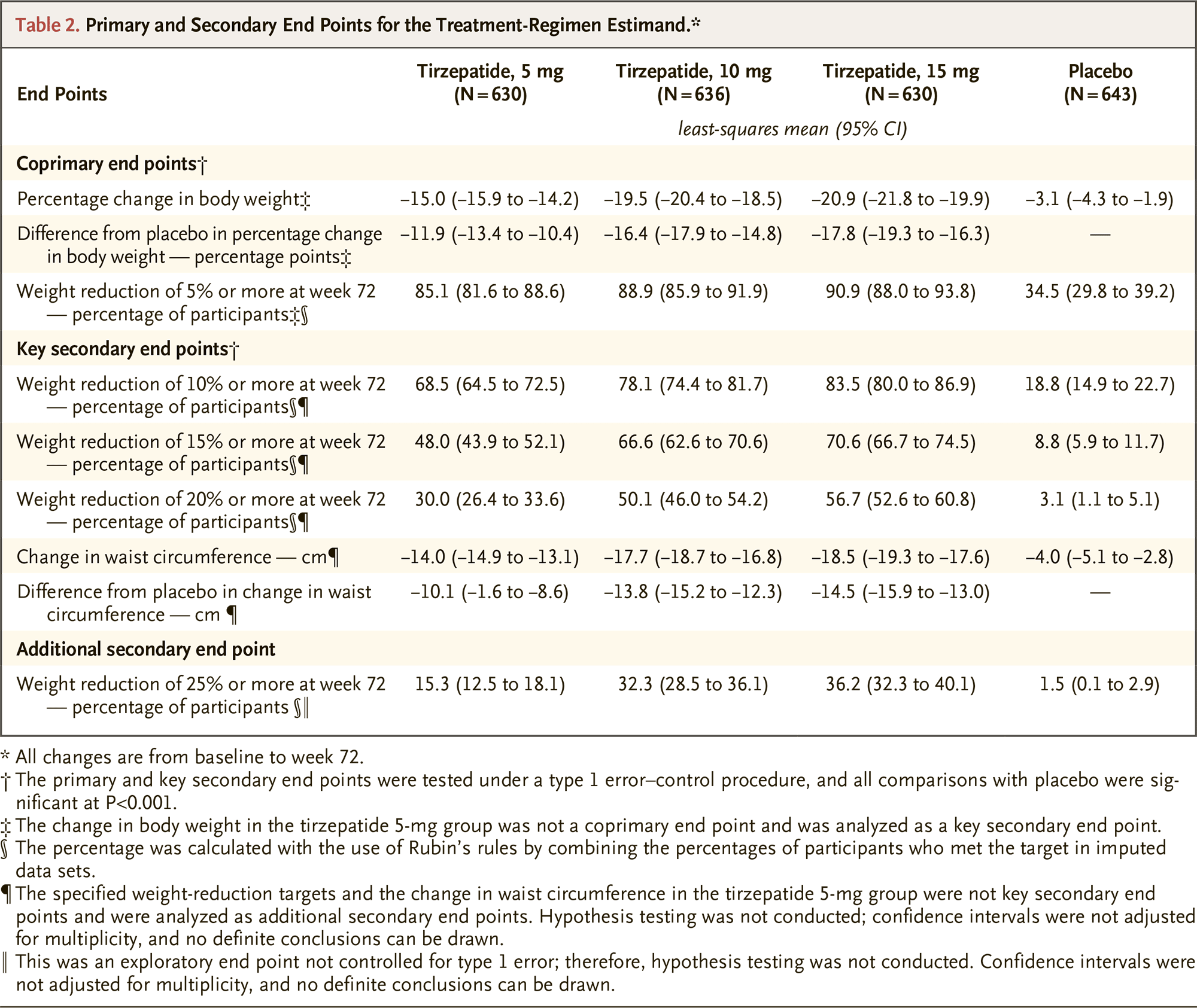
Assessment #2
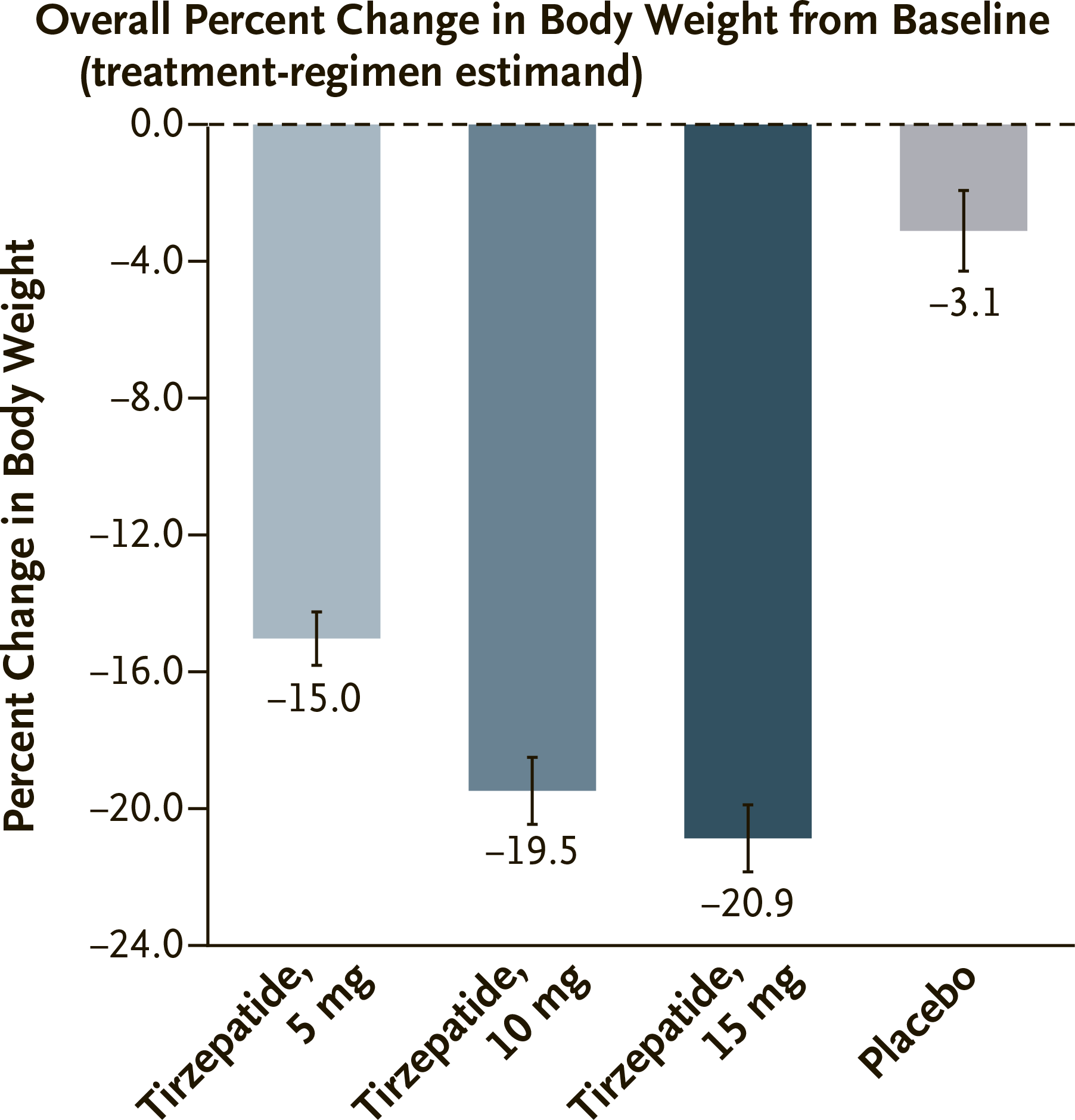
Weight loss in the tirzepatide subgroups (5 mg, 10 mg, and 15 mg) was 15.0% (95% CI: 14.2 to 15.9), 19.5% (95% CI: 18.5 to 20.4), and 20.9% (95% CI: 19.9 to 21.8) — versus 3.1% (95% CI: 1.9-4.3) in the placebo group.
Proportion of patients who lost at least 5% of their body weight was 85% (95% CI: 82 to 89), 89% (95% CI: 86 to 92), and 91% (95% CI: 88 to 94) — vs. 35% (95% CI: 30 to 39).
Proportion of patients who lost at least 20% of their body weight was 30% (95% CI: 26 to 34), 50% (95% CI: 46 to 54), and 57% (95% CI: 53 to 61) — vs. 3.1% (95% CI: 1.1 to 5.1).
Proportion of patients who lost at least 25% of their body weight was 15% (95% CI: 13 to 18), 32% (95% CI: 29 to 36), and 36% (95% CI: 32 to 40) — vs. 1.5% (95% CI: 0.1 to 2.9).
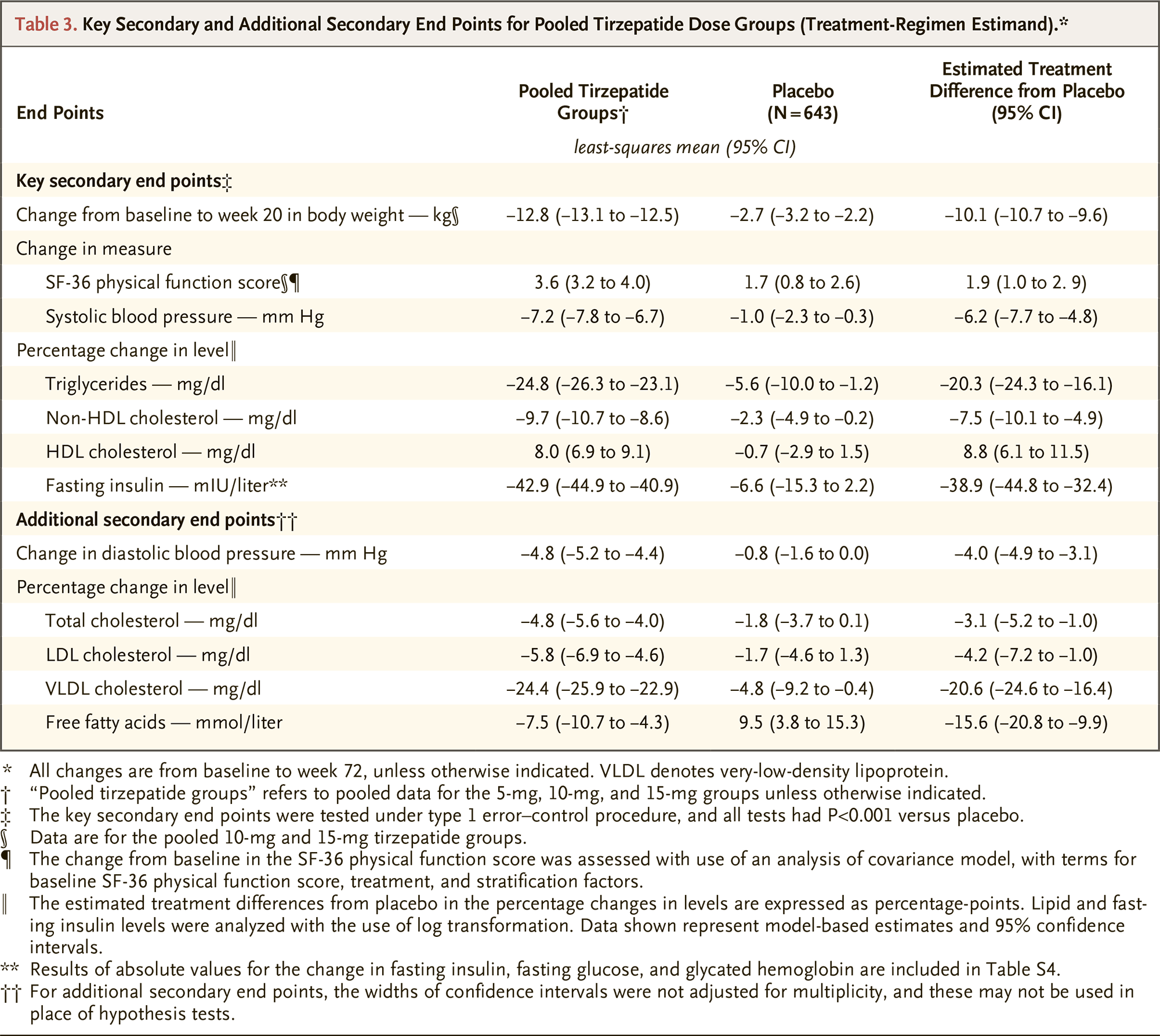
Others
Administration of tirzepatide resulted in corresponding improvements in numerous cardiometabolic parameters, which obviously resulted from weight loss, such as systolic and diastolic blood pressure, glycated hemoglobin (HbA1c), fasting glucose, fasting insulin, triglycerides, cholesterol, free fatty acids, ALT, and AST.
The majority of tirzepatide-treated subjects (95%) who were pre-diabetic before treatment (HbA1c ranging from 5.7% to 6.4%) achieved normoglycemic status — versus 62% in the placebo group.
Safety of Tirzepatide
The administration of tirzepatide did not reveal any new safety concerns. Among the most common adverse events, characterized mostly by mild-to-moderate severity and usually occurred during dose escalation: nausea (in 25%, 33%, and 31% of patients receiving tirzepatide in doses of 5 mg, 10 mg, and 15 mg), diarrhea (19%, 21%, and 23%), constipation (17%, 17%, and 12%), dyspepsia (9%, 9%, and 11%), vomiting (8%, 11%, and 12%), and decreased appetite (9%, 12%, and 9%).
The rates of treatment discontinuation due to adverse events were 4%, 7%, and 6% — versus 3% in the placebo group. The rates of treatment discontinuation for any reason came out to 14%, 16%, and 15% — vs. 26%.
Tirzepatide: Mechanism of Action
Tirzepatide (LY3298176) is a biological drug compound that is an agonist for glucagon-like peptide-1 receptor (GLP-1R) and glucose-dependent insulinotropic polypeptide receptor (GIPR).
Glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) belong to the incretins, a group of metabolic hormones that stimulate blood glucose lowering. The incretins are released after meals, by a glucose-dependent mechanism, enhancing the production of insulin secreted by the beta cells of the islets of Langerhans in the pancreas. Together, GIP and GLP-1 are responsible for secreting approximately 70% of insulin in response to food intake.
From the point of view of the therapeutic reduction of excessive body weight, agonist activation of GLP-1R signaling manifested by delayed gastric evacuation, decreased gastric juice secretion, and weakened gastric motility. All this leads to a suppression of appetite and a decrease in the postprandial rise in blood glucose levels. Among other things: decrease in plasma glucagon levels (glucagon raises blood glucose concentration and promotes gluconeogenesis and glycogenolysis) and activation of anorexigenic pathways in the brain (mediates weight loss).
GIPR agonism, which is expressed in many organs and tissues, including the central nervous system and adipose tissue, and which synergistically complements the effects of GLP-1R, affects appetite and satiety regulation. GIP, unlike GLP-1, simultaneously exhibits glucagonotropic and insulinotropic effects, depending on glycemia; it dose-dependently stimulates glucagon secretion in hypoglycemic conditions and insulin secretion in hyperglycemic conditions.
Tirzepatide or Semaglutide: Which Is Better for Weight Loss?
The closest competitor to tirzepatide is semaglutide, a GLP-1R agonist developed by Novo Nordisk.
Semaglutide, implemented in the form of subcutaneous injections, is available on the market in two drugs: Ozempic is for the therapy of type 2 diabetes and Wegovy is for the reduction of excess body weight.
Comparing the therapeutic efficacy of tirzepatide and semaglutide is methodologically wrong. No relevant clinical trials have been conducted that directly compare these drugs, and studies for each drug vary in both design and patient populations. Nevertheless, it is appropriate to provide Wegovy’s efficacy rates from a trial that approximated the tirzepatide trial as closely as possible.

Wegovy: Most Effective Drug for Weight Loss
At least 20% of the weight will be lost in every third patient.
The STEP 1 (NCT03548935) phase 3 clinical trial examined semaglutide in adult patients (n=1961) without type 2 diabetes, who were obese or overweight and with a history of weight-related comorbidities (hypertension, dyslipidemia, obstructive sleep apnea, cardiovascular disease). The baseline mean weight of the participants was 105,3 kg.
The administration of Wegovy by weekly subcutaneous injections for 68 weeks resulted in a 14.9% reduction in body weight. These are patients whose behavior is closer to reality, that is, assessing therapeutic efficacy does not take into account the degree of adherence to treatment (compliance) and does not take into account the facts of whether patients have taken other weight-loss medications.
If patients were “perfect,” that is, strictly followed the treatment protocol throughout the study and did not use additional weight-loss medications, they were able to lose 16.9% of their excess weight.
Absolute weight loss with Wegovy treatment was an average of 15.3 kg for “normal” patients and 17.4 kg for “perfect” patients.
The proportion of “normal” patients whose weight loss was at least 5% was 87% and at least 20% was 32%. The proportions of “perfect” patients were slightly higher: 92% and 35%, respectively.
As we can see, semaglutide failed to outperform tirzepatide in all measures of weight loss efficacy. First, tirzepatide, when compared to semaglutide, increased weight loss by 5.6%, which was reflected in the reduction of an additional 6.6 kg. Second, 20% or more extra kilograms were lost in nearly two-thirds of patients taking tirzepatide, but only in one-third of patients treated with semaglutide.
In terms of side reactions, the safety profiles of semaglutide and tirzepatide were similar in gastrointestinal (GI) adverse events (AEs), but the former drug was more severely tolerated than the latter. Thus, 44% and 31% of patients who received Wegovy or the maximum 15-mg dose of tirzepatide experienced nausea, 32% and 23% diarrhea, 25% and 12% vomiting, and 23% and 12% constipation. It should be understood that these GI AEs were mild-to-moderate in most cases, were fixed during dose escalation, and disappeared in the course of treatment.
By the way, Wegovy also failed to outperform tirzepatide, even when used with intensive behavioral therapy aimed at lifestyle changes (reduced-calorie diets and increased physical activity). The 68-week STEP 3 (NCT03611582) phase 3 clinical trial demonstrated that in “perfect” patients, semaglutide reduced weight by an average of 17.6%, with a loss of 20% or more body weight in 39% of these patients.
Tirzepatide for Weight Loss: What’s Next
Eli Lilly expected to submit an application to the U.S. Food and Drug Administration (FDA) for tirzepatide for patients with obesity or overweight only after a number of other clinical trials were completed, which would not happen until mid-2023. Now the U.S. drugmaker, encouraged by the superior efficacy of tirzepatide, intends to secure the regulator’s favor by providing it only with the data collected in SURMOUNT-1.
It is possible that Eli Lilly will use its existing priority review voucher to have the FDA review the dossier on an expedited basis.
It should be understood that the demand for anti-obesity drugs is growing relatively slowly. This is mainly due to the fact that all previous attempts at weight loss medication had very modest results: the previous medicines had essentially a cosmetic function rather than a therapeutic one. The situation began to change with the appearance of Wegovy by Novo Nordisk, which offered previously unattainable results in the task of losing excess weight.
According to industry forecasts, Wegovy’s sales will reach an annual $3.9 billion by 2026. That’s why Eli Lilly is passionate about the early launch of tirzepatide against obesity.
In order to finally see the therapeutic validity of tirzepatide in the fight against obesity, Eli Lilly continues its extensive clinical review:
- SURMOUNT-2 (NCT04657003): tirzepatide versus placebo — among patients (n=900) with type 2 diabetes and obesity or overweight adhering to either diet and/or exercise or any oral antidiabetic drug except DPP-4 inhibitors and GLP-1R agonists
- SURMOUNT-3 (NCT04657016): tirzepatide vs. placebo — among patients (n=800) without type 2 diabetes who are either obese or overweight with comorbidities (hypertension, dyslipidemia, obstructive sleep apnea, or cardiovascular disease) and who had previously completed an intensive lifestyle change program
- SURMOUNT-4 (NCT04660643): among patients (n=750) from SURMOUNT-1 who wished to extend the clinical trial
- SURMOUNT-J (NCT04844918) [Japan only]: tirzepatide vs. placebo — among patients (n=260) without type 2 diabetes who are obese and have some associated condition (impaired glucose tolerance, hyperlipidemia, nonalcoholic fatty liver disease) on a low-fat diet and increased physical activity
- SURMOUNT-CN (NCT05024032) [China only]: tirzepatide vs. placebo — among patients (n=700) without type 2 diabetes who are either obese or overweight with comorbidities (hypertension, dyslipidemia, obstructive sleep apnea, or cardiovascular disease)
- SUMMIT (NCT04847557): tirzepatide vs. placebo — among patients (n=700) with obesity and heart failure (NYHA class II–IV) with preserved ejection fraction (LVEF ≥ 50%).
Extras
Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022 Jun 4. [source]